






Languages
Pages
Legal


CLINICAL PROTOCOL FOR MANAGEMENT
OF
CHRONIC OBSTRUCTIVE PULMONARY DISEASE
(COPD) IN COMMUNITY NURSING
November 2014
FAMILY NURSING & HOME CARE RATIFICATION FORM
Type
i.e. Strategy, Policy, Protocol Education Package etc.
Name Management of COPD in the Community
Category Clinical i.e. organisational, clinical,
Corporate, Finance etc
Version 1.0
Author Clare Stewart
Approved by Operational Governance Group i.e. Operational
Governance Group
Date Approved 20/11/14
Review Date 20/11/17
Person
responsible for Clare Stewart
review
Approved by n/a i.e.Sub
Committee, H&SS
Copy of this form to be given to Information Governance Officer
2
RATIONALE
An estimated 3 million people have chronic obstructive Pulmonary Disease (COPD) in the United Kingdom (National Institute for Health and Clinical Excellence [NICE], 2010). Patients with COPD will therefore form a significant percentage of the wider Community Nursing Caseload. The prevalence of COPD in Jersey is currently estimated at 3.8%, 1 of the population aged 16+, which equates to 3,000 individuals. It should be noted that this estimation includes all grades of the disease – mild, moderate and severe. According to the World Health Organisation, approximately 15% of smokers will develop COPD, and by 2020, COPD will be the third leading cause of death and the fifth leading cause of disability.
AIMS
By improving community nurses’ knowledge of COPD and its management it is anticipated that there may be:
A reduction in acute and emergency admissions to hospital and the associated risks
appropriate use of inhaled corticosteroids, bronchodilators and vaccination An improvement in patient self care and management An Improvement in the confidence and clinical skills in COPD
TARGET GROUP
This protocol applies to all community nurses who are required to follow this protocol as part of their job description. Patient centered care will be provided by the most appropriate trained member of the team and this may require joint assessments.
TRAINING
All staff within the organisation are required to attend all the mandatory training and their service specific core training. RELATED POLICIES: Relevant organisational policies are currently in progress by the Respiratory Team and include: Oxygen Policy Peak Flow Policy Inhalers Policy End of Life COPD Policy Nebuliser Policy Pulse Oximetry Policy
DIAGNOSIS OF COPD – (FOR INFORMATION ONLY)
There is no single diagnostic test for COPD. Diagnosis relies on a combination of history, physical examination and confirmation of airflow obstruction using spirometry. COPD is predominately caused by smoking and is characterised by airflow obstruction that is not fully reversible. The airflow obstruction does not change markedly over several months, but is usually progressive in the long
3

term. Exacerbations often occur, when there is a rapid and sustained worsening
of the patient’s symptoms beyond normal day to day variations. A diagnosis of
COPD should be considered in patients over the age of 35 who have a risk factor
(generally smoking, or ex smokers) and present with any of the following:
Exertional breathlessness Chronic cough Regular sputum production Frequent winter ‘bronchitis’ Wheeze
The following clinical features are more suggestive of asthma:
Chronic unproductive cough Significantly variable breathlessness Night-time wakening with breathlessness and/or wheeze Significant diurnal or day to day variability of symptoms
Patients in whom a diagnosis of COPD is considered should also be asked
about the presence of the following factors:
Weight loss Effort intolerance Waking at night Ankle swelling Fatigue Occupational hazards Chest pain Haemoptysis
NB the last two symptoms are uncommon in COPD and raise possibility of
alternative diagnoses. One of the primary symptoms of COPD is breathlessness.
The Medical Research Council (MRC) dyspnoea scale (see table below) should
be used to grade the breathlessness according to the level of exertion required to
elicit it.
Medical Research Council Dyspnoea Scale
Grade degree of breathlessness related to activities
1 Not troubled by breathlessness except on strenuous exercise
2 Short of breath when hurrying or walking up a slight hill
3 Walks slower than contemporaries on level ground because of
breathlessness, or has to stop for breath when walking at own pace
4 Stops for breath after walking about 100 metres or after a few minutes on
level ground
5 Too breathless to leave the house, or breathless when dressing or
undressing 4

Adapted from Fletcher CM, Elmes PC, Fairbairn MB et al. (1959) The significance of
respiratory symptoms and the diagnosis of chronic bronchitis in a working population.
British Medical Journal 2: 257–66
MANAGEMENT OF COPD
COPD care should be delivered by a multidisciplinary team and assessment of the patient should include the following:
Spirometry Assessing the need for oxygen The need for aids for daily living Appropriateness of delivery systems for inhaled therapy Pulmonary rehabilitation Rapid Response/early discharge schemes Palliative care Identifying and managing anxiety and depression Teaching relaxation techniques Advising on dietary issues e.g. weight loss Exercise education
Smoking cessation Social security benefits and travel Self-management strategies Management of exacerbations of COPD
SPIROMETRY
Spirometry is a non invasive test that measures the lungs ability to exhale. Spirometry is usually performed by the patient’s General Practitioner (GP), Hospital in the clinical investigations department or in Respiratory Clinics. It is beyond the scope of this document to outline all the tests performed, however as the forced expiratory volume in 1 second (FEV¹) is used to assess the severity of COPD it is therefore outlined below: The forced expiratory volume after 1 second (FEV¹) is the volume of air in litres
that is forcefully exhaled in the first second of exhalation. In patients with healthy lungs about 70–75 per cent of air is exhaled in the first second.
ADDITIONAL TESTS
At the time of their initial diagnostic evaluation, in addition to spirometry all patients should have:
A chest radiograph to exclude other pathologies
A full blood count to identify anaemia or polycythaemia Body mass index (BMI) calculated.
5
VACCINATION
Infection can complicate COPD and some infections can be prevented by vaccination. All COPD patients should therefore be offered pneumococcal vaccination and an annual influenza vaccination.
MANAGEMENT OF STABLE COPD
SMOKING CESSATION
Record smoking history, including pack years smoked, for everyone withCOPD
People with COPD who smoke must be regularly encouraged to stop
Advise and refer consenting patients to local smoking cessation services
Help2Quit 445015
NUTRITIONAL FACTORS
All patients to have their nutritional status assessed and all patients should be monitored for any rapid weight gain/loss
Body mass Index (BMI) should be calculated in patients with COPD, the normal range for BMI is 20 to less than 25. However, for patients who are South Asian and overweight a BMI should be ideally 23 or less.
If the patient’s BMI is abnormally low, or the patient is underweight or
losing weight consider providing written information and refer to the relevant professional services i.e. dietician
For patients with a BMI greater than 25 who require weight reducing advice, consider referral to Dietetics Department
A reduction in BMI could be associated with an alternative diagnosis and
for those patients who have deterioration in symptoms a referral to a chest
physician may be appropriate for further tests and investigations.
INHALED THERAPY
Recommended use of inhaled therapies for COPD is divided into steps dependent on the presenting symptoms and spirometry results.
Breathlessness and/or exercise limitation
Symptoms may be alleviated by short-acting beta-2-agonists (e.g. salbutamol [Ventolin], or terbutaline [Bricanyl]) or a short acting antimuscarinic bronchodilators (e.g. ipratropium [Atrovent]) used as required. Short acting beta-2-agonists can be continued throughout all stages of COPD. Short acting antimuscarinics should be discontinued on progression of the disease (see below)
Exacerbations or persistent breathlessness
When the airways obstruction is more severe, regular inhaled therapy should be used as follows
If the Forced Expiratory Volume in 1 second (FEV¹) is 50% of predicted or
more: Patients should receive either a long acting antimuscarinic
6
bronchodilator (e.g. tiotropium [Spiriva] ) or a long acting beta-2-agonist
(e.g. formoterol or salmeterol [Serevent])
Short acting antimuscarinic bronchodilators should be discontinued when
a long acting antimuscarinic bronchodilator is started. A long acting beta-2-agonist with a corticosteroid in a combination inhaler
can be used for patients who remain symptomatic despite regular long acting beta-2-agonist
If the Forced Expiratory Volume in 1 second (FEV¹) is less than 50%:
Either a long-acting antimuscarinic bronchodilator or a long-acting beta-2-
agonist with a corticosteroid in a combination inhaler should be used.
Persistent exacerbations or breathlessness
In any patient who remains breathless or continues to have exacerbations, triple therapy with a long-acting beta-2-agonist and a corticosteroid in a combination inhaler plus a long acting antimuscarinic bronchodilator should be used. If an inhaled steroid is not appropriate, a long acting antimuscarinic bronchodilator can be used with a long acting beta-2-agonist. Nurses should be aware of the risk of developing side effects from inhaled therapies and be prepared to discuss the potential side effects to the patient. More information can be accessed here: patient
ASSESS THE EFFECTIVENESS OF INHALED THERAPY
Improvements in symptoms
Activities of daily living Exercise capacity Speed of symptom relief (short acting bronchodilators only)
INSTRUCTION ON INHALER DEVICES
In most cases bronchodilator therapy is best administered using a hand-held inhaler device (including a spacer device if appropriate).
Inhalers should be prescribed only after patients have received training in
the use of the device and have demonstrated satisfactory technique Inhaler technique should be checked at every opportunity to ensure
patients are still receiving optimum doses, as poor technique may be mistaken for lack of response
Check inhaler technique and modify if necessary, consider suitability of
devices used and consider spacer devices
SPACERS
It is recommended that spacers are used in the following way: the drug is administered by one actuation followed by 5 breaths to the prescribed number of actuations (tidal breathing technique)
Spacers should be cleaned monthly as more frequent cleaning affects
their performance (because of a build up of static). They should be
7
cleaned with water and washing-up liquid and allowed to air dry. The
mouthpiece should be wiped clean of detergent before use.
NEBULISERS
SHORT TERM USE
Nebulisers are sometimes loaned for a short period to avoid hospital admission /reduce stay in hospital; this requires a review and reassessment of continual need for nebuliser. If a patient is using a tiotropium inhaler and considering changing to nebuliser, the tiotropium inhaler must be stopped prior to commencement of nebulised antimuscarinic bronchodilator.
LONG TERM USE
Patients with long term distressing or disabling breathlessness despite maximal therapy using inhalers should be considered for nebuliser therapy. Teaching of how to use a nebuliser and implications of prescribed medicines should be performed by a person with the appropriate knowledge and skills. Nebulised therapy should not continue to be prescribed without assessing and confirming that one or more of the following occurs:
A reduction in symptoms An increase in the ability to undertake activities of daily living An increase in exercise capacity An improvement in lung function. Nebulised therapy should not be prescribed without an assessment of the
patient’s and/or carer’s ability to use it Patients will be provided with a mouthpiece to administer their nebulised
therapy
If nebuliser therapy is prescribed, the patient should be provided with equipment, education and support.
Nebuliser filters require changing every three months All nebulisers should be driven by compressed air For advice on caring for your nebuliser refer to nebuliser care plan or
information leaflet.
SERVICING OF NEBULISERS
Nebulisers do not require annual servicing as per manufacturers guidance. They have no servicing for 3 years then annual checks with the Clinical Investigations Department (for standard portaneb nebulisers)
The Clinical Investigation Dept at JGH will check and repair nebulisers if they are taken to the Saturday morning drop in clinic or by arranging an appointment by telephone.
If applicable clinical nebuliser reviews will be carried out at least 3 monthly
by the respiratory specialist team
ORAL STEROIDS
8
Some patients with advanced COPD may require maintenance oral
corticosteroids; this decision is usually made by the consultant. In these cases,
the dose of oral corticosteroids is kept as low as possible and patients should be
taking optimal doses of medication before this is undertaken.
Patients treated with long-term oral corticosteroid therapy should be
monitored for the development of osteoporosis and given appropriate prophylaxis treatment.
Patients under the age of 65 commenced on oral corticosteroids should
have their bone density monitored.
THEOPHYLLINE
For a small number of patients theophylline may be added if breathlessness continues to be a concern despite other therapies
Theophylline should be used with caution, because serum levels can be elevated due to interactions with other medications, including some antibiotics, smoking, heart failure, hepatic impairment, viral infections or in the elderly.
Differences in the half life of theophylline are important because the toxic
dose is close to the therapeutic dose. Measurement of plasma-
theophylline concentration may therefore be helpful – recommended 3-6 monthly dependant on physician preference
ORAL MUCOLYTIC THERAPY
Mucolytic drug therapy should be considered in patients with a chronic cough who have difficulty expectorating sputum
Mucolytic therapy should be continued if there is symptomatic improvement (for example, reduction in frequency of cough and sputum production or exacerbation)
Do not routinely use mucolytic drugs to prevent exacerbations in people
with stable COPD.
ANTI-TUSSIVE THERAPY (COUGH PREPARATIONS)
Anti-tussive therapy should not be used in the management of stable COPD.
ORAL PROPHYLACTIC ANTIBIOTIC THERAPY
There is insufficient evidence to recommend prophylactic antibiotic therapy in the management of stable COPD.
PULMONARY REHABILITATION
Pulmonary rehabilitation should be made available to all appropriate people with COPD including those who have had a recent hospitalisation for an acute exacerbation
OXYGEN THERAPY
LONG-TERM OXYGEN THERAPY (LTOT)
9

Clinicians should be aware that inappropriate oxygen therapy in people with
COPD may cause respiratory depression. LTOT is indicated in patients with
COPD who have been assessed by the Oxygen service in clinical investigations
department JGH.
To get the benefits of LTOT patients should breathe supplemental oxygen
for at least 15 hours per day; there is no greater benefit of remaining on
oxygen longer than 20 hours per day. Most patients requiring oxygen for more than 15 hours per day will not
normally need ambulatory oxygen. However, this does not exclude this cohort from assessment for ambulatory oxygen should they feel they require it.
Patients should be warned about the risks of fire and explosion if they
continue to smoke when prescribed oxygen. All patients must have a risk assessment and specific care plan for the
management of oxygen therapy. (standard template for this can be obtained on central filing)
AMBULATORY OXYGEN THERAPY
Ambulatory oxygen therapy should only be prescribed after an appropriate assessment has been performed by a specialist. The purpose of the assessment is to assess the extent of desaturation, and the improvement in exercise capacity with supplemental oxygen, and the oxygen flow rate required to correct desaturation.
Small light-weight cylinders, oxygen-conserving devices are available for the treatment of patients with COPD.
A choice about the nature of equipment prescribed should take account of the hours of ambulatory oxygen use required by the patient and the oxygen flow rate required.
SHORT BURST OXYGEN THERAPY (SBOT)
Short-burst oxygen therapy is not routinely considered for COPD patients.
In some instances short-burst oxygen therapy may be prescribed if there is an improvement in breathlessness following therapy and this is documented following assessment.
SBOT can be beneficial for palliative care patients to reduce
breathlessness although there is no clinical evidence to support this.
FAN THERAPY
Patients should be encouraged to use hand held fans or bigger fans to help with the movement of air; this lowers their perception of breathlessness by stimulating their chemoreceptors
EXACERBATION OF COPD
MANAGEMENT OF EXACERBATIONS
10
An exacerbation is a sustained worsening of the patient’s symptoms from their
usual stable state which is beyond normal day-to-day variations, and is acute in
onset. (A COPD Pathway will be available for the clinical management of acute
exacerbation)
PHYSIOTHERAPY
If patients have excessive sputum, they should be taught the use of active cycle of breathing techniques, consider referral to physiotherapy services. (Referral form on Central Filing)
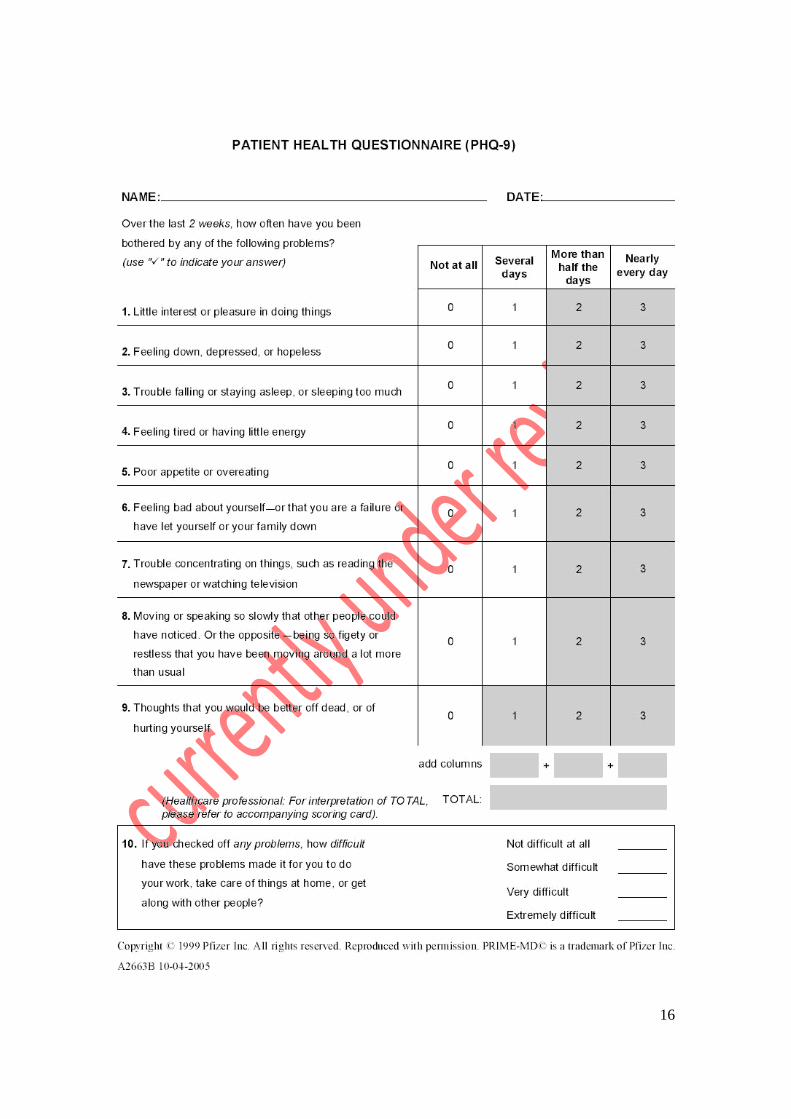
DEPRESSION AND ANXIETY
The presence of depression and anxiety should be considered in all patients with stable COPD, patients should be assessed using appropriate tools by approved trained person. The HADS score is preferred whilst in hospital, the PHQ9 (Appendix 1) is preferred in the community setting. Anxiety and breathlessness is a recognised feature of COPD. Sudden bouts of breathlessness can be debilitating and cause fear and panic. It is essential that this is recognised and treated to prevent exacerbation and hospital attendance.
PALLIATIVE CARE
People with advanced COPD and their carers must be offered palliative care that addresses physical, social and emotional needs. For advice contact the Palliative Care Clinical Nurse Specialist &/or the Respiratory Care Clinical Nurse Specialist until FNHC approved End Of Life guidelines completed.
ASSESSMENT FOR OTHER SERVICES
Occupational Therapy
Patients should be regularly asked about their ability to undertake activities of daily living and how breathless they become when carrying out these activities
If a patient requires assessment for a wheelchair or other equipment the
clinician should make a referral to Occupational Therapy
Social Services
Patients disabled by COPD should be offered referral to social services department for assessment and if appropriate information about available benefits.
Voluntary Organisations
All patients can access the respiratory voluntary services available in Jersey who can offer support and advice;
Jersey Asthma & Respiratory Society - 01534 499774 Breathing Space Group- www.gov.je/BreathingSpace Respiratory Information Mornings , Jersey General Hospital (Saturdays
only ) 01534 442554
11
EDUCATION AND SELF MANAGEMENT
Advice on Travel
All patients on LTOT planning air travel should be assessed in line with the British Thoracic Society recommendations (BTS, 2002) and can be referred to the clinical investigation department (respiratory physiologist)
EXACERBATION OF COPD All patients with COPD should be advised to:
Keep warm in winter
Keep well hydrated Keep all windows closed in the house in winter after dusk Maintain a good diet taking meals little and often Be educated to recognise the signs and symptoms of exacerbation (see
section below for signs and symptoms) Remember the importance of remaining active Patients should be encouraged to start antibiotic therapy if their sputum is
purulent adjusting their bronchodilator therapy to control their symptoms. The appropriate use of antibiotics should be monitored.
Patients should be aware of side effects of increasing bronchodilators Patients given self-management plans should be advised to contact a
healthcare professional when experiencing an exacerbation, so that the patient may be closely monitored and supported and further rescue supplies given.
When experiencing exacerbations all patients need to be closely
monitored and supported
IF ANY CONCERNS SEEK ADVICE ESPECIALLY IF PATIENT HAS COMMENCED
MEDICATION AND THERE IS FAILURE TO RESPOND TO TREATMENT
PRIMARY CARE
In patients who have their exacerbation managed in primary care the sending of a sputum sample for culture is not recommended as routine practice. However this may be useful for those patients who do not respond to treatment or have frequent exacerbations
SIGNS AND SYMPTOMS OF EXACERBATION Increased shortness of breath Pyrexia
Fatigue
Generally unwell
Cough
Changes to sputum colour, consistency and volume
Increased respiratory rate and/or cyanosis
Reduction in activities of daily living
Headache / Confusion – may indicate hypercapnia in some patients
12
INVESTIGATIONS / CONSIDERATIONS Oxygen saturation levels Blood Pressure
Pulse Temperature
Respiratory rate NEWS score
Bloods – FBC, CRP, UEs, Glucose, ABGs (if able) theophylline levels if applicable
Sputum C&S – only if indicated Early intervention and treatment key in managing exacerbation
Check if your patient has a home rescue pack, if initiating home rescue pack
ensure patients contact the Respiratory specialist nurse team for assessment
and support to ensure timely and safe treatment, and obtain a replacement
rescue pack (If appropriate)
PHARMACOLOGICAL MANAGEMENT
Increased breathlessness is a common feature of an exacerbation of COPD. This is usually managed by taking increased doses of short-acting bronchodilators.
Both nebulisers and hand-held inhalers can be used to administer inhaled therapy during exacerbations of COPD. Doses of bronchodilators through hand held inhalers will need to be increased.
The choice of delivery system should reflect the dose of drug required the ability of the patient to use the device and the resources available to supervise the administration of the therapy.
If nebulisers are used for an exacerbation these should be gradually reduced when their condition has stabilised and the medication continued through hand-held inhalers if possible.
Systemic corticosteroids
Prednisolone 30 mg orally should be prescribed for 7 to 10 days.
It is recommended that a course of corticosteroid treatment should not be
longer than 14 days, as there is no advantage in prolonged therapy. If the patient has taken steroids for less than 21 days, the patient can stop
steroid therapy without the need for tapering the dose. However if the patient has had several courses in the year and these have been relatively close together it may be better to reduce slowly. These patients should be referred for close monitoring by the most appropriate person.
Antibiotics
Refer to HSSD / Community antimicrobial guidelines if available otherwise utilize NICE / GOLD COPD guidelines
CARERS ASSESSMENT
13
All informal carers caring for patients with a long term condition must be offered
carers assessment, if a carer declines an assessment this must be recorded in
the patient’s health records. If a carer’s assessment is required refer to social
services department for a full assessment.
WHERE TO GET ADVICE FROM
If specialist advice is required contact Respiratory team for advice at JGH – 444226 Consultant Microbiologist Ivan Muscat - 442596
INCIDENT REPORTING
Clinical incidents or near misses must be reported using the Organisational Incident reporting system
SAFEGUARDING
In any situation where staff may consider the patient to be a vulnerable adult, they need to follow the organisational Safeguarding Adult Policy and discuss with their line manager and document outcomes.
EQUALITY ASSESSMENT
The organisation has considered the clinical needs of each protected characteristic (age, disability, gender, gender reassignment, pregnancy and maternity, race, religion or belief, sexual orientation). There is no evidence of exclusion of these named groups. If staff become aware of any clinical exclusions that impact on the delivery of care, the incident should be reported using the organisational Incident Reporting System and an appropriate action plan put in place. If any concerns re this section discuss with your operational lead who may take further advice from the Senior Management Team
REFERENCES
Fletcher CM, Elmes PC, Fairbairn MB et al. (1959) The significance of respiratory
symptoms and the diagnosis of chronic bronchitis in a working population. British
Medical Journal 2: 257–66
States of Jersey (2012) Long-term Condition Management in the Community: Commencing with Chronic Obstructive Pulmonary Disease (COPD) Scheme- level Outline Business Case (OBC) http://www.gov.je/SiteCollectionDocuments/Government%20and%20administrati on/R%20HSSD%20OBC%20COPD%2020120912%20MC.pdf
National Institute for Clinical Excellence (2004) Chronic obstructive pulmonary Disease: Management of chronic obstructive pulmonary disease in adults in primary and secondary care. http://www.nice.org.uk/nicemedia/pdf/CG012_niceguideline.pdf Guideline
14
National Institute for Health and Clinical Excellence (2010) Chronic Obstructive
pulmonary Disease: Management of chronic obstructive pulmonary disease in
adults in primary and secondary care (partial update) NICE Clinical Guideline 101 http://guidance.nice.org.uk/CG101
National Institute for Health and Clinical Excellence (2011) Chronic Obstructive Pulmonary Disease Quality Standards http://www.nice.org.uk/guidance/qualitystandards/chronicobstructivepulmonarydi sease/copdqualitystandard.jsp
15
16

17
Top Related