






Languages
Pages
Legal


Nutritional Aspects of Eating Disorders
Glenda McPherson, MA, RD
Clinical Dietitian, Unity Health System
February 29, 2008

Nutrition program purpose
• Identify treatment team members and their roles.• Discuss cycles of eating disorders as they relate to
nutrition treatment.• Explain specific tasks of nutritionist on treatment team.• Increase understanding of food-related behaviors from
individual point of view.• Explain rationale for nutrition treatment approaches.• Give examples of treatment strategies.• Identify signs of recovery.
Eating disorder treatment team
Team must be multidimensional and must address• biochemistry• physiology • psychological issues• behaviors

Eating disorder treatment team
To change food-related behavior permanently the following aspects must be addressed concurrently:
• Medical• Nutritional• Pharmacological• Psychological

Cycles in eating disorders
• Family • Individual • Environment, culture• Stressors• Behaviors
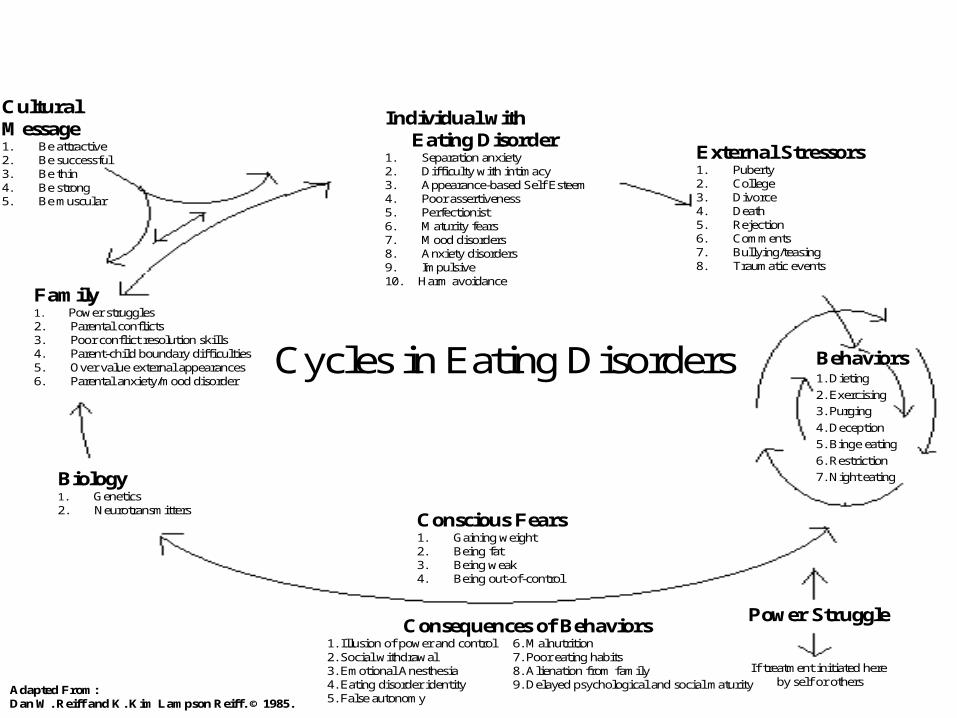
Cycles in Eating Disorders Behaviors1. Dieting
2. Exercising
3. Purging
4. Deception
5. Binge eating
6. Restriction
7. Night eating
Power Struggle
If treatment initiated hereby self or others
Conscious Fears1. Gaining weight2. Being fat3. Being weak4. Being out-of-control
Consequences of Behaviors1. Illusion of power and control 6. Malnutrition2. Social withdrawal 7. Poor eating habits3. Emotional Anesthesia 8. Alienation from family4. Eating disorder identity 9. Delayed psychological and social maturity5. False autonomy
Biology1. Genetics2. Neurotransmitters
Family1. Power struggles2. Parental conflicts3. Poor conflict resolution skills4. Parent-child boundary difficulties5. Over value external appearances6. Parental anxiety/mood disorder
Individual withEating Disorder
1. Separation anxiety2. Difficulty with intimacy3. Appearance-based Self Esteem4. Poor assertiveness5. Perfectionist6. Maturity fears7. Mood disorders8. Anxiety disorders9. Impulsive10. Harm avoidance
External Stressors1. Puberty2. College3. Divorce4. Death5. Rejection6. Comments7. Bullying/teasing8. Traumatic events
CulturalMessage1. Be attractive2. Be successful3. Be thin4. Be strong5. Be muscular
Adapted From:Dan W. Reiff and K. Kim Lampson Reiff. © 1985.

Role of the nutritionist
Provide nutrition therapy:• education• cognitive behavioral therapy• family therapy• health belief modelLevel of involvement depends on team, division of
responsibilities within the team, dietitian’s background or experience.
With Maudsley Approach, nutritionist acts as a consultant to the family, as needed by the family.

Goals of the nutritionist
• Guide the individual or family in developing a healthy relationship with food tonormalize eating patterns.maintain a healthy/stable weight range.
• Communicate with team members throughout the process.

Tasks of the nutritionist
Educate individual and family about normal and abnormal• food intake patterns.• hunger patterns.• somatic sensations resulting from above.

Eating Disorders
Binge Eaters
Chronic Dieters
Overeaters
Occasional Dieters
Normal Eating
Dysfunctional Eating
Dieting and bingeing are the norm—
disordered eating

Optimal (normal), “healthy” eating
• Promotes clear thinking and mood stability.• Fosters healthy relationships in family, work, school,
community. Thoughts of eating, food, and weight 10–15% of day.
• Nurtures food health, vibrant energy, and healthy growth and development. Stable weight results expressing genetics and (appropriate) environment.
Reference: Berg, F. (2001) Afraid to Eat: Children and Teens in Weight Crisis.
Optimal, “healthy” eating (continued)
• Includes eating at regular times and regulation mostly by internal signals of hunger, appetite and fullness/satiety.
• Enhances feelings of well-being. Involves eating for nourishment, energy, health, pleasure, social reasons. After eating, you feel good!
• Reflects food choices that are varied, moderate in amounts, and balanced in nutrient composition.
Reference: Berg, F. (2001) Afraid to Eat: Children and Teens in Weight Crisis.

Disordered/dysfunctional eating
• Irregular and chaotic eating patterns (fasting, bingeing, dieting, skipping meals; undereating or overeating); feel bad after eating.
• Feeling fatigued, irritable, moody, chilled, less able to concentrate, and increasingly self-absorbed; thoughts of food, eating, weight 20 to 65% or more.
Reference: Berg, F. (2001) Afraid to Eat: Children and Teens in Weight Crisis.
Case 1
• Female• 15 years old• Lost 15 pounds in less than two months• Star middle distance runner on track team• Same eating pattern for two months

Typical Food Intake PatternTime of Day
6:15–7:00 a.m.7:00–7:15 a.m.10:00 a.m.
12:00 noon–12:20 p.m.2:00 p.m. 3:00–5:00 p.m. 6:30–7:45 p.m.7:45–8:00 p.m.
9:00 p.m.
Food Eaten or Exercise Done
1 c. skim milk1 1/2 c. Special K Pushups and crunches, 50–100 each2 c. waterBagel, apple, Diet CokeGummy bears, 2 c. waterTrack practice2 oz. chicken, 1 c. fast-food yogurt200 crunches1 c. salad, fast-food dressing, Diet CokeApple

Missing nutrients
• Carbohydrates• Protein• Essential fat• Vitamins• Minerals • Water

Most commonly eliminated foods
• Red meat• Fats and foods containing fat• Desserts• High-quality protein especially if vegetarian• Breads (complex carbohydrates)• High-sugar foods—juices

Effects of restriction
• Obsession with food and eating• Tendency to binge eat in some cases• Increase in oral behavior: chewing gum, drinking water
or diet soda• Intensification of negative body image• Breakdown of natural mechanisms for determining
hunger and satiety• Physical problems: constipation, light-headedness,
feeling cold• Lowered metabolic rate• Rituals

Typical hunger pattern for person with anorexia nervosa
• Wants to feel hungry all the time. • Hunger = control.• Intense hunger needs to be present to
legitimize eating.• Eating to fullness and to the slightest
stomach expansion is frightening.

6 7 8 9 10 11 12 1 2 3 4 5 6 7 8 9 10 11 12 1 2 3 4 5 6
10
9
8
7
6
0
1
2
3
4
5
PM AMAM
ANOREXIA NERVOSA
NORMAL
Time (one day in hours) Adapted from Reiff, D. W. & Reiff, K. K. (1991) Eating Disorders: The Health Professional’s Guide to the Process of Recovery.
Typical hunger pattern Person who has anorexia nervosa
Compared with a person who has recovered
Intense Hunger
Moderately Intense Hunger
Minimal Hunger
No Hunger
Moderate Hunger
Biochemical changes
Food intake
Carbohydrate
SerotoninDepressionOC thoughtsGastroparesis

Tasks of the nutritionist
Assist individual in understanding connection between emotions and behaviors enabling her or him to nourish the body and deal with emotions separately.

Nutrition therapists access feelings by
• Getting to know the person.• Teaching the language of feelings.• Listening.• Teaching that “fat” is not a feeling and decode its
feelings.• Helping to identify feelings.• Exploring the correlation between use of food
and dealing with feelings.

One helpful technique is food journals
Journals are used to:• empower—identify and describe patterns;
self-assessment.• develop confidence in food.• identify hunger/fullness patterns; challenge false
beliefs.• identify cognitive distortions.• be a private communication between
nutritionist/therapist and child and are not to be monitored by parents.
Journals are not typically used with initial phases of the Maudsley Approach.

Dietary treatment for anorexia nervosa
• Cease weight loss.• Establish regular eating: every 3 to 4 hours.• Establish meal plans.
Gradually increase calorie levels depending on individual’s needs and treatment model being used.
Consider likes/dislikes. Include protein, carbohydrate, fat.
• Maintain adequate hydration.• Eliminate diet foods, caffeine.• Use supplements if necessary and only during initial
stages of treatment.

Processing in anorexia nervosa
• Help individual process food fears and other distortions. Cognitive behavior therapy
• Explain the physiology of starvation.• Work to identify and accept internal cues and
respond appropriately.• Help patient process gradual increases in
weight.• Help to legitimize eating.

Tips for parents/caretakers
• Provide food to support treatment plan as communicated by individual.
• Individual determines how much and whether to eat unless she or he is in initial stage of Maudsley Approach, in which case parent(s) decide.
• Avoid talk and questioning about food (e.g., “What did you eat at school today?”).
• Avoid talk about body size or weight of self or others! Focus on feelings and other matters.
• Sit down together for meals as often as possible; insist on sitting during family meal.
• Avoid power struggles with individual about eating disorders.

Case 2
• Female• 17 years old• Normal weight• Started acting

Typical food intake pattern
6:00 a.m. 1 grapefruit
12:00 noon 1 apple, ½ bagel, 1 nonfat yogurt
7:00 p.m. 4 c. salad greens
10:00–10:30 p.m. 1 brownie, 1 granola bar, 1 bagel, 2 c. dry cereal, 1 bag chocolate chip cookies, 1 box animal crackers, ½ coffee cake, 1 pt. ice cream
Afterward Guilt

Time (one day in hours)
6 7 8 9 10 11 12 1 2 3 4 5 6 7 8 9 10 11 12 1 2 3 4 5 6AM
10
9
8
7
6
0
1
2
3
4
5
PM AM
Typical hunger and food intake patternPerson who has bulimia nervosa
Intense Hunger
Moderately Intense Hunger
Minimal Hunger
No Hunger
Moderate Hunger
Several cups coffee over one hour
Gum
2 cups coffee over ½ hour and one apple
Three hard candies
Ice cubes
Salad
Gum
One cup coffee
Three hard candies
Gum
Celery & carrot sticks
One diet pop
BingePurge followed by drinking one diet pop and chewing one package gum
Large salad
Gum
Two cups coffee
Continuous binge
Binge
Purges followed by drinking one diet pop and chewing one package gum
Adapted from Reiff, D. W. & Reiff, K. K. (1991) Eating Disorders: The Health Professional’s Guide to the Process of Recovery.
Binge eating disorder
• Similar to bulimia nervosa; absence of purging behaviors.
• Ongoing and/or repetitive cycles often includeunusually fast eating, usually alone.unusually large amounts consumed.uncomfortably full; often “buzzed” after eating.embarrassment, shame, guilt, depression.

Dietary treatment for bulimia nervosa and binge eating disorder
• Set healthy weight range.• Keep food journal: food, timing, thoughts,
feelings, events—difficult for these disorders.• Record hunger cues and feelings to uncover
distortions. • Experience weight control without purging to
build trust and self-esteem.• Encourage moderate, regular exercise.

Dietary strategies for bulimia nervosa or BED
Establish regular eating and stabilize weight:• Identify safe and unsafe foods.• Set an agreed-upon food and eating plan (will vary with
treatment approach).• Include adequate protein, fat, carbohydrate. Incorporate
high-bulk foods: fruits and veggies. Work with trigger foods to fit intervention strategy—team will decide.
• Help maintain adequate nutrition.• Include food in first part of day.
BreakfastLunch

Tips for parents
• Same as for anorexia nervosa.• Request that individual eat at the table.• Make eating pleasurable.• Focus on positive aspects of food other
than nutrient content.• Eliminate specific binge trigger foods from
home if necessary.

Tools of the trade (varies among nutritionists)
• Food journals• Food acceptance/fears survey• Beliefs about food, hunger, and weight• Good foods/bad foods• Others

Indicators of recoveryIt takes time!
• Metabolic rate• Variety of foods• Body symptoms: menstruation, thermoregulation, hair
and skin health, dental health, energy, digestion and absorption
• Weight shifts• Food consumption pattern
Reference: Reiff, D. W., and Reiff, K. K. (1991) Eating Disorders: The Health Professional’s Guide to the Process of Recovery .

Indicators of recovery (continued)
• Hunger• Amount of time spent thinking about food, body,
weight• Exercise level• Caloric intake• Food fears• Weight• Social eating
Reference: Reiff, D. W., and Reiff, K. K. (1991) Eating Disorders: The Health Professional’s Guide to the Process of Recovery.

The end
“Eating with hunger is about beginning to know the self on an intimate level. It is about feeling entitled to take care of the self. It is about being okay with the self. For those moving away from eating problems, eating with hunger is about forming a new, healthy, nurturing relationship with the self.”
Reference: Johnston, Anita. Eating in the Light of the Moon.

ReferencesBerg, F. M. (2001) Children and Teens Afraid to Eat: Helping Youth in
Today’s Weight Obsessed World. Hettinger, N.D.: Healthy Weight Network.
Garner, D. M. (1997) “Psychoeducational Principles in Treatment.” In Garner, D. M., and Garfinkel, P. E., eds., Handbook of Treatment for Eating Disorders, 2nd ed., pp. 145–177. New York: Guilford Press.
Glanz, K., Lewis, F. M., and Rimer, B. K. (1997) Health Behavior and Health Education: Theory Research, and Practice, pp. 153–178. San Francisco: Jossey–Bass.
Kratina, K. (1993) Counseling Forms. Plantation, Fla: Reflective Image, Inc.
Kreipe, R. E., and Travis, S. (2002) “Eating Disorders.” In Finberg, L., and Kleinman, R., eds., Manual of Pediatric Practice, 2nd ed. Orlando, Fla.: W. B. Saunders.
“Position of the American Dietetic Association: Nutrition Intervention in the Treatment of Anorexia Nervosa, Bulimia Nervosa, and Eating Disorders Not Otherwise Specified (EDNOS)” (2001) Journal of the American Dietetic Association 101:7, 810–819.
Reiff, D. W., and Reiff, K.K.L. (1991) Eating Disorders: The Health Professional’s Guide to the Process of Recovery. Frederick, Md.: Aspen.
Wall, J. M. (1991) Eating Disorders: A Manual for Nutritionists. Brattleboro, Vt.: Nutrition Resources.
Top Related