






Languages
Pages
Legal

Noon Conf 7/19/06
How to Help your Elderly Patient Survive Hospitalization
Karen Hall, M.DAssociate Professor
Division of Geriatric MedicineUniversity of Michigan

Noon Conf 7/19/06
Objectives
• Review pathophysiology of aging
• Define areas of risk
• Outline management

Noon Conf 7/19/06
Case86 year old woman seen at 8pm in EDBrought in by her daughter because of increasing confusion over
past 24-48 hoursPatient moved in with daughter and son-in-law 1 year ago because
of “memory problems” and difficulty caring for herself. In past 24 hours patient has been wandering around the house, is very confused, fell twice, had several episodes of urinary and fecal incontinence. No cough, SOB. No head trauma. Family denies ETOH.
PHx: HTN, GERD, depression, insomnia, osteoporosis, constipation, diarrhea
Medications: lisinopril, HCTZ, Protonix, Fosamax, Nortriptyline at night, fiber supplement, Ambien at night

Noon Conf 7/19/06
CasePx:Vitals: BP 102/58 - sitting 93/46, heart rate increases from 84 to 100 on
sitting, temperature 95 deg F, RR 16Weight 100 lbs, height 5 feet 3 inches (BMI <25)Confused: not oriented to place, time, keeps trying to get out of bed, unable
to give history, keeps asking for her daughterH/N – dry mouth, pupils reactive, no thyromegaly, chest clear, CVS - no signs of heart failure or murmer or arrythmia, JVP at sternal angle, abdomen - soft and no guarding or rebound, patient moans when lower quadrants palpated, CNS – no focal weakness
Labs: Na 129, K 3.3, Cl 97, HCO3 18; Cr 1.6, BUN 48; CBC: WBC 7 with left shift, Hb 9.2, HCT 29, Plts 138
CXR – poor inspiratory effort, no masses or opacitiesUA - + leukocytes, nitrites, bloodCT head – small vessel disease and mild atrophy, no subdural or CVA
.
Noon Conf 7/19/06
CaseAdmitted: diagnosis of UTI/Sepsis with dehydrationOrders: iv NS 500 cc bolus in ED at 10 pm then 100 cc/hrZocin 3.376 g iv q6h (sodium salt)Docusate sodium (stool softener)Foley catheterPrn: Tylenol, morphine iv 1-3 mg, trazodone 25-50 mg for sleepSent to MedPath overnightArrives on unit at 8am
Examined by medical team at 9am – still confused, JVD 2 cm above SA, trace edema both legs
Haloperidal ordered for agitation: 1-3 mg tid prn
Noon Conf 7/19/06
CaseAt 4pm noted to be increasingly agitated – fighting the nursesFalls out of bed and fractures R hipOn exam has crackles in lung fields, JVD 4 cm above SA, 1+ edema,
pulse O2 86 on RA, 91 on 4 liters O2Diuresed with lasix (60 mg bolus, repeat 20 mg x 2)K drops to 2.9 – bolus of 40 mEq then added to ivHip pinned next day, continues confused, has to be restrained to avoid
pulling out ivs, develops troponin leak (MI), DVT, skin breakdown over sacrum, no BM in 4 days
Haloperidol switched to Seroquel without improvement
Becomes increasingly somulent, vomits and aspirates on 2nd postop day
Develops aspiration pneumonia and dies on 5th postop day
Noon Conf 7/19/06
CaseWhat happened to this patient?Delirium Fluid overload Hip fractureHypokalemiaMIDVTDecubitus ulcersAspiration pneumoniaDeath
Noon Conf 7/19/06
Case
Was this outcome inevitable?
Could we have intervened or prevented some of these complications?

Noon Conf 7/19/06
Why do older patients have problems in hospital?
1. Patients of advanced age lose the ability to maintain homeostatic control of physiologic processes. This is particularly true of “old-old” patients: age > 85 years.
Cardiac and vascular compliance decreases: increased systolic BP, decreased diastolic BP, widened pulse pressure (HTN)
Renal GFR decreases: slower excretion of an excess fluid loadDecreased activity of P450 enzyme system in the liver: slower
hepatic metabolism of drugsColonic motility slows: constipation (risk for gastroparesis)Aging-related peripheral neuropathy: decreased autonomic
sensation with acute disease (acute abdomen)Increased incidence of CNS neurodegeneration: dementia
Noon Conf 7/19/06
Iatrogenic Burden• Steel et al. (1981) identified the burden in a university hospital:
815 patients on two medical floors– 36% of patients had at least one iatrogenic illness– 9% had a major iatrogenic illness– 2% had an iatrogenic illness that contributed to death
• Drugs were a major culprit– Nitrates, digoxin, lidocaine, aminophylline, quinidine and other
antiarrhythmics, heparin/warfarin, penicillin, benzodiazepines, antihypertensives, propranolol, “other”
• Cardiac catheterization and falls• Admitted from nursing home or hospital• HO of “poor” or “critical”, admission to ICU• Age only important if correlated with “poor” condition on admit
Steel K, Gertman PM, Cresenzi C et al. Iatrogenic illness on a general medical service at a university hospital. NEJM 1981; 304:638-42.

Noon Conf 7/19/06
Identified Risks• Multiple chronic diseases (65% of Medicare beneficiaries have
two or more chronic conditions; 4 or more = 99x risk)• Multiple physicians (uncoordinated care)• Multiple drugs and inappropriate drugs/doses• Hospitalization (dementia or immobilization)• Pre-morbid functional status (dependent in ADLs)
Prevention:Case management – facilitate communicationGeriatric interdisciplinary team (only for complex cases)Pharmacist consulationAcute Care for the Elderly (ACE) Units – team sensitive to
preventionAdvance Directives
Wolf JL, Starfeld B, Anderson G. Prevalence, expenditures, and complications of multiple chronic conditions in the elderly. Arch Intern Med 2002; 162:2269-76.
Noon Conf 7/19/06
On admission• Cognition – document mental status and changes
– Delirium, dementia, depression• Pre-morbid functional status
– mobility• Sensory (vision and hearing)• Nutrition• Fluid status• Bowel function• Pain• Skin Integrity• Medication review• Social supports and caregiver status
Granieri EC, Turner GH, Organist L. Geriatric assessment, coordinated case management, and information systems: an integrated model for delivery of services to nursing home residents. Topics Health Info Management 1997; 18:38-46.

Noon Conf 7/19/06
Cognition • Prevalence of dementia increases dramatically with age• <3% of patients under age 65 are demented• >40% of patients over age 85 are demented• Age over 75 are at risk for confusion and delirium if
they are illOR
if we add new stressor (medications with CNS side effects)
Noon Conf 7/19/06
Cognition • MMSE – best test (validated, tests multiple domains)• Mini-Cog – three item short term recall and clock draw (“draw
a clock face, put the hands at 8:20”)• Delirium testing – Confusion Assessment Method (CAM):
acute onset, fluctuating + disorganized thinking or altered level of consciousness
• Orientation less useful as screen because patients in hospital do not have usual cues to date, time etc.
• Ideally should be easily accessible in medical record• Objective assessment allows tracking of response to
interventions
Noon Conf 7/19/06
Delirium• Most important risk factor for adverse
events• Delirious patients are 5x more likely to
have adverse event in hospital (falls, fractures, aspiration)
• Significant risk for institutionalization• Once present may take days-weeks to
clear
Noon Conf 7/19/06
Delirium• Present on admission – needs to be listed as admitting
diagnosis• Her underlying dementia increases her risk of delirium• Screen for reversible causes on admission and
minimize further exacerbation• UTI is extremely common cause – always worth
checking the UA• Other infections (pneumonia) also common cause of
sudden confusion• CNS (stroke, bleed, infection)• Cancer
Noon Conf 7/19/06
Delirium• Hypoxia, low Hb (<9)• Hyponatremia, hypercalcemia, renal
impairment (elevated Cr), dehydration (elevated BUN)
• Hypoglycemia, thyroid (either up or down)• Medications: narcotics, anticholinergics,
neuroleptics, benzodiazepenes, CNS active– “Old” meds may be the culprit – if in doubt
consider withdrawing if possible– Rapid withdrawal of benzodiazepenes is
dangerous
Noon Conf 7/19/06
Mobility • Dependence in 2 or more ADLs predicts increased risk
of complications in hospital• Important to document baseline (what they did 1 month
ago or before illness) and on admission– Ideally should be in easily accessed part of medical record– 60% have lost 2 or more ADLs from baseline
• Document falls – may be first sign of illness• Gait, Timed Up and Go Test, muscle strength
Noon Conf 7/19/06
Mobility • Observe state of the bed – bedcrumbs, can patient
turn over?• Ask patient to slide to edge of bed• Ask patient to get out of bed if possible every day• Early PT/OT – usually 24 hour delay between
admission and being seen by PT
Unfortunately if they continue to be dependent in 2 or more ADLs at discharge – significant risk for institutionalization
Noon Conf 7/19/06
Vision and Hearing • Sensory deprivation can look like
delerium, or worsen delerium
• If hearing aids lost or family concerned about bringing them – use a pocket amplifier ($50 at Radio Shack)
• Get glasses or other visual aids – prompt patient to use them
Noon Conf 7/19/06
Nutrition• Document BMI (<19 is very high risk)
• Weight loss
• Demented patients at risk for malnutrition (protein calorie or vitamin)
• Check albumin on admission
• Consider swallowing/aspiration risk if demented or neuromuscular disease
• Keep track of “NPO” days

Noon Conf 7/19/06
Fluid status• Dehydration is common
BUT
Aggressive replacement of fluids may overload the heart and kidneys
• Patients lying in bed can tolerate lower BP – main goal is adequate perfusion of organs
• Usually replacing up to ~2/3 of deficit in 24 hours is tolerated, but this patient became overloaded with 2 liters of NS in 18 hours
• An exam at midday would have detected the overload

Noon Conf 7/19/06
Electrolytes• Patient was already hypokalemic and likely
to become worse with NS• If replacing K – need to recheck within 6
hours, as patient may have significant renal disease and be unable to excrete a K load

Noon Conf 7/19/06
Bowel function • Ask about pre-existing constipation, find
out when last BM occurred
• Fiber alone or stool softener alone is usually useless if patient is bedbound
• Constipation can lead to gastroparesis and is a risk for vomiting and aspiration
Noon Conf 7/19/06
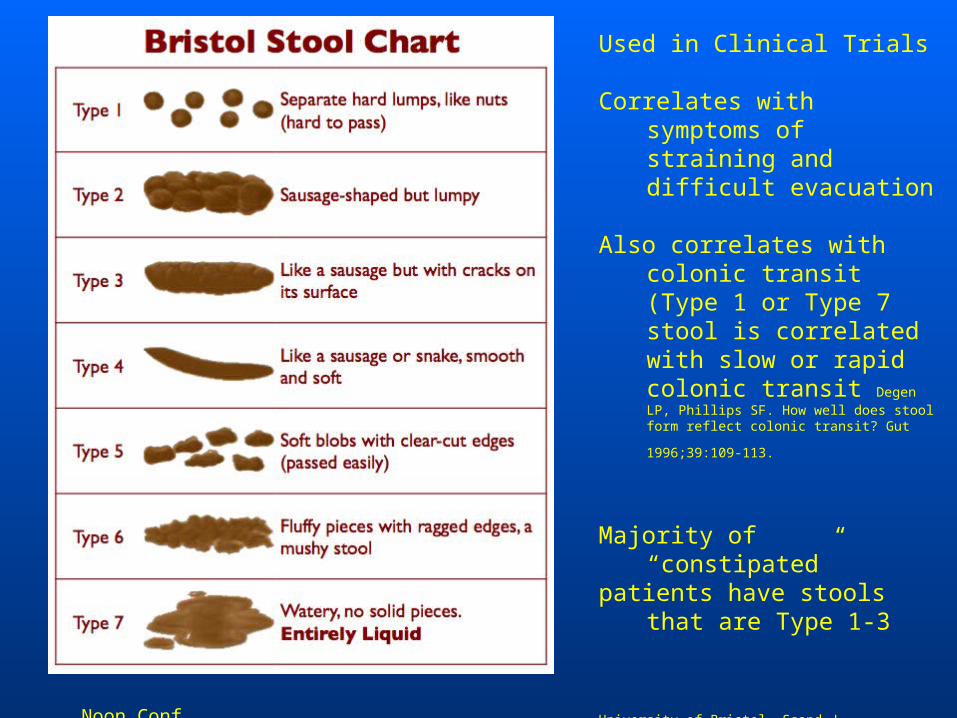
Used in Clinical Trials
Correlates with symptoms of straining and difficult evacuation
Also correlates with colonic transit (Type 1 or Type 7 stool is correlated with slow or rapid colonic transit Degen LP, Phillips SF. How well does stool form reflect colonic transit? Gut
1996;39:109-113.
Majority of “constipated”patients have stools that are
Type 1-3
University of Bristol, Scand J Gastroenterol, 1997

Noon Conf 7/19/06
Constipating MedicationsOTC
• Sympathomimetics
• NSAIDS
• Antacids: aluminum, calcium
• Ca supplements
• Iron supplements
• Antidiarrheals: loperamide; bismuth
Noon Conf 7/19/06
Prescription Medications• Narcotics - codeine,morphine• Anticholinergics - benztropine, trihexyphenedyl• Antipsychotics - chlorpromazine • Antidepressants - tricyclics• Antiparkinson - levodopa• Antispasmodics - dicyclomine• Antihistamines - diphenhydramine• Ca blockers - verapamil• Diuretics - furosemide
Noon Conf 7/19/06
Treat impaction first• Patients with fecal impaction should have the
impacted feces removed manually or with enemas before starting laxatives– Tap water– Milk and molasses (1 liter:½ cup)– Mineral oil (less effective)– Not soapsuds (increased risk of colitis)– May take several attempts
Wrenn K. Fecal impaction. N Engl J Med 1989;321:658-662
Noon Conf 7/19/06
Constipation
• Non pharmacologic– Bowel training (go to bathroom after
breakfast)– Fiber – Exercise and increased fluid intake
(beneficial for patients who are dehydrated)
Will not be enough for patients in hospital with immobility and medications
Noon Conf 7/19/06
Laxatives• Osmotic laxatives
– Poorly absorbed or nonabsorbed– Draws water along osmotic gradient– Be careful using in renal insufficiency or cardiac dysfunction– Magnesium (MOM)– Lactulose - synthetic disaccharide (10-30 g/day) GAS– Sugar alcohols
• Sorbitol & Mannitol
– Polyethylene glycol & Electrolytes GoLYTELY, NuLYTELY– Polyethylene glycol 3350 (Miralax) (17g/day) EXPENSIVE
• Overuse can cause dehydration

Noon Conf 7/19/06
Stimulant laxativesIncrease intestinal motility and secretionEffective within hours and may cause abdominal
crampsConcern about long term use causing cathartic colon
(loss of haustration and dilatation of the colon) –phenolthalein (old formulation of Exlax) and cascara
Melanosis coli may develop in patients who take stimulant laxatives containing anthraquinones, but this is not a risk for development of colon cancer
Badiali D, Marcheggiano A, Pallone F, et al. Melanosis of the rectum in patients with chronic constipation. Dis Colon Rectum 1985;28:241-245.
van Gorkom BA, de Vries EG, Karrenbeld A, Kleibeuker JH. Anthranoid laxatives and their potential carcinogenic effects. Aliment Pharmacol Ther 1999;13:443-452.
Noon Conf 7/19/06
Stimulant LaxativesUseful in multifactorial refractory constipation
without obstruction• Anthraquinones
– senna (recent trials indicate safe for long term use) Senakot titrate up to 4-6 per day
• Diphenylmethane derivatives– bisacodyl, sodium picosulphate
• “Stool softener”– Docusate sodium (not very effective in severe constipation)
• Avoid cascara, castor oil (very irritating – colitis) and mineral oil (risk of aspiration pneumonia)

Noon Conf 7/19/06
Other treatments rarely used
Cholinergic agents– Bethanechol– Likely to cause cramps, may cause
confusion in older patients with underlying cognitive disorders
• Miscellaneous– Misoprostol 200-400 mcg/day– Colchicine

Noon Conf 7/19/06
“Prokinetic Drugs”• Cisapride - substituted benzamide
– Stimulates peristalsis by increasing acetylcholine release from myenteric plexus
– Increased risk of cardiac arrhythmias
• 5-hydroxytryptamine receptor agonists– Tegaserod - partial 5-HT4 receptor agonist– Improves stool consistency and frequency in
women with irritable bowel syndrome characterized by constipation
Muller-Lissner SA, Fumagalli I, Bardhan KD, et al. Tegaserod, a 5-HT(4) receptor partial agonist, relieves symptoms in irritable bowel syndrome patients with abdominal pain, bloating and constipation. Aliment Pharmacol Ther 2001;15:1655-1666.

Noon Conf 7/19/06
Lubiprostone (Amitza)
• Selectively activates type 2 chloride channels (ClC-2) in apical membrane of the gastrointestinal tractCuppoletti J. Malinowska DH. Tewari KP. Li QJ. Sherry AM. Patchen ML. Ueno R. . SPI-
0211 activates T84 cell chloride transport and recombinant human ClC-2 chloride currents. American Journal of Physiology - Cell Physiology. 287(5):C1173-83, 2004.
• Increased fluid secretion into lumen
• No significant systemic absorption but has absorbed metabolites
Noon Conf 7/19/06
Skin
• Check for pre-existing skin pressure
• Stage 1 non-blanching erythema
• Stage 2-4 actual breakdown
• Order aggressive treatment (turning, mobilization, protection)
Noon Conf 7/19/06
Electrolytes• Patient was already hypokalemic and likely
to become worse with NS• If replacing K – need to recheck within 6
hours, as patient may have significant renal disease and be unable to excrete a K load

Noon Conf 7/19/06
Hematologic• Patient was already anemic and likely to
become worse with fluid replacement• Main issue is oxygenation – this will worsen
her delirium, and needs to be monitored• Her agitation makes continuous pulse O2
difficult, but monitoring during the morning would have detected hypoxia
• Hb below 9 is likely to worsen delirium
Noon Conf 7/19/06
Social Supports• Living with family – memory problems suggest dementia
and this is a major risk for delirium and adverse reactions to medications
• Patient may benefit from family being present – try to arrange family to stay in the room
• Sitter can decrease need for restraints in delirium• Other interventions for delirium
– Private room– Minimize interruptions – same medical team (!), no nightime vitals,
predictable routine (!)– Lower the bed (fall less injurious)– Hip protectors– Minimize iv poles, Foleys etc – less chance of tripping and falling– Mobilize – ambulate if possible with assistance

Noon Conf 7/19/06
Orders• Think about fluid load – when should this be reassessed and
who will do it – write it down• Same for electrolytes, constipation, diet• Avoid prns – yes it is annoying to be woken up but the
patient’s nightime agitation may be due to hypoxia – think before ordering neuroleptics or sedatives if you are cross-covering
• If you have to use neuroleptics - use low doses (no more than 3 “haloperidal equivalents” in one day, less is better) - 0.25 – 0.5 mg doses at any one time
• Atypical neuroleptics less likely to cause extrapyramidal side effects, but studies indicate a modest increase in CVS risk (MI)
• Watch for sedation – aspiration risk
Noon Conf 7/19/06
Orders• Useful to sign out to covering team – “delirious
patient” management• Think ahead – will you need a sitter? Easier to get
one arranged during the day• Discuss with the nurses what to do at night• If hospital has a delirium unit (“Nest” at VA) then
use it• Anticipate alternative placement (CNH) as patient
may remain delirious for days• Get help from Geriatric Inpatient Consult Team,
psychiatry, neurology to manage risks• Warn the family of risks – “risk management”

Noon Conf 7/19/06
Orders• If the patient does end up with an adverse
event – keep trying to minimize further risks• Elderly patients who have developed
complications from delirium may benefit from earlier admission to ICU for intensive monitoring
• Before ICU admission – make sure the goals of treatment are clear (another reason to discuss the risks with the family early in the admission)
Noon Conf 7/19/06
On Discharge• Assuming there was a better outcome…
– Define residual delirium– Arrange for repeat cognitive testing in a few
weeks to define the level of dementia – and record it in the chart
– Work up the anemia if not already done – if possible neoplasm, patient’s cognitive status may be important to define
– Arrange repeat labs soon after d/c – someone will need to be responsible for followup of renal function, electrolytes
• An email to the PCP could be helpful
Top Related