







Languages
Pages
Legal


Hilary Hodgdon, Ph.D. – Complex Trauma in Children 1
Complex Trauma Complex Trauma
TreatmentsTreatments
The Problem of Treating Complex TraumaThe Problem of Treating Complex Trauma
�� Need for intervention that:Need for intervention that:
�� Can address continuum of exposures (layers of Can address continuum of exposures (layers of chronic and acute), including ongoing exposurechronic and acute), including ongoing exposure
�� Is embedded in a social/contextual frameworkIs embedded in a social/contextual framework
�� Is sensitive to individual developmental Is sensitive to individual developmental competencies and vulnerabilities, and flexible in competencies and vulnerabilities, and flexible in its approachits approach
�� Addresses individual, familial, and systemic Addresses individual, familial, and systemic needs and strengthsneeds and strengths
Hilary Hodgdon, Ph.D. – Complex Trauma in Children 2
CORE ComponentsCORE Components
What are Evidenced Based Treatments?What are Evidenced Based Treatments?
��Treatments that have strong research supportTreatments that have strong research support
��Clinical trials & Randomized Controlled Clinical Clinical trials & Randomized Controlled Clinical
TrialsTrials
��Typically involve a manual, series of training and Typically involve a manual, series of training and
consultation to learn the treatment modelconsultation to learn the treatment model

Hilary Hodgdon, Ph.D. – Complex Trauma in Children 3
EBTEBT’’ss for Complex Traumafor Complex Trauma
��TraumaTrauma--Focused Cognitive Behavioral Therapy Focused Cognitive Behavioral Therapy
(TF(TF--CBT)CBT)
��ChildChild--Parent Psychotherapy (CPP)Parent Psychotherapy (CPP)
��Attachment, SelfAttachment, Self--Regulation and Competency Regulation and Competency
(ARC)(ARC)
��ParentParent--Child Interaction Therapy (PCIT)Child Interaction Therapy (PCIT)
��Seeking SafetySeeking Safety
��Trauma Systems TherapyTrauma Systems Therapy
��And many moreAnd many more……. .
EBT TrainingEBT Training
Trauma EBT developers and experts believe in order Trauma EBT developers and experts believe in order for a clinician to be considered trained the following for a clinician to be considered trained the following criteria are needed: criteria are needed:
��TwoTwo--day basic training, monthly consultation for 12 day basic training, monthly consultation for 12 months by a certified EBT trainermonths by a certified EBT trainer
��Weekly supervision by an agency EBT trained Weekly supervision by an agency EBT trained supervisor who monitors clinician fidelity to the supervisor who monitors clinician fidelity to the modelmodel
�� Implementation of the model with a minimum of 3 Implementation of the model with a minimum of 3 families per year.families per year.

Hilary Hodgdon, Ph.D. – Complex Trauma in Children 4
Trauma Focused Cognitive Trauma Focused Cognitive
Behavioral Therapy Behavioral Therapy
(TF(TF--CBT)CBT)
TFTF--CBTCBT��Model Developed by Cohen, Model Developed by Cohen, MannarinoMannarino, & , &
DeblingerDeblinger
��An EvidenceAn Evidence--Based PracticeBased Practice
��A SAMHSA Model ProgramA SAMHSA Model Program
��One of Kaufman Best PracticesOne of Kaufman Best Practices
Hilary Hodgdon, Ph.D. – Complex Trauma in Children 5
TFTF--CBT: A hybrid treatment model that integrates:CBT: A hybrid treatment model that integrates:
�� Trauma sensitive interventionsTrauma sensitive interventions
�� CognitiveCognitive--behavioral principlesbehavioral principles
�� Attachment theoryAttachment theory
�� Developmental NeurobiologyDevelopmental Neurobiology
�� Family TherapyFamily Therapy
�� Empowerment TherapyEmpowerment Therapy
�� Humanistic TherapyHumanistic Therapy
TFTF--CBT: The EvidenceCBT: The Evidence
�� Model initially tested:Model initially tested:�� DeblingerDeblinger et al (1990). Journal of American Academy of Child and et al (1990). Journal of American Academy of Child and
Adolescent Psychiatry, 29, 5, 747Adolescent Psychiatry, 29, 5, 747--752752�� Stauffer & Stauffer & DeblingerDeblinger (1996). Child Maltreatment, 1, 65(1996). Child Maltreatment, 1, 65--76.76.
�� Randomized controlled trials:Randomized controlled trials:�� DeblingerDeblinger et al, (1996). Child Maltreatment, 1, 4, 310et al, (1996). Child Maltreatment, 1, 4, 310--321.321.�� Cohen & Cohen & MannarinoMannarino (1996). Journal of American Academy of (1996). Journal of American Academy of
Child and Adolescent Psychiatry, 35, 1, 42Child and Adolescent Psychiatry, 35, 1, 42--50.50.�� Cohen & Cohen & MannarinoMannarino (1998). Child Maltreatment, 3, 1, 17(1998). Child Maltreatment, 3, 1, 17--26.26.�� DeblingerDeblinger et al (2001). Child Maltreatment, 6, 4, 332et al (2001). Child Maltreatment, 6, 4, 332--343.343.�� Cohen & Cohen & MannarinoMannarino (1997). JAACAP, 36, 9, 1228(1997). JAACAP, 36, 9, 1228--1235.1235.�� Cohen & Cohen & MannarinoMannarino (1998). JAACAP, 37, 1, 44(1998). JAACAP, 37, 1, 44--51.51.�� DelbingerDelbinger, et al, (1999). Child Abuse and Neglect, 23, 12, 1371, et al, (1999). Child Abuse and Neglect, 23, 12, 1371--
1378.1378.�� King, et al (2000). JAACP, 59, 1, 1347King, et al (2000). JAACP, 59, 1, 1347--1355.1355.

Hilary Hodgdon, Ph.D. – Complex Trauma in Children 6
TFTF--CBTCBT
TFTF--CBT maintains the following treatment focus:CBT maintains the following treatment focus:
PRACTICEPRACTICE
��PPsychoeducationsychoeducation and Parenting Skillsand Parenting Skills
��RRelaxationelaxation
��AAffective Expression and Regulationffective Expression and Regulation
��CCognitive Copingognitive Coping
��TTrauma Narrative Development and Processingrauma Narrative Development and Processing
�� IIn Vivo Gradual Exposuren Vivo Gradual Exposure
��CConjoint Parentonjoint Parent--Child SessionsChild Sessions
��EEnhancing Safety and Future Developmentnhancing Safety and Future Development
TFTF--CBT: Affect ExpressionCBT: Affect Expression
Hilary Hodgdon, Ph.D. – Complex Trauma in Children 7
TFTF--CBT: SUDSCBT: SUDS
TFTF--CBT: Processing (8 CBT: Processing (8 yoyo))

Hilary Hodgdon, Ph.D. – Complex Trauma in Children 8
Child Parent Psychotherapy Child Parent Psychotherapy
(CPP)(CPP)
CPPCPP
�� Targets children (ages 0Targets children (ages 0--5 years) 5 years)
and caregivers.and caregivers.
�� Heavy emphasis on dyadic work.Heavy emphasis on dyadic work.
�� Developed by Alicia Lieberman, Ph.D., Developed by Alicia Lieberman, Ph.D.,
Patricia Van Horn, J.D., Ph.D., Patricia Van Horn, J.D., Ph.D.,
Chandra Chandra GhoshGhosh--IppenIppen, Ph.D., Ph.D.
�� UCSF Child Trauma Research ProjectUCSF Child Trauma Research Project
�� An EvidenceAn Evidence--Based PracticeBased Practice
�� A SAMHSA Model ProgramA SAMHSA Model Program

Hilary Hodgdon, Ph.D. – Complex Trauma in Children 9
CPP: The EvidenceCPP: The Evidence
�� Randomized controlled trials:Randomized controlled trials:
�� CicchettiCicchetti, D. et al, (2000). JOACP, 28, 135, D. et al, (2000). JOACP, 28, 135--148.148.
�� CicchettiCicchetti, D. et al, (2006). Development and Psychotherapy, 18, , D. et al, (2006). Development and Psychotherapy, 18, 623623--650.650.
�� CicchettiCicchetti, D. et al, (1999). Attachment and Human Development, , D. et al, (1999). Attachment and Human Development, 1, 341, 34--66.66.
�� Lieberman, A.F. et al, (2005). JAACAP, 44(12), 1241Lieberman, A.F. et al, (2005). JAACAP, 44(12), 1241--1248.1248.
�� Lieberman, A.F. et al, (2006). JAACAP, 45(8), 913Lieberman, A.F. et al, (2006). JAACAP, 45(8), 913--918.918.
�� Lieberman, A. F. et al, (1991). Child Development, 62, 199Lieberman, A. F. et al, (1991). Child Development, 62, 199--209.209.
�� TothToth S.L. et al, (2002). Developmental Psychopathology, 14, 877S.L. et al, (2002). Developmental Psychopathology, 14, 877--908.908.
�� TothToth, S. L. et al, (2006). Journal of Consulting and Clinical , S. L. et al, (2006). Journal of Consulting and Clinical Psychology,74(6), 1006Psychology,74(6), 1006--10161016
CPPCPP�� A hybrid treatment model that A hybrid treatment model that
identifies the following goals:identifies the following goals:
�� To support and strengthen the To support and strengthen the
caregivercaregiver--childchild’’s relationship as a s relationship as a
vehicle for restoring and protecting vehicle for restoring and protecting
the childthe child’’s mental health. s mental health.
�� Improve the caregiversImprove the caregivers’’ and and
childrenchildren’’s maladaptive s maladaptive
representations of themselves and representations of themselves and
each other and interactions and each other and interactions and
behaviors that interfere with the behaviors that interfere with the
childchild’’s mental health. s mental health.
Hilary Hodgdon, Ph.D. – Complex Trauma in Children 10
CPPCPP
�� ChildChild--parent interactions are the focus of six intervention parent interactions are the focus of six intervention
modalities:modalities:
�� Promoting developmental progress through play, Promoting developmental progress through play,
physical contact and language.physical contact and language.
�� Offering developmental guidance.Offering developmental guidance.
�� Modeling appropriate protective behavior.Modeling appropriate protective behavior.
�� Interpreting feelings and actions.Interpreting feelings and actions.
�� Providing emotional support/empathetic Providing emotional support/empathetic
communication.communication.
�� Offering crisis intervention, case management and Offering crisis intervention, case management and
concrete assistance with problems of living.concrete assistance with problems of living.
Attachment, SelfAttachment, Self--regulation regulation
and Competency (ARC)and Competency (ARC)
Hilary Hodgdon, Ph.D. – Complex Trauma in Children 11
Where does ARC come from?Where does ARC come from?
�� Translation of clinical principles across settings Translation of clinical principles across settings
(out(out--pxpx, residential, school, home, residential, school, home--based)based)
�� OrOr……what is it that we actually do?what is it that we actually do?
�� ““EvidenceEvidence--based practicebased practice””??
�� OrOr……how to fit real kids into scientific boxeshow to fit real kids into scientific boxes
�� Staying true to the inner clinicianStaying true to the inner clinician
�� OrOr……keeping the art in keeping the art in ttrreeaa ttmentmentrr
Protocol vs. Component based Protocol vs. Component based
InterventionsInterventions
�� Clinical Objectives FocusedClinical Objectives Focused
�� Developmentally TailoredDevelopmentally Tailored
�� Context SpecificContext Specific
�� Individual TargetsIndividual Targets
�� MenuMenu--DrivenDriven
Hilary Hodgdon, Ph.D. – Complex Trauma in Children 12
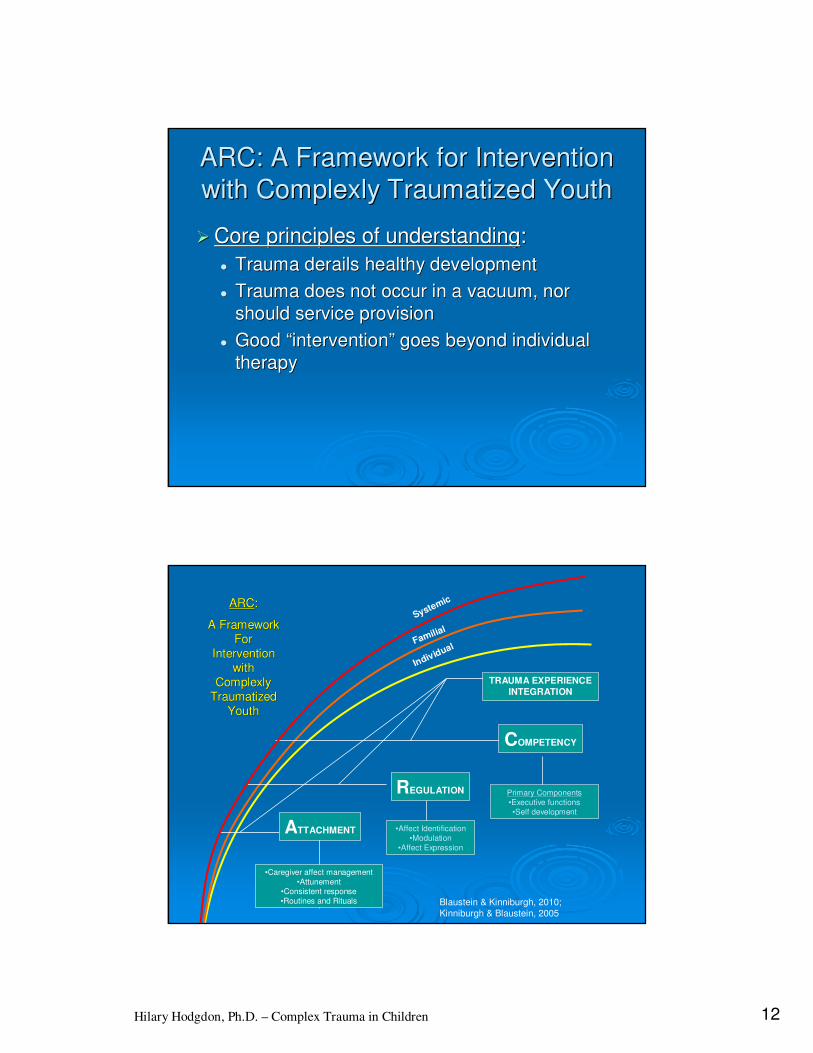
ARC: A Framework for Intervention ARC: A Framework for Intervention
with Complexly Traumatized Youthwith Complexly Traumatized Youth
�� Core principles of understandingCore principles of understanding::
�� Trauma derails healthy developmentTrauma derails healthy development
�� Trauma does not occur in a vacuum, nor Trauma does not occur in a vacuum, nor
should service provisionshould service provision
�� Good Good ““interventionintervention”” goes beyond individual goes beyond individual
therapytherapy
Systemic
Familial
Individual
ATTACHMENT
•Caregiver affect management
•Attunement
•Consistent response
•Routines and Rituals
REGULATION
•Affect Identification
•Modulation
•Affect Expression
COMPETENCY
Primary Components
•Executive functions
•Self development
ARCARC: :
A Framework A Framework
For For
Intervention Intervention
with with
Complexly Complexly
Traumatized Traumatized
YouthYouth
Blaustein & Kinniburgh, 2010;
Kinniburgh & Blaustein, 2005
TRAUMA EXPERIENCE
INTEGRATION

Hilary Hodgdon, Ph.D. – Complex Trauma in Children 13
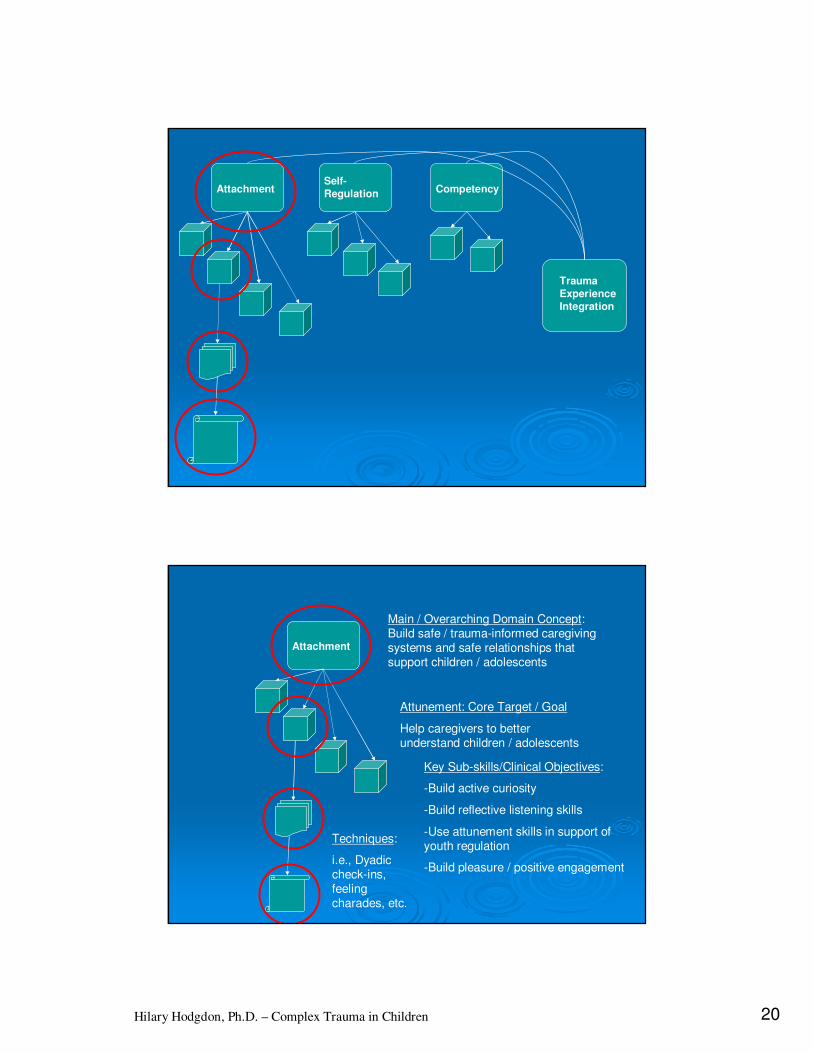
ARC ARC -- 10 Building Blocks10 Building Blocks
Caregiver
Affect
Mgmt.
Attunement Consistent
Response
Routines
and
Rituals
Affect
IdentificationModulation Affect
Expression
Self Dev’t
& Identity
Executive
Functions
Trauma
Experience
Integration
Attachment
Self-
Regulation
Competency
Who does ARC target?Who does ARC target?
�� Designed to target the needs of children, Designed to target the needs of children,
families, and systems impacted by complex families, and systems impacted by complex
traumatrauma
�� Core domains translate across children/ families/ Core domains translate across children/ families/
systems; applications and goals will varysystems; applications and goals will vary
�� Crucial importance of: Crucial importance of:
�� Keep an eye on the clinical objective, rather than the Keep an eye on the clinical objective, rather than the
techniquetechnique
�� Pay attention to relative goals and relative successesPay attention to relative goals and relative successes
�� Have a plan, but catch the momentsHave a plan, but catch the moments

Hilary Hodgdon, Ph.D. – Complex Trauma in Children 14
Programs Applying ARC PrinciplesPrograms Applying ARC Principles�� Anchorage CMHC (OutAnchorage CMHC (Out--pxpx))
�� Beth Israel NY (OutBeth Israel NY (Out--pxpx, school, school--based)based)
�� B.C. ChildrenB.C. Children’’s Hospital (Ins Hospital (In--pxpx))
�� Bethany Christian Services (OutBethany Christian Services (Out--pxpx))
�� Butler Center (DYS residential)Butler Center (DYS residential)
�� Calgary Public Schools (Classroom / Calgary Public Schools (Classroom / wholewhole--school)school)
�� ChildrenChildren’’s Hospital L.A. (Highs Hospital L.A. (High--risk risk youth programs)youth programs)
�� The ChildrenThe Children’’s Guild (Therapeutic s Guild (Therapeutic foster care)foster care)
�� CohannetCohannet Academy (DMH IRTP)Academy (DMH IRTP)
�� CrittentonCrittenton ChildrenChildren’’s Services (Multiple s Services (Multiple programs programs –– outout--pxpx, Head Start, Group , Head Start, Group Home)Home)
�� DV Crisis Center (DV Shelter and DV Crisis Center (DV Shelter and Advocacy)Advocacy)
�� GatewayGateway--Longview (Child Welfare Longview (Child Welfare Agency)Agency)
�� GlenhavenGlenhaven Academy (Residential Academy (Residential School)School)
�� Harmony Hill (Residential treatment)Harmony Hill (Residential treatment)
�� Hertfordshire County Council Hertfordshire County Council (Adolescent programs)(Adolescent programs)
�� House of Mercy (Domestic Violence House of Mercy (Domestic Violence shelter program)shelter program)
�� Kennedy Krieger (Therapeutic Foster Kennedy Krieger (Therapeutic Foster Care Program)Care Program)
�� La La RabidaRabida ChildrenChildren’’s Hospital (Outs Hospital (Out--pxpx))
�� Lower Naugatuck Valley PCRC (DV Lower Naugatuck Valley PCRC (DV Resource Center)Resource Center)
�� Mosaic ChildrenMosaic Children’’s Services (Group s Services (Group Home)Home)
�� MGH Chelsea (Group/OutMGH Chelsea (Group/Out--pxpx))
�� New England Counseling & Trauma New England Counseling & Trauma Center (OutCenter (Out--pxpx))
�� Safe from the Start (CommunitySafe from the Start (Community--based based agencies)agencies)
�� Southern Trust (Residential / group Southern Trust (Residential / group homes)homes)
�� SutterSutter--Yuba Mental Health (OutYuba Mental Health (Out--pxpx))
�� The Trauma Center at JRI (OutThe Trauma Center at JRI (Out--pxpx))
�� UCSF/CASARC (OutUCSF/CASARC (Out--pxpx))
�� Vermont Department of Mental Health Vermont Department of Mental Health (Outpatient programs)(Outpatient programs)
�� Youth on Fire (Adolescent dropYouth on Fire (Adolescent drop--in in center)center)
Treatments Utilized in the NCTSNTreatments Utilized in the NCTSN
63.88.3
4.5
3.5
2.5
17.4
TF-CBT
ARC
CPP
PCIT
SPARCS
Other /Unknown
NCTSN FY 2010 Annual Progress Report – Executive Summary
Total n=966
Hilary Hodgdon, Ph.D. – Complex Trauma in Children 15
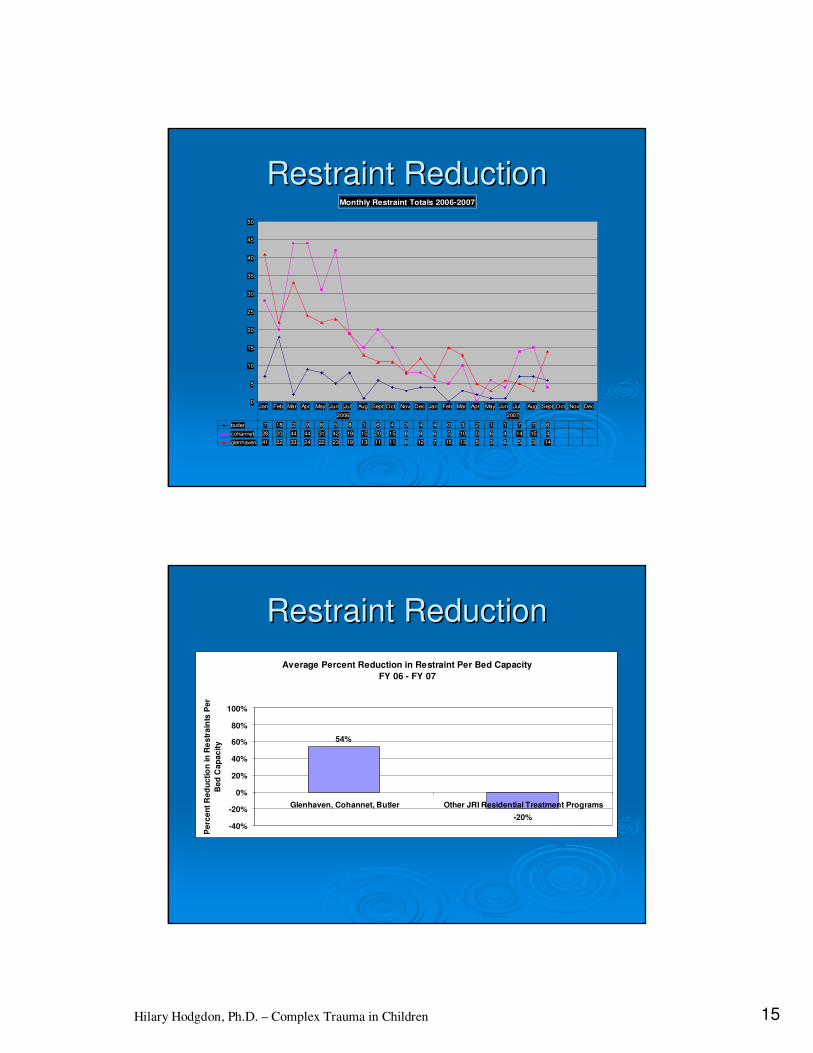
Restraint ReductionRestraint ReductionMonthly Restraint Totals 2006-2007
0
5
10
15
20
25
30
35
40
45
50
butler 7 18 2 9 8 5 8 1 6 4 3 4 4 0 3 2 1 1 7 7 6
cohannet 28 20 44 44 31 42 19 15 20 15 8 8 6 5 10 0 6 4 14 15 4
glenhaven 41 22 33 24 22 23 19 13 11 11 8 12 7 15 13 5 3 6 5 3 14
Jan Feb Mar Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sept Oct Nov Dec
2006 2007
Restraint ReductionRestraint Reduction
Average Percent Reduction in Restraint Per Bed Capacity
FY 06 - FY 07
54%
-20%-40%
-20%
0%
20%
40%
60%
80%
100%
Glenhaven, Cohannet, Butler Other JRI Residential Treatment Programs
Pe
rce
nt
Re
du
cti
on
in
Re
str
ain
ts P
er
Be
d C
ap
ac
ity

Hilary Hodgdon, Ph.D. – Complex Trauma in Children 16
66--Month Change in CBCL ScoresMonth Change in CBCL Scores
545556575859606162636465666768
Baseline 3 Months* 6 Months*
TF-CBT
ARC
SPARCS
NCTSN FY 2010 Annual Progress Report – Executive Summary
*Significant decreases on CBCL scores; no significant differences across interventions
66--Month Change in UCLA PTSDMonth Change in UCLA PTSD--RI RI
ScoresScores
15
17
19
21
23
25
27
29
Baseline 3 Months* 6 Months*
TF-CBT
ARC
NCTSN FY 2010 Annual Progress Report – Executive Summary
*Significant decreases on CBCL scores; no significant differences across interventions

Hilary Hodgdon, Ph.D. – Complex Trauma in Children 17
ARC Treatment Outcomes to DateARC Treatment Outcomes to Date
�� PTSD Symptom Reduction (Outpatient, PTSD Symptom Reduction (Outpatient, Residential)Residential)
�� Child Behavior Improvement (CBCL) Child Behavior Improvement (CBCL) ((Outpt/ResiOutpt/Resi))�� Outpatient (85%percentile to 50% percentile)Outpatient (85%percentile to 50% percentile)
�� Residential (sig reduction Externalizing Problems; Residential (sig reduction Externalizing Problems; positive trend Internalizing)positive trend Internalizing)
�� Significant Restraint Reduction (JRI)Significant Restraint Reduction (JRI)
�� Significant increase in Placement Permanency Significant increase in Placement Permanency (92% vs. under 50%) (ACMHS)(92% vs. under 50%) (ACMHS)
�� Increased staff perceived competence, reduced Increased staff perceived competence, reduced staff burnout and turnover (VTstaff burnout and turnover (VT--DMH)DMH)
ARC Intervention ComponentsARC Intervention Components
�� Integration into clinical work (structured and Integration into clinical work (structured and unstructured); individual and/or dyadic unstructured); individual and/or dyadic applicationapplication
�� Caregiver support Caregiver support
�� Caregiver training workshopsCaregiver training workshops
�� Group treatmentGroup treatment
�� Milieu training, consultation, and staff supportMilieu training, consultation, and staff support
�� Milieu interventions and initiativesMilieu interventions and initiatives
�� CommunityCommunity--based applicationsbased applications
��Importance of building an internal team to Importance of building an internal team to support integration goalssupport integration goals

Hilary Hodgdon, Ph.D. – Complex Trauma in Children 18
Attachment: The Big PictureAttachment: The Big Picture
�� OverarchingOverarching: Develop safety and positive : Develop safety and positive
capacities within the childcapacities within the child’’s caregiving s caregiving
systemsystem
�� How?How?
�� Supporting caregiversSupporting caregivers
�� Increasing knowledge and skillsIncreasing knowledge and skills
�� Creating positive relationshipsCreating positive relationships
�� Increasing predictabilityIncreasing predictability
SelfSelf--Regulation: The Big PictureRegulation: The Big Picture
�� OverarchingOverarching: Increase child/adolescent capacity : Increase child/adolescent capacity to manage emotional and physiological to manage emotional and physiological experienceexperience
�� How?How?�� Build a language for emotions, energy, and body Build a language for emotions, energy, and body
statesstates
�� Build capacity to recognize these states in self and Build capacity to recognize these states in self and otherother
�� Explore and support use of tools (individual as well as Explore and support use of tools (individual as well as external and systemic) to better manage experienceexternal and systemic) to better manage experience
�� Increase communication resources, and capacities to Increase communication resources, and capacities to use those resources effectivelyuse those resources effectively
Hilary Hodgdon, Ph.D. – Complex Trauma in Children 19
Competency: The Big PictureCompetency: The Big Picture
�� OverarchingOverarching: Support key reflective capacities, : Support key reflective capacities,
including ability to make active choices and including ability to make active choices and
sense of selfsense of self
�� How?How?
�� Notice choices, assist with problemNotice choices, assist with problem--solving, link solving, link
actions and outcomes, and reflect on causeactions and outcomes, and reflect on cause--andand--
effecteffect
�� Tune in (and support child in tuning in) to attributes, Tune in (and support child in tuning in) to attributes,
experiences, values, goals, opinions, etc.experiences, values, goals, opinions, etc.
�� Pay attention to the range of areas in which a child Pay attention to the range of areas in which a child
may build developmental masterymay build developmental mastery
Trauma Experience Integration: Trauma Experience Integration:
The Big PictureThe Big Picture
�� OverarchingOverarching: Support self: Support self--reflective reflective capacities, and ability to understand the capacities, and ability to understand the self and act in the self and act in the presentpresent, while taking , while taking into account the context of the past.into account the context of the past.
�� How?How?�� Doing all of those things weDoing all of those things we’’ve just talked ve just talked
aboutabout……..the integration of many different ..the integration of many different skills to manage, tolerate, explore, and skills to manage, tolerate, explore, and understand personal experience, understand personal experience, relationships, and systems of meaningrelationships, and systems of meaning
Hilary Hodgdon, Ph.D. – Complex Trauma in Children 20
AttachmentSelf-
Regulation Competency
Trauma
Experience
Integration
Attachment
Main / Overarching Domain Concept: Build safe / trauma-informed caregivingsystems and safe relationships that support children / adolescents
Attunement: Core Target / Goal
Help caregivers to better understand children / adolescents
Key Sub-skills/Clinical Objectives:
-Build active curiosity
-Build reflective listening skills
-Use attunement skills in support of youth regulation
-Build pleasure / positive engagement
Techniques:
i.e., Dyadic check-ins, feeling charades, etc.

Hilary Hodgdon, Ph.D. – Complex Trauma in Children 21
ATTACHMENTATTACHMENT
Caregiver Affect Mgmt.
Attunement Consistent Response
Routines and
Rituals
Caregiver Affect ManagementCaregiver Affect Management
�� The Main Idea:The Main Idea: Support the childSupport the child’’s s
caregiving system caregiving system –– whether parents or whether parents or
professionals professionals –– in understanding, in understanding,
managing, and coping with their own managing, and coping with their own
emotional responses, so that they are emotional responses, so that they are
better able to support the children in their better able to support the children in their
care.care.Caregiver
Affect
Mgmt.
Hilary Hodgdon, Ph.D. – Complex Trauma in Children 22
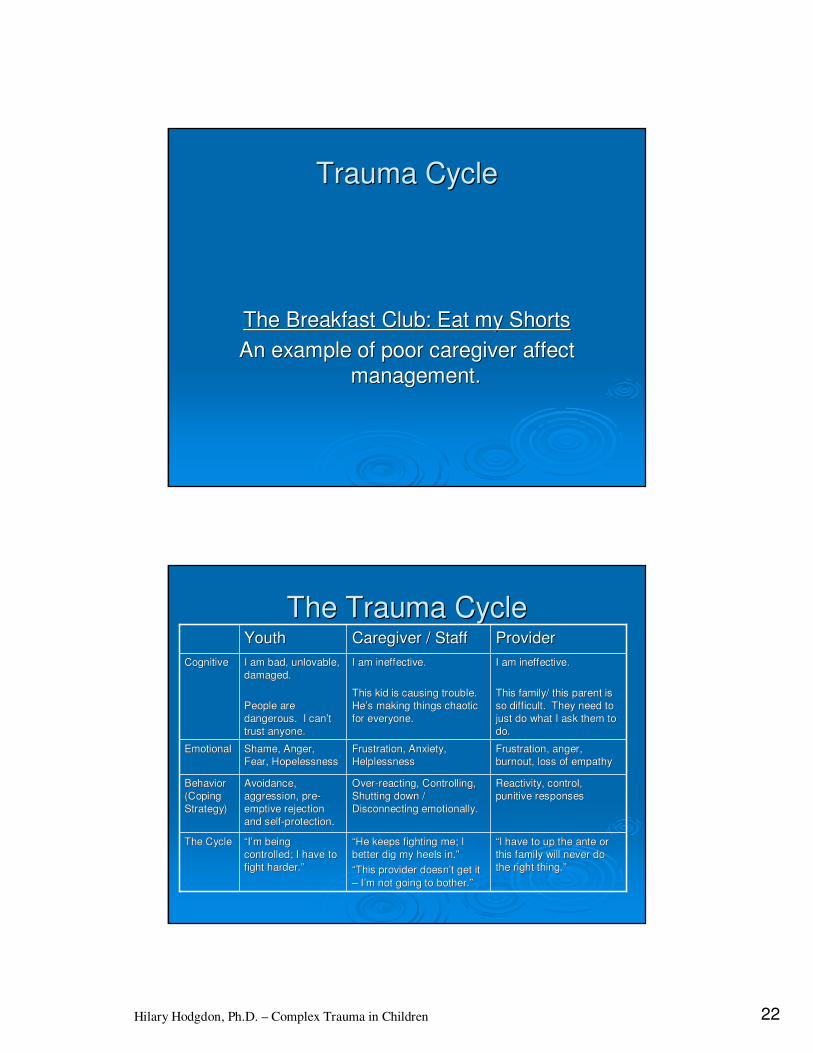
Trauma CycleTrauma Cycle
The Breakfast Club: Eat my ShortsThe Breakfast Club: Eat my Shorts
An example of poor caregiver affect An example of poor caregiver affect
management.management.
The Trauma CycleThe Trauma Cycle
““I have to up the ante or I have to up the ante or
this family will never do this family will never do
the right thing.the right thing.””
Reactivity, control, Reactivity, control,
punitive responsespunitive responses
Frustration, anger, Frustration, anger,
burnout, loss of empathyburnout, loss of empathy
I am ineffective.I am ineffective.
This family/ this parent is This family/ this parent is
so difficult. They need to so difficult. They need to
just do what I ask them to just do what I ask them to
do.do.
ProviderProvider
““He keeps fighting me; I He keeps fighting me; I
better dig my heels in.better dig my heels in.””
““This provider doesnThis provider doesn’’t get it t get it
–– II’’m not going to bother.m not going to bother.””
““II’’m being m being
controlled; I have to controlled; I have to
fight harder.fight harder.””
The CycleThe Cycle
OverOver--reacting, Controlling, reacting, Controlling,
Shutting down / Shutting down /
Disconnecting emotionally.Disconnecting emotionally.
Avoidance, Avoidance,
aggression, preaggression, pre--
emptive rejection emptive rejection
and selfand self--protection.protection.
Behavior Behavior
(Coping (Coping
Strategy)Strategy)
Frustration, Anxiety, Frustration, Anxiety,
HelplessnessHelplessnessShame, Anger, Shame, Anger,
Fear, HopelessnessFear, HopelessnessEmotionalEmotional
I am ineffective.I am ineffective.
This kid is causing trouble. This kid is causing trouble.
HeHe’’s making things chaotic s making things chaotic
for everyone.for everyone.
I am bad, unlovable, I am bad, unlovable,
damaged.damaged.
People are People are
dangerous. I candangerous. I can’’t t
trust anyone.trust anyone.
CognitiveCognitive
Caregiver / StaffCaregiver / StaffYouthYouth
Hilary Hodgdon, Ph.D. – Complex Trauma in Children 23
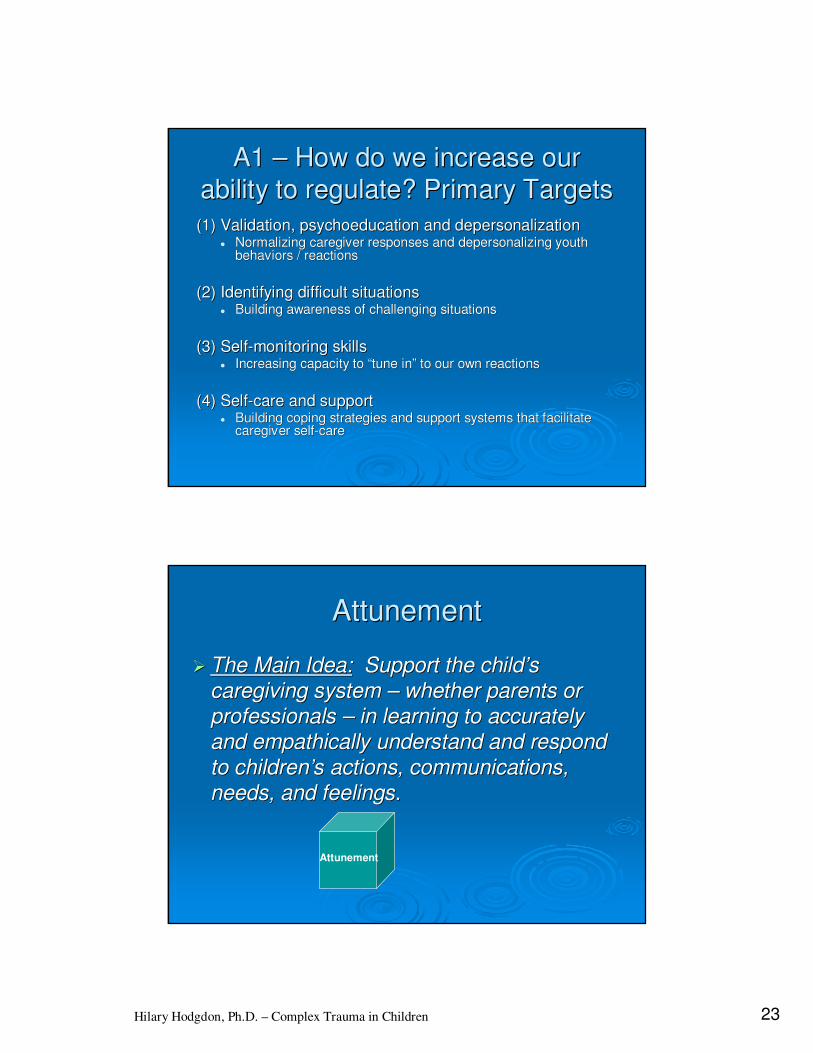
A1 A1 –– How do we increase our How do we increase our
ability to regulate? Primary Targetsability to regulate? Primary Targets
(1) Validation, (1) Validation, psychoeducationpsychoeducation and depersonalizationand depersonalization�� Normalizing caregiver responses and depersonalizing youth Normalizing caregiver responses and depersonalizing youth
behaviors / reactionsbehaviors / reactions
(2) Identifying difficult situations(2) Identifying difficult situations�� Building awareness of challenging situationsBuilding awareness of challenging situations
(3) Self(3) Self--monitoring skillsmonitoring skills�� Increasing capacity to Increasing capacity to ““tune intune in”” to our own reactionsto our own reactions
(4) Self(4) Self--care and supportcare and support�� Building coping strategies and support systems that facilitate Building coping strategies and support systems that facilitate
caregiver selfcaregiver self--carecare
AttunementAttunement
�� The Main Idea:The Main Idea: Support the childSupport the child’’s s
caregiving system caregiving system –– whether parents or whether parents or
professionals professionals –– in learning to accurately in learning to accurately
and empathically understand and respond and empathically understand and respond
to childrento children’’s actions, communications, s actions, communications,
needs, and feelings.needs, and feelings.
Attunement
Hilary Hodgdon, Ph.D. – Complex Trauma in Children 24
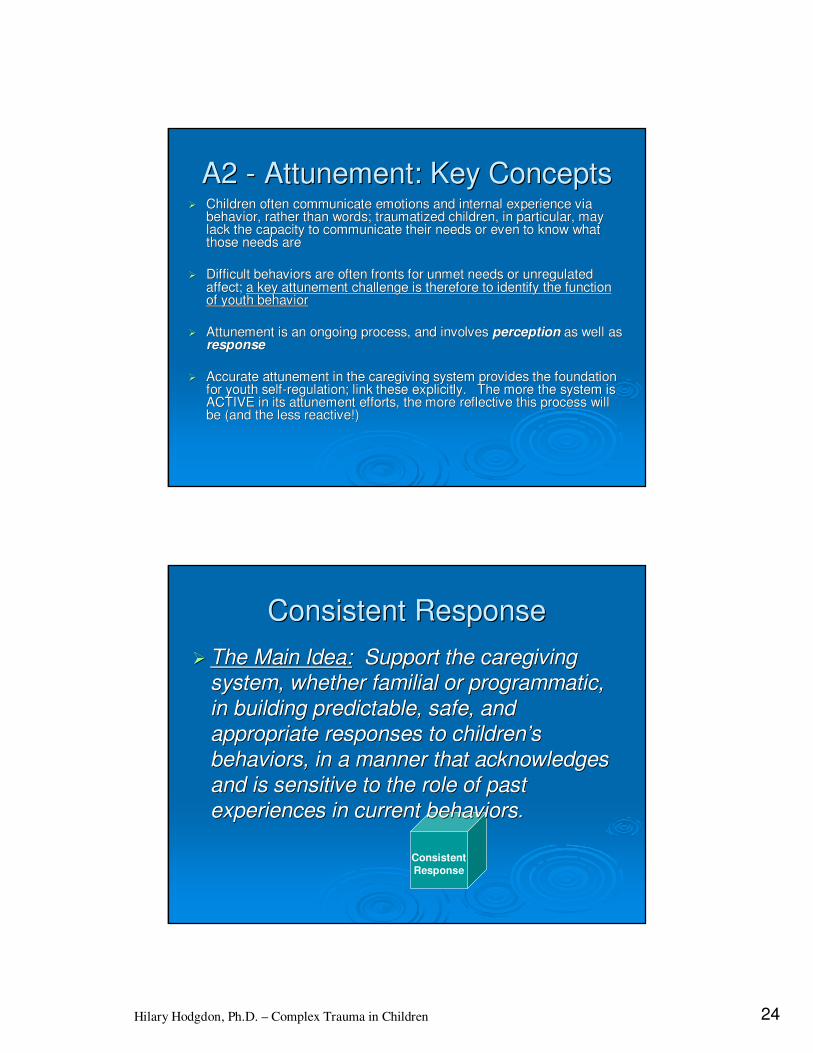
A2 A2 -- Attunement: Key ConceptsAttunement: Key Concepts�� Children often communicate emotions and internal experience via Children often communicate emotions and internal experience via
behavior, rather than words; traumatized children, in particularbehavior, rather than words; traumatized children, in particular, may , may lack the capacity to communicate their needs or even to know whalack the capacity to communicate their needs or even to know what t those needs arethose needs are
�� Difficult behaviors are often fronts for unmet needs or unregulaDifficult behaviors are often fronts for unmet needs or unregulated ted affect; affect; a key attunement challenge is therefore to identify the functiona key attunement challenge is therefore to identify the functionof youth behaviorof youth behavior
�� Attunement is an ongoing process, and involves Attunement is an ongoing process, and involves perceptionperception as well as as well as responseresponse
�� Accurate attunement in the caregiving system provides the foundaAccurate attunement in the caregiving system provides the foundation tion for youth selffor youth self--regulation; link these explicitly. The more the system is regulation; link these explicitly. The more the system is ACTIVE in its attunement efforts, the more reflective this proceACTIVE in its attunement efforts, the more reflective this process will ss will be (and the less reactive!)be (and the less reactive!)
Consistent
Response
Consistent ResponseConsistent Response
�� The Main Idea:The Main Idea: Support the caregiving Support the caregiving
system, whether familial or programmatic, system, whether familial or programmatic,
in building predictable, safe, and in building predictable, safe, and
appropriate responses to childrenappropriate responses to children’’s s
behaviors, in a manner that acknowledges behaviors, in a manner that acknowledges
and is sensitive to the role of past and is sensitive to the role of past
experiences in current behaviors.experiences in current behaviors.

Hilary Hodgdon, Ph.D. – Complex Trauma in Children 25
An alternative approach: An alternative approach:
Two primary goalsTwo primary goals
�� (1) Incorporate the system(1) Incorporate the system’’s s understanding understanding of of
youth behavior into their youth behavior into their response toresponse to the the
behavior (i.e., incorporate attunement into youth behavior (i.e., incorporate attunement into youth
management strategies, ideally reducing the management strategies, ideally reducing the
need for limits)need for limits)
�� (2) Build responses to behavior that are (2) Build responses to behavior that are
consistent, appropriate, and sensitive to trauma consistent, appropriate, and sensitive to trauma
influences on youth responses (i.e., building influences on youth responses (i.e., building
consistent responses that consistent responses that increaseincrease, rather than , rather than
decreasedecrease, felt safety), felt safety)
Building Consistent ResponseBuilding Consistent Response
�� Support caregivers in understanding their own Support caregivers in understanding their own emotional / physiological / cognitive / behavioral emotional / physiological / cognitive / behavioral responses in the face of child behaviorsresponses in the face of child behaviors
�� Support attunement efforts: what is the function Support attunement efforts: what is the function of the childof the child’’s behavior? Is this a regulation s behavior? Is this a regulation moment, or a limitmoment, or a limit--setting moment? (Or both?)setting moment? (Or both?)
�� Provide support, education, and coaching in Provide support, education, and coaching in parenting strategies, as needed. Build slowly. parenting strategies, as needed. Build slowly. Explore the caregiverExplore the caregiver’’s personal / cultural beliefs s personal / cultural beliefs about appropriate parenting and their own about appropriate parenting and their own historical parenting experiences.historical parenting experiences.
Hilary Hodgdon, Ph.D. – Complex Trauma in Children 26
Building Consistent ResponseBuilding Consistent Response
�� Actively engage youth in setting / defining / Actively engage youth in setting / defining / understanding household / milieu / understanding household / milieu / contextual rules, as appropriatecontextual rules, as appropriate
�� Explore values underlying rules, and find Explore values underlying rules, and find common groundcommon ground
�� Solicit youth input on ways adults can Solicit youth input on ways adults can support them in following established support them in following established structures; anticipate / collaborate on structures; anticipate / collaborate on building successbuilding success
Routines and RitualsRoutines and Rituals
�� The Main Idea:The Main Idea: Build predictability through Build predictability through
use of individual, familial, and systemic use of individual, familial, and systemic
routines and rituals.routines and rituals.
Routines
and
Rituals
Hilary Hodgdon, Ph.D. – Complex Trauma in Children 27
A4 A4 –– The role of routines: The role of routines:
Key ConceptsKey Concepts�� Trauma is often associated with chaos and loss of Trauma is often associated with chaos and loss of
control; predictability helps build feelings of safety in control; predictability helps build feelings of safety in traumatized childrentraumatized children
�� When children feel safe, they are able to shift their When children feel safe, they are able to shift their energy from survival to healthy developmentenergy from survival to healthy development
�� Repetition is an important way that children gain skill; Repetition is an important way that children gain skill; children often notice routines more in their absence than children often notice routines more in their absence than in their presencein their presence
�� Routines should be part of the daily fabric, as well as Routines should be part of the daily fabric, as well as targeting areas of vulnerability or difficultytargeting areas of vulnerability or difficulty
A4 A4 –– The role of ritual: The role of ritual:
Key ConceptsKey Concepts�� RitualsRituals (traditions, celebrations, patterns of experience) (traditions, celebrations, patterns of experience)
offer felt coherence among members of a family, culture, offer felt coherence among members of a family, culture, or community, and may repeat across generationsor community, and may repeat across generations
�� Shared rituals may provide a sense of belonging; feeling Shared rituals may provide a sense of belonging; feeling disconnected from dominant culture rituals may highlight disconnected from dominant culture rituals may highlight a feeling of differencea feeling of difference
�� Exploration and celebration of ritual may include both Exploration and celebration of ritual may include both establishment and celebration of establishment and celebration of wholewhole--systemsystem rituals, rituals, as well as exploration, sharing, and celebration of many as well as exploration, sharing, and celebration of many individual ritualsindividual rituals
Hilary Hodgdon, Ph.D. – Complex Trauma in Children 28
Domain 2:Domain 2:
SELFSELF--REGULATIONREGULATION
Affect Identification
ModulationAffect
Expression
Affect
Identification
Affect Identification:Affect Identification:
�� The Main Idea:The Main Idea: Work with children to build an Work with children to build an
awareness of internal experience, the ability to awareness of internal experience, the ability to
discriminate and name emotional states, and an discriminate and name emotional states, and an
understanding of where these states come from.understanding of where these states come from.

Hilary Hodgdon, Ph.D. – Complex Trauma in Children 29
ConsiderationsConsiderations
�� Pair attunement with affect identificationPair attunement with affect identification:Caregiver attunement :Caregiver attunement skills can be used to support the child in affect identificationskills can be used to support the child in affect identification. . Consider doing the work simultaneously.Consider doing the work simultaneously.
�� Be mindful of cultural influencesBe mindful of cultural influences: Culture and context impact our : Culture and context impact our language for emotion, as well as our experience of it. Be cautilanguage for emotion, as well as our experience of it. Be cautious of ous of making assumptions.making assumptions.
�� Use your own imagination and creativityUse your own imagination and creativity to create feelingsto create feelings--relevant activities.relevant activities.
�� Work with all caregiversWork with all caregivers to incorporate basic feelings identification to incorporate basic feelings identification into their own interactions with the child.into their own interactions with the child.
�� Choose your momentsChoose your moments: Much of this work happens in the : Much of this work happens in the moment, and in conversation. Tune into opportunities to exploremoment, and in conversation. Tune into opportunities to exploreaffect in the material children are already bringing in.affect in the material children are already bringing in.
Affect Identification Affect Identification -- BasicBasic

Hilary Hodgdon, Ph.D. – Complex Trauma in Children 30
Affect Identification Affect Identification -- BasicBasic
Affect
Modulation
ModulationModulation
�� The Main Idea:The Main Idea: Work with children to develop Work with children to develop
safe and effective strategies to manage and safe and effective strategies to manage and
regulate physiological and emotional regulate physiological and emotional
experience, in service of maintaining a experience, in service of maintaining a
comfortable state of arousal.comfortable state of arousal.

Hilary Hodgdon, Ph.D. – Complex Trauma in Children 31
ModulationModulation
Little Girl Throwing a TantrumLittle Girl Throwing a Tantrum
R2 R2 -- ModulationModulationModulation Involves Multiple SkillsModulation Involves Multiple Skills::
�� Ability to identify initial emotional/physiological stateAbility to identify initial emotional/physiological state
�� Ability to identify and Ability to identify and connectconnect to subtle changes in state. to subtle changes in state. A note about A note about connectionconnection: This is the ability to : This is the ability to tune intotune into, , toleratetolerate, and , and sustainsustain connection to connection to emotional/physiological states. emotional/physiological states.
�� Ability to identify what it Ability to identify what it feelsfeels like in the body to like in the body to experience subtle changes in stateexperience subtle changes in state
�� Ability to identify and use strategies to manage those Ability to identify and use strategies to manage those state changesstate changes
Hilary Hodgdon, Ph.D. – Complex Trauma in Children 32
R2 R2 -- ModulationModulationSpecific Targets / SkillsSpecific Targets / Skills: :
�� Build understanding of Build understanding of comfortablecomfortable and and effectiveeffective states states
�� Build an understanding of degrees of feelings and Build an understanding of degrees of feelings and energyenergy
�� Support children in exploring arousal states, and in Support children in exploring arousal states, and in developing a sense of agency over tools that allow them developing a sense of agency over tools that allow them to manage emotions and energy (build a to manage emotions and energy (build a ““feelings feelings toolboxtoolbox””). ).
�� Support and facilitate strategies which effectively and Support and facilitate strategies which effectively and comfortably lead to state changescomfortably lead to state changes
Modulation: Safe PlaceModulation: Safe Place

Hilary Hodgdon, Ph.D. – Complex Trauma in Children 33
Affect Expression:Affect Expression:
�� The Main Idea:The Main Idea: Help children build the Help children build the
skills and tolerance for effectively sharing skills and tolerance for effectively sharing
emotional experience with othersemotional experience with others
Affect
Expression
R3 R3 –– Key Skills and TargetsKey Skills and Targets
�� Exploration of the goals of expression; Exploration of the goals of expression; build comfort and safety in relationshipbuild comfort and safety in relationship
�� Identifying resources for safe expressionIdentifying resources for safe expression
�� Effectively using resourcesEffectively using resources�� Initiating communicationInitiating communication
�� Effective nonverbal communication skillsEffective nonverbal communication skills
�� Effective verbal communication skillsEffective verbal communication skills
�� Building and supporting forums for selfBuilding and supporting forums for self--expressionexpression
Hilary Hodgdon, Ph.D. – Complex Trauma in Children 34
Domain 3: CompetencyDomain 3: Competency
Dev’tal Tasks
Executive
FunctionsSelf Dev’t
& Identity
Developmental CompetenciesDevelopmental Competencies
�� Each developmental stage builds on the learning and Each developmental stage builds on the learning and experience of the previous stageexperience of the previous stage
�� Competency and mastery of tasks at each stage lead to Competency and mastery of tasks at each stage lead to construction of an internal sense of construction of an internal sense of efficacyefficacy and and achievementachievement; in turn, this increases confidence in ; in turn, this increases confidence in approaching new tasksapproaching new tasks
�� When children are exposed to chronic trauma, energy When children are exposed to chronic trauma, energy that is normally invested into development of that is normally invested into development of competencies is instead invested in survivalcompetencies is instead invested in survival

Hilary Hodgdon, Ph.D. – Complex Trauma in Children 35
Executive FunctionsExecutive Functions
�� The Main Idea:The Main Idea: Work with children to act, Work with children to act,
instead of react, by using higherinstead of react, by using higher--order order
cognitive processes to solve problems and cognitive processes to solve problems and
make active choices in service of reaching make active choices in service of reaching
identified goalsidentified goals
Executive
Functions
Self and IdentitySelf and Identity
�� The Main Idea:The Main Idea: Support children in Support children in
exploring and building an understanding of exploring and building an understanding of
self and personal identity, including self and personal identity, including
identification of unique and positive identification of unique and positive
qualities, building of coherence across qualities, building of coherence across
time and experience, and support in the time and experience, and support in the
capacity to imagine and work toward a capacity to imagine and work toward a
range of future possibilitiesrange of future possibilities
Self Dev’t
& Identity
Hilary Hodgdon, Ph.D. – Complex Trauma in Children 36
ConsiderationsConsiderations
�� Consider group as well as individual identity goals for all Consider group as well as individual identity goals for all domains; i.e.:domains; i.e.:�� Unique self:Unique self:
•• What characteristics does each child contribute?What characteristics does each child contribute?
•• What makes this setting unique? (Group values, goals, etc.)What makes this setting unique? (Group values, goals, etc.)
�� Positive self:Positive self:•• Support and reinforce child successesSupport and reinforce child successes
•• Establish community pride; set collaborative group goalsEstablish community pride; set collaborative group goals
�� Coherent self:Coherent self:•• Notice and normalize differences in child presentation and Notice and normalize differences in child presentation and
experience across moments and settingexperience across moments and setting
•• Notice coherence and fragmentation among group membersNotice coherence and fragmentation among group members
�� Future self:Future self:•• Support individual youth in setting and working toward future goSupport individual youth in setting and working toward future goalsals
•• Set programmatic / community goals, and support members of the Set programmatic / community goals, and support members of the system in working toward thesesystem in working toward these
Trauma Experience IntegrationTrauma Experience Integration
The Main Idea: The Main Idea: Work with children to actively Work with children to actively
explore, process, and integrate historical explore, process, and integrate historical
experiences into a coherent and comprehensive experiences into a coherent and comprehensive
understanding of self in order to enhance understanding of self in order to enhance
childrenchildren’’s capacity to effectively engage in s capacity to effectively engage in
present life.present life.
Trauma
Experience
Integration
The Main Idea: The Main Idea: Work with children to actively Work with children to actively
explore, process, and integrate historical explore, process, and integrate historical
experiences into a coherent and comprehensive experiences into a coherent and comprehensive
understanding of self understanding of self in order toin order to enhance enhance
childrenchildren’’s capacity to effectively engage in s capacity to effectively engage in
present lifepresent life..

Hilary Hodgdon, Ph.D. – Complex Trauma in Children 37
Children are not simply a composite of their Children are not simply a composite of their
deficits, but are whole beings, with deficits, but are whole beings, with
strengths, vulnerabilities, challenges, and strengths, vulnerabilities, challenges, and
resources.resources.
ARC provides a framework that seeks to ARC provides a framework that seeks to
recognize factors that derail normative recognize factors that derail normative
development, and to work with children, development, and to work with children,
families, and systems to build or refamilies, and systems to build or re--build build
healthy developmental pathways.healthy developmental pathways.
Sensory Motor Arousal Sensory Motor Arousal
Regulation Therapy Regulation Therapy
(SMART)(SMART)
Hilary Hodgdon, Ph.D. – Complex Trauma in Children 38
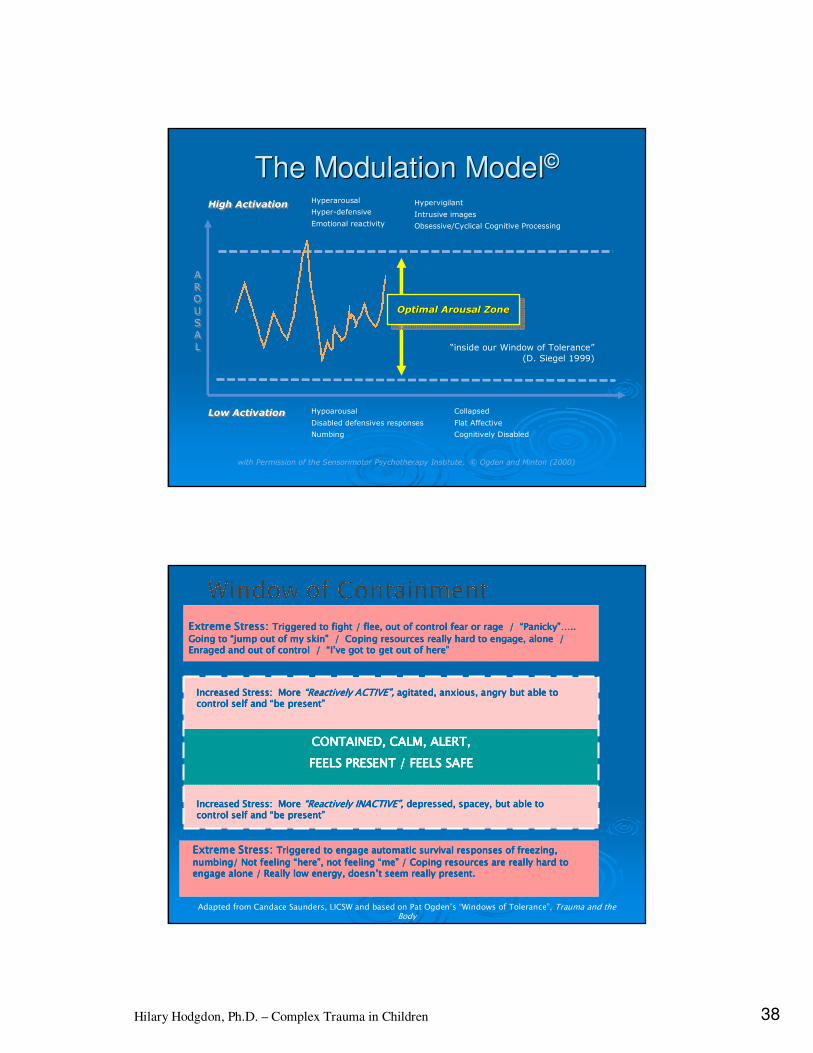
The Modulation ModelThe Modulation Model©©
High ActivationHigh Activation
with Permission of the Sensorimotor Psychotherapy Institute, © Ogden and Minton (2000)
A
RO
US
AL
A
RO
US
AL
Hyperarousal
Hyper-defensive
Emotional reactivity
Hypoarousal
Disabled defensives responses
Numbing
“inside our Window of Tolerance”
(D. Siegel 1999)
Optimal Arousal ZoneOptimal Arousal ZoneOptimal Arousal Zone
Hypervigilant
Intrusive images
Obsessive/Cyclical Cognitive Processing
Low ActivationLow Activation Collapsed
Flat Affective
Cognitively Disabled
Extreme Stress:Extreme Stress:Extreme Stress:Extreme Stress: Triggered to fight / flee, out of control fear or rage / Triggered to fight / flee, out of control fear or rage / Triggered to fight / flee, out of control fear or rage / Triggered to fight / flee, out of control fear or rage / ““““PanickyPanickyPanickyPanicky”…”…”…”….. .. .. ..
Going to Going to Going to Going to ““““jump out of my skinjump out of my skinjump out of my skinjump out of my skin”””” / Coping resources really hard to engage, alone / / Coping resources really hard to engage, alone / / Coping resources really hard to engage, alone / / Coping resources really hard to engage, alone / Enraged and out of control / Enraged and out of control / Enraged and out of control / Enraged and out of control / ““““IIII’’’’ve got to get out of hereve got to get out of hereve got to get out of hereve got to get out of here””””
Extreme Stress:Extreme Stress:Extreme Stress:Extreme Stress: Triggered to engage automatic survival responses of freezing, Triggered to engage automatic survival responses of freezing, Triggered to engage automatic survival responses of freezing, Triggered to engage automatic survival responses of freezing,
numbing/ Not feeling numbing/ Not feeling numbing/ Not feeling numbing/ Not feeling ““““herehereherehere””””, not feeling , not feeling , not feeling , not feeling ““““memememe”””” / Coping resources are really hard to / Coping resources are really hard to / Coping resources are really hard to / Coping resources are really hard to engage alone / Really low energy, doesnengage alone / Really low energy, doesnengage alone / Really low energy, doesnengage alone / Really low energy, doesn’’’’t seem really present.t seem really present.t seem really present.t seem really present.
CONTAINED, CALM, ALERT,CONTAINED, CALM, ALERT,CONTAINED, CALM, ALERT,CONTAINED, CALM, ALERT,
FEELS PRESENT / FEELS SAFEFEELS PRESENT / FEELS SAFEFEELS PRESENT / FEELS SAFEFEELS PRESENT / FEELS SAFE
Adapted from Candace Saunders, LICSW and based on Pat Ogden’s “Windows of Tolerance”, Trauma and the Body
Increased Stress: More Increased Stress: More Increased Stress: More Increased Stress: More ““““Reactively ACTIVEReactively ACTIVEReactively ACTIVEReactively ACTIVE””””,,,, agitated, anxious, angry but able to agitated, anxious, angry but able to agitated, anxious, angry but able to agitated, anxious, angry but able to control self and control self and control self and control self and ““““be presentbe presentbe presentbe present””””
Increased Stress: More Increased Stress: More Increased Stress: More Increased Stress: More ““““Reactively INACTIVEReactively INACTIVEReactively INACTIVEReactively INACTIVE””””,,,, depressed, spacey, but able to depressed, spacey, but able to depressed, spacey, but able to depressed, spacey, but able to control self and control self and control self and control self and ““““be presentbe presentbe presentbe present””””
Hilary Hodgdon, Ph.D. – Complex Trauma in Children 39
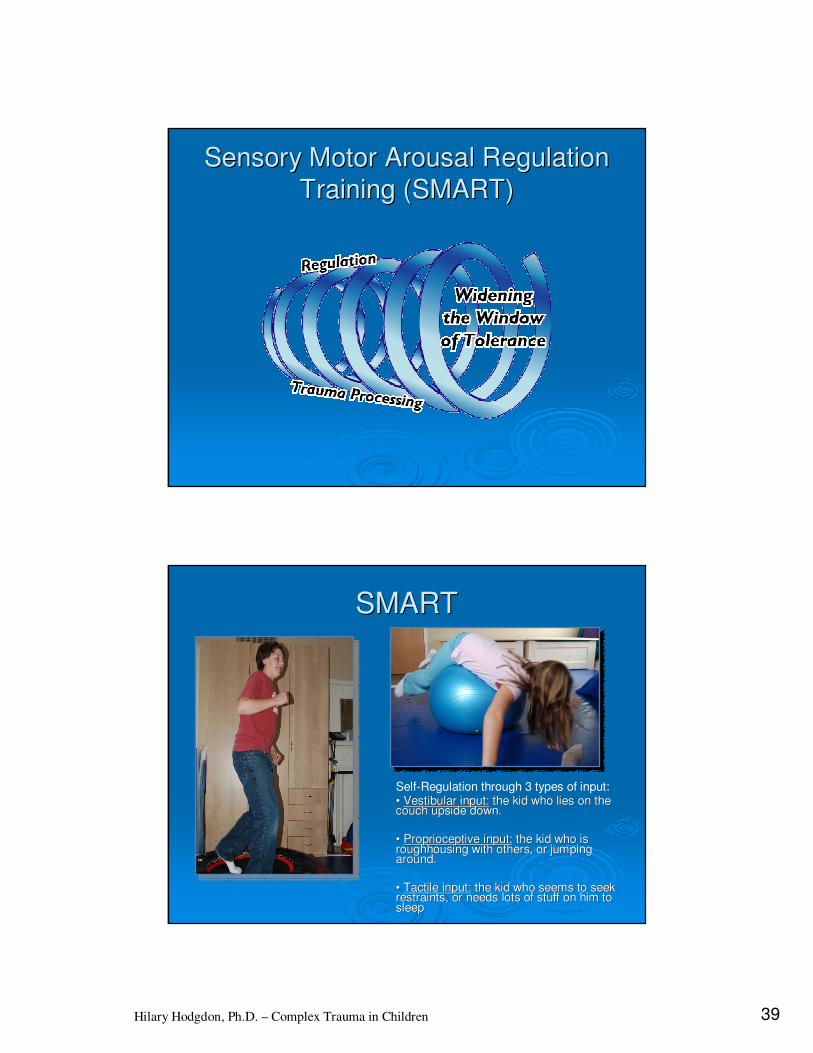
Sensory Motor Arousal Regulation Sensory Motor Arousal Regulation
Training (SMART)Training (SMART)
SMARTSMART
Self-Regulation through 3 types of input:•• Vestibular input:Vestibular input: the kid who lies on the the kid who lies on the couch upside down.couch upside down.
•• ProprioceptiveProprioceptive input:input: the kid who is the kid who is roughhousing with others, or jumping roughhousing with others, or jumping around.around.
•• Tactile input:Tactile input: the kid who seems to seek the kid who seems to seek restraints, or needs lots of stuff on him to restraints, or needs lots of stuff on him to sleepsleep
Hilary Hodgdon, Ph.D. – Complex Trauma in Children 40
Why SMART for trauma?Why SMART for trauma?
A treatment aimed at A treatment aimed at subcorticalsubcortical as well asas well as
cortical systems:cortical systems:..
�� Begins with movement and sensation, exploration and Begins with movement and sensation, exploration and
curiosity as routes to better regulation.curiosity as routes to better regulation.
�� Does not rely on language as entry point.Does not rely on language as entry point.
�� Allows integration of affect through Allows integration of affect through engagement of the engagement of the whole body.whole body.
�� Cognitive understanding or a coherent narrative emerges Cognitive understanding or a coherent narrative emerges
as the consequence of full engagement of the as the consequence of full engagement of the subcorticalsubcortical
systems (sensory, motor, limbic/emotional, and autonomic systems (sensory, motor, limbic/emotional, and autonomic
arousal).arousal).
�� Uses present moment new experience to expand and Uses present moment new experience to expand and
create new capacity for attachment through cocreate new capacity for attachment through co-- and selfand self--
regulation.regulation.
NeurofeedbackNeurofeedback (NFB)(NFB)
Hilary Hodgdon, Ph.D. – Complex Trauma in Children 41
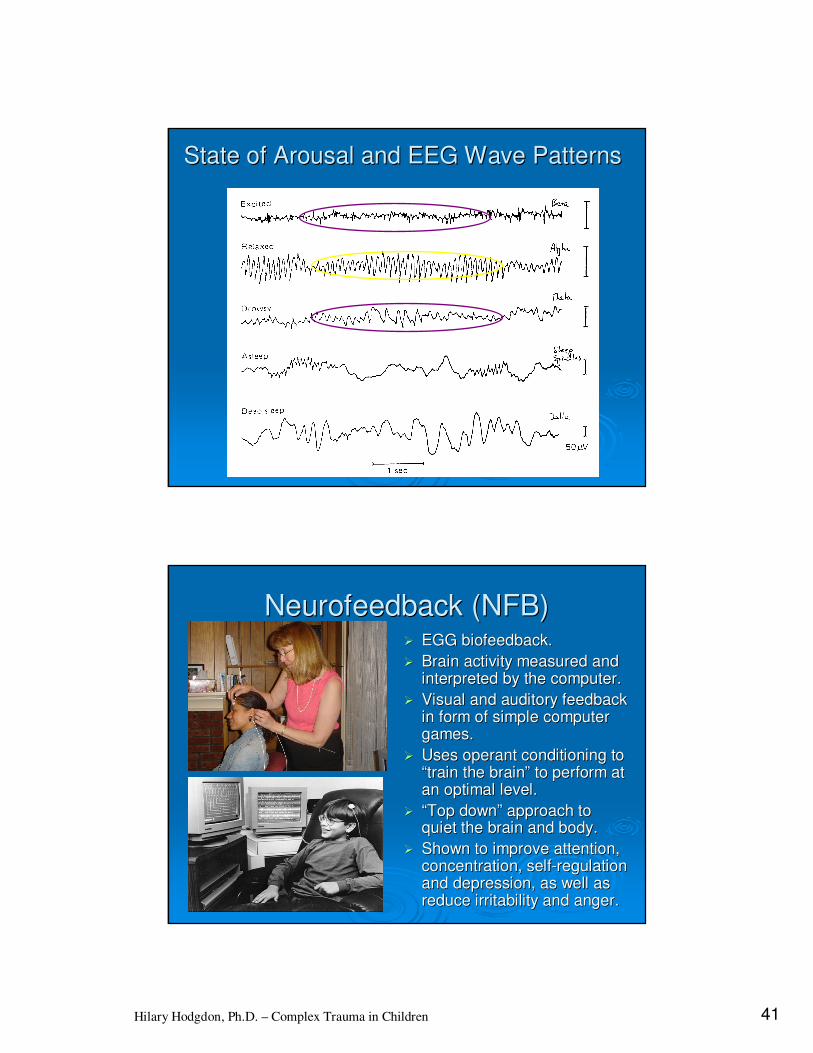
State of Arousal and EEG Wave PatternsState of Arousal and EEG Wave Patterns
NeurofeedbackNeurofeedback (NFB)(NFB)�� EGG biofeedback.EGG biofeedback.
�� Brain activity measured and Brain activity measured and interpreted by the computer.interpreted by the computer.
�� Visual and auditory feedback Visual and auditory feedback in form of simple computer in form of simple computer games.games.
�� Uses operant conditioning to Uses operant conditioning to ““train the braintrain the brain”” to perform at to perform at an optimal level.an optimal level.
�� ““Top downTop down”” approach to approach to quiet the brain and body.quiet the brain and body.
�� Shown to improve attention, Shown to improve attention, concentration, selfconcentration, self--regulation regulation and depression, as well as and depression, as well as reduce irritability and anger.reduce irritability and anger.

Hilary Hodgdon, Ph.D. – Complex Trauma in Children 42
NFB Trauma ProtocolNFB Trauma Protocol
�� T4T4--P4 placement.P4 placement.
�� Training focused on Training focused on inhibiting slow wave inhibiting slow wave (Delta and Theta) and (Delta and Theta) and high wave (High Beta) high wave (High Beta) activity, while rewarding activity, while rewarding Alpha activity.Alpha activity.
�� Protocol designed to Protocol designed to increase selfincrease self--regulation regulation and reduce and reduce hypersensitivity to stimuli.hypersensitivity to stimuli.
Case ExampleCase Example
Hilary Hodgdon, Ph.D. – Complex Trauma in Children 43
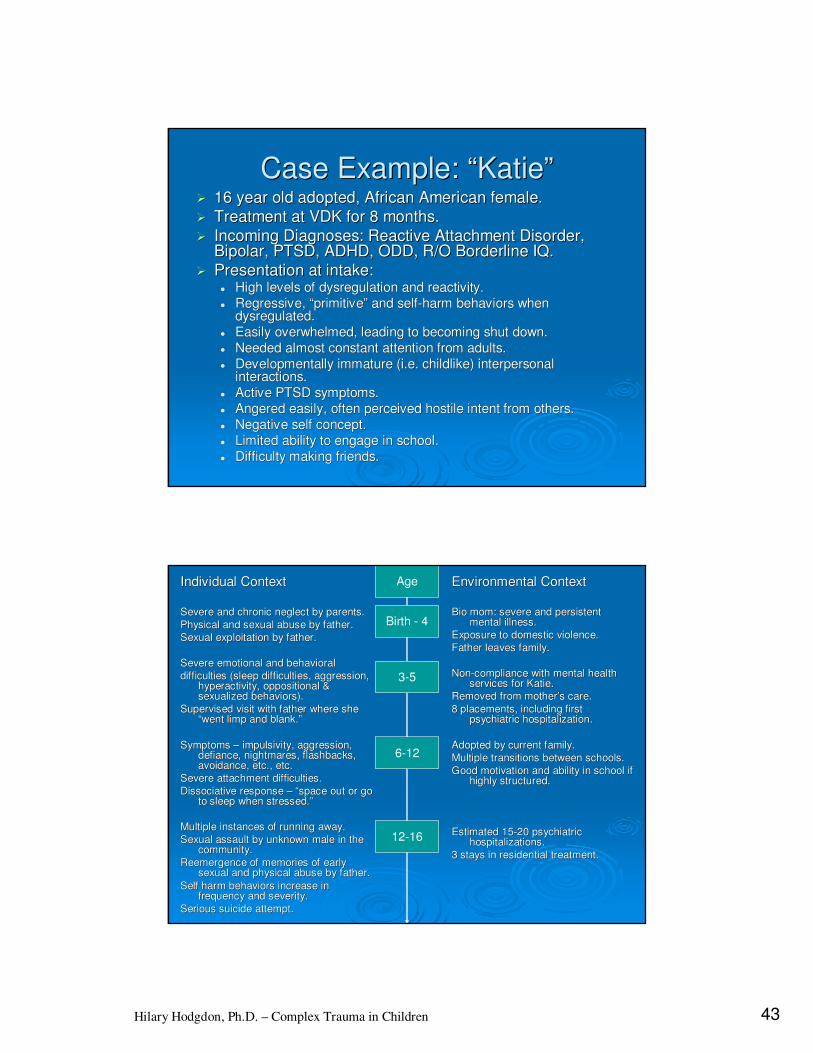
Case Example: Case Example: ““KatieKatie””�� 16 year old adopted, African American female.16 year old adopted, African American female.
�� Treatment at VDK for 8 months.Treatment at VDK for 8 months.
�� Incoming Diagnoses: Reactive Attachment Disorder, Incoming Diagnoses: Reactive Attachment Disorder, Bipolar, PTSD, ADHD, ODD, R/O Borderline IQ.Bipolar, PTSD, ADHD, ODD, R/O Borderline IQ.
�� Presentation at intake:Presentation at intake:�� High levels of High levels of dysregulationdysregulation and reactivity.and reactivity.�� Regressive, Regressive, ““primitiveprimitive”” and selfand self--harm behaviors when harm behaviors when
dysregulateddysregulated..�� Easily overwhelmed, leading to becoming shut down.Easily overwhelmed, leading to becoming shut down.�� Needed almost constant attention from adults.Needed almost constant attention from adults.�� Developmentally immature (i.e. childlike) interpersonal Developmentally immature (i.e. childlike) interpersonal
interactions.interactions.�� Active PTSD symptoms.Active PTSD symptoms.�� Angered easily, often perceived hostile intent from others.Angered easily, often perceived hostile intent from others.�� Negative self concept.Negative self concept.�� Limited ability to engage in school.Limited ability to engage in school.�� Difficulty making friends.Difficulty making friends.
Individual ContextIndividual Context
Severe and chronic neglect by parents.Severe and chronic neglect by parents.
Physical and sexual abuse by father.Physical and sexual abuse by father.
Sexual exploitation by father.Sexual exploitation by father.
Severe emotional and behavioralSevere emotional and behavioral
difficulties (sleep difficulties, aggression, difficulties (sleep difficulties, aggression, hyperactivity, oppositional & hyperactivity, oppositional & sexualized behaviors).sexualized behaviors).
Supervised visit with father where she Supervised visit with father where she ““went limp and blank.went limp and blank.””
Symptoms Symptoms –– impulsivity, aggression, impulsivity, aggression, defiance, nightmares, flashbacks, defiance, nightmares, flashbacks, avoidance, etc., etc.avoidance, etc., etc.
Severe attachment difficulties.Severe attachment difficulties.
Dissociative response Dissociative response –– ““space out or go space out or go to sleep when stressed.to sleep when stressed.””
Multiple instances of running away. Multiple instances of running away.
Sexual assault by unknown male in the Sexual assault by unknown male in the community.community.
Reemergence of memories of early Reemergence of memories of early sexual and physical abuse by father.sexual and physical abuse by father.
Self harm behaviors increase in Self harm behaviors increase in frequency and severity.frequency and severity.
Serious suicide attempt.Serious suicide attempt.
Environmental ContextEnvironmental Context
Bio mom: severe and persistent Bio mom: severe and persistent mental illness.mental illness.
Exposure to domestic violence.Exposure to domestic violence.
Father leaves family.Father leaves family.
NonNon--compliance with mental health compliance with mental health services for Katie.services for Katie.
Removed from motherRemoved from mother’’s care.s care.
8 placements, including first 8 placements, including first psychiatric hospitalization.psychiatric hospitalization.
Adopted by current family.Adopted by current family.
Multiple transitions between schools.Multiple transitions between schools.
Good motivation and ability in school if Good motivation and ability in school if highly structured.highly structured.
Estimated 15Estimated 15--20 psychiatric 20 psychiatric hospitalizations. hospitalizations.
3 stays in residential treatment.3 stays in residential treatment.
Birth - 4
3-5
Age
6-12
12-16
Hilary Hodgdon, Ph.D. – Complex Trauma in Children 44
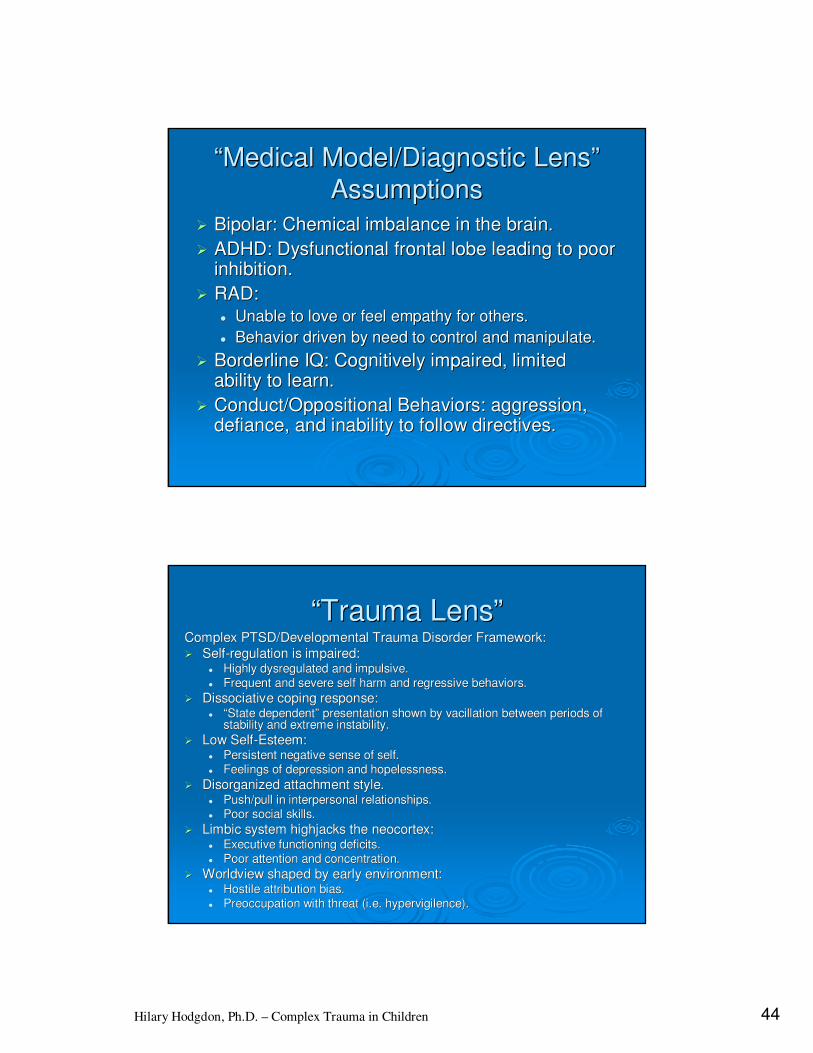
““Medical Model/Diagnostic LensMedical Model/Diagnostic Lens””
AssumptionsAssumptions
�� Bipolar: Chemical imbalance in the brain.Bipolar: Chemical imbalance in the brain.
�� ADHD: Dysfunctional frontal lobe leading to poor ADHD: Dysfunctional frontal lobe leading to poor inhibition.inhibition.
�� RAD: RAD: �� Unable to love or feel empathy for others.Unable to love or feel empathy for others.
�� Behavior driven by need to control and manipulate.Behavior driven by need to control and manipulate.
�� Borderline IQ: Cognitively impaired, limited Borderline IQ: Cognitively impaired, limited ability to learn.ability to learn.
�� Conduct/Oppositional Behaviors: aggression, Conduct/Oppositional Behaviors: aggression, defiance, and inability to follow directives.defiance, and inability to follow directives.
““Trauma LensTrauma Lens””Complex PTSD/Developmental Trauma Disorder Framework:Complex PTSD/Developmental Trauma Disorder Framework:
�� SelfSelf--regulation is impaired: regulation is impaired: �� Highly Highly dysregulateddysregulated and impulsive. and impulsive. �� Frequent and severe self harm and regressive behaviors.Frequent and severe self harm and regressive behaviors.
�� Dissociative coping response: Dissociative coping response: �� ““State dependentState dependent”” presentation shown by vacillation between periods of presentation shown by vacillation between periods of
stability and extreme instability.stability and extreme instability.
�� Low SelfLow Self--Esteem:Esteem:�� Persistent negative sense of self.Persistent negative sense of self.�� Feelings of depression and hopelessness.Feelings of depression and hopelessness.
�� Disorganized attachment style.Disorganized attachment style.�� Push/pull in interpersonal relationships.Push/pull in interpersonal relationships.�� Poor social skills.Poor social skills.
�� Limbic system Limbic system highjackshighjacks the the neocortexneocortex::�� Executive functioning deficits.Executive functioning deficits.�� Poor attention and concentration.Poor attention and concentration.
�� Worldview shaped by early environment:Worldview shaped by early environment:�� Hostile attribution bias.Hostile attribution bias.�� Preoccupation with threat (i.e. Preoccupation with threat (i.e. hypervigilencehypervigilence).).
Hilary Hodgdon, Ph.D. – Complex Trauma in Children 45
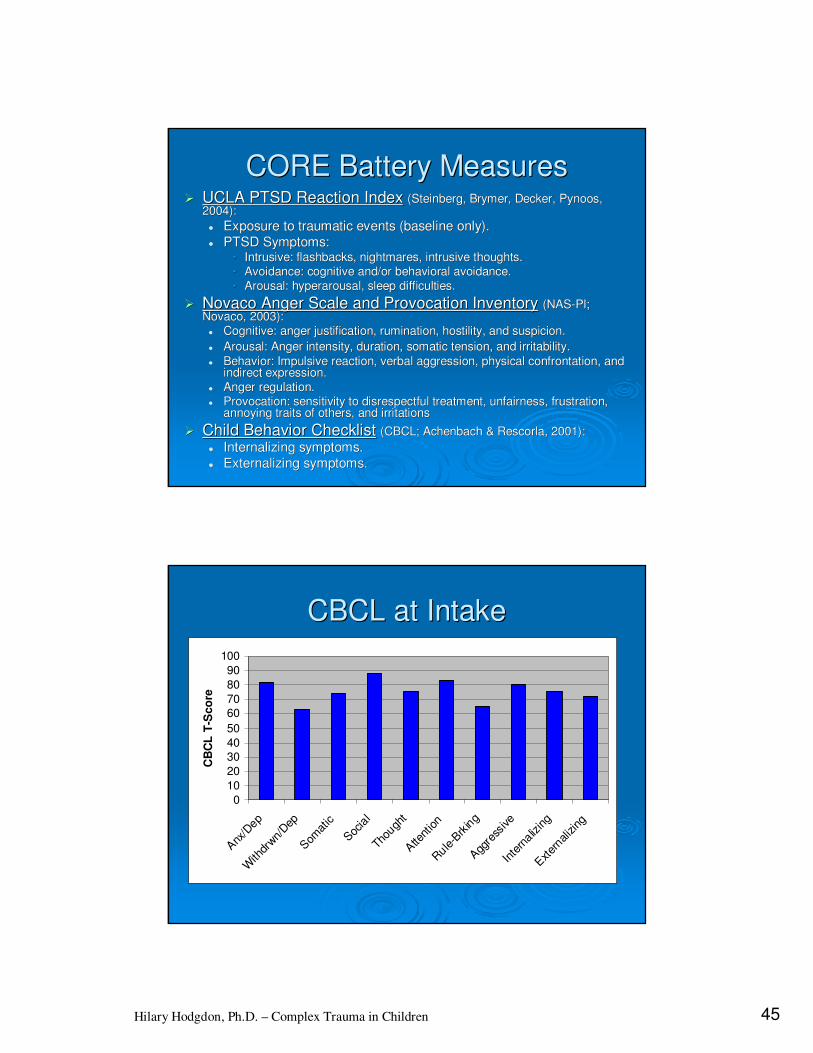
CORE Battery MeasuresCORE Battery Measures�� UCLA PTSD Reaction IndexUCLA PTSD Reaction Index (Steinberg, (Steinberg, BrymerBrymer, Decker, , Decker, PynoosPynoos, ,
2004):2004):
�� Exposure to traumatic events (baseline only).Exposure to traumatic events (baseline only).�� PTSD Symptoms:PTSD Symptoms:
•• Intrusive: flashbacks, nightmares, intrusive thoughts.Intrusive: flashbacks, nightmares, intrusive thoughts.
•• Avoidance: cognitive and/or behavioral avoidance.Avoidance: cognitive and/or behavioral avoidance.
•• Arousal: Arousal: hyperarousalhyperarousal, sleep difficulties., sleep difficulties.
�� NovacoNovaco Anger Scale and Provocation InventoryAnger Scale and Provocation Inventory (NAS(NAS--PI; PI; NovacoNovaco, 2003):, 2003):�� Cognitive: anger justification, rumination, hostility, and suspiCognitive: anger justification, rumination, hostility, and suspicion.cion.
�� Arousal: Anger intensity, duration, somatic tension, and irritabArousal: Anger intensity, duration, somatic tension, and irritability.ility.
�� Behavior: Impulsive reaction, verbal aggression, physical confroBehavior: Impulsive reaction, verbal aggression, physical confrontation, and ntation, and indirect expression. indirect expression.
�� Anger regulation.Anger regulation.�� Provocation: sensitivity to disrespectful treatment, unfairness,Provocation: sensitivity to disrespectful treatment, unfairness, frustration, frustration,
annoying traits of others, and irritations annoying traits of others, and irritations
�� Child Behavior ChecklistChild Behavior Checklist (CBCL; Achenbach & (CBCL; Achenbach & RescorlaRescorla, 2001):, 2001):
�� Internalizing symptoms.Internalizing symptoms.�� Externalizing symptoms.Externalizing symptoms.
CBCL at IntakeCBCL at Intake
0
10
20
30
40
50
60
70
80
90
100
Anx
/Dep
With
drwn/
Dep
Som
atic
Socia
l
Thou
ght
Atte
ntion
Rule
-Brk
ing
Agg
ress
ive
Inte
rnaliz
ing
Exter
naliz
ing
CB
CL
T-S
co
re
Hilary Hodgdon, Ph.D. – Complex Trauma in Children 46
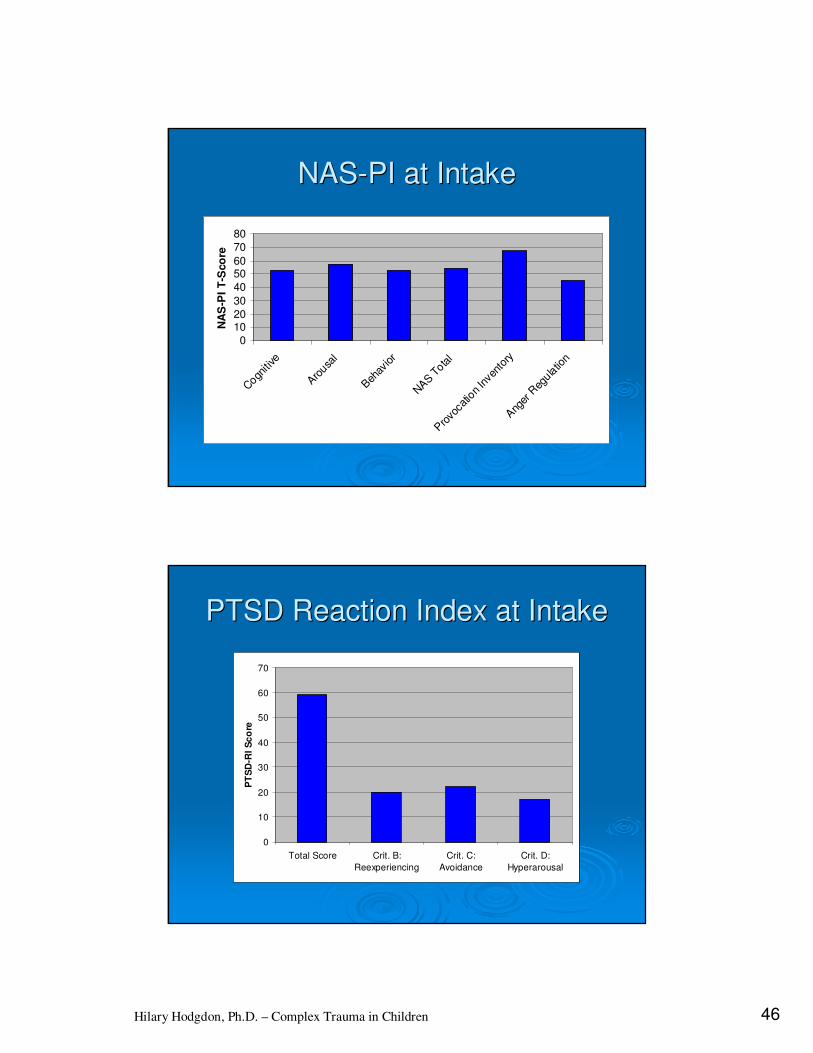
NASNAS--PI at IntakePI at Intake
0
1020
30
40
5060
70
80
Cogn
itive
Aro
usal
Beh
avior
NAS T
otal
Pro
voca
tion In
vent
ory
Ang
er R
egula
tion
NA
S-P
I T
-Sco
re
PTSD Reaction Index at IntakePTSD Reaction Index at Intake
0
10
20
30
40
50
60
70
Total Score Crit. B:
Reexperiencing
Crit. C:
Avoidance
Crit. D:
Hyperarousal
PT
SD
-RI
Sc
ore
Hilary Hodgdon, Ph.D. – Complex Trauma in Children 47
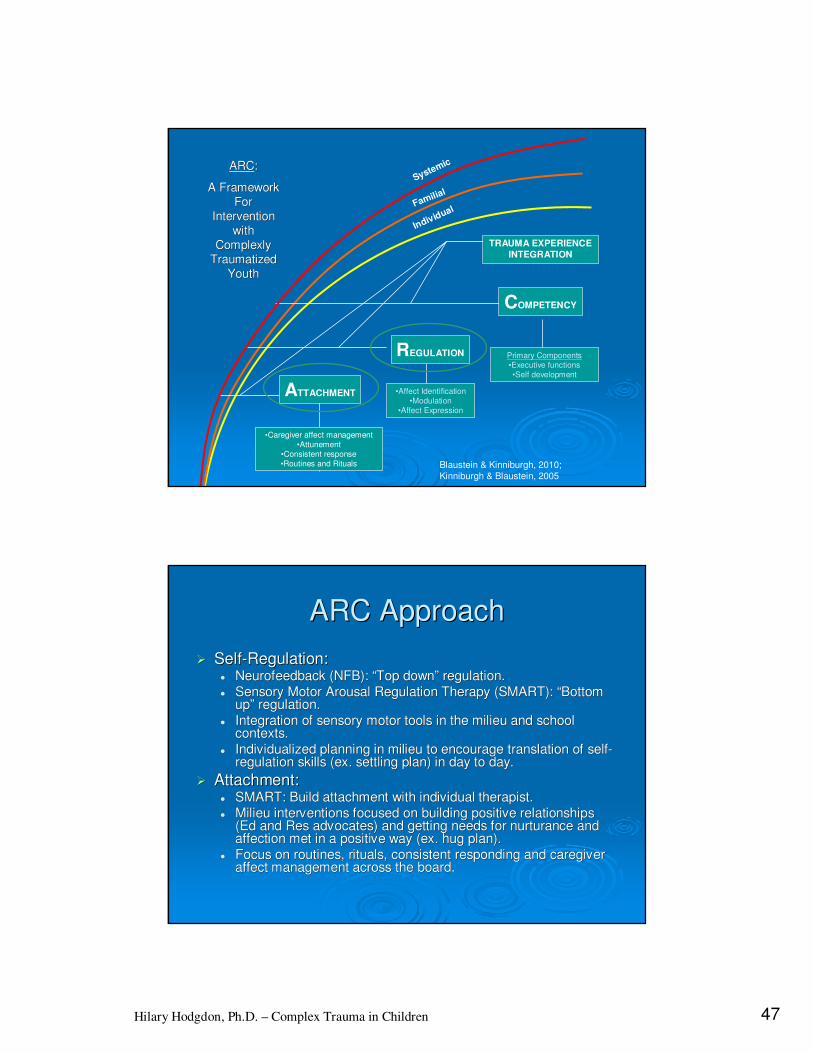
Systemic
Familial
Individual
ATTACHMENT
•Caregiver affect management
•Attunement
•Consistent response
•Routines and Rituals
REGULATION
•Affect Identification
•Modulation
•Affect Expression
COMPETENCY
Primary Components
•Executive functions
•Self development
ARCARC: :
A Framework A Framework
For For
Intervention Intervention
with with
Complexly Complexly
Traumatized Traumatized
YouthYouth
Blaustein & Kinniburgh, 2010;
Kinniburgh & Blaustein, 2005
TRAUMA EXPERIENCE
INTEGRATION
ARC ApproachARC Approach
�� SelfSelf--Regulation:Regulation:�� NeurofeedbackNeurofeedback (NFB): (NFB): ““Top downTop down”” regulation.regulation.�� Sensory Motor Arousal Regulation Therapy (SMART): Sensory Motor Arousal Regulation Therapy (SMART): ““Bottom Bottom
upup”” regulation.regulation.�� Integration of sensory motor tools in the milieu and school Integration of sensory motor tools in the milieu and school
contexts.contexts.�� Individualized planning in milieu to encourage translation of seIndividualized planning in milieu to encourage translation of selflf--
regulation skills (ex. settling plan) in day to day.regulation skills (ex. settling plan) in day to day.
�� Attachment:Attachment:�� SMART: Build attachment with individual therapist.SMART: Build attachment with individual therapist.�� Milieu interventions focused on building positive relationships Milieu interventions focused on building positive relationships
(Ed and Res advocates) and getting needs for nurturance and (Ed and Res advocates) and getting needs for nurturance and affection met in a positive way (ex. hug plan). affection met in a positive way (ex. hug plan).
�� Focus on routines, rituals, consistent responding and caregiver Focus on routines, rituals, consistent responding and caregiver affect management across the board.affect management across the board.
Hilary Hodgdon, Ph.D. – Complex Trauma in Children 48
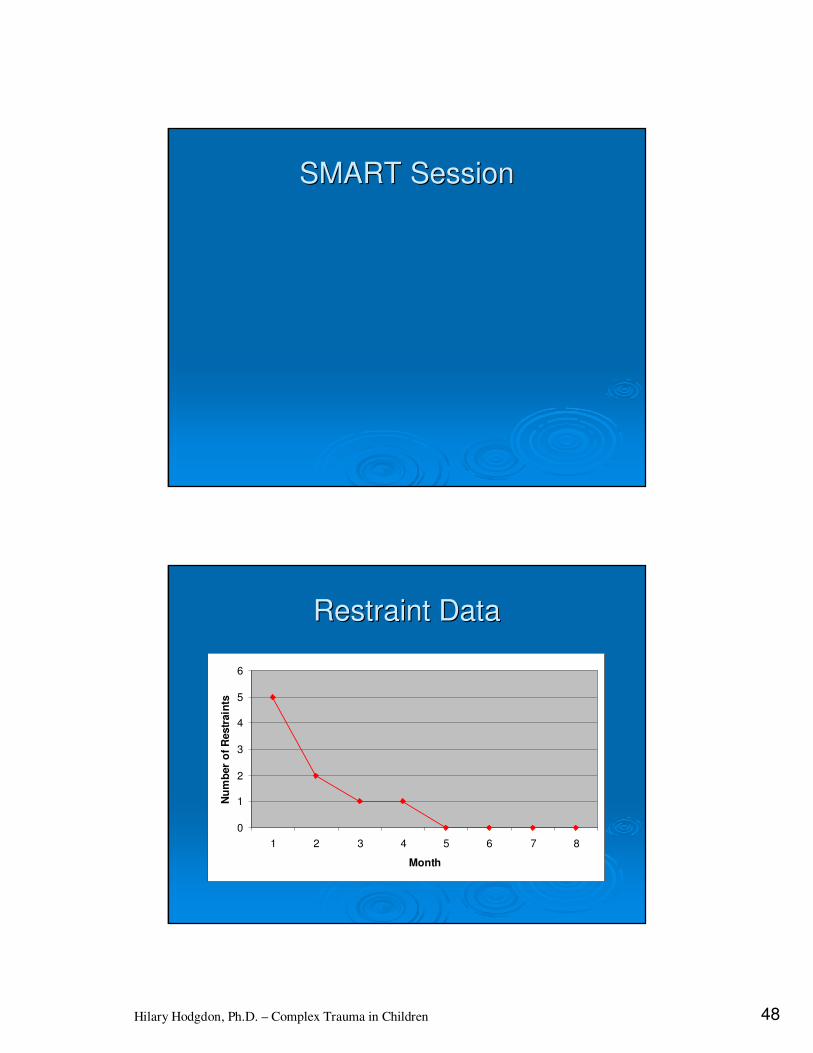
SMART SessionSMART Session
Restraint DataRestraint Data
0
1
2
3
4
5
6
1 2 3 4 5 6 7 8
Month
Nu
mb
er
of
Restr
ain
ts
Hilary Hodgdon, Ph.D. – Complex Trauma in Children 49
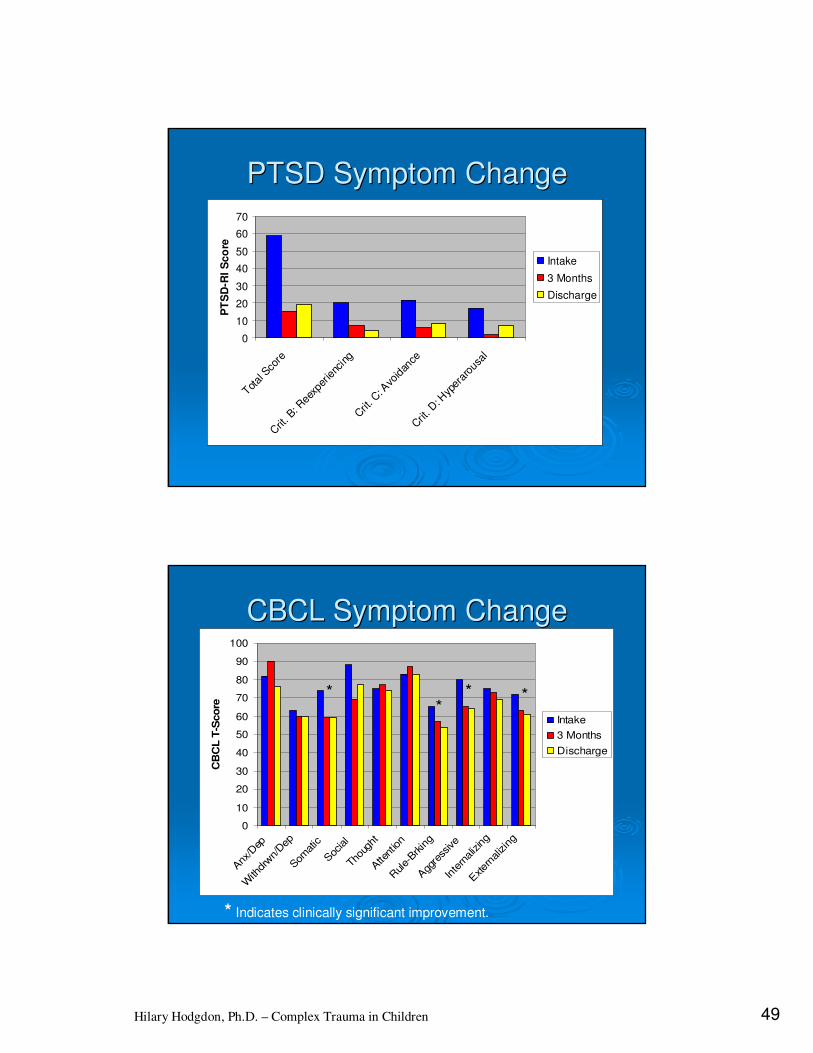
PTSD Symptom ChangePTSD Symptom Change
0
10
20
30
40
50
60
70
Total S
core
Crit
. B: R
eexp
erie
ncin
g
Crit
. C: A
void
ance
Crit
. D: H
yper
arou
sal
PT
SD
-RI
Sc
ore
Intake
3 Months
Discharge
CBCL Symptom ChangeCBCL Symptom Change
**
* *
0
10
20
30
40
50
60
70
80
90
100
Anx
/Dep
With
drwn/Dep
Som
atic
Soc
ial
Thoug
ht
Atte
ntion
Rule-
Brkin
g
Agg
ress
ive
Inte
rnalizing
Exter
naliz
ing
CB
CL
T-S
co
re
Intake
3 Months
Discharge
* Indicates clinically significant improvement.

Hilary Hodgdon, Ph.D. – Complex Trauma in Children 50
NASNAS--PI Symptom ChangePI Symptom Change
0
1020
30
40
5060
70
80
Cogn
itive
Aro
usal
Beh
avior
NAS T
otal
Pro
voca
tion In
vent
ory
Ang
er R
egula
tion
NA
S-P
I T
-Sco
re
Intake
3 Months
Discharge
Treatment SummaryTreatment Summary
�� Treatment approach was individualized and integrated Treatment approach was individualized and integrated across contexts.across contexts.
�� Initial focus on building selfInitial focus on building self--regulation skills through both regulation skills through both ““top downtop down”” and and ““bottom upbottom up”” approaches (SMART, NFB).approaches (SMART, NFB).
�� Attachments across the program and with family played Attachments across the program and with family played in integral role.in integral role.
�� Underlying capacity was revealed once extreme Underlying capacity was revealed once extreme dysregulationdysregulation had stabilized.had stabilized.
�� Significant clinical improvement in PTSD, somatic, and Significant clinical improvement in PTSD, somatic, and externalizing symptoms over 8 months.externalizing symptoms over 8 months.
�� Competency piece of ARC has continued beyond Competency piece of ARC has continued beyond residential treatment residential treatment –– such as returning to her parentsuch as returning to her parent’’s s home to live, getting her drivers license, etc.home to live, getting her drivers license, etc.
Top Related