






Languages
Pages
Legal


Disorders of FeetDisorders of Feet
Maria Carmela L. Domocmat, RN, MSN
Instructor
Northern Luzon Adventist College
Overview
• Part 1: Degenerative & Metabolic bone disorders:
• Part 2: Bone infections
3/5/2012Maria Carmela L. Domocmat, RN, MSN
2
• Part 2: Bone infections
• Part 3: Muscular disorders
• Part 4: Disorders of the hand
• Part 5: Spinal column deformities
• Part 6 : Disorders of feet
• Part 7: Sports Injuries

Disorders of Feet
• Hallux valgus (bunions)
• Morton’s neuroma (plantar neuroma)
• Hammer toe
3/5/2012Maria Carmela L. Domocmat, RN, MSN
3
• Hammer toe
• Tarsal tunnel syndrome
• Plantar Fasciitis
• Corn
• Callus
• Ingrown Nail
• Hypertrophic Ungual Labium
Disorders of Feet
• Hallux valgus (bunions), Morton’s neuroma(plantar neuroma), Hammer toe , Tarsal tunnel syndrome , Plantar Fasciitis, Corn, Callus,
3/5/2012Maria Carmela L. Domocmat, RN, MSN
4
syndrome , Plantar Fasciitis, Corn, Callus, Ingrown Nail, Hypertrophic Ungual Labium
3/5/2012Maria Carmela L. Domocmat, RN, MSN
5
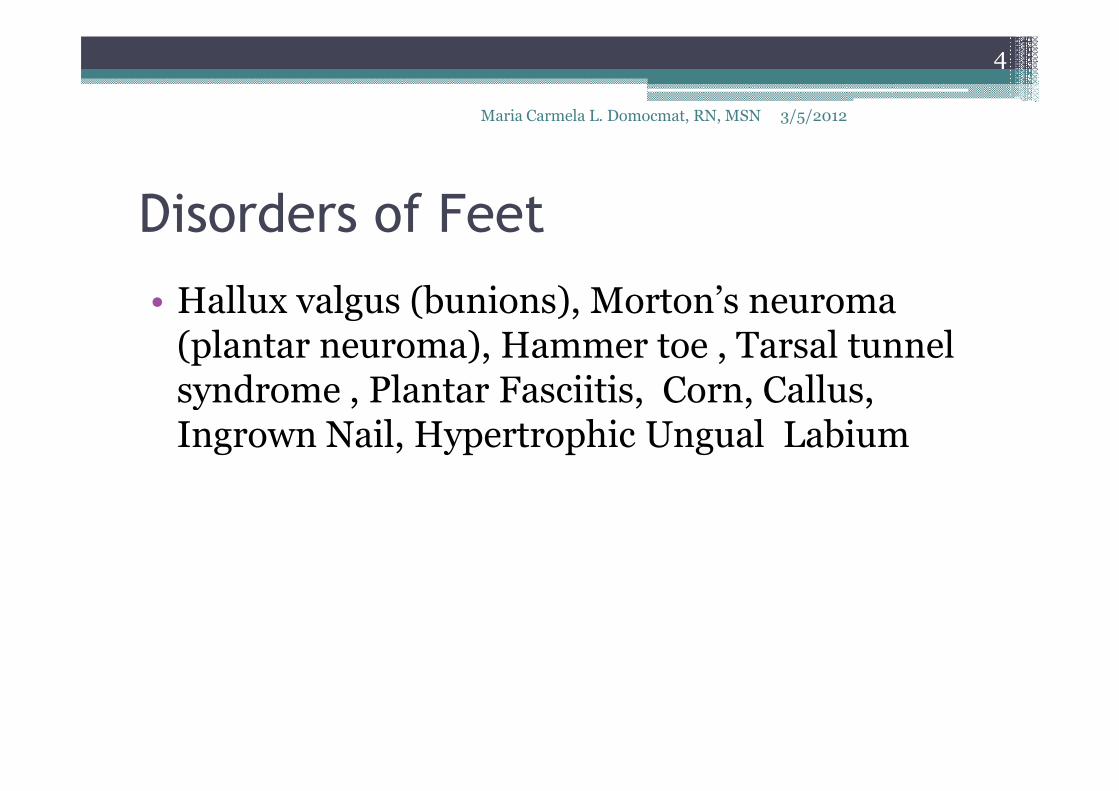
http://familyfootcarenj.com/web/images/layout/conditions_map.jpg
3/5/2012Maria Carmela L. Domocmat, RN, MSN
6
3/5/2012
7
Maria Carmela L. Domocmat, RN, MSN
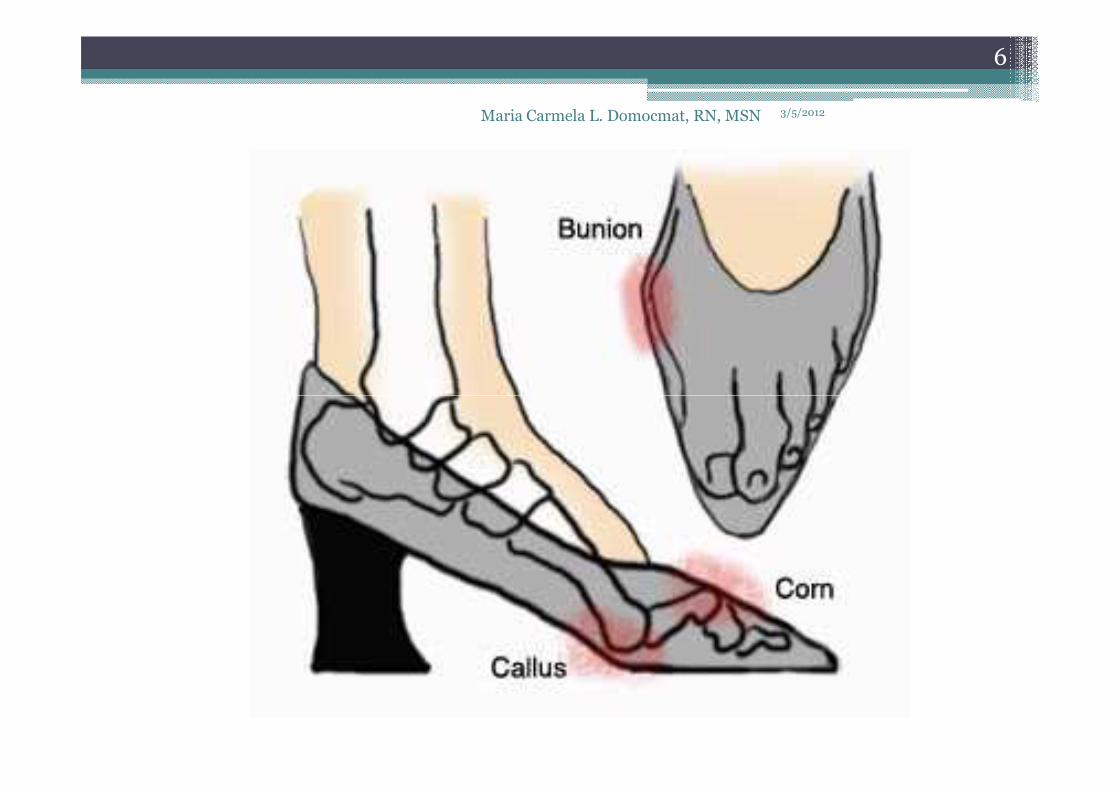
Hallux valgus
• is a condition that affects the joint at the base of the big toe.
• The condition is commonly called a bunion.
3/5/2012
8
Maria Carmela L. Domocmat, RN, MSN
• The condition is commonly called a bunion.
▫ bunion - refers to the bump that grows on the side of the first metatarsophalangeal (MTP) joint.

Hallux valgus (bunion)
• The deformity involves the big toe and the long bone behind the big toe, the 1st metatarsal.
• Over time, the 1st metatarsal will begin to move
3/5/2012
9
Maria Carmela L. Domocmat, RN, MSN
• Over time, the 1st metatarsal will begin to move towards the other foot (medial) while the big toe will move out of joint towards the 2nd toe (lateral).
http://www.footankleinstitute.com/hallux-valgus-bunion-surgery/

Hallux valgus (bunion)
• As the end of the 1st metatarsal bone begins to stick out, it will be under pressure from shoes and the ground.
3/5/2012
10
Maria Carmela L. Domocmat, RN, MSN
and the ground.
• this constant pressure and friction will cause extra bone formation, leading to the bump that is seen on the side of the foot.
http://www.footankleinstitute.com/hallux-valgus-bunion-surgery/

Hallux valgus (bunion)
• The big toe will continue to shift towards the second toe causing an unbalanced big toe joint. Over time arthritis can develop in the joint due
3/5/2012
11
Maria Carmela L. Domocmat, RN, MSN
Over time arthritis can develop in the joint due to the mal-positioned joint.
• A bunion deformity is always progressive. It will always get worse over time.
http://www.footankleinstitute.com/hallux-valgus-bunion-surgery/

3/5/2012
12
Maria Carmela L. Domocmat, RN, MSN

3/5/2012Maria Carmela L. Domocmat, RN, MSN
13
Hallux valgus (bunion)
• term hallux valgus actually describes what happens to the big toe.▫ Hallux - medical term for big toe
3/5/2012
14
Maria Carmela L. Domocmat, RN, MSN
▫ Hallux - medical term for big toe▫ Valgus - anatomic term that means the deformity
goes in a direction away from the midline of the body.
• hallux valgus - big toe begins to point towards the outside of the foot. ▫ As this condition worsens, other changes occur in
the foot that increase the problem.
Etiology
• Contrary to common belief,
▫ high-heeled shoes with a small toe box or tight-fitting shoes do not cause hallux valgus.
3/5/2012
15
Maria Carmela L. Domocmat, RN, MSN
fitting shoes do not cause hallux valgus.
▫ such footwear does keep the hallux in an abducted position if hallux valgus is present, causing mechanical stretch and deviation of the medial soft tissue.
▫ In addition, tight shoes can cause medial bump pain and nerve entrapment.

Etiology
• Biomechanical instability
• Arthritic/metabolic conditions
• Structural deformity
3/5/2012
16
Maria Carmela L. Domocmat, RN, MSN
• Structural deformity
• Neuromuscular disease
• Traumatic compromise

Etiology
• Biomechanical instability▫ most common yet most difficult to understand etiology ▫ Contributing factors, if present, include
� gastrocnemius or gastrocsoleus equinus,
3/5/2012
17
Maria Carmela L. Domocmat, RN, MSN
� gastrocnemius or gastrocsoleus equinus,
� flexible or rigid pes plano valgus,
� rigid or flexible forefoot varus,
� dorsiflexed first ray,
� hypermobility, or
� short first metatarsal.
� Most often, excessive pronation at the midtarsal and subtalar joints compensates for these factors throughout the gait cycle.
Etiology
• Biomechanical instability
▫ Some pronation must occur in gait to absorb ground-reactive forces. However, excessive
3/5/2012
18
Maria Carmela L. Domocmat, RN, MSN
ground-reactive forces. However, excessive pronation produces too much midfoot mobility, which decreases stability and prevents resupination and creation of a rigid lever arm; these effects make propulsion difficult.

Etiology
• Biomechanical instability▫ During normal propulsion
� approximately 65° of dorsiflexion is necessary at the first metatarsophalangeal joint,
� only 20-30° is available from hallux dorsiflexion.
3/5/2012
19
Maria Carmela L. Domocmat, RN, MSN
� only 20-30° is available from hallux dorsiflexion. � Therefore, the first metatarsal must plantarflex at the sesamoid
complex to gain the additional 40° of motion needed. � Failure to attain the full 65° because of jamming of the joint
during pronation subjects the first metatarsophalangeal to intense forces from which hallux valgus develops.
▫ If the foot is sufficiently hypermobile as a result of excessive pronation, the metatarsal tends to drift medially and the hallux drifts laterally, producing hallux valgus. If no hypermobility is present, hallux rigidus develops instead.

EtiologyArthritic/metabolic conditions
Structural deformity
▫ Gouty arthritis
▫ Rheumatoid arthritis
• Malalignment of articular surface or metatarsal shaft
• Abnormal metatarsal length
3/5/201220Maria Carmela L. Domocmat, RN, MSN
▫ Psoriatic arthritis
▫ Connective tissue disorders such as Ehlers-Danlossyndrome, Marfansyndrome, Down syndrome, and ligamentous laxity
• Abnormal metatarsal length
• Metatarsus primus elevatus
• External tibial torsion
• Genu varum or valgum
• Femoral retrotorsion
Etiology
Neuromuscular disease Traumatic compromise
• Multiple sclerosis
• Charcot-Marie-Tooth disease
• Malunions
• Intra-articular damage
3/5/201221
• Cerebral palsy • Soft-tissue sprains
• Dislocations
Symptoms
• Symptoms of Hallux valgus depending on the degree of severity:
▫ Aesthetic problem.
3/5/2012
22
Maria Carmela L. Domocmat, RN, MSN
▫ Aesthetic problem.
▫ Formation of calluses, chronic irritation of the skin and bursa.
▫ Increasing pain under load and when moving.
▫ Progressive arthrosis and stiffening in the base joint of the toe.
▫ Corollary deformities such as hammer and claw toe.
http://www.hallufix.org/english/hallux_valgus.html
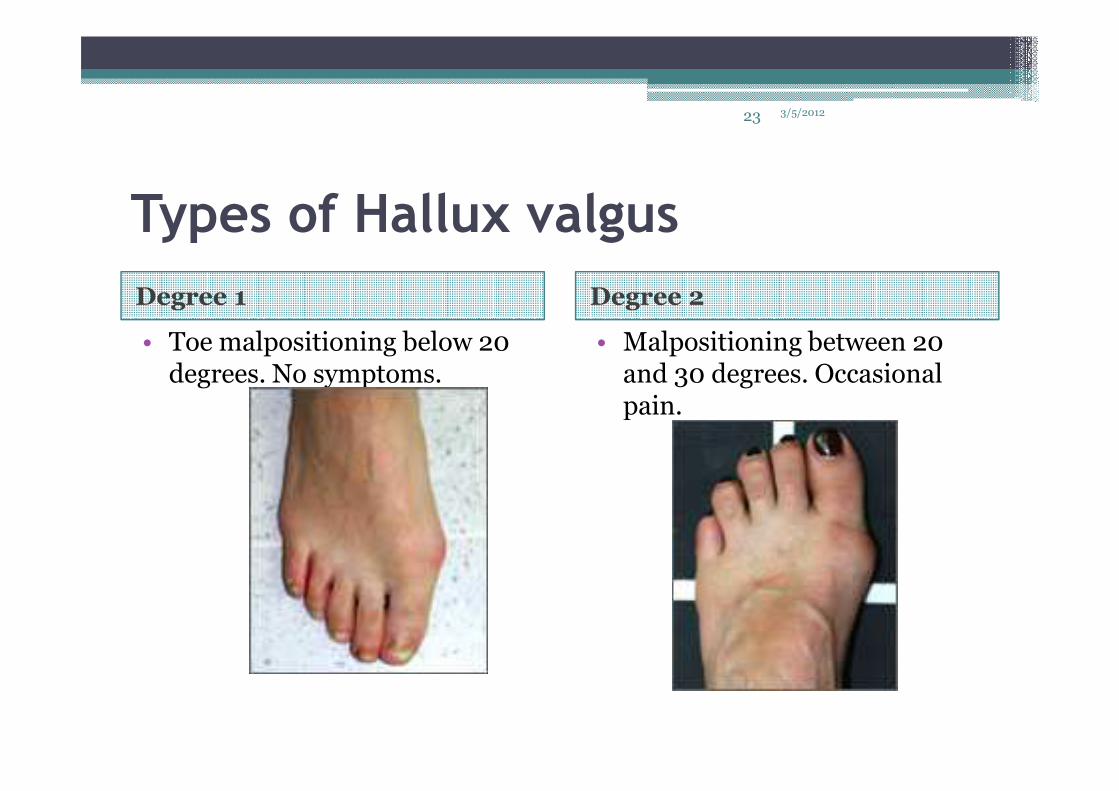
Types of Hallux valgus
Degree 1 Degree 2
• Toe malpositioning below 20 degrees. No symptoms.
• Malpositioning between 20 and 30 degrees. Occasional pain.
3/5/201223
pain.

Types of Hallux valgus
Degree 3 Degree 4
• Malpositioning between 30 and 50 degrees. Regular pain. Increasing restraints on
• Severest form with malpositionings over 50 degrees and painful restraints
3/5/2012Maria Carmela L. Domocmat, RN, MSN
Increasing restraints on activities. Pronounced malpositioning!
degrees and painful restraints on the activities of everyday life.Surgical treatment

Treatment
• Medical Therapy▫ Adapting footwear▫ Pharmacologic or physical therapy▫ Functional orthotic therapy
3/5/2012
25
Maria Carmela L. Domocmat, RN, MSN
▫ Functional orthotic therapy
• Surgical Therapy▫ Capsulotendon balancing or exostectomy▫ Osteotomy▫ Resectional arthroplasty▫ Resectional arthroplasty with implant▫ First metatarsophalangeal joint arthrodesis▫ First metatarsocuneiform joint arthrodesis

3/5/2012
26
Maria Carmela L. Domocmat, RN, MSN

3/5/2012Maria Carmela L. Domocmat, RN, MSN
27

Bunionectomy• remove the bump that makes up the bunion. • performed through a small incision on the side of the foot immediately over
the area of the bunion. • Once the skin is opened the bump is removed using a special surgical saw or
chisel.
3/5/2012
28
Maria Carmela L. Domocmat, RN, MSN
chisel. • The bone is smoothed of all rough edges and the skin incision is closed with
small stitches.• It is more likely that realignment of the big toe will also be necessary. The
major decision that must be made is whether or not the metatarsal bone will need to be cut and realigned as well. The angle made between the first metatarsal and the second metatarsal is used to make this decision. The normal angle is around nine or ten degrees. If the angle is 13 degrees or more, the metatarsal will probably need to be cut and realigned.
• When a surgeon cuts and repositions a bone, it is referred to as an osteotomy. There are two basic techniques used to perform an osteotomy to realign the first metatarsal.
http://www.concordortho.com/patient-education/topic-detail-popup.aspx?topicID=a5cea3a8a6d8093483657c959125dbaf
Distal Osteotomy
• the far end of the bone is cut and moved laterally • This effectively reduces the angle between the first
and second metatarsal bones. • usually requires one or two small incisions in the
3/5/2012
29
Maria Carmela L. Domocmat, RN, MSN
• usually requires one or two small incisions in the foot.
• Once the surgeon is satisfied with the position of the bones, the osteotomy is held in the desired position with one, or several,metal pins.
• Once the bone heals, the pin is removed. The metal pins are usually removed between three and six weeks following surgery.
http://www.concordortho.com/patient-education/topic-detail-popup.aspx?topicID=a5cea3a8a6d8093483657c959125dbaf

Proximal Osteotomy• the first metatarsal is cut at the near end of the bone • usually requires two or three small incisions in the foot. • Once the skin is opened the surgeon performs the osteotomy. The bone is
then realigned and held in place with metal pins until it heals. Again, this reduces the angle between the first and second metatarsal bones.
3/5/2012
30
Maria Carmela L. Domocmat, RN, MSN
reduces the angle between the first and second metatarsal bones.• Realignment of the big toe is then done by releasing the tight structures on
the lateral, or outer, side of the first MTP joint. This includes the tight joint capsule and the tendon of the adductor hallucis muscle. This muscle tends to pull the big toe inward. By releasing the tendon, the toe is no longer pulled out of alignment. The toe is realigned and the joint capsule on the side of the big toe closest to the other toe is tightened to keep the toe straight, or balanced.
• Once the surgeon is satisfied that the toe is straight and well balanced, the skin incisions are closed with small stitches. A bulky bandage is applied to the foot before you are returned to the recovery room.
http://www.concordortho.com/patient-education/topic-detail-popup.aspx?topicID=a5cea3a8a6d8093483657c959125dbaf

Good footwear is often all that is needed• Wearing good footwear does not cure the deformity but may
ease symptoms of pain and discomfort. Ideally, get advice about footwear from a podiatrist or chiropodist.
Advice may include:
3/5/2012
31
Maria Carmela L. Domocmat, RN, MSN
Advice may include:• Wear shoes, trainers or slippers that fit well and are roomy.• Don't wear high-heeled, pointed or tight shoes.• You might find that shoes with laces or straps are best, as they
can be adjusted to the width of your foot.• Padding over the bunion may help, as may ice packs.• Devices which help to straighten the toe (orthoses) are still
occasionally recommended, although trials investigating their use have not found them much better than no treatment at all.
http://www.patient.co.uk/health/Bunions-(Hallux-Valgus).htm

How to Choose Shoes
1. Know your foot. Take a look at your old shoes. Look at what areas the most worn out shoes. A well-chosen shoes will help to endure the physical stress well. One way to
3/5/2012
32
Maria Carmela L. Domocmat, RN, MSN
to endure the physical stress well. One way to determine your foot's shape is to do a "wet test"---wet your foot, step on a piece of brown paper and trace your footprint. Or just look at where your last pair of shoes shows the most wear.
2. Don't buy uncomfortable shoes even if they are hot!3. Ideally, you should avoid wearing heels4. Don't make shoes multitask.
http://hallux-valgus-rigidus.com/index.php?option=com_content&view=article&id=74&Itemid=88

3/5/2012
33
Maria Carmela L. Domocmat, RN, MSN

How to Choose Shoes
5. Knowing your foot's particular quirks is key to selecting the right pair of shoes.
6. You must find shoes with well cushioned soles and ideally, some type of soft arch-support.
3/5/2012
34
Maria Carmela L. Domocmat, RN, MSN
ideally, some type of soft arch-support.7. 7. Measure your foot frequently. Foot size changes
as we get older.8. 8. You should not buy shoes in the morning. The
size of our feet at night more than in the morning. Feet swell over the course of the day; they also expand while you run or walk, so shoes should fit your feet when they're at their largest.
http://hallux-valgus-rigidus.com/index.php?option=com_content&view=article&id=74&Itemid=88

3/5/2012Maria Carmela L. Domocmat, RN, MSN
35
How to Choose Shoes
9. Always buy shoes to fit the larger or wider foot.Buy well-fitting shoes with a wide toe box.
10. Use bunion shields, bunion pads or bunion cushions to protect the bunion when wearing shoes. A bunion sleeve can be especially effective at relieving shoe pressure when walking
3/5/2012
36
Maria Carmela L. Domocmat, RN, MSN
protect the bunion when wearing shoes. A bunion sleeve can be especially effective at relieving shoe pressure when walking with a hallux valgus.
11. Utilize an orthotic device or insert, such as a bunion splint or bunion brace, to redistribute the pressure along the arch and ball of the foot and control the separation of the bones. These devices help support your foot and reduce the tendency toward hallux valgus formation.
12. Use a bunion regulator to stretch tight tendons and toe muscles overnight – especially if you want to avoid surgery.
http://hallux-valgus-rigidus.com/index.php?option=com_content&view=article&id=74&Itemid=88

3/5/2012Maria Carmela L. Domocmat, RN, MSN
37

Resectional arthroplasty
• is a joint-destructive procedure
• most commonly reserved for elderly patients with advanced degenerative joint disease and
3/5/2012
38
Maria Carmela L. Domocmat, RN, MSN
with advanced degenerative joint disease and significant limitation of motion.
• The typical resectional arthroplasty that is performed is known as a Keller procedure.
http://emedicine.medscape.com/article/1232902-treatment#showall

Resectional arthroplasty
• performed when morbidity might be increased with the more aggressive osteotomy that would otherwise be selected.
• The procedure includes resection of the base of the
3/5/2012
39
Maria Carmela L. Domocmat, RN, MSN
• The procedure includes resection of the base of the proximal phalanx with reapproximation of the abductor and adductor tendon groups.
• The technique is inherently unstable and should be used judiciously.
• The postoperative course includes limited-to-full weight bearing in a surgical shoe immediately after the procedure.
http://emedicine.medscape.com/article/1232902-treatment#showall

Resectional arthroplasty with implant • is the same procedure as the resectional
arthroplasty, with similar indications, but stability is markedly improved with the addition
3/5/2012
40
Maria Carmela L. Domocmat, RN, MSN
stability is markedly improved with the addition of the total implant.
http://emedicine.medscape.com/article/1232902-treatment#showall
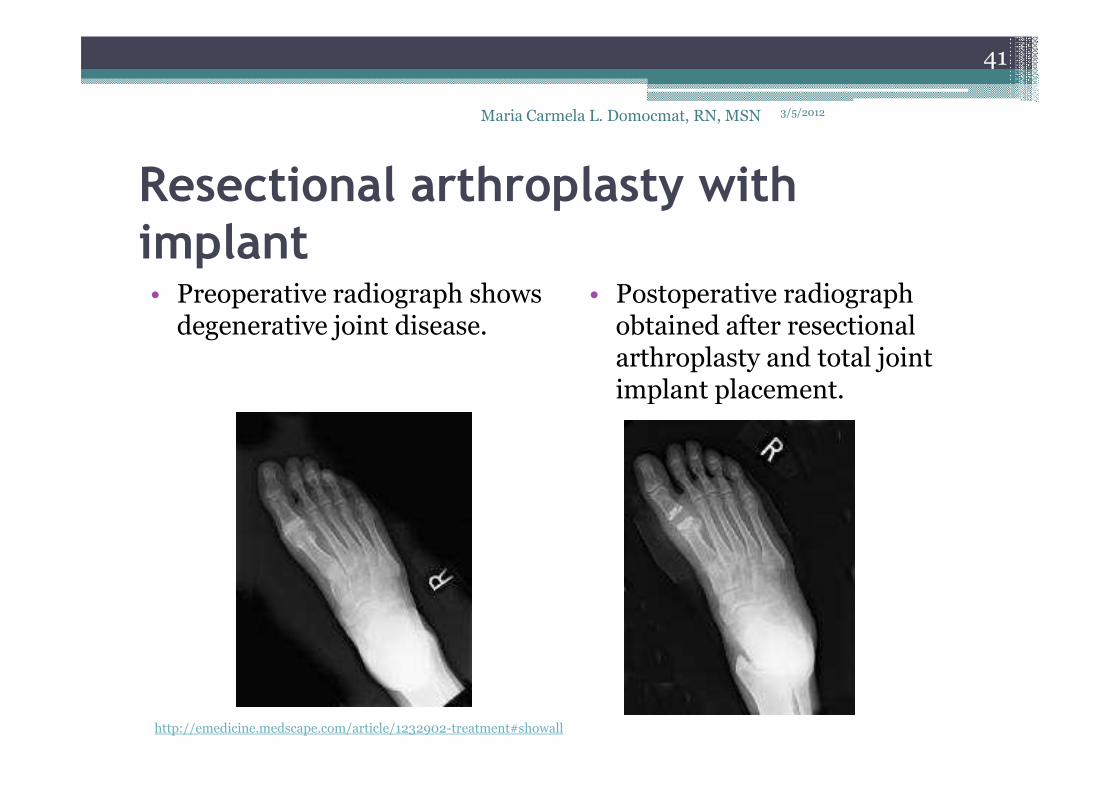
Resectional arthroplasty with implant • Preoperative radiograph shows
degenerative joint disease.• Postoperative radiograph
obtained after resectionalarthroplasty and total joint implant placement.
3/5/2012Maria Carmela L. Domocmat, RN, MSN
41
implant placement.
http://emedicine.medscape.com/article/1232902-treatment#showall
First metatarsophalangeal joint arthrodesis• is a joint-destructive procedure that offers a
higher degree of stability and functionality.
• considered the definitive procedure for
3/5/2012
42
Maria Carmela L. Domocmat, RN, MSN
• considered the definitive procedure for degenerative joint disease.
• results in complete loss of motion at the first metatarsophalangeal joint and is reserved for patients with high activity levels and functional demands.

First metatarsophalangeal joint arthrodesis• Preoperative radiograph shows
arthrodesis.• Postoperative radiograph show
arthrodesis.
3/5/2012Maria Carmela L. Domocmat, RN, MSN
43

First metatarsocuneiform joint arthrodesis• Significant and/or hypermobile hallux
abductovalgus may be reduced with arthrodesisof the first metatarsocuneiform joint (see images
3/5/2012
44
Maria Carmela L. Domocmat, RN, MSN
of the first metatarsocuneiform joint (see images below).
• Indications include metatarsus primus varus, hypermobility of the first ray, metatarsalgia of the lesser metatarsals, and degenerative joint disease of the metatarsocuneiform joint.

First metatarsocuneiform joint arthrodesis• Preoperative radiograph shows
a hypermobile first ray.• Postoperative radiograph
shows arthrodesis of the first metatarsocuneiform.
3/5/2012Maria Carmela L. Domocmat, RN, MSN
45

3/5/2012
46
Maria Carmela L. Domocmat, RN, MSN
Marfan syndrome (MFS)
• is a spectrum disorder caused by a heritable genetic defect of connective tissue that has an autosomal dominant mode of transmission
3/5/2012
47
Maria Carmela L. Domocmat, RN, MSN
autosomal dominant mode of transmission• The defect itself has been isolated to
the FBN1 gene on chromosome 15, which codes for the connective tissue protein fibrillin.
• Abnormalities in this protein cause a myriad of distinct clinical problems, of which the musculoskeletal, cardiac, and ocular system problems predominate.

Marfan syndrome (MFS)
• The skeleton of patients with MFS typically displays multiple deformities including arachnodactyly (ie, abnormally long and thin
3/5/2012
48
Maria Carmela L. Domocmat, RN, MSN
arachnodactyly (ie, abnormally long and thin digits), dolichostenomelia (ie, long limbs relative to trunk length), pectus deformities (ie, pectusexcavatum and pectus carinatum), and thoracolumbar scoliosis
Marfan syndrome (MFS)
• In the cardiovascular system, aortic dilatation, aortic regurgitation, and aneurysmsare the most worrisome clinical findings. Mitral
3/5/2012
49
Maria Carmela L. Domocmat, RN, MSN
are the most worrisome clinical findings. Mitral valve prolapse that requires valve replacement can occur as well. Ocular findings include myopia,cataracts, retinal detachment and superior dislocation of the lens
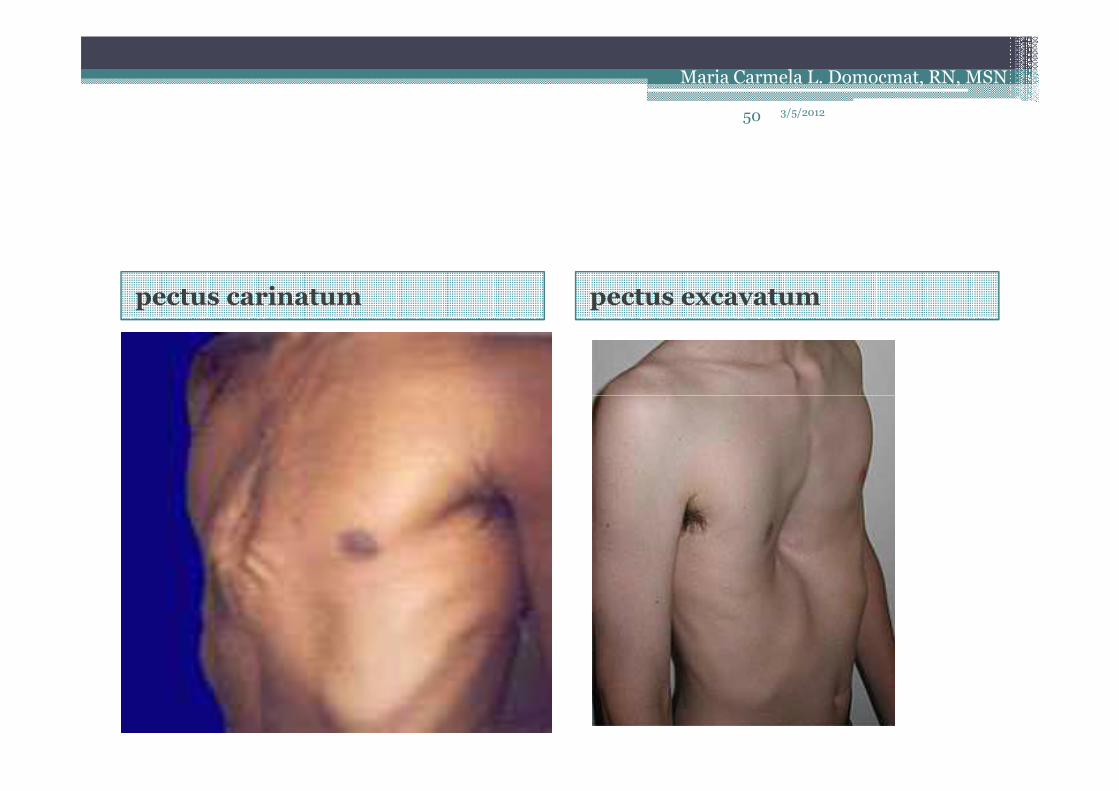
pectus carinatum pectus excavatum
3/5/201250
Maria Carmela L. Domocmat, RN, MSN
Genetics of Ehlers-Danlos Syndrome
• Ehlers-Danlos family of disorders is a group of related conditions that share a common decrease in the tensile strength and integrity of the skin,
3/5/2012
51
Maria Carmela L. Domocmat, RN, MSN
in the tensile strength and integrity of the skin, joints, and other connective tissues.
Genetics of Ehlers-Danlos Syndrome
• The first detailed clinical description of the syndrome is attributed to Tschernogobow in 1892.
• The syndrome derives its name from reports by
3/5/2012
52
Maria Carmela L. Domocmat, RN, MSN
• The syndrome derives its name from reports by Edward Ehlers, a Danish dermatologist, in 1901 and by Henri-Alexandre Danlos, a French physician with expertise in chemistry of skin disorders, in 1908.
• These 2 physicians combined the pertinent features of the condition and accurately delineated the phenotype of this group of disorders.

Ehlers-Danlos syndrome
• The amazing, almost unnatural, contortions that some patients with Ehlers-Danlos syndrome can perform often arouse curiosity.
3/5/2012
53
Maria Carmela L. Domocmat, RN, MSN
perform often arouse curiosity.
• Historically, some patients with Ehlers-Danlossyndrome displayed the maneuvers publically in circuses, shows, and performance tours.

Ehlers-Danlos syndrome
• Some achieved modest degrees of fame and bore titles such as "The India Rubber Man," "The Elastic Lady," and "The Human Pretzel."
3/5/2012
54
Maria Carmela L. Domocmat, RN, MSN
Elastic Lady," and "The Human Pretzel."
• Such clinical features also raise suspicion of the diagnosis when identified upon physical examination.
• Unfortunately, patients often go many years before being diagnosed
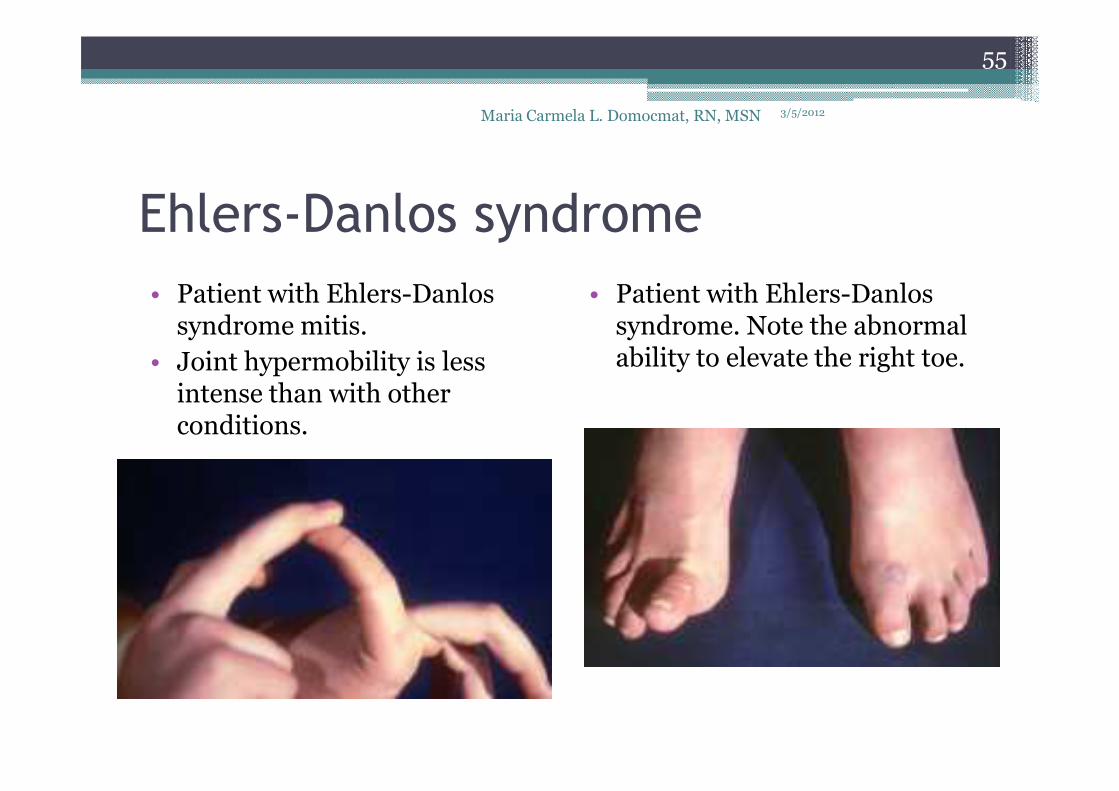
Ehlers-Danlos syndrome
• Patient with Ehlers-Danlossyndrome mitis.
• Joint hypermobility is less intense than with other
3/5/2012Maria Carmela L. Domocmat, RN, MSN
55
• Patient with Ehlers-Danlossyndrome. Note the abnormal ability to elevate the right toe.
intense than with other conditions.
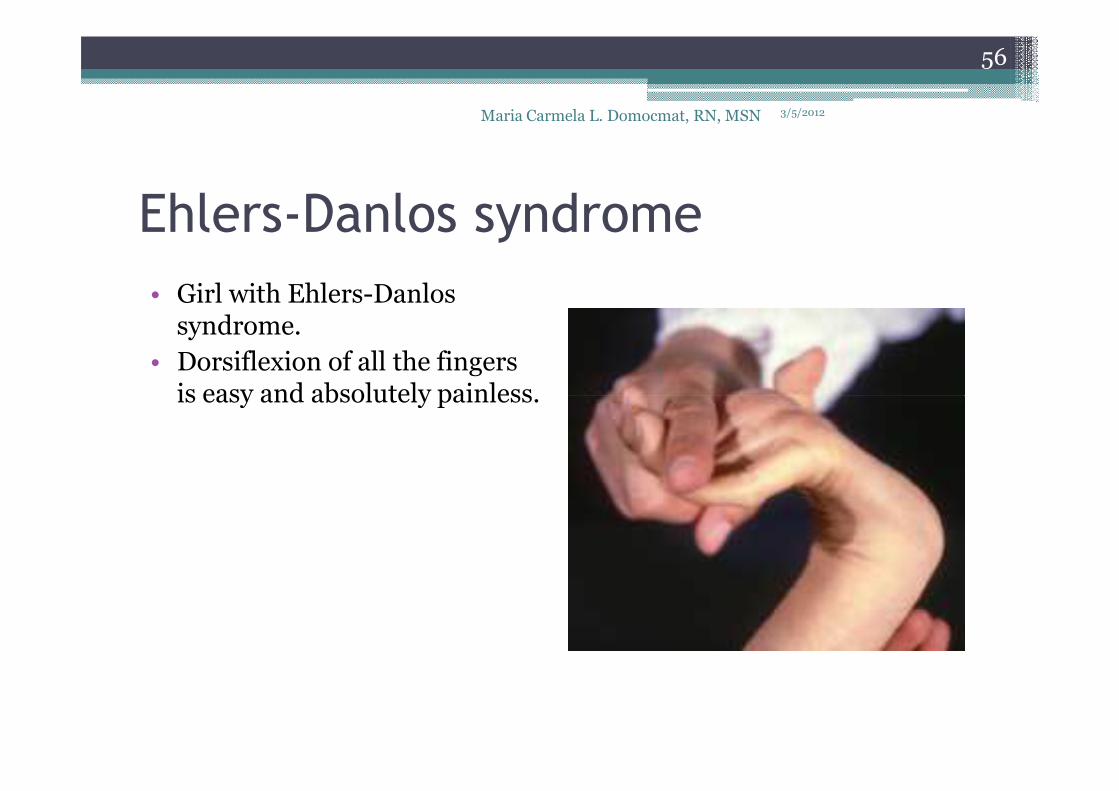
Ehlers-Danlos syndrome
• Girl with Ehlers-Danlossyndrome.
• Dorsiflexion of all the fingers is easy and absolutely painless.
3/5/2012Maria Carmela L. Domocmat, RN, MSN
56
is easy and absolutely painless.

• All forms of Ehlers-Danlos syndrome share the following primary features to varying degrees:
▫ Skin hyperextensibility
3/5/2012
57
Maria Carmela L. Domocmat, RN, MSN
▫ Skin hyperextensibility
▫ Joint hypermobility and excessive dislocations
▫ Tissue fragility
▫ Poor wound healing, leading to wide thin scars: The classic description of abnormal scar formation in Ehlers-Danlos syndrome is "cigarette paper scars."
▫ Easy bruising
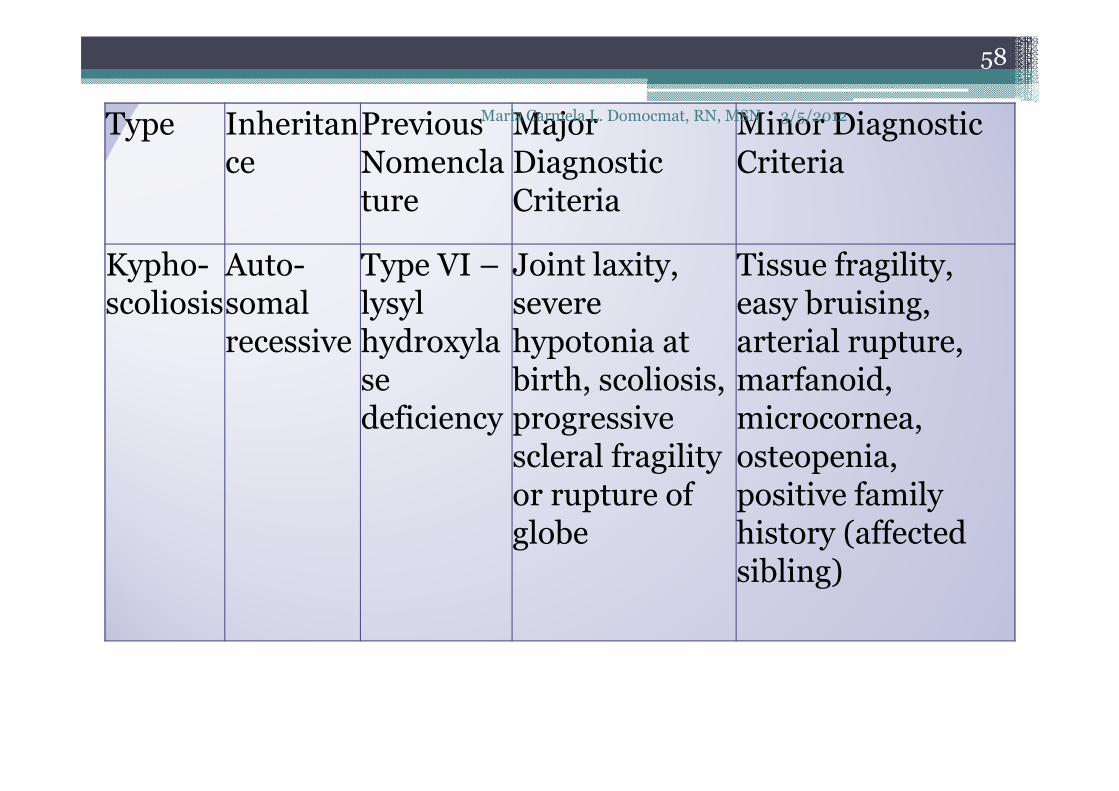
Type Inheritance
Previous Nomenclature
Major Diagnostic Criteria
Minor Diagnostic Criteria
Kypho-scoliosis
Auto-somalrecessive
Type VI –lysylhydroxylase
Joint laxity, severe hypotonia at birth, scoliosis,
Tissue fragility,easy bruising, arterial rupture,marfanoid,
3/5/2012
58
Maria Carmela L. Domocmat, RN, MSN
sedeficiency
birth, scoliosis, progressive scleral fragility or rupture of globe
marfanoid,microcornea,osteopenia,positive familyhistory (affected sibling)
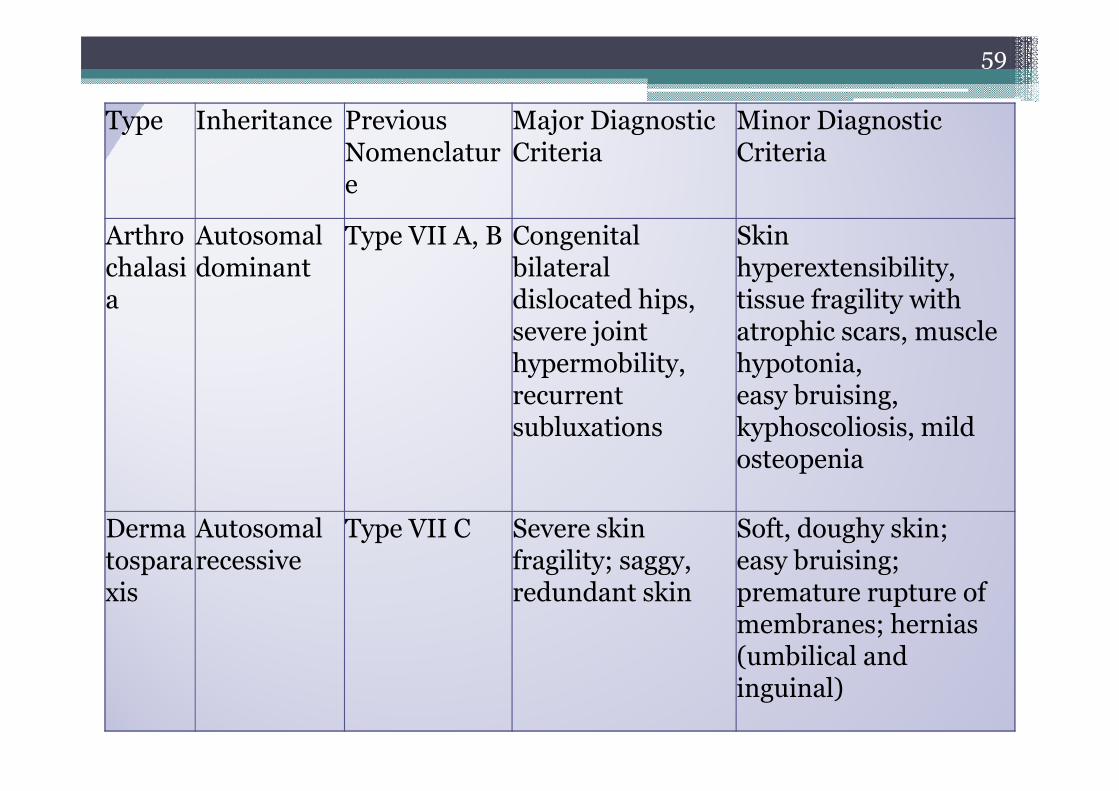
Type Inheritance Previous Nomenclature
Major Diagnostic Criteria
Minor Diagnostic Criteria
Arthrochalasia
Autosomal dominant
Type VII A, B Congenital bilateral dislocated hips,severe joint hypermobility,recurrent
Skin hyperextensibility,tissue fragility with atrophic scars, muscle hypotonia,easy bruising,
59
recurrent subluxations
easy bruising,kyphoscoliosis, mild osteopenia
Dermatosparaxis
Autosomal recessive
Type VII C Severe skin fragility; saggy, redundant skin
Soft, doughy skin;easy bruising; premature rupture of membranes; hernias (umbilical and inguinal)
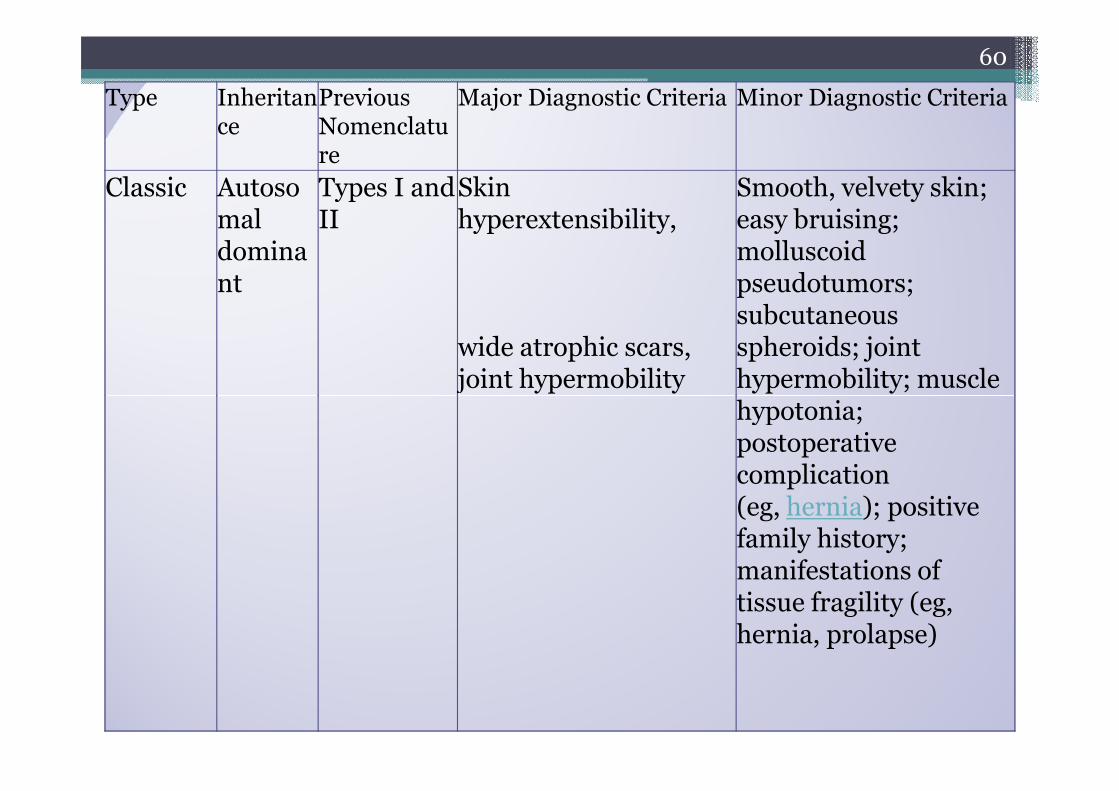
Type Inheritance
Previous Nomenclature
Major Diagnostic Criteria Minor Diagnostic Criteria
Classic Autosomal dominant
Types I and II
Skin hyperextensibility,
wide atrophic scars, joint hypermobility
Smooth, velvety skin; easy bruising; molluscoidpseudotumors; subcutaneous spheroids; joint hypermobility; muscle hypotonia;
60
hypotonia; postoperative complication (eg, hernia); positive family history; manifestations of tissue fragility (eg, hernia, prolapse)

Type Inheritance
Previous Nomenclature
Major Diagnostic Criteria
Minor Diagnostic Criteria
Hypermobility
Autosomaldominant
Type III Skin involvement (soft, smooth and velvety), joint hypermobility
Recurrent joint dislocation; chronic joint pain, limb pain, or both; positive family history
Vascular Autosomal
Type IV Thin, translucent skin; arterial/intestinal
Acrogeria,hypermobile small
61
mal dominant
arterial/intestinal fragility or rupture; extensive bruising; characteristic facial appearance
hypermobile small joints; tendon/muscle rupture; clubfoot; early onset varicose veins; arteriovenous, carotid-cavernous sinus fistula;pneumothorax;gingival recession; positive family history; sudden death in close relative

Down syndrome
• Down syndrome is by far the most common and best known chromosomal disorder in humans and the most common cause of
3/5/2012
62
Maria Carmela L. Domocmat, RN, MSN
humans and the most common cause of intellectual disability.
• Mental retardation, dysmorphic facial features, and other distinctive phenotypic traits characterize the syndrome

3/5/2012Maria Carmela L. Domocmat, RN, MSN
63

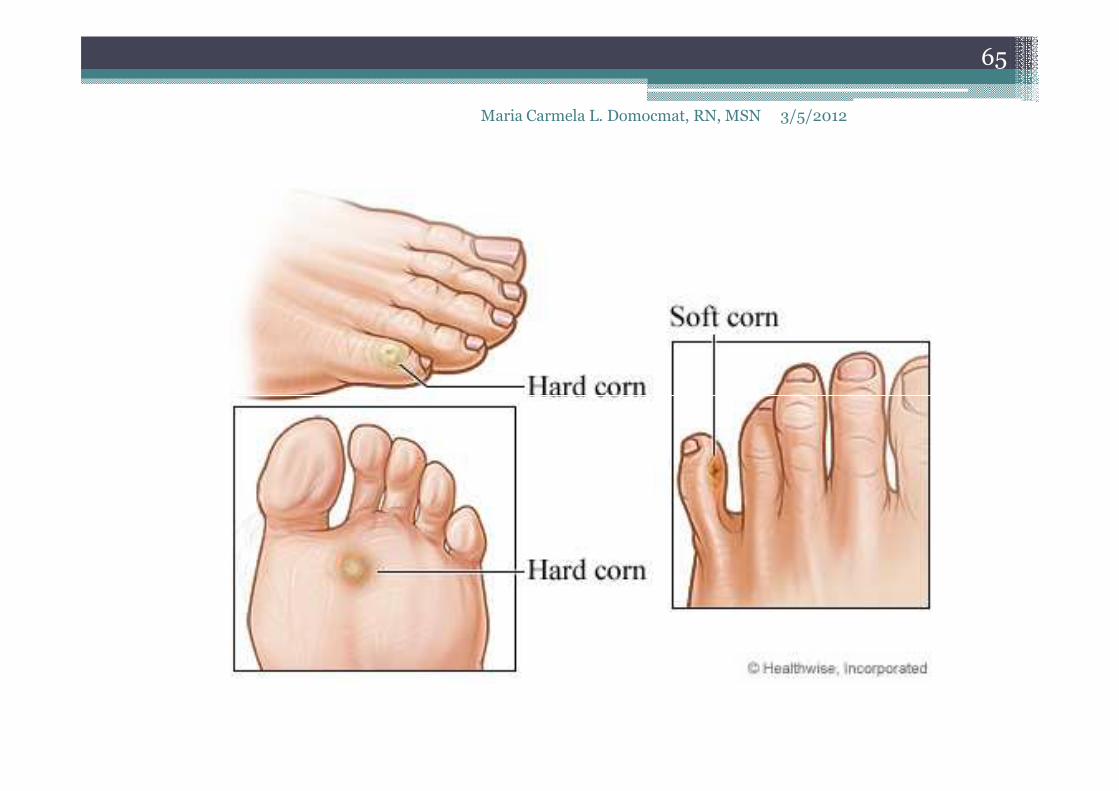
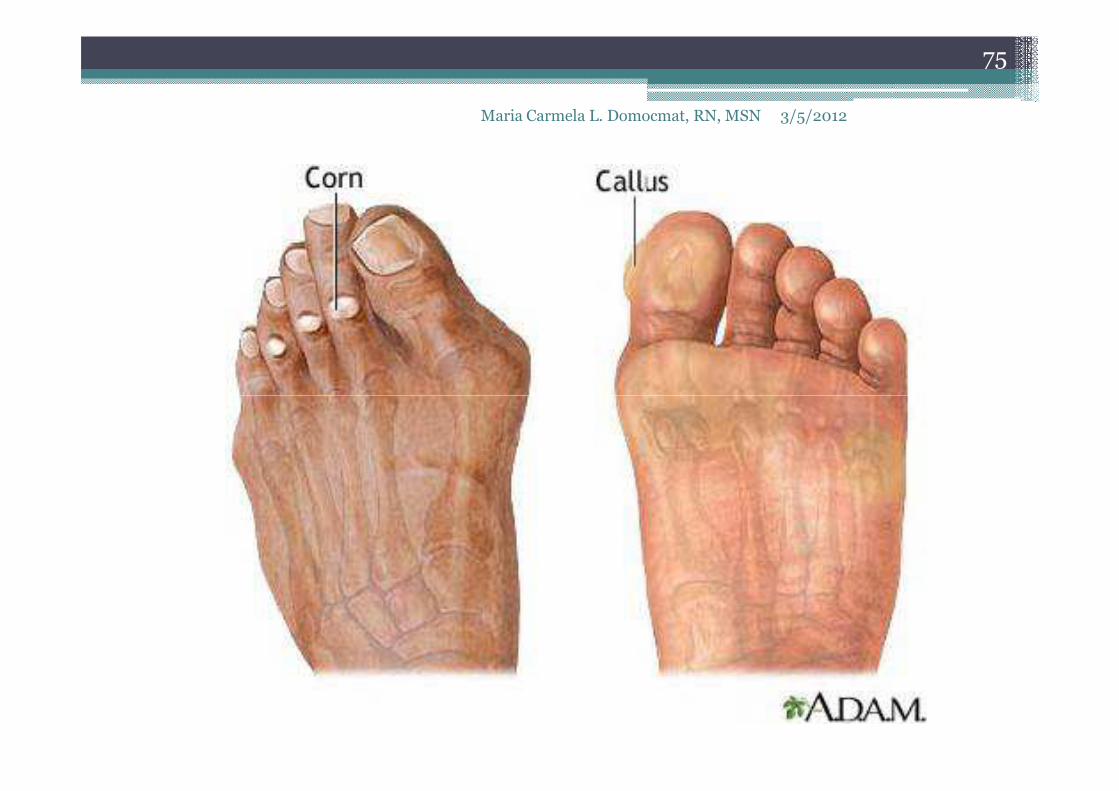
Corn
• induration and thickening of skin
caused by friction and pressure,
painful conical mass
3/5/2012Maria Carmela L. Domocmat, RN, MSN
64
painful conical mass
• appear as a horny thickening of the
skin on the toes.
• this thickening appears as a cone
shaped mass pointing down into
the skin.
3/5/2012Maria Carmela L. Domocmat, RN, MSN
65
Types of Corn
oHard corns� most common
� are concentrated areas of dry, hardened skin
3/5/2012Maria Carmela L. Domocmat, RN, MSN
66
� are concentrated areas of dry, hardened skin
about the size of a pea
� usually located on the outer surface of the little
toe or on the upper surface of the other toes,
but can occur between the toes
� may develop within a broader area of callused
skin
� sometimes called digital corns
Types of Corn
o Soft corns� are white and rubbery� can be extremely painful and tend to develop
between toes
3/5/2012Maria Carmela L. Domocmat, RN, MSN
67
between toes� are like hard corns that have been softened by
continual exposure to moisture, usually because you don’t dry between toes properly or from sweat.
� may form opposite one another and are known as ‘kissing lesions’.
� Sometimes, soft corns can become infected by bacteria or fungi.
Other, rarer types of corn include:
• seed corns ▫ may appear as one corn or as clusters of small
corns on the bottom foot; they are usually painless
3/5/2012Maria Carmela L. Domocmat, RN, MSN
68
painless
• vascular corns ▫ occur in blood vessels and bleed if cut
• fibrous corns ▫ are corns that have been around for a long time
and have become attached to the deeper layers of your skin, sometimes causing pain

Causes of corns
oCorns are caused by constant pressure on a
bony area of foot. This can happen for a
number of different reasons. These include:
3/5/2012Maria Carmela L. Domocmat, RN, MSN
69
number of different reasons. These include:
� poorly fitting footwear – for example, shoes that
are too small, cramp toes or have uneven soles;
this is the most common cause of corns
� being very active – doing lots of exercise can put
pressure on feet
� prominent bones – these can press against shoes

Causes of corns
oCorns are caused by constant pressure on a
bony area of foot. This can happen for a
number of different reasons. These include:
3/5/2012Maria Carmela L. Domocmat, RN, MSN
70
number of different reasons. These include:
� a misshapen foot because foot or toes have
developed unusually –may have a toe that is
overly curved or a particular bone that is too short
� poorly healed fractures – if have broken a toe or
another bone in foot, it may have set out of place
causing foot to press against shoe

Corn
• Treatment:
• surgical removal by podiatrist
3/5/2012Maria Carmela L. Domocmat, RN, MSN
71
Prevention of corns
owearing sensible, low-heeled footwear
(maximum 4cm heel) with a rounded toe
not wearing slip-on shoes because these
3/5/2012Maria Carmela L. Domocmat, RN, MSN
72
onot wearing slip-on shoes because these
cause feet to move forward and squash
toes
onot wearing court shoes because they
don’t support feet and can cramp toes

Corn pad
3/5/2012Maria Carmela L. Domocmat, RN, MSN
73
Prevention of corns
odrying properly between toes
o losing excess weight – this will help to
reduce pressure on feet
3/5/2012Maria Carmela L. Domocmat, RN, MSN
74
reduce pressure on feet
o If already have a corn, apply an antifungal
or antibacterial powder after washing foot
to help prevent it becoming infected.
3/5/2012Maria Carmela L. Domocmat, RN, MSN
75
3/5/2012Maria Carmela L. Domocmat, RN, MSN
76

Callus
• flat, poorly defined mass on the sole over a
bony prominence caused by pressure
• When skin is exposed to lots of pressure or
3/5/2012Maria Carmela L. Domocmat, RN, MSN
77
• When skin is exposed to lots of pressure or
friction, the keratin layer thickens to protect it,
and develops into a callus.
• Although calluses can cover a wide area, they
aren't usually painful.
Callus
• Treatment:
o padding and lanolin creams
o overall good skin hygiene
3/5/2012Maria Carmela L. Domocmat, RN, MSN
78
o overall good skin hygiene

• Self treatment or management of corns and
callus includes:
▫ following the advice of a Podiatrist
3/5/2012Maria Carmela L. Domocmat, RN, MSN
79
▫ following the advice of a Podiatrist
▫ proper fitting of footwear
▫ proper foot hygiene and the use of emollients to
keep the skin in good condition
3/5/2012
80
Maria Carmela L. Domocmat, RN, MSN

• Neuromas
▫ are non-cancerous growths of the nerve tissue that develop in different parts of the body.
3/5/2012
81
Maria Carmela L. Domocmat, RN, MSN
develop in different parts of the body.
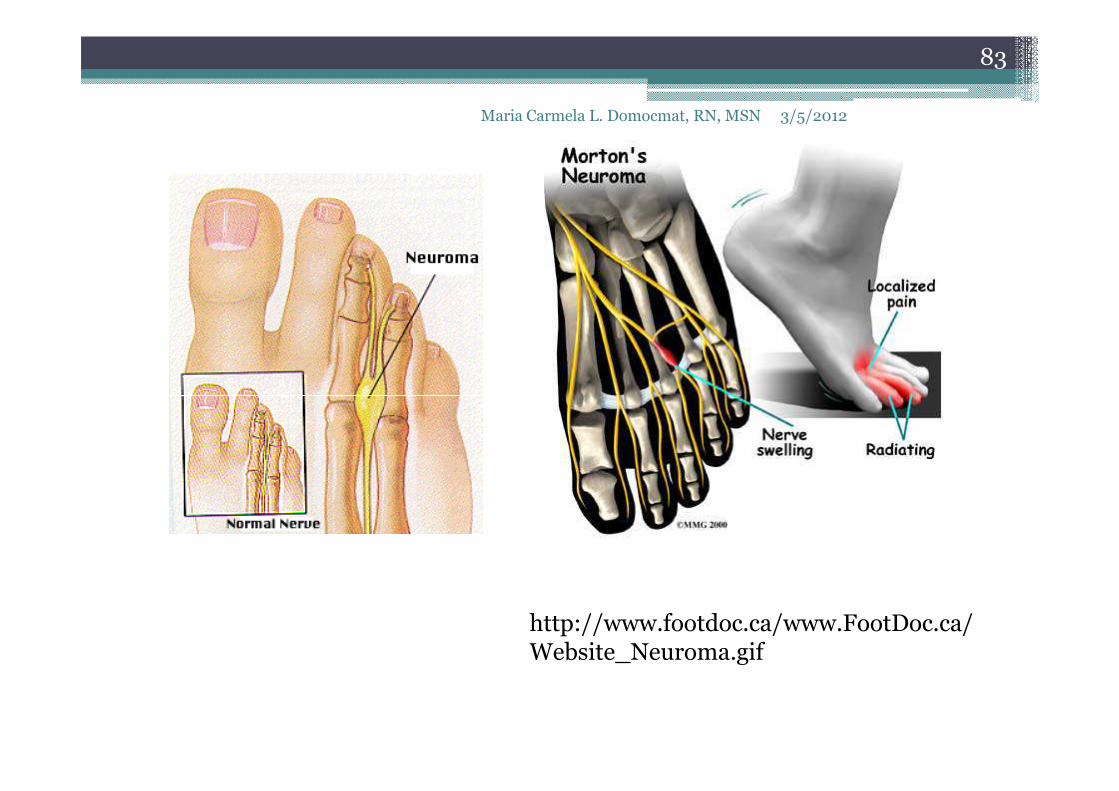
Mortons Neuroma
• affects a nerve in the foot, often times the nerve between the third and fourth toe.
• thickens the tissue around the nerves that lead
3/5/2012
82
Maria Carmela L. Domocmat, RN, MSN
• thickens the tissue around the nerves that lead to the toes, causing sharp, burning sensations in the ball of the foot, as well as a numbing or stinging feeling.
• AKA: plantar neuroma or intermetatarsalneuroma.
3/5/2012
83
Maria Carmela L. Domocmat, RN, MSN
http://www.footdoc.ca/www.FootDoc.ca/Website_Neuroma.gif
• Sex
▫ The female-to-male ratio for Morton's neuroma is 5:1.
3/5/2012
84
Maria Carmela L. Domocmat, RN, MSN
5:1.
• Age
▫ The highest prevalence of Morton's neuroma is found in patients aged 15-50 years, but the condition may occur in any ambulatory patient.
http://emedicine.medscape.com/article/308284-clinical#showall
Causes
• Various factors have been implicated in the precipitation of Morton's neuroma.
• Morton's neuroma is known to develop as a result of
3/5/2012
85
Maria Carmela L. Domocmat, RN, MSN
• Morton's neuroma is known to develop as a result of chronic nerve stress and irritation, particularly with excessive toe dorsiflexion.
• Poorly fitting and constricting shoes (ie, small toe box) or shoes with heel lifts often contribute to Morton's neuroma. Women who wear high-heeled shoes for a number of years or men who are required to wear constrictive shoe gear are at risk.
http://emedicine.medscape.com/article/308284-clinical#showall

Causes
• A biomechanical theory of causation involves the mechanics of the foot and ankle. For instance, individuals with tight gastrocnemius-soleusmuscles or who excessively pronate the foot may
3/5/2012
86
Maria Carmela L. Domocmat, RN, MSN
individuals with tight gastrocnemius-soleusmuscles or who excessively pronate the foot may compensate by dorsiflexion of the metatarsals subsequently irritating of the interdigital nerve.
• Certain activities carry increased risk of excessive toe dorsiflexion, such as prolonged walking, running, squatting, and demi-pointeposition in ballet.
http://emedicine.medscape.com/article/308284-clinical#showall
Manifestations
• Obtaining an accurate history is important to making the diagnosis of Morton's neuroma. Possible reported findings provided by the patient with Morton's neuroma include the
3/5/2012
87
Maria Carmela L. Domocmat, RN, MSN
Possible reported findings provided by the patient with Morton's neuroma include the following:
• The most common presenting complaints include pain and dysesthesias in the forefoot and corresponding toes adjacent to the neuroma.
• Pain is described as sharp and burning, and it may be associated with cramping.
http://emedicine.medscape.com/article/308284-clinical#showall

3/5/2012
88
Maria Carmela L. Domocmat, RN, MSN

Manifestations
• Numbness often is observed in the toes adjacent to the neuroma and seems to occur along with episodes of pain.
• Pain typically is intermittent, as episodes often occur for minutes to hours at a time and have long intervals (ie,
3/5/2012
89
Maria Carmela L. Domocmat, RN, MSN
minutes to hours at a time and have long intervals (ie, weeks to months) between a single or small group of multiple attacks.
• Some patients describe the sensation as "walking on a marble."
• Massage of the affected area offers significant relief.• Narrow tight high-heeled shoes aggravate the symptoms.• Night pain is reported but is rare.
http://emedicine.medscape.com/article/308284-clinical#showall
Dx tests
• palpable mass or a "click" between the bones. • Doctor put pressure on the spaces between the
toe bones to try to replicate the pain and look for
3/5/2012
90
Maria Carmela L. Domocmat, RN, MSN
toe bones to try to replicate the pain and look for calluses or evidence of stress fractures in the bones that might be the cause of the pain.
• Range of motion tests will rule out arthritis or joint inflammations.
• X-rays may be required to rule out a stress fracture or arthritis of the joints that join the toes to the foot.
http://emedicine.medscape.com/article/308284-clinical#showall

Treatment
• Rehabilitation Program: Physical Therapy
• Treatment strategies range from conservative to
3/5/2012
91
Maria Carmela L. Domocmat, RN, MSN
• Treatment strategies range from conservative to surgical management.
• The conservative approach may benefit from the involvement of a PT. ▫ Recommend soft-soled shoes with a wide toe box
and low heel (eg, an athletic shoe). ▫ High-heeled, narrow, nonpadded shoes should not
be worn, because they aggravate the condition.
http://emedicine.medscape.com/article/308284-clinical#showall
Treatment
• Rehabilitation Program: PT• conservative management
▫ to alter alignment of the metatarsal heads.
3/5/2012
92
Maria Carmela L. Domocmat, RN, MSN
▫ One recommended action is to elevate the metatarsal head medial and adjacent to the neuroma, thereby preventing compression and irritation of the digital nerve.
▫ A plantar pad is used most often for elevation. Have the patient insert a felt or gel pad into the shoe to achieve the desired elevation of the above metatarsal head.
http://emedicine.medscape.com/article/308284-clinical#showall

Treatment
• Rehabilitation Program: PT
• Cryotherapy
• Ultrasonography
3/5/2012
93
Maria Carmela L. Domocmat, RN, MSN
• Ultrasonography
• deep tissue massage
• stretching exercises.
http://emedicine.medscape.com/article/308284-clinical#showall
Treatment
• Rehabilitation Program: PT
• Ice is beneficial to decrease the associated inflammation.
3/5/2012
94
Maria Carmela L. Domocmat, RN, MSN
inflammation.
• Phonophoresis also can be used, rather than just ultrasonography, to further decrease pain and inflammation.
http://emedicine.medscape.com/article/308284-clinical#showall

Phonophoresis
3/5/2012Maria Carmela L. Domocmat, RN, MSN
95

Phonophoresis
3/5/2012Maria Carmela L. Domocmat, RN, MSN
96
Treatment
• Changes in footwear. Avoid high heels or tight shoes, and wear wider shoes with lower heels and a soft sole. This enables the bones to
3/5/2012
97
Maria Carmela L. Domocmat, RN, MSN
heels and a soft sole. This enables the bones to spread out and may reduce pressure on the nerve, giving it time to heal.
• Orthoses. Custom shoe inserts and pads also help relieve irritation by lifting and separating the bones, reducing the pressure on the nerve.
http://orthoinfo.aaos.org/topic.cfm?topic=a00158
Treatment
• Injection. One or more injections of a corticosteroid medication can reduce the swelling and inflammation of the nerve, bringing some relief.
3/5/2012
98
Maria Carmela L. Domocmat, RN, MSN
swelling and inflammation of the nerve, bringing some relief.
• Combination ▫ Several studies have shown that a combination
of roomier, more comfortable shoes, nonsteroidal anti-inflammatory medication, custom foot orthoses and cortisone injections provide relief in over 80 percent of people with Morton's Neuroma. http://orthoinfo.aaos.org/topic.cfm?topic=a00158

Surgical Intervention
• When conservative measures for Morton's neuroma are unsuccessful, surgical excision of the area of fibrosis in the common digital nerve may be curative.
• Common adverse outcomes include
3/5/2012
99
Maria Carmela L. Domocmat, RN, MSN
• Common adverse outcomes include ▫ dysesthesias radiating from a painful nerve stump.
Dysesthesias may be treated as any other dysesthetic pain.
• Surgical options include the following:▫ Neurectomy with nerve burial
▫ Transverse intermetatarsal ligament release, with or without neurolysis
▫ Endoscopic decompression of the transverse metatarsal ligament
http://emedicine.medscape.com/article/308284-clinical#showall

Other Treatment
• Perform injection into the dorsal aspect of the foot, 1-2 cm proximal to the webspace, in line with the MTP joints.
3/5/2012
100
Maria Carmela L. Domocmat, RN, MSN
with the MTP joints.
• Advance the needle through the midwebspaceinto the plantar aspect of the foot until the needle gently tents the skin. Then withdraw it about 1 cm to where the tip of the neuroma is located.
Other Treatment
• Inject a corticosteroid/anesthetic mix. A reasonable volume is 1 mL of corticosteroid and 2 mL of anesthetic. T
3/5/2012
101
Maria Carmela L. Domocmat, RN, MSN
2 mL of anesthetic. T
• the anesthetic used should not contain epinephrine, as necrosis may result. Care also should be taken not to inject into the plantar pad.

Other Treatment
• Adverse outcomes include plantar fat pad necrosis. Transient numbness of the toes also may occur. Although many practitioners use
3/5/2012
102
Maria Carmela L. Domocmat, RN, MSN
may occur. Although many practitioners use multiple injections, the likelihood of benefit from subsequent injections, after failure to achieve relief from the initial injection, is negligible.
Other Treatment
• An Australian investigation using a single, ultrasonographically guided corticosteroid injection for Morton's
3/5/2012
103
Maria Carmela L. Domocmat, RN, MSN
corticosteroid injection for Morton's neuroma found that 9 months after treatment, complete pain relief had occurred in 11 of the 39 neuromas studied.

Neurectomy: typical incision location. Neurectomy: superficial exposure.
3/5/2012
104
Maria Carmela L. Domocmat,
RN, MSN
Neurectomy: typical incision location. Neurectomy: superficial exposure.
Neurectomy: deeper dissection. Neuroma and adherent fibrofatty tissue.http://emedicine.medscape.com/article/308284-clinical#showall

Medication Summary
• Dysesthesias may be treated as any other dysesthetic pain.
• Tricyclic antidepressants, such as amitriptyline
3/5/2012
105
Maria Carmela L. Domocmat, RN, MSN
• Tricyclic antidepressants, such as amitriptylineat 10-25 mg PO qhs, may be tried.
• If this approach is unsuccessful, anticonvulsants (eg, gabapentin, carbamazepine) often are effective.

Tricyclic Antidepressants
• A complex group of drugs that have central and peripheral anticholinergic effects, as well as sedative effects. They have central effects on pain transmission, and they block the active re-
3/5/2012
106
Maria Carmela L. Domocmat, RN, MSN
sedative effects. They have central effects on pain transmission, and they block the active re-uptake of norepinephrine and serotonin.
• Amitriptyline (Elavil)▫ Analgesic for certain chronic and neuropathic
pain. Low doses, 10-25 mg qhs, may provide pain relief from burning and tingling occurring at rest but function only as an adjunct to definitive treatment.
Anticonvulsants
• Use of certain antiepileptic drugs (AEDs), such as the GABA analogue Neurontin (gabapentin), has proven helpful in some cases of neuropathic pain. Thus, although unstudied, a trial of such an agent might conceivably provide analgesia for symptomatic
3/5/2012
107
Maria Carmela L. Domocmat, RN, MSN
although unstudied, a trial of such an agent might conceivably provide analgesia for symptomatic neuropathy. Used for dysesthesias not controlled with definitive treatment plus tricyclic antidepressants (or in patients unable to take tricyclic antidepressants).
• Gabapentin (Neurontin)▫ Neuromembrane stabilizer useful in pain reduction with
dysesthetic pain. Has antineuralgic effects; however, exact mechanism of action is unknown. Structurally related to GABA, but does not interact with GABA receptors.
Anticonvulsants
• Pregabalin (Lyrica)▫ Structural derivative of GABA. Mechanism of
action unknown. Binds with high affinity to alpha2-delta site (a calcium channel subunit). In
3/5/2012
108
Maria Carmela L. Domocmat, RN, MSN
alpha2-delta site (a calcium channel subunit). In vitro, reduces calcium-dependent release of several neurotransmitters, possibly by modulating calcium channel function. FDA approved for neuropathic pain associated with diabetic peripheral neuropathy or postherpetic neuralgia and as adjunctive therapy in partial-onset seizures.
Serotonin-Norepinephrine Reuptake Inhibitors• These agents inhibit neuronal serotonin and
norepinephrine reuptake.
• Duloxetine (Cymbalta)
3/5/2012
109
Maria Carmela L. Domocmat, RN, MSN
• Duloxetine (Cymbalta)
▫ Description Indicated for diabetic peripheral neuropathic pain. Potent inhibitor of neuronal serotonin and norepinephrine reuptake

3/5/2012Maria Carmela L. Domocmat, RN, MSN
110

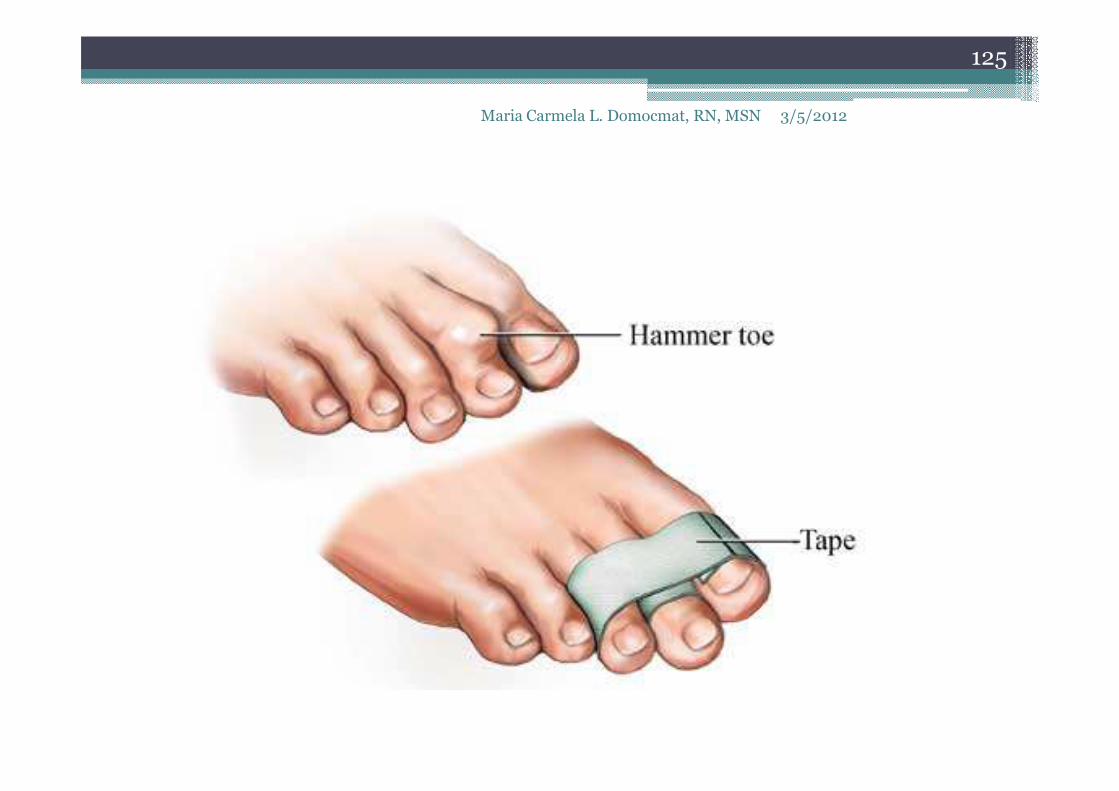
Hammer toe
• is a deformity of the toe, in which the end of the toe is bent downward.
• usually affects the second toe. However, it may
3/5/2012
111
Maria Carmela L. Domocmat, RN, MSN
• usually affects the second toe. However, it may also affect the other toes. The toe moves into a claw-like position.

Hammer toe
3/5/2012Maria Carmela L. Domocmat, RN, MSN
112

Causes, incidence, and risk factors
• most common cause of hammer toe is wearing short, narrow shoes that are too tight. The toe is forced into a bent position. Muscles and tendons
3/5/2012
113
Maria Carmela L. Domocmat, RN, MSN
forced into a bent position. Muscles and tendons in the toe tighten and become shorter.
Causes, incidence, and risk factors
• Hammer toe is more likely to occur in:▫ Women who wear shoes that do not fit well or
have high heels
3/5/2012
114
Maria Carmela L. Domocmat, RN, MSN
▫ Children who keep wearing shoes they have outgrown
• The condition may be present at birth (congenital) or develop over time.
• In rare cases, all of the toes are affected. This may be caused by a problem with the nerves or spinal cord.

Causes, incidence, and risk factors
• may be present at birth (congenital) or develop over time.
• In rare cases, all of the toes are affected. This
3/5/2012
115
Maria Carmela L. Domocmat, RN, MSN
• In rare cases, all of the toes are affected. This may be caused by a problem with the nerves or spinal cord.

Symptoms
• The middle joint of the toe is bent. The end part of the toe bends down into a claw-like deformity. At first, you may be able to move and straighten
3/5/2012
116
Maria Carmela L. Domocmat, RN, MSN
At first, you may be able to move and straighten the toe. Over time, you will no longer be able to move the toe.
• A corn often forms on the top of the toe. A callus is found on the sole of the foot.
• Walking or wearing shoes can be painful.

Hammer toe
3/5/2012Maria Carmela L. Domocmat, RN, MSN
117
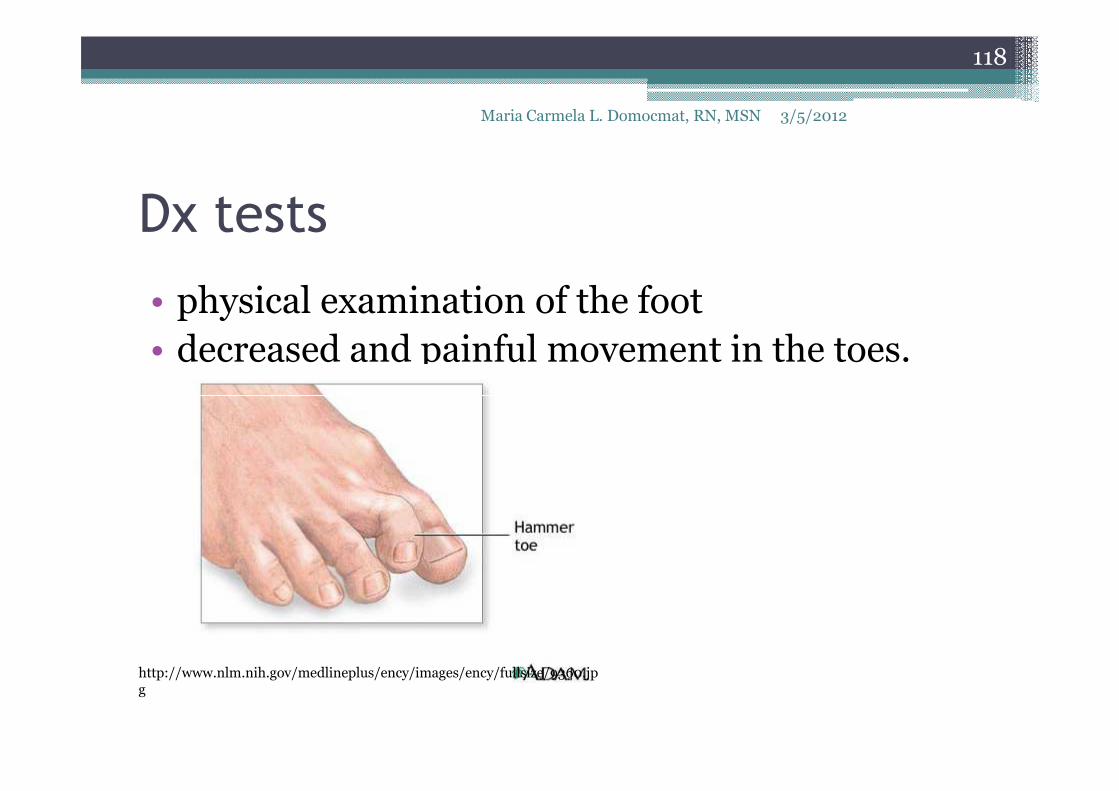
Dx tests
• physical examination of the foot
• decreased and painful movement in the toes.
3/5/2012
118
Maria Carmela L. Domocmat, RN, MSN
http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/9360.jpg

3/5/2012
119
Maria Carmela L. Domocmat, RN, MSN
http://www.myfootshop.com/images/medical/ortho/hammer_toe_differences_mod.jpg

Treatment
• Mild hammer toe in children can be treated by manipulating and splinting the affected toe.
3/5/2012
120
Maria Carmela L. Domocmat, RN, MSN
http://www.family-foot.com/images/hammer_toe_whatis.jpg
Treatment
• The following changes in footwear may help relieve symptoms:
▫ Wear the right size shoes or shoes with wide toe
3/5/2012
121
Maria Carmela L. Domocmat, RN, MSN
▫ Wear the right size shoes or shoes with wide toe boxes for comfort, and to avoid making hammer toe worse.
▫ Avoid high heels as much as possible.
▫ Wear soft insoles to relieve pressure on the toe.
▫ Protect the joint that is sticking out with corn pads or felt pads
Treatment
• A foot doctor can make foot devices called hammer toe regulators or straighteners for you, or you can buy them at the store.
3/5/2012
122
Maria Carmela L. Domocmat, RN, MSN
or you can buy them at the store.
• Exercises may be helpful.
▫ You can try gentle stretching exercises if the toe is not already in a fixed position.
▫ Picking up a towel with your toes can help stretch and straighten the small muscles in the foot.
Treatment
• For severe hammer toe, you will need an operation to straighten the joint.
• The surgery often involves cutting or moving
3/5/2012
123
Maria Carmela L. Domocmat, RN, MSN
• The surgery often involves cutting or moving tendons and ligaments.
• Sometimes the bones on each side of the joint need to be connected (fussed) together.
• Most of the time, you will go home on the same day as the surgery. The toe may still be stiff afterward, and it may be shorter.

Prevention and Cure of Hammer Toes with Products• Hammer Toe
Regulator
• Hammer Toe Cushion
• Yoga Toes Toe Stretcher
• Toe Rings
3/5/2012
124
Maria Carmela L. Domocmat, RN, MSN
• Hammer Toe Cushion
• Foam Toe Tubes
• Gel Toe Cap
• Toe Spreader
• Silicone Toe Crest
• Toe Spacer Cushion
• Digital Toe Pad
• Toe Rings
• Toe Brace
• Toe Alignment Splint
• Toe Trainers
• Hammer Toe Straightener
3/5/2012
125
Maria Carmela L. Domocmat, RN, MSN

Hammer Toe Correction Bandage
• Price $14.95
3/5/2012
126
Maria Carmela L. Domocmat, RN, MSN

Hammer Toe Regulator
• Toe regulator efficiently integrates the middle joint of toe with other joints.
• It reduces the pressure and
3/5/2012Maria Carmela L. Domocmat, RN, MSN
127
• It reduces the pressure and irritation at toe tips and region over the toes.
• The toe regulator straightens the joint of hammer toes (or) claw toes with a slight and smooth pressure.
• Toe regulator is effective for pain relief and proper alignment of hammer toes.

Hammer Toe Regulator
3/5/2012Maria Carmela L. Domocmat, RN, MSN
128

Hammer Toe Cushion
• provides ease feel over the contracted part and comforts Hammer toe with enough support.
3/5/2012Maria Carmela L. Domocmat, RN, MSN
129
support.
• assists for a stress free movement and aid in lifting the toe to normal position.
• minimizes pressure at the top and tip of toes with a spongy effect.
• is provided with an adjustable toe loop for comfortable and secure fit.

Foam Toe Tubes
• The soft foam present in the tube safeguard toes from rash rubbing against footwear.
• Foam toe tube is easy to wear
3/5/2012Maria Carmela L. Domocmat, RN, MSN
130
• Foam toe tube is easy to wear for getting effective pain relief from hammer toes.
• It reduce the pressure and swelling over Hammer toes for trouble free walks.
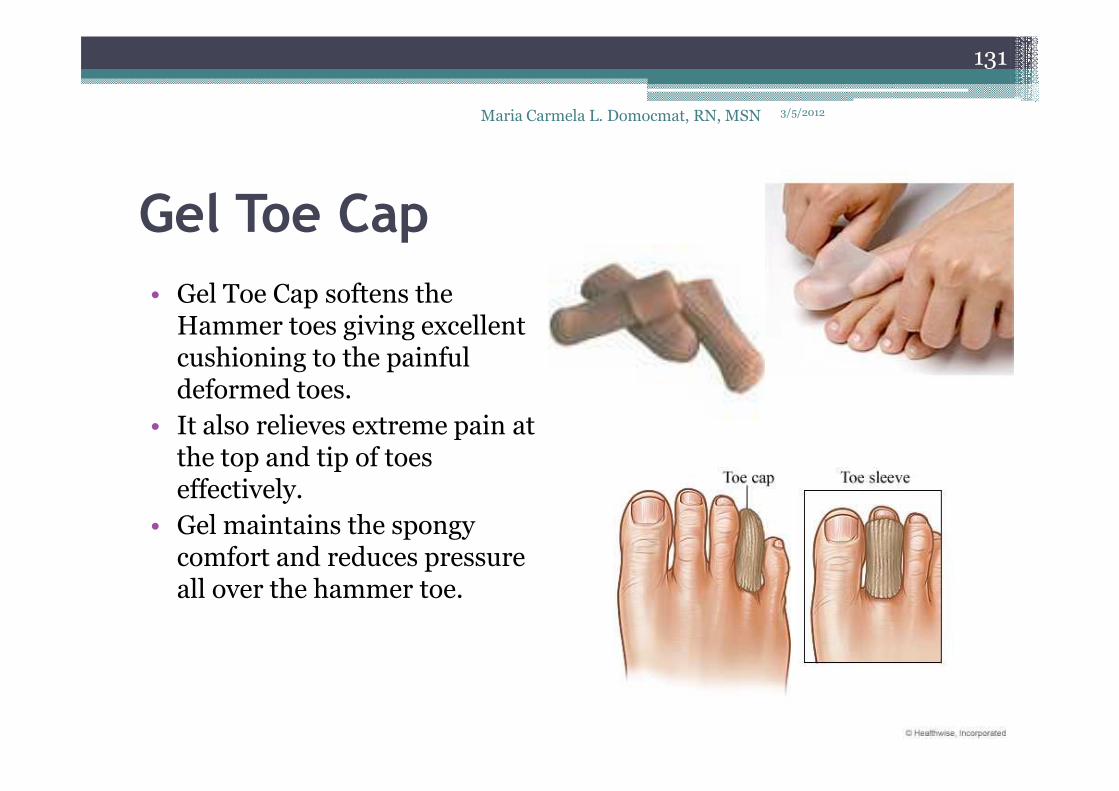
Gel Toe Cap
• Gel Toe Cap softens the Hammer toes giving excellent cushioning to the painful deformed toes.
3/5/2012Maria Carmela L. Domocmat, RN, MSN
131
deformed toes.
• It also relieves extreme pain at the top and tip of toes effectively.
• Gel maintains the spongy comfort and reduces pressure all over the hammer toe.
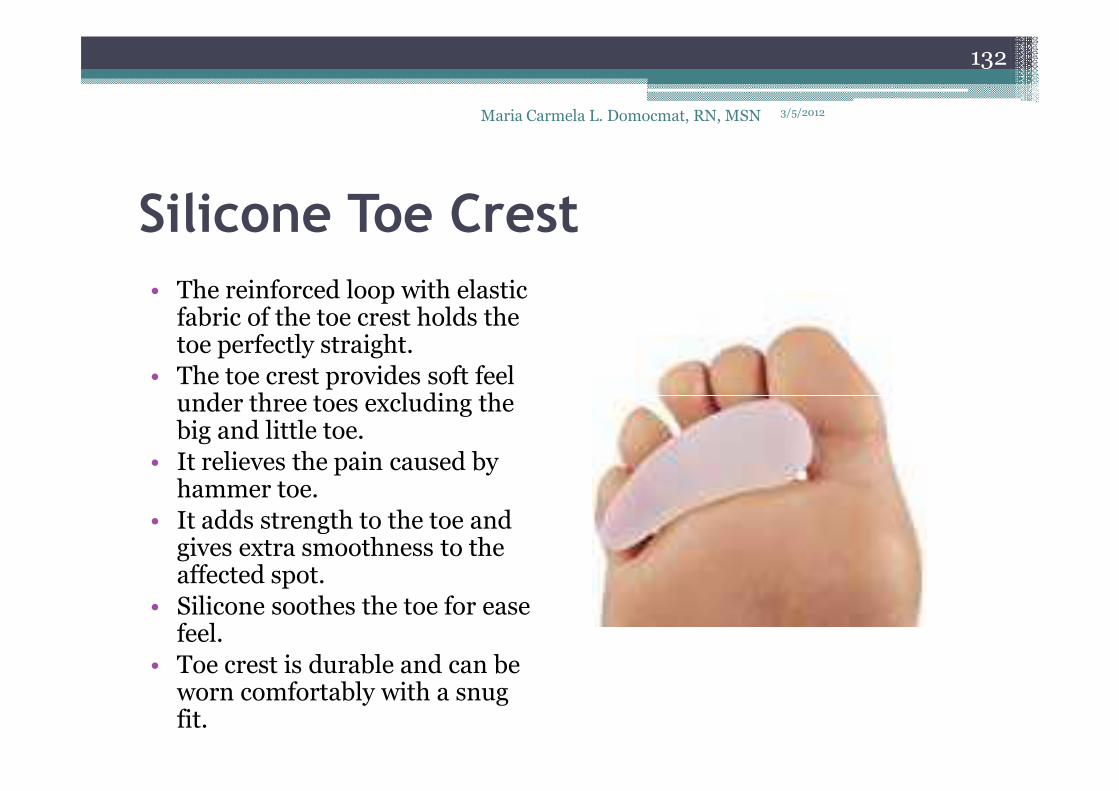
Silicone Toe Crest
• The reinforced loop with elastic fabric of the toe crest holds the toe perfectly straight.
• The toe crest provides soft feel under three toes excluding the
3/5/2012Maria Carmela L. Domocmat, RN, MSN
132
under three toes excluding the big and little toe.
• It relieves the pain caused by hammer toe.
• It adds strength to the toe and gives extra smoothness to the affected spot.
• Silicone soothes the toe for ease feel.
• Toe crest is durable and can be worn comfortably with a snug fit.
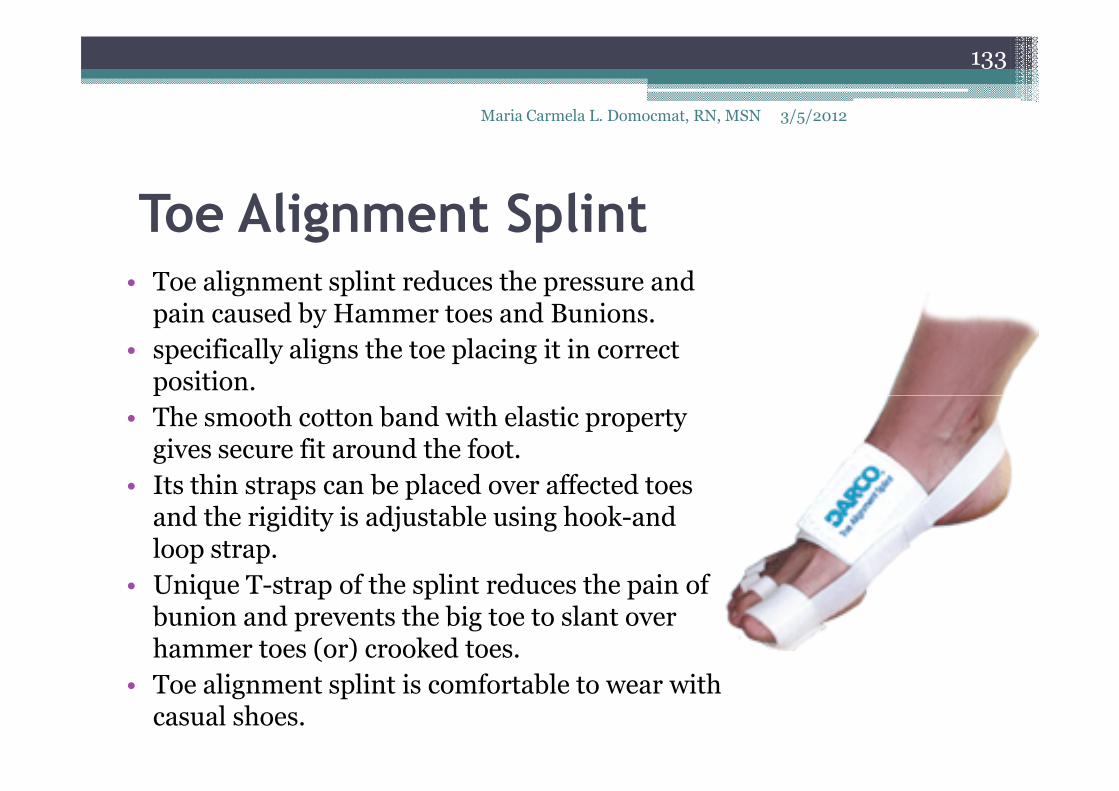
Toe Alignment Splint• Toe alignment splint reduces the pressure and
pain caused by Hammer toes and Bunions.
• specifically aligns the toe placing it in correct position.
3/5/2012
133
Maria Carmela L. Domocmat, RN, MSN
position.
• The smooth cotton band with elastic property gives secure fit around the foot.
• Its thin straps can be placed over affected toes and the rigidity is adjustable using hook-and loop strap.
• Unique T-strap of the splint reduces the pain of bunion and prevents the big toe to slant over hammer toes (or) crooked toes.
• Toe alignment splint is comfortable to wear with casual shoes.
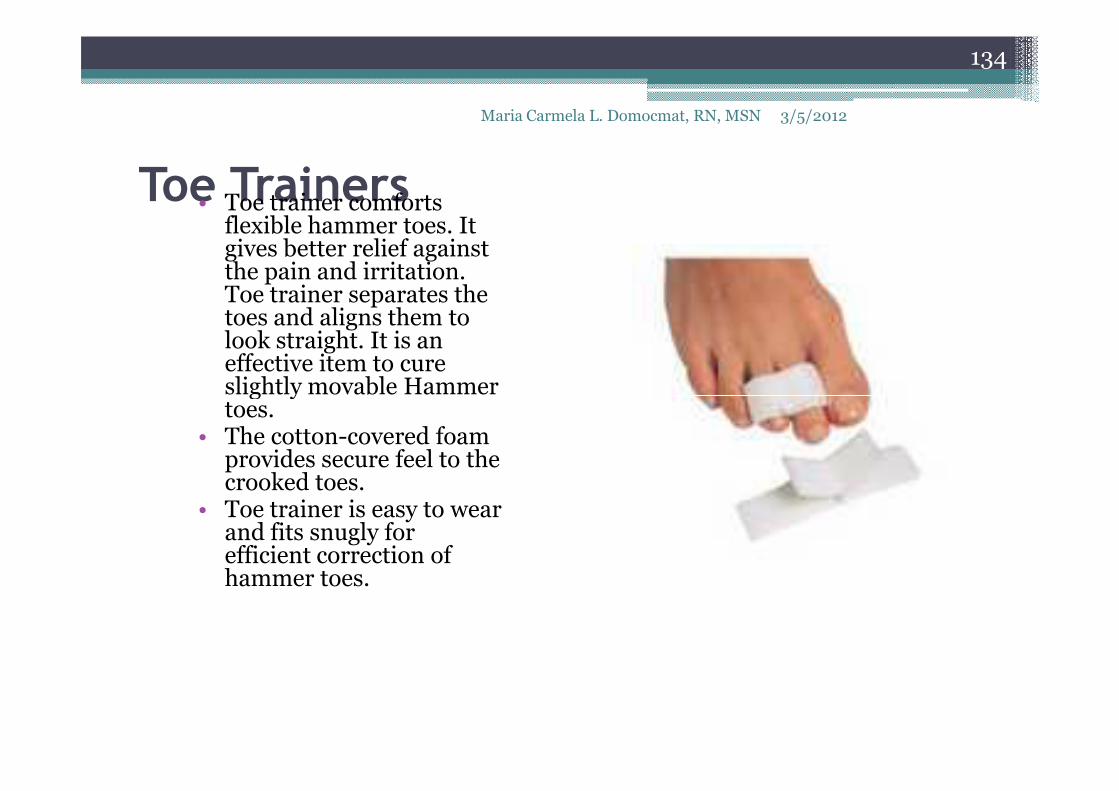
Toe Trainers• Toe trainer comforts flexible hammer toes. It gives better relief against the pain and irritation. Toe trainer separates the toes and aligns them to look straight. It is an effective item to cure slightly movable Hammer toes.
3/5/2012
134
Maria Carmela L. Domocmat, RN, MSN
slightly movable Hammer toes.
• The cotton-covered foam provides secure feel to the crooked toes.
• Toe trainer is easy to wear and fits snugly for efficient correction of hammer toes.

Hammer Toe Straightener• The toe Straightener perfectly aligns Hammer toes with little pressure. Its cotton-covered loop with elasticity holds the toe firmly in proper place and it can be easily adjusted for stress free movements. The smooth foam pad molds accordingly with the foot shape and renders superior cushioning at the bottom of the feet. It also stops the
3/5/2012
135
Maria Carmela L. Domocmat, RN, MSN
and renders superior cushioning at the bottom of the feet. It also stops the pain caused by hammer toes. The hook closure present in the toe straightenerpulls down and aligns the deformed toes to keep you always smiling.
• Hammer toe Straightener assists for healthy feet by strengthening the toes and forefoot muscles.

Prevention
• Avoid wearing shoes that are too short or narrow.
• Check children's shoe sizes often, especially
3/5/2012
136
Maria Carmela L. Domocmat, RN, MSN
• Check children's shoe sizes often, especially during periods of fast growth.
Expectations (prognosis)
• If the condition is treated early, you can often avoid surgery.
• Treatment will reduce pain and walking
3/5/2012
137
Maria Carmela L. Domocmat, RN, MSN
• Treatment will reduce pain and walking difficulty.

Complications
• Foot deformity
• Posture changes caused by difficulty in walking
3/5/2012
138
Maria Carmela L. Domocmat, RN, MSN

3/5/2012Maria Carmela L. Domocmat, RN, MSN
139

3/5/2012Maria Carmela L. Domocmat, RN, MSN
140

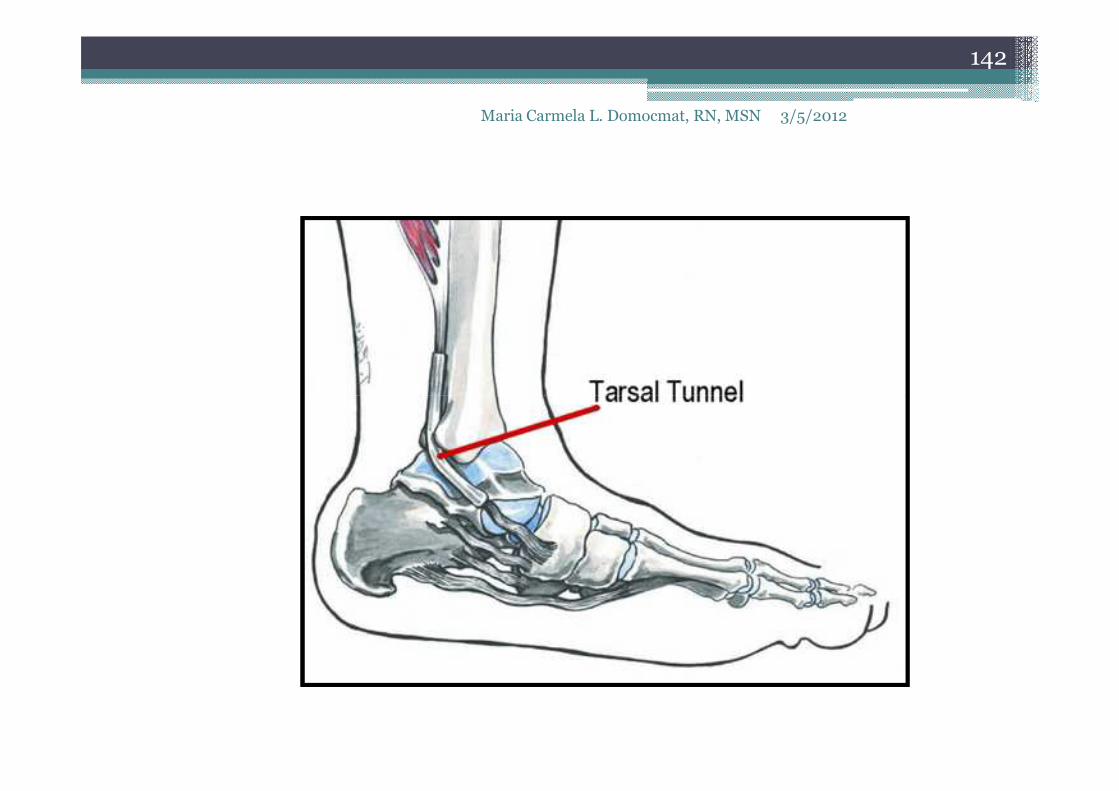
Tarsal tunnel syndrome
• the ankle version of carpal tunnel syndrome
(CTS)
• posterior tibial nerve in the ankle becomes
3/5/2012Maria Carmela L. Domocmat, RN, MSN
141
• posterior tibial nerve in the ankle becomes
compressed, resulting in loss of sensation and
pain in a portion of the foot
3/5/2012Maria Carmela L. Domocmat, RN, MSN
142
Tarsal tunnel syndrome
• median and lateral plantar branches, which
supply the sole of the and distal phalanges, are
affected by nerve compression
3/5/2012Maria Carmela L. Domocmat, RN, MSN
143
affected by nerve compression
• dx and treatment: same with CTS

3/5/2012Maria Carmela L. Domocmat, RN, MSN
144

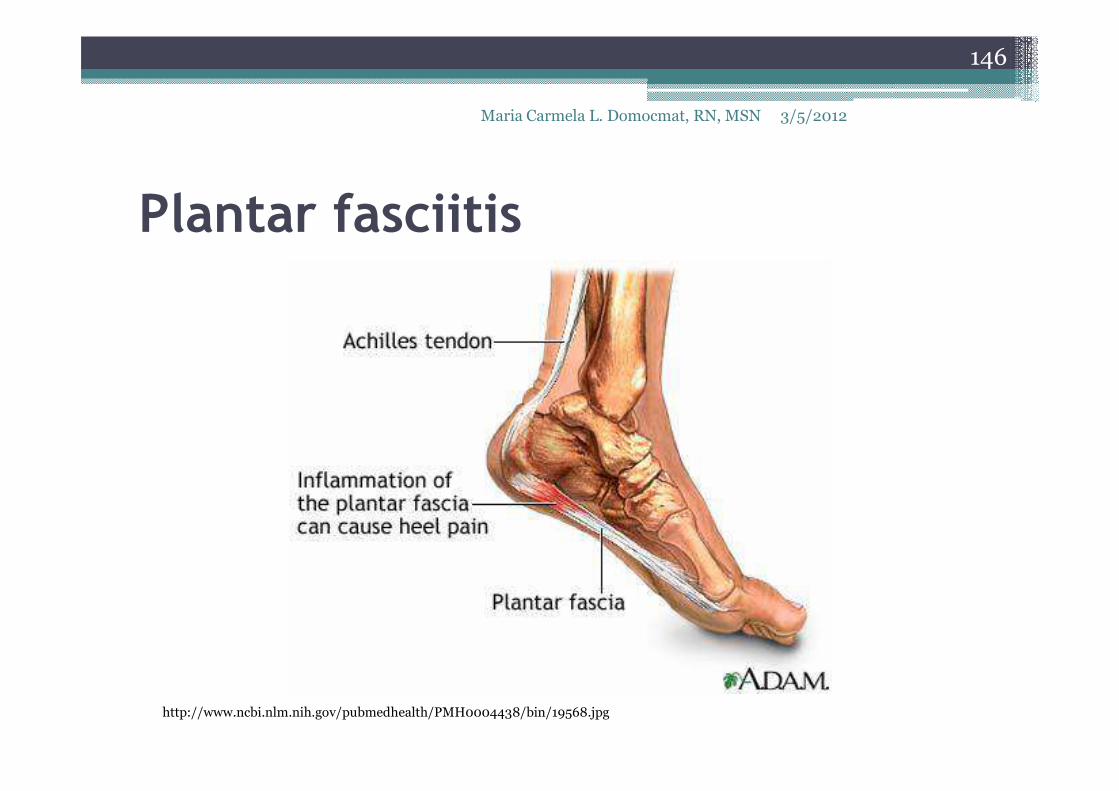
Plantar fasciitis
• an inflammation of the plantar fascia, which is
located in the area of the arch of the foot
• common: middle-aged and older adults,
3/5/2012Maria Carmela L. Domocmat, RN, MSN
145
• common: middle-aged and older adults,
athletes esp runners
Plantar fasciitis
146
Maria Carmela L. Domocmat, RN, MSN 3/5/2012
http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0004438/bin/19568.jpg

Plantar fascia
• A very thick band of tissue that covers the bones on the bottom of the foot.
• extends from the heel to the bones of the ball of the foot and acts like a rubber band to create tension
147
Maria Carmela L. Domocmat, RN, MSN 3/5/2012
foot and acts like a rubber band to create tension which maintains the arch of the foot.
• If the band is long it allows the arch of the foot to be low, which is most commonly known as having a flat foot.
• A short band of tissue causes a high arch.• This fascia can become inflamed and painful in
some people, making walking more difficult.

Plantar fascia
148
Maria Carmela L. Domocmat, RN, MSN 3/5/2012
http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0004438/bin/19567.jpg
Risk factors
o Foot arch problems (both flat feet and high
arches)
oObesity or sudden weight gain
3/5/2012Maria Carmela L. Domocmat, RN, MSN
149
oObesity or sudden weight gain
o Long-distance running, especially running
downhill or on uneven surfaces
o Sudden weight gain
o Tight Achilles tendon (the tendon connecting
the calf muscles to the heel)
o Shoes with poor arch support or soft soles

s/s:
• The most common complaint is pain and
stiffness in the bottom of the heel. The heel
pain may be dull or sharp. The bottom of the
3/5/2012Maria Carmela L. Domocmat, RN, MSN
150
pain may be dull or sharp. The bottom of the
foot may also ache or burn.
s/s
oThe pain is usually worse:
� In the morning when you take r first steps
� After standing or sitting for a while
3/5/2012Maria Carmela L. Domocmat, RN, MSN
151
� After standing or sitting for a while
� When climbing stairs
� After intense activity
oThe pain may develop slowly over time, or
suddenly after intense activity.
Treatment
oconservative treatment:
� rest
� ice - at least twice a day for 10 - 15 minutes,
3/5/2012Maria Carmela L. Domocmat, RN, MSN
152
� ice - at least twice a day for 10 - 15 minutes,
more often in the first couple of days.
� stretching exercises
� strapping of foot to maintain arch
� orthotics

Treatment
oconservative treatment:
� heel stretching exercises
� resting as much as possible for at least a week
3/5/2012Maria Carmela L. Domocmat, RN, MSN
153
� resting as much as possible for at least a week
� shoes with good support and cushions
� wear heel cup, felt pads in the heel area, or
shoe inserts
� use night splints to stretch the injured fascia
and allow it to heal.
Treatment
o If these treatments do not work, doctor may
recommend:
� Wearing a boot cast, which looks like a ski boot,
3/5/2012Maria Carmela L. Domocmat, RN, MSN
154
� Wearing a boot cast, which looks like a ski boot,
for 3-6 weeks. It can be removed for bathing.
� Custom-made shoe inserts (orthotics)
� Steroid shots or injections into the heel
� NSAIDs or steroids
� endoscopic surgery – to remove inflamed tissue
may be required

Boot cast
3/5/2012Maria Carmela L. Domocmat,
RN, MSN
155
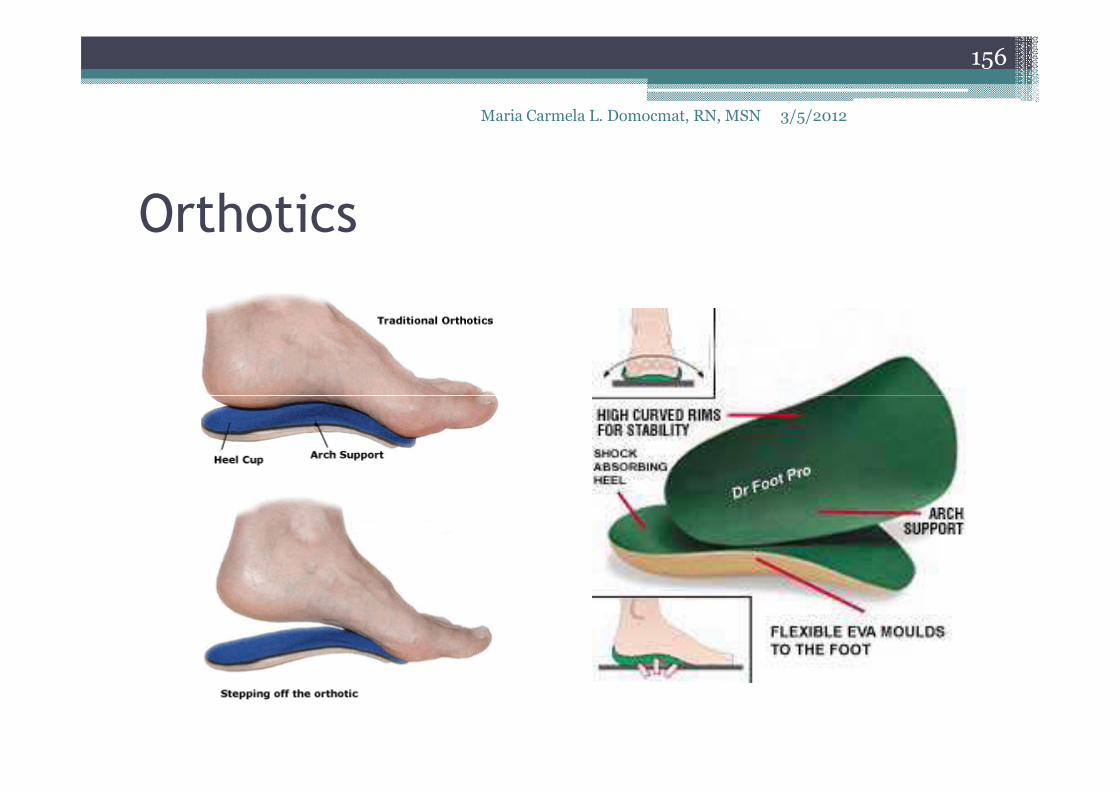
Orthotics
3/5/2012Maria Carmela L. Domocmat, RN, MSN
156

Orthotic devices
3/5/2012Maria Carmela L. Domocmat, RN, MSN
157

Expectations (prognosis)
oNonsurgical treatments almost always
improve the pain.
• Treatment can last from several months to 2
3/5/2012Maria Carmela L. Domocmat, RN, MSN
158
• Treatment can last from several months to 2
years before symptoms get better. Most
patients feel better in 9 months. Some people
need surgery to relieve the pain.

Complications
oPain may continue despite treatment.
oSome may need surgery.
3/5/2012Maria Carmela L. Domocmat, RN, MSN
159
3/5/2012Maria Carmela L. Domocmat, RN, MSN
160

Ingrown Nail
• nail silver penetration of the skin, causing
inflammation
• occurs when the edge of the nail grows down
3/5/2012Maria Carmela L. Domocmat, RN, MSN
161
• occurs when the edge of the nail grows down
and into the skin of the toe. There may be pain,
redness, and swelling around the nail.

Anatomy of a toenail
3/5/2012Maria Carmela L. Domocmat, RN, MSN
162
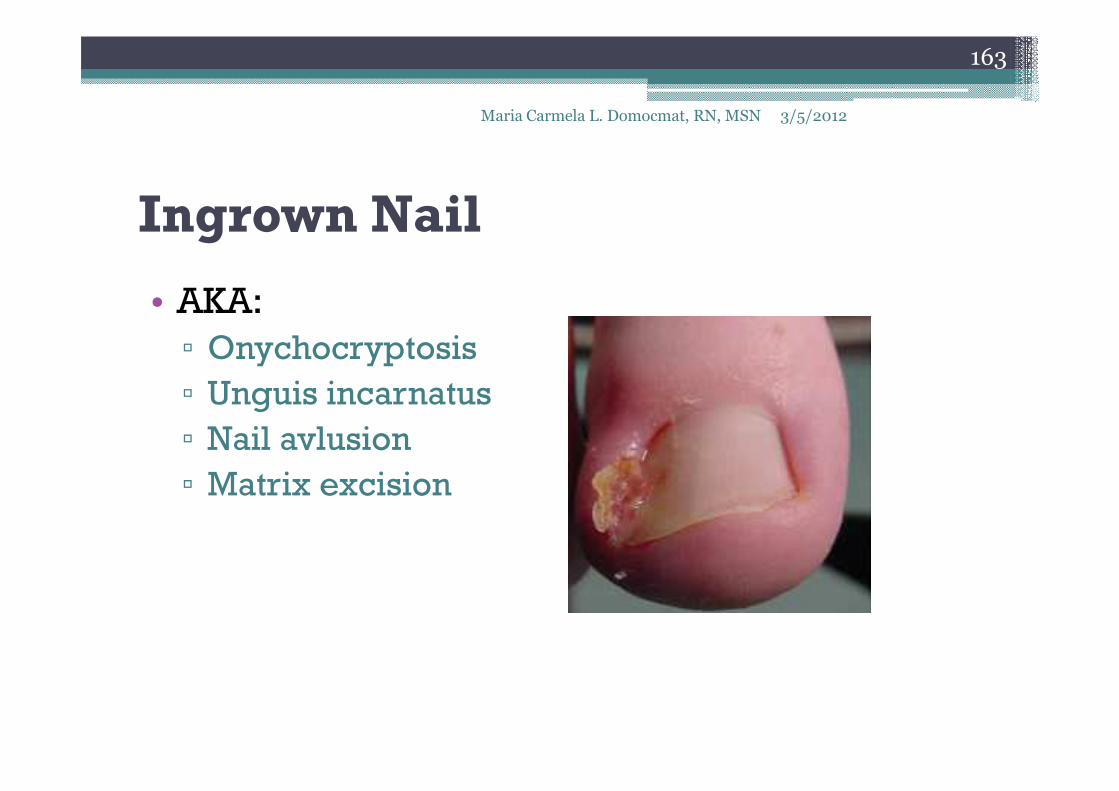
Ingrown Nail
• AKA:
▫ Onychocryptosis
▫ Unguis incarnatus
3/5/2012Maria Carmela L. Domocmat, RN, MSN
163
▫ Unguis incarnatus
▫ Nail avlusion
▫ Matrix excision
Causes, incidence, and risk factors
• An ingrown toenail can result from a number of
things,
• but poorly fitting shoes and toenails that are
3/5/2012Maria Carmela L. Domocmat, RN, MSN
164
• but poorly fitting shoes and toenails that are
not trimmed properly are the most common
causes.
• The skin along the edge of a toenail may
become red and infected.
• The great toe is usually affected, but any
toenail can become ingrown.
3/5/2012Maria Carmela L. Domocmat, RN, MSN
165

Causes, incidence, and risk factors
• Ingrown toenails may occur when extra
pressure is placed on toe.
• Most commonly, this pressure is caused by
3/5/2012Maria Carmela L. Domocmat, RN, MSN
166
• Most commonly, this pressure is caused by
shoes that are too tight or too loose.
• If walk often or participate in athletics, a shoe
that is even a little tight can cause this
problem.
• Some deformities of the foot or toes can also
place extra pressure on the toe.

Infected ingrown toenail
3/5/2012Maria Carmela L. Domocmat, RN, MSN
167

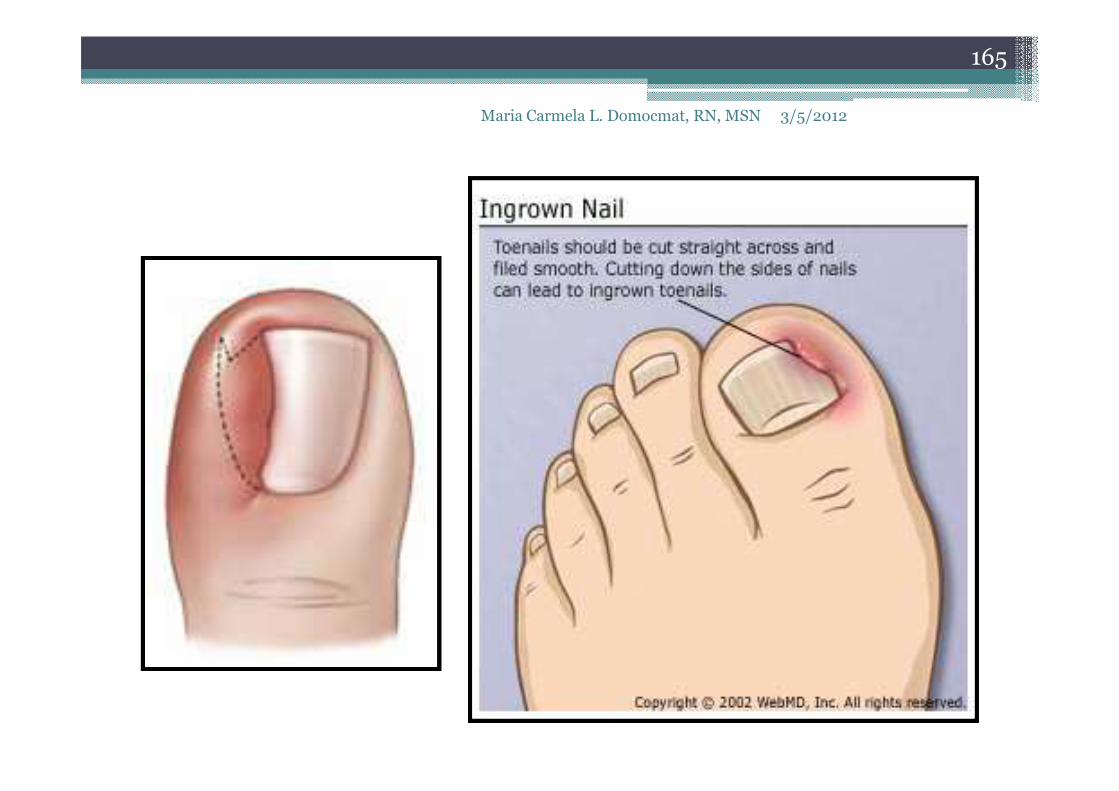
Causes, incidence, and risk factors
oNails that are not trimmed properly can also
cause ingrown toenails.� When toenails are trimmed too short or the edges
3/5/2012Maria Carmela L. Domocmat, RN, MSN
168
� When toenails are trimmed too short or the edges
are rounded rather than cut straight across, the
nail may curl downward and grow into the skin.
� Poor eyesight and physical inability to reach the
toe easily, as well as having thick nails, can make
improper trimming of the nails more likely.
� Picking or tearing at the corners of the nails can
also cause an ingrown toenail.

Causes, incidence, and risk factors
• Some people are born with nails that are
curved and tend to grow downward. Others
have toenails that are too large for their toes.
3/5/2012Maria Carmela L. Domocmat, RN, MSN
169
have toenails that are too large for their toes.
Stubbing your toe or other injuries can also
lead to an ingrown toenail.

Treatment
• If have diabetes, nerve damage in the leg or
foot, poor blood circulation to foot, or an
infection around the nail, go to the doctor right
3/5/2012Maria Carmela L. Domocmat, RN, MSN
170
infection around the nail, go to the doctor right
away.
• Do NOT try to treat this problem at home
(Bathroom treatment)

Treatment
oTo treat an ingrown nail at home:
� Soak the foot in warm water 3 to 4 times a day
if possible. Keep the toe dry, otherwise.
3/5/2012Maria Carmela L. Domocmat, RN, MSN
171
if possible. Keep the toe dry, otherwise.
� Gently massage over the inflamed skin.
� Place a small piece of cotton or dental floss
under the nail. Wet the cotton with water or
antiseptic.
Treatment
� may trim the toenail one time, if needed. When trimming toenails:� Consider briefly soaking your foot in warm water to
soften the nail.
3/5/2012Maria Carmela L. Domocmat, RN, MSN
172
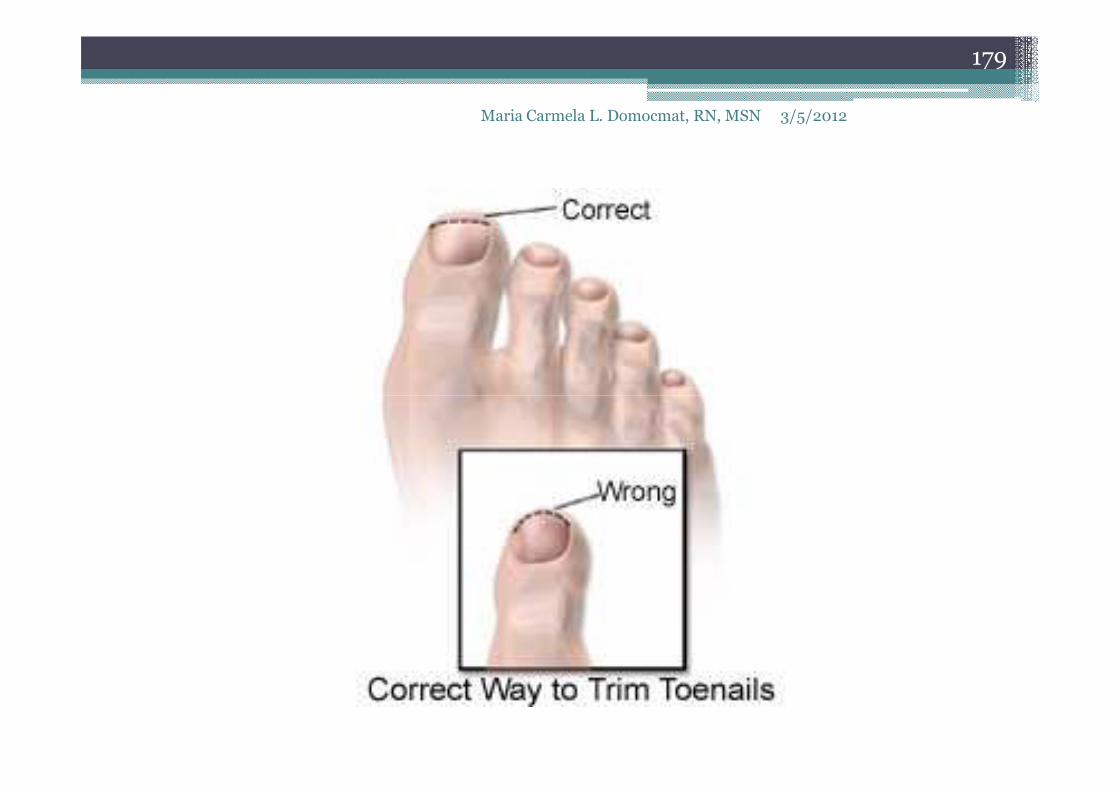
soften the nail.� Use a clean, sharp trimmer.� Trim toenails straight across the top. Do not taper or
round the corners or trim too short. Do not try to cut out the ingrown portion of the nail. This will only make the problem worse.
� Consider wearing sandals until the problem has gone away. Over-the-counter medications that are placed over the ingrown toenail may help some with the pain but do not treat the problem.

Proper and improper toenail trimming.
3/5/2012Maria Carmela L. Domocmat, RN, MSN
173

Treatment
� If this does not work and the ingrown nail gets
worse, see family doctor, a foot specialist
(podiatrist) or a skin specialist (dermatologist).
3/5/2012Maria Carmela L. Domocmat, RN, MSN
174
(podiatrist) or a skin specialist (dermatologist).
� removal of silver by podiatrist
� partial nail avulsion
o If ingrown nail does not heal or keeps coming
back, doctor may remove part of the nail.
3/5/2012Maria Carmela L. Domocmat, RN, MSN
175
back, doctor may remove part of the nail.
o Numbing medicine is first injected into the toe.
o Using scissors, your doctor then cuts along the
edge of the nail where the skin is growing over.
This portion of the nail is then removed. This is
called a partial nail avulsion.
o It will take 2 to 4 months for the nail to regrow

� Sometimes doctor will use a chemical,
electrical current, or another small surgical cut
to destroy or remove the area from which a new
3/5/2012Maria Carmela L. Domocmat, RN, MSN
176
to destroy or remove the area from which a new
nail may grow.
� antibiotic ointment - If the toe is infected
Prevention
• Wear shoes that fit properly.
• Shoes worn every day should have plenty of
room around toes.
3/5/2012Maria Carmela L. Domocmat, RN, MSN
177
room around toes.
• Shoes that wear for walking briskly or for
running should have plenty of room also, but
not be too loose.

Prevention
oWhen trimming toenails:� Considering briefly soaking foot in warm
water to soften the nail.
3/5/2012Maria Carmela L. Domocmat, RN, MSN
178
water to soften the nail.
� Use a clean, sharp nail trimmer.
� Trim toenails straight across the top. Do not
taper or round the corners or trim too short.
� Do not pick or tear at the nails.
� Keep the feet clean and dry. People with
diabetes should have routine foot exams and
nail care.
3/5/2012Maria Carmela L. Domocmat, RN, MSN
179

3/5/2012Maria Carmela L. Domocmat, RN, MSN
180
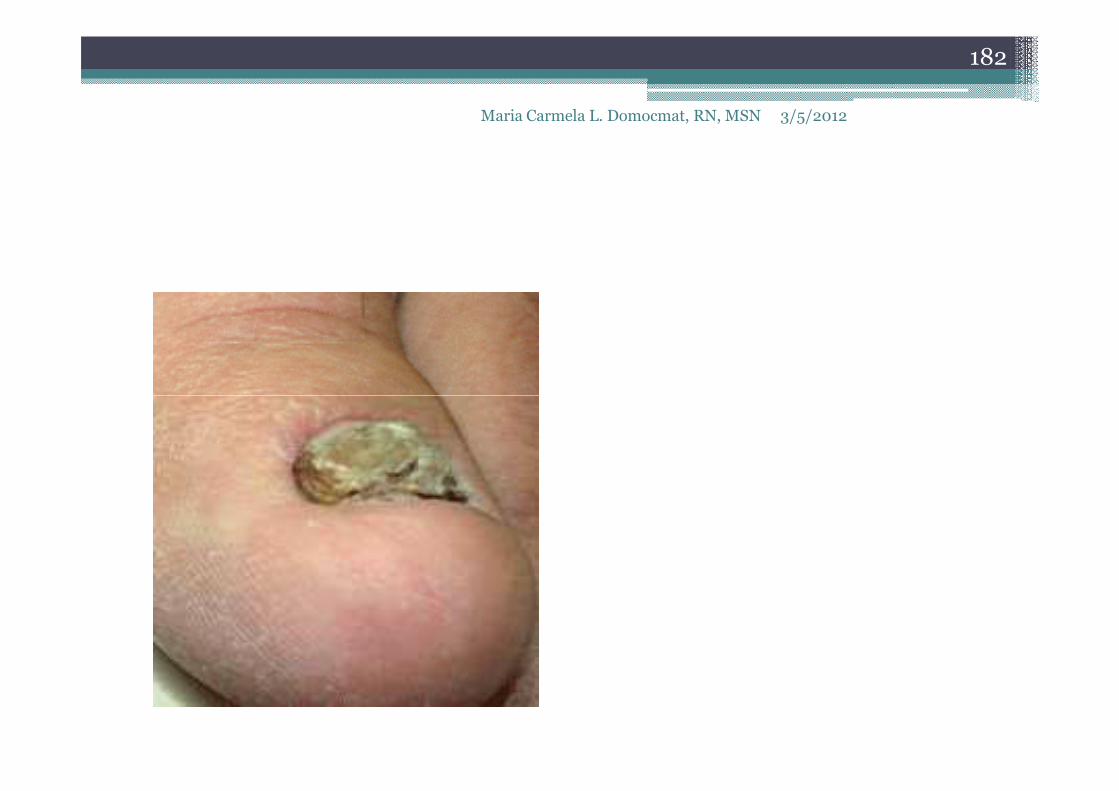
Hypertrophic Ungual Labium
• chronic hypertrophy of nail lip
• caused by improper nail trimming
• results from untreated ingrown toenail
3/5/2012Maria Carmela L. Domocmat, RN, MSN
181
• results from untreated ingrown toenail
• treatment:
o surgical removal of necrotic nail and skin
o treatment of secondary infection
3/5/2012Maria Carmela L. Domocmat, RN, MSN
182

References
• Krug RJ, Lee EH, Dugan S, Mashey K. Hammer toe. In: Frontera WR, Silver JK, Rizzo TD Jr., eds. Essentials of Physical Medicine and
3/5/2012
183
Maria Carmela L. Domocmat, RN, MSN
eds. Essentials of Physical Medicine and Rehabilitation. 2nd ed. Philadelphia, Pa: Saunders Elsevier;2008:chap 82.
• http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0002215/
References
• Ignatavicius and Workman (2006). Medical surgical nursing [5th ed]. Singapore: Elsevier.
• http://www.epodiatry.com/corns-callus.htm
3/5/2012Maria Carmela L. Domocmat, RN, MSN
184
• http://www.epodiatry.com/corns-callus.htm
• http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0004438/
• http://www.bupa.co.uk/individuals/health-information/directory/c/corns
• http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0002217/
• http://orthoinfo.aaos.org/topic.cfm?topic=a00154
Top Related