







Languages
Pages
Legal

1
Movement System Impairment Syndromes of the Lumbar Spine
Shirley Sahrmann, PT, PhD, FAPTAProfessor Emerita
Program in Physical Therapy
Program in Physical Therapy
Purposes
• Importance of promoting the movement system• Describe how movement induces/exacerbates
lumbar pain conditions• The Importance of emphasizing the role of
movement in the patient’s condition.• Movement as a cause, exacerbator, treatment, prevention
• Discuss Movement system impairment diagnoses of lumbar spine,
• Diagnostic labels are essential • Diagnoses increase efficiency and can reduce treatment variability
• Demonstrate an examination of subject with back pain
Program in Physical Therapy
Why the Movement System?• The goal of physical therapy is to • Regain or Improve Movement for function, health,
prevention• Requires being movement and exercise experts and able to
optimize movement, • Need to consider all aspects of major component systems
• Musculoskeletal = biomechanics – muscle physiology – skeletal physiology
• Nervous = biocontrol – biobehavioral (psychosocial) - biomechanics • Activation patterns = interaction of muscle adaptions & motor learning
with gravity as major influence
• Cardiovascular, pulmonary, endocrine = bioenergetics
Program in Physical Therapy
THE KINESIOPATHOLOGICMODEL A THEORETICAL CONSTRUCT OF THE MOVEMENT SYSTEM HOW MOVEMENT IS CAUSE AND EXACERBATOR OF PATHOLOGY
THUS HOW PHYSICAL THERAPY CAN TREAT CAUSE
APTA "THE INTEGRATION OF BODY SYSTEMS THAT
GENERATE AND MAINTAIN MOVEMENT AT ALL LEVELS OF BODILY FUNCTION”
Program in Physical Therapy
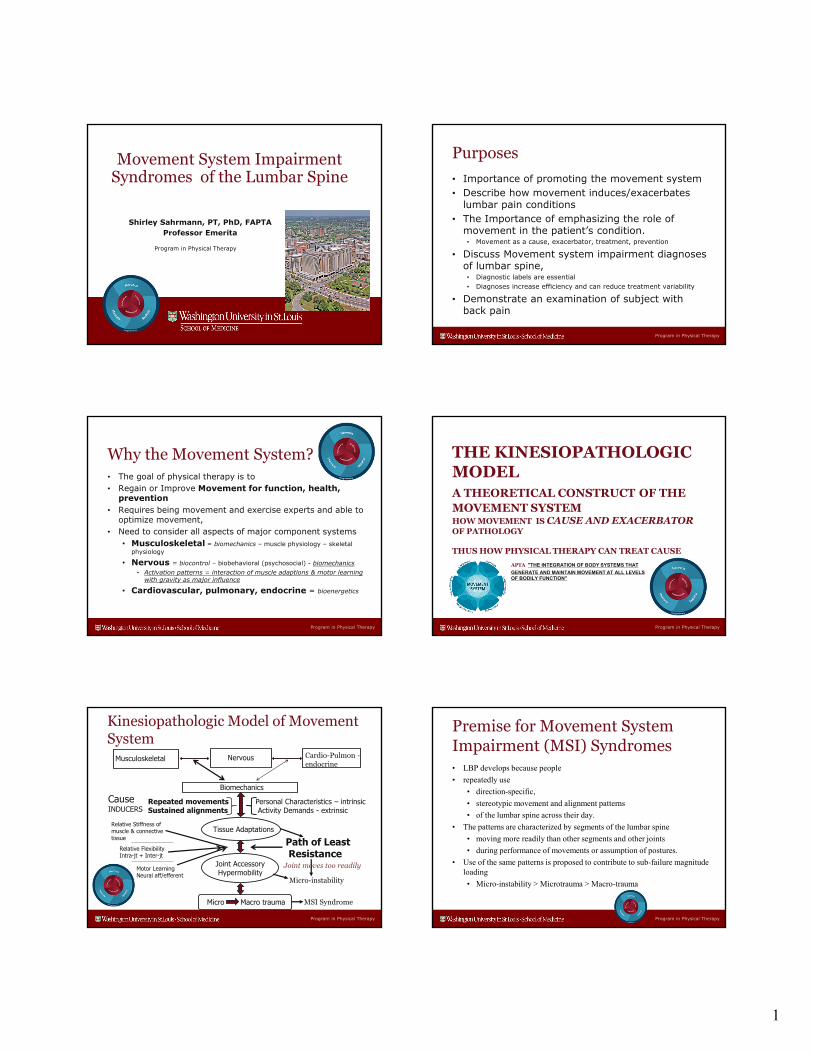
Kinesiopathologic Model of Movement System
Musculoskeletal Nervous
Biomechanics
Repeated movementsSustained alignments
CauseINDUCERS
Personal Characteristics – intrinsicActivity Demands - extrinsic
Tissue Adaptations
Joint AccessoryHypermobility
Relative Stiffness of muscle & connective tissue
Relative FlexibilityIntra-jt + Inter-jt
Micro Macro trauma
Path of Least Resistance
Cardio-Pulmon -endocrine
Motor LearningNeural aff/efferent
Micro-instability
MSI Syndrome
Joint moves too readily
Program in Physical Therapy
Premise for Movement System Impairment (MSI) Syndromes • LBP develops because people
• repeatedly use
• direction-specific,
• stereotypic movement and alignment patterns
• of the lumbar spine across their day.
• The patterns are characterized by segments of the lumbar spine
• moving more readily than other segments and other joints
• during performance of movements or assumption of postures.
• Use of the same patterns is proposed to contribute to sub-failure magnitude loading
• Micro-instability > Microtrauma > Macro-trauma
2
Program in Physical Therapy
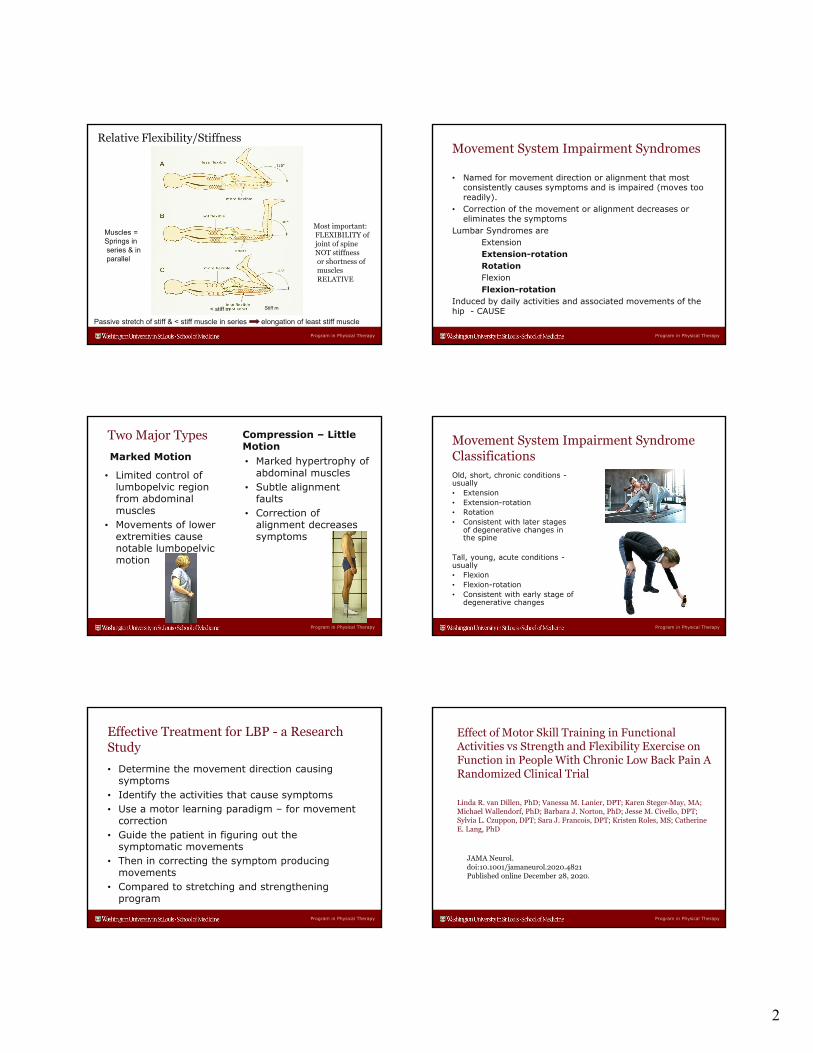
Muscles =Springs in series & inparallel
Passive stretch of stiff & < stiff muscle in series elongation of least stiff muscle
Stiff m< stiff m
Most important:FLEXIBILITY ofjoint of spineNOT stiffnessor shortness ofmusclesRELATIVE
Relative Flexibility/Stiffness
Program in Physical Therapy
Movement System Impairment Syndromes
• Named for movement direction or alignment that most consistently causes symptoms and is impaired (moves too readily).
• Correction of the movement or alignment decreases or eliminates the symptoms
Lumbar Syndromes areExtension Extension-rotationRotationFlexionFlexion-rotation
Induced by daily activities and associated movements of the hip - CAUSE
Program in Physical Therapy
Two Major Types
Marked Motion
• Limited control of lumbopelvic region from abdominal muscles
• Movements of lower extremities cause notable lumbopelvic motion
Compression – Little Motion• Marked hypertrophy of
abdominal muscles• Subtle alignment
faults• Correction of
alignment decreases symptoms
Program in Physical Therapy
Movement System Impairment SyndromeClassificationsOld, short, chronic conditions -usually• Extension• Extension-rotation• Rotation• Consistent with later stages
of degenerative changes in the spine
Tall, young, acute conditions -usually• Flexion• Flexion-rotation• Consistent with early stage of
degenerative changes
Program in Physical Therapy
Effective Treatment for LBP - a Research Study
• Determine the movement direction causing symptoms
• Identify the activities that cause symptoms• Use a motor learning paradigm – for movement
correction• Guide the patient in figuring out the
symptomatic movements• Then in correcting the symptom producing
movements • Compared to stretching and strengthening
program
Program in Physical Therapy
Effect of Motor Skill Training in Functional Activities vs Strength and Flexibility Exercise on Function in People With Chronic Low Back Pain A Randomized Clinical Trial
Linda R. van Dillen, PhD; Vanessa M. Lanier, DPT; Karen Steger-May, MA; Michael Wallendorf, PhD; Barbara J. Norton, PhD; Jesse M. Civello, DPT; Sylvia L. Czuppon, DPT; Sara J. Francois, DPT; Kristen Roles, MS; Catherine E. Lang, PhD
JAMA Neurol. doi:10.1001/jamaneurol.2020.4821 Published online December 28, 2020.
3
Program in Physical Therapy
Van Dillen et al. JAMA, Neurolo12-2020
Treatment once a week for 6 weeksSystematic increase in treatment program
Program in Physical Therapy
Use of MST appeared to
(1) result in improved short‐term but more importantly long termOutcomes with only 6 one‐hour treatments,
(2) Promote better adherence to training for a prolonged period, and
(3) enable a person to practice the activities across the day, thus providing a means of self‐management. Such benefits could be key in a condition typically characterized by a clinical course of recurrent, fluctuating, or persistent functional limitation and pain.
Requirements for Implementation
(1) Classify the patients according to movement direction or alignment causing symptoms
(2) Guide the patient using motor learning principles in recognizing the offending movements or alignments associated with daily activities
(3) Guide the patient in learning to correct the offending movements and alignments with suitable practice of daily activities
Program in Physical Therapy
REPEATED MOVEMENTSSUSTAINED ALIGNMENTSOF DAILY ACTIVITIES
Examples: Walking and Hip motions affecting the spineSleeping alignment
Program in Physical Therapy
EXTENSION EXTENSION - ROTATION
Program in Physical Therapy
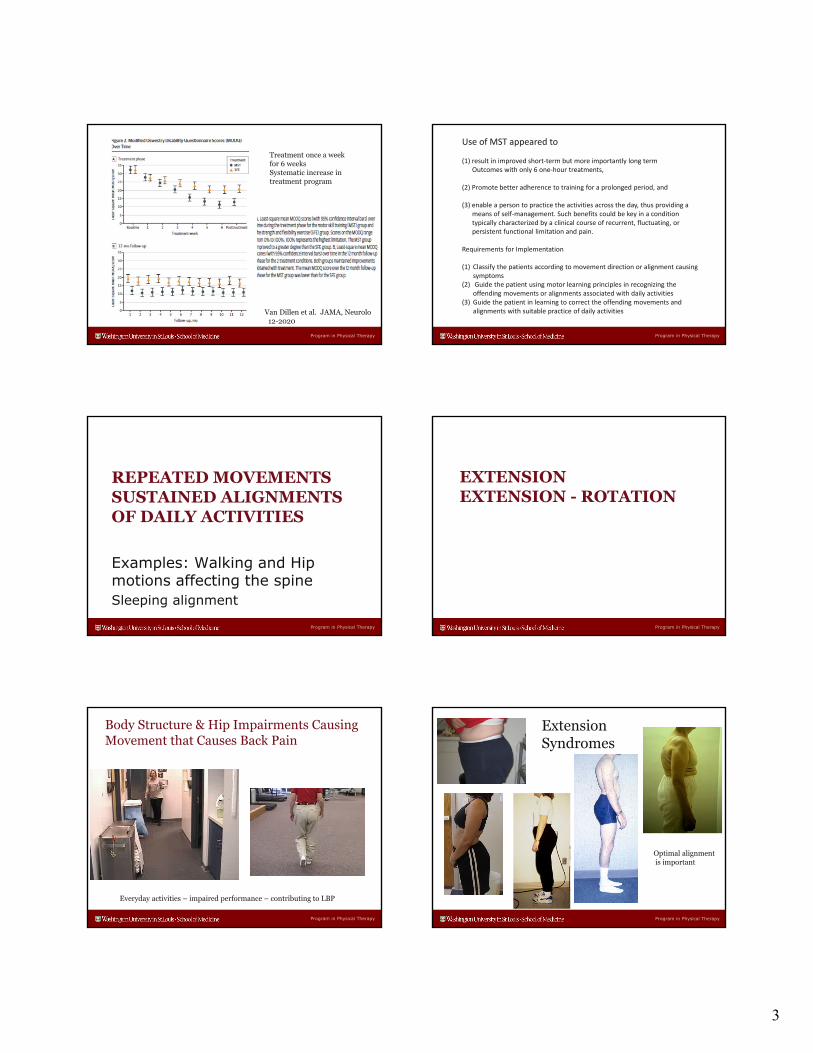
Body Structure & Hip Impairments Causing Movement that Causes Back Pain
Everyday activities – impaired performance – contributing to LBP
Program in Physical Therapy
Extension Syndromes
Optimal alignmentis important

4
Program in Physical Therapy
Gymnast with Low Back Pain –Correction Eliminates Pain - Extension Syndrome
Program in Physical Therapy
Movement Pattern used with this AlignmentReturn From Forward Bending
Hip extension Back extension Ankle sway
Program in Physical Therapy
Extension Syndrome - Short Hip Flexor Muscles
Program in Physical Therapy
Extension Syndrome - Short Hip Flexors
Program in Physical Therapy
Hip extensor muscles more flexible than Back extensor muscles
Extension Syndrome - Hypermobility
Back extensorsare cause of anteriorpelvic tilt
Program in Physical Therapy
FLEXIONFLEXION - ROTATION

5
Program in Physical Therapy
Flexion Syndrome - UltramarathonistFAI - Stiffness of Hip Extensors and of
Abdominal Muscles (compression)
Program in Physical Therapy
Lordotic?
Excessive flexion
Flexion Moment
Flexion Syndrome – student/diverTall – sit-up exercises (psoas flexing lumbar spine)
Hip extensors not short Relative stiffness: abdominals > back ext
Program in Physical Therapy
Case Presentation – Lumbar Flexion 64 yo
Program in Physical Therapy
Spinal Flexion and Rotation
DDD of entire lumbar spine: Having chronic pain and acute episodes
Program in Physical Therapy
Quadruped Alignment
Doing all the wrong exercises
Program in Physical Therapy
Immediate Change Post Quadruped Rocking Backward
Pre Immediate Post

6
Program in Physical Therapy
ROTATION SYNDROME
Two subclassifications:
Primary – lumbar spine is rotated (easier if flat or flexed) and is the pain generation site
Secondary – usually lower thoracic and high lumbar are rotated (fixed) pain generation is lower lumbar site -Moves more because other lumbar segments are not
moving
Program in Physical Therapy
PRIMARY ROTATION
Rotation of lumbar spine is site of pain (primary site)Rotation must be corrected
Program in Physical Therapy
LBP in standing. Lumbar side bend to right with shift of trunk to left.
Primary Rotation Syndrome –Radiculopathy – scheduled for surgery
Played ice hockey
Program in Physical Therapy
Rotated Spine – flexion/rotation increases when rocking backward
Hip flexion limited – Cam hip impingement
Program in Physical Therapy
Treatment Effect
Before Post quadruped rocking
Program in Physical Therapy
Quadruped – Instant Effects

7
Program in Physical Therapy
Modified Quadruped
Program in Physical Therapy
SECONDARY ROTATION SYNDROME
The examination
Program in Physical Therapy
Alignment – low thoracic/high lumbar right rotation
Program in Physical Therapy
Rotation – to right > to left
Hands out drugtrays to right
Program in Physical Therapy
Hip Lateral Rotation/Abduction –lumbopelvic rotation
Wide hips –in sidebend when on side
Program in Physical Therapy
Passive Knee Flexion – lumbopelvic rotation

8
Program in Physical Therapy
Hip Rotation – lumbopelvic rotation
Program in Physical Therapy
Comments
• Correction of the movement impairment during daily activities –
• corrects the impaired muscle adaptions and the relative flexibility
Program in Physical Therapy
Examination• Movement tests –
• Primary =preferred • Secondary = corrected• Note symptoms and movement if impaired
• Positions – standing, supine, side-lying, prone, quadruped, sitting, sit to stand, gait
• Most important is symptoms in a position or during a movement and change in symptoms with correction
• Alignment• Anterior pelvic tilt flex hips, lateral pelvic tilt – abduct hips,
overdeveloped abdominal muscles – lift trunk, take deep breath
• Forward bending, return, side-bending, rotation • All motions used during day with activity
Program in Physical Therapy
Examination 2 Need to Knows• Supine – need to knows
• Femoral ante or retroversion, femoroacetabular impingement• Log roll, hip flexion• Active hip/knee flexion
• Sidelying• Getting to position • In position (primarily women) – side bending, because of
width of pelvis/hips
• Prone • Getting to position• In position• Effect on pelvis of passive knee flexion and hip rotation
• Quadruped • Getting to position • In position – preferred alignment
Program in Physical Therapy
Examination 3
• Sitting • Symptoms – slumped, extended• Knee extension – effect on lumbar spine• Sit to stand and reverse - symptoms
• Gait• Symptoms – what phase of gait• Lumbopelvic rotation or anterior pelvic tilt
• Stairs • Symptoms – what phase?
Program in Physical Therapy
EVIDENCE FOR CLASSIFICATION
AND
KINESIOPATHOLOGICMODEL

9
Program in Physical Therapy
Evidence from Clinical Studies
To develop evidence – for classification and the model The following were accomplished• Inter-rater reliability of exam items • Inter-rater reliability of classification• Validity of classification based on exam • Daily Activities causes symptoms• Movements of the spine and of the limbs that cause low
back symptoms, when spine movement is prevented symptoms are reduced or eliminated
• Earlier & greater (fractions of seconds, few degrees) movements of spine in LBP than No LBP with LE motion
• Spine patterns are generalized across activities• Treatment effectiveness
Program in Physical Therapy
Validity of Classifications• Subgroup names describe the directions of lumbar
movements and alignments considered to be contributing to the LBP condition
• A number of studies have been conducted to test aspects of the validity of the proposed subgroups
Van Dillen LR et al, JOSPT, 2003; 33(3):126-142Norton BJ et al, JOSPT, 2004; 84(3):524-553Van Dillen LR et al, APMR, 2007; 88(3):351-360Gombatto SP et al, Phys Ther, 2007; 87(4):441-454Scholtes SA et al, Clin Biomech, 2009; 24(1):7-12Hoffman SL et al, PMR, 2010; 2(10):1113-1118Hoffman SL et al, Man Ther, 2011; 16(4):344-350Hoffman SL et al, Man Ther, 2012; 17(2):157-163Gombatto SP et al, Clin Biomech, 2006; 21(3):263-71
Program in Physical Therapy
Reliability of Exam and Validity of Classification• Reliability of physical examination items used for classification of patients
with low back pain.• Van Dillen LR, et al. Phys Ther. 1998 Sep;78(9):979-88.
• Movement system impairment-based categories for low back pain: stage 1 validation.
• Van Dillen LR, et al. J Orthop Sports Phys Ther. 2003 Mar;33(3):126-42.
• Reliability of novice raters in using the movement system impairment approach to classify people with low back pain.
• Henry SM, et al. Man Ther. 2013 Feb;18(1):35-40
• The inter-tester reliability of physical therapists classifying low back pain problems based on the movement system impairment classification system.
• Harris-Hayes, et al. PM&R. 2009 Feb;12:117-26.
• Differences in measurements of lumbar curvature related to gender and low back pain.
• Norton BJ, et. al. J Orthop Sports Phys Ther. 2004 Sep;34(9):524-34.• Luomajoki H et al, BMC Musc Dis, 2007; 8:90-101• Roussell NA et al., Man Ther, 2009; 14(6):630-635
Program in Physical Therapy
Inter-rater Reliability of Classification
• Reliability to classify is clinically acceptable• Experienced clinicians: % agreement: 78, kappa = .57
(1 study)
• Novice clinicians: average % agreement: 81 ± 4.56, average kappa = .74 ±.08 (5 studies)
Norton BJ et al., JOSPT, 2004; 34(9):524-533Trudelle-Jackson et al, JOSPT, 2008; 38(6):371-376Harris-Hayes et al, PMR, 2009; 24(1):117-126Henry SM et al, Man Ther, 2012; 92(2):136-142Kim MH et al, J Elec Kines, 2013; 23:387-393Henry SM et al, Man Ther, 2013;18(1):35-40
Program in Physical Therapy
Correction of Symptom Producing Movement Reduces or Eliminates Symptoms
Determine relationship of movement and alignment patterns to symptom behavior
• Primary tests: Patient’s preferred strategy (symptoms and direction of movement or alignment observed)
• Secondary tests: Systematic modification of patient’s specific movement or alignment pattern
• Goal: Determine effect of secondary test on symptoms compared to symptoms with primary test
Van Dillen LR et al, APMR, 2003; 84(3):313-22Van Dillen LR et al, Man Ther, 2009; 14:52-60
Program in Physical Therapy
EVIDENCE FOR DAILY ACTIVITIES AS CAUSE
Keep spine still during performance of basic mobility activities – Performance Training

10
Program in Physical Therapy
Randomized Control Study –Low Back Pain100 patients – Van Dillen
• All classified into Movement System Impairment syndrome categories
• Group 1 – category specific exercise; keep neutral spine during functional activities
• Group 2 – general exercise – keep neutral spine
• In PT – 1x / week for 6 weeks – programs carefully progressed
Manual Therapy, Volume 24, 2016, 52–64
Program in Physical Therapy
Modified Oswestry Score % - both groups same
20
15
1012
INITIAL VISIT POST TX 6 MONTHS 12 MONTHS
Series 1
Modified from Van Dillen LR Manual Therapy 24;2016 52 - 64
Program in Physical Therapy
Adherence toPerformance Training & Exercise
8075
52
41
80 80 7870
INITIAL POST TX 6 MONTHS 12 MONTHS
Exercise
Performance Training
Modified from Van Dillen LR Manual Therapy 24;2016 52 - 64
Program in Physical Therapy
EVIDENCE FOR LUMBAR SPINE MOVING READILY DURING LOWER EXTREMITY MOTION
Low back pain subjects that played rotational sports –
Motion Capture In prone with Active Knee Flexion & Hip Rotation
Program in Physical Therapy
Timing Difference with Knee Flexion Test in Prone
Scholtes et al., Clin Biomech, 2009
Onset of lumbopelvic motion after onset of knee flexion.
Program in Physical Therapy
Timing Difference with Hip Lateral Rotation Test
Scholtes et al., Clin Biomech, 2009

11
Program in Physical Therapy
Repeated Movements & Sustained Alignments• Chimenti RL, Scholtes SA, Van Dillen LR. Activity characteristics and
movement patterns in people with and people without low back pain who participate in rotation-related sports. J Sport Rehabil. 2013
• Harris-Hayes M, Sahrmann SA, Van Dillen LR. Relationship between the hip and low back pain in athletes who participate in rotation-related sports. J Sport Rehabil. 2009 Feb;18(1):60-75. Review.
• Weyrauch SA, Bohall SC, Sorensen CJ, Van Dillen LR. Association between rotation-related impairments and activity type in people with and without low back pain. Arch Phys Med Rehabil. 2015
• Sorensen CJ, Johnson MB, Callaghan JP, George SZ, Van Dillen LR. Validity of a Paradigm for Low Back Pain Symptom Development During Prolonged Standing. Clin J Pain. 2015
Program in Physical Therapy
Standing for 2 Hours Induced Back Pain
• Pain develops in 28 – 42% of subjects• Pain characteristics are the same as in people with back
pain• Have greater lumbar curve than non-pain developers• Pain developers have earlier lateral pelvic tilt with left hip
abduction in sidelying, than non pain developers
Sorensen CJ et. al., Clin J Pain. 2015
Program in Physical Therapy
EVIDENCE FOR GENERALIZATION OF LUMBAR MOVEMENT PATTERN
Picking up an Object from Different Placements
Program in Physical Therapy
Early Lumbar Excursion (deg)
4
7
8
8.5
9.5
4
9
9
9.5
9.5
7
14
12
13.5
16
0 5 10 15 20
HIGH
STANDARD
FAR
LOW
LOW FAR
Chart Title
LBP-high LBP-Low back health
significant
Back pain low < 20 OswestryBack pain high > 20 Marich et al Clinical Biomechanics 2017
Adapted from
Program in Physical Therapy
One Session of Motor Skill Training to Prevent Early Lumbar Flexion Marich et al PTJ 2018
0
2
4
6
8
10
12
BackHealthy LBP Mot skill train
Early Lumbar Flexion during Pick Up an Object
91% no longerhad LBP with correction offorward bending
Degrees of Lumbar Flexion
Program in Physical Therapy
Summary• Relative (which muscles) stiffness of the hip muscles can
contribute to increasing the relative (which direction) flexibility of the lumbar spine
• The flexibility is evident in the early movement of the spine• Elicited by movement of the hips or trunk• The movement becomes the path of least resistance and
thus occurs during daily activities• Instruction in the movement direction causing the
symptoms and learning how to correct the movement is effective treatment
• Supports the proposal that the way daily activities are performed is the cause of the problem
Top Related