






Languages
Pages
Legal

MICR 420
Emerging and Re-EmergingInfectious Diseases
Lecture 7:C. trachomatis
Dr. Nancy McQueen & Dr. Edith Porter
Overview C. trachomatis The genus Chlamydia
Morphology Growth and metabolic
characteristics Virulence factors Diseases Diagnosis
Direct antigen test Culture PCR Immune response
Therapy Threats:
Apparently under control
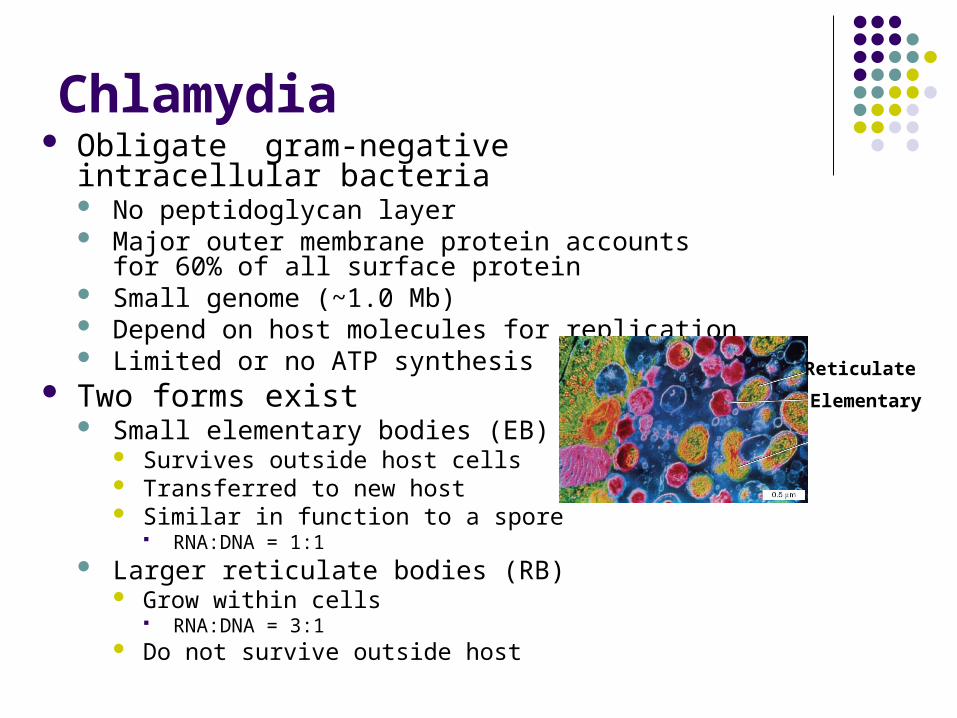
Chlamydia Obligate gram-negative intracellular bacteria
No peptidoglycan layer Major outer membrane protein accounts for 60% of
all surface protein Small genome (~1.0 Mb) Depend on host molecules for replication Limited or no ATP synthesis
Two forms exist Small elementary bodies (EB)
Survives outside host cells Transferred to new host Similar in function to a spore
RNA:DNA = 1:1 Larger reticulate bodies (RB)
Grow within cells RNA:DNA = 3:1
Do not survive outside host
Elementary
Reticulate

Chlamydia Developmental Cycle
48h – 72h
Persistent Forms
EB attach to epithelial host cell Endocytosis Prevention of fusion with
lysosome Development into RB RB proliferation, formation of
large inclusion bodies Visible in light microscope
Development into EB Rupture of host cell and
release of EB
Chlamydia Species C. pneumoniae
World wide ~ 10% of pneumonias and 5% of all
bronchitis cases C. psittaci
Psittacosis Zoonotic pneumonia Inhalation of droppings from infected
birds Category B biological weapon
C. trachomatis Various serotypes
Eye infections STI

Inclusion conjunctivitis Transmitted to newborn's eyes during passage
through the birth canal Preventive erythromycin
Spread through swimming pool water Treated with tetracycline
Trachoma Greatest cause of blindness worldwide
Chlamydia Infection of the Eyes
Trachoma World wide ~ 80 (150?) million people infected and
~ 6 million blind Mostly in developing countries 3% of cause of all blindness world wide
Transmitted eye-hand-eye, eye-fomite-eye, flies Infection occurs usually during childhood Chronic follicular conjunctivitis inversion of
eyelashes irritation of cornea corneal ulcerations, scarring vision loss typically at age 30 – 40
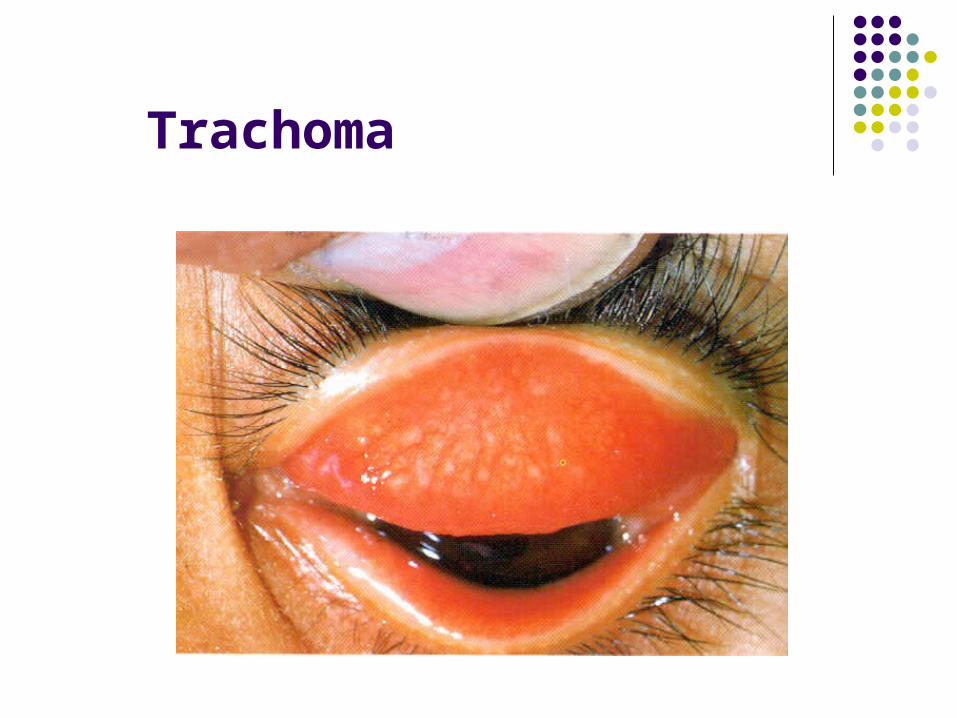
Trachoma

Histopathology of Trachoma
http://www.lenntech.com/images/Water%20Borne%20Diseases/Trachoma.jpg

Simplified WHO System to Assess Trachoma
(from Matthew J. Burton, British Medical Bulletin, 2007)
Grade Description
TF Trachomatous inflammation—Follicular: The presence of five or more follicles (>0.5 mm) in the upper tarsal conjunctiva
TI Trachomatous inflammation—Intense: Pronounced inflammatory thickening of the tarsal conjunctiva that obscures more than half of the deep normal vessels
TS Trachomatous scarring: The presence of scarring in the tarsal conjunctiva
TT Trachomatous trichiasis: At least one lash rubs on the eyeball
CO Corneal opacity: Easily visible corneal opacity over the pupil
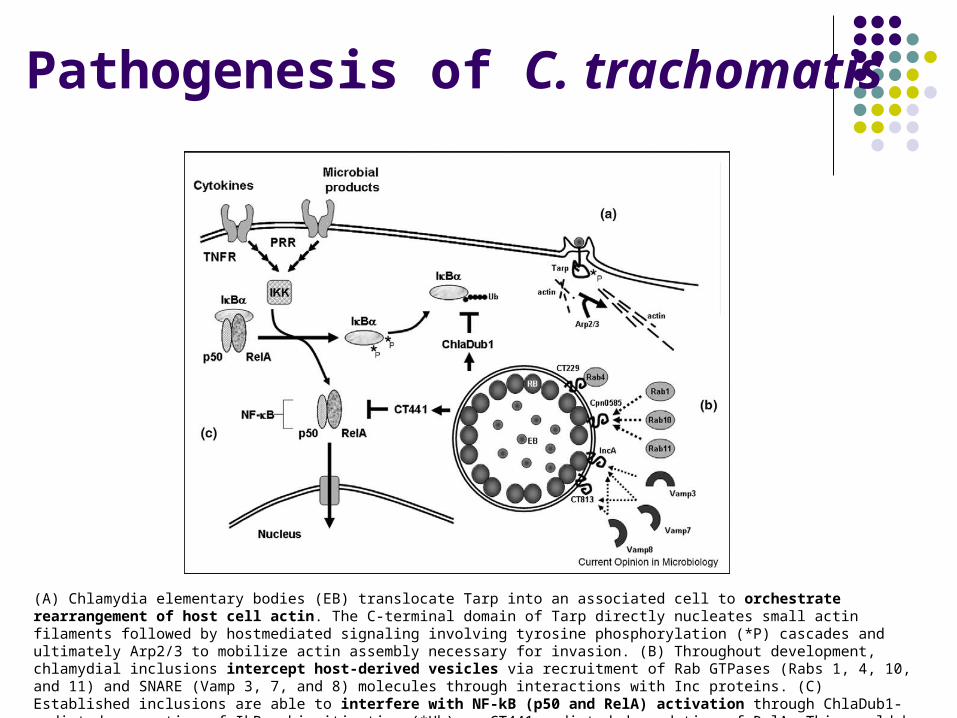
Pathogenesis of C. trachomatis
(A) Chlamydia elementary bodies (EB) translocate Tarp into an associated cell to orchestrate rearrangement of host cell actin. The C-terminal domain of Tarp directly nucleates small actin filaments followed by hostmediated signaling involving tyrosine phosphorylation (*P) cascades and ultimately Arp2/3 to mobilize actin assembly necessary for invasion. (B) Throughout development, chlamydial inclusions intercept host-derived vesicles via recruitment of Rab GTPases (Rabs 1, 4, 10, and 11) and SNARE (Vamp 3, 7, and 8) molecules through interactions with Inc proteins. (C) Established inclusions are able to interfere with NF-kB (p50 and RelA) activation through ChlaDub1-mediated prevention of IkBa ubiquitination (*Ub) or CT441-mediated degradation of RelA. This would be predicted to interfere with proinflammatory signals originating from ligand binding to TNF family (TNFR) or pattern recognition (PRR) receptors.

Virulence Factors of C. trachomatis (CT)
Contribute to intracellular survival and proliferation In part secreted via Type III secretion apparatus Tarp (Translocated actin recruiting phosphoprotein):
effects actin rearrangement and endocytic uptake of CT
CT inserts proteins (Inc and others) in inclusion (endosome) membrane that prevent fusion of host lysosomes
CT releases proteins (ChlaDub1, CT441) into the cytoplasma that interfere with NFB signal transduction, a key pathway of the acute inflammatory and innate immune response.
Immune Response to C. trachomatis
Not well understood Infection controlled by cell mediated immune
response However: contributes also to the scarring
Antibodies are formed Tear IgG actually enhance uptake Tear IgA appear to be protective
(Matthew J. Burton, British Medical Bulletin, 2007)
Diagnosis of Trachoma No “gold standard” test Direct antigen test PCR ELISA to measure patient antibodies against outer
membrane proteins, conserved heat shock proteins Culture
inoculating specimens onto cell culture monolayers Visualization of inclusion bodies after 48 – 72 h using
fluorescent labeled monoclonal antibodies against CT LPS or MOMP

Therapy and Prophylaxis of Trachoma Eyelid surgery Antibiotics to treat the infection
Tetracycline Azithromycin
Education about facial cleanliness and personal hygiene
Environmental improvements
WHO’s Global Alliance for the Elimination of Blinding Trachoma by
2020

Take Home Messages
Chlamydia are obligate intracellular bacteria that have a unique life cycle alternating between infectious elementary bodies and proliferative reticulate bodies.
Pathogenic factors include rearrangement of cytoskeleton promoting uptake, inhibition of fusion of lysosomes with endosomes and inhibition of NfkB activation.
C. trachomatis serotypes A-C (-K) cause trachoma, a chronic conjunctivitis leading to blindness.
Trachoma is diagnosed by direct antigen and nucleic acid based test and treated with tetracyline and azithromycin.

Resources
http://www.who.int/topics/trachoma/en/ http://www.cdc.gov Textbooks
Microbiology: A clinical Approach (2010) Garland Science
Prescott’s Principles of Microbiology (2009) McGraw-Hill Microbiology: An Evolving Science (2009) Norton
Primary literature Betts et al., Current Opinion in Microbiology, 2009, 12:81–87 Matthew J. Burton, British Medical Bulletin, 2007
Top Related