





Languages
Pages
Legal


Unit 4Metabolism & Metabolic
Disease
Protein & Amino AcidMetabolism
Paul Anderson FALL 2008
Pathophysiology 101-823

Learning Objectives1. List the metabolic functions of proteins & amino acids.2. Explain the importance of protein in the human diet and define
INCOMPLETE PROTEIN, COMPLETE PROTEIN ESSENTIAL AMINO ACID: NON-ESSENTIAL AMINO ACID3. Define the AMINO ACID POOL.4. Define NITROGEN BALANCE and state under what conditions a
POSITIVE NITROGEN BALANCE and a NEGATIVE NITROGENBALANCE occur.
5. State the effects that the following hormones have on proteinmetabolism, naming the metabolic pathways affected.INSULIN, GLUCAGON, GROWTH HORMONE, GLUCOCORTICOIDS(CORTISOL), SEX HORMONES.THROXINE
6. Define each of the following pathways in protein metabolism andstate their importance.
TRANSAMINATION: OXIDATIVE DEAMINATION: UREABIOSYNTHESIS: PROTEIN SYNTHESIS: GLUCONEOGENESIS
7. State the importance of the interconversion of amino acids andintermediates of carbohydrate and lipid metabolism.
8. Distinguish between KETOGENIC and GLUCOGENIC amino acids.References: Porth, Essentials, Ch. 8 , p. 167: Ch. 29. pp 634-635: Ch. 32Porth, Pathophysiology, Ch. 11, p.220 Ch. 43 Martini, Essentials of A & P, Ch. 17

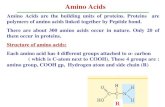
Metabolic Functions of Proteins & Amino Acids
Proteins have a variety of structures so have avariety of functions in the body.enzymes, many hormones, antibodies, hemoglobin,cytochromes, support (collagen), movement (actin,myosin)
Amino acids form hormones, neurotransmitters.Thyroxine, epinephrine, dopamine (from tyrosine)
Amino acids can be a source of energy.• Dietary proteins contain about the same amount of energy pergram as carbohydrates.
• the non-nitrogen part of amino acids can be oxidised directly incell respiration or after conversion to ketone bodies.
• Normally about 12% of our daily energy needs come fromamino acids.
• Excessive use of amino acids for energy causes a deficiency oftissue proteins and an excess of ketone bodies.

Dietary Protein, Amino Acid Pool &Metabolic Pathways
•Unlike carbohydrate or fat there is no specificstorage depot for proteins or amino acids.
•Instead the amino acid pool of the blood plasmaacts as a reservoir which each tissue can drawupon.
•Each tissue makes those specific proteins which itneeds, controlled by the active genes in that tissue.
•The liver is the major organ involved in proteinmetabolism especially for deamination, ureasynthesis and gluconeogenesis
A normal diet should contain•sufficient protein for metabolic needs•Complete proteins with 9 essential amino acidswhich the body cannot synthesize, e.g.phenylalanine. Most plant proteins are incomplete

Metabolic Pathways of Proteins & Amino Acids
Dietaryproteins
AMINO ACIDPOOL inplasma
amino acidproducts
α keto acidsNH3 urea
energy
glucoseketonebodies
cellularproteins
transaminationdeamination
gluconeogenesisExcretedin urine
ketogenesis

Nitrogen Balance
•Nitrogen balance means that N intake (dietaryprotein) = N output in urine (NH3, urea, uric acid)
•N balance is controlled by diet & hormones.•Normally hormones control proteinanabolism/catabolism to maintain N balance.
Dietaryproteins
AMINO ACIDPOOL
Tissueproteins
ProteinCatabolism
ProteinAnabolism
Catabolic HormonesGlucocorticoids
Anabolic HormonesGH (via IGF)Sex hormonesInsulinThyroxine (children)
Urinary N
GH: Growth HormoneIGF: Insulin like Growth factor

Nitrogen Imbalance
Nitrogen Imbalance means N intake does not equalN output.
•Positive N balance means N intake > N output withweight gain due to increased tissue protein stimulated byanabolic hormones. Occurs in: -normal growth
- Convalescence-Pregnancy
•Negative N balance means N output > N intake withweight loss due to tissue protein breakdown caused bydisease or lack of dietary protein. Occurs in- Starvation- Wasting diseases (cancer, paralysis)- Diabetes mellitus- Excess glucocorticoids (Cushing’s syndrome)

Protein & Amino Acid Anabolism
• PROTEIN SYNTHESIS occurs onribosomes in every cell and is stimulatedby Anabolic Hormones- Insulin-like Growth Factor(IGF)- Thyroxine (in growing children)- Insulin
- Estrogen & Testosterone• Weight-bearing exercise causes
anabolism & growth of muscle.
Non essential amino acids can be synthesized byTRANSAMINATION (transfer of an amino groupto a keto acid to create an amino acid).

Transamination
• TRANSAMINATION is the exchange of Rgroups between amino acids and keto acidsforming a new amino acid & keto acid.
• Transamination builds non essentialamino acids in cells by using a keto acid withthe desired R group.
R group of α keto acid becomes R group of new amino acid
R R R R

Protein Mobilisation & Deamination
• Protein Mobilisation is the widespread breakdownof proteins to amino acids is stimulated byglucocorticoids in starvation & in diabetes mellitus.
• Liver cells take in amino acids from the amino acid pooland convert glucogenic amino acids into glucose(gluconeogenesis) and ketogenic amino acids intoketo acids by deamination.
• Deamination prepares amino acids for catabolism byremoving the amino group (NH2) forming a keto acid.
• Keto acids produced by deamination ortransamination may be
- oxidised for energy (in the Krebs cycle)
- used in gluconeogenesis (glucogenic amino acids)- converted to acetyl CoA & ketone bodies (ketogenicamino acids) by ketogenesis: ketone bodies are thenreleased into the blood for oxidation by other tissues.

Proteins
AMINO ACID POOL in plasma
Glucogenicaminoacids
KrebsCycle
ProteinMobilisation
NH3Glucose
Gluconeogenesis
Tissue Cells
Aminoacids
Liver Cell
Ketoacids
BloodGlucose
Deamination
Aminoacids
Protein Mobilisation & Fate of Amino Acids
Ketonebodiesin blood
Ketonebodies
Ketogenesis

Deamination & Nitrogen Excretion
•When amino acids are no longer needed theyare deaminated by the liver and kidneysremoving NH2 and forming NH3 in the processof oxidative deamination.
•The keto acid may be used as a source ofenergy or for making glucose.
Amino acid
NH3
oxidativedeamination
Keto acid

Formation of Urea
.
• Ammonia produced by deamination is highly toxicto the brain.
• The liver detoxifies NH3. by converting it to ureaexcreted by the kidneys.
•In the UreaCycle NH3combines withCO2 to formurea.
•In advancedliver diseaseincreasedblood NH3causes mentaldisturbancesand coma.
Ammonia
UREA
UreaCycle
Urea Excreted by kidneys
Liver Cell

Martini EssentialsFigure 17-9
1
2
3
6
54
87
11
109
Ketonebodies
12
IdentifyPathways1 - 12
Summary of Metabolic Pathways
NH313
13
13
1

Answers for Metabolic Pathways
1. GLYCOLYSIS2. KREBS (TCA) CYCLE3. OXIDATIVE PHOSPHORYLATION4. GLYCOGENOLYSIS5. GLYCOGENESIS6. GLUCONEOGENESIS7. LIPOLYSIS (LIPID MOBILISATION)8. LIPOGENESIS9. PROTEIN HYDROLYSIS (PROTEIN MOBILISATION)10. PROTEIN SYNTHESIS11. BETA OXIDATION12. KETOGENESIS13. DEAMINATION
Top Related