







Languages
Pages
Legal


Medicare is as sustainable as we want it to be
Michael M Rachlis MD MSc FRCPC LLD (Hon)University of Toronto February 7, 2013
www.michaelrachlis.ca

Current received wisdom
• Health Care costs are wildly out of control• My fellow baby boomers and I will really
deep six Medicare as we get older• The only alternatives are to either cut real
services or use more private care and finance.
• We need an “adult conversation” to reduce our expectations and make us see the need for private involvement


What’s my story?
• Health Care costs are not “out of control”• The aging population won’t break the bank• Medicare was and is good public policy• Healthcare uses antiquated processes of delivery• The two key solutions are:– Complete the First Stage of Medicare– Implement the Second Stage of Medicare

Health Care costs are not out of control
But Health care hasn’t been starved either

19751978
19811984
19871990
19931996
19992002
20052008
2011 f / p
0
2
4
6
8
10
12
14Public Private Total
Canadian Health Care Costs as % of GDP
% GDP
Data from Canadian Institute for Health Information NHEX 2012

198119831985198719891991199319951997199920012003200520072009
2011 f / p
0%
1%
2%
3%
4%
5%
6%
7%
8%
9%
ONCAN
Provincial Government HC Exp as % of GDP
% GDP
Data from Canadian Institute for Health Information NHEX 2012

198119831985198719891991199319951997199920012003200520072009
2011 f / p
0%
2%
4%
6%
8%
10%
12%NS ON
AB CAN
Provincial Government HC Exp as % of GDP
% GDP
Data from Canadian Institute for Health Information NHEX 2012

1975
1977
1979
1981
1983
1985
1987
1989
1991
1993
1995
1997
1999
2001
2003
2005
2007
2009
2011
f / p
0%5%
10%15%20%25%30%35%40%45%50%
ON CAN
%ProgExp
Data from Canadian Institute for Health Information NHEX 2012
Provincial Government HC Expas share of Program Spending

19811983
19851987
19891991
19931995
19971999
20012003
20052007
2009
2011 f/p
0%
5%
10%
15%
20%
25%
Provincial Government Program Exp as % of GDP
% GDP
Data from Canadian Institute for Health Information NHEX 2012

1981
1983
1985
1987
1989
1991
1993
1995
1997
19
99
2001
20
03
2005
20
07
2009
20
11
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%Prov Fed Total
Canadian government Program Spending
% GDP
Data from: http://www.fin.gc.ca/frt-trf/2012/frt-trf-12-eng.asp

19811983
19851987
19891991
19931995
19971999
20012003
20052007
2009
2011 f/p
0%
5%
10%
15%
20%
25%
30%
35%NS ONAB CAN
Prov Gov Program Exp as % of GDP
% GDP
Data from Canadian Institute for Health Information NHEX 2012

1990–911992–931994–951996–971998–992000–012002–032004–052006–072008–092010–112012–13
- 200 400 600 800
1,000 1,200 1,400 1,600 1,800 2,000
ON GDP CAN GDP
Ontario and Canadian GDP
GDP$Bil
Data from Canadian Institute for Health Information NHEX 2012

1970197319761979198219851988199119941997 2000 2003 2006 2009
05
101520253035404550
CANUSG7 Avg
% GDP
Data from: Data from: http://www.fin.gc.ca/frt-trf/2012/frt-trf-12-eng.asp
Revenues as % of GDP

19911993
19951997
19992001
20032005
20072009
2011 0
10
20
30
40
50
60
Govt outlays as % GDP
% GDP
Data from: http://www.fin.gc.ca/frt-trf/2012/frt-trf-12-eng.asp
?

AUTBEL
CANDEN FIN FR
AGER ICE IRE ITA
KORNET NZ
NORSP
ASW
ESW
IUK
USA02468
101214161820
% GDP
Average
Health Care as % of GDP (2010 Data)
Data from: http://www.oecd.org/els/healthpoliciesanddata/oecdhealthdata2012-frequentlyrequesteddata.htmAll OECD countries included with 2010 data and GDP per capita > $30K US PPP (from http://en.wikipedia.org/wiki/List_of_OECD_countries_by_GDP_per_capita )

The aging population won’t kill Medicare
• Canada is aging and health costs increase with age• But aging of the population per se has had and will
have only a moderate impact on health expenditures
• Aging is like a glacier not a tsunami. We have lots of time to prepare and adapt our health system before we get swamped!– The elderly are healthier than ever– High performing health systems can hold costs while
enhancing quality of care for the frail elderly

Health costs are related to illness and Canadian seniors are
healthier than ever
19

Year
Disability
1984 1989 1994 1999 2004
NoDisability
73.8% 75.2% 76.8% 78.8% 81.0%
Light or Moderate
15.9% 14.8% 13.9% 13.3% 11.8%
SevereRequiring > 2.5 hrs personal care daily
10.3% 10.0% 9.2% 7.9% 7.2%
American prevalence of disabled elderly 1984 - 2004
Manton et al. PNAS. 2006:103(48):18734-9

2005-2010 2025-2030 2045-2050
Old Age Dependency Ratios
(OADRs)
0.28 0.41 0.53
Prospective Old Age Dependency Ratios
(POADRs)
0.19 0.23 0.27
Adult Disability Dependency Ratios
(ADDRs)0.11 0.12 0.12
Dependency of the elderly in wealthy countries
W Sanderson. Science. 2010;329:1287-8. Canada was not included

CANADA
NL PEI NS NB PQ ON MB SA AB BC YT NWT NT0.0%
0.5%
1.0%
1.5%
2.0%
2.5%
From Mackenzie and Rachlis 2010
Annual impact of Aging on health costs 2010-2036

“It is not the aging of our population that threatens to precipitate a financial crisis in health care, but a failure to examine and make appropriate changes to our health care system, especially patterns of utilization.”
Dr. William Dalziel. CMAJ. 1996;115:1584-6

Most of health care’s problems are due to antiquated, processes of care

After-Hours Care and Emergency Room Use
Percent
Difficulty getting after-hours care without going to the emergency room
Used emergency room in past two years
Source: 2011 Commonwealth Fund International Health Policy Survey of Sicker Adults in Eleven Countries.
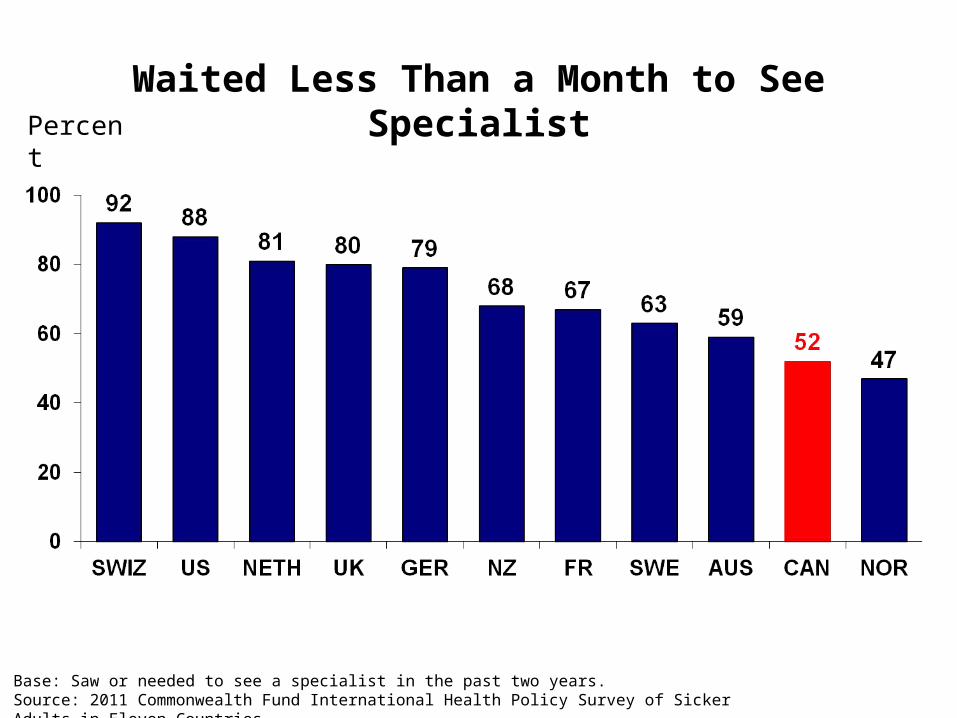
Waited Less Than a Month to See SpecialistPercent
Base: Saw or needed to see a specialist in the past two years.Source: 2011 Commonwealth Fund International Health Policy Survey of Sicker Adults in Eleven Countries.

Spine surgeons in Ontario: A wasted precious resource
• Only 10% of patients referred to a spine surgeon actually need surgery
• $24 million in unnecessary MRI scans
(http://www.theglobeandmail.com/news/opinions/editorials/spine-surgery-can-become-much-more-efficient/article2023173)

The three solutions are:
• Complete the First Stage of Medicare• Implement the Second Stage of
Medicare• Develop a healthier population
financed by fair taxation

Complete the First Stage of Medicare
• Medicare’s founders intended public coverage for pharmaceuticals, long term care, home care, and dental care
• Mainly private finance and for profit delivery for these sectors means higher costs, poorer quality, and needless suffering
• This would prevent cost shifting and “passive privatization”

There are affordable solutions to the delivery system’s apparently
intractable problems: The Second Stage of Medicare

We need to change the way we deliver services“Removing the financial barriers between the provider of health care and the recipient is a minor matter, a matter of law, a matter of taxation. The real problem is how do we reorganize the health delivery system. We have a health delivery system that is lamentably out of date.”
Tommy Douglas 1982

“I am concerned about Medicare – not its fundamental principles -- but with the problems we knew would arise. Those of us who talked about Medicare back in the 1940’s, the 1950’s and the 1960’s kept reminding the public there were two phases to Medicare. The first was to remove the financial barrier between those who provide health care services and those who need them. We pointed out repeatedly that this phase was the easiest of the problems we would confront.” Tommy Douglas 1979
Catching Medicare’s second stage

“The phase number two would be the much more difficult one and that was to alter our delivery system to reduce costs and put the emphasis on preventative medicine…. Canadians can be proud of Medicare, but what we have to apply ourselves to now is that we have not yet grappled seriously with the second phase.”
Tommy Douglas 1979

The Second Stage of Medicare is delivering
health services differently to keep people well

With few if any new resources, Canada’s health system could provide:
• Elective surgery within two months• Elective specialized care within one week• Same day access to one on our regular primary
health care providers – NOT a walk in clinic or ER!• A healthier population!

These improvements should be implemented in such a way that:• Empowers patients and families in their own
healthcare, in program planning, and in policy development and implementation
• Ensures that health care providers are available where patients need care
• Enhances the quality of worklife of providers• Strengthens communities• And, Improves Canada’s overall health status
and quality of life

Toronto Arthroplasty ModelCentral Intake
AssessmentAdvanced Practice Physio
SurgeonConsult
Surgery Post-Op Discharge Follow-Up
Referring Physician
Holland Centre
andToronto Western
Holland Centre
Holland Centre
Mt. Sinai
St. Michael’s
St. Joseph’s
Toronto East General
Toronto Western

Good News in Hamilton, Winnipeg, Nova Scotia, etc! We could have elective specialty input into patients’ care within 7 days
– The Hamilton Family Medicine Mental Health Program increased access for mental health patients by 1100% AND decreased psychiatry outpatients’ clinic referrals by 70%.
– The program staff includes 22 psychiatrists, 129 family physicians, 114 Nurses and Nurse Practitioners, 20 Registered Dietitians, 77 Mental Health Counsellors, 7 pharmacists and provides care to 250,000 patients

Good News in Cambridge, Cape Breton, Penticton, etc! We could access primary health care within 24 hrs
In Cambridge, Dr. Janet Samolczyk aims to see her patients WHEN they want to be seen including within 24 hours

New models of care for the elderly and those with serious chronic illness, show great potential for
improved quality

Step right up!Get your ELIXIR of Health Promotion! Reduce your risk of dying or ending up in a nursing home by over
40%!Increase your chances of staying in your own home by nearly
30%!N Hall et al. Canadian Journal on Aging. 1992;11(1):72-91

42
Get your community
services corrective right here!
They will reduce your health costs by
50% in 3 years!
http://www.hollanderanalytical.com/Hollander/Reports_files/preventivehomecarereport.pdf

Going for gold: Re-engineering services to immigrants in Toronto• Access Alliance works with immigrant and
refugee communities to identify women who are leaders and hires them as community health workers (CHWs)
• They are given 3 months of paid training and 3 year contracts
• The CHWs run educational workshops and facilitate well children and well women care
• CHWs have brought services to more than 12,000 women and their children
• 85% of CHWs get jobs in health or social services after their contracts are over
43

Denmark: A country of best practices
• 1987 moratorium on building new nursing home beds– Accompanied by giving all benefits of long term
care to home care clients– Scandinavian public responsibility for housing– Increased construction of supportive housing
• 1998 country-wide policy of home visits/assessments for people > 75– Provide health promotion and system linkages

Denmark: A country of best practices
• Denmark has 17.1% population > 65 while Canada has 15.9% > 65
• Total Health spending as share of GDP is about the same in Denmark (11.1%) as in Canada (11.4%) 2010 OECD data
• Public funding: Denmark 85% Canada 71%– Denmark has better public coverage for home
care, drugs, and appliances and devices

There is substantial evidence that for profit patient care tends
to cost more and is of poorer quality -- but the most salient argument is Tony Soprano’s:
“Fuhgetaboutit!”
We don’t need it.

Summary:
• Health Care costs are not “out of control”• The aging population won’t break the bank• Medicare was and is good public policy• Healthcare uses antiquated processes of delivery• The two key solutions are:– Complete the First Stage of Medicare– Implement the Second Stage of Medicare

Courage my Friends, it is
Not Too Late to Make a Better
World!
Tommy Douglas(paraphrasing
Tennyson)
Top Related