







Languages
Pages
Legal


Medical Management of Renal
Cell Carcinoma
Lin Mei, MD
Hematology-Oncology Fellow
Hematology, Oncology and Palliative Care
Virginia Commonwealth University

Educational Objectives
• Background of RCC (epidemiology, pathology and
stage)
• Management of metastatic RCC (new drugs and
mechanism)
• Controversy in adjuvant treatment in high risk advanced
RCC
• Cytoreductive nephrectomy mRCC in the era of targeted
therapy

Epidemiology

Histological Classification of RCC
BHD=Birt-Hogg-Dubé; FH=fumarate hydratase;
VHL=von Hippel-Lindau.
Modified from Linehan WM et al. J Urol. 2003;170:2163-2172.
RCC
Clear cell
75%
Type
Incidence (%)
Associated mutations
VHL
Papillary type 1
5%
c-Met
Papillary type 2
10%
FH
Chromophobe
5%
BHD
Oncocytoma
5%
BHD

AJCC Stage (2010)
Stage Description5-Year
Survival (%)
Stage I T1, N0, M0 95
Stage II T2, N0, M0 88
Stage III T1-2, N1 or T3, N0-1 59
Stage IVT4 (any N or M) or
N2 (any T or M) or M120

MSKCC Risk Factor Model in mRCC
0 risk factors (n=80 patients)
1 or 2 risk factors (n=269 patients)
3, 4, or 5 risk factors (n=88 patients)
Risk factors associated with worse prognosis
• KPS <80
• Low serum hemoglobin (13 g/dL/11.5 g/dL: M/F)
• High corrected calcium (10 mg/dL)
• High LDH (300 U/L)
• Time from Dx to IFN- <1 yr
Pro
po
rtio
n S
urv
ivin
g
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 2 1614131195436 151210876
Motzer RJ et al. J Clin Oncol. 2002;20:289-296.
MS:
20 mo
10 mo
4 mo
Time From Start of treatment (years)

Medical Management of mRCC

Treatment of mRCC

Historical treatment of mRCC
• Chemotherapy
– RCC is highly resistant, <10% ORR
• IFN-
– 15% ORR, but responses rarely complete or durable
• HD IL-2
– 15% ORR in stage IV patients, only 5% were CR
• Urgent need for additional options in late-stage RCC

Pathophysiology of RCC

VEGF Signaling Mechanisms
Antibodies to VEGF
or VEGFR
mTOR
inhibitorsTyrosine kinase inhibitors

VEGF Correlated With Poorer Survival
Jacobsen J, et al. BJU Int. 2004;93:297-302.

VEGF inhibitor (Bevacizumab)
• Bevacizumab as monotherapy is not curative
• Usual combined with other medications with
different mechanism of action (eg. IFN-)
• Side effects: Hypertension, proteinuria, impaired
wound healing, GI perforation
Sunitinib (Sutent®)
• Oral broad-spectrum multitarget TKI (VEGF, PDGF,
FLT3 and c-KIT)
• Dose: 50mg daily, 4 weeks on and 2 weeks off
• PFS (11 mos) and OS (26.4 mos) compared with IFN-
• 90% undergone nephrectomy with good- or
intermediate-risk
Motzer, et al. NEJM, 2007;356: 115-124.

Pazopanib (Votrient®)
• Similar kinase targets as sunitinib
• Dose: 800mg once daily
• Improved PFS and OS in both treatment-naïve and cytokine-
resistant patients
• Non-inferior to sunitinib (COMPARZ trial)
• Favorable: less fatigue, hand-foot syndrome, thrombocytopenia
• Side-effect: higher incident of transaminitis
Sternberg et al. JCO. 2010; 28:1061-1068Motzer et al. NEJM. 2013; 369: 722-731

Sorafenib (Nexavar®)
• Oral multikinase inhibitor (RAF, VEGF, PDGF, FLT3 and
c-KIT)
• Dose: 400mg twice daily
• 2nd line treatment (TARGET trial)
• 1st line treatment: in selected patients with stage IV RCC
(Category 2A, NCCN)
Ratain, et al. JCO, 2006;24: 2505-2512.

Temsirolimus (Torisel®)
• mTOR inhibitor
• Dose: 25mg IV once weekly
• ARCC trial: include 3 or more unfavorable prognostic
factors (high risk) patients
• Category 1 recommendation for 1st line treatment of
poor-risk patients
Hudes et al. NEJM. 2007; 356:2271-2281

Everolimus (Afinitor®)
• Oral mTOR inhibitor
• Dose: 10mg once daily (2nd line treatment)
• RECORD-1 trial: mRCC progressed on sunitinib,
sorafenib or both (First study to evaluate disease
progression on VEGFi)
• Side effect: Rash, mucositis, nausea, myelosuppression,
hyperglycemia, pneumonitis etc.
Motzer et al. Lancet. 2008; 372:449-456.

Axitinib (Inlyta®)
• Oral 2nd generation VEGF inhibitors (VEGF1-3)
• Dose: initiate with 5mg twice daily
• AXIS trial: compared with sorafenib in 2nd line setting
• NCCN: can be considered in 1st line treatment option
(Category 2A)
Rini et al. Lancet. 2011; 378:1931-1939

Cabozantinib (Cabometyx®)
• Oral multitarget TKI (VEGF, MET, AXL)
• Dose: 60mg once daily (2nd line treatment)
• METEOR trial: compared with everolimus, showed improved PFS
and OS
• Side effect: hypertension, diarrhea, fatigue.
• CABOSUN trial: evaluate intermediate- or poor-risk mRCC
compared with sunitinib in 1st line setting
Choueiri et al. NEJM. 2015; 373: 1814-1823Choueiri et al. JCO. 2017; 35: 591-597

Lenvatinib (Lenvima®)
• Oral multitarget TKI (VEGF, FGF)
• Dose: 18mg once daily (combined with everolimus) as 2nd line
treatment
• Phase II trial, lenvatinib alone or combined with everolimus,
compared with everolimus monotherapy
• NCCN: Category 1 for 2nd line treatment
Mozter et al. Lancet Oncol. 2015; 16: 1473-1482.

Combination therapy
• May improve response rate, however, result in increased
toxicity
• Failed to improve PFS
• RECORD-3 trial: support 1st line sunitinib followed by 2nd
line everolimus upon progression
Mozter et al. JCO. 2014; 32: 2765-2772.

Immune therapy

Nivolumab (Opdivo®)
• Monoclonal antibody against PD-1 receptor
• Dose: 240mg IV once every 2 weeks
• Checkmate 025 trial: 2nd line setting compared with everolimus with
improved OS
• Side effect: autoimmune reaction (rash, colitis, endocrinopathy,
hepatitis, pneumonitis)
Mozter et al. NEJM. 2015; 373: 1803-1813

Pathway and current drugs in mRCC

Decision-making strategy
Choueiri TK and Motzer RJ. NEJM. 2017; 376: 354-366.

Adjuvant therapy in high-risk RCC

Risk of recurrence
• Curative therapy is surgery
• Nephrectomy either radical or nephron-sparing
• 20% of these population eventually relapse
• Median time to relapse: 18 months, within 2-3 years after
surgery

High risk population
• Poor PS, obesity, weight loss, presence of symptoms,
paraneoplastic syndrome
• Leibovich score: tumor stage, reginal LN, tumor size, nuclear grade,
tumor necrosis
• SSIGN score (mayo clinic), Karakiewicz et al. UISS (UCLA system)
• Molecular test is controversial
Patel et al. CAHO. 2016; 14: 907-914

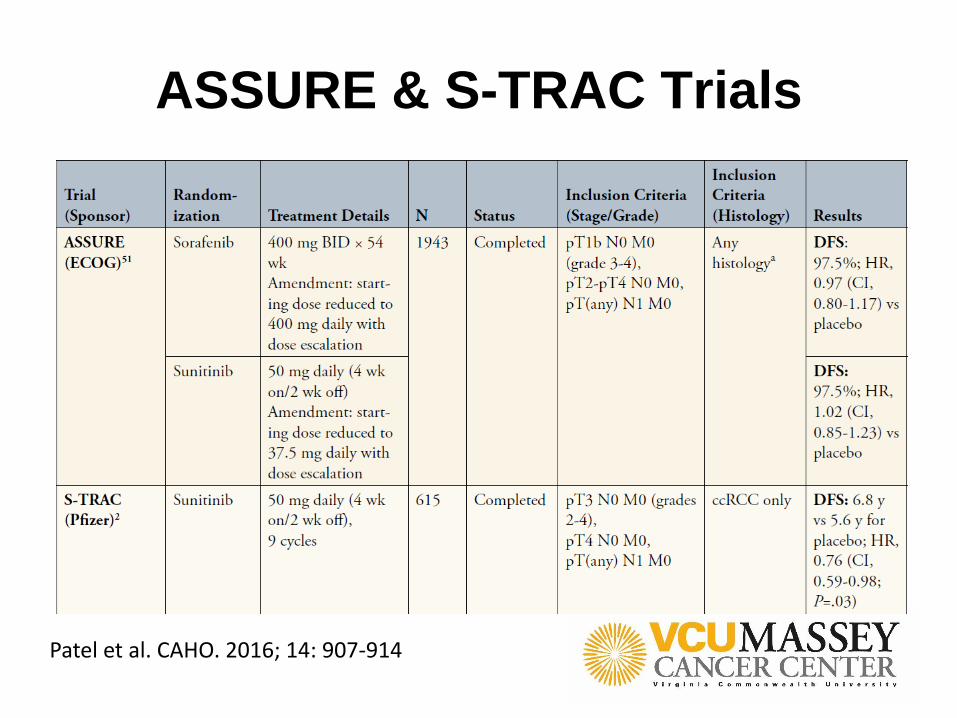
ASSURE & S-TRAC Trials
Patel et al. CAHO. 2016; 14: 907-914

Difference
S-TRAC ASSURE
Population Higher risk group (pT3-4) Greater than pT1b
Pathology Only clear cell All subtypes
Toxicity Better tolerance High dropout rate
Evaluation Central review No central review
Maturation Immature data (OS) Matured
Design DFS (primary endpoint)
OS (secondary endpoint)
DFS (primary endpoint)
Question May just delay time to
recurrence without
changing OS

Challenge in adjuvant treatment for RCC
• Population selection
• Revisit previous negative trials
• Molecular marker, oncogenomics
• Evaluation of newer agents and immune therapy

Cytoreductive nephrectomy in mRCC

History of cytoreductive nephrectomy (CN)
Flanigan et al. NEJM. 2001; 345: 1655 Mickisch et al. Lancet. 2001; 358: 966
SWOG 8949 EORTC 30947


CN in patients treated with VEGF therapy
Choueiri et al. J Urol. 2011; 185: 60-66

International mRCC database consortium
Heng et al. Eur Urol. 2014; 66: 704-710.

National Cancer Database Study
• Retrospective study with 15,390 with TT, 35% underwent CN between
2006 and 2013.
• Median OS (CN: 17.1 mos vs. non-CN: 7.7 mos)
Hanna et al. JCO. 2016; 34: 3267-3275
Summary
• CN before systemic therapy is recommended
• Patient selection is important
– Lung-only metastases
– Good PS and good prognostic feature
• Palliative nephrectomy
• Expected survival < 12 months based on risk factors is unlikely to be
benefited from CN

Thank you!
Top Related