







Languages
Pages
Legal


MACRA in 2018David HellerIndustry & Government Affairs

© Greenway Health, LLC. All rights reserved. Confidential and proprietary. Not for distribution except to authorized persons. 2
• Overview
• Assistance for small practices
• Reporting and scoring
• Advancing Care Information
• Quality
• Clinical Practice Improvement Activities
• Alternative Payment Models
Agenda

© Greenway Health, LLC. All rights reserved. Confidential and proprietary. Not for distribution except to authorized persons. 3
Adjusted Medicare Part B payment to clinician
MIPS Payment Adjustments
2022+
±4% for 2017’s performance
±5% for 2018’s performance
±7% for 2019’s performance
±9% for 2020’s performance and future years
• The potential maximum adjustment % will increase each year from 2019 to 2022.
Maximum adjustments
• Composite performance score, clinicians will receive +/- or neutral adjustments up to the percentages shown here.
Based on MIPS
2021
2020
2019

© Greenway Health, LLC. All rights reserved. Confidential and proprietary. Not for distribution except to authorized persons. 4
MACRA’s CY 2018 top takeaways: More flexibility for providers
More measures
and activities to choose from
New reporting options
The transition continues

Other notable impacts
21st Century Cures
Patients over paperwork
Meaningful measures
Extreme and uncontrollable circumstances

Overview

The HouseThe Senate
Bottom line
92 yeas
2 nays
392 yeas
37 nays
2 abstained
MACRA, MIPS, APMs are not going away
MACRA, by the votes

© Greenway Health, LLC. All rights reserved. Confidential and proprietary. Not for distribution except to authorized persons. 8
Provider flexibility
Interoperability
Physician burden a serious concern
Looking at possible
scaleback of MU, ACI
Support from both sides of the aisle
Measures cost and quality
It’s here to stay, with some tweaks possible
MACRA
8 I

What is MACRA?
MAC
RA
MIPS (standard)
MIPS (MIPS APMs)
Advanced APMs

Regulatory implementation
2019201820172016
• Final performance period for MU/PQRS/VBM.
• Payment year for 2014 performance period.
MACRA activities
• Payment year MU/PQRS/VBM (2015 performance).
• Final payment year for MU/PQRS/VBM (2016 performance)
• First MIPS performance period.
• Report on either ACI Transition Year (Modified Stage 2) objectives or ACI (Stage 3) objectives.
• 4 reporting options. • Must begin
reporting by Oct. 2.
• 2014 or 2015 CEHRT.
• Report on either ACI Transition Year (Modified Stage 2) objectives or ACI (Stage 3) objectives.
• May elect 90 day ACI/CPIA reporting period.
• Cost implemented.
• Payment year for 2017 MIPS performance period.
• 2015 CEHRT implemented.
• Mean/median scoring.
• Expansion of APM models.
Sunsetactivities

© Greenway Health, LLC. All rights reserved. Confidential and proprietary. Not for distribution except to authorized persons. 11
A single MIPS composite performance score will factor in performance in four weighted categories on a scale of 0-100.
What is MIPS?
QUALITY RESOURCE USE/COST
CLINICAL PRACTICE IMPROVEMENT
ACTIVITES
ADVANCING CARE INFORMATION
Replaces PQRS. Accounts for 50%
of total performance score in year
two.
Replaces VBM. Accounts for 10%
of total performance score in year
two.
Accounts for 15% of total
performance score in year
two.
Replaces Medicare MU.
Accounts for 25% of total
performance score in year
two.

Medicaid MU goes on separately
Medicaid meaningful
useMIPS

Regulatory cycle: H1
Jan. Feb. March April May June
• NQF MAP convenes.• Quality MUC
template published.
• Call for ACI measures.
• Call for IA measures.
• Call for quality measures.
• Measures from prior year’s process implemented.
• MACRA notice and comment continues.
• CMMI may issue new innovation models.
• IA measures submission closes EOM.
• MACRA proposed regulation issued, notice and comment begins.
• Closure of call for new quality measures.
• CMMI may issue new innovation models.
• CMMI new innovation models may issue.
• PTAC votes on physician designed APMs (quarterly meetings).

Regulatory cycle: H2
July Aug. Sep. Oct. Nov. Dec.
• MACRA notice and comment closes early in the month.
• Proposed Physician Fee Schedule is issued, notice and comment opens.
• CMMI may issue new innovation models.
• Proposed Physician Fee Schedule notice and comment continues.
• PTAC meets on proposed APMs.
• CMMI may issue new innovation models.
• PTAC meets on proposed APMs.
• PTAC issues RFP for new APMs.
• MACRA final regulation issued by Nov. 1, final list of new measures.
• Physician fee schedule finalized (may be combined with MACRA regulation).
• PTAC votes on physician designed APMs (quarterly meetings).
• Proposed Physician Fee Schedule notice and comment closes early in the month.
• PTAC meets on proposed APMs.

© Greenway Health, LLC. All rights reserved. Confidential and proprietary. Not for distribution except to authorized persons. 15
QualityMore outcomes based quality measures, special emphasis on care coordination, patient/caregiver experience, utilization, and performance gaps.
Advancing Care InformationMore interoperability measures. Specifically, closing the referral loop. Also asking for ways to measure CEHRT workflow disruption for the purpose of health IT specifications.
Improvement ActivitiesMore IAs that line up with PCMH or other existing programs, importance on improving health outcomes, reducing care disparity, broadly applicable, easy to implement, and whether CMS can validate the activity.
APMsMore APMs and Advanced APMs, private payer models, small practice and rural setting APMs.
Physician updates will be measured regularly, with a special emphasis on outcomes and interoperability.
Where’s MACRA going?

Assistance for small practices

Virtual group reporting
Up to 10 ECs per Tax ID.
Election by Dec. 1.
Allows small practices to scale reporting and performance.
Assess Quality and Cost uniformly.
Applications open in September.
No limit on the number of TINs.

Small practice bonus
2024
5 point bonus to
MIPS composite

Less than $90,000 in Medicare revenue
excluded.
Fewer than 200 Medicare
unique patients are excluded.
ACI hardship exemption.
More flexibility for small practices.
Driving flexibility through exclusions and exemptions

Reporting & scoring

© Greenway Health, LLC. All rights reserved. Confidential and proprietary. Not for distribution except to authorized persons. 21
Performance thresholds, the MIPS composite score, and your bottom line
0 3 15 70 100
In the 2018 performance period, ECs who earn a composite score between 0-15 are subject to a 0%-5% penalty in 2020. 15 is
the performance threshold, increased from 3 in 2017. CMS estimates $118 million in
penalties will be assessed.
ECs who earn a composite score between 15-70 are eligible for a 0%-5% incentive in
2020. CMS estimates $118 million in incentives for this group.
ECs who exceed 70 are eligible for increased MIPS
bonuses, which will be paid out of a pool of $500 million that is not subject
to budget neutrality.

Who is eligible to participate in MIPS?
Years 1 and 2
Years 3+
Physical or occupational therapists, speech-language pathologists, audiologists, nurse midwives, clinical social workers, clinical psychologists, dietitians/nutritional professionals.
HHS Secretary may broaden EC groups to include others,
such as:
Physicians (MD/DO and DMD/DDS), PAS, NPS, clinical nurse specialists, certified registered nurse anesthetists.

© Greenway Health, LLC. All rights reserved. Confidential and proprietary. Not for distribution except to authorized persons. 23
MIPS does not apply to hospitals or facilities.
Who is not eligible to participate in MIPS?
First year of Medicare Part B
participation
Below low-patient
volume threshold
Certain participants in Advanced
APMs
Medicare billing charges ≤ $90,000 OR providers care for ≤ 200 patients in one year

© Greenway Health, LLC. All rights reserved. Confidential and proprietary. Not for distribution except to authorized persons. 24
Eligible clinicians can participate in MIPS as an individual or group.
Eligible Clinician reporting
GROUPA group, as defined by taxpayer
identification number (TIN), would be assessed as a group practice across all
four MIPS performance categories.
INDIVIDUAL VIRTUALTo be implemented in 2018
performance period, defined with a virtual group identifier,
TIN, and NPI combination.

MIPS 2017 reporting options
Don’t participate and receive a 4% negative adjustment rate.1
Submit one quality measure, one improvement activity, or the required ACI measures for at least 90 days and avoid a negative adjustment.
Submit more than one quality measure, more than one improvement activity, or more than the required ACI measures for at least 90 days, and get no adjustment or a small positive one.
Submit data to MIPS for the full year and get a positive adjustment.
2
3
4

Sample reporting options in 2018
Don’t participate and receive a 5% negative adjustment rate.1
Report on the required ACI measures and one quality measure.
Fully report on and participate in improvement activities.
Submit six quality measures that meet data completeness criteria.
2
3
4

Reporting timelines for 2018
90 days for Advancing Care Information.1
90 days for Improvement Activities.
Full year for Quality.
Full year for Cost.
2
3
4

60%15%
25%
0%Advancing Care Information
Quality
Clinical Practice Improvement Activities
MIPS scoring in 2017

50%
15%
25%
10%Quality
Clinical Practice Improvement Activities
Final Rule: MIPS scoring in 2018
Cost
Advancing Care Information

30%
15%25%
30%
Quality
Clinical Practice Improvement Activities
MIPS scoring in 2019
Cost
Advancing Care Information

More points for complex patients
Bonus based on average
HCC scores

Improvement scoring
80%
45%
30%
Improvement scoring rewards clinicians for
improvement in the Quality and Cost categories
by comparing the current performance period
with the prior performance period.
Quality improvement will be assessed at the
category level because different clinicians may
select very different measures that are not
comparable. Your improvement score is added
onto your Quality performance.
Cost improvement will be assessed at the
measure level because all clinicians are generally
measured on the same measures. Your
improvements score is added onto your Cost
performance.

Facility-based measurement coming in future years
Cost

© Greenway Health, LLC. All rights reserved. Confidential and proprietary. Not for distribution except to authorized persons. 35
• Medicare Spending per Beneficiary (MSPB) in 2018.
• Introducing episode-based measures in 2019.
How is Cost measured?

Advancing Care Information

Scoring Advancing Care Information
Performance score, where the more you do, the
more you earn (up to 50).
Bonus scores up to 25% for
miscellaneous. Total (up to 100).
Base score to get any credit (50).

Which certified edition?
• 10% bonus to 2018 ACI score.
• May use 2014 CEHRT.
• May Use 2015 CEHRT.
• May report on 2017 Transition Year ACI Objectives (derived from Stage 2).
• May report on ACI Objectives (derived from Stage 3).
Benefits of 2015 CEHRT
2017 performance period
2015 ONC
CEHRT
2017performance
2018 performance
• May use 2014 CEHRT.
• May Use 2015 CEHRT.
• May report on 2017 Transition Year ACI Objectives (derived from Stage 2).
• May report on ACI Objectives (derived from Stage 3).
2018 performance period

The return of exclusions
BUSINESS ECOSYSTEM
Protect patient health information
(yes required)
Electronic prescribing (numerator/denominator)
Health information exchange (numerator/
denominator)
Coordination of care through patient engagement (numerator/
denominator)
Public health and clinical registry reporting Patient electronic access
(numerator/denominator)
Advancing Care Information

A shift in measuring public health reporting
Beyond the performance score
A 5% bonus score is available for submitting to another public health agency or clinical data registry.
Performance score
Connecting to a public health registry gives you 10% to your ACI performance score.

Bonus score
2015 CEHRT
Registry reporting
Reporting improvement
activities through CEHRT
Bonus up to 25%

What’s next with ACI?
New call for measures.
Use case: Closing the
referral loop.
Interoperability in non-office
settings.

What about interoperability?
National Patient Identifier1
21st Century Cures, standards and penalties2
Interopereability and outcomes3

CommonWell to become Carequality implementer.
Future projects and integration.
Working to create Carequality compliant version of CommonWell
record locator service.Initial C-CDA integration.
Carequality and CommonWell Health Alliance partnership

Quality & Clinical Practice Improvement Activities

Data completeness threshold raised from 50% to 60%.
Quality updates
Choice More CQMs available, focused on outcomes and other high priority measures.
Reporting May not submit measures using multiple data submission mechanisms in 2018.
Removing measures
Phase out process introduced for topped out measures.
Floor Three point floor for each measure.

More outcomes measures and more specialist measures.
What’s coming with Quality
COMPANY 47
1
May see continued focus on qualified registry reporting and QCDR reporting.
Preference for outcomes measures over process measures.
National Quality Forum’s Measure Applications Partnership: Call for measures.
2
3
4

More improvement activities, expanding PCMH
50% of practices within a TIN need PCMH recognition
for full CPIA credit.
PCMH definition expanded to
include CPC+.No change to scoring or weight.
More activities in general, and
more activities that relate to
CEHRT.

Expanded subcategories based on contribution to improvements in patient care, cost, and quality.
What’s coming with CPIA
1
More activities to come based on relevance to existing programs, importance towards improving health outcomes, alignment with PCMH, and more.
2

Alternative Payment Models

50%
20%
30%
0%Advancing Care Information
Quality
Clinical Practice Improvement Activities
MIPS APM scoring in 2017

Advanced APM impact to providers
20242026+202020182016
5% Lump Sum
Bonus
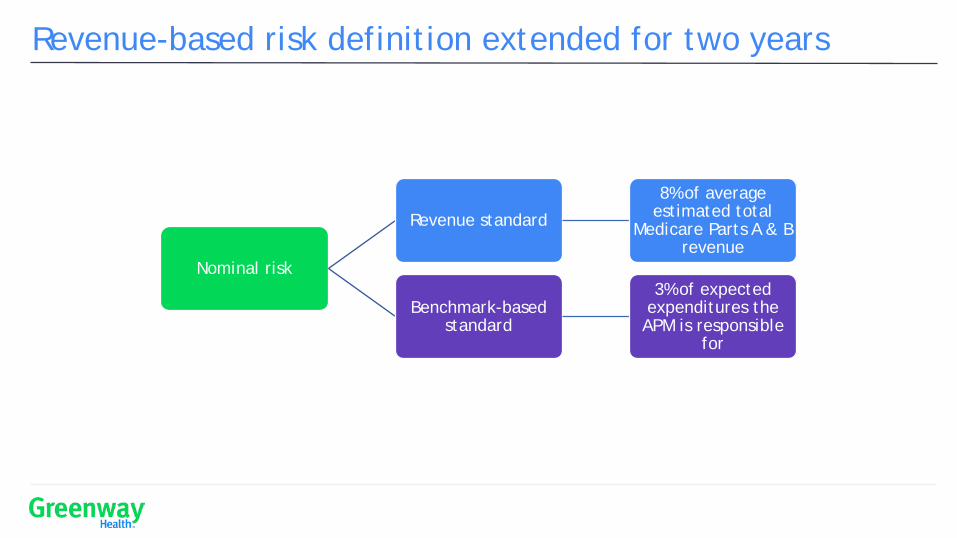
Revenue-based risk definition extended for two years
Nominal risk
Revenue standard
8% of average estimated total
Medicare Parts A & B revenue
Benchmark-based standard
3% of expected expenditures the APM is responsible
for

The Medical Home Model – A more gradual ramp
Or
General definition
Quality incentive or PMPM at risk
2018: 2% 2019: 3%
2020: 4%
2021: 5%
RISK

Who’s in the APM track?
201720152024+20232022202120202019
Payments
25%
Patients
20%
Payments
50%
2019-2020
• Medicare APMs only
2021+•Include private payers
Payments
75%
Patients Patients
35% 50%

More ways to qualify coming
1
2
3
All payer combination options
Medicaid & CHIP
CMS Multi-Payer models

Performance thresholds and Cost in the future
0 3 15 70 100
The performance threshold in 2019 will be set as the mean or median of prior MIPS
composite scores, unless Congress amends MACRA.
30%
15%25%
30%
Cost
To change how CMS sets thresholds and Cost’s portion of the score for future years, an act of Congress would be
required.

1
2
3
Measure quality and costFirst, clinicians become accustomed to capturing metrics and measuring performance on quality and cost.
Implement technological and clinical processesAs MIPS ramps up, clinicians are incented to implement process changes that can quanitifiably move the needle on quality and cost.
Prepare for riskBy changing the way the clinicans deliver care over time, clinicans are equipped to take advantage of risk-bearing contracts that reward superior care over volume.
Congress’ vision: From MIPS to APMs

© Greenway Health, LLC. All rights reserved. Confidential and proprietary. Not for distribution except to authorized persons. 59
Don’t take the transition year off. Instead, prepare for success.
How to succeed with MACRA
Learn about the programLearn what it means for your bottom line, and what’s coming in the future through qpp.cms.gov and Greenway Health webinars.
Compare your dataLook at your historical data and measures — and focus on what you’re good at, what’s relevant to your patient population, and where you can make the easiest improvements.
Design a planDesign a plan based on your data that accounts for 2017 and 2018. Use the transition year to test your plan. Don’t slack this year or 2018 might catch you off-guard.
Design
Compare
Learn

© Greenway Health, LLC. All rights reserved. Confidential and proprietary. Not for distribution except to authorized persons. 60
Are you interested in learning more? Let us know:
a) I would like to pre-register for your webinar on Feb. 28 at 12:00 p.m. Eastern time.
b) I would like to speak with a Greenway Health representative.
c) I'm not interested at this time.
Poll question

Questions

© Greenway Health, LLC. All rights reserved. Confidential and proprietary. Not for distribution except to authorized persons. 62
• ACI: Advancing Care Information
• APM: Alternative Payment Model
• CPIA: Clinical Practice Improvement Activities
• EC: Eligible Clinician
• HHS: The US Department of Health & Human Services
• MACRA: Medicare Access & CHIP Reauthorization Act of 2015
• MIPS: Merit-based Incentive Payment System
• MU: Meaningful Use
• NP: Nurse Practitioner
• NPRM: Notice of Proposed Rulemaking
• PA: Physician Assistant
Acronyms cheat sheet

© Greenway Health, LLC. All rights reserved. Confidential and proprietary. Not for distribution except to authorized persons. 63
• The Final Rule for 2018
• Year 2 Overview fact sheet
• 2017 Extreme and Uncontrollable Circumstances Policy for MIPS fact sheet
Resources
Top Related