








Languages
Pages
Legal

Lahir di Garut, 16-1-1955Lahir di Garut, 16-1-1955
SD-SMA : GarutSD-SMA : GarutDokter umum: FK UNSRI PalembangDokter umum: FK UNSRI PalembangInternist: FK UNPAD BandungInternist: FK UNPAD BandungClinical Rheumatology & Osteoporosis Clinical Rheumatology & Osteoporosis TrainingTraining: :
Arthritis Foundation of WA PerthArthritis Foundation of WA PerthKonsultan Reumatologi : FKUIKonsultan Reumatologi : FKUI Jakarta Jakarta
Divisi Divisi ReumatologiReumatologi RS Dr Hasan SadikinRS Dr Hasan Sadikin
IRA, PAPDI, PEROSI, PERALMUNI, APLAR, IASP, IRA, PAPDI, PEROSI, PERALMUNI, APLAR, IASP, OARSIOARSI
Infection autoimmunity Autoimmune disease infection
08/04/15

Source: http://www.biologymad.com/
Classical systemic autoimmune disease (12) Systemic vasculitis (16) Idiopathic inflammatory myopathies (8) 0ther immune mediated systemic diseases (4) Endocrine and reproductive autoimmune diseases (13) Hepatobillary and pancreatic autoimmune diseases (5) Gasrointestinal autoimmune disease (4) Cutaneous autoimmune diseases (4) Cardiovascular and pulmonary autoimmune diseases (6) Neurological autoimmune disease (11) Ocular autoimune diseases (4) Renal autoimmune diseases (5) Hematologic autoimmune diseases (11)
08/04/15

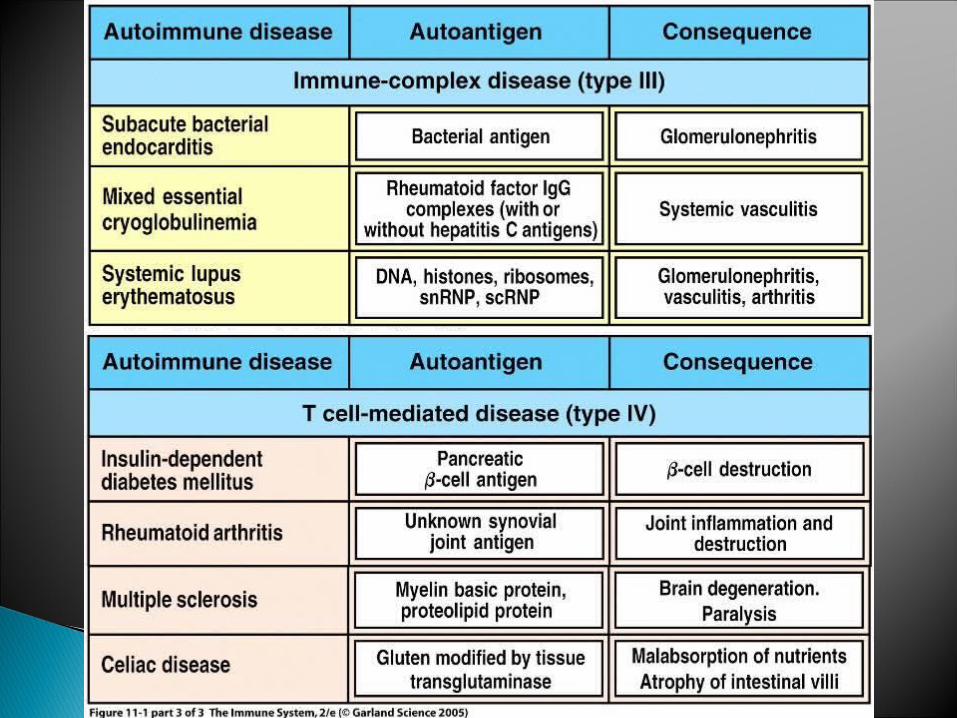
Organ-specific diseasesDamage is confined to the organ
against which the immune response is mounted
Non-organ-specific diseasesImmune response against
antigens which are not associated with the organ involved
Organ-specific diseasesDamage is confined to the organ
against which the immune response is mounted
Non-organ-specific diseasesImmune response against
antigens which are not associated with the organ involved

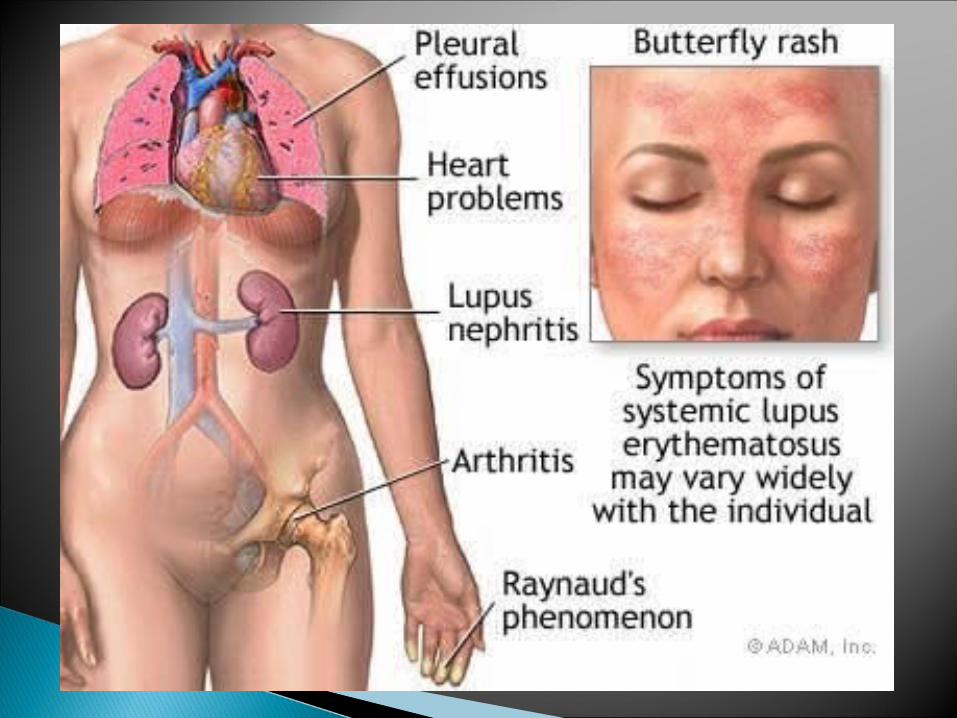
Systemic lupus erythematosus (SLE ) is a chronic autoimmune connective tissue disease that can affect any part of the body.
SLE most often harms the heart, joints, skin, lungs,
blood vessels, liver, kidneys, and nervous system. The course of the disease is unpredictable, with
periods of illness (called flares) alternating with remissions.
The disease occurs nine times more often in women than in men, especially between the ages of 15 and 50.

SLE is treatable through addressing its symptoms, mainly with corticosteroids and immunosuppressants; there is currently no cure.
SLE can be fatal, although with recent medical advances, fatalities are becoming increasingly rare.
Survival for people with SLE in the United States, Canada, and Europe is approximately 95% at five years, 90% at 10 years, and 78% at 20 years.
There are several types of lupus; in general, when the word lupus alone is used, reference is to systemic lupus erythematosus,
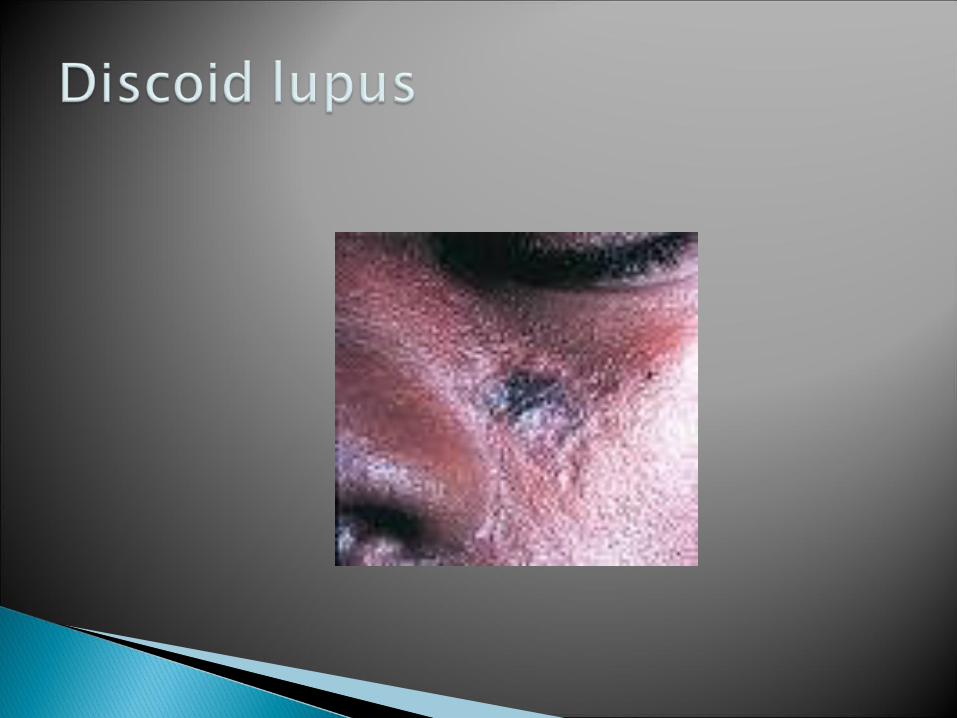
Other types include:1-Discoid lupus E ;chronic cutaneous lupus, lead to skin disorder in which
there is red, raised rash on the face or scalp. limited to the skin and diagnosed by skin biopsy.
2-Drug-induced lupus (procainamide,hydralazin,quinidine,phenytoin)
3-Lupus nephrit is:an inflammation of kidneys, caused by SLE.
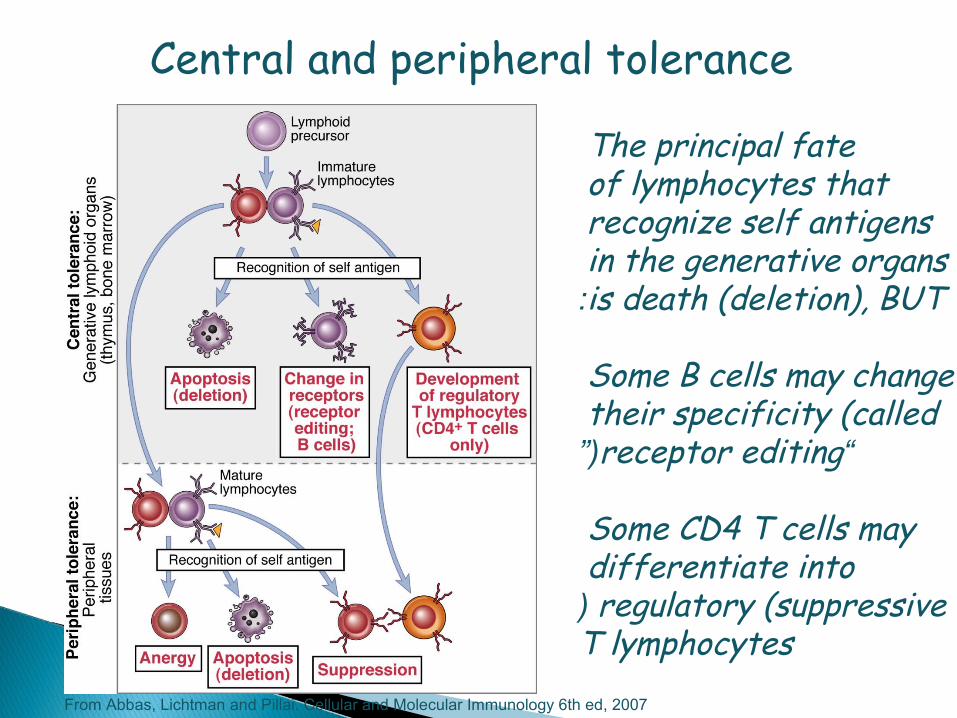
The principal fate of lymphocytes that recognize self antigens in the generative organs is death (deletion), BUT:
Some B cells may change their specificity (called
“receptor editing”(
Some CD4 T cells may differentiate into regulatory (suppressive(
T lymphocytes
Central and peripheral tolerance
From Abbas, Lichtman and Pillai. Cellular and Molecular Immunology 6th ed, 2007

Consequences of self antigen recognition in thymus
From: Abbas & Lichtman, Cellular & Molecular Immunology 5th ed 2003

08/04/15
Age Gender * Genotype* Life style choices Stress

Skin cell
T cell T cell
B cell
APC
APC
Defective IC clearance
UV light Infection
External AgSelf Ag
Ab
IC
Target
Gen
etic suscep
tibility

Common initial and chronic complaints are fever, malaise, joint pains, myalgias, fatigue, and temporary loss of cognitive abilities.
Because they are so often seen with other diseases, these signs and symptoms are not part of the diagnostic criteria for SLE.
When occurring in conjunction with other signs and symptoms, however, they are considered suggestive.

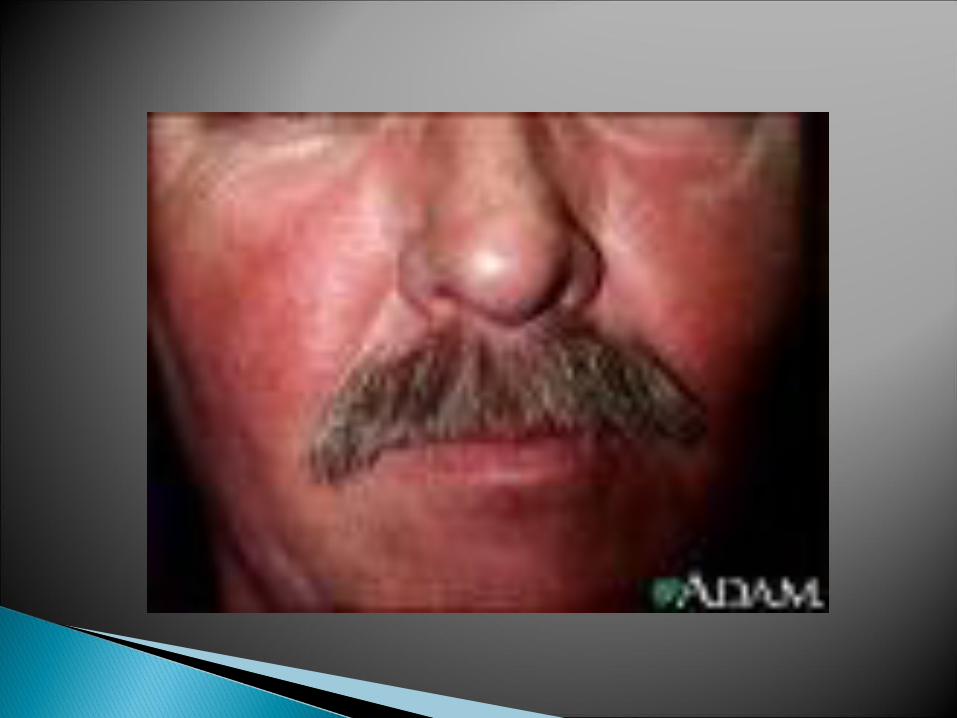
30% to 50% suffering from the classic malar rash (or butterfly rash) associated with the disease.
Alopecia; mouth, nasal, and vaginal ulcers.
Musculoskeletal manifestations The most commonly sought medical attention is
for joint pain, with the small joints of the hand and wrist usually affected, although all joints are at risk.
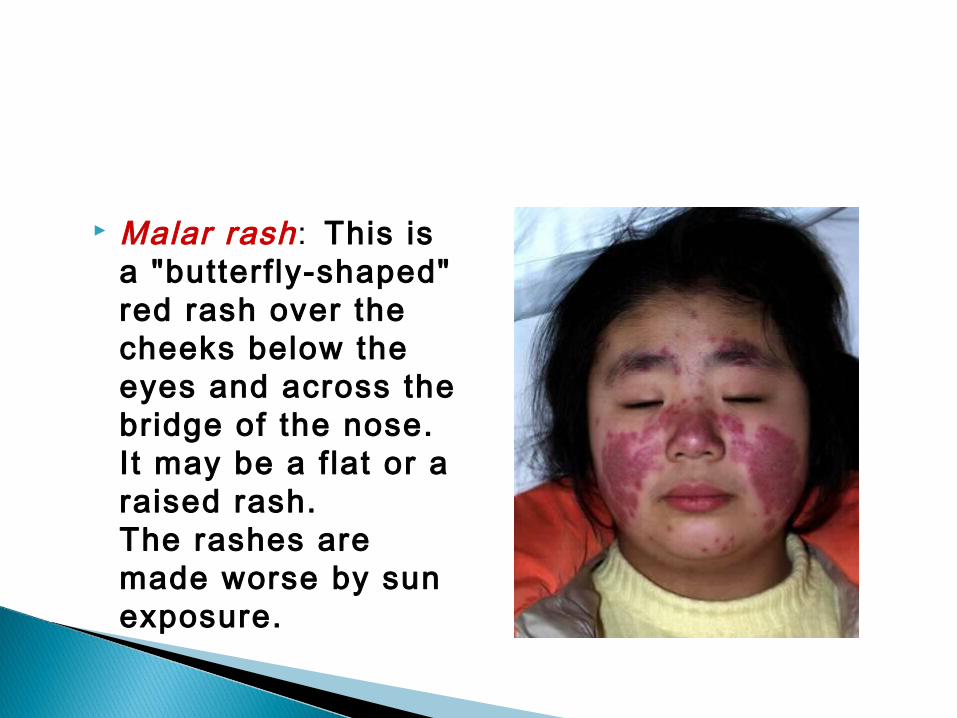
Malar rash: This is a "butterf ly-shaped" red rash over the cheeks below the eyes and across the bridge of the nose. I t may be a f lat or a raised rash.The rashes are made worse by sun exposure.

Maculopapular eruption
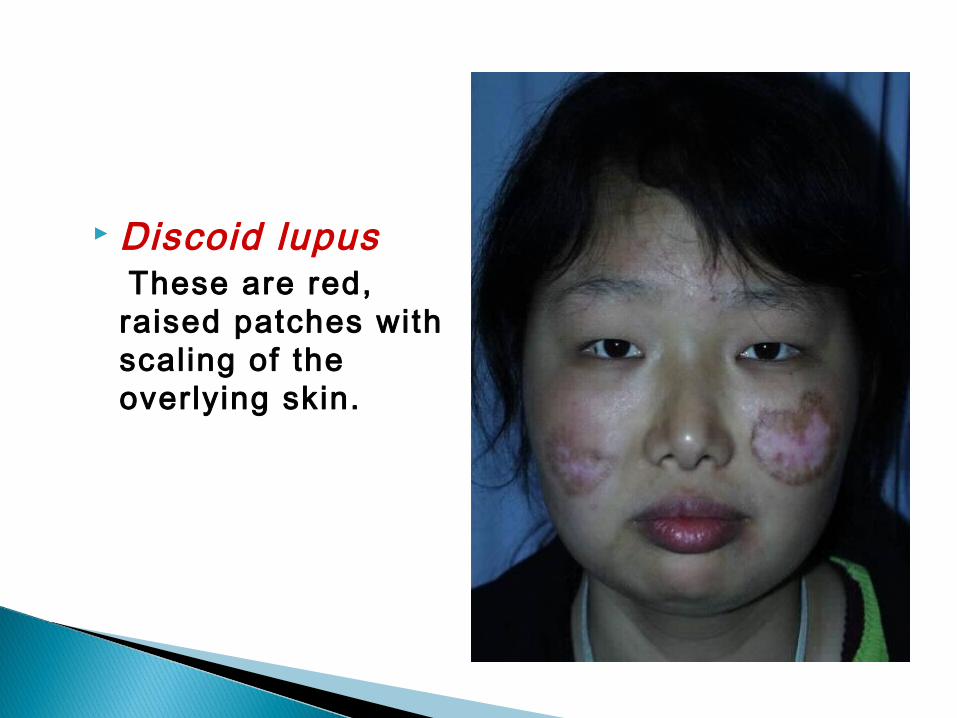
Discoid lupus These are red,
raised patches with scaling of the overlying skin.
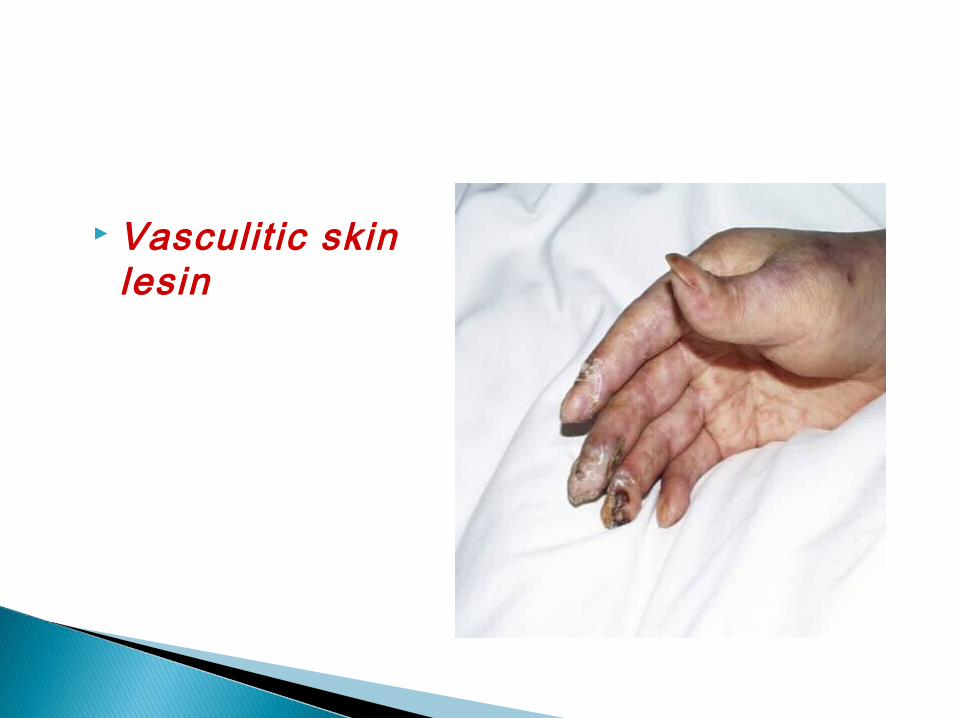
Vasculit ic skin lesin
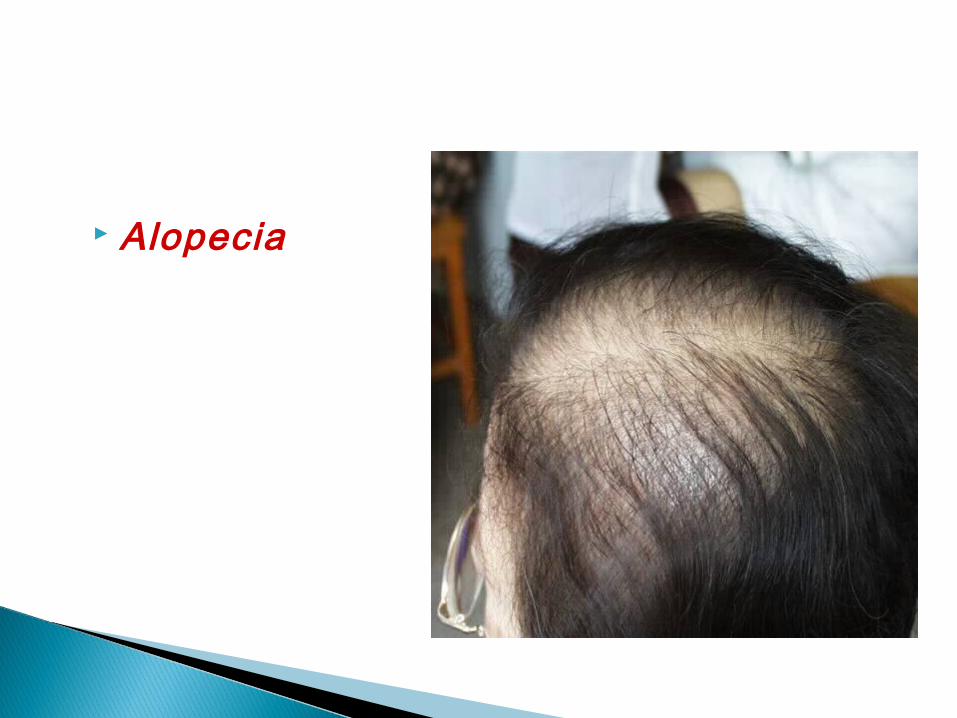
Alopecia
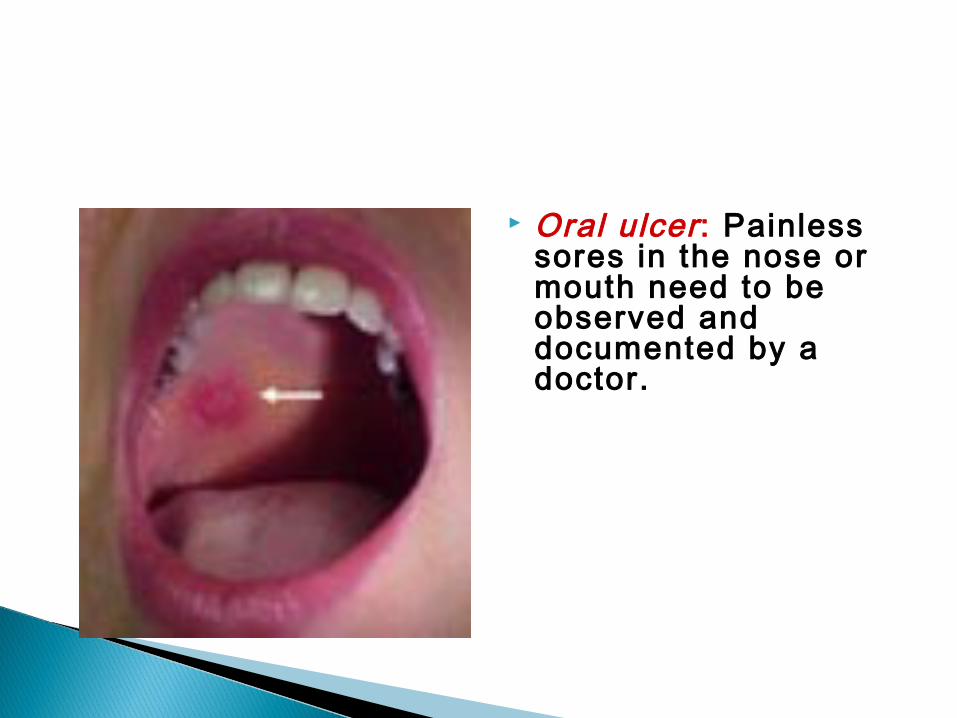
Oral ulcer: Painless sores in the nose or mouth need to be observed and documented by a doctor.
Unlike rheumatoid arthritis, lupus arthritis is less disabling and usually does not cause severe destruction of the joints. Fewer than ten percent of people with lupus arthritis will develop deformities of the hands and feet.
SLE patients are at particular risk of developing
osteoarticular tuberculosis.

Hematological manifestations
Anemia usually present in up to 50% of cases. Low platelet and white blood cell counts may be due to the disease or a side-effect of pharmacological treatment.
People with SLE may have an association with antiphospholipid antibody syndrome, (thrombotic disorder), wherein autoantibodies to phospholipids are present in their serum.
Abnormalities associated with antiphospholipid antibody syndrome usually present ,and a positive test for antiphospholipid antibodies; lupus anticoagulant-positive. Another autoantibody is the anticardiolipin antibody.
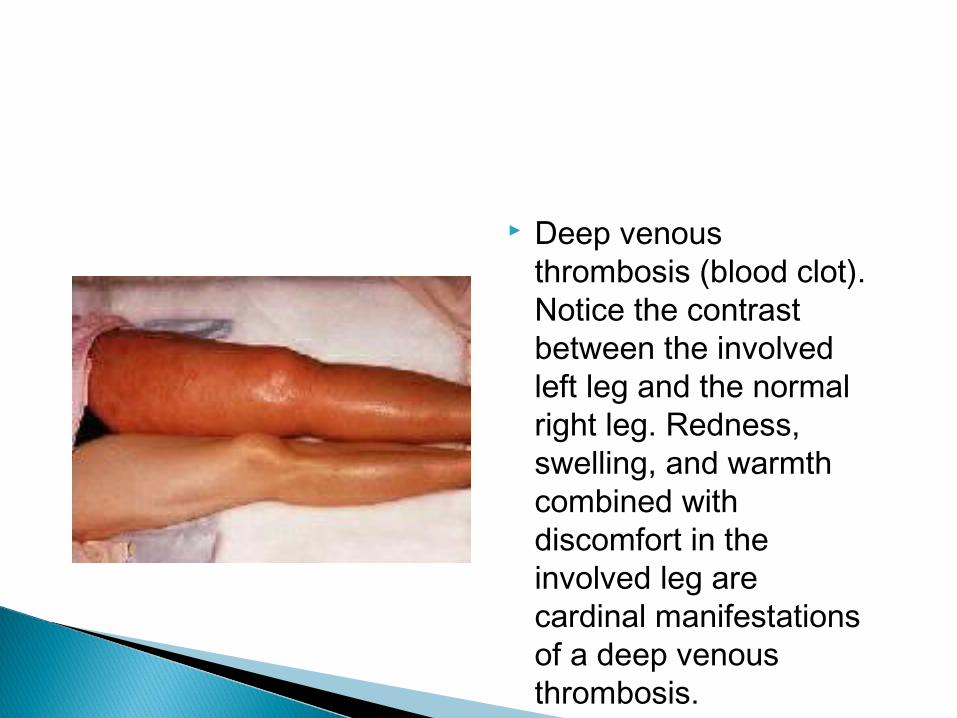
Deep venous thrombosis (blood clot). Notice the contrast between the involved left leg and the normal right leg. Redness, swelling, and warmth combined with discomfort in the involved leg are cardinal manifestations of a deep venous thrombosis.

Cardiac manifestations A person with SLE may have inflammation of various
parts of the heart, such as pericarditis, myocarditis, and endocarditis.
The endocarditis of SLE is characteristically noninfective (Libman-Sacks endocarditis),
and involves either the mitral valve or the tricuspid valve.
Atherosclerosis also tends to occur more often and advances more rapidly than in the general population.
Vasculitis may produce myocardial infarction, and Raynaud’s phenomenon.

Pericardit is

SLE can be associated with endocarditis. Shown here is Libman-Sacks endocarditis in which there are many flat, reddish-tan vegetations spreading over the mitral valve and chordae.
Pulmonary manifestations
Lung and pleura inflammation can cause pleuritis, pleural effusion, lupus pneumonitis, chronic diffuse interstitial lung disease, pulmonary hypertension, pulmonary emboli, pulmonary hemorrhage.
Renal involvement
Painless hematuria or proteinuria may often be the only presenting renal symptom.
Acute or chronic renal impairment may develop with lupus nephritis, leading to acute or end-stage renal failure.
A histological hallmark of SLE is membranous glomerulonephritis.
This finding is due to immune complex deposition along the glomerular basement membrane.

Neuropsychiatric syndromes
can result when SLE affects the central or peripheral nervous system.
The most common neuropsychiatric disorder people with SLE have is headache.
Other common neuropsychiatric manifestation of SLE include cognitive dysfunction, mood disorder, cerebrovascular disease, seizures, polyneuropathy, anxiety disorder, and psychosis.
Systemic manifestat ions
Fatigue in SLE is probably multifactorial and has been related not only to disease activity or complications such as anemia ,but also to pain, depression, poor sleep quality, and poor physical fitness.

1. Malar rash: Fixed erythema over malar areas, sparing nasolabial folds
2. Discoid rash: Erythematous raised patches with keratotic scaling and follicular plugging
3. Photosensitivity: Skin rash after exposure to sunlight, history or physical exam
4. Oral ulcers: Oral or nasopharyngeal, painless, by physical exam
5. Arthritis:Tenderness, swelling, effusion in 2 or more peripheral joints
6. Serositis: A) pleuritis or B) pericarditis
7. Renal disorder A) proteinuria>0.5g/24hour or 3+ or B) cellular casts 8. Neurological disorder: A) seizures or B) psychiatric disorder (having
excluded other causes, e.g. drigs(9. Haematological disorder: A) haemolytic anaemia or B) leucopenia or C)
thrombocytopenia 10. Immunologic disorder: A) positive LE cells or B) raised anti-native DNA
antibdy binding or C) anti-Sm antibody or D) false positive serological test for syphilis.
11. Positive antinuclear antibody:
Criteria of the ARA for the classification of SLE
Investigations ■ Blood: ■ A full blood count may show a leucopenia,lymphopenia and/or thrombocytopenia. Anaemia ofchronic disease or autoimmune haemolytic anaemiaalso occurs. The ESR is raised in proportion to thedisease activity. In contrast, the CRP is usuallynormal but may be high when the patient has lupuspleuritis or arthritis or a coexistent infection. ■ Urea and creatinine only rise when renal disease isadvanced. Low serum albumin or high urine protein/creatinine ratio are earlier indicators of lupusnephritis.
Autoantibodies – many different autoantibodies may be present in SLE but the most significant are ANA, anti-dsDNA, anti-Ro, anti-Sm and anti-La .
Antiphospholipid antibodies are present in25–40% of cases but not all of these patientsdevelop antiphospholipid syndrome . ■ Serum complement C3 and C4 levels are oftenreduced during active disease. The combination ofhigh ESR, high anti-dsDNA and low C3 may heralda flare of disease. All these markers tend to returntowards normal as the flare improves

The lupus erythematosus (LE( cell
i t has been superseded by the ANA and anti-dsDNA techniques.
ANA is a screening test anti-Sm, anti-dsDNA
antibodies are lupus specif ic antoantibodies.

This homogenous pattern of diffuse bright green staining of nuclei seen by immunofluorescence microscopy with a Hep2 cell substrate is called homogenous, and is the most common pattern with autoimmune diseases overall.
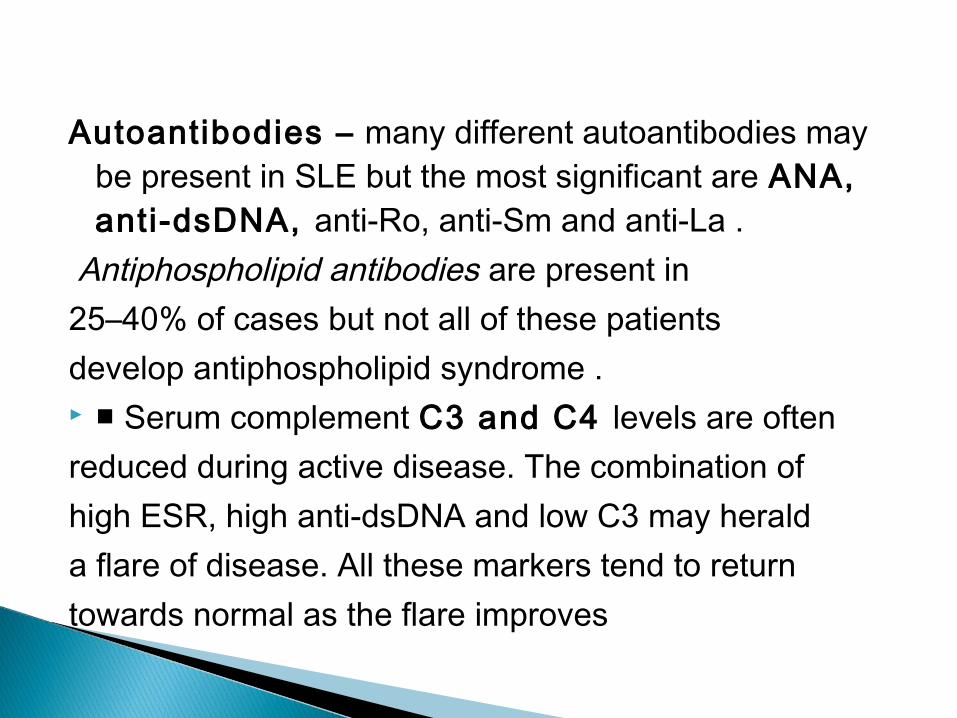
This rim (peripheral ( pattern of linear bright green staining around the peripheral of nuclei seen by immunofluorescence microscopy with a Hep2 cell substrate .
dsDNA
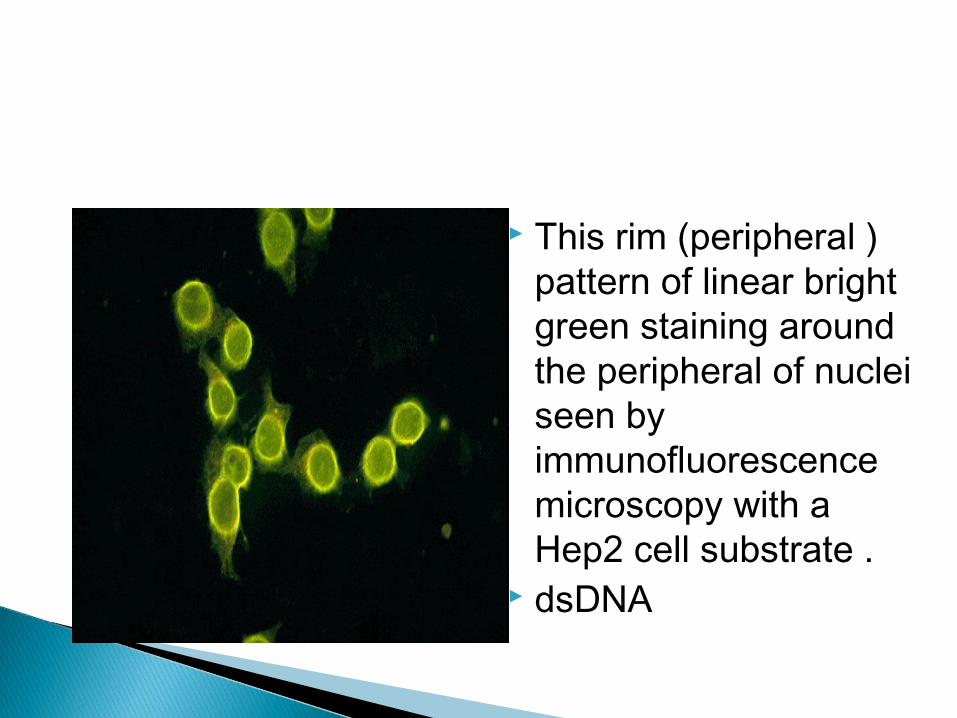
Nucleolar pattern
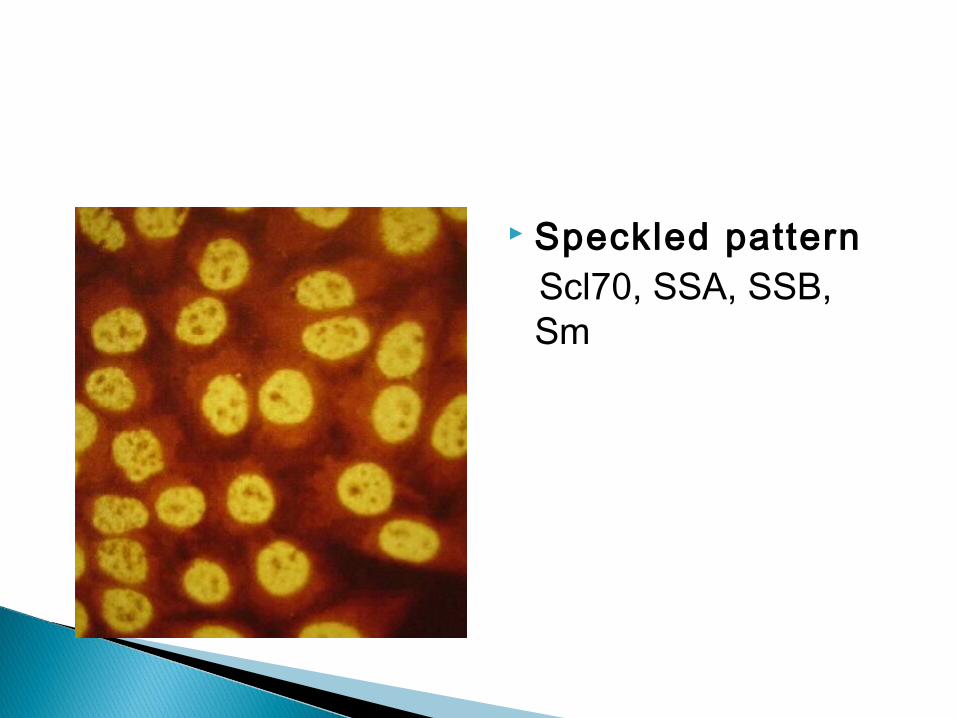
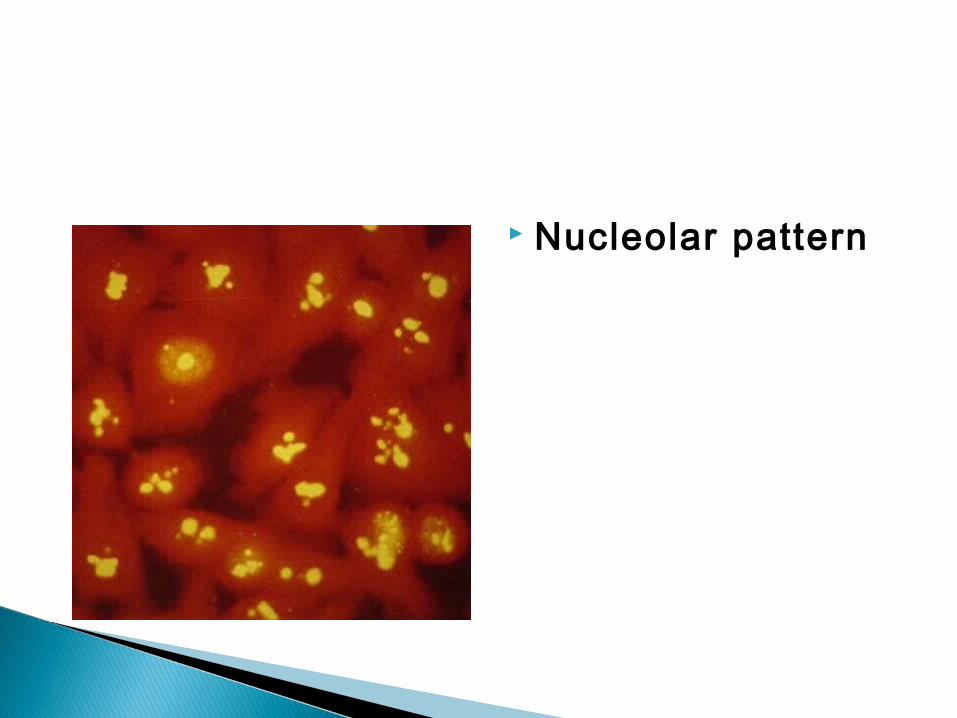
Speckled pattern Scl70, SSA, SSB,
Sm

These little Crithidia organisms have a small kinetoplast between the nucleus and the flagella which glows bright green under immunofluorescence microscopy, and is indicative of anti-native DNA antibody that is very specific for SLE.
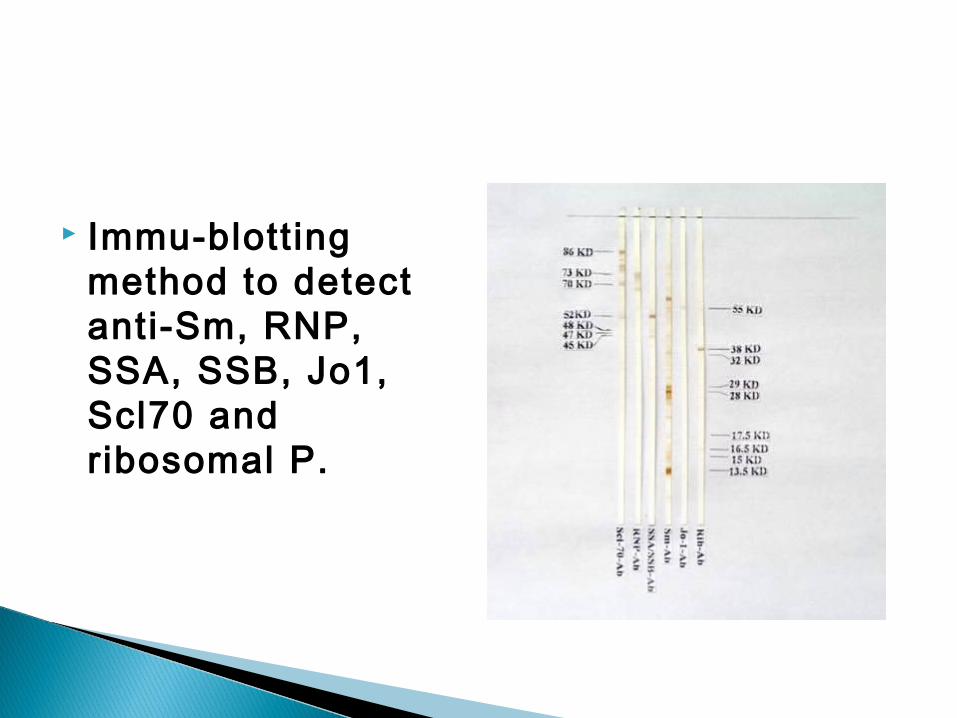
Immu-blott ing method to detect anti-Sm, RNP, SSA, SSB, Jo1, Scl70 and ribosomal P.

Immunofluorescence of skin with antibody to IgG demonstrates a band-like deposition of immune complexes that is bright green at the dermal epidermal junction in this skin biopsy taken from an area with a visible rash. With SLE such deposition can be found in skin uninvolved by a rash, whereas with DLE the immune complexes are found only in involved skin.
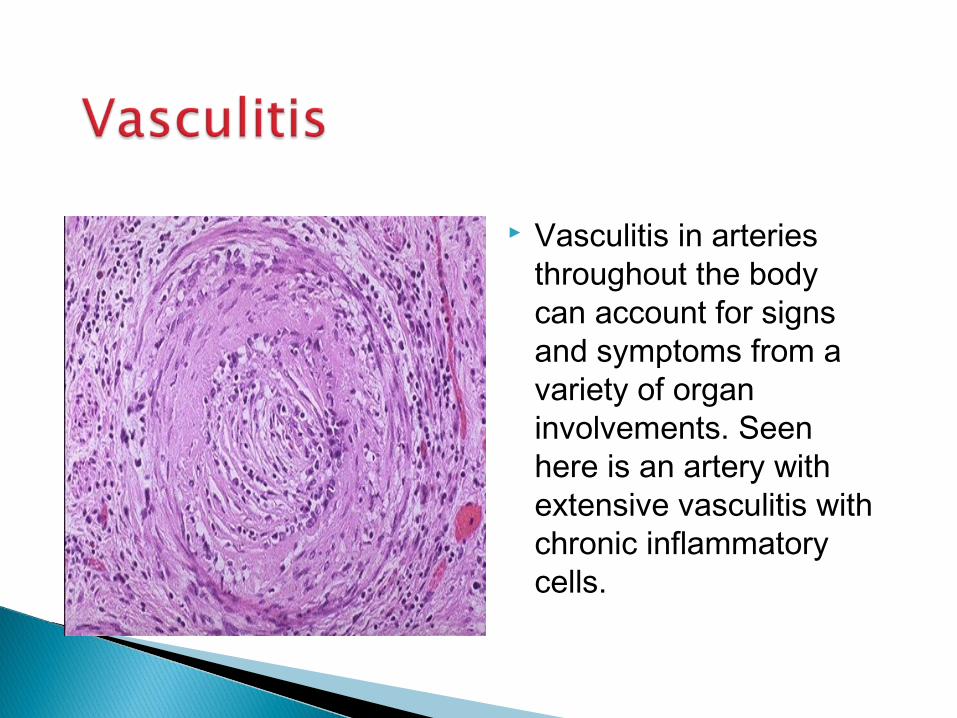
Vasculitis in arteries throughout the body can account for signs and symptoms from a variety of organ involvements. Seen here is an artery with extensive vasculitis with chronic inflammatory cells.

SLE is associated with a peculiar periarteriolar f ibrosis in the spleen, as shown here.
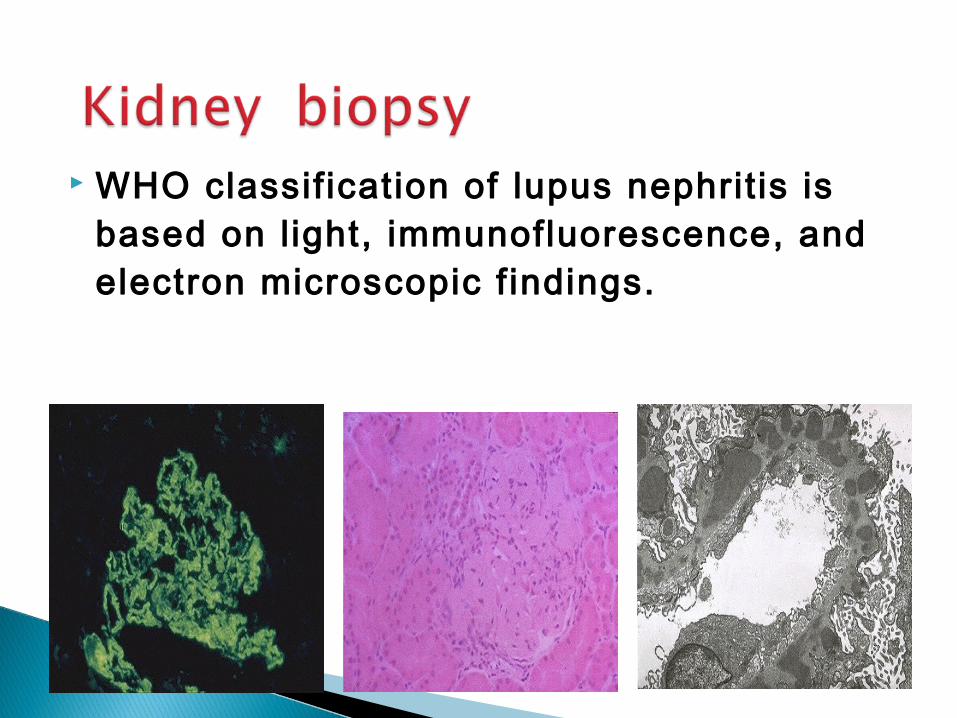
WHO classif ication of lupus nephrit is is based on l ight, immunofluorescence, and electron microscopic f indings.

Treatment Being a chronic disease with no known cure, the
treatment of SLE is symptomatic. ,this involves preventing flares and reducing their severity and duration when they occur. Currently, medication is the main form of treatment.
Medications Due to the variety of symptoms and organ system
involvement with SLE, its severity in an individual must be assessed in order to successfully treat SLE.
Mild or remittant disease can sometimes be safely left untreated. If required, nonsteroidal anti-inflammatory drugs and antimalarials may be used.

Disease-modifying antirheumatic drugs
Disease-modifying antirheumatic drugs (DMARDs( are used preventively to reduce the incidence of flares, the process of the disease, and lower the need for steroid use; when flares occur, they are treated with corticosteroids.
DMARDs commonly in use are antimalarials and immunosuppressants (e.g. methotrexate and azathioprine(.
Hydroxychloroquine is an FDA-approved antimalarial used for constitutional, cutaneous, and articular manifestations,
whereas cyclophosphamide is used for severe glomerulonephritis or other organ-damaging complications.

Clinical featureinit ial dose of prenisolone
Arthrit is (poorly responding to NSAIDs) 20-30mg/d, reducing
pleurit is by about 5mg/wk if
Pericardit is symptoms abate
Haemolytic anemia 1mg/kg/d for about 1M
Thrombocytopenia reduce by 10mg/d if
blood tests improve
Nephritis 1mg/kg/d for about 1M
Neuropsychiatric controversal! 1-2mg/kg/d, 0.5-1g/d
methylprednisolone

Plasma exchange Intravenous Immunoglobulin Stem cell transplantation Immune therapy ( anti-IL10, anti-CD20,
and immune tolerance therapy)
SLE has been stable for more than 1 year. Prednisone is no more than 10mg/d, and
cytotoxic drug has been stopped for more than 6 moth.
SLE patients can plan to have a baby.

Depending on the dosage, people that require steroids may develop side-effects such as central obesity, puffy round face, diabetes mellitus, increased appetite, difficulty sleeping and osteoporosis. Those side-effects can subside if and when the large initial dosage is reduced, but long-term use of even low doses can cause elevated blood pressure and cataracts.

Lifestyle changes Avoiding sunlight is the primary change to the
lifestyle of SLE sufferers, as sunlight is known to exacerbate the disease. Drugs unrelated to SLE should be prescribed only when known not to exacerbate the disease
Prognosis.
High serum creatinine, hypertension, nephrotic syndrome, anemia and hypoalbuminemia are poor prognostic factors.
The ANA is the most sensitive screening test for evaluation, whereas anti-Sm (anti-Smith) is the most specific.
The dsDNA (double-stranded DNA) antibody is also fairly specific and often fluctuates with disease activity; as such, the dsDNA titer is sometimes useful to monitor disease flares or response to treatment.





Thank you
Top Related