







Languages
Pages
Legal


Place picture here
Laying a “SAFE” Foundation
Julie ApoldMickey Reid
Minnesota Hospital Association

MHA Calls-to-ActionBrief History
AHE Law went into effect July 2003Report any of the 28 National Quality Forum
Serious Reportable Events Event types with highest # of reports:• Wrong Body Part Surgery• Retained Foreign Objects• Falls• Pressure Ulcers

Focused Approach to Improvement
Focus on top events• Determine Best Practices• Implement Best Practices
Convened Advisory Groups• Reviewed National and Local Best Practices• Reviewed AHE Data• Developed Implementation Best Practices

Patient Safety Roadmaps

MHA Statewide Calls-to-Action

Roadmap Work Group
Danielle Abel Lakewood Health Center Mary Ellen Bennett Hennepin County Medical Center Jane Harper Minnesota Department of Health Sheila Higbe Olmsted Medical Center Jane Hirst LifeCare Medical Center Lindsey Lesher Minnesota Department of Health Vicki Olson Stratis Health Kate Peterson Stratis Health Gail Pries Gillette Children’s Specialty Healthcare Jean Rainbow Minnesota Department of Health Mickey Reid Minnesota Hospital Association Linell Santella Park Nicollet Methodist Hospital Cindi Welch Essentia Health Boyd Wilson HealthEast Care System

SAFE from HAI Roadmap

Roadmap Structure
SAFE Building Blocks Infection-specific Gap Analyses

“SAFE”

SAFE = S (Safety Teams/Org Structure)
Action 1: Secure endorsements and resources for HAI Prevention Program
• Leadership:o Endorses the worko Clearly communicates goalso Regularly reviews progress toward goalso Supports adding resources as appropriateo Designates a senior leadership sponsor

SAFE = S (Safety Teams/Org Structure)
Action 2: Promote HAI prevention representation/champions/liaisons throughout the facility• Regular Interdisciplinary team• Champions• Liaisons• Ad-hoc for specific projects• Designated coordinator(s)
o With designated time!

SAFE = S (Safety Teams/Org Structure)
Action 3: Identify gaps and develop action plans
• The interdisciplinary team:o Reviews and updates the HAI prevention programo Reviews data results at least quarterly and identifies
strengths and opportunitieso Develops a plan to prioritize and address improvement
opportunitieso Commissions subgroups as needed

SAFE = A (Access to Information)
Action 1: Track progress on process and outcome measures• Observational audits• Inter-rater reliability• Capture infection event details

SAFE = A (Access to Information)
Action 2: Review and analyze data for improvement opportunities• Routinely review and analyze data• Track progress against established targets
o Run charts, control charts, dashboards, scorecards
• Prioritize and act upon identified issues

SAFE = A (Access to Information)
Action 3: Data is shared on a regular basis to promote system-wide learning and transparency• Share vertically and horizontally• A story with worth 1,000 data points

SAFE = F (Facility Expectations)
Action 1: Leadership establishes and communicates clear expectations• All staff informed of expectations• Culture supports speaking up/stopping the line• The “stop the line” process clearly outlines:
o When to stop the lineo How to stop the line (verbal/non-verbal cue)o The chain of command to follow if not supported in
stopping the lineo Clear communication to staff from managers and
leadership that staff will be supported if they speak up

SAFE = F (Facility Expectations)
Action 2: Education for HCP and prescribers• Orientation • Annually

SAFE = F (Facility Expectations)
Action 3: Establish a structured communication process • Structured communication tools, e.g., Situation,
Background, Assessment, Recommendation (SBAR); isolation signage
• A structured hand-off process (what should be communicated; how?)o During shift changeo Between departments/unitso To other facilities
SAFE = F (Facility Expectations)
Action 4: Disclose unanticipated events• Promptly inform patients/families when an
unanticipated event occurs that has potential to contribute to an HAI
• Establish who should discuss with the patient/family and how
• Provide training and support to staff oneffective disclosure strategies
• Keep patient/family updated

SAFE = E (Engagement of Pts/Families)
Action 1: Educate and empower patient/ families• Address any barriers to patient/family
understanding their role in HAI prevention o Cultural, language, hearing impairment, health literacy
• Educated on their role and what they can expect to see from caregivers
• Assess patient /families’ level of understanding e.g., teach back
• Encourage “speaking up”

Building Blocks – Hand Hygiene

Building Blocks – Transmission Precautions

Building Blocks – Antimicrobial Stewardship

Building Blocks – Injection Practices

Building Blocks – Environmental Cleaning

Topic Specific Gap Analyses

Topic Specific Gap Analyses

Topic Specific Gap Analyses

Topic Specific Gap Analyses

Topic Specific Gap Analyses

Thresholds
Each infection topic area will have a process and outcome threshold
Thresholds incorporated into the dashboard and in the Registry home page
Goal: Assist in prioritizing efforts The Patient Safety Registry will automatically
recognize if thresholds are being met and provide a visual indication
If exceeding process and outcome thresholds, visual indication that threshold is met

ThresholdsHealthcare Acquired Conditions
Healthcare-Associated Infections
Process Measures SAFE from HAI Roadmap
Outcome Measure Infection Rates
Thresholds 1) SSI and CAUTI = TBD (per NHSN)2) VAP and CLABSI = 0
Source MHA patient safety registry, Calls to Action; NHSN
Criteria 1. ≥90% Safe from HAI Roadmap for 2 consecutive quarters
2. Rates below target
Actions - If criteria met Monitor rates, if above target, begin quarterly roadmap updates
Actions - If criteria not met Continued participation and quarterly updates for Safe from HAI

Data Submission Schedule
HAI Roadmap Data Updates • Submit quarterly with other roadmap updates• Baseline due September 30 (Grace-period -
October 14th) Outcome Data• Setting up agreement with hospitals submitting to
NHSN designating MHA as user-group

Outcome measures
Current mandated state reporting (through MHA maintained website)• VAP bundle• Central Line Insertion bundle • Surgical Site Infections (SSI) for Total Knee and Vaginal
Hysterectomy
Federally IPPS hospitals report through NHSN:• Central line infections• SSIs (including colon and abdominal hysterectomy) • More in coming years
Outcome measures
Move to align state and federal reporting• Discontinue reporting through MHA site• Begin reporting through NHSN
o January 1st, 2013 for IPPS hospitals
• Determine approach for non-IPPS facilities:o A staggered approacho Allow time for training and support of NHSN systemo Consider attestation for low volume procedureso Tentative goal of first reporting for non-IPPS hospitals
will be starting July 1st, 2013

Roadmap Data Submission

Roadmap Data Submission

Roadmap Data Submission

Roadmap Data Submission

Roadmap Data Submission

New Hospital Reports – Action Plan

New Hospital Reports: Progress Report

New Hospital Reports: Section Report
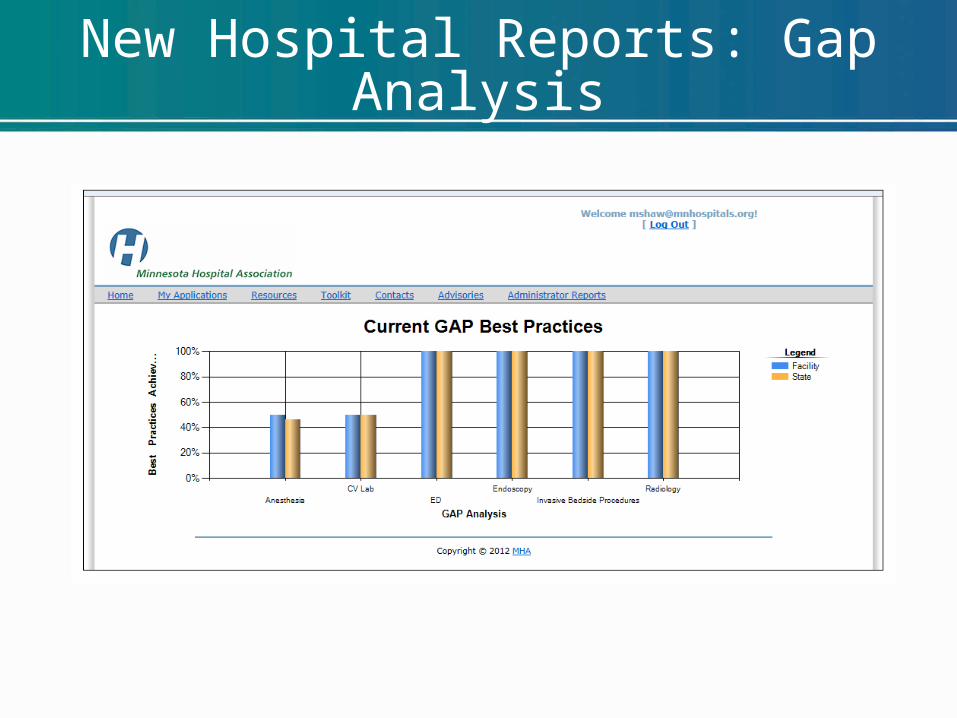
New Hospital Reports: Gap Analysis
Dashboards
Patient Safety Dashboards are sent to CEOs quarterly
Gradual expansion of Dashboard HAI Roadmap and Outcome data targeted to
be included in dashboard 4th quarter 2012

Next Step for SAFE from HAI Sign-up for SAFE from HAI initiative• Designate key contact• Receive access to Patient Safety Registry for data
submission
Complete SAFE from HAI Baseline by September 30th• Use Gap Analysis Report to begin addressing gaps
Participate in Activities• Listserv (automatically enrolled if in SAFE
from HAI)• Webinars/educational opportunities
Update SAFE from HAI Roadmap quarterly

Questions?
Top Related