






Languages
Pages
Legal


It Will Work: The First Successful Mitral Valve Replacement Nina S. Braunwald, MD Division of Cardiac Surgery, Brigham and Women’s Hospital, Boston, Massachusetts
In 1959, a prosthetic mitral valve of flexible polyurethane with Teflon chordae tendineae was designed and fabri- cated. After a series of experiments in dogs carried out at the Clinic of Surgery at the National Heart Institute, on March 11, 1960, this valve was used as a total replace- ment of the mitral valve of a 44-year-old woman with
mitral regurgitation. After an uneventful postoperative course, she was discharged from the hospital and did well thereafter, but died suddenly, presumably of an arrhythmia, 4 months after operation.
(Ann Thorac Surg 1989;48:S1-3)
he environment in which we train and the scientific T problems of the time help to shape the course of the kind of research problems that we tackle. I completed my residency training in General Surgery as Chief Resident at Georgetown University Medical Center at a time when Charles Hufnagel, newly arrived from Boston, was using a methyl methacrylate ball valve prosthesis in the de- scending aorta for the treatment of aortic regurgitation. Armed with a core knowledge of biomaterials and heart valve modifications and graduate training in tissue trans- plantation, I was offered and accepted a staff position and my own laboratory in the Clinic of Surgery of the intra- mural program of what was then the National Heart Institute.
Together with another then-young investigator, The- odore Cooper, later Assistant Secretary of Health and now Chief Executive Officer of Upjohn, I began laboratory investigations on the development of a prosthesis that would completely replace the mitral valve at a time when patients with end-stage mitral regurgitation were dying regularly despite vigorous medical treatment.
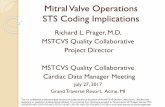
Material and Methods Using hearts from animals and humans, plaster casts were made of normal mitral valves, the annulus, and the tissue around the atrioventricular junction. Using a plastic steel called Devcon, two-piece molds from which the finished valves were to be fabricated were made. A thin Dacron locked knit fabric was stretched over the male half of the mold and cemented in place, and the female half of the mold was filled with an open cell liquid polyurethane 111. The mold was closed while the polymer was setting to assure that the leaflets would remain thin. Woven Teflon fabric chordae tendineae, made specially for us by the U.S. Catheter Co, were sewn to the valve leaflets (Fig 1).
During the developmental phase of the work, valve
Presented at the World Congress on Heart Valve Replacement, San Diego, CA, Jan 15-18, 1989.
Address reprint requests to Dr Braunwald, Brigham and Women’s Hos- pital, 75 Francis St, Boston, MA 02115.
function was tested in the laboratory using a pulse dupli- cator modeled on the one described by Davila and col- leagues [2]. The fabricated valve was sewn into hearts obtained at autopsy. This permitted leaflet motion to be correlated with atrioventricular distention at various pulse rates and left atrial pressures. It soon became evident that the length of the artificial chordae was crucial in assuring valve competency with a prosthesis in which the leaflets were extremely pliable. If the chordae were too tight, the valve was rendered incompetent in the open position; if they were too loose, the leaflets prolapsed into the left atrium, again causing incompetence.
Once fabricated, the prosthesis was used to replace the mitral valve in 24 dogs with the aid of cardiopulmonary bypass, a technique that had been introduced into cardiac surgery a relatively short time previously. The left atrial pressure could be altered by adjusting the length of the artificial chordae. In surviving dogs, the left atrial pres- sure was found to be in the normal range. At the time of postmortem examination, a thin platelet fibrin deposit was seen covering the leaflets. After review of the prog- ress in the laboratory, the decision was made to employ this valve in a patient with end-stage mitral regurgitation in whom a reconstructive procedure was not possible
On March 11, 1960, with Dr Morrow at the table, I completely replaced the diseased mitral valve of a 44- year-old woman with the flexible open cell prosthetic mitral valve described.
The patient had had a heart murmur of mitral regurgi- tation since the age of 8 years and was in New York Heart Association functional class IV with severe congestive heart failure despite intensive medical management. Her valve was noted to be severely thickened and scarred; the left atrium and ventricle were huge. The prosthetic valves had been fabricated in several annulus sizes and an appropriate one was sewn into the mitral annulus using four equidistant tacking sutures; the suture line was completed with a running suture. The artificial chordae had been brought out of the left ventricular wall in the region of the papillary muscle through small stab wounds. After ending bypass and allowing the left ven-
13-51.
0 1989 by The Society of Thoracic Surgeons 0003-4975/89/$3.50

s2 BRAUNWALD FIRST SUCCESSFUL MITRAL VALVE REPLACEMENT
Fig 1 . The completed valve after at- tachment of the chordae tendineae. (Reproduced from [31 by permission of The C.V. Mosby Company.)
tricle to assume its normal dimensions and contractility, these chordae were fixed in place with Teflon felt pledgets (Fig 2). The leaflets were then fixed to the ventricular wall in diastole over Teflon felt pledgets.
After the patient was weaned from cardiopulmonary bypass, the left atrial pressure was in the normal range, confirming satisfactory valve function. A small diastolic pressure gradient across the prosthetic valve was noted at the conclusion of the procedure.
The patient made an uneventful recovery and was discharged fully ambulatory from the hospital on May 22, 1960, clinically improved. No precordial murmur was audible. Four months after operation, her referring cardi- ologist called to say that she had experienced arrhythmias and had died one day after being admitted to a local hospital for an arrhythmia. Her heart was returned to the National Institutes of Health for postmortem examina-
Ann Thorac Surg 1989;48:S1-3
tion. The leaflets of the prosthesis were thin and pliable, with a thin fibrinous deposit over the polyurethane sur- faces. The Teflon pledgets at the site of exit of the chordae tendineae on the ventricle were all well healed.
Comment During the course of developing an open cell polyure- thane leaflet mitral valve, it was appreciated that when the leaflets were made thin and pliable enough to provide minimal resistance to flow they would invert during systole, unless artificial chordae tendinae were used to restrict their motion. Once a technique was developed for optimizing tension on the chords in a beating heart, complete replacement of the mitral valve was achieved in a woman who was discharged from the hospital after an uneventful postoperative course. This was carried out at a
Fig 2 . (A) Fixation of the valve to the mitral annulus; the prosthesis is sutured to the annulus. ( B ) Appearance of the flexible polyurethane mitral valve prosthesis after insertion and adjustment of the artificial chordae tendineae. Reproduced from [31 by permission of The C . V . Mosby Company.

Ann Thorac Surg 1989;48S1-3
time in the history of open heart surgery when this operation (complete replacement of the mitral valve) had, to our knowledge, not been previously carried out, al- though other investigators were working on valve substi- tutes.
References 1. Akutsu T, Dreyer B, Kolff W. Polyurethane artificial heart
valves in animals. J Appl Physiol 1959;141045-51. 2. Davila JC, Trout RG, Summer JE, Glover RP. A simple
mechanical pulse duplicator for cinematography of cardiac valves in action. Ann Surg 1956;14354&51.
BRAUNWALD s3 FIRST SUCCESSFUL MITRAL VALVE REPLACEMENT
3. Braunwald NS, Cooper TC, Morrow AG. Complete replace- ment of the mitral valve. J Thorac Cardiovasc Surg 1960; 40:1-11.
4. Braunwald NS, Cooper TC, Morrow AG. Experimental re- placement of the mitral valve with a flexible polyurethane foam prosthesis. Trans Am SOC Artif Intern Organs 1960; 6:315-22.
5. Braunwald NS, Cooper T, Morrow AG. Clinical and experi- mental replacement of the mitral valve: experiences with the use of a flexible polyurethane prosthesis. In: Merendino KA, ed. Prosthetic valves for cardiac surgery. 1st Ed. Springfield, IL: Charles C Thomas, 1961:307.
Top Related