





Languages
Pages
Legal


Intraventricular HemorrhageIntraventricular Hemorrhage
John Baier MDJohn Baier MD

Incidence of IVHIncidence of IVH
Late 1970’s- 80’s Late 1970’s- 80’s 39-49%39-49% Late 1980’sLate 1980’s
– < 34 weeks< 34 weeks 19%19%– <1501 g<1501 g 16%16%
Still large problemStill large problem– 1.24% of 4 million births are < 1500 g1.24% of 4 million births are < 1500 g– 7400 infants per year sustain IVH7400 infants per year sustain IVH

Incidence of IVHIncidence of IVH
500-750g
751-1000g
1001-1500g
1501-2000g
0
10
20
30
40
50
60
70
80In
cid
en
ce
of
IVH
(%
)
500-750g
751-1000g
1001-1500g
1501-2000g

Developmental AnatomyDevelopmental Anatomy Bleeds originate in the subependymal germinal Bleeds originate in the subependymal germinal
matrixmatrix Site of neuronal and glial proliferationSite of neuronal and glial proliferation
– cerebral neuroblasts 10-24 weekscerebral neuroblasts 10-24 weeks– after 24 weeks cerebral astrocytes and oligodendrogliaafter 24 weeks cerebral astrocytes and oligodendroglia
Size decreases as fetus maturesSize decreases as fetus matures– 2.5 mm at 23-24 weeks2.5 mm at 23-24 weeks– 1.4 mm at 32 weeks1.4 mm at 32 weeks– disappears at 36 weeksdisappears at 36 weeks

Developmental AnatomyDevelopmental Anatomy
Arterial SupplyArterial Supply– Heubner’s artery Heubner’s artery
(branch of anterior (branch of anterior cerebral artery)cerebral artery)
– deep lateral striate deep lateral striate arteries arteries (middle (middle cerebral artery)cerebral artery)
– anterior choroidal anterior choroidal artery (internal carotid) artery (internal carotid)

Developmental AnatomyDevelopmental Anatomy
Venous drainageVenous drainage– medullary veinsmedullary veins
– choroidal veinchoroidal vein
– thalamostriate veinthalamostriate vein
– enters the enters the terminal vein terminal vein atat head of caudate head of caudate
– veins change direction veins change direction at at internal cerebral internal cerebral vein vein making a U turnmaking a U turn

Developmental AnatomyDevelopmental Anatomy
Capillary NetworkCapillary Network– large irregular vesselslarge irregular vessels– lined only with endotheliumlined only with endothelium– gelatinous matrixgelatinous matrix– as term approaches these vessels develop as term approaches these vessels develop
adventiaadventia

Why is this region prone to bleeding ?Why is this region prone to bleeding ?

Pathogenesis of IVHPathogenesis of IVH
Fluctuating cerebral blood flowFluctuating cerebral blood flow Increase in cerebral blood flowIncrease in cerebral blood flow Increase in cerebral venous pressureIncrease in cerebral venous pressure Decrease in cerebral blood flow and Decrease in cerebral blood flow and
reperfusion injuryreperfusion injury Platelet and coagulation defectPlatelet and coagulation defect Vascular factorsVascular factors

Fluctuating cerebral blood flowFluctuating cerebral blood flow
NormalNormal– even arterial pressure waveeven arterial pressure wave
» peak to peak systolic < 10% differencepeak to peak systolic < 10% difference
– cerebral blood flow parallels arterial wavecerebral blood flow parallels arterial wave FluctuatingFluctuating
– systolic and diastolic pressure vary beat to beatsystolic and diastolic pressure vary beat to beat– cerebral blood flow parallels arterial wavecerebral blood flow parallels arterial wave

Fluctuating cerebral blood flowFluctuating cerebral blood flow
Fluctuations of CBFFluctuations of CBF– ventilation ventilation
» out of synchronyout of synchrony
– PDAPDA
– hypercarbiahypercarbia
– hypovolemiahypovolemia
– high FiOhigh FiO22
– restlessnessrestlessness
improved by improved by neuromuscular blockadeneuromuscular blockade

Increase in cerebral blood flowIncrease in cerebral blood flow
intact cerebral autoregulation in term intact cerebral autoregulation in term infantsinfants
pressure passive cerebral autoregulation in pressure passive cerebral autoregulation in sick preterm infantssick preterm infants

Increased arterial BP occurs inIncreased arterial BP occurs in HypercarbiaHypercarbia StimulationStimulation Tracheal suctioningTracheal suctioning PneumothoraxPneumothorax Rapid volume expansionRapid volume expansion Exchange TransfusionExchange Transfusion Ligation of PDALigation of PDA SeizureSeizure DrugsDrugs
– mydriaticsmydriatics

Increased Cerebral Venous Increased Cerebral Venous PressurePressure
Caused byCaused by– asphyxiaasphyxia– labor and deliverylabor and delivery– respiratoryrespiratory
» pneumothoraxpneumothorax
» high PIPhigh PIP
» tracheal suctiontracheal suction
» respiratory mechanicsrespiratory mechanics

Decreases in Cerebral Blood Decreases in Cerebral Blood FlowFlow
Caused by asphyxia or hemorrhageCaused by asphyxia or hemorrhage– may be the required precedent for IVHmay be the required precedent for IVH– may be caused by less obvious factorsmay be caused by less obvious factors
» taking temperaturetaking temperature
» chest auscultationchest auscultation
» suctioningsuctioning
Ischemic changes in germinal matrixIschemic changes in germinal matrix– free radical productionfree radical production– can be reduced by superoxide dismutase in animal modelscan be reduced by superoxide dismutase in animal models

Platelets and coagulationPlatelets and coagulation
Uncertain role in IVHUncertain role in IVH Platelet-capillary functionPlatelet-capillary function
– 40% of VLBW infants have platelets < 100,00040% of VLBW infants have platelets < 100,000– IVH rate is greater in thrombocytopenic infantsIVH rate is greater in thrombocytopenic infants– increased PGI may interfere with platelet functionincreased PGI may interfere with platelet function
CoagulationCoagulation– common in VLBW infantscommon in VLBW infants– FFP may decrease IVH without changing coagulationFFP may decrease IVH without changing coagulation

Vascular FactorsVascular Factors Tenuous capillary integrityTenuous capillary integrity
– Remodeling capillary bedRemodeling capillary bed
– Deficient vascular liningDeficient vascular lining» absent muscle and collagenabsent muscle and collagen
– Large vascular and luminal areaLarge vascular and luminal area Vulnerability of matrix capillariesVulnerability of matrix capillaries
– Vascular border zoneVascular border zone» Between striate and thalamic arteriesBetween striate and thalamic arteries
– High metabolic activityHigh metabolic activity

Extravascular FactorsExtravascular Factors
Deficient vascular supportDeficient vascular support Increased fibrinolytic activityIncreased fibrinolytic activity Postnatal decrease tissue pressurePostnatal decrease tissue pressure

Changes in CBF with AsphyxiaChanges in CBF with Asphyxia Initially hypotension with decreased CBFInitially hypotension with decreased CBF
– ischemia to germinal matrixischemia to germinal matrix
– generation of free radicalsgeneration of free radicals
– injury of endotheliainjury of endothelia Resuscitation (PPV,Bicarbonate,volume etc)Resuscitation (PPV,Bicarbonate,volume etc)
– loss of cerebral autoregulationloss of cerebral autoregulation
– hypercarbiahypercarbia Increase in blood pressure and CBFIncrease in blood pressure and CBF Fluctuation of CBFFluctuation of CBF

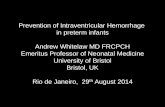
Ventilated Premature Infant with RDS
Decreases in CBF
FluctuatingCBF
Increases inCBF
Increases in cerebral venous
pressure
Capillary rupture
INTRAVENTRICULAR HEMORRHAGE
Vulnerable germinalmatrix capillaries
Extravascular:fibronolytic activity
Intravascular:platelet/capillary and/orcoagulation disturbances
Endothelial injury(+/- prior decrease in
CBF)

Pathogenesis of Pathogenesis of Intraparenchymal HemorrhageIntraparenchymal Hemorrhage
Terminal vein passes Terminal vein passes through germinal through germinal matrixmatrix
Increased pressure Increased pressure from germinal matrix from germinal matrix hemorrhage obstructs hemorrhage obstructs venous flowvenous flow
venous infarctionvenous infarction

Timing of IVHTiming of IVH
Postnatal DayPostnatal Day % infants with IVH% infants with IVH
11 50 50
22 25 2533 15 15
4+4+ 10 10

Clinical features of IVHClinical features of IVH
3 clinical presentations3 clinical presentations– catastrophiccatastrophic– saltatorysaltatory– silentsilent

Clinical features of IVHClinical features of IVH
Catastrophic Syndrome (least common)Catastrophic Syndrome (least common)– evolution over minutes to hoursevolution over minutes to hours
– Stupor or comaStupor or coma
– arrhythmias, hypoventilation and apneaarrhythmias, hypoventilation and apnea
– Generalized seizures and “Decerebrate posturing”Generalized seizures and “Decerebrate posturing”
– Fixed Pupils, eyes fixed to vestibular stimulationFixed Pupils, eyes fixed to vestibular stimulation
– Flaccid quadriparesisFlaccid quadriparesis

Clinical features of IVHClinical features of IVH
Catastrophic syndromeCatastrophic syndrome– falling hematocritfalling hematocrit– bulging anterior fontanellebulging anterior fontanelle– hypotension and bradycardiahypotension and bradycardia– temperature changestemperature changes– SIADH and very rarely DISIADH and very rarely DI– Outcome generally poor because of associated Outcome generally poor because of associated
large intraparenchymal bleedslarge intraparenchymal bleeds

Clinical features of IVHClinical features of IVH
SaltatorySaltatory– more subtlemore subtle
– alteration in level of consciousnessalteration in level of consciousness
– change in movement (decrease)change in movement (decrease)
– hypotoniahypotonia
– minor changes in eye movementsminor changes in eye movements
– decreased popliteal angledecreased popliteal angle
– outcome more favorableoutcome more favorable» depends of degree of underlying IVHdepends of degree of underlying IVH

Clinical features of IVHClinical features of IVH
Clinically silentClinically silent– symptoms may not be detected on routine examsymptoms may not be detected on routine exam– 50% of cases of IVH50% of cases of IVH– unexplained fall in hematocritunexplained fall in hematocrit

Clinical Staging of IVHClinical Staging of IVH
PapilePapile II bleeding confined to subependymableeding confined to subependyma IIII intraventricular bleed without dilationintraventricular bleed without dilation IIIIII intraventricular bleed with dilationintraventricular bleed with dilation IVIV parenchymal bleedparenchymal bleed

Clinical Staging of IVHClinical Staging of IVH
II bleeding confined to subependymableeding confined to subependyma IIII intraventricular bleed without dilationintraventricular bleed without dilation IIIIII intraventricular bleed with dilationintraventricular bleed with dilation Periventricular Intraparenchymal Periventricular Intraparenchymal
Echodensity (IPE) Echodensity (IPE)

Outcome of IVHOutcome of IVH
AcuteAcute– seizuresseizures– acute hydrocephalusacute hydrocephalus– intracranial hypertensionintracranial hypertension– deathdeath

Outcome of IVHOutcome of IVH
Long Term Long Term – neurologic impairmentneurologic impairment
» motormotor
» sensorysensory
– developmental impairmentdevelopmental impairment» cognitivecognitive
» related to sensory deficitsrelated to sensory deficits
– hydrocephalushydrocephalus

Neurologic Impairment in IVHNeurologic Impairment in IVH
Incidence of impairment related to degree of IVHIncidence of impairment related to degree of IVH
Incidence ofIncidence of
Severity Severity Neurological sequelaeNeurological sequelae
MildMild 5% 5%
ModerateModerate 15 % 15 %
SevereSevere 35 % 35 %
Severe + IPESevere + IPE 90 % 90 %

Neurologic Impairment in IVHNeurologic Impairment in IVH
Outcome is also related to extent of IPEOutcome is also related to extent of IPE
OutcomeOutcome Extensive IPEExtensive IPE Localized Localized IPEIPE
MortalityMortality 81 % 81 % 37 %37 %
Major Motor abn Major Motor abn 100 %100 % 80 %80 %
IQ < 80IQ < 80 85 % 85 % 53 %53 %
““Normal”Normal” 00 10 %10 %

Motor Problems in IVHMotor Problems in IVH Periventricular lesion Periventricular lesion
affects fibres from both affects fibres from both upper and lower upper and lower extremities extremities – Spastic hemiparesis Spastic hemiparesis
(unilateral)(unilateral)
– Spastic quadraparesis Spastic quadraparesis (bilateral)(bilateral)

Pathogenesis of Brain Injury in IVHPathogenesis of Brain Injury in IVH Preceding hypoxic-ischemic injuryPreceding hypoxic-ischemic injury
– PVLPVL
– pontine hemorrhagepontine hemorrhage
Destruction of glial precursors in germinal matrixDestruction of glial precursors in germinal matrix– effects on mylenationeffects on mylenation
– cerebral organizationcerebral organization
Destruction of periventricular white matterDestruction of periventricular white matter– infarctioninfarction
– intraventricular bloodintraventricular blood» potassium potassium
» glutamateglutamate
» vasoactive compoundsvasoactive compounds

Pathogenesis of Brain Injury in IVHPathogenesis of Brain Injury in IVH
Arterial vasospasm with focal brain Arterial vasospasm with focal brain ischemiaischemia
HydrocephalusHydrocephalus

HydrocephalusHydrocephalus
Progressive ventricular dilation secondary Progressive ventricular dilation secondary to alteration in CSF dynamicsto alteration in CSF dynamics
Distinguish from ventriculomegaly with Distinguish from ventriculomegaly with normal CSF dynamicsnormal CSF dynamics– atrophy “hydrocephalus ex evacuo”atrophy “hydrocephalus ex evacuo”
» PVLPVL
» IPEIPE

Pathophysiology of Pathophysiology of HydrocephalusHydrocephalus
most are communicatingmost are communicating– chronic obliterative arachnoiditis (most chronic obliterative arachnoiditis (most
common)common)– obstruction of aqueduct by blood, clot and obstruction of aqueduct by blood, clot and
debris (infrequent)debris (infrequent)

Clinical Aspects of Clinical Aspects of HydrocephalusHydrocephalus
onset 1 - 3 weeks after IVHonset 1 - 3 weeks after IVH rapidity of progression relates to degree of rapidity of progression relates to degree of
IVHIVH Head growth and signs of increased ICP Head growth and signs of increased ICP
follow ventricular dilationfollow ventricular dilation– days to weeksdays to weeks
Posterior horn dilate earlier and greater than Posterior horn dilate earlier and greater than anterior hornsanterior horns

Management of HydrocephalusManagement of Hydrocephalus
MedicalMedical– acetazolamide with or with out furosemideacetazolamide with or with out furosemide– serial lumbar puncturesserial lumbar punctures– serial ventricular puncturesserial ventricular punctures
SurgicalSurgical– ventriculostomyventriculostomy– Rickham reservoirRickham reservoir– VP or subgaleal shuntVP or subgaleal shunt

Prevention of HydrocephalusPrevention of Hydrocephalus
Intraventricular injection of tPA may reduce Intraventricular injection of tPA may reduce the incidence of hydrocephalusthe incidence of hydrocephalus
only a single small pilot studyonly a single small pilot study

Prevention of IVHPrevention of IVH
Antenatal and PerinatalAntenatal and Perinatal– PREVENTION OF PREMATURE BIRTHSPREVENTION OF PREMATURE BIRTHS– Maternal Transfer to high risk facilityMaternal Transfer to high risk facility– Maternal PhenobarbitalMaternal Phenobarbital– Maternal Vitamin KMaternal Vitamin K– Maternal SteroidsMaternal Steroids– Management of Labor and DeliveryManagement of Labor and Delivery
» breech delivery or prolonged laborbreech delivery or prolonged labor
» ? CS? CS

Prevention of IVHPrevention of IVH
Maternal PhenobarbitalMaternal Phenobarbital– controversial (now largely abandoned)controversial (now largely abandoned)
» treated infants were more illtreated infants were more ill
» lower BP required increased fluidslower BP required increased fluids
– may decrease incidence of severe IVHmay decrease incidence of severe IVH– may increase need for ventilation at birthmay increase need for ventilation at birth– may increase RDSmay increase RDS

Prevention of IVHPrevention of IVH
Maternal Vitamin KMaternal Vitamin K– vitamin K administered 4 hours prior to deliveryvitamin K administered 4 hours prior to delivery– vitamin K administered to all infants at birthvitamin K administered to all infants at birth– PT normal in treated (67% normal in controls)PT normal in treated (67% normal in controls)
» IVH was not related to PTIVH was not related to PT
– incidence of IVH was decreased in two studiesincidence of IVH was decreased in two studies

Prevention of IVHPrevention of IVH
Antenatal glucocorticoidsAntenatal glucocorticoids– currently in favorcurrently in favor– significant reduction in IVHsignificant reduction in IVH– reduction in degree not incidence of HMDreduction in degree not incidence of HMD– may relate to brain maturationmay relate to brain maturation
» glucocorticoids mature other organ systemsglucocorticoids mature other organ systems
» gut and respiratory tractgut and respiratory tract

Prevention of IVHPrevention of IVH
NeonatalNeonatal– Resuscitation must be prompt and adequateResuscitation must be prompt and adequate
» avoid hypercarbia and hypoxemiaavoid hypercarbia and hypoxemia
– Avoid rapid infusion of volume expanders and Avoid rapid infusion of volume expanders and hypertonic solutionshypertonic solutions
– Correction of fluctuation in cerebral blood flow velocityCorrection of fluctuation in cerebral blood flow velocity» paralysisparalysis
» however not easy to identify which infants have this however not easy to identify which infants have this fluctuationfluctuation

Prevention of IVHPrevention of IVH
NeonatalNeonatal– Prevention and treatment of hemodynamic aberrationsPrevention and treatment of hemodynamic aberrations
» apneaapnea
» acute hypercarbia (COacute hypercarbia (CO22) > 60 mm Hg ) > 60 mm Hg
» pneumothoraxpneumothorax
» suctioningsuctioning
» rapid transfusionsrapid transfusions
» inotrope useinotrope use
» exchange transfusionsexchange transfusions

Prevention of IVHPrevention of IVH
NeonatalNeonatal– Correction of abnormal coagulationCorrection of abnormal coagulation
» unclear dataunclear data
– PhenobarbitalPhenobarbital– IndomethacinIndomethacin– EthamsylateEthamsylate– Vitamin EVitamin E

Prevention of IVHPrevention of IVH
PhenobarbitalPhenobarbital– not currently usednot currently used– largest controlled study showed worse outcome largest controlled study showed worse outcome
in treated infantsin treated infants

Prevention of IVHPrevention of IVH IndomethacinIndomethacin
– effect first noted in studies to prevent symptomatic PDAeffect first noted in studies to prevent symptomatic PDA– decreases baseline cerebral blood flow decreases baseline cerebral blood flow – attenuates cerebral hyperemia in asphyxiaattenuates cerebral hyperemia in asphyxia– may be deleterious if hypotension occursmay be deleterious if hypotension occurs
» decreased oxidized cytochrome oxidasedecreased oxidized cytochrome oxidase» decreased cerebral intracellular oxidationdecreased cerebral intracellular oxidation
– inhibits free radical formationinhibits free radical formation– may accelerate maturation of germinal matrixmay accelerate maturation of germinal matrix

Prevention of IVHPrevention of IVH
Ethamsylate (not available in US)Ethamsylate (not available in US)– inhibits prostaglandin synthesis distal to cyclo-oxygenaseinhibits prostaglandin synthesis distal to cyclo-oxygenase
» inhibits prostacyclin predominatelyinhibits prostacyclin predominately
» does not affect cerebral blood flowdoes not affect cerebral blood flow
– polymerization of hyaluronic acid in basement membranespolymerization of hyaluronic acid in basement membranes– promotes platelet adhesivenesspromotes platelet adhesiveness– placental transferplacental transfer
» ??? antenatal use??? antenatal use

SummarySummary IVH remains a significant problem in the NICU despite IVH remains a significant problem in the NICU despite
recent improvements in carerecent improvements in care Pathogenesis include anatomical susceptibility and Pathogenesis include anatomical susceptibility and
pathologic changes in CBF pathologic changes in CBF Incidence varies with gestational ageIncidence varies with gestational age Prognosis depends on clinical stagePrognosis depends on clinical stage Current therapies are unsatisfactory and prevention Current therapies are unsatisfactory and prevention
remains the best way to reduce the incidence and impact remains the best way to reduce the incidence and impact of IVHof IVH
Top Related