







Languages
Pages
Legal

Integrating Behavioral Health and Physical Health:
The Time is Now
Introductions
Noreen Fredrick Executive Director Mon Yough Community Services McKeesport, PA
Stephen Christian-Michaels COO Family Services of Western Pa New Kensington, PA

Overview
Health Status of People with SPMI Fractured System Models of Integration Chronic Care Model Impact Model Person Centered Healthcare Home Cherokee Model – CMHC/FQHC Research Based Best Practice Components Types of Integration Initiatives Family Services of W. Pa Experience Mon Yough Experience
Health Status of People with Serious Mental Health Diagnoses
High prevalence of modifiable risk factors:
Obesity; tobacco use and alcohol use
Group homes -- exposure to infectious diseases
-- peers negatively influencing unhealthy risk factors
60% of premature deaths in individuals with schizophrenia due to:
cardiovascular disease pulmonary infectious diseases
Higher rates of COPD and Diabetes than in the general population
Premature death - 25 years younger than the general population.
Medication side effects often exacerbates health status
Health Status of People with Serious Mental Health Diagnoses
Hispanics, African Americans or Asian and Pacific Islanders have varying disparities in death rates
The widest gap is seen in black males with a life expectancy of 69.5 years in 2004, 8.3 years shorter than the national average.
None have a life expectancy that is equivalent to those with serious mental illness. 25 years……..
This disparity is alarming
Health Status of People with Serious Mental Health Diagnoses
Adults in Health Choices: Annual increases: 24% - 28% (new consumers)
Have not previously used services In addition to already burgeoning caseloads
Main Diagnoses 27% major depression 23% schizophrenia 15% bipolar disorder 15% other depressive disorders
About 40% co-occurring 51% MH only 6% substance abuse/dependence only

Health System is a Fractured System
People not identified w/depression early enough
Post Partum Depression often not diagnosed
75% Anti-Depressant meds prescribed by PCP’s
PCP’s often discontinue anti-depressant before full effect is realized

Community Mental Health/Primary Care Split
•Consumers not engaged with PCP…… …….use Emergency Departments for routine care
•PCP’s often feel unprepared to deal with behavioral health
disorders
•PCP’s frustrated when they refer into CMHC’s long waiting lists, drop out’s before first appointment/soon after
•CMHC’s feel unprepared to deal with even routine health issues
•CMHC’s busy, refer people back to PCP’s for depression, ADD, etc
•No infrastructure readily available to enhance communication
•Difficult for real communication given busy schedules

What contributes to the Fractured Health System
Billing systems are different
Evolving EHR are usually separate w/no interfaces
BH is carved out of managed care plans
Referrals from PCP’s tend to be to MD’s they know
Psychiatry is the lowest paid specialty of physicians
Psychiatry/Therapy split off from medicine
Integrated Care: To Be Or NOT
Models of integration Separate Locations – Coordinated cross referral Co-Location – BH on site, parallel practice Integrated/Joint Care – separate but combined Integrated Centers - Fiscally and Structurally Integrated Health Systems – Kaiser HMO
5 Years from now in a reformed healthcare system there may not be a role for CMHC’s that are not involved in Integrated Care

Characteristics of Current System
Current care is crisis driven
Provider centric not patient/consumer centric
Care is episodic and reactive
There is not a life time view of disorders
Care tends to be more modality driven, not population driven

Chronic Care: A Model to Assist in Integration
Developed by Edward H. Wagner, MD, MPH MacColl Institute for Healthcare Innovation
Organized, planned & productive interactions improve outcomes: More fully engage individual is in self care activities and Leads to better health outcomes.
People w/SMI share same characteristics as chronic physical conditions:
dealing with symptoms disabilityemotional impact family issuescomplex medication regimens difficult lifestyle adjustments
difficult to obtain helpful care
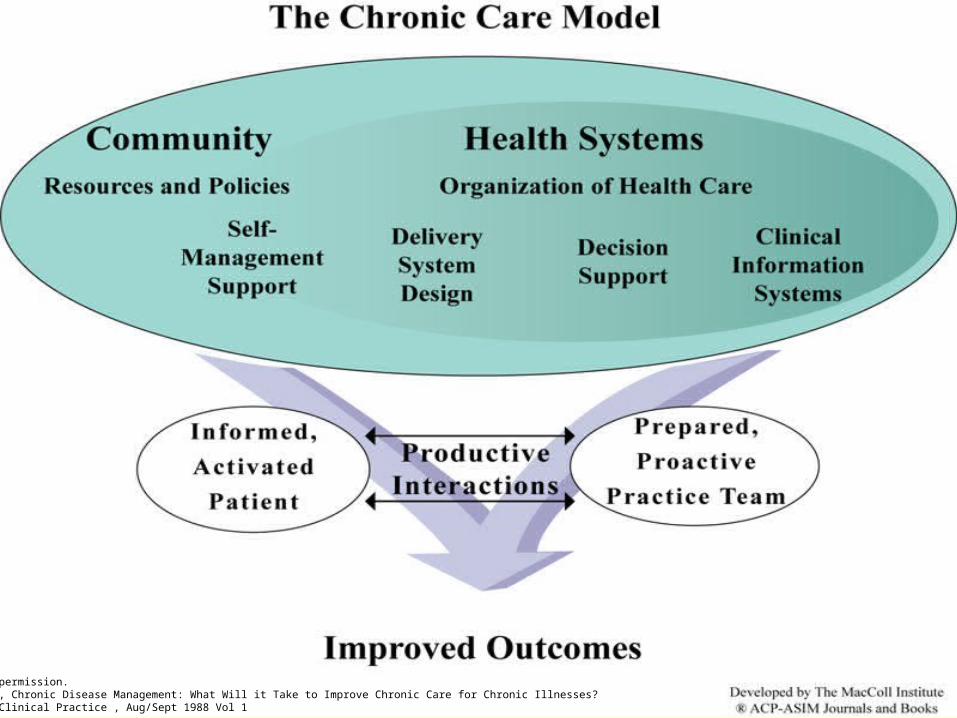
Used with permission.Wagner, E., Chronic Disease Management: What Will it Take to Improve Chronic Care for Chronic Illnesses?Effective Clinical Practice , Aug/Sept 1988 Vol 1

Essential Element of Good Chronic Illness Care
Informed,Activated
Patient
ProductiveInteractions
PreparedPractice
Team
Used with permission.Wagner, E., Chronic Disease Management: What Will it Take to Improve Chronic Care for Chronic Illnesses?Effective Clinical Practice , Aug/Sept 1988 Vol 1

What characterizes an “informed, activated patient”?
Informed,Activated
Patient
They have the motivation, information, skills,They have the motivation, information, skills, and confidence necessary to and confidence necessary to
effectively make decisions abouteffectively make decisions about their health and manage it.their health and manage it.
Used with permission.Wagner, E., Chronic Disease Management: What Will it Take to Improve Chronic Care for Chronic Illnesses?Effective Clinical Practice , Aug/Sept 1988 Vol 1

What characterizes a “prepared” practice team?
PreparedPractice
Team
At the time of the interaction they have At the time of the interaction they have the patient information, decision support, and the patient information, decision support, and
resources necessary to deliver resources necessary to deliver high-quality care. high-quality care.
Used with permission.Wagner, E., Chronic Disease Management: What Will it Take to Improve Chronic Care for Chronic Illnesses?Effective Clinical Practice , Aug/Sept 1988 Vol 1

Six Components of Chronic Care Model
Self-Management Support – individuals are supported in achieving goals and fully engaged in care.
Delivery System Design – transform practice form reactive to planned and proactive.
Decision Support - care is based on evidence based guidelines and uses systems to inform and prompt providers and individuals about care needs.

Six Components of Chronic Care Model
Clinical Information Systems – use of registries to provide patient specific and population based support to teams, reminders, data and provider feedback. With the correct tools providers can analyze all of their consumer needs, access recent lab work, prescriptions filled, and visits.
Community – utilize resources in the community. This is a natural strength for the CMHC with integration existing as part of the community supports.
Health System – creation of a quality oriented system through leadership and continuous quality improvement.

Four Quadrant Integrated Care Model
The NCCBH proposed model for the clinical integration of health and behavioral health services starts with a description of the populations to be served.
• Quadrant I: Low MH - Low PH, served in primary care BH staff on-site provides services
• Quadrant II: High MH - Low PH, served in the MH system PH service provided at CMHC
• Quadrant III: Low MH - High PH, served in primary care BH staff on-site provide services PH case mgt provided
• Quadrant IV: High MH - High PH, served in MH system with specialty care case management for both PH and BH disorders National Council for Community Behavioral Healthcare
The Person-Centered Healthcare Home
Stepped care clinical approach
Healthcare implemented bi-directionally
A. Identify people in primary care with behavioral health conditions ands serve them there unless they need stepped specialty behavioral health care; and
B Identify and serve people in behavioral health care that need routine primary care and step them to full-scope health care home for more complex care
www.TheNationalCouncil.org/ResourceCenter

Impact Model - Depression
Collaborative care – individual PCP’s works with BH care manager/behavioral health consultant to implement a treatment plan with consultation with the psychiatrist and pharmacist
Depression Screen of all Patients in Medical Practice Motivational Interviewing, Behavioral Activation and
Problem Solving Therapy Goal is to make incremental changes in life style practices Medication prescribed by PCP Health registry used to
Prompts follow-up sessions, outreach, staged interventions Collects medical and behavioral health data Tracks changes, outcomes
Cherokee Model
Fully integrated structurally and financially Combined Services
Community Mental Health Center Federally Qualified Health Center
National Council for Community Behavioral Health Care
Federally Qualified Health CentersPossible Structures FQHC and CMHC merged to one organization
Federally Qualified Health Centers provides its own BH services via its own staff = integrated team
Funding from one stream, One EHR
Federally Qualified Health Centers with contracted CMHC services integrated
CMHC co-locates staff at FQHC and provides BH services in a parallel practice…one stop shop
Research Based Best Practice Components
Regular screens & registry tracking/outcome measurement
Medical nurse practitioners/PCP located in BH clinic
Primary care supervising MD
Embedded RN care manager
Evidenced based practices to improve health of SMI pop.
Wellness programs
National Council of Community Behavioral Health Care

Integration Initiatives
Screening of Depression for all PCP patients (PHQ-9)
Screening for Unhealthy Substance Use (SBIRT)
Screening of Post Partum Depression – OB and Pediatricians Depression Screening, Motivational Interviewing,
Behavioral Activation, Problem Solving Therapy (IMPACT)
Medical Services provided in MH Centers
Challenges
We need to be part of putting the mind and body back together
Healthcare reform is going to drive more focus on integration

Family Services Experience
Co-location
Integrated Care, BH service at Medical Clinic
Proposed Medical Services at CMHC
Family Services – Co-Location
MD Frustration at long waiting time to see Psychiatrist
MH CRNP at Family Practice office in New Kensington (UPMC) Started at ½ day/week, moved to two half days per week
50 – 75 new clients seen per year
Moderate Depression, often linked to MH Clinic
Very little collaborative care
Some phone consultation between MD and Psychiatrist
Family Services – Integrated Care at Medical Clinic
Partnership matured Agreed to seek out funding to move to integrated care Together support regional Integrated Care Summit mtg Family Practice-UPMC started screening for Depression Applied for several grants, not funded Approached Managed Care Company Managed Care – Health/BH – funded project/collect data
Family Services – Integrated Care at Medical Clinic
Foundation sought out partnership along with 3 other sites Goals:
Establish communication policies between medical & BH Providers Increase the appropriate assessment & utilization of BH services Decrease:
Emergency Department usage hospital admissions Re-admissions Hospital length of stays
Assure that BH provider is a financially viable position
Family Services – Integrated Care at Medical Clinic IMPACT/Depression Screening SBIRT/Unhealthy Substance Use Screening Engagement/Behavioral Activation/Problem Solving
Treatment Grant fund position for 18 months
Goal: Demonstrate ability to reduce by 6 inpatient hospital admits
Pgh Regional Healthcare Initiative provides consult/project mgt
University of Washington/IMPACT provides Training Consultation Health Registry

Family ServicesMedical Services at CMHC SAMHSA Proposal Family Practice staff contracted to provide medical services MD, Nurse Practitioner and Nurse become part of MH Teams Build a physical fitness center at CMHC Peer support used to engage consumers in healthy lifestyles Build EHR Interfaces to share summary notes Build Health Registry into BH EHR to implement Chronic Care Model Change physical layout of office for (4) interdisciplinary teams Services:
Health Screening, Nutrition Counseling, Fitness Groups Health Improvement plans, Consultation, Care Mgt

Mon Yough ExperienceSAMHSA Grant: Emerg Dept Diversion Partners:
UPMC for Life UPMC McKeesport Hospital Latterman Family Health clinic UPMC McKeesport Internal medicine MYCS
Goal: Decrease Emergency Department usage Determined Access as the issue Increased midlevel practitioner time at Latterman and
MYCS as we agreed that we all serve the same group of clients

Mon YoughEvolution of the Partnership Grant led to beginning of “partnership model” between
Latterman Family health and MYCS. CRNP .5 FTE located in Behavioral health clinic Primary care supervising physician Imbed Psych Rehab in clinic setting to promote wellness as
core goals and work with nursing staff to structure wellness activities
Next Steps: Create registry tracking Embed evidenced based practice in daily practice
Mon YoughChronic Care Model CMHC Development of a “chronic care” team
within adult Outpatient clinic
Co-locate treatment; psych rehab,
supported employment and service
coordinator in one area
PH and BH team live in the same building

Mon YoughPerinatal Depression Project
Rand project – targeting perinatal depressed Moms in a variety of settings including OB clinic; pediatricians
MYCS partnered with Magee in Clairton Behavioral health time provided on site Lessons learned… Helped with imbedding of BH case manager in Latterman
clinic to assess need /level of support and type of integration Next Step use existing “SHIP” infrastructure to create
collaboration among community using logic model approach
Mon YoughTraining the Work Force
Latterman Clinic is a Family Practice education site. MYCS will serve as the rotation site for dual boarded
Family Practice/Psych Fellowship 4 hours a week Latterman Clinic
Provide physical health care in MYCS clinic Provide supervision of primary care at MYCS clinic
MYCS will serve as the psych rotation education site for Family Practice Residents

Learning Collaborative
Set up learning collaboratives Use consultants to help cross walk systems Share information across projects Examples:
Collaborative learning across BH and PH Collaborative learning across CMHC’s List Serves on Integrated Care Regional Learning Collaboratives

Resources
Wagner, E., Chronic Disease Management: What Will it Take to Improve Chronic Care for Chronic Illnesses: Effective Clinical Practice, Aug/Sept 1988 Vol. 1
National Council of Community Behavioral Health Care. Winter 2009. A Two-Way Street Behavioral Health Care and Primary Care Collaboration.
Morbidity and Mortality in People with Serious Mental Illness, National Association of State mental Health program Directors, Medical Directors Council; Editors: parks, Svendson, Singer, Foti, Technical Writer: B Mauer. October 2006; Report available at www.namsmhpd.org
List Serve: http://lists101.his.com/mailman/listinfo/pc-bh-integration

Contact Information
Noreen Fredrick
(412) 673-8035
Stephen Christian-Michaels
(412) 820-2050 x438
Top Related