







Languages
Pages
Legal


INNOVATION:
Building the Culture &
Realizing the Benefits
Presented by:Rolando BarriosJulian MarsdenBarbara Trerise
National Healthcare Leadership ConferenceJune 6, 2011

2
Purpose
• Understand the approach Providence Health Care is
taking to building a culture of innovation
• Hear about the experience and some lessons learned on
the bleeding edge of innovation
3
Providence Health Care
• 6,000 staff
• 1,000 physicians
• 1,400 volunteers
• $709-million budget
• 8 sites + 7 community dialysis clinics
• 1,500 beds (acute, residential, rehab, assisted living and hospice)
• Academic Health Science Centre with PHC Research Institute

4

5
6
A nation’s (organization’s) culture resides in the hearts and in the souls of its people.
Mahatma Gandhi

7
Agenda
• Building an Culture of Innovation at Providence Health
Care
• Evidence to Excellence
• Immunodeficiency Clinic
• Lessons learned
• Questions

8
Quality and Safety Enablers
• Strategic directions and annual plans;
• Accountability and Performance Improvement Framework;
• Support infrastructure
• Quality and Lean, Change Initiatives, Administrative Decision Support, Safety, Practice Consultants and Infection Prevention and control, expert skills, accessible data and data analysis
• Organizational structure;
• Program management, executive responsibilities, committees, engaged board
• Capacity building;
• Team and leadership development, standard project management methodologies, visible CEO leadership, stakeholder engagement

9
“The organization demonstrates a strong commitment to quality
and safety and has developed this culture across the organization.
Providence Health Care is a model organization. It is evident…that
there is a culture of quality improvement. There is a systematic
process to understand, manage and communicate quality from a
system-wide perspective from the board level, to the leadership
team right to front line staff. The surveyors saw many examples of
quality improvements and innovation to improve work life and the
quality of patient care. Furthermore there is an awareness at all
levels of the tools that can be utilized to make improvements to
their areas.”
Accreditation Canada
November 2010

10
2010 Self Assessment
• Positive reputation – awards, examples of innovation,
sought out by others, lots of firsts, pockets of excellence
and innovation
• Pace of improvement is too slow
• Uptake of new knowledge is spotty and spread is difficult
• Lack of reliability
• No real priorities
• Reputation exceeds our current performance
• Relying on structures, methods and skills designed for a
different time and strategy

11

12
What is Innovation?
• No commonly agreed upon
definition
• A discovery and/or invention that:
• Is unique
• Has value, and is
• Worthy of spreading, exchanging with others, or commercialization

13
Perceptions of Executive Teams –Weiss & Legrand
Innovative
Org
Non-
innovative
Org
Innovation is important to organization’s
future success
95% 79%
Executives believe innovation is crucial 86% 24%
Executive team is an excellent example
of teamwork
67% 12%
Executives understand the process of
innovation
68% 6%
Executives role-model innovation
practices
68% 2%

14
Dimensions of a Culture of Innovation –What the Evidence Says….
• Performance orientation and everyone understands the
organizational direction
• Risk taking that adds value is expected and supported;
acceptance of failure
• Innovation is a priority and there is autonomy to try new things
• Executive team model the way and remove barriers
• Orientation to people and teams - enabled with trust, honesty,
transparency and diversity
• Balance innovative thinking with the discipline to implement
solutions

15
Seven Dimensions of a Culture of Innovation - NHS

16
THINK PHC
To transform the health of the populations we serve through innovative solutions and new knowledge

17
Aims of ThinkPHC
• To develop a model which will accelerate the pace, impact and spread of
change in support of quality improvement, financial and other
performance targets;
• To improve the quality of clinical care through accelerating the adoption
of research findings and new knowledge by care providers;
• To increase leadership, team capacity and skill to effectively engage in,
and sustain innovation
• To further PHC’s contributions to the health system through leading
practice and knowledge translation

18
Our approach …
• Executive consensus
• Board support
• Institute for Healthcare Improvement

19
IHI Recommendations Action/Next Steps
Assure leadership clarity of
purpose
Vision statement
Innovation strategy; strategic
planning process
Select the vital few aims Quality and safety foci:
• Patient centeredness
• Harm
• Reliability
Measures, drivers, detailed plans; what and how do we let go
Assure academic integration into
work and focus on physician
engagement
Research leadership and
engagement; R&D team
Innovation strategy

20
IHI Recommendations Action/Next Steps
Develop an innovation focus to
assure continuing projects and
plan for spread
R&D team
Spread plan
Align organization resources to
support the work
Leadership – VP, Corporate Director, ThinkPHC
Innovation Team - Change Initiatives, Accreditation, Administrative Decision Support, Quality; Practice
Improve organizational
practices to support and
assure a ‘Line of Site from
front line to executives and the
board
Effective Governance
Innovation strategy; assess risk; manage the whole as well as the parts; make the work visible through cascading strategies and metrics

21
Innovation Strategy• Culture of Innovation - Vision
• PHC has a reputation for its dynamic culture of innovation leading to excellent health outcomes. It is widely known for a "performance orientation" with a focused, rapid-paced approach to inquiry, innovation and implementation that other organizations wish to emulate.
• Plan
• Culture
• Quality and safety
• Effective Governance
• Leadership
• Academic integration
• Organizational practices
• Metrics

22
Acknowledgements
• Board of Directors
• Senior Leadership Team
• Innovation Team Directors
• Inspirational researchers and providers

Evidence 2 Excellence: BC Emergency Medicine Improvement Community
2011 National Healthcare Leadership Conference June 6th, 2011
Julian Marsden MD

A Collaborative Improvement Network:
To create a sustainable culture of improvement

A community of health care providers and administrators committed toexcellence in emergency health care for all British Columbians.

26
The Journey of E2E
1. Why E2E?
2. What is E2E?
3. How does it work?
4. What have we done?
5. What next?

27
Why was E2E created?
1. An opportunity to leverage all the good work that is already being done:
> Share and spread improvements across BC
> Accelerate improvements
2. Create new networks and partnerships to bridge:
> Rural-urban divide
> Interprofessional divide

What is E2E?

29
Implement & Spread
Sustain & Monitor
Design & Develop
Improvement Life Cycle

30
Implement & Spread
Sustain & Monitor
Design & Develop
Scope & Elements of E2E
Grassrootsdriven
Provincial Communit
y&
Network
Knowledge
Translation
Academic
Evaluation
Quality
Improvement
Adapt to local
context
Interprofession
al collaboration
MoHS Supported
(BC PSQC)
How does it work?

32
www.evidence2excellence.ca
Community of Practice
Homepage

33
The Collaborative Model
The Breakthrough Series: IHI’s Collaborative Model for Achieving
Breakthrough Improvement. IHI Innovation Series white paper. Boston: Institute for Healthcare Improvement; 2003. (Available on www.IHI.org)

34
Approval Process
• Topics chosen by the E2E community
• Involvement is voluntary
• Executive sponsorship required
> Responsibility of individual site or health authority
• All teams submit a monthly self assessment report of their progress against the collaborative action areas.

What have we done?
Our Successes

36
Website Usage
• ~700 resources posted
• YouTube video has 350+ views to date worldwide
2926
0
500
1000
1500
2000
2500
3000
Apr-
10
May-1
0
Jun-1
0
Jul-
10
Aug-1
0
Sep-1
0
Oct-
10
Nov-1
0
Dec-1
0
Jan-1
1
Feb-1
1
Mar-
11
Number of E2E Website Visits
Number of visits
Cumulative visits
2,570
109 100 26 11 5 3 3 2 2 10
500
1,000
1,500
2,000
2,500
3,000
Provincial Visits

37
2009-10 Collaborative Overview
Jan 2011Virtual
January 16th
2010Vancouver
March 25th
20103 hoursVirtual
May 28th 2010Partial
Attendance +Virtual
Oct 16th 2010Partial
Attendance +Virtual
Oct 2009
Jan 2010May –Oct 2010
Oct – Dec 2010

38
2008-2009 Collaboratives
• 36 teams from 26 sites>13 ED Sepsis Teams>23 ED Triage Teams

39
2009-2010 Collaboratives
• 38 teams from 26 sites�20 ED Flow Teams�18 Sepsis Teams
• 200 + TEAM MEMBERS registered• All Health Authorities represented
40
Province Wide Rounds
• E2E began hosting Provincial Wide Rounds in June 2010.
• WebEx presentations by key leaders in Sepsis research/care or improving ED Flow.
• Each talk attracted 100 participants.
Dr. Emanuel Rivers Dr. Derek AngusDr. Grant Innes
Mary Ackenhusen COO

41
Data Collection
• All teams submit a monthly self assessment report of their progress against the collaborative action areas.
• ED Flow
> Data obtained from Health Authority Decision Support to assess teams progress against the ED Flow goals
• Sepsis
> Sepsis teams manually collect data on patients that meet the criteria for Systemic Inflammatory Response Syndrome (SIRS)

42
Team Self Assessment (Sepsis)
Self Assessment Scale
1.0 Forming a team
1.5 Planning for project begun
2.0 Activities but no changes
2.5 Changes tested - no improvement
3.0 Modest improvement
3.5 Improvement
4.0 Significant improvement
4.5 Sustained improvement
5.0 Outstanding

43
Team Self Assessment (ED Flow)
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
5.0
% o
f te
am
s re
po
rtin
g
AV
E S
elf
Ass
ess
me
nt
SUMMARY ED Flow Self Assessment
Ave Self Assessment Score
% of Teams Reporting
Self Assessment Scale
1.0 Forming a team
1.5 Planning for project begun
2.0 Activities but no changes
2.5 Changes tested - no improvement
3.0 Modest improvement
3.5 Improvement
4.0 Significant improvement
4.5 Sustained improvement
5.0 Outstanding

44
What did the Sepsis teams do?
• created sepsis posters
• developed sepsis screening tools
• created Pre-printed Order Sets
> nurse initiated
• improved communication strategies
• adopted a report card system to highlight issues

45
And the ED Flow teams?
• process maps
• a triage surge plan - flexible triage staffing model
• match capacity to demand
> studied patient volumes
> at triage
> waiting for an ED bed
> waiting for admission/ discharge

46
ED Flow continued
• monitored and controlled for incident report issues
• standardized equipment and supplies
• tested for bed control/access services
• trialed and created a Rapid Assessment Zone to allow for quick turn around of CTAS 3 patients

47
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
%
Patient # in chronological order
Percent within target for Site X
% patients getting
fluid in < 90 min
% patients getting
Abx in < 60 min
Improvement in Fluid
Time Trend line
Time Trend line
Improvement in Abx
Time Trend line
Example of Sepsis Results
48
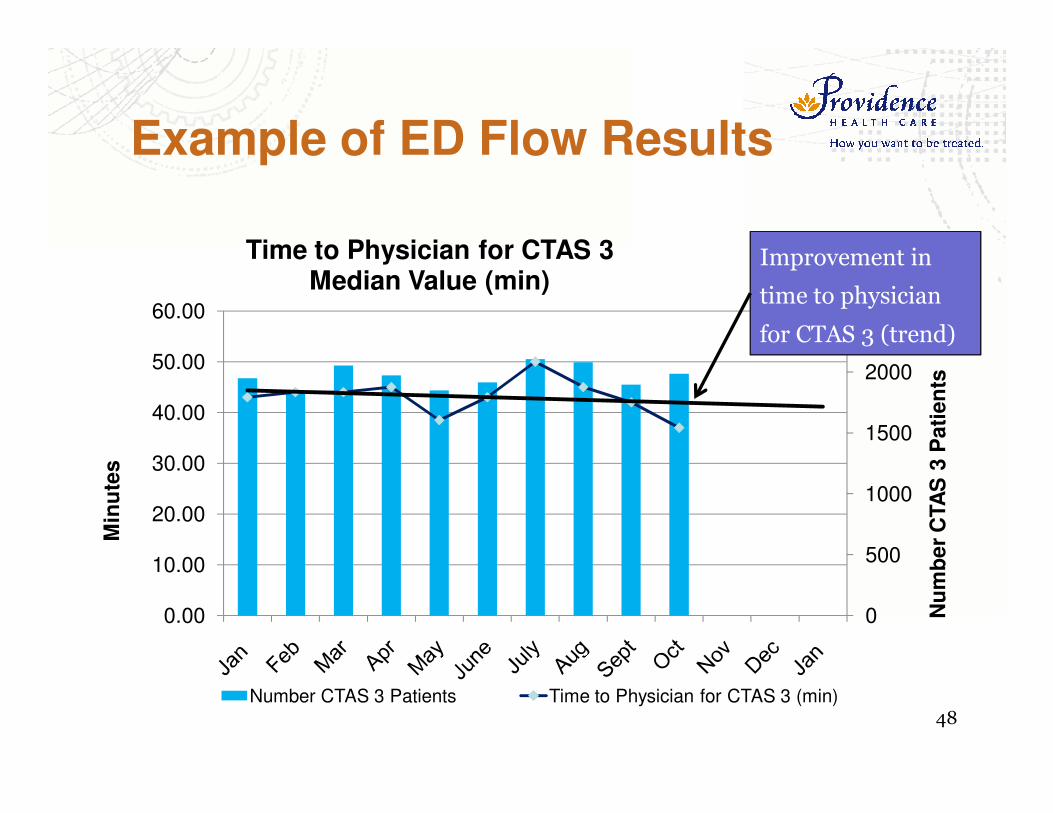
0
500
1000
1500
2000
2500
0.00
10.00
20.00
30.00
40.00
50.00
60.00
Nu
mb
er
CTA
S 3
Pati
en
ts
Min
ute
s
Time to Physician for CTAS 3 Median Value (min)
Number CTAS 3 Patients Time to Physician for CTAS 3 (min)
Improvement in
time to physician
for CTAS 3 (trend)
Example of ED Flow Results
The Challenges

50
The Challenges
1. Collaborative experience variable
2. Finite resources & competing priorities
3. Data measurement & reporting
4. Clinician engagement
5. Funding stability

What next?

52
Going Forward
1. Demonstrate value & results
2. Increase awareness of collaborative process
> Action orientated
3. Align with decision/policy makers/other grps
4. Broaden value
> Beyond the ED
5. Lengthen timeline
> Beyond “collaborative projects”
6. Academic evaluation

53
In Summary, E2E is a model:
1. A tremendous opportunity to leverage all the good work that is already being done:
> Share, spread & accelerate improvements
2. Create new networks and partnerships to bridge:
> Rural-urban divide
> Interprofessional silos

54
Acknowledgement
• Dr. Lawrence Cheng
• Dr. Mike Ertel
• Dr. Ran Goldman
• Ali Gregory
• Dr. Kendall Ho
• Dr. Kirk Hollohan
• Dr. Grant Innes
• Dr. Sandra Jarvis-Selinger
• Noreen Kamal
• Christina Krause
• Dr. Julian Marsden
• Anna Needs
• Dr. Helen Novak Lauscher
• Katie Procter
• Sherry Stackhouse
• Dr. Rob Stenstrom
• Dr. David Sweet
• Brent Woodley
• Lindsay Zibrik

55
Acknowledgement
• All the teams and team members who committed their time and energy to this work
• BC Ministry of Health
• BC Patient Safety and Quality Council
• UBC eHealth Strategy Office

Thank you.

Innovation:Immunodeficiency ClinicProvidence Health Care
Rolando Barrios, MD, FRCPCOn Behalf of the Quality Improvement TeamHIV/AIDS Outpatient ProgramProvidence Health Care

BackgroundInnovation – RedesignWhat was our comparator?Results: How did we knew we changed?Impact on other Programs

Background

60
HIV/AIDS
HIV – changing epidemic
Antiretroviral (ARV) Therapy
•Better, more tolerable, simpler combinations
•Decreases morbidity and mortality
•Increases survival and return to a productive life
HIV – Became chronic manageable disease
•Stigma, adherence, competence important differences

61
However …. not every one benefiting from ART
Community Consultation:
Most of the admissions to hospital were preventable (e.g. PCP)
Significant number of “orphan” patients
Using ER for primary care
Complex co-morbidities (e.g. mental health, addictions, hepatitis)
Providence Health Care – Leading HIV/AIDS Program in the province

62
Partners:
BC Centre for Excellence in HIV/AIDS
Providence Health Care

Innovation

64
Redesign:
•Focus on patient centre care
•Accessible, flexible (low-threshold), quality
•Interdisciplinary approach
•Complex medical/psycho-social issue
•Proactive care
•Informed patient interacting with a prepared proactive team
•Clinical information systems
•Monitor individual and population outcomes
•Evaluation

65
Adapted the Chronic Disease Model

66
Quality Improvement Model
67
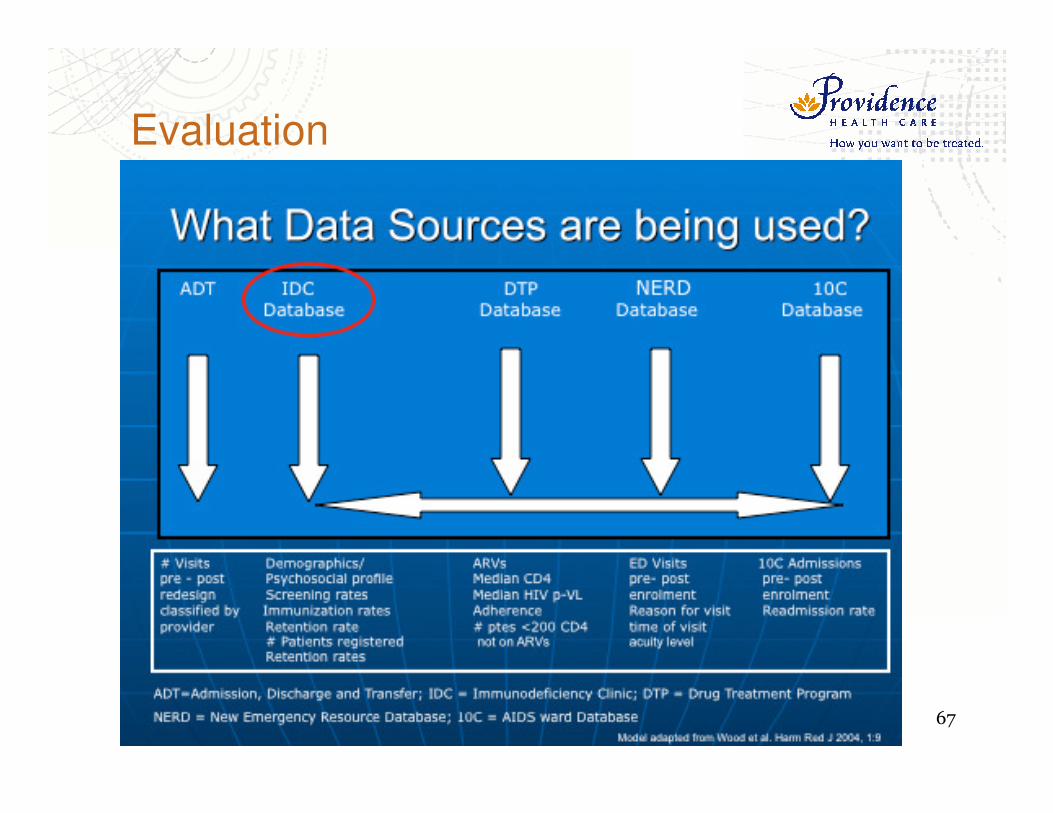
Evaluation

What comparators were used when assessing Quality?

69
What comparators were used when assessing Quality: Clinical Practice Guidelines

70
Clinical Information Systems

71
INDICATORS

Results

73
Cumulative number of patients registered in IDC for HIV Primary Care
Data source: IDC Database

7474Source: IDC Database (Dec-2009)
INDICATORS: Screening Immunization
INDICATORS: Population CD4s & Plasma Viral Load

75

76
Patient : Physician contact time
0
10
20
30
40
50
60
70
Baseline Dec-04 Dec-05 Dec-06 Dec-07 Dec-08 Dec-09
# m
inu
tes
Data sources: IDC Database and Physician sessional utilization data
77
Impact on ER and admissions to hospital
Linkage of IDC and New Emergency Room Database.
ED visits leading to hospitalization decreased from 64% to 27% (1)
(1) Barrios R, et al., XVI International AIDS Conference, Toronto 13-18
August 2006 Abstract Number: A-011-0103-03610.

78
Impact on other programs

79
Vancouver Native Health Clinic
David Tu, et al. 2010

80
Central Interior Native Clinic
Balda P. et al. Unpublished 2011

81
Provincial Structured Learning Collaborative: STOP HIV/AIDS
Based on IHI framework
Launched Jan 2011
Using same models of Care and Quality Improvement
20 Primary Care teams across the province are actively participating
The aims of the collaborative are to increase linkage and retention in HIV care.
Expected to be completed by January 2011
83
Questions
Top Related