






Languages
Pages
Legal


Inmunoterapia en tumores digestivos no colorrectales
Santander, 13 de Julio del 2017
Maria Alsina, MD PhD
Hospital Universitari Vall d’Hebron

Outline
• Introduction
• Hepatocarcinoma
• Pancreatic Cancer
• Gastric Cancer
• Conclusions

Outline
• Introduction
• Hepatocarcinoma
• Pancreatic Cancer
• Gastric Cancer
• Conclusions

Introduction Tumors are complex systems
•Successful growth of tumors and metastasis is not determined solely by genetic alterations in tumor cells, but also by the advantage that such mutations confer in the environment
• Tumor formation involves the co-evolution of neoplastic cells together with extracellular matrix, tumor vasculature and immune cells.
Tumor Antigen Transport
Lymphocyte trafficking
Junttila Nature 2013

Introduction: Therapeutic approaches to target the cancer immunity cycle
Chen & Mellman Immunity 2013, Moehler Eur J Can 2016
Tumor
Lymph node
Blood vessel

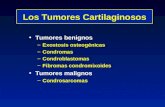
Introduction Frequency of genetic somatic mutations in cancer
Altered proteins contain new epitopes for immune recognition, providing a common denominator for cancer immunotherapy
Rh
abd
oid
tu
mo
ur
Ewin
g sa
rco
ma
Thyr
oid
Acu
te m
yelo
id
leu
kaem
ia
Med
ullo
bla
sto
ma
Car
cin
oid
Neu
rob
last
om
a
Pro
stat
re
Ch
ron
ic ly
mp
ho
cyti
c le
uka
emia
Low
-gra
de
glio
ma
Bre
ast
Pan
crea
s
Mu
ltip
le m
yelo
ma
Kid
ney
cle
ar c
ell
Kid
ney
p
apill
ary
cell
Ova
rian
Glio
bla
sto
ma
mu
ltif
orm
e
Cer
vica
l
Dif
fuse
larg
e B
-cel
l ly
mp
ho
ma
Hea
d a
nd
nec
k
Co
lore
ctal
Eso
ph
agea
l ad
eno
carc
ino
ma
Sto
mac
h
Bla
dd
er
Lun
g ad
eno
-ca
rcin
om
a Lu
ng
squ
amo
us
cell
carc
ino
ma
Mel
ano
ma
0.01
0.1
1
10
100
1000
Som
atic
mu
tati
on
fre
qu
ency
(/M
b)
22 20 52 134 26 23 81 227 91 57 121 13 63 214 11 394 219 20 49 181 231 76 88 35 335 179 121
C→T
C→A
C→G T→C T→A T→G
Lawrence Nature 2013
No at Risk

Outline
• Introduction
• Hepatocarcinoma
• Gastric Cancer
• Pancreatic Cancer
• Conclusions

HCC: microenvironment and immune landscape
Koontongkaew, 2013
• HCC is an immunogenic cancer which express tumor-associated antigens and neo-antigens arising from gene mutations
• The 90% of the HCC are associated with prolonged hepatitis the immune microvenvironment has pivotal role in its pathogenesis
• The presence of immune infiltrates is asssociated with a better prognosis
• Antitumor immune responses are subverted by a variety of stromal cells and multiple immunoinhibitory molecules
• Chronic HBV and HCV infection are associated with PD-1 and PD-L1 upregulation

Nivolumab in HCC
Melero GI ASCO 2017, El-Khoureiy Lancet 2017

Nivolumab in HCC
Melero GI ASCO 2017, El-Khoureiy Lancet 2017

Nivolumab in HCC
Melero GI ASCO 2017

Checkpoint Blockade in advanced HCC
1. Sangro Hepatology 2013
2. El Khouelry Lancet 2017
3. Wainberg ASCO 2017 # 4071
4. Kelley ASCO 2017 # 4074

Future in HCC

Outline
• Introduction
• Hepatocarcinoma
• Pancreatic Cancer
• Gastric Cancer
• Conclusions

Immunotherapy for pancreatic cancer
• The microenvironment of PC is unique

Immunotherapy for pancreatic cancer
• PC is non-immunogenic secondary to immunosuppressive elements, low mutational burden, and paucity of T cells
• Single agent therapeutic approaches with immune checkpoint inhibitors or vaccines have not been encouraging
• Combinatorial approaches appear key • Overcome T-cell immunologic endpoints
Royal J Immunother 2010; Topalian NEJM 2012

Immunotherapy for pancreatic cancer

Targeting tumor infiltrating macrophages (TAMs) and myeloid derived suppressor cells • Targeting macrophage signaling (CCR2) will block myeloid monocyte/macrophage
recruitment to tumor microenvironment, which would improve cytotoxic efficacy and increase antitumor T-cell response.
Sideras Can Treat Reviews 2013; Lesokhin Cancer Res 2011, Mitchem Cancer Res 2013
Nywering Lancet Oncol 2016

Outline
• Introduction
• Hepatocarcinoma
• Pancreatic Cancer
• Gastric Cancer
• Conclusions

50%
20%
22%
9%
TCGA Nature 2014

TILs are predictive of overall survival in GC
Lee Br J Cancer 2008
Pooled OS data for 220 patients with gastric cancer surgically resected

PDL1 expression and T cells infiltration in GC
• 1014 GC pts
• CD3+ High and CD8+ High → Better OS
• PD-L1High (TC and IC) → Better OS
• Close relationship between CD3+, CD8+ cell density and PDL1 expression (TC and IC)
Xing ASCO GI 2017
Immune cells (IC) Tumor cells (TC)
PD-L1 74.9% 37.8%
Patients with higher CD8 and CD3 T cell densities also have higher PD-L1 expression, indicating an adaptive immune resistance
mechanism may be occurring

Anti-CTLA-4 therapy in GC
• Tremelimumab • Ph 2 in 2nd Line, not randomized
• Ipilimumab • Ph 2 for maintenance after 1st Line, randomized
• Stopped after interim analysis
Ralph Clin Cancer Res 2012; Moehler ASCO & World GI 2016

Anti-PD1 & anti-PD-L1 therapies in GC
• Anti-PD1 • Pembrolizumab: KEYNOTE 012, KEYNOTE 059
• Nivolumab: Checkmate 032, ATTRACTION-2 (ONO-4538/BMS-936558)
• Anti-PDL1 • Avelumab: JAVELIN Japanese
• Atezolizumab1
• Durvalumab2 Only old activity reported, from Ph 1 basket trials
Herbst JCO 2013; Segal Ann Oncol 2014

KEYNOTE 012 Pembrolizumab in GC
Bang 2015 ASCO Annual Meeting

53.1% of patients experienced a decrease from
baseline
–100
–80
–60
–40
–20
0
20
40
60
80
100
Ch
ange
Fro
m B
assl
ine,
%
Maximum Change Asia
Rest of world
Ch
ange
Fro
m B
ase
line,
%
0 8 16 24 32 40 48 56 64 –100
–75
–50
–25
0
25
50
75
100
125
150
Time, weeks
Change Over Time Asia Rest of world
Bang YJ et al. Proc ESMO GI 2015
KEYNOTE 012 Pembrolizumab in GC
• OS (ITT)
• 6-months OS rate: 66%
• mOS: 11m

Fuchs ASCO 2017
• ORR • All patients: 11.6% • PD-L1 pos: 15.5% (vs 6.4% in PD-L1 neg) • 3rd Line: 16.4% (vs 6.4% in > 3rd L) • MSI-H: 57.1% (vs 9% in non MSI-H)
KEYNOTE 059 Pembrolizumab in GC

Yoon-Koo Kang ESMO World Congress on Gastrointestinal Cancer 2017
• 31 pts, all PD-L1 positive • ORR (1ary End Point): 25.8%
• 1 pt with complete response • mPFS: 3,3m (95% CI 2.0-6.0) • mOS: not reached
KEYNOTE 059 Pembrolizumab in GC

KEYNOTE 059 Pembrolizumab in GC

Janjigian ASCO 2016 & ASCO 2017
Checkmate 032 Nivolumab in GC

ATTRACTION-2 Nivolumab in ≥ 3rd Line
Kang ASCO GI 2017
Nivolumab 3 mg/kg (n = 268)
Placebo (n = 131)
ORR, n (%) [95% CI] P value
30 (11.2) [7.7–15.6] < 0.0001
0 [0–2.8]
—
BOR, n (%) Complete response Partial response Stable disease Progressive disease
0
30 (11.2) 78 (29.1) 124 (46.3)
0 0
33 (25.2) 79 (60.3)
DCR, n (%) [95% CI] P value
108 (40.3) [34.4–46.4]
0.0036
33 (25.2) [18.0–33.5]
—
Median TTR (range), months 1.61 (1.4–7.0) —
Median DOR, months [95% CI]
9.53 [6.14–9.82]
—
Overall Survival

Avelumab in GC
• Ph 1b in GC/GEJ pts • Irrespectively of PD-L1 status
Chung ASCO 2016
2L (n = 22) Mn (n = 52)
PD-L1+ (n = 11) PD-L1− (n = 11) PD-L1+ (n = 20) PD-L1− (n = 32)
ORR % (95% CI) 18.2
(2.3, 51.8)
9.1
(0.2, 41.3)
10.0
(1.2, 31.7)
3.1
(0.1, 16.2)
mPFS w (95% CI) 6.3
(5.4, 18.0)
10.4
(4.1, 21.9)
17.6
(6.0, 24.1)
11.6
(5.7, 14.1)

Which biomarker?
• PD-L1 IHC • Different positivity rate (57.1% in KEYNOTE 059, 31% in Checkmate 032)
• IHC test not standardized
• Different Ab, different positivity criteria
• Other issues: sampling time, simple type (heterogeneity)
• Trend of higher activity in PDL1+
• Gene expression signature • IFN-γ signature (18 gene) as a predictor for inefficacy
• Usefulness not evident: much overlap
Shankaran V et al. Abstract 3026. Presented at the 2015 ASCO

Which biomarker?
• MSI • MSI-High rate is quite low (≈5% in incidence)
• Very high activity in MSI-high (KEYNOTE 059)
• Useful for clinical practice
Seruca Int J Can 1995 Hye Seung Lee Mod Pathol 2002
P = .046

Combined strategies
Anti-angiogenic agents Immune response
• Vasculature normalization • ↓ Interstitial pressure • ↑ Perfusion • ↑ Adhesion molecules • Preserve endothelial cell anergy
• Availability of glucose, amino acids and oxygen • ↑ Lymphocyte infiltration • ↑ T-cell access and function
Manning Clin Ca Res 2007
Hodi Cancer Immunol Res 2014
Sznol J Clin Oncol 2015 (suppl)

Combined strategies
• Immunotherapy + anti-angiogenesis
• Pembrolizumab + Ramucirumab1
• Immunotherapy + radiotherapy (Abscopal Effect)
• Pembrolizumab + palliative radiotherapy (30 Gy on 1ary tumor or single metastasis) → Pembrolizumab until PD2
• Immunotherapy + targeted agents • With anti-HER2 agents (margetuximab)3
• With anti-MMP9 agents (GS-5745)4
• With PARP-inhibitors (Olaparib) 5
1. Chau ASCO GI 2017; 2. Chao ASCO GI 2017;3, Catenacci ASCO GI 2017; 4. NCT02864381; 5. NCT02734004

The future in GC

Outline
• Introduction
• Hepatocarcinoma
• Pancreatic Cancer
• Gastric Cancer
• Conclusions

Conclusions
• Pancreatic Cancer • PC is an immune privileged tumor
• Still too early for immunotherapy, but many opportunities using rational combinations
• HCC • Activity for anti-CTLA-4 and anti-PD1
• Efficacy observed irrespective of HCV, HBV or PDL1 status

Conclusions
• Esophago-Gastric Cancer • Single agent anti-CTLA4 – no activity
• Very interesting activity with single agent anti-PD1 and anti-PD-L1
• Dual PD-1/CTLA-4 (nivo/ipi) may be more active, but with higher toxicity
• Biomarkers • PD-L1 IHC: multiple technical factors, response in PDL1 negative patients
• Gene expression profiles, MSI/EBV status, mutational load
• Combinatorial strategies

Take home messages
• Activity in subset of patients, particularly in esophago-gastric tumors
• ≈ 25% long term survivors
• Pembrolizumab as a standard in MSI+ patients
• Combination strategies may improve the efficacy
• Biomarkers beyond MSI are crucial
• Need to further understand the immune-pattern of response and how to manage related adverse events

¡Muchas gracias!
Top Related