







Languages
Pages
Legal


Idiopathic Eosinophilic PneumoniaIdiopathic Eosinophilic Pneumonia
Dr. Hadil Alotair Dr. Hadil Alotair
KKUHKKUH
HistoryHistory
A 18 Y/O saudi lady living in Riyadh. she is a student
–C/O •Fever 8 days•productive cough 8 days•Chest pain 2 days•Dizziness+syncope 2 days

–She was seen in a private hospital and was given Augmentin and azithromycin for five days without any improvement.
Past H/O– BA – Eczema– Allergic rhinitis– WPW

Drug HxDrug Hx
•Budesonide•Flexinase•Ventolin•Singulare

ExaminationExamination • looked sick. • Pulse 125/minute, BP 108/67 mm
Hg. • Temperature 37. 8c. • Respiratory rate 22/minute. • No lymphadenopathy.• 02 saturation was 88% on room
air.
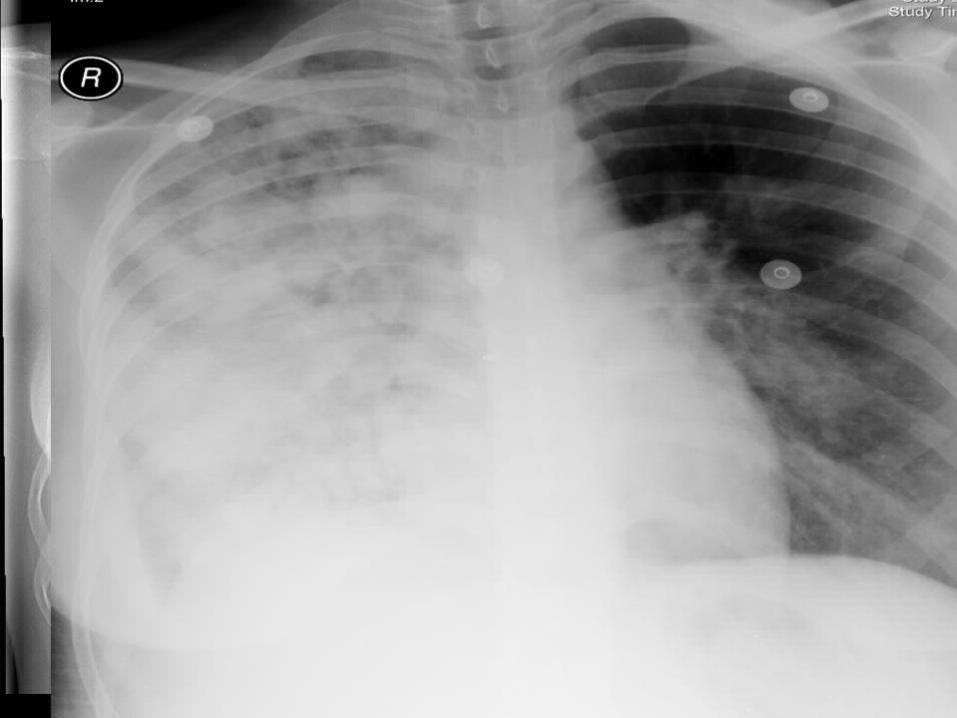
• Chest
–Decreased chest expansion on the right side
–Dull ness –Bronchial breathing –Coarse crepitations –Pleural rub
•Other systemic examination- NAD
Rt. InfrascapularRt. Infrascapular

InvestigationsInvestigations • CBC:
– WBC 29,000– RBC 4.5– Hb 137– Plt 327 – ESR 14.
• Differential: neut 51, lymph 14,mono 5, eos 30%
• Urea and electrolytes: Normal• LFT – Normal.

• ABG: –pH 7.43–PC02 36–Po2 51.9–HC03 23.2– 02 saturation 87.9 on RA
Hospital courseHospital course• The patient was admitted initially
with the impression of - CAP• on the following day
– increasing SOB , cough -- Desaturated.
• she was transferred to the MICU
MICUMICU• In MICU -- Ceftriaxone increased (2 g iv BD)
– CIarithromycin – along with 02 10 lt – active nebulization with Ventolin, Atrovent
and Pulmicort,
• ABG on 10 l o2 via NRBM
– PH 7.39 Pco2 41 Po2 88 HCo3 24
• She was put on non invasive ventilation BIPAP 60% O2
IPAP-10 EPAP-4
• Her blood culture - Streptococcus pneumoniae
• Meropenem and levoftoxacin
• she was not responding to BiPAP
• hemodynamically unstable – inotropes
• She was Intubated


•Her ventilator mode was– ACMV ,PEEP 10, FIO2 60%, Vt 350,
RR 22
pH – 7.49 PCO2- 42 PO2- 85 HCO3 – 31 %O2Sat-97
–CT scan showed •Large pneumonic consolidation of the right lung with para pneumonic effusion
•Dense opacification in the apical segment of left lower lobe
•Early ARDS.




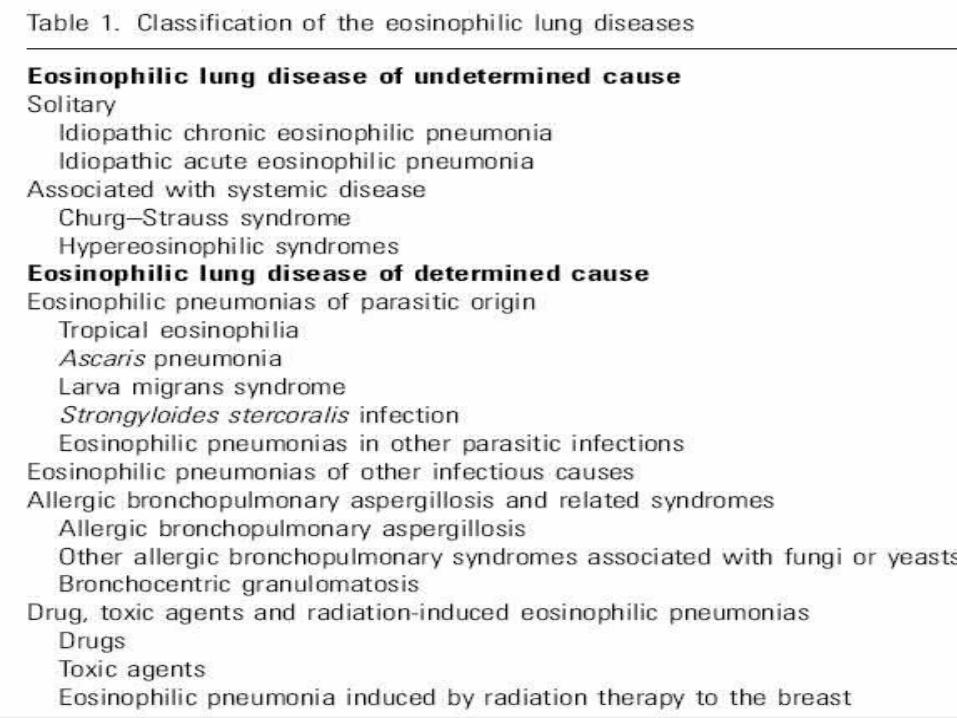
• At this stage the DDx was:– CAP– ABPA– Churg Strauss Syndrome– Pulmonary eosinophilic
syndrome such as•Loffler’s syndrome•Acute eosinophillic pneumonia
•Hyper eosinophilic syndrome
– Drug induced

Investigation resultsInvestigation results• PLF
– Negative for malignant cells•
– Inflammatory infiltrate consists mainly of neutrophil mixed with moderate no. of eosinophil & few plasma cells & lymphocytes
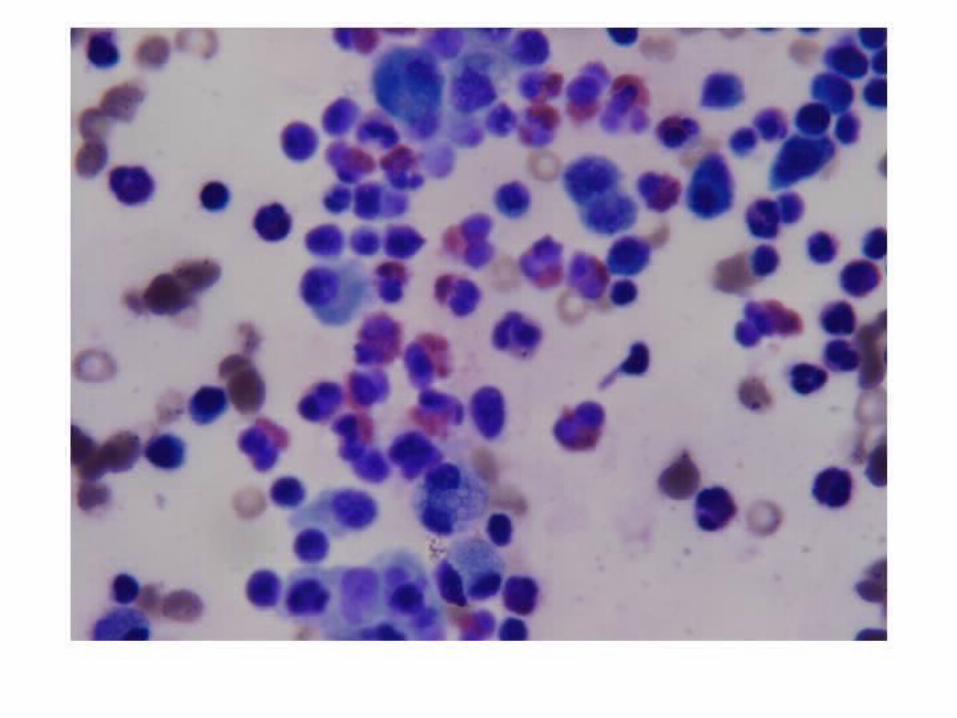

Bronchial lavage :Eosinophils – 35%Negative for malignant cells.
Negative for fungal element and gram staining and AFB


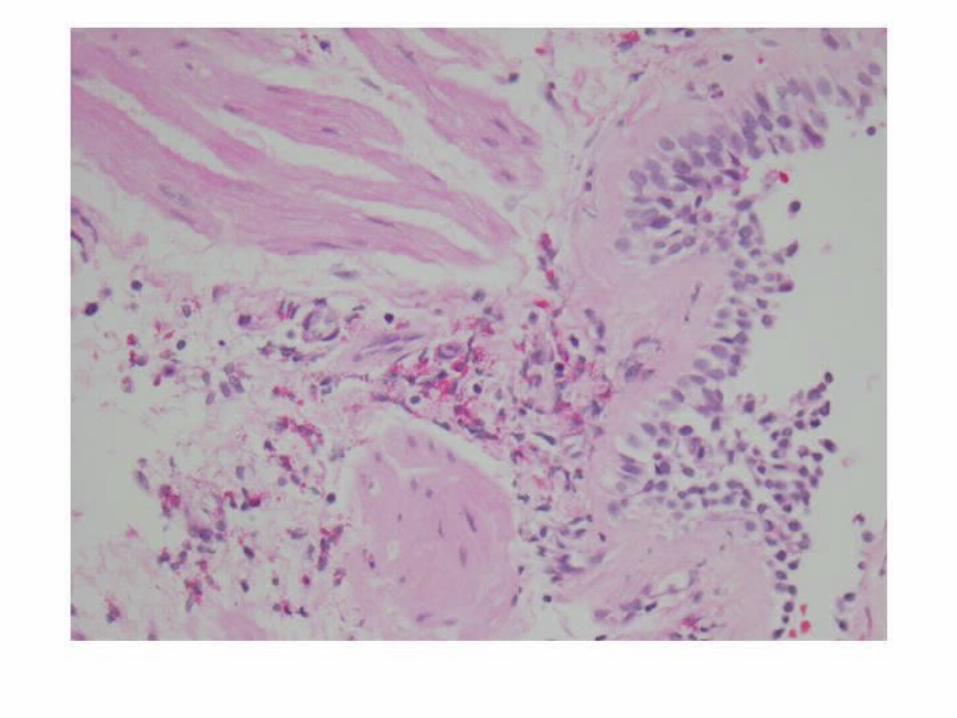
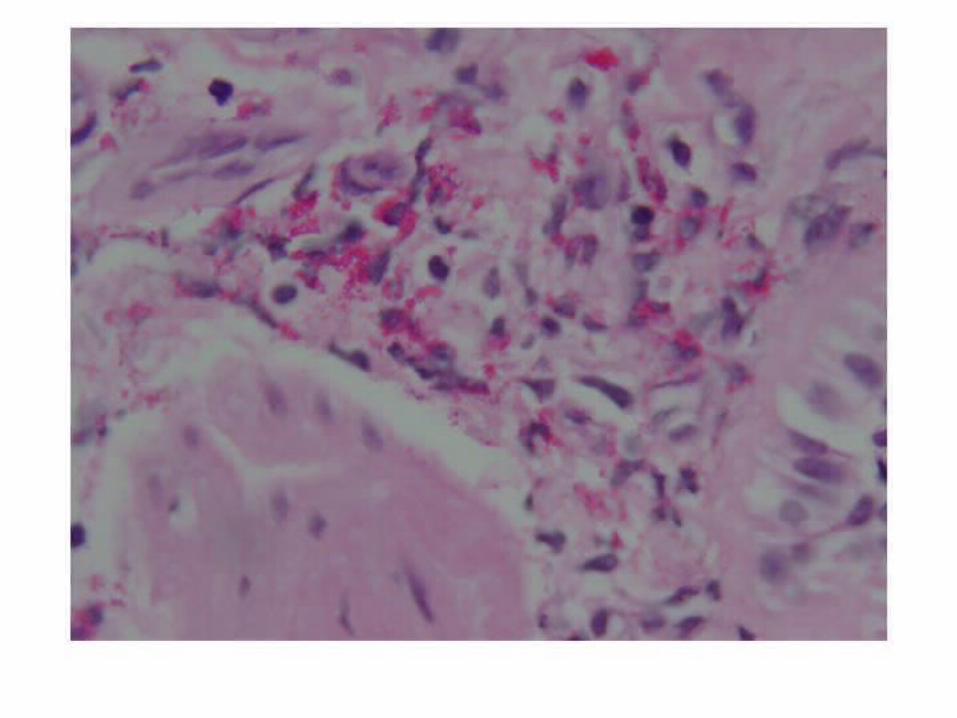
•Endobronchial biopsy:
Marked eosinophilic infiltration in bronchial mucosa.

•Skin biopsy:
Drug related dermatitis.

Methylprednisolone 40 mg iv q8h
• Improved
• Extubated - 5 days

Results of pending Results of pending investigationsinvestigations
• Serum Aspergillus antibodies: Negative for all variants.
• Serum anti-mycoplasma IgM: Negative
• ANA, Anti DNA – Negative• ANCA – Negative

EtiologyEtiology
• Acute hypersensitivity reaction to inhaled antigen in a previously healthy Individual
• Enviromental factors
• Cigarette smoking
• World trade centre
• Military personnel in Iraq
• HIV
Clinical presentationClinical presentation
• Cough
• Dyspnea
• Pleuritic chest pain
• Myalgia
• Night sweats

Physical examPhysical exam
• Fever
• Tachypnea
• Tachycardia
• Bibasilar crackers
• rhonchi
ComplicationComplication
• Hypoxemic respiratory failure
• 14 of 22 patients(63%) required MV
• Hyper dynamic Shock

LabLab
• Neutrophilia
• Eosinophilia
• IgE
• ESR

CXRCXR
• Reticular infiltrate
• Kerly B line
• Bil.diffuse alveolar &reticular opacities
• Isolated reticular or alveolar
• Small bil effusion)Eosinophilic)

HRCTHRCT
• Bil.patchy ground glass or reticular opacities
• Effusion

BALBAL
• Eosinophilia >25%(mean 37%)
• IL-5
• GM-CSF
• IL-1ra
• VEGF

PathologyPathology
• Acute &organising diffuse alveolar damage
• Interstitial&alveolar &bronchiolar infiltration of eosinophil
• Hyaline membranes and interstitial widening
• Organising intra alveolar fibrinous exudate


TreatmentTreatment
• Spontaneous improvement rare
• Resp. failure (50-60%)
• Steroids
• Clinical response 12-48 hrs
• Continue steroids for 2-4 wks after plain X-ray normalises (2-6wks)


ACR – Classification CriteraACR – Classification Critera::
Asthma
Eosinophilia of > 10%
Mono or poly-neuropathy
Migratory or transient pulmonary opacities
Para-nasal sinus abnormalities
Biopsy containing blood vessel –extra vascular eosinophils

Top Related