







Languages
Pages
Legal


Hydrocephalus
Pembimbing : dr. Nick Tobing, Sp. BS
Michelle Husin (2013-061-118)Ellysa Virgiana (2013-061-119)

Cereberospinal Fluid

The Function of the CSF
The CSF acts as a “water jacket” for the brain and spinal cord
The 1300 g adult brain weighs approximately 45 g when suspended in CSF
The Function of the CSF
The CSF acts like a “sink”, effectively flushing waste products as new fluid is secreted reabsorbed
A constant CSF electrolyte composition helps maintain a stable medium for excitable cells (neurons)

Hydrocephalus
Increase in cereberospinal fluid (CSF) volume usually resulting from impaired absorption, rarely from excessive secretion.
This definition excludes ventricular expansion secondary to brain shrinkage from a diffuse atrophic process (Hydrocephalus ex vacuo)

Classification
By Pathophysiology
By Etiology
Obstructive Hydrocephalus
Communicating Hydrocephalus
Congenital Hydrocephalus
Acquired Hydrocephalus

Causes


Non-communicating hydrocephalus
There is no communication between the ventricular system and the subarachnoid space.
The commonest is aqueduct blockage or stenosis

Aqueductal stenosis
The normal aqueduct measures about 1 mm in diameter, and is about 11 mm in length.
Aqueductal stenosis
Is the most common cause of congenital hydrocephalus(43%)Aqueduct develops about the 6th week
of gestation M:F = 2:1 Other congenital anomalies (16%):
thumb deformitiesPrognosis: 11-30% mortality

Etiology of aqueductal stenosis
Extrinsic Pathology of the Aqueduct:Infectious: Abscesses.Neoplastic: Pineal tumors,
brainstem gliomas, medulloblastoma, ependymoma.
Vascular: AVM, aneurysm, Galen aneurysm.
Developmental: Arachnoid cysts.

Etiology of aqueductal stenosis
Intrinsic Pathology of the Aqueduct
Septum or Membrane Formation: A thin membrane of neuroglia may occlude the aqueduct
Forking of the Aqueduct: Typically, there are two channels seen in midsagittal plane unable to handle CSF volume. Most often seen with spina bifida.
Gliosis of the Aqueduct: Usually of infectious origin showing a marked gliofibrillary response.
Stenosis of the Aqueduct: Narrowed aqueduct without evidence of gliosis. This may have hereditary basis.

Imaging of Aqueductal Stenosis
Ultrasonography can detect aqueductal stenosis in utero
Sonogram

Imaging of Aqueductal Stenosis
CT and MRI. MRI is essential if third ventriculostomy is to be considered.
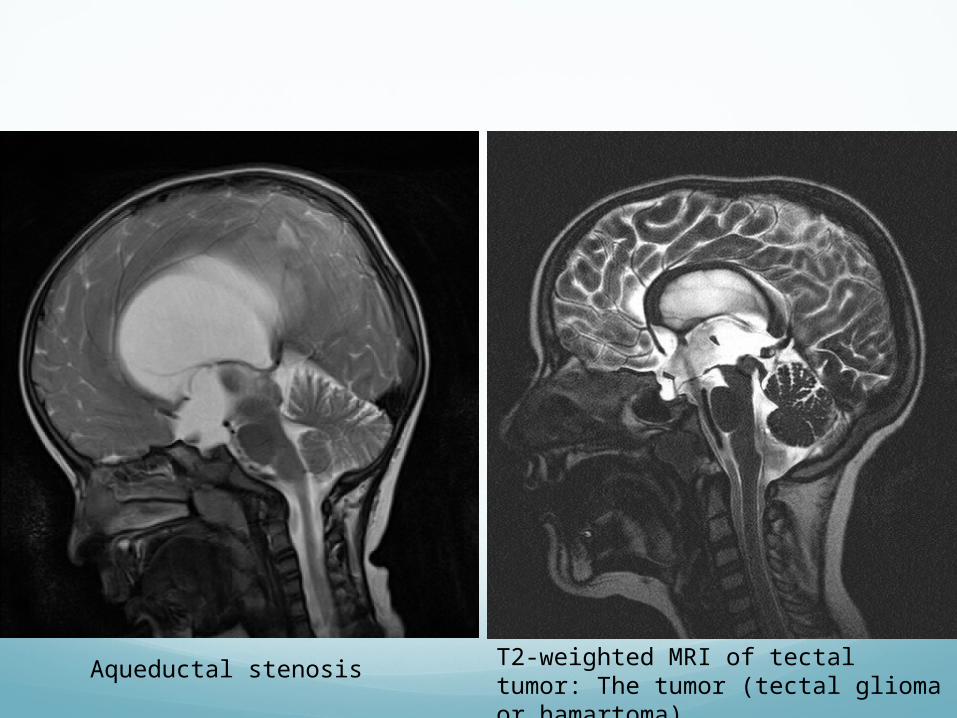
T2-weighted MRI of tectal tumor: The tumor (tectal glioma or hamartoma)
Aqueductal stenosis

Dandy Walker SyndromeA common cause of
obstructive hydrocephalus is Dandy Walker Syndrome where there is blockage of foramina of the 4th ventricle (atresia of foramina of Luschka and Magendie)

Communicating hydrocephalus
In communicating or non-obstructive hydrocephalus there is communication between the ventricular system and the subarachnoid space. The commonest cause of this group is post-infectious and post-hemorrhagic hydrocephalus.

Causes of communicating hydrocephalus
Overproduction of CSF
Blockage of CSF circulation
Blockage of CSF resorption
Hydrocephalus ex-vacuo
Normal pressure hydrocephalus

Overproduction of CSF
Excessive secretion of CSF by the choroid plexus as in cases of choroid plexus papilloma or carcinoma. This is a rare cause.

Blockage of CSF circulation
This could be at any level of the CSF circulation with either unilateral or bilateral occlusion of the foramen of Monroe. Dilatation of one or both lateral ventricles. This is commonly seen in the colloid cyst and tumors of the third ventricle.

Blockage of CSF resorption
Poor resorption of CSF into the venous sinuses caused by scarring of the arachnoid villi and is commonly seen after meningitis or hemorrhage

Hydrocephalus Ex Vacuo
Hydrocephalus ex-vacuo involves the presence of too much CSF, although the CSF pressure itself is normal. This condition occurs when there is damage to the brain and there may be an actual shrinkage of brain.

Normal pressure hydrocephalus
Normal pressure hydrocephalus is usually due to a gradual blockage of the CSF drainage pathways. NPH is an unusual cause of dementia, which can occur as a complication of brain infection or bleeding (hemorrhage).

Pathology of Hydrocephalus

Clinical Manifestation
In infants & young children
In adult



InvestigationsX-ray
!!: - skull size, suture width- evidence of chronic raised pressure erosion of the
posterior clinoids)- associated defects

Aqueduct stenosis
3rd ventricle and anterior horns are dilated, 4th ventricle are normal
Normal• CT Scan

Posterior fossa mass
Dilated 3rd and lateral ventricle, deviated or absent 4th ventricle

Communicating hydrocephalus
Dilated lateral, 3rd, normal 4th ventricle
UltrasonographyLess good than CT Scan

Magnetic Resonance ImagingMore clear vision of periventricular lucency, neoplastic mass
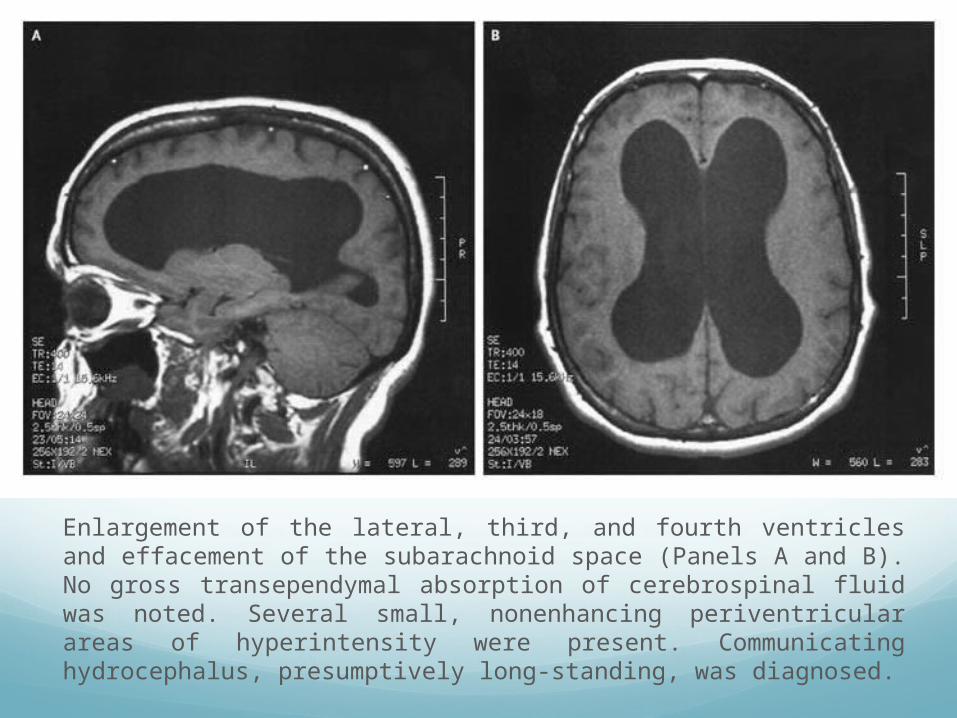
Enlargement of the lateral, third, and fourth ventricles and effacement of the subarachnoid space (Panels A and B). No gross transependymal absorption of cerebrospinal fluid was noted. Several small, nonenhancing periventricular areas of hyperintensity were present. Communicating hydrocephalus, presumptively long-standing, was diagnosed.

Intracranial pressure (ICP) monitoringUseful for normal pressure hydrocephalusTo predict the likelihood of a beneficial response to shunting

Developmental assessment & psychometric analysisTo detect impaired cerebral function and provide a baseline for
future comparison

Management

Complications of ShuntingInfections
Subdural haematoma
Shunt obstruction
Low pressure state
Top Related