







Languages
Pages
Legal


Homes and Jobs
Social Inclusion for the disadvantaged

Homes and Jobs
Ian Bainbridge – Deputy Regional Director –Department of Health South East

Why do we need your help?
Homes and Jobs
Some groups find it very difficult to get jobs and houses without support. The Department of Health are keen to increase the number of vulnerable people
with their own home and a jobs, as work and settled accommodation are shown to increase the health, wealth and wellbeing of these groups, including;
• People with learning disabilities• People in contact with secondary mental health services• Care leavers• Offenders
Health, Work and Wellbeing
Dame Carol Black

Dame Carol Black National Director for Health and Work
Work and health
Increasing opportunities in the public sector
Guildford 25 June 2010

As far as possible all working age people
should have the opportunity to flourish at work
FLOURISHING IN WORK
CHILDREN AND YOUNG PEOPLE
PEOPLE WHO ARE EMPLOYED
PEOPLE WHO ARE NOT
EMPLOYED
In School, Training, Further
Education, or University
Flourishing in work
In Work
On Sick Leave
On Job Seekers
Allowance
On health related benefits
Not on work related benefits
Flourishing at work
Work and Health
Waddell and Burton (2006) Work is generally good for physical and
mental health and well-being
Galen (129-200)Employment is nature’s physician
and is essential to human happiness.
Theodore Roosevelt (1858-1919)The best prize that life offers is the chance to work hard at work worth doing.
William Osler (1849-1919)To the young it brings hope, to the middle-
aged confidence, to the aged repose: work.
Voltaire (1694-1778)Work banishes those three great evils:
boredom, vice and poverty.
And yet for too long, people with disabilities have been kept from work by discrimination, lack of reasonable adjustments and other peoples’ low expectations.

Long-term Worklessness – a Great Risk to Health
• Greater risk than many “killer
diseases”
• Greater risk than most
dangerous jobs (e.g.
construction, fishing, etc)
• 2 to 3 times risk of mental
illness
• Poor health in children of
workless families
• Social exclusion and poverty

Health of unemployed andre-employed men
Nottingham health profile
Emotional reaction Social isolation Physical mobility
A. Newman Taylor, after McKenna and Payne, 1989
Mean scores
Unemployed 18-24 months
Re-employed (unemployed
more than 6 months before)
Weighted random
population sample
0
5
10
15
20
25
30
35
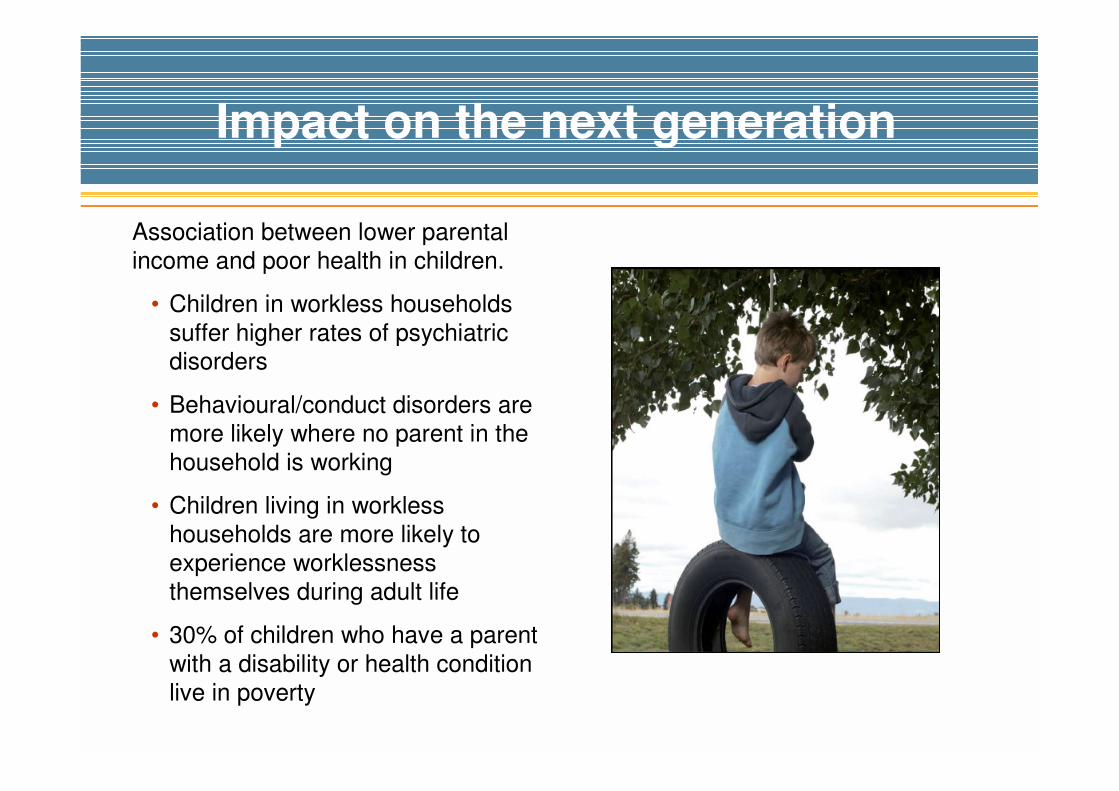
Association between lower parental
income and poor health in children.
• Children in workless households
suffer higher rates of psychiatric disorders
• Behavioural/conduct disorders are
more likely where no parent in the
household is working
• Children living in workless
households are more likely to
experience worklessness
themselves during adult life
• 30% of children who have a parent
with a disability or health condition
live in poverty
Impact on the next generation

The Fundamentals
“People’s social and economic circumstances affect health throughout life, so health policy must be linked to the social and economic determinants of health.” Michael Marmot
Work & unemployment are social determinants of health.

“At the heart of this Review is a recognition of,
and a concern to remedy, the human, social
and economic costs of impaired health and
well-being in relation to working life in Britain.
The aim is not to offer a utopian solution for
improved health in working life, but rather to
identify the factors that stand in the way of
good health and to elicit interventions,
including changes in attitudes, behaviours and
practices – as well as services – that can help
overcome them.”
Working for a healthier tomorrow, 2008
Working for
a Healthier
Tomorrow
A new vision for health and work
Prevent illness, promote health, intervene early, improve the health of the workless.

Costs of working-age ill-health
Financial
• Overall costs of working-age ill-health in UK exceed £100 billion per year
• Around 172 million working days were lost to sickness absence in 2007, at a cost to the economy of over £13 billion (CBI)
Social
“If people are not healthy enough to work – or are inadequately supported through ill health to make a return to work possible – it is not just the individual or the business which is affected. The bottom line is often the impact on his or her family and children.”
Lane Lecture, University of Manchester, November 2007
Worklessness is a greater risk to health than many ‘killer’ diseases.

Problems with the UK system in 2007-2008
Workplace culture
• Misconceptions about health and work – “need to be 100% fit”.
• Poor retention in work of those with disabilities or chronic disease.
• Workplace and employers often needing a different culture and approach.
Inadequate systems
• Inflexible system of sickness certification that labelled you as sick even when it was inappropriate.
• No pathways of rapid intervention to keep you in work or return you to it.
• Health, work and well-being not part of training curricula or clinical practice,
leading to poorly-informed healthcare professionals with little
understanding of work as a determinant of health.
Lack of Primary Care involvement
• Rehabilitation to work not a performance measure for Primary Care Trusts,
which therefore show little interest.
• No Occupational Health services in Primary Care. Patchy OH elsewhere.

• Two-thirds of sickness absence and long-term incapacity is due to mild and treatable conditions:
• Depression, anxiety, stress-related mental health problems (est. cost £28.3 bn in 2008)
• Musculoskeletal conditions – mild and often soft tissue (est.cost £7 bnin 2007)
• Cardio-respiratory conditions
• Inappropriate “medicalisation”
• Poor retention in the workplace of those with disabilities or chronic disease
Why people are off work in the UK and many other countries
‘Causes of the causes’?

Economic Costs of Mental Ill-Health
£100 billion is lost to the economy because of working-age ill health and
associated sickness absence and worklessness. Estimated that between
£30-40 billion can be attributed to mental ill-health. This includes:
• Lost production of people who are on sickness absence or out-of-work
benefits
• Lost production of people of working age who provide informal care, and
• A proportion of NHS healthcare costs used to treat people of working age
with a mental health condition
“Some of these costs fall directly to individuals with mental health conditions and are mitigated through the tax and benefit system.Estimated that the government pays around £8 billion every year in benefit payments to people with a diagnosed mental health condition.”Working for a Healthier Tomorrow

Mental health as a reason for claiming incapacity benefit : Scotland
Percentages of all IB claimants who were claiming for a mental health problem in February 2000 and 2007:
56.237.844.2February 2007
46.528.833.6February 2000
Of credits-only claimants (%)
Of payment claimants (%)
Of total claimants (%)
Quarter ending
Note: “Credits-only claimants” have a poor employment history.
• The ‘mental health’ proportions are all increasing.
• More of those with poor employment history claim because of a mental health problem.
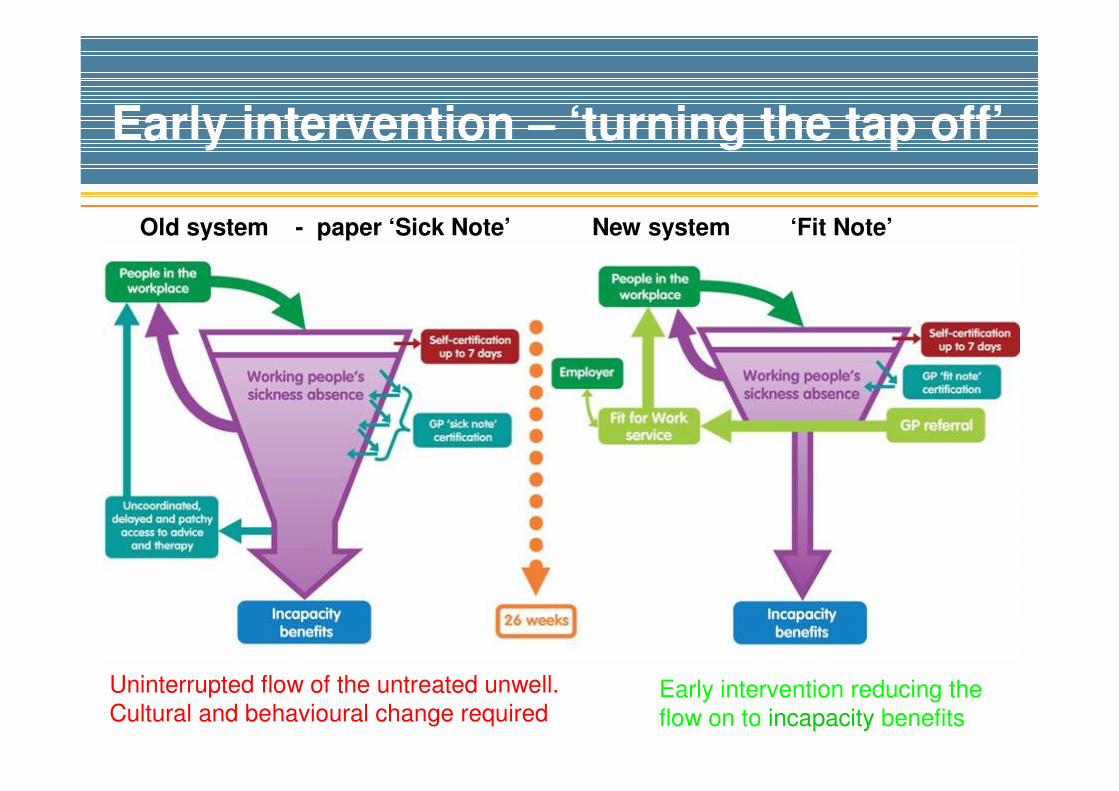
Early intervention – ‘turning the tap off’
Old system - paper ‘Sick Note’ New system ‘Fit Note’
Uninterrupted flow of the untreated unwell.
Cultural and behavioural change requiredEarly intervention reducing the
flow on to incapacity benefits

Working for a healthier tomorrow, 2008
“Tackling stigma around ill-health and disability will be key to enabling
more people with health conditions find work and stay in work. This is
particularly true for those with mental ill-health, as many organisations
often fail to recognise the full value of the contribution they can make”
“The sheer scale of the numbers of people on incapacity benefits
represents an historical failure of healthcare and employment support to
address the needs of the working age population in Britain. Over 200,000
people with mental health conditions flow on to incapacity benefits each
year, and this figure has not changed over the last decade.”
“Government must fully integrate the option of specialist mental health
provision into its employment programmes – not just for those on
incapacity benefits – but for all those who are workless, whether lone
parent, jobseeker or Income Support recipient.”
‘Working for a healthier tomorrow’. Dame Carol Black 2008
The System and the Barriers
The system may help or hinder people:
• GPs, specialists, counsellors etc. need to support the role of work.
• a joined-up approach with agreed goals and coordinated themes for all those involved is needed.
Potential barriers:
• how to get started in work if you have had a mental health problem whilst in the education system
• occupational health questionnaires which filter out people with mental health problems or force them to disguise the truth
• sick leave and benefits systems which, for some, become traps preventing return to work rather than supporting it
• lack of flexible and supported entry or return to work
Achieving well-being at work
• Reward small business workplace innovation with
Challenge Fund
• Develop a UK-wide network of Health, Work and
Well-being Co-ordinators
• Work with EU partners - on new criteria for
organisations to assess the quality of their mental-
health-related workplace health
• Encourage managers to use HSE’s competency
framework for line managers and commit to training for managers
• Encourage the public sector to review their
recruitment retention and prevention procedures for
people who use secondary mental health services
• Promote good practice – there are some fine
examples
Employment Advisors
• Part of Improving Access to Psychological Therapies (IAPT)
• Pilot study started mid 2009
• So far, around 1000 people have accessed their services
• 70-80% of those seen retain employment
• Early intervention is key
Case study
My client was employed in I.T.
His depression and shift
rotatations were causing him
problems with sleep, resulting in
tiredness at work. I set up a
meeting with his employer, at
which we agreed changes to his
shift patterns. He returned to
work in October and is coping
well.

Common Mental Health problems at work: surveying progress
• Common Mental Health Problems are widespread, and are the health problem of working
age; but most employers are not aware of the high levels of associated morbidity
• Employees do not have to be entirely symptom-free to remain in or return to work
successfully.
• Line managers need effective skills development and training
• Independent case management by third-party specialists is critical to achieving successful
outcomes for individuals and organisations where employees are not recovering as
expected.
• The workplace is an important but not the only setting for delivery of effective interventions
• There is a sufficient body of evidence to inform the development of important services and
interventions that can keep people with CMHPs in work or facilitate their return.
• Research in the UK has not advanced far in the five years covered by this update review,
and there is a need to replicate critical findings within a British context.
(Courtesy of Bob Grove, Sainsbury Centre for Mental Health)

Sainsbury Centre
Workplace Programme
• Training programme aimed at giving managers confidence to respond to staff experiencing mental distress.
• Based on the proven beyondblue National Workplace Programme (Australia)
• Excellent results in UK pilot:• Builds awareness of
depression and
anxiety, and trains
managers to spot symptoms.
• Allows time for
discussion, and helps

Health for Work Adviceline
• Free GB-wide Occupational Health telephone advice line pilot aimed at reducing sickness absence and avoidable job loss
• Professional occupational health advice on individual problems, and information about local services, by nurses with extra Mental Health training
• Focus on helping manager resolve individual employee health at work problems (especially mental health issues)
• Target audience: employers/managers in businesses with fewer than 50 employees
• Also in scope: businesses with 50-249 employees, GPs
08000 77 88 44

Early life: building resiliencefor our future workforce
To increase the life chances of young people :
• Improve support in education
• Encourage supportive parenting and relationships
• Provide early and co-ordinated intervention
Four recent Reports address this:
• Foresight, Mental Capital and Wellbeing;
• The Black Review Working for a Healthier Tomorrow;
• Working our way to better mental health: a framework for action;
• The Marmot Review.
“…to give every child and young person the best possible chance tothrive, families carers and health and education systems must act together to promote wellbeing and foster skills for resilience.”
So how much of the journey is left to go?
• We’re not there yet!
• All individuals and
organisations concerned
with working-age
healthcare need to
cooperate if we are to
improve the health of the
working-age population

Homes and Jobs
Social Inclusion for the disadvantaged

Care Leavers experience of
working with their service- Jessica Inwood, a young persons perspective

My Story
Dawn North and Robert King

Workshops
Please choose one

Workshops
Janine Hobbs – Jobcentre Plus
WORKSHOP A
How Job Centre plus can support your organisation
Kathy Melling – National Lead for VPN (Learning Disabilities)
WORKSHOP B)
Making Recruitment accessible for hard to reach groups
Clare Cherry – HMPS –Partnerships Team
WORKSHOP C
Managing and Minimising Risks
David Raison – Richmond Fellowship (Mental Health employment specialists)
WORKSHOP D
Improving Retention

Workshop Feedback
Feedback from workshop facilitators and questions

Harnessing the power of
the wider organisation
Influencing jobs and training for disadvantaged groups through
the procurement process

Lunch
Lunch is Served - Please be back promptly

36
respect trust listen responsible
June 2010
Carmel Millar
Head of HR&OD
Making a Difference

DVD

• Valuing People Now
• What we have done
• Our success in realising potential
• Working with Employability
Realising Everyone’s Potential

Jenni Brown

Surrey County Council’s Supported Employment
service
Currently only Learning Disability and Autism
Open Referral
Work with colleges and schools
Supporting around 630 people across the county

Support
Train
Place
Minimal monitoring
Employer Support
Resolution
Advocacy
Induction
Workplace training
Travel Training
Meet client
Vocational profile
Job search
Work experience
Job Carving
Recruitment
Risk Assessment
Supported Employment

• 43 year old, never worked
• Attending day centre for 15 years
• Communication difficulties
• Wanted to work in an office
• Liked cooking
• Job Carving
• Works 2 days a week
• Travel Training – catches bus
“I enjoy everything about
my job. It is important to me
that I get paid. My job
makes me feel good, and
the staff I work with are
friendly. Every Friday I look
forward to having fish and
chips in the staff canteen”
Sarah
Case Study

Working together HR&OD and EmployAbility
Established
Job carving
Work trials
Working Interviews
Easy-Read documentation
30 People found paid work

• Benefits for individuals
• Benefits for the council
• Benefits for the community

Commitment
• Recruitment strategy and methods
• Objective in E&D action plans
• Job carving at source
• Job design
• Support & Training
• Website meets accessibility standards

Homes & Jobs – Social Inclusion
INCREASING EMPLOYMENT OPPORTUNITIES IN THE PUBLIC SECTOR
25th June 2010.

Who we are
West Sussex Works
Paritas Synchronise
Recruitment servicesfor people who have experienced mental health problems
Employer engagement forum in West Sussex

Leading by Example

Managing Wellbeing
Strategic
National Mental Health and Employment strategy
Perkins review ‘Realising ambitions’.
NICE guidance Mental Health in the Workplace.
NHS Health & Wellbeing (Boormanreview)
New Horizons
Public Service Agreements (PSA16)
Public Sector as exemplar employers.
Disability & Equality Duties.
Local Area Agreements.
Strategic & Policy Public Sector Duties

Managing WellbeingEmployer
Over 200,000 working days are likely to be lost across the public sector in West Sussex due to mental ill health every year.(average absence per employee 2.8 days due to stress & mental health- Sainsbury
Centre)
Mental Illness related absence is likely to cost public sector employers in West Sussex over £75 million pounds a year.(The cost per employee is over £1000 Sainsbury Centre)
3 in 10 employees will experience some kind of mental health problem in any given year
Stress is the second biggest reason for absence in the UK
Over 50 % of employees conceal mental ill health in the workplace.
Very real need to keep employees in work and performing during a time of recession.

Managing WellbeingCommunities
1 in 6 people will be experiencing a mental health problem at any given time. (over 100,000 people of working age in West Sussex)
Around 10,000 people are receiving Incapacity benefit or Employment
Support Allowance (ESA) on the basis of a mental health condition in
West Sussex .
Possibility of developing depression after 6 months unemployment is 1 in 6. Total people not in employment (including Jobseekers Allowance claimants) is over 12,000 people in West Sussex.
Low employment rate of under 25 % for people with a mental health
condition.
Over 50 % of people would not disclose to an employer.

What we do

Paritas Services
Paritas provides talented people to meet recruitment needs
Paritas helps to manage wellbeing in your workplace
Paritas provides ongoing access to mental healthinformation, training and resources.
Paritas acts as a champion in promoting wellbeing in the workplace and positive images of mental health.
The audit tool
Designed to enable public sector to,
Meet strategic objectives & policy requirements.
Support wellbeing of current workforce.
Recruit people who have experienced mental health problems
Create workplace accessible to disadvantaged people
Exemplar Employer
Employer Training
Delivered to over 300 managers across WSCC, NHS West Sussex,Library service & Fire and Rescue service
‘Mental Health and Employment’ training designed to provide in-depth and stimulating training to managers
Delivered through training seminars and supported byParitas Line managers guide

Recruitment services
Partnership with Recruitment Agency
Assessment and matching
Ongoing vocational support
Impact and success
Recommendations for introduction

Creating mentally healthy organisations
Enable
Develop
The Paritas services can
The Paritas services could
achievement of strategic objectivities and policy requirements.
support for wellbeing of current workforce
recruitment of people who have experienced mental health problems.
becoming an exemplar employer
partnership working of public sector in South East.
setting of cross organisation benchmarks
sharing of good practice
becoming an exemplar public sector network

Enabling People

David Cain
01903 204083 [email protected] 603813
diversity is a fact of being human
diversityis inclusive of all people
diversityis how we are different

Panel Discussion
How to make it work

Panel Discussion
How to make it work

Locality Support Groups
Diversity in practice

Case Study
“Out of the blue your job is gone, and with it any financial security you may have had. At a stroke, you have no
purpose in life, and no contact with other people. You find
yourself totally isolated from the rest of the world. No one telephones you. Much less writes. No-one seems to care
if you are alive or dead.”Realising ambition December 2009
Posed by model

Case Study“My first job, a few months after leaving
the psychiatric hospital, was as a
customer services assistant. Previous to this I had no experience in the retail
industry so the prospect of serving customers, during probably the busiest
time of the year, was incredibly
daunting. But what became apparent was that, whilst working in a busy store
and having so many customers to serve I wasn’t reflecting on my thoughts or
becoming paranoid about my problems. Remaining focused upon the jobs
required, coping with having lots of
people around, made it much easier.”Realising Ambitions (Dec 2009) Posed by model

Case Study
• Started part time work at school
• Foxes Academy
• Moved to supported Living
• Work experience in local pub
• Prepares sandwiches, vegetables etc
• Learnt to travel on bus
• Offered paid job
• Staff very supportive
• Parents support important
“All we wanted for Mikael was a normal life. Thanks all those who have helped, he
now has a job, a flat and friends and is part of his local community”
Mikael’s mum

Close
Thank you for coming and to all those who contributed to today’s event – please complete feedback
Top Related