







Languages
Pages
Legal


7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 1/70
IV
and the liver

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 2/70

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 3/70
Introduction

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 4/70
Introduction
Managing liver disease is an increaimportant component to the caindividuals infected with himmunodeficiency virus (HIV).
Since the advent of effective antirettherapy (ART) for HIV, there has bsubstantial decrease in deaths relatacquired immunodeficiency syndrome (
7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 5/70

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 6/70
HIV
and the liver
However, liver disease has emerged most common non-AIDS related caudeath among HIV-infected paaccounting for 14-18% of all deaths.
In some series, nearly half of deaths ahospitalized HIV-infected patients in thera have been attributed to liver disease

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 7/70
HIV
and the liver
Just as the burden of non-AIDS morbidmortality has changed in the ART-etypes of liver disease the clinician is lencounter among these patients have cas well.

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 8/70
HIV
and the liver
Landscape of liver disease has changed◦pre-ART : CMV, mycobacteria, NHL & KS
◦post-ART: HCV, HBV, DILD, alcohol abuse,

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 9/70
The effect of HIV on the liver
Liver disease in human immunodeficien(HIV)-infected individuals encompassspectrum from:◦abnormal liver function tests,◦liver decompensation, with and without ev
cirrhosis on biopsy,◦non-alcoholic liver disease and its more sevnon-alcoholic steatohepatitis,
◦hepatocellular cancer.

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 10/70

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 11/70
Pathogenesis of HIV and liver
disease
HIV may alter liver function by either diindirect mechanisms.
HIV predominantly infects CD4+ monocyte/macrophages and dendritic cells.
However, there are multiple studies now sHIV infection of a wide range of non hemacells, including cells in the liver.

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 12/70
Pathogenesis of HIV and liver
disease
In addition, changes in gastrointestitract permeability via massive depletiotract associated CD4+ T-cells by HIV mindirect consequences on immune acand liver disease.

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 13/70

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 14/70

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 15/70

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 16/70

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 17/70
Differential diagnosis of liver disease
in HIV infection in the ART-era
HEPATIC PARENCHYMAL DISEASE◦Infection◦ Viral Hepatitis: HCV, HBV, HDV, HAV, HEV, CMV, EBV
HHV6◦ Mycobacterium avium complex◦ Cryptococcus neoformans
◦ Microsporidium◦ Pneumocystis jirovecii◦ Bacillary peliosis hepatis◦ Histoplasma capsulatum

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 18/70
Differential diagnosis of liver disease
HIV infection in the ART-era
HEPATIC PARENCHYMAL DISEASE◦Nonalcoholic fatty liver disease
◦Medication toxicity
◦Alcoholic liver disease
◦Recreational Drugs◦Cocaine
◦MDMA (Ecstasy)

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 19/70
Differential diagnosis of liver disease in H
infection in the ART-era
Neoplasm◦Lymphoma◦Kaposi's sarcoma◦Hepatocellular carcinoma
Nodular regenerative hyperplasia Autoimmune hepatitisHemochromatosisWilson's disease
Alpha-1 antitrypsin deficiency

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 20/70

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 21/70
Coinfection
People with HIV infection are often affeviral hepatitis; about one-third are coiwith either HBV or HCV, which can cauterm illness and death.

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 22/70
Coinfection
Although drug therapy has extended expectancy of people with HIV, liver much of which is related to HCV and Hbecome the leading cause of non-AIDS
deaths in this population.

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 23/70
Coinfection
More people living with HIV have HCHBV.
Viral hepatitis progresses faster andmore liver-related health problems people with HIV than among those whohave HIV.

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 24/70

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 25/70
HIV Hepatitis C Virus
Overall, approximately 30% of HIV-individuals in the United States and Eurcoinfected with HCV.
Due to shared risk factors, coinfectioHCV and HIV is common.

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 26/70
HIV Hepatitis C Virus
Reported prevalence rates of Hcoinfection vary depending on the routtransmission, from 10% among thohigh-risk sexual behavior to 90% with i
drug use.

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 27/70
Effect of HIV on HCV
◦Less likely to clear HCV◦Higher HCV viral load◦Accelerated fibrosis and more cirrhosis (2-fold◦Higher risk of liver failure once cirrhotic (5-fo◦Probably higher risk of HCC
◦Less likely to respond to treatment
Effect of HCV on HIV less clear

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 28/70
HCV HIV/HCV Coinfection
Sexual transmission islow (0-3%)
Mother-to-ChildTransmission ~5-6%
HCV meds can cause birthdefects
Sexual transmissionhigher ~ 15-25%
Mother-to-ChildTransmission ~25%
HCV meds can cause bdefects
HCV Transmission
www.hcvadvocate.org
i i C
7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 29/70
Hepatitis C HIV/HCV Coinfection
Antibody Test
HCV Viral load toconfirm activeinfection
Antibody Test
Note: If low cd4 cellcount use HCV RNA
HCV RNA to confirmactive infection
Diagnosing HCV
www.hcvadvocate.org
*People with a comprised immune system may not develop HCV antibodies

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 30/70
Hepatitis C HIV/HCV Coinfection
Slow rate of diseaseprogression – usuallyover 10, 20, 30 years
Faster rate of diseaseprogression to cirrhosiup to 2-3 times faster &can occur in as little as years
HCV coinfection is theleading cause of deathamong people with HIV
HCV Disease Progression
www.hcvadvocate.org
Guidelines for Prevention of Opportunisti

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 31/70
Guidelines for Prevention of OpportunistiInfections
HIV–
Infected persons should be screened for HC Patients should be advised on alcohol use
Patients should be screened for HAV & HBV ifnegative, they should be vaccinated
Patients should be evaluated for liver disease and
possible need for treatment Liver enzymes should be monitored after initiatio
HAART
*U.S. Public Health Service and the Infectious Disease Society of America
www.hcvadvocate.org
7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 32/70
Treatment of hepatitis C virus
infection in the HIV-infected patient
HCV REGIMEN SELECTIONRegimen options by genotype
- Genotype 1 infection
- Genotype 2 infection- Genotype 3 infection
- Genotypes 4 infection

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 33/70
Treatment of hepatitis C virus
infection in the HIV-infected patie
Potential drug interactions with ART- Ribavirin
- Sofosbuvir
- Ledipasvir-sofosbuvir- Ombitasvir-paritaprevir-ritonavir plus da
- Simeprevir
7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 34/70
Clinical management of
HCV/HIV patients
The key issue in the clinical management of HCV/HIV
patients is the treatment decision for each condition ainitiate it.
By the end of the laboratory and clinical assessment with HCV/HIV coinfection, patients can be split
categories:◦ 1. patients not requiring hepatitis C or HIV/AIDS treatmen◦ 2. patients requiring only hepatitis C treatment◦ 3. patients requiring only HIV/AIDS treatment◦ 4. patients requiring both hepatitis C and HIV/AIDS treatm

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 35/70
1. Coinfected patients not
requiring any treatment
Coinfected patients not requiring any trmeet the following criteria:
◦ CD4 count >350 cells/mm3 and absence of HIV-relatedand
◦ HCV antibodies, but absence of HCV RNA replication.
Coinfected patients not needing treatment smonitored every six months (clinical followfunction tests) and every three years for hisliver lesions (using alternatives to liver biopsie

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 36/70
2. Coinfected patients requiring
only HCV treatment
Coinfected patients requiring onltreatment meet the following condition◦ CD4 count >350 cells/mm3 and absencerelated symptoms, and
◦ active or chronic hepatitis CHCV treatment offers the possiberadicating HCV within a defined treperiod.

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 37/70
2. Coinfected patients requiring
only HCV treatment
In the following situations, where the outweigh the risks, there are two main reconsider all HCV/HIV-coinfected patients treatment:◦ The liver disease progresses more rapidly to complications and at earlier ages than
monoinfected patients.◦ Patients are at higher risk for developing hepafollowing the initiation of ART than HIV-mopatients. Efficient HCV treatment will hence facsubsequent management of ART.

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 38/70
3. Coinfected patients requiring
only HIV/AIDS treatment
Coinfected patients requiring only Htreatment satisfy at least one condition inthe following◦ CD4 count ≤350 cells/mm3 in symptomaticor patients with viral load >100 000 copies/mcount ≤200 cells/mm3 irrespective of symptoand◦ HCV antibodies but no HCV RNA replichepatitis C with contraindications to treatme

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 39/70
Why Is HCV Therapy Deferred in
Many HIV/HCV-Coinfected Patient
Challenges with interferon- and/or ribavirregimen
Anticipated approval of new agents◦Greater efficacy
◦All-oral regimens◦Shorter duration◦Improved tolerability◦Fewer drug-drug interactions
clinicaloptions.com/hepatitisBest Practices in the Management of HCV/HIV Coinfection

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 40/70
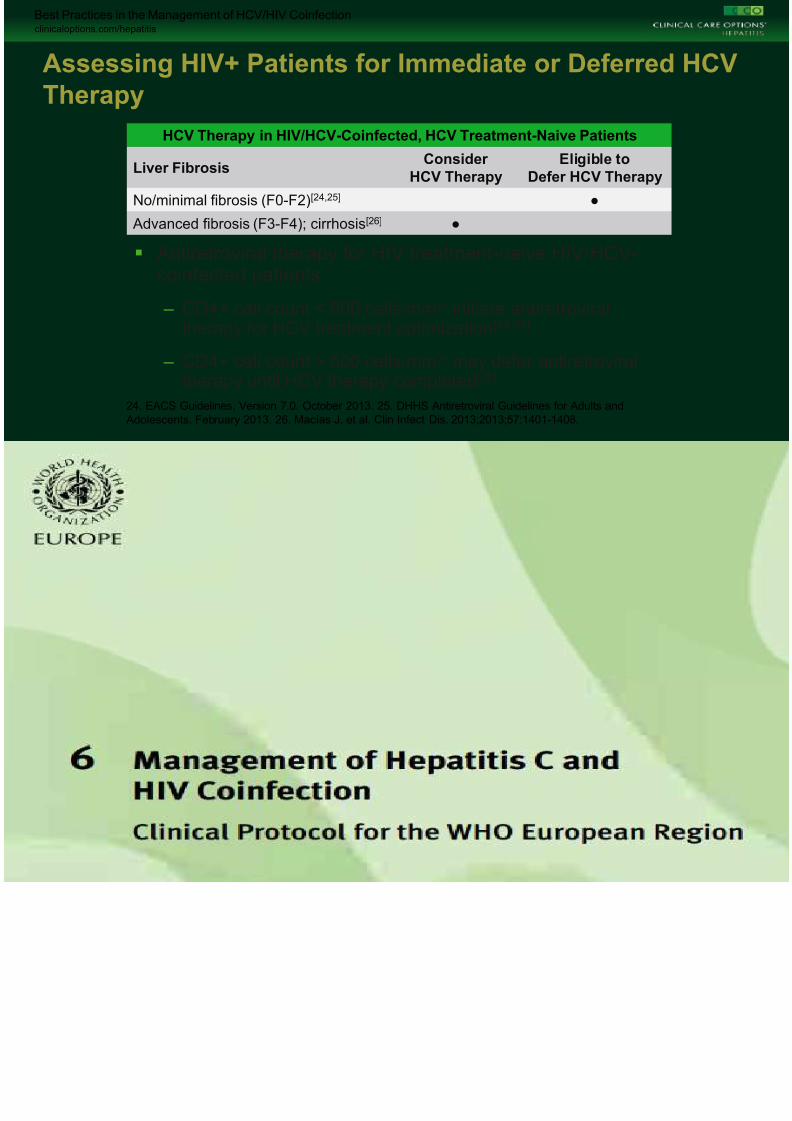
Assessing HIV+ Patients for Immediate or Defer
Therapy
Antiretroviral therapy for HIV treatment-naive HIV/HCVcoinfected patients
– CD4+ cell count < 500 cells/mm3: initiate antiretroviraltherapy for HCV treatment optimization[24,25]
– CD4+ cell count > 500 cells/mm3: may defer antiretroviratherapy until HCV therapy completed[25]
24. EACS Guidelines, Version 7.0. October 2013. 25. DHHS Antiretroviral Guidelines for Adults and
Adolescents. February 2013. 26. Macías J, et al. Clin Infect Dis. 2013;2013;57:1401-1408.
HCV Therapy in HIV/HCV-Coinfected, HCV Treatment-Naive Patients
Liver FibrosisConsider
HCV Therapy
Eligible to
Defer HCV The
No/minimal fibrosis (F0-F2)[24,25] ●
Advanced fibrosis (F3-F4); cirrhosis[26] ●

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 41/70

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 42/70
Clinical management of
HCV/HIV patients
1. Coinfected patients not requiring any
2. Coinfected patients requiring only HCV ◦ Indicationsfor HCV treatment◦ Predictors of sustained virological response ◦ Contraindications for hepatitis C treatm◦ Treatment of acute hepatitis C
◦ Treatment of chronic hepatitis C (doseschedules)
◦ Treatment duration

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 43/70
Clinical management of
HCV/HIV patients
3. Coinfected patients requiring HIV/AIDS treatment◦ Initiation of HAART
◦ Considerations in choosing a
regimen◦ First-line HAART regimens
◦ Second-line HAART regimens

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 44/70
Clinical management of
HCV/HIV patients
4. Coinfected patients requiring bothand HIV/AIDS treatment
◦ Strategy for initiationof treatment◦ Considerations of ARVs when
both HCV and HIV infections
◦ Hepatotoxicity of ARV drugs◦ ARV dose adjustment in patients
cirrhosis

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 45/70
HBV

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 46/70
HIV Hepatitis B Virus
Although the prevalence of Hcoinfection varies by geographic lapproximately 10% of HIV-infected indworldwide are also chronically infect
HBV.

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 47/70
Effect of HIV on HBV
Like HIV-HCV coinfection, HIV alters thehistory of HBV.
Individuals with HIV infection are 3-6 timlikely to develop chronic HBV after aexposure than individuals without HIV inand hepatitis B surface antibody (adevelopment is improved with higher counts.

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 48/70
Effect of HIV on HBV
In addition, HIV-infected patients have a lowe
spontaneous clearance of HBeAg, increased HBV rand a higher rate of loss of anti-HBs and reactivatio
Coinfected individuals also experience an progression to cirrhosis and higher liver-related
compared to HBV monoinfected individuals.
The impact of HBV infection on the natural historless clear.

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 49/70
Clinical management of
HBV/HIV patients
The decision to initiate HBV treatment on whether the patient meets indicationseither the HIV or HBV.
Treatment regimens for either virus must both infections, as many anti-viral agendual activity, including tenofovir, lamemtricitabine, entecavir, and adefovir a>10mg.
Clinical management of

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 50/70
HBV/HIV patients
Treatment for HBV is indicated in any paticirrhosis and detectable HBV DNA.
Although a specific HBV DNA threshtreatment in the absence of cirrhosis has n
determined, treatment should be consipatients with HBV DNA ≥ 2,000 IU/mL athan mild liver disease on biopsy
Clinical management of

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 51/70
HBV/HIV patients
Rx: initiation depends on meeting criteria for either virus
~ dual activity of antivirals: TDF, LAM, emtricitabine, entecavir• Rx if HBV DNA > 2000 iu/ml & > mild disease on Bx
• Use Truvada or TDF and LAM
• Use entecavir if TDF contraindicated
• If ART not feasible try pIFN, adefovir, telbivudine
• Worsening ALT and AST during ART:
~ DILD, HBV reactivation on drug withdrawal esp LAM, HBeAg
loss or IRIS
• Screen for HCC

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 52/70

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 53/70
Drug Induced liver Disease
Risk factors for DILD:
• ~ HBV or HCV coinfection~ advanced hepatic fibrosis
~ pre-Rx ALT, AST
~ alcohol
~ older age
~ first exposure to ART~ CD4
~ concomitant anti-TB rx
~ cocaine use
Partial list of potentially hepatotoxic non-A

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 54/70
medications prescribed to HIV-infected
individuals

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 55/70
Most common ART agents associated
with liver injury in HIV-infected patien
MEDICATION TYPICAL DOSE DOSE ADJUSTMENT
FOR HEPATICINSUFFICIENCY
MEC
NNRTI
Nevirapine (NVP) 200 mg po bid Child-Pugh Class B or
C: Contraindicated
H
rea
Etravirine (ETR) 200 mg po bid Child-Pugh Class A or
B: No adjustment
Child-Pugh Class C: Not
H

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 56/70
Most common ART agents associated
with liver injury in HIV-infected patien
MEDICATION TYPICAL DOSE DOSE ADJUSTMENT FOR
HEPATIC
INSUFFICIENCY
MECH
PI
Ritonavir (RTV) full-
dose
No longer used Di
Tipranavir (TPV) + RTV
low-dose
(TPV 500 mg + RTV 200 mg) po
bid
Child-Pugh Class A: Use with
caution
Child-Pugh Class B or C:Contraindicated
Di
Atazanavir (ATV) 400 mg po once daily Child-Pugh Class B : 300 mg po
once daily
Child-Pugh Class C:
Contraindicated
Indi
doe
Indinavir (IDV) 800 mg po q8h Mild to moderate hepatic
insufficiency:
Indi
doe

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 57/70
Most common ART agents associated
with liver injury in HIV-infected patient
MEDICATION TYPICAL DOSE DOSE ADJUSTMENT FOR
HEPATIC
INSUFFICIENCY
MECH
NRTI
Stavudine (D4T) ≥60 kg: 40 mg po bid
<60 kg: 30 mg po bid
Not defined M
Zidovudine (AZT, ZDV) 300 mg po bid Not defined M
Didanosine (ddI) Enteric coated:
≥60 kg: 400 mg po once daily
<60 kg: 250 mg po once daily
Oral Solution:
≥60 kg: 200 mg po bid or 400
mg po once daily
<60 kg: 150 mg po bid or 250
mg po once daily
No adjustment M
cry

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 58/70
Most common ART agents associated
with liver injury in HIV-infected patient
MEDICATION TYPICAL DOSE DOSE ADJUSTMENT FOR
HEPATIC
INSUFFICIENCY
MECH
NRTI
Abacavir (ABC) 300 mg po bid Child-Pugh Class A: 200 mg po
bid (use
oral solution)
Hy
es
Lamivudine (3TC) 300 mg po once daily or 150
mg po bid
No adjustment H
me
Emtricitabine (FTC) Oral capsule: 200 mg po once
daily
Oral solution: 240 mg po once
daily
Not defined H
me
Tenofovir (TDF) 300 mg po once daily No adjustment H
me
Most common ART agents associated

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 59/70
with liver injury in HIV-infected patien
MEDICATION TYPICAL DOSE DOSE ADJUSTMENT FOR
HEPATICINSUFFICIENCY
M
Other
Enfuvirtide (T20) 90 mg subcutaneous
bid
Not defined H
Maraviroc (MVC) Recommended dose
depends on other
drugs in
regimen
Not defined, caution
advised
H
rea

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 60/70

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 61/70
Fatty liver disease in HIV
NAFLD is now commonly reported ihigh income countries in the presenabsence of HIV infection.
The spectrum of NAFLD ranges frosteatosis to NASH, which may progsevere fibrosis and cirrhosis.

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 62/70
Fatty liver disease in HIV
NAFLD has been identified in up to 30%
mono-infected Americans, although thwas unable to demonstrate whethprevalence of NAFLD was different negative individuals.
While risk factors for NAFLD may be sipeople with or without HIV

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 63/70
• Screen all HIV-infected patients with HCV antibody
• Test HCV RNA in patients with positive HCV antibody If Ab negat

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 64/70
HCV
• Test HCV RNA in patients with positive HCV antibody. If Ab negatif suspected acuteHCV, or significant risk factors and advanced immunosuppression
• If chronic HCV, immunize against HBV and HAV if not immune
HBV
• All HIV-infected patients should be screened with HBsAg, anti-HB
• Vaccinate patients without HBV immunity
• When initiating or adjusting ART, regimen must include adequatecoverage
• Vaccinate against HAV, if not immune
• Requires concomitant HBV infection for replication
• Acquired during simultaneous infection with HBV or as superinfection in set

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 65/70
HDV• HDV superinfection is associated with fulminant acute hepatitis and severe
hepatitis
HEV
• Consider in patients with travel to endemic areas; autochthonous cases havreported inUnited Kingdom, France, Germany, and the United States
• Chronic infection has been reported in HIV-infected patients
HAV• Can cause fulminant hepatitis especially in presence of underlying liver dise
• Rarely symptomatic; may present with fever, malaise, weight loss
• Usually mild transaminitis and mild cholestasis

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 66/70
CMV
• Usually mild transaminitis and mild cholestasis
• May present as mass and mimic neosplasm on CT
• Liver biopsy with large intranuclear and small cytoplasmic inclusigranulomas
Mycobacterium
avium complex
• Presents with fever, night sweats, weight loss, abdominal pain, nHSM
• Marked elevation of AP (>10-20x ULN) is hallmark
• U/S shows diffusely hyperechoic liver +/− focal lesions
• Liver biopsy with poorly formed non-caseating granulomas, foamacid-fast bacilli
• Presents with fever, night sweats, weight loss, LAD, and hepatomegaly
• AP usually elevated with mildly elevated aminotransferases and bilirubin
U/S h diff l h h i li / f l l i b h l b

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 67/70
Mycobacterium
tuberculosis
• U/S shows diffusely hyperechoic liver +/- focal lesions; abscesses have also been
• Liver biopsy with well formed granulomas
Pneumocystis
jirovecii
• More common in patients receiving inhaled pentamidine for PCP prophylaxis
• Usually moderate increases in aminotransferases and AP, but high elevations hav
• CT may show hepatic calcifications
• Liver biopsy with foamy nodules with pneumocystis cysts on methamine silver st
Microsporidium
• May cause increased bilirubin, transaminases, and especially AP
• Consider in patients with a history of cat contact
• May present with HSM, liver failure, portal hypertension, fever, anemia, LAD

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 68/70
Bartonella
henselae
• AP elevated; may develop coagulopathy
• U/S may show irregular hypoechoic regions
• CT may reveal multiple hypoattenuating lesions of varying size
• Liver biopsy with multiple blood-filled cavities of varying size
Histoplasma
capsulatum
• May be asymptomatic or present with constitutional symptoms, LAD and HSorganfailure in fulminant cases
• Labs usually show cholestasis with increased AP, variable bilirubin
• Liver biopsy with poorly formed granulomas, rounded yeast with budding on

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 69/70

7/23/2019 HIV&liver (1)
http://slidepdf.com/reader/full/hivliver-1 70/70
Top Related