






Languages
Pages
Legal


Global impact of ischemic heart disease
World Heart Federation, 2011
The Problems Despite recent advances in treatment, cardiovascular disease
(CVD) remains the leading cause of death in the US. From 1996 to 2006 the number of inpatient cardiovascular procedures
increased from 5,400,000 to 7,235,000 annually. Costs of CVD in the U.S. – both direct and indirect – are estimated to
be $503 billion this year. At the present rate, due in large part to the ticking time bomb of obesity
and poor nutrition in children, within 20 yr over 40% of the U.S. population will have CVD, with a cost to our health care system of over $1 trillion dollars per year.
While improved CVD prevention is of critical importance, there are major barriers: Current screening does not identify many who are at risk. Dietary and lifestyle guidance has failed to substantially impact risk
factors, particularly those related to overweight and obesity.
American Heart Association, Circulation 2010
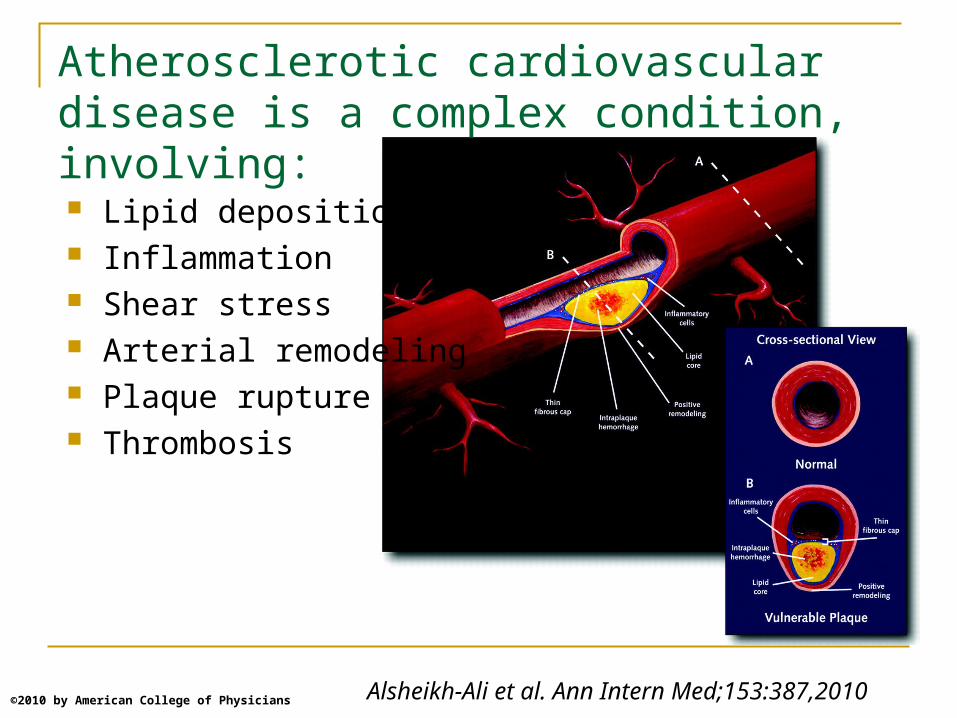
Alsheikh-Ali et al. Ann Intern Med;153:387,2010©2010 by American College of Physicians
Atherosclerotic cardiovascular disease is a complex condition, involving:
Lipid deposition Inflammation Shear stress Arterial remodeling Plaque rupture Thrombosis

What are the major risk factors for CVD?
Unmodifiable: age, family history, sex Modifiable:
Lipids: LDL (high) and HDL (low) Elevated blood pressure Smoking Diabetes
Other factors Diet Overweight/obesity Physical activity
NHLBI Adult Treatment Panel 3, 2001

CHD Risk: HDL-Chol and LDL-Chol as Predictors
0.0
1.0
2.0
3.0
100 160 220 8565
4525
LDL Cholesterol mg/dL
HDL Cholesterol mg/dL
Adapted with permission from Castelli WP. Can J Cardiol.4:5A. 1988
Ris
k o
f CH
D a
fter
4 y
r
Men aged 50–70 y in the Framingham Heart Study

How well do standard cholesterol values predict CVD risk?
LDL cholesterol
HDL cholesterol
mg/dL
MI Cases (n=1575)
146 44
Controls (n=1570)
139 48
Baseline values in Malmo Diet and Cancer Studyin myocardial infarction (MI) cases and controls at 15 year followup
I have some bad news. While yourcholesterol level has remained the same,the research findings have changed.
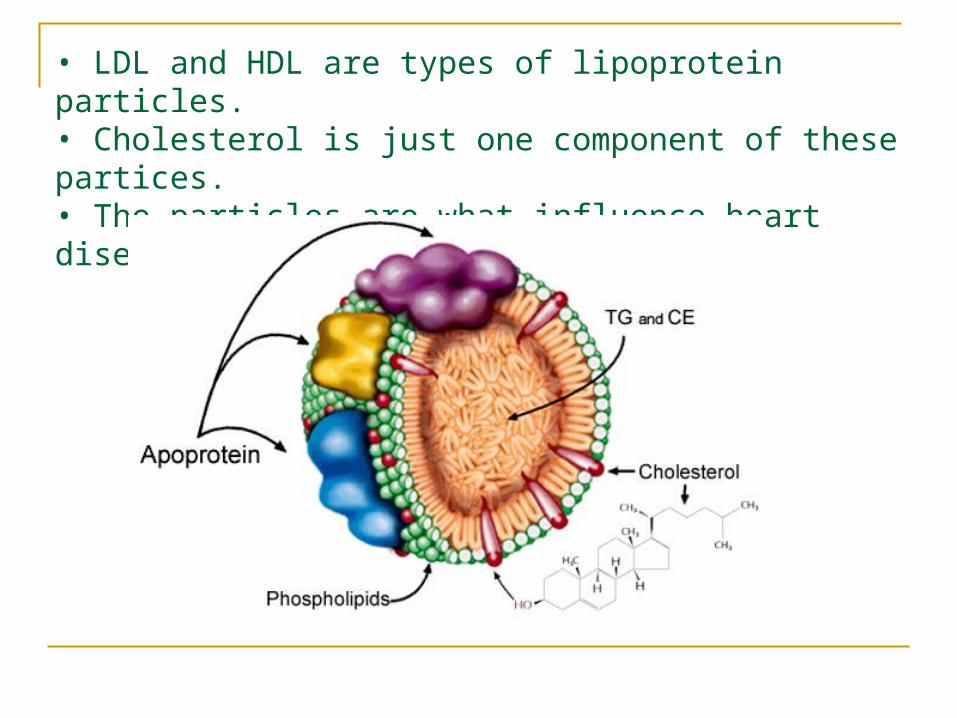
• LDL and HDL are types of lipoprotein particles.• Cholesterol is just one component of these partices.• The particles are what influence heart disease risk.
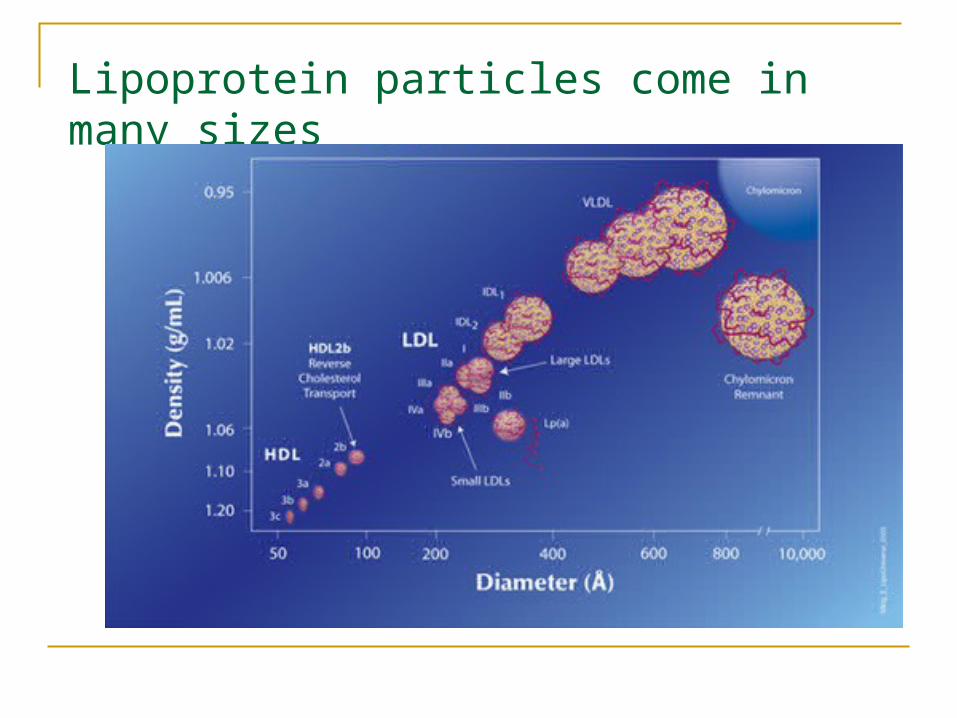
Lipoprotein particles come in many sizes

Large MediumSmallVery Small
• Most abundant subclass in healthy individuals
• Reduced blood clearance• Greater entry in artery• Faster oxidation• Associated with metabolic syndrome/ diabetes/obesity• Genetic influences
Distinct LDL subclasses have differing properties
Distribution of subclasses varies widely among individuals and is independent of total LDL cholesterol
Lp (a)
• Multiple atherogenic effects
• Very strong genetic influence
0
50
100
150
200
250
300
350Particle conc.nmol/L
IDL large med small v small
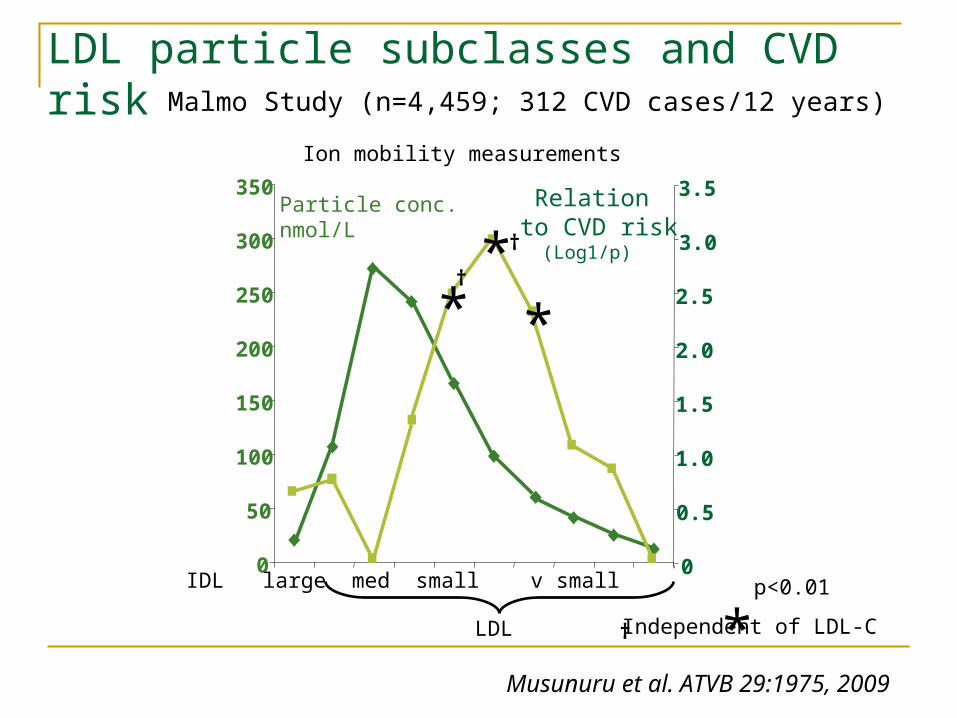
LDL particle subclasses and CVD risk
†
0
0.5
1.0
1.5
2.0
2.5
3.0
3.5 Relationto CVD risk (Log1/p)***
*p<0.01
†
† Independent of LDL-C
Malmo Study (n=4,459; 312 CVD cases/12 years)
Ion mobility measurements
LDL
Musunuru et al. ATVB 29:1975, 2009

Issues regarding HDL cholesterol as a CVD biomarker and drug target• There is strong epidemiologic and pathophysiologic evidence for a relation of HDL cholesterol to CVD risk.
• However, HDL is even more heterogeneous than LDL and includes multiple subpopulations of particles with differing functional properties and disparate effects on atherogenic mechanisms.
• HDL levels are regulated by pathways that also affect LDL subclasses and other lipids; and Increases in HDL-C by lifestyle and drug interventions can result from multiple different metabolic effects.
• There is as yet no conclusive evidence in humans for an independent benefit of HDL increase on CVD outcomes.
Case study: AIM-HIGH study of HDL raising with niacin added to statin
All pts had CVD and most were on a statin at entry, with very low LDL cholesterol during the study.
HDL cholesterol increased by ~22%. During the 32 mo follow-up period, the rate of clinical events
was not different with niacin vs. placebo, and there was no evidence that this would change by continuing the trial (p<0.0001).
There was also an excess of strokes in the niacin group. The study was terminated 5/26/11. Thus, at least in the setting of maximal LDLreduction in
patients with CVD, there appears to be no benefit of raising HDL-C with niacin.

New findings and issues involving lipoproteins and CVD risk
LDL There is considerable residual CVD risk with statins, the
drug class most widely used to reduce LDL levels Statins are less effective in reducing small vs. large LDL Genetic factors can contribute to variation in statin
efficacy Effects of statin on inflammation appear to contribute to
CVD benefit, and are weakly correlated with LDL reduction
New findings and issues involving lipoproteins and CVD risk
HDL There at least 30 different proteins in HDL particles that
may influence multiple functions. One of these functions, the ability of HDL to promote
removal of cholesterol from arterial cells, is significantly related to CVD risk benefit – and this effect is independent of HDL cholesterol.
The specific features of HDL responsible for this effect are poorly understood.
And, there appear to be some forms of HDL particles that are pro-inflammatory, and hence may increase CVD risk.
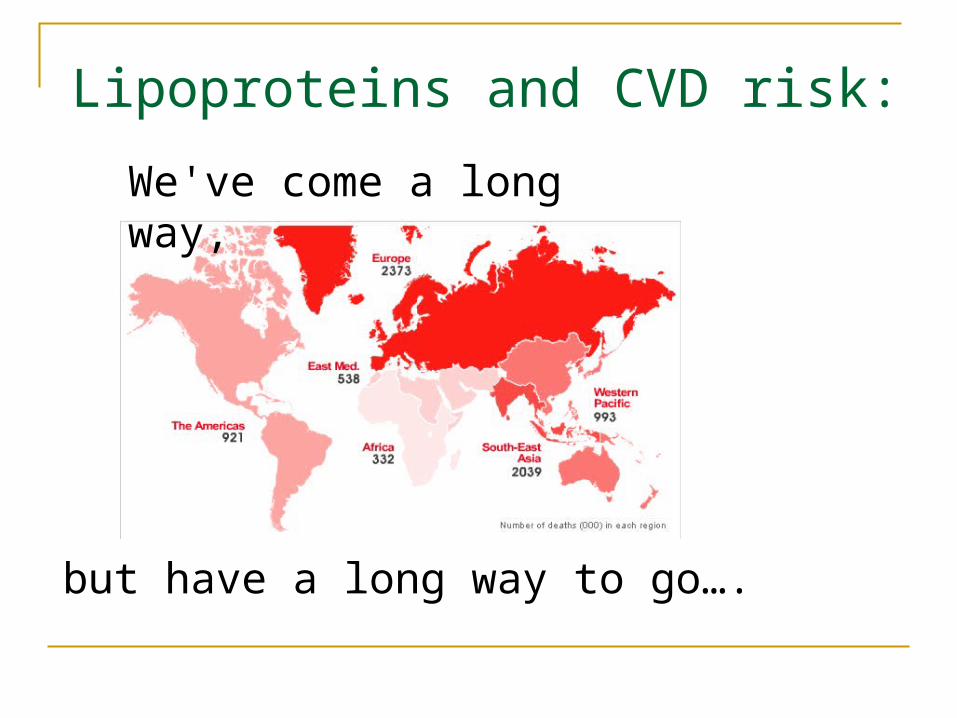
Lipoproteins and CVD risk:
We've come a long way,
but have a long way to go….
Top Related