






Languages
Pages
Legal


Ageing well: a complex topic for research and for practice
Gail MountainProfessor of Health Services Research
(assisted living)

What makes it complex?

Incorporates our own perceptions and experiences
What we knowThe following are key to wellbeing in later life:-•Participation•Health
These factors erode wellbeing:-•Poor physical health•Loss such as unplanned retirement, widowhood•Loneliness/ poor psychological health
How to limit the negative factors and promote those that are positive?
No simple solutionsForthcoming NICE guidance will promote the importance of multi component interventions that can be personalised (in addition to PH guidance 16)

University of Southern California
Centre for Lifestyle Redesign
Starting with the Concept of Lifestyle
Redesign.....The process of developing and enacting a customised routine of health promoting and meaningful daily activities (Clark 1998 in Mandel 1999)
The Well Elderly study of Lifestyle Redesign
Clark, et al (1997) Occupational Therapy for independent older living adults: a randomised controlled trial. Journal of the American Medical Association, 278, 1321-1326
•Participants experienced benefit; health, function and quality of life •Benefit was sustained six months later
•The interventions were cost effective
The Lifestyle Matters ethos
• A preventive health approach which focuses on the benefits of activity
• Underpinned by the belief that what we do on a day to day basis is central to our health and wellbeing
• And that positive changes can only be sustained if they are embedded within what a person does on a day to day basis

UK Medical Research Council Complex Interventions framework (2008)
Development
Feasibility and Pilot
Evaluation
Implementation
http://www.bmj.com/content/337/bmj.a1655
Complexity: need for research and clinical skills/ knowledge
Lifestyle Matters programme
• Developed in partnership with older people for older people in the UK
• Inspired by Lifestyle Redesign®; a programme developed and tested in the US

A model of preventive health: group and individual interventions

The UK programme: selecting from a menu of activities
Beginnings: celebration
Activity and health
• The ageing process and activity• Personal energy, time and activity • Goals; realising hopes and wishes• Pulling things together – how is activity related to
health
Ideas continued…
Maintaining mental wellbeing
• Sleep as an activity• Keeping mentally active• Memory
Maintaining physical wellbeing
• Nutrition• Pain• Keeping physically active

And more…Occupation in the home and community
• Transportation• Opportunities for new learning• Experiencing new technologies
Safety in and around the home
• Keeping safe in the community• Keeping safe in the home

Yet more….
Personal circumstances
• Dealing with finance• Social relationships and maintaining friendships• Dining as an activity• Interests and pastimes• Caring for others, caring for self• Spirituality
Endings
Feasibility Study (2004-2005)What we had to consider
Recruitment of older people: community living
Who will deliver the programme and how will they be trained and supported: different to US model
Outcome measures necessary for a future randomised controlled trial

Results of feasibility study
• Twenty eight people aged 60 and over commenced the eight month programme and 26 completed it
• They still meet together independently (several years later)
• Post intervention interviews illustrated the benefits participants experienced with greater self efficacy being a significant theme
(Mountain & Craig, Occupational Therapy International, 2011)

Results cont.
• Comparison of pre and post scores on quantitative measures showed upward trends on all dimensions of quality of life (Mountain et al, British Journal of Occ Therapy, 2008)
• Measurement of cognition and dependency proved useful for screening purposes and for identifying individuals at risk, but not as outcome measures

Outputs from the feasibility study
Results used to inform national guidance alongside well elderly study http://guidance.nice.org.uk/PH16
Intervention published

Funded by the UK Medical Research Council 2011-2015
1.3M over 4 years
http://www.sheffield.ac.uk/lifestylematters
Lifestyle Matters programme of research
Population based study of effectiveness: RCT
Evaluation of cost effectiveness: HE evaluation embedded
Research into implementation: process evaluation and fidelity assessment
Translation of findings into practice: open source – video, audio and web based material
Trial design• Two arm cluster randomised controlled trial (Lifestyle Matters and
‘standard care’)
• Two recruitment sites – Sheffield (urban) and Bangor, North Wales (rural)
• Outcome measures applied at baseline (consent), six months and two years
• Primary outcome: SF36 (mental health)
• Secondary outcomes: SF36 (physical health), General Self Efficacy scale, EQ5D, PHQ9, de Jong loneliness scale, health and social care utilisation
Intervention delivery
• Intervention delivered for 4 months in a community venue
• All participants offered monthly 1:1 sessions
• Intervention facilitated by grade 4 NHS equivalent staff (lower pay than for occupational therapists)
• Training provided for intervention delivery and weekly supervision
Recruitment
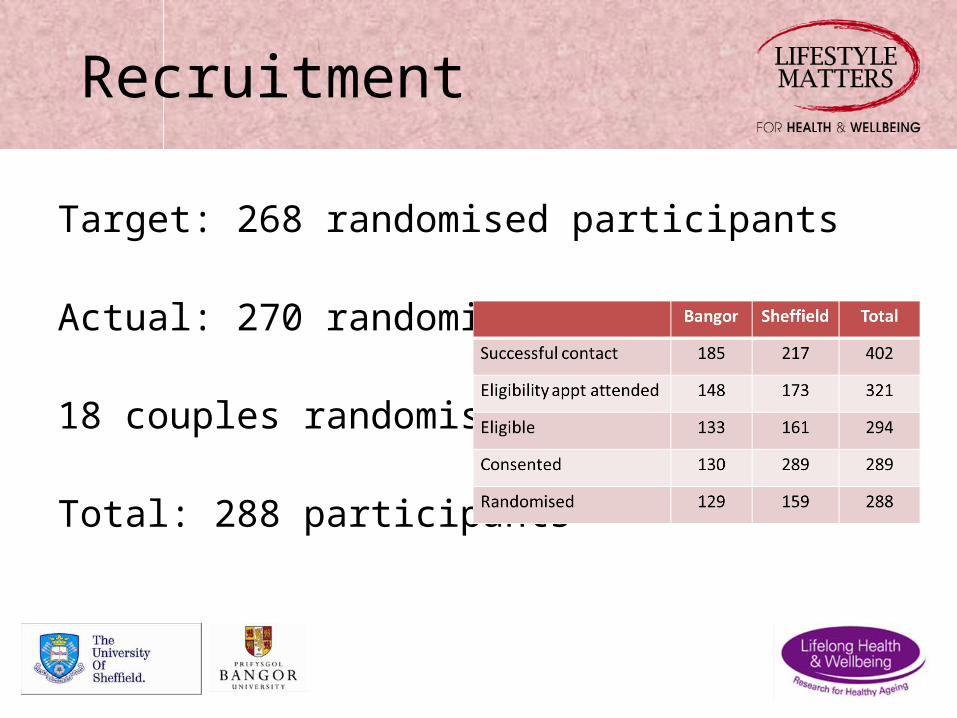
Target: 268 randomised participants
Actual: 270 randomised
18 couples randomised
Total: 288 participants

Review of recruitment strategies
•Most successful method was GP mail-outs
•9379 letters, sixteen surgeries in Sheffield and North Wales
•414 enquires. 389 result of the GP mail-outs representing a 4% response rate
•25 enquiries from direct referrers from NHS and community services and general advertising

Cycles of intervention delivery (9-16 participants per group)Sheffield Six groups
Two locations used
Bangor, North Wales Five groupsFour locations used
From feasibility to population based study
• Less ‘hands on’ - larger project team and range of involvement
• Broader range of participants, locations and venues and facilitators
• Devolved supervision arrangements
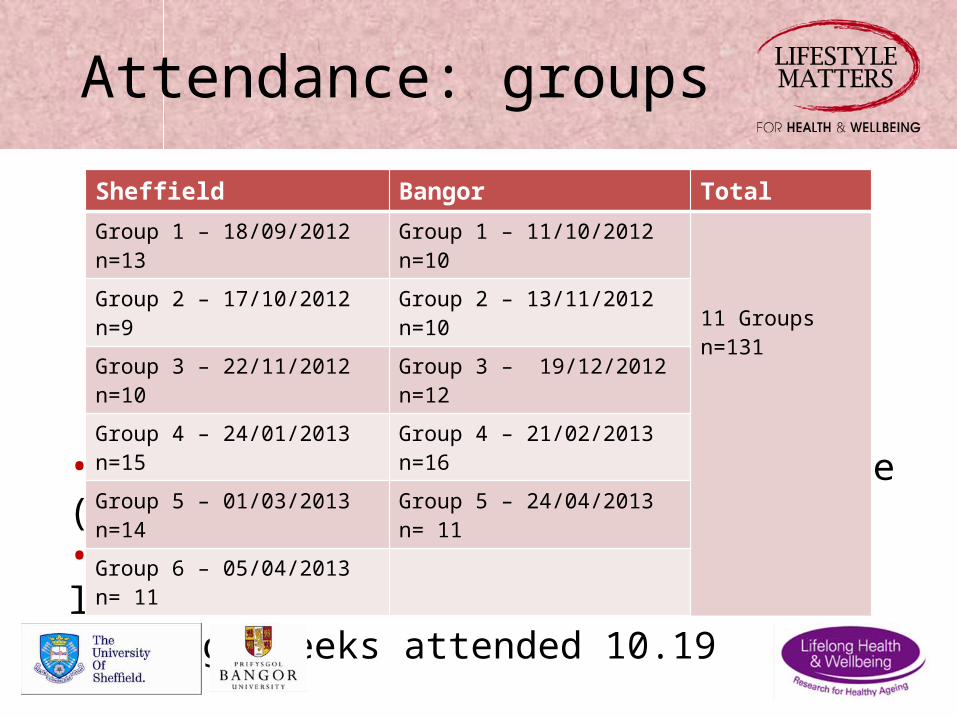
Attendance: groups
•n=97 (74%) received therapeutic dose (8 weeks)•n=34 attended 7 weekly sessions or less•Average weeks attended 10.19
Sheffield Bangor TotalGroup 1 – 18/09/2012 n=13 Group 1 – 11/10/2012 n=10
11 Groupsn=131
Group 2 – 17/10/2012 n=9 Group 2 – 13/11/2012 n=10
Group 3 – 22/11/2012 n=10 Group 3 – 19/12/2012 n=12
Group 4 – 24/01/2013 n=15 Group 4 – 21/02/2013 n=16
Group 5 – 01/03/2013 n=14 Group 5 – 24/04/2013 n= 11
Group 6 – 05/04/2013 n= 11

Outcomes of attendance: 1-1s
• 113 participants approached
• n=404 meetings offered
• n=143 meetings accepted (35% of those offered)
• n=124 meetings attended (87% of those accepted)
Number of 1-1 sessions attended
Number of participants
0 361 412 223 104 4
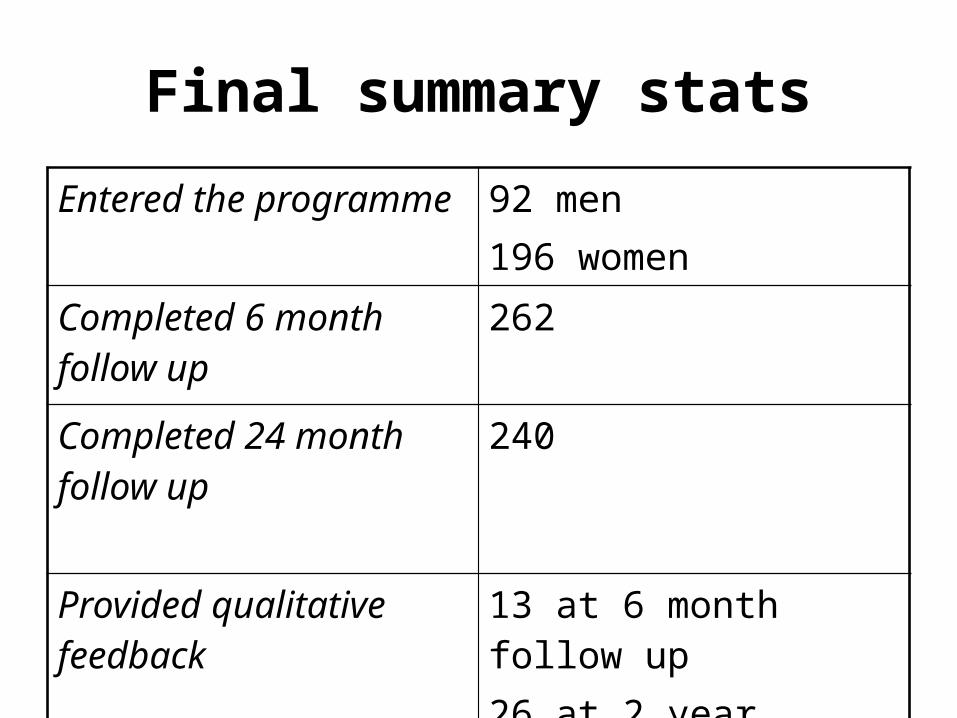
Final summary statsEntered the programme 92 men
196 women
Completed 6 month follow up
262
Completed 24 month follow up
240
Provided qualitative feedback
13 at 6 month follow up26 at 2 year follow up

Process evaluation
• Interviewed all 4 facilitators, 2 time points
• Interviewed all 3 OT supervisors post intervention
• Interviewed 13 participants (10% purposive sample) post intervention– Participants from 6 groups across all 3 cycles– Both sites (Sheffield n=7, Bangor n=6)– Selection criteria included age, sex, geographical area,
attendance as individual or part of a couple, education, previous occupation, level of current activity, number of sessions attended
Emergent results from process evaluation (facilitators)
• The facilitators did not change attitudes and understanding but did develop and improve their skills
• They enabled people to contribute and encouraged the group to make decisions rather than instructing and leading
• Group dynamics were important• Older people shared and developed coping strategies for
managing the challenges of ageing• The programme provided opportunities to try out new activities
and community facilities, which led to changes in routines and behaviour
• There was less evidence of the older people taking over the organisation of the group over the 4 months of delivery

Emergent results from process evaluation at 6 months (participants)
• Main reasons for not attending were illness or being ‘too busy’ but non attendance was also viewed negatively
• Concerns over male/ female mix"I remember when I went in there that first day and, oh
god, I was the only bloke there and I thought, what the hell have I let myself in for here? And when I was going, the last one [group meeting], I was quite, I was quite sad that it was over with, you know, because the group had joined in…as a gel, yeah, you know.
Emergent results from process evaluation (participants)
Challenges were posed by transport and the climate;
Shall we go, shan’t we go because of the snow and one thing and another, which again was unfortunate...when er, you know, we had two out of the, three out of the sixteen weeks...where I couldn’t go, er, and I mean I only live a couple of hundred yards away”.

Emergent results from process evaluation (participants)
Most of those interviewed indicated that with the support of the group and the facilitators they had found the impetus to pursue one or more activities or interests since taking part in the programme
I think what we’re going to do now, [wife] and I have decided that on Thursdays it should be an activity day for us…Erm but we’ve said, ‘OK, Thursday, we’ve enjoyed it so much, why don’t we go out and make Thursday an activity day’. We’ve nothing else to worry about, we’ve no dependents as such, we can go, go out any day, but Thursday ‘cause we’ve got into a routine, ‘yeah, let’s go and try so-and-so.

What might be the outcome?
• Results of feasibility study could be ‘diluted’ due to wider application
• Problems with implementing 1:1 sessions may have also diluted the effect
• Were the outcome measures most appropriate – no measure of participation

Some of the learning pointsso far• Methodological contribution - evaluation of complex, group
based interventions
• Recruitment challenges – how to reach those in most need?
• Service readiness – existing implementation has largely involved use of the programme within existing secondary care services; no infrastructure for preventive services
• Training and supervision requirements for best delivery

Trying the Lifestyle Matters intervention with other user groups
People with early stage dementia in Sheffield
‘Journeying through Dementia’ programme content Recruitment methods Sample size for an RCT Outcome measures – tolerance and suitability Length and modes of delivery
Older people with diagnosed mild to moderate depressionin Wales
Recruitment strategies Explore research methods and study design Outcome measures – tolerance and suitability Develop and modify selected topics from intervention

Two preparatory studies in dementia to produce a draft manual
Mountain GA and Craig C (2012) what should be in a self management programme for people with early stage dementia?Aging and Mental Health, 2012, 16(5)

Thank [email protected]
Top Related