







Languages
Pages
Legal


Fracture prevention services An economic evaluation

DH INFORMATION READER BOX
Policy EstatesHR/Workforce CommissioningManagement IM&TPlanning/ FinanceClinical SocialCare/PartnershipWorking
Document purpose BestPracticeGuidance
Gateway reference 13081
Title FracturePreventionServices:aneconomicevaluation
Author DH/SC,LG&CPdirectorate/OlderPeopleandDementia
Publication date 25November2009
Target audience PCTCEs,CareTrustCEs,DirectorsofPH,DirectorsofAdultSSs,DirectorsofFinance,AlliedHealthProfessionals
Circulation list
Description Thiseconomicevaluationmodelsthecostsandbenefitsfromestablishingafractureliaisonservice,toreducetheriskofsecondaryfractures.
Cross reference N/A
Superseded documents N/A
Action required N/A
Timing N/A
Contact details GillAylingOlderPeopleandDementiaDepartmentofHealthRoom8E28QuarryHouseQuarryHillLeedsLS27UE01132546068
For recipient use
©Crowncopyright2009
FirstpublishedNovember2009
ProducedbyCOIfortheDepartmentofHealth
Thetextofthisdocumentmaybereproducedwithoutformalpermissionorchargeforpersonalorin-houseuse.
www.dh.gov.uk/publications

Fracture prevention services An economic evaluation

1
Thiseconomicevaluationassessesthecostsandbenefitsofservicestoreducefracturesamongolderpeople.Localcommunitiescanusethistodeveloptheirownproposals.
Thereisstrongevidenceabouttheimpactandcostbenefitargumentsforfracturepreventioninterventions,basedonsystematicimplementationofnationalguidanceonsecondarypreventionofosteoporoticfracturesandotherinterventionsforatargetedat-riskpopulation.
Thefollowingisasummaryofthemainfindingsofaneconomicmodelfortheimpactofafractureliaisonservice,asdescribedintheguideFalls and fractures: effective interventions in health and social care1.
Inthismodel,overa5yearperiod£290,708issavedinNHSacuteandcommunityservicesandlocalauthoritysocialcarecosts,againstanadditional£234,181revenuecosts(fallingbothinyear1andcoveringdrugtherapyforfiveyearsspentbytheNHSonthispatientcohort).Thisisforanannualpatientcohortof797hip,humerus,spineandforearmfractures,anticipatedfroma320,000population.
Atanationallevel,thisequatestoapproximately£8.5millionsavingover5years.
1
1 Fallsandfractures:effectiveinterventionsinhealthandsocialcare,DepartmentofHealth,2009.
Summary

2
FallsareamajorcauseofdisabilityandmortalityintheUK.Thirtypercentofthoseaged65oroverwholiveinthecommunityfalleachyear,increasingto45percentinthoseaged80orabove1.Themaincauseoffallsisunsteadinessduringmovement.Inaddition,somearecausedbyblackouts(syncope)associatedwithcardiacorcirculationproblems.Bothbecomemorecommonwithage,duetoincreasingprevalenceoffrailtyandotherlongtermconditions.
Recurrentfallsareassociatedwithincreasedmortality,increasedratesofhospitalisation,curtailmentofdailyactivitiesandhigherratesofinstitutionalisation.Thisiscompoundedbythepsychologicalconsequences,suchaslossofconfidence,increasedfearoffallingandlowerqualityoflife2.Halfoffallerswillhaveafurtherfallwithinthenext12months3.Therateoffallsamongpeopleininstitutionsisalmostthreetimesthatofolderpeoplelivinginthecommunity,4withinjuryratesalsoconsiderablyhigher.
Bonedensityandstrengthalsofallwithage,particularlyinthosewithotherlongtermconditionssuchasdiabetes.Thus,thechancethatafallwillresultinafracturewillincrease.Fractureswhichoccurafteralowimpactinjury,suchasafallfromstandingheight,arecalledfragilityfractures.Halfofolderwomenwillexperienceoneintheirlifetime.Themorefrailtheindividual,themorelikelyafracture.Forexample,10-20percentofinstitutionalfallsresultinahipfracture.
2 CummingRG,SalkeldG,ThomasM,SzonyiG.Prospectivestudyoftheimpactoffearoffallinginactivitiesofdailyliving,SF-36scoresandnursinghomeadmission.J Gerontology2000;55:299-305.
3 CloseJ,EllisM,HooperR,GlucksmanE,JacksonS,SwiftC.Preventionoffallsintheelderlytrial(PROFET):arandomisedcontrolledtrial.Lancet1999;353:93-97.
4 TinettiME,SpeechleyM,GinterSF.Riskfactorsforfallsamongelderlypersonslivingwithinthecommunity.NEngJMed1988;319:1701-07.
1. Falls and fractures: who is affected?

3
Thepopulationisgrowingolder.InEngland,thenumberofpeopleagedover65isduetorisebyathirdby2025.Inthesameperiodthenumberofpeopleover80willdoubleandthenumberover100willincreasefourfold.Thiswelcomeincreaseinlifeexpectancyishoweverassociatedwithanincreaseinyearsspentwithsomedisablingillness.Asignificantriseinfallsandassociatedfracturesisthereforelikelyunlessspecificpreventativeinterventions,outlinedbelow,becomewidespread.
Thenumbersarelarge.ForaPCTandlocalauthoritywithapopulationof320,000,therewillbearound45,000peopleagedover65in2009.Ofthese1:
●● 15,500willfalleachyear,6,700twiceormore
●● mostwillnotseekhelp
●● 2,200willattendA&Eoraminorinjuryunit(MIU)
●● asimilarnumberwillcalltheambulanceservice
●● 1,250wiIlhaveafracture,with360oftheselikelytobehipfractures.
Hipfracturesremainthemostseriousconsequenceofafall.Thereisasignificantincreaseinmortality,with30%mortalityat12months.Moreover,approximatelyhalfofthosepeoplewhowerepreviouslyindependentbecomepartlydependentfollowingahipfracture,whileone-thirdbecometotallydependent.
Hipfracturesaccountformorethan20percentoforthopaedicbedoccupancyintheUK,andinwomenover45hipfracturesaccountforahigherproportionofhospitalbedoccupancythanmanycommondisorders.
2. What is the size and cost of the challenge of fractures?
4
Osteoporosisisachronicdiseasethatweakensbonestrengthandaffectsoneinthreewomenandonein12menagedover50,particularlypost-menopausalwomen.Theincidenceinbothsexesrisesrapidlyasthepopulationages.Itsonsetisasymptomaticanditisoftenonlyrecognisedafteranolderpersonfallsandsustainsafracture.Almosthalfofallwomenandoneinsixmenexperienceanosteoporoticfracturebeforedeath.
Severalstudieshaveconsideredfuturefractureriskassociatedwithdifferentkindsoffractures,andidentifiedthatapriorfractureatanysiteisassociatedwithadoublingoffuturefracturerisk.Post-menopausalwomenareathighriskoffracturesbecausetheyareatparticularriskofosteoporosis.
InaPCTpopulationof320,000,therearelikelytobe:
●● 55,000post-menopausalwomen
●● 17,400post-menopausalwomenwithosteoporosis
●● 6,900post-menopausalwomenwithapreviousfractureofanykind
●● 1,000post-menopausalwomenwithanewfractureeachyear.
Thelasttwogroupsaboveconstitutejust16percentofthelocalpopulation.Butitisamongthis16%thathalfofthehipfracturesoccur.Targetingthesegroupsinprimarycareandthroughfractureliaisoncase-findingservicesinhospitalprovidesreadyaccesstothoseatgreatestriskofhipfractures.
3. Why is identification of osteoporosis important?

5
Mostlocalcommunitieslackanysystematiclocalprogramme–suchasafractureliaisonservicecoveringfallerswhofracturepresentingtourgentcareoraprimarycare-basedcase-findingservice–toidentifyandtreatosteoporosisinhigh-riskgroups,particularlypost-menopausalwomen.
Withoutsuchprogrammesorservices,compliancewithNationalInstituteforClinicalEvidence(NICE)guidelinesTA1615andCG216onsecondarypreventionofosteoporoticfragilityfracturesislow.ThishasbeenhighlightedmostrecentlybytheRoyalCollegeofPhysicians(RCP)2009audit7offallsandbonehealthservices.ThisconfirmedthatacrossmuchoftheNHSinEnglandNICEguidanceisnotbeingwidelyemployedand“systems to ensure initiation of secondary prevention medical treatments for osteoporotic fragility fractures are not in place”.
Asaresult,theopportunitytotargetkeygroupsatmostriskofhipfractureandinitiateandoverseeosteoporosistreatmentsthatsignificantlyreducefractureriskisbeingmissed.IntheRCPnationalclinicalauditof2007,only19percentofover5,000patientspresentingtohospitalwithanon-hipfragilityfracturewereontheappropriatebonemedicationthreemonthslater.Thisisamajoropportunitylostasover40%ofpeoplewhosustainahipfracturehavehadapreviousnon-hipfragilityfracture.
5 Technicalappraisal(TA)161Osteoporosis – secondary prevention including strontium ranelateNICE2008http://guidance.nice.org.uk
6 Clinicalguideline21Clinical practice guideline for the assessment and prevention of falls in older peopleNICE2004http://guidance.nice.org.uk
7 National audit of the organisation of services for falls and bone health of older peopleRoyalCollegeofPhysicians2009http://www.rcplondon.ac.uk
4. What is the problem?

6
Theestablishmentoffractureliaisonservice,basedwithacuteservices,isforpatientsagedover50whoareadmittedtohospitalorwhoattendoutpatientclinicsorA&Edepartmentsduetoalowimpact(fragility)fracture,gainedfromafall,sliportrip.Fora320,000populationtheservicewouldassessabout1250olderpeoplewithfragilityfractureseachyear,whowillhaveaclinicalassessmentbyaspecialistFractureliaisonservice(orOsteoporosis)nurseandsomeofwhomwillundergoDXA8bonedensitymeasurementsatthespineandhip(inaccordancewithNICEguidanceTA161).Osteoporosistreatmentistypicallyrecommendedinabout75%ofcases.
Theroleofthespecialistnurseisto:
●● investigate,usingbonescansandlocalprotocols,andstartdrugandothertreatments,accordingtoNICEguidanceforwomenandlocalagreementsformen,toreducetheriskofafuturebreakifsomeonehasosteoporosis
●● linkdirectlywithfallsservices
●● monitorandmaintainmedicationadherence
●● Supportthemonitoringandmaintenanceofmedicationadherenceincollaborationwithprimarycare.
Themaincostsareforthenurse,aconsultantsessionforclinicalsupportandsupervisionandsomedirectpatientcare,someclericalsupport,revenuecostsforthescanningandpharmacycostsofosteoporosistreatment,usuallycomprisedofagenericbisphosphonateincombinationwithcalciumandvitaminD.
Theinputofthenurserelatesprimarilytothefirstyear’smembershipofthecohortprogramme,withminimalcontactthereafter(forexamplethroughlettercontactandoccasionaltelephonecalls).Soitfallstoprimarycaretomakethenecessaryarrangementstomaintainmedicationadherencelongerterm.
8 Dualenergyx-rayabsorptiometry(DXA)scansareusedtomeasurebonemineraldensity
5. The proposal for a fracture liaison service

7
Theinterventionsandtheireffecthavebeenmodelled(Tables1-5)andtheservicecostsestimated.Itisimportanttonotethatthisstudyisbasedonacohortofpeople.Inotherwords,themodellooksatthecostsofaninterventionforthetotalnumberofpeopleidentifiedwhohavefracturedinanyoneyearinalocalpopulation.Thecostssavedarethencalculatedtoreflectthesavingsthatcanbeachievedfromthatcohortoverfiveyears,withtheimplementationofthisintervention.
Localcommunitiescanusetheassumptionsinthismodeltodeveloptheirownproposals,orincludedifferentassumptionsthatmatchlocalcircumstances.Thereisanon-linemodellingtoolforafractureliaisonservicebusinesscaseathttp://fracture-liaison-model.co.uk
Keyassumptionsbuiltintothemodelareasfollows:
●● OutofatypicalPCTpopulationofaround320,000therewill,ashighlightedabove,bearound1,250fragilityfracturesofanytypeperyear. PublisheddatafromanexistingFractureLiaisonService9showsalikelybreakdownbyageandfracturetypeinTable1overaoneyearperiod.
●● Ofthisgroupofaround1,250fractureannually,thiseconomicevaluationisfocusingonthe797hip, humerus, spine and forearm fracturesperyear,asthereisrobustresearchdataontheimpactofafractureliaisonservicesinthesemostsignificantfracturetypes.Thisisintermsofimpactonqualityoflifeandhigherservicecost.Fortheremainingonethirdoffractures(pelvis,lowerlimb,handsandfeet)afractureliaisonservicecouldreasonablyexpecttohaveapositiveimpactinreducingfurtherfracturesbutthecostsorbenefitsarenotmodelledinthisstudy.
●● Allthe797hip,humerus,spineandforearmfractureswillbeassessedbythefractureliaisonnurse,andifnecessarytheconsultant,and20%ofhipfracturepatientsand80%ofhumerus,forearmandspinepatientsareanticipatedtoreceivebonescans.ThisisapragmaticinterpretationofNICETA161combinedwithpracticalexperiencefromexistingfractureliaisonservices.
9 Implementing and running a fracture liaison service,Clunie&Stephenson,JournalofOrthopaedicNursing,(2008)12:156-162
6. Summary of interventions and their effect

8
●● InlinewithNICEguidance5,manybutnotallpatientsscannedwillrequiretreatmentforosteoporosis:estimatedat100%ofthehipfractures(373),50%ofthewristfractures(159),75%ofspines(17)and75%ofhumerus(62):atotalof611outof797.
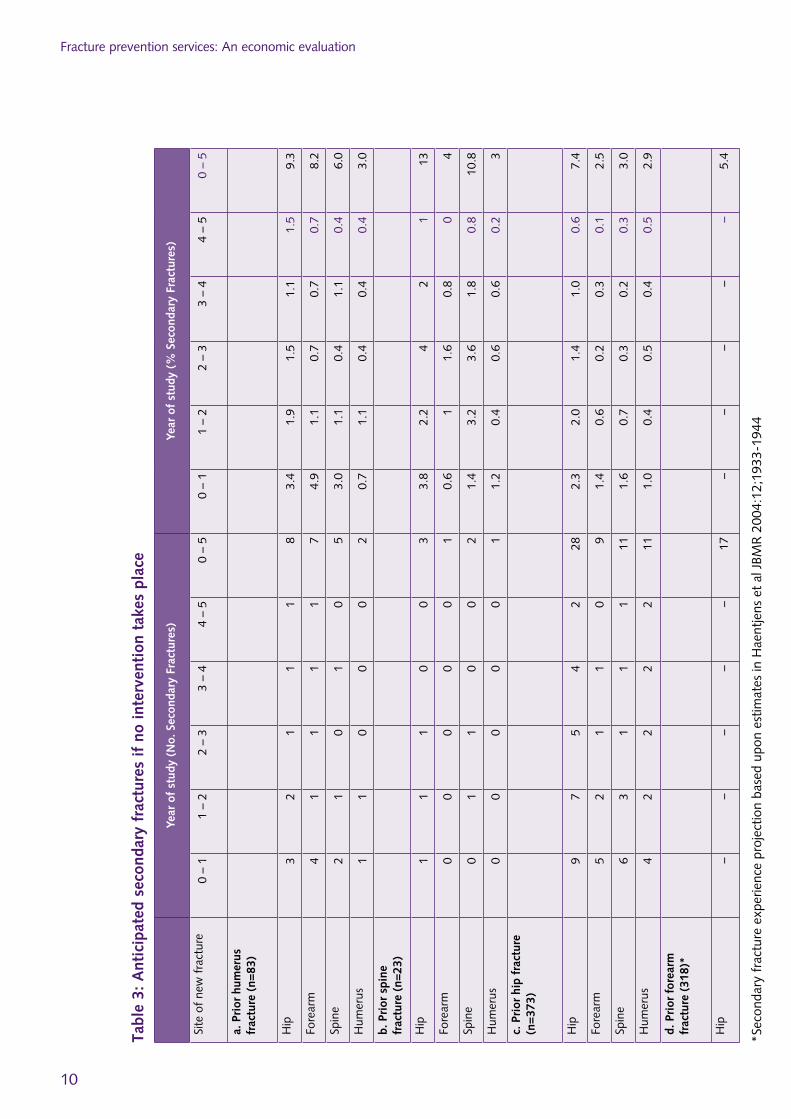
●● Usingdatafromaretrospectivestudy–fromJohnell10abouttheincidenceofsecondaryfracture,bytype,over5years–thepatternofsecondaryfracturesfora320,000populationforeachannualcohortcanbeidentified(Table2).Thisisbasedontheageprofileexpectedforpatientspresentingwithfracturesattheseskeletalsites.
●● Factoredintothecalculationisa)thepercentageofeachfracturetypetobetreated,rangingfrom100%ofhipfracturestoonly50%offorearmfractures,andb)arelativeriskreductionthroughafractureliaisonserviceof40%(NICETA1615).Fromthistherefore,canbeestimatedthenumberoffracturesactuallyavertedthroughtheserviceover5years(Table3).
●● Anassumptionofonly80%medicationcompliancehasbeenincluded(Table4),givingactualfracturesavertedof18hips,5forearms,6spineand4humerusover5yearsforeachannualcohort.
Table 1: Likely age breakdown by fracture type (Data from Ipswich Fracture Liaison Service)9
Fracture Age Range (years) over 1 year period
45-59 60-69 70-79 80-89 90+ Total
Hip 12 22 90 173 77 373
Forearm 98 86 93 37 6 318
Humerus 23 21 27 10 3 83
LowerLimb 67 50 33 14 4 167
Pelvis 2 2 9 17 7 35
Spine 3 3 9 6 3 23
Other 92 60 48 18 2 219
NotSpecified 11 8 6 5 1 30
Total 306 251 313 277 102 1247
●● Researchevidence5suggeststhatafractureliaisonservicewouldproduceasimilarimpactonthefuturefractureincidenceforthe453otherfracturesites,inadditiontohip,humerus,spineandforearmfractures(forexamplepelvis,ribs,handsandanklefractures).
10Fracture risk following an osteoporotic fracture,Johnell,Kanisetal,OsteoporosisInternational,(2004)15:175-179

Summaryofinterventionsandtheireffect
9
Tabl
e 2:
Stu
dy o
f th
e in
cide
nce
of s
econ
dary
fra
ctur
es b
y ty
pe o
ver
5 ye
ars
(Joh
nell
et a
l 20
04)10
Year
of
stud
y (N
o. S
econ
dary
Fra
ctur
es)
Year
of
stud
y (%
Sec
onda
ry F
ract
ures
)
Site
of
new
fra
ctur
e0
– 1
1 –
22
– 3
3 –
44
– 5
0 –
50
– 1
1 –
22
– 3
3 –
44
– 5
0 –
5
a. P
rior
hum
erus
fra
ctur
e (n
=26
8)
Hip
95
43
425
3.4
1.9
1.5
1.1
1.5
9.3
Fore
arm
133
22
222
4.9
1.1
0.7
0.7
0.7
8.2
Spin
e8
31
31
163.
01.
10.
41.
10.
46.
0
Hum
erus
23
11
18
0.7
1.1
0.4
0.4
0.4
3.0
b. P
rior
spi
ne f
ract
ure
(n=
500)
Hip
1911
2010
565
3.8
2.2
42
113
Fore
arm
35
84
020
0.6
11.
60.
80
4
Spin
e7
1618
94
541.
43.
23.
61.
80.
810
.8
Hum
erus
62
33
115
1.2
0.4
0.6
0.6
0.2
3
c. P
rior
hip
fra
ctur
e (n
=11
50)
Hip
2723
1612
785
2.3
2.0
1.4
1.0
0.6
7.4
Fore
arm
167
23
129
1.4
0.6
0.2
0.3
0.1
2.5
Spin
e18
84
23
351.
60.
70.
30.
20.
33.
0
Hum
erus
115
65
633
1.0
0.4
0.5
0.4
0.5
2.9
d. T
otal
s (n
=19
18)
Hip
5539
4025
1617
52.
92.
02.
11.
30.
89.
1
Fore
arm
3215
129
371
1.7
0.8
0.6
0.5
0.2
3.7
Spin
e33
2723
148
105
1.7
1.4
1.2
0.7
0.4
5.5
Hum
erus
1910
109
856
1.0
0.5
0.5
0.5
0.4
2.9
Tota
ls13
991
8557
3540
77.
24.
74.
43.
01.
821
.2
Fracturepreventionservices:Aneconomicevaluation
10
Tabl
e 3:
Ant
icip
ated
sec
onda
ry f
ract
ures
if
no i
nter
vent
ion
take
s pl
ace
Year
of
stud
y (N
o. S
econ
dary
Fra
ctur
es)
Year
of
stud
y (%
Sec
onda
ry F
ract
ures
)
Site
of
new
fra
ctur
e0
–1
1–
22
–3
3–
44
–5
0–
50
–1
1–
22
–3
3–
44
–5
0–
5
a. P
rior
hum
erus
fr
actu
re (
n=83
)
Hip
32
11
18
3.4
1.9
1.5
1.1
1.5
9.3
Fore
arm
41
11
17
4.9
1.1
0.7
0.7
0.7
8.2
Spin
e2
10
10
53.
01.
10.
41.
10.
46.
0
Hum
erus
11
00
02
0.7
1.1
0.4
0.4
0.4
3.0
b. P
rior
spi
ne
frac
ture
(n=
23)
Hip
11
10
03
3.8
2.2
42
113
Fore
arm
00
00
01
0.6
11.
60.
80
4
Spin
e0
11
00
21.
43.
23.
61.
80.
810
.8
Hum
erus
00
00
01
1.2
0.4
0.6
0.6
0.2
3
c. P
rior
hip
fra
ctur
e (n
=37
3)
Hip
97
54
228
2.3
2.0
1.4
1.0
0.6
7.4
Fore
arm
52
11
09
1.4
0.6
0.2
0.3
0.1
2.5
Spin
e6
31
11
111.
60.
70.
30.
20.
33.
0
Hum
erus
42
22
211
1.0
0.4
0.5
0.4
0.5
2.9
d. P
rior
for
earm
fr
actu
re (
318)
*
Hip
––
––
–17
––
––
–5.
4
*Sec
onda
ryf
ract
ure
expe
rienc
epr
ojec
tion
base
dup
one
stim
ates
inH
aent
jens
et
alJ
BMR
200
4:12
;193
3-19
44
11
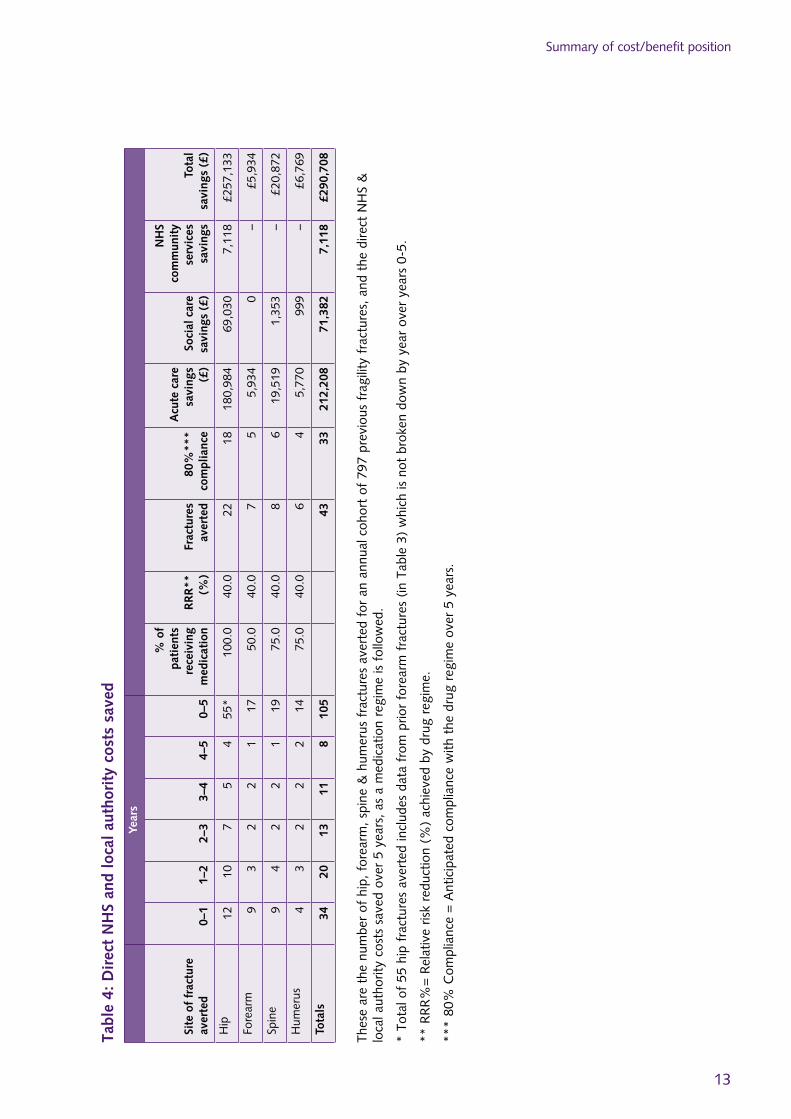
Anticipatedsavingsorcostsavertedareasfollows:
●● NHSandlocalauthoritysocialcaredirectsavingscombinedfora320,000populationhavebeencalculatedat£290,708 overthe5years,withthemajorityoffracturesavoided,andconsequentsavingsinthefirstthreeyears(Table4).Therewillinadditionbereducedsocialcarecostsforpeoplewhofundtheirowncare,whichhavenotbeenincludedinthisanalysis.
●● Keyassumptionsoncostsavings(Table4)areasfollows,basedon2009/10costs:
●– Eachhipfractureavertedwillavoidcommissionersincurring£10,170PbRtariffcosts11,reduceNHScommunityservicecostsby£1,600percommunityhospitaladmissionand£400perreferraltointermediatecare,andsave£3,879inlocalauthoritysocialcarecostsover2yearsonaverageperhipfracture(outlinedinAppendixA).
●– Fracturesofthehumerus,spineandforearmavertedwillavoidcommissionersincurringPbRtariffcostsestimatedforcombinedinandoutpatientsof£1,300,£3,246and£1,082respectively,pluslocalauthoritysocialcarereducedby£225percaseonaverageforspineandforearmfractures(outlinedinAppendixA).
●– Theassumptionsaboutcommunityservicesinputasarefollows.Forhipfractures,around20%willhavefollow-upinacommunityunit,foranestimatedstayof8daysatamarginalcostof£200perbedday.Afurther20%willreceiveanintermediatecarepackageof20hours,ataround£20perhour.Communityservicesavingsforhumerus,spineandforearmfracturesareestimatedtobesmallandhavenotbeenincluded.
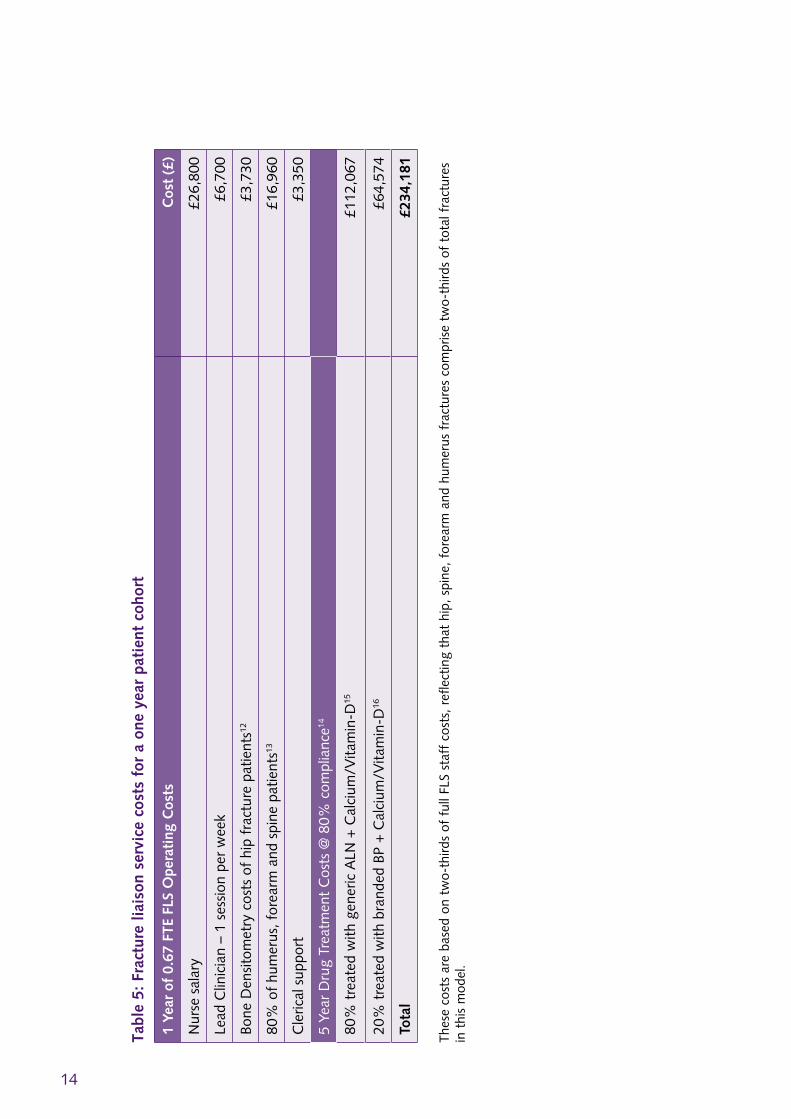
●● Thecostsacrossprimaryandsecondarycareofrunningafractureliaisonserviceforeachyear’scohortofhip,humerus,spineandforearmfractures(comprisingtwothirdsofallfragilityfractures)is£234,181outlinedinTable5.Thisconsistsof:
●– Staffcosts:twothirdsofthetotalfractureliaisonservicestaffcostsinyear1(withstafftimefortheyear1patientcohortcoveredbyotheryears’cohortcostsfromyear2onwards).Thisreflectsthecostsassociatedwith
11Basedon2009/10PaymentbyResultstariffcostsHA11-14,andincludingaMarketForcesFactorof1.082
7. Summary of cost/benefit position

Fracturepreventionservices:Aneconomicevaluation
12
hip, humerus, spine and forearm fractures, which comprise two-thirds of toal fractures in this model.Onthisbasis,staffcostsofrunningaFractureLiaisonServiceforthesefracturetypesfora320,000populationfor1yearare£36,850
●– DXA:bonescanninginyear1isafurther£20,690,basedonamarginalcostperscanof£50.BasedontheageprofileandapragmaticapplicationofNICETA161around20%ofhipfracturepatientswillneedaDXA,withahigherproportion(estimatedat80%)forforearm,spineandhumeruspatients.
●– Drugcosts:Thetotaltreatmentcostdistributedover5yearsiscalculatedinthismodelat£176,641takingintoaccount12%mortality,80%complianceandtheavailabilityoverthenextfewyearsofgenericrisedronate(from2010),ibandronate(2011)andzoledronate(2012),basedonaforecastreductionof50%overalloverfouryearsinthecostofthesedrugs.
●● InadditiontosavingsandcapacityreleasedinNHSacuteandcommunityandlocalauthoritysocialcare,therewillalsobeaverysignificantqualityoflifegainforolderpeoplewhodonotincurasecondaryfracture.ThishasnotbeenreviewedindetailinthiseconomicevaluationbutisdocumentedintheDHpublication:Falls and fractures: effective interventions in health and social care(2009).
●● Thereforeinthismodel,overa5yearperiod£290,708willbesavedinNHSacuteandcommunityservicesandlocalauthoritysocialcarecosts,againstanadditional£234,181revenuecostsinyear1andcoveringdrugtherapyforfiveyearsspentbytheNHSonthispatientcohort.Thisisforanannualpatientcohortof797hip,shoulder,spineandforearmfractures.AsensitivityanalysisofthebasecaseestimateisprovidedinAppendixB.
13
Summaryofcost/benefitposition
Tabl
e 4:
Dir
ect
NH
S an
d lo
cal
auth
orit
y co
sts
save
d
Year
s
Site
of
frac
ture
av
erte
d0–
11–
22–
33–
44–
50–
5
% o
f pa
tien
ts
rece
ivin
g m
edic
atio
nR
RR
**
(%)
Frac
ture
s av
erte
d80
%**
* co
mpl
ianc
e
Acu
te c
are
savi
ngs
(£)
Soci
al c
are
savi
ngs
(£)
NH
S co
mm
unit
y se
rvic
es
savi
ngs
Tota
l sa
ving
s (£
)
Hip
1210
75
455
*10
0.0
40.0
2218
180,
984
69,0
307,
118
£257
,133
Fore
arm
93
22
117
50.0
40.0
75
5,93
40
–£
5,93
4
Spin
e9
42
21
1975
.040
.08
619
,519
1,35
3–
£20
,872
Hum
erus
43
22
214
75.0
40.0
64
5,77
099
9–
£6,
769
Tota
ls34
2013
118
105
4333
212,
208
71,3
827,
118
£290
,708
Thes
ear
eth
enu
mbe
rof
hip
,for
earm
,spi
ne&
hum
erus
fra
ctur
esa
vert
edf
ora
nan
nual
coh
ort
of7
97p
revi
ous
frag
ility
fra
ctur
es,a
ndt
hed
irect
NH
S&
lo
cala
utho
rity
cost
ssa
ved
over
5y
ears
,as
am
edic
atio
nre
gim
eis
fol
low
ed.
*To
talo
f55
hip
fra
ctur
esa
vert
edin
clud
esd
ata
from
prio
rfo
rear
mf
ract
ures
(in
Tab
le3
)w
hich
isn
otb
roke
ndo
wn
byy
ear
over
yea
rs0
-5.
**R
RR
%=
Rel
ativ
eris
kre
duct
ion
(%)
achi
eved
by
drug
reg
ime.
***
80%
Com
plia
nce
=A
ntic
ipat
edc
ompl
ianc
ew
itht
hed
rug
regi
me
over
5y
ears
.
14
Tabl
e 5:
Fra
ctur
e lia
ison
ser
vice
cos
ts f
or a
one
yea
r pa
tien
t co
hort
1 Ye
ar o
f 0.
67 F
TE F
LS O
pera
ting
Cos
tsC
ost
(£)
Nur
ses
alar
y£2
6,80
0
Lead
Clin
icia
n–
1se
ssio
npe
rw
eek
£6,7
00
Bone
Den
sito
met
ryc
osts
of
hip
frac
ture
pat
ient
s12£3
,730
80%
of
hum
erus
,for
earm
and
spi
nep
atie
nts13
£16,
960
Cle
rical
sup
port
£3,3
50
5Ye
arD
rug
Trea
tmen
tC
osts
@8
0%c
ompl
ianc
e14
80%
tre
ated
with
gen
eric
ALN
+C
alci
um/V
itam
in-D
15£1
12,0
67
20%
tre
ated
with
bra
nded
BP
+C
alci
um/V
itam
in-D
16£6
4,57
4
Tota
l£2
34,1
81
Thes
eco
sts
are
base
don
tw
o-th
irds
off
ullF
LSs
taff
cos
ts,r
efle
ctin
gth
ath
ip,s
pine
,for
earm
and
hum
erus
fra
ctur
esc
ompr
ise
two-
third
sof
tot
alf
ract
ures
in
thi
sm
odel
.12 13
14 15 16 12
Bon
ede
nsito
met
ry@
£50
per
sca
n13
Bon
ede
nsito
met
ry@
£50
per
sca
n14
Bas
edo
ntr
eatin
g10
0%o
fhi
p,5
0%o
ffo
rear
m,7
5%o
fsp
ine
and
75%
of
hum
erus
fra
ctur
epa
tient
s.A
ssum
es1
2%m
orta
lity.
The
dru
gsp
end
assu
mes
av
aila
bilit
yov
ert
hen
ext
few
yea
rso
fge
neric
ris
edro
nate
(fr
om2
010)
,iba
ndro
nate
(20
11)
and
zole
dron
ate
(201
2),b
ased
on
afo
reca
str
educ
tion
of
50%
ove
rall
over
fou
rye
ars
int
hec
ost
oft
hese
dru
gs.
15D
rug
tarif
fpr
ice
Oct
ober
200
9fo
rge
neric
ale
ndro
nate
=£
1.16
for
28
day
supp
ly=
£15
.08
per
year
.Hig
hst
reng
thC
a/V
it-D
cos
ts£
50p
ery
ear.
C
ombi
ned
trea
tmen
tth
eref
ore
cost
s£6
5.08
per
yea
r.16
Com
bina
tion
trea
tmen
tof
ab
rand
edb
isph
osph
onat
eor
Str
ontiu
mR
anel
ate
plus
hig
hst
reng
thC
a/V
it-D
cos
ts£
300
per
year
15
InadditiontothecostsavingsfortheNHSinreducingtheincidenceofhipfracture,thereisalsothepositiveimpactfromreducedhipfracturesonlocalauthority-fundedsocialcareservices.Thesecostsareanintegralpartofthecost-benefitcaseforFLS.
(Thefollowingareillustrativeestimatesonly,andlocalcostsandservicepatternsareknowntovaryconsiderably,notablybasedontheextentofhomecarereablementserviceslocally)
●● Foreach10hipfracturesaverted,theworkingassumptionisthattherewillbealocalauthoritycostsavingof:
●– 0.9carehomeplacements….
Thisisbasedon10%rateofpost-hipfracturedirecttransferfromhospitaltocarehome17andwithinthisgroupa60%rateoflocalauthorityfundedplacements,comparedtoself-funders18.Thedurationofthisplacementcouldvaryfromafewmonthstoseveralyears.Aworkingassumptionisthateachcarehomeplacementisfor2yearsat£600perweek,thoughcostanddurationofaveragestayvariesconsiderablyacrossregionsandbetweenlocalities.
Thus,totallocalauthoritycarehomecosts=£37,440over2yearsforevery10hipfractures,or an average of £3,744 per hip fracture.
●– plusthreehomecarepackages
Thisisbasedon6outof10hipfracturesdischargedfromhospitalbacktotheirownhomerequiringahomecarepackage;andofthese1in2areeligibleforlocalauthorityfunding.Intensityofsupportwillvaryaccordingtoneed–suchasfrailty,needfordoublehandedpackages,andhomeenvironment–andtheextenttowhichreablementservicesarecommissioned.
Aworkingassumptionisthatforeachgroupof10hipfractures3outof10wouldincurcostsofacarepackagecostedasfollows:3x(1hoursperdayonweekdaysfor6weeksat£15perhour19,or£450)x3hipfractures.
17NationalHipFractureDatabase2009andHospitalEpisodeStatistics2007/8,DH.18Older People in the United Kingdom,AgeConcern,200819DepartmentofHealthestimate
Appendix A: Cost benefits for local authority social care from reducing fractures

Fracturepreventionservices:Aneconomicevaluation
16
Thistotals£1,350(forevery10hipfractures),or £135 per hip fracture.
Thecombinedvalueofboththecarehomeandthecarepackagesavingelementis£3,744+£135=£3,879per hip fracture
●– Themortalityrateforhipfracturesis30%at12months,so3in10ofavertedhipfractureswouldnotincuranysocialcarecosts.
●● Foreveryanticipatedreductionin2 vertebraoranklefractures(at1in2eligibilityforLAfundingwithintheclientgroup)asimilarlocalauthoritysavinginhomecareisanticipated:of(1hoursperdayonweekdaysfor6weeksat£15perhour,or£450)x50%or£225 per vertebra/ankle fracture
Aworkingassumptionisthatwristfracturesocialcaresupportcanbemetatminimalcost,throughlowcastaidsandadaptationsforexample.
17
ASensitivityAnalysiscanbedefinedasinvestigationintohowprojectedperformancevariesalongwithchangesinthekeyassumptionsonwhichtheprojectionsarebased.ThefollowingSensitivityAnalysisprovidescommissionersofserviceswithanindicationofthepotentialrangeofcostsandsavingsthatmightbeachievedinrealworldpractice.Thebasecaseestimatepresentedinthebodyofthedocumentabovehasbeeninformedbyapragmaticsynthesisofallrelevantresearchevidenceandsoprovidesthemostlikelyindicationofthecost-effectivenessofimplementingaFractureLiaisonService.
Thebasecasemakesthefollowingassumptions:
1. Fracture incidence:Intheabsenceofintervention,thenumberofsecondaryfracturesbysiteis56hip,17forearm,19spineand14humerus.
2. Drug efficacy:TheRelativeRiskReduction(RRR)forsecondarypreventionoffractureis40%forallsecondaryfracturesafterincidentfracturesatallsites.ThisestimateisbaseduponNICETechnologyAppraisalestimates.
3. Drug compliance:SeveralFractureLiaisonServiceshavepresenteddrugcompliancedataaspostersatnationalcongresseswhichsuggest80%compliancewithosteoporosismedicationscanbeachieved20,21,22,23.Accordingly,drugcomplianceissetat80%.
4. Treatment rates:BasedonNICETechnologyAppraisals,theproportionofpatientstreatedbyfracturesitewouldbe100%ofhips,75%ofhumerus,75%ofspinesand50%offorearms.
5. Drug spend:ThecostofgenericalendronateissetaccordingtotheOctober2009NHSDrugTariffpriceof£1.16for28dayssupply(i.e.£15.08peryear).Thecostofacombinedcalciumandvitamin-Dpreparationissetat£50peryear.Therefore,theannualcostofgenericalendronateco-prescribedwithacalciumandvitamin-Dsupplementissetat£65.08peryear.Thecostforanon-alendronatebrandedosteoporosismedicationco-prescribedwitha
20OsteoporosisInt2004;15(S2):S56:P141HarknessMetal21OsteoporosisInt2003;14(S4):S53:P55FraserMetal22OsteoporosisInt2006;17(S3):425:P115LockwoodSetal23OsteoporosisInt2003;14(S4):S12:OC27BartonJetal
Appendix B: Sensitivity Analysis of Base Case Estimate
Fracturepreventionservices:Aneconomicevaluation
18
calciumandvitamin-Dsupplementissetat£300peryear.Thecostfor5yearstreatmentinlinewithNICETechnologyAppraisalsfor80%ofpatientswithgenericalendronateandcalciumandvitamin-Dis£112,067.Thecostfor5yearstreatmentfortheremaining20%ofpatientstreatedwithacurrentlybrandeddrugandcalciumandvitamin-Dis£64,574.Thedrugspendassumes80%compliance,12%mortalityandtheavailabilityoverthenextfewyearsofgenericrisedronate(from2010),ibandronate(2011)andzoledronate(2012),basedonaforecastreductionof50%overalloverfouryearsinthecostofthesedrugs.
6. FLS staff costs:Thesereflecttheproportion(twothirds)ofallfracturesconsideredinthiscost/benefitstudy.FractureLiaisonNursesalarysetat£26,800peryear,Lead-Clinicianat1sessionperweeksetat£6,700peryearandclericalsupportsetat£3,350peryear.
7. Bone density scanning (DXA):Bonescanninginyear1isafurther£20,690,basedonamarginalcostperscanof£50.BasedontheageprofileandapragmaticapplicationofNICETA161around20%ofhipfracturepatientswillneedaDEXAscan,withahigherproportion(estimatedat80%)forforearm,spineandhumeruspatients.
Eachoftheabovesourcesofcostandsaving,whereappropriate,willbevariedbyafixedpercentageaboveandbelowthebasecaseestimate.
1. Fracture incidence
Theincidenceofsecondaryfractureswasvariedby±20%(thebasecaseestimatebysitewas56hips,17forearms,19spinesand14humerus).
Ifsecondaryfractureincidencewas20%lowerthanthebasecase,thenumberoffracturesbysiteoverthe5yearperiodwouldbe44hip,14forearm,15spineand11humerus.Thesavingswouldbe£232,566.
Ifsecondaryfractureincidencewas20%higherthanthebasecase,thenumberoffracturesbysiteoverthe5yearperiodwouldbe67hip,21forearm,23spineand17humerus.Thesavingswouldbe£348,850.
Assumingthattheoperationalcostsremainedasestimatedinthebasecase(i.e.234,181),the20%lowerestimatetranslatestotheFLScosting£1,615tooperate.The20%higherestimatetranslatestotheFLSsaving£114,669.
AppendixB:SensitivityAnalysisofBaseCaseEstimate
19
2. Drug efficacy
TheRelativeRiskReduction(RRR)achievedbydrugtreatmentwasmodelledat35%and45%(versus40%inthebasecase).
IfRRRwas35%,thenumberoffracturesavertedbysitewouldbe16hips,5forearms,5spinesand4humerusThesavingwouldbe£254,370.
IfRRRwas45%,thenumberoffracturesavertedbysitewouldbe20hips,6forearms,7spinesand5humerusThesavingwouldbe£327,047.
Assumingthattheoperationalcostsremainedasestimatedinthebasecase(i.e.234,181),the35%RRRestimatetranslatestotheFLSsaving£20,189tooperate.The45%RRRestimatetranslatestotheFLSsaving£92,866.
3. Drug compliance
Drugcompliancewasmodelledat60%and100%.
Ifcompliancewas60%,thenumberoffracturesavertedbysitewouldbe13hips,4forearms,5spinesand3humerusThesavingwouldbe£218,031.Assumingthedrugspendwouldbereducedonaccountofreducedcompliance(i.e.patientswouldnotcollect40%ofprescriptions),theoperationalcostswouldbe£190,021.Inthisscenario,theoverallsavingwouldbe£28,000.
Ifcompliancewas100%,thenumberoffracturesavertedbysitewouldbe22hips,7forearms,8spinesand6humerusThesavingwouldbe£363,385.Assumingthedrugspendwouldbeincreasedonaccountofincreasedcompliance(i.e.patientswouldcollect100%ofprescriptions),theoperationalcostswouldbe£278,341.Inthisscenario,theoverallsavingwouldbe£85,044.
4. Treatment rates
OnaccountofthetreatmentratesbeingalignedtoNICETechnologyAppraisalguidance,thisinputtothemodelwasnotsubjecttovariation.
5. Drug spend
Fourscenarioshavebeenmodelledrelatingtovariationsindrugspendoverthe5yearperiod.
a) 25% Reduction in total drug spend on alendronate treated patients:Thisscenariowouldresultinthedrugspendonpatientstreatedwithalendronate
Fracturepreventionservices:Aneconomicevaluation
20
andcalciumandvitamin-Dreducefrom£112,067to£84,050.TotalFLScostswouldreducefrom£234,181to£206,164.
b) 75% Reduction in spend on currently branded drugs:Thisscenariowouldresultinthedrugspendonpatientstreatedwithcurrentlybrandeddrugsandcalciumandvitamin-Dreducefrom£64,574to£32,287.TotalFLScostswouldreducefrom£234,181to£201,894.
c) Combination of scenarios a and b:Thisscenariowouldresultinthetotaldrugspendreducefrom£176,641to£116,337.TotalFLScostswouldreducefrom£234,181to£173,877
d) No new generic drugs available as projected:Thisscenariowouldresultinthedrugspendonpatientstreatedwithcurrentlybrandeddrugsandcalciumandvitamin-Dincreasefrom£64,574to£129,149.TotalFLScostswouldincreasefrom£234,181to£298,756.
Assumingnoimpactuponthesavingsestimatedinthebasecase,themosteconomicallyfavourablescenarioabove(c)wouldresultinanoverallsavingof£116,831over5years.Theleasteconomicallyfavourablescenario(d)wouldresultinFLScosting£8,048over5years.
6. and 7. FLS and bone densitometry operating costs
TheFLSandbonedensitometry(DEXA)scanningcostswerevariedby±20%assumingdrugcostsremainedasinthebasecase.Thisvariationresultsinarangeofoverall5yearoperatingcosts,includingdrugspend,from£222,673to£245,689.Assumingthenumbersoffracturesavertedandassociatedcostsremainedthesameasforthebasecase,theoverallsavingsdeliveredbyFLSwouldbeintherange£45,019to£68,035.
Summary
ThemajorityofscenariosexploredintheSensitivityAnalysissuggestthatimplementationofFractureLiaisonServiceswillbecostsaving.CombiningseveralvariationsininputvaluestotheeconomicmodelprovidesanillustrationofabroaderrangeofthepotentialeconomicimpactofFLS:
Assume 20% lower secondary fracture rate + 35% Relative Risk Reduction + 60% compliance:Thenumberoffracturesavertedbysitewouldbe9hip,3forearm,3spineand2humerus.Theassociatedcostsavingwouldbe£152,622.

AppendixB:SensitivityAnalysisofBaseCaseEstimate
21
TotalFLSoperationalcostsanddrugspendover5yearswouldbe£190,021.Inthisscenario,operatingtheFLS would cost£37,399.
Assume 20% higher secondary fracture rate + 45% Relative Risk Reduction + 100% compliance:Thenumberoffracturesavertedbysitewouldbe30hip,9forearm,10spineand7humerus.Theassociatedcostsavingwouldbe£490,570.TotalFLSoperationalcostsanddrugspendover5yearswouldbe£278,341.Inthisscenario,operatingtheFLS would save£212,229.
TheDrugTariffpriceofgenericalendronatewillcontinuetodeclineandsignificantreductionsincurrentlybrandeddrugspendwilloccuronaccountofnewgenericentriesfrom2010to2012.Accordingly,theleasteconomicallyfavourablescenariodepictedaboveislikelytobecomecost-neutraltomarginallycostsaving,thebasecasescenariosignificantlycostsavingandthemostfavourablescenariosubstantiallycostsaving.

22
1 Fallsandfractures:effectiveinterventionsinhealthandsocialcare,DepartmentofHealth,2009.
2 CummingRG,SalkeldG,ThomasM,SzonyiG.Prospectivestudyoftheimpactoffearoffallinginactivitiesofdailyliving,SF-36scoresandnursinghomeadmission.J Gerontology2000;55:299-305.
3 CloseJ,EllisM,HooperR,GlucksmanE,JacksonS,SwiftC.Preventionoffallsintheelderlytrial(PROFET):arandomisedcontrolledtrial.Lancet1999;353:93-97.
4 TinettiME,SpeechleyM,GinterSF.Riskfactorsforfallsamongelderlypersonslivingwithinthecommunity.NEngJMed1988;319:1701-07.
5 Technicalappraisal(TA)161Osteoporosis – secondary prevention including strontium ranelateNICE2008http://guidance.nice.org.uk
6 Clinicalguideline21Clinical practice guideline for the assessment and prevention of falls in older peopleNICE2004http://guidance.nice.org.uk
7 National audit of the organisation of services for falls and bone health of older peopleRoyalCollegeofPhysicians2009http://www.rcplondon.ac.uk
8 Dualenergyx-rayabsorptiometry(DXA)scansareusedtomeasurebonemineraldensity.
9 Implementing and running a fracture liaison service,Clunie&Stephenson,JournalofOrthopaedicNursing,(2008)12:156-162.
10Fracture risk following an osteoporotic fracture,Johnell,Kanisetal,OsteoporosisInternational,(2004)15:175-179.
11Basedon2009/10PaymentbyResultstariffcostsHA11-14,andincludingaMarketForcesFactorof1.082.
12Bonedensitometry@£50perscan.
13Bonedensitometry@£50perscan.
14Basedontreating100%ofhip,50%offorearm,75%ofspineand75%ofhumerusfracturepatients.Assumes12%mortality.Thedrugspendassumesavailabilityoverthenextfewyearsofgenericrisedronate(from2010),ibandronate(2011)andzoledronate(2012),basedonaforecastreductionof50%overalloverfouryearsinthecostofthesedrugs.
15DrugtariffpriceOctober2009forgenericalendronate=£1.16for28daysupply=£15.08peryear.HighstrengthCa/Vit-Dcosts£50peryear.Combinedtreatmentthereforecosts£65.08peryear.
16CombinationtreatmentofabrandedbisphosphonateorStrontiumRanelateplushighstrengthCa/Vit-Dcosts£300peryear.
17NationalHipFractureDatabase2009andHospitalEpisodeStatistics2007/8,DH.
18Older People in the United Kingdom,AgeConcern,2008.
19DepartmentofHealthestimate.
20OsteoporosisInt2004;15(S2):S56:P141HarknessMetal.
21OsteoporosisInt2003;14(S4):S53:P55FraserMetal.
22OsteoporosisInt2006;17(S3):425:P115LockwoodSetal.
23OsteoporosisInt2003;14(S4):S12:OC27BartonJetal.
End notes

©Crowncopyright2009
297173October09
ProducedbyCOIfortheDepartmentofHealth
Top Related