





Languages
Pages
Legal


Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
FRACTURE HEALINGMALUNIONNONUNION

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
STAGES IN FRACTURE HEALING

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
• Hematoma formation– Torn blood vessels
hemorrhage– A mass of clotted
blood (hematoma) forms at the fracture site
– Site becomes swollen, painful, and inflamed
Hematoma

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
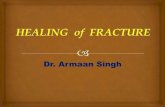
• Fibrocartilaginous callus forms
• Granulation tissue (soft callus) forms a few days after the fracture
• Capillaries grow into the tissue and phagocytic cells begin cleaning debris Figure 6.14.2
2 Fibrocartilaginous callus formation
External callus
New blood vessels
Spongy bone trabeculae
Internal callus (fibrous tissue and cartilage)

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
• The fibrocartilaginous callus forms when:– Osteoblasts and fibroblasts migrate to the
fracture and begin reconstructing the bone– Fibroblasts secrete collagen fibers that connect
broken bone ends– Osteoblasts begin forming spongy bone– Osteoblasts furthest from capillaries secrete an
externally bulging cartilaginous matrix that later calcifies

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
• Bony callus formation– New bone trabeculae
appear in the fibrocartilaginous callus
– Fibrocartilaginous callus converts into a bony (hard) callus
– Bone callus begins 3-4 weeks after injury, and continues until firm union is formed 2-3 months later
Figure 6.14.3
3 Bony callus formation
Bony callus of spongy bone

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
• Bone remodeling– Excess material on
the bone shaft exterior and in the medullary canal is removed
– Compact bone is laid down to reconstruct shaft walls
Figure 6.14.4
4 Bone remodeling
Healing fracture

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
PATHOLOGY
• REPAIR BEGINS WITH INFLAMMATION
• WHICH RESULTS IN CHEMOTAXIS AND INFLAMMATORY CELLS LIKE POLYMORPHS,LYMPHOCYTES AND MACROPHAGES MIGRATE TO THE FRACTURE SITE
• WHICH STIMULATE POLYPEPTIDE GROWTH FACTORS (TGF,PDGF)

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
• POLYPEPTIDE GROWTH FACTORS ACTS ON TARGET CELLS AND FACILITATES DNA SYNTHESIS AND CAUSES
• CELL DIVISION AND PROLIFERATION
• ANGIOGENESIS• COLLAGEN SYNTHESIS HEALING• STIMULATION OF STEM CELLS –
OSTEOBLAST FORMATION

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
VARIABLES THAT INFLUENCE FRACTURE HEALING
• INJURY VARIABLES
• PATIENT VARIABLES
• TISSUE VARIABLES

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
INJURY VARIABLESa) OPEN FRACTURES – soft tissue
disruption,# displacement,significant bone loss delays # healing and can also result in infection & chronic osteomyelitis
b) SEVERITY OF INJURY
c) INTRA ARTICULAR FRACTURE : healing delays due to instability and prolonged immobilisation can result in joint stiffness also

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
a) SEGMENTAL FRACTURE – disrupts intramedullary blood supply to middle fragment
b) SOFT TISSUE INTERPOSITION – compromises # healing
c) DAMAGE TO BLOOD SUPPLY – causes significant delay in # healing.
eg: femoral head,scaphoid,talus,distal tibia

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
PATIENT VARIABLES• AGE – infants,rapid rate of # healing
• NUTRITION – cell migration,proliferation and matrix synthesis needs substantial energy. Malnutrition can also result in infection,wound dehiscence,impaired healing and slow rehabilitation
• SYSTEMIC HORMONES – corticosteroids compromises # healing.
Thyroid hormone,calcitonin,insulin are good
• NICOTINE – cigarette smoking inhibit fracture healing

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
TISSUE VARIABLES
• FORM OF BONE – opposed cancellous bone unite rapidly
• BONE NECROSIS – if # is avascular-healing may be delayed.Prolonged use of corticosteroids and radiation can cause bone necrosis.
• BONE DISEASES – osteoporosis,osteomalacia,bone tumours,pagets disease,bone cyst,osteogenesis imperfecta etc can influence # healing
• INFECTION

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
TREATMENT VARIABLES
• APPOSITION OF FRACTURE FRAGMENTS – decreasing fracture gap decreases volume of repair tissue needed for # healing
• FRACTURE STABILISATION – traction, cast immobilisation,external fixation,internal fixation

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
TREATMENT THAT INTERFERES WITH HEALING
• SURGERY – blood supply disruption and infection
• INADEQUATE IMMOBILISATION
• DISTRACTION OF FRACTURE FRAGMENTS BY EF/IF/TRACTION
• REPEATED MANIPULATIONS
• EXCESSIVE EARLY MOBILISATION

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
METHODS PROMOTING # HEALING
• BONE GRAFT
• BONE TRANSFER –to replace a lost portion of long bone diaphysis,surgeons perform corticotomy through normal bone creating a mobile bone segment and then uses an external fixation device to transfer the segment across the defect.
As segment moves a column of bone forms behind it

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
• ELECTRICAL FIELDS – stimulate cell proliferation,synthetic function and promrte bone formation
• ULTRASOUND – low intensity pulse ultrasound helps in # healing

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
NON UNION
- failure of fracture to unite by bony continuity.
DEFINITION:
Non union is said to be established when a minimum of nine months has elasped since the injury and the fracture shows no radiologically visible progressive signs of healing continuously for three months

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
DELAYED UNION
• Where healing has not occurred at the expected time of union for the type and site of fracture

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
CLASSIFICATION
• PALEY,S CLASSIFICATION-
Type A – less than 1 cm boneloss
Type B – more than 1cm bone loss
• MULLER AND WEBER CLASSIFICATION
Hypervascular nonunion
Avascular non union

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
Hypervascular non union –fracture ends are viable and show biological
reaction,hence stable internal fixation is enough no bone grafting required

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
AVASCULAR NON UNION – the fracture ends are not viable due to poor blood supply. Needs rigid internal fixation with bone grafting after decortication of non viable ends
• Torse wedge non union – intermediate fragment has healed at one end and not at the other,seen in segmental #
• Comminuted non union – in comminuted #
• Defect/gap nonunion-in compound#,OM
• Atrophic non union-ends are thin and sclerotic with excessive scar tissue in b/w

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
Causes for nonunion
• Compound #
• Infection
• Segmental #
• Distraction of # fragments
• Soft tissue interposition
• Ill advised open reduction
• Insecure and inadequate fixation
• General factors

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
Clinical features
• h/o multiple injuries, open #, inadequqte trt etc
• Symptoms : no pain/minimal pain,presence of deformity/loss of function
• Signs : painless abnormal mobility,no crepitus,shortening,scars and sinuses,deformity,wasting of limb muscles etc

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
Investigations
• Radiograph :
gap b/w # fragments
fragments are rounded/sclerotic
amount of callus will be more (hypervascular) or less (avascular)

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
Management
• Principles :
• Non union is an absolute indication for surgery it requires open reduction rigid internal fixn and bone grafting
• No role for conservative mngmnt
• Other methods- electrical stimulation,interlocking nails and ilizarov,s technique

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
Bone grafting - types• Cancellous bone graft : defect less than 2.5 cm.
It is better tolerated and rapidly revascularised
• Cortical bone graft : it has a stabilising property and can be used for non union of shafts of any long bones.
-single onlay: wen placed on one surface
-dual onlay : wen placed on both the sides
-sliding graft : wen a piece is slided from above to the fracture site

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
• Phemister bone graft : here, graft is placed subperiosteally.simple,blood supply is not disturbed.
• It is placed posteriorly and is found to be useful in tibia

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
Electrical stimulation• Weak electric current of 20 mA delivered to
# site by a cathode converts fibrous tissue to fibrocartilage wich gets ossified later by enchondral ossification.
• 3 types : invasive – if cathode is placed inside the # site
semi-invasive –when it is placed s/c
non invasive – wen in corporated into the plaster cast externally.
Union occurs in 85% of cases

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
Ilizarov,s technique
• Best way to treat infected non union
• Allows simultaneous correction of all deformities and bone loss

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
Mal union
• Definition : when # fragment heals in an abnormal position,it is called malunion

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
• Causes cosmetically unsightly deformity
• Alteration in posture and balance in lower limb fractures
• It may cause shortening
• May interfer with joint function
• Altered wt bearing mechanism may lead to premature osteoarthritis of the hip and knee joints.

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
Causes
• Trt methods : eg closed reduction
• Improper immobilisation techniques
• Trt by quacks
• Multiple and multisystem injuries

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
Classification
• Length malunion
• Rotatory malunion
• Angulatory malunion

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
Types
• Significant mal union : interfers with function
• Insignificant mal union : does not interfere with function

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
Clinical features
• Deformity
• Loss of function
• Shortening
• Muscle wasting

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
Treatment
• Operative trt : if it affects function
• Corrective osteotomy
• Optimum time to carry out surgery : 6-12 months after the fracture

Copyright © 2004 Pearson Education, Inc., publishing as Benjamin Cummings
THANK YOU
Top Related