







Languages
Pages
Legal


Marci Anderson, VAOIG
Mark Myers, VAOIG
May 10, 20171
Federal Government Processes
and Standards
VA Structure and Best Practices
• Procurement in VA is not centralized.
• Contracts and task orders are awarded by the
Office of Acquisition, Logistics, and Construction
or by the various VA administrations, the largest
being the Veterans Health Administration.
May 10, 20172
May 10, 20173
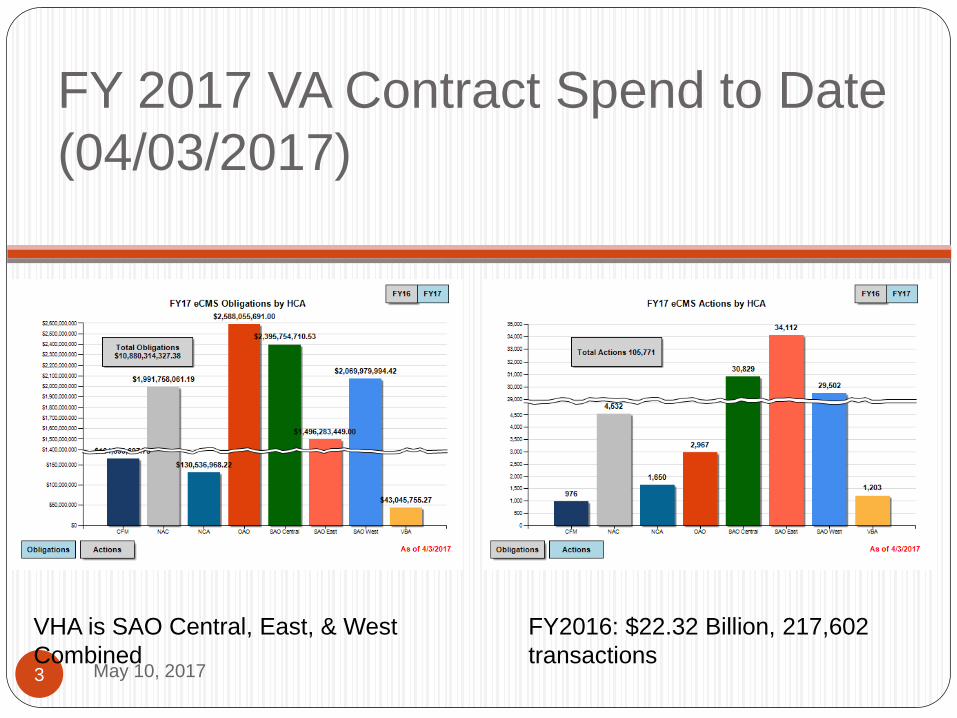
FY 2017 VA Contract Spend to Date
(04/03/2017)
FY2016: $22.32 Billion, 217,602
transactions
VHA is SAO Central, East, & West
Combined
OFFICE OF ACQUISITION AND
LOGISTICS
May 10, 20174
Funded through VA Supply Fund which is a
revolving fund
Office of Acquisitions provides overall policy
for VA’s acquisition operations
Major units:
Acquisition Resource Service (ARS)
Acquisition Operations Service (AOS)
Denver Acquisition and Logistics Center (DALC)
National Acquisition Center (NAC)
Technical Acquisition Center (TAC) (IT
procurements)
May 10, 20175
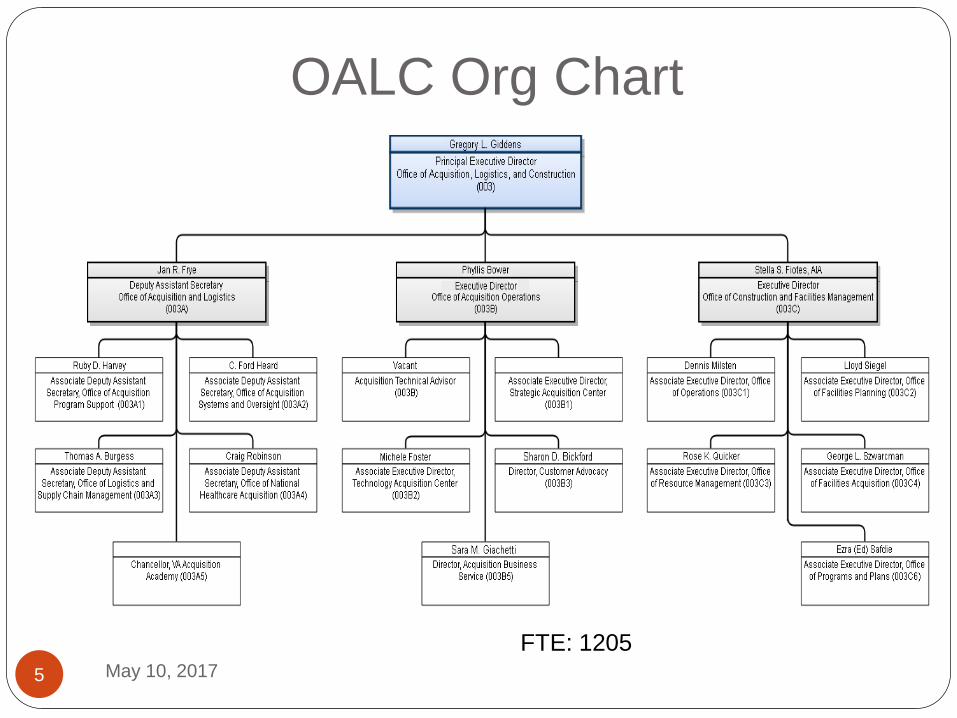
OALC Org Chart
FTE: 1205
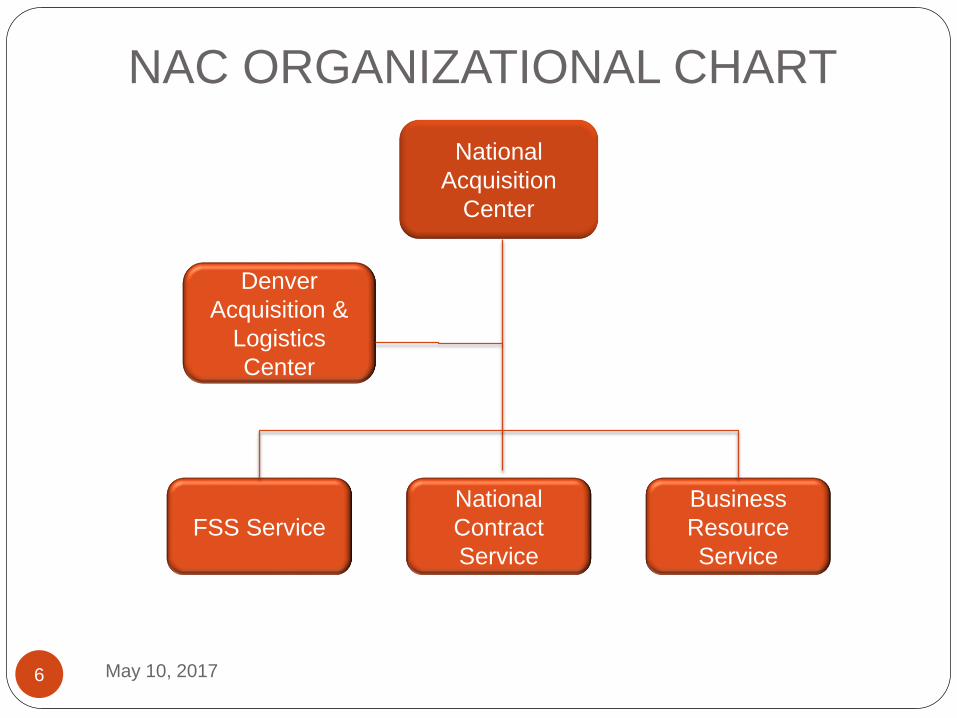
NAC ORGANIZATIONAL CHART
6
National
Acquisition
Center
FSS Service
Denver
Acquisition &
Logistics
Center
Business
Resource
Service
National
Contract
Service
May 10, 2017

FSS Service
7
Vacant
Director FSS Service
708-786-4957
James Booth (A)
Deborah Zuckswerth(B)
Chief, Med/Surgical
James: 708-786-5223
Deborah: 708-786-5128
Bob Satterfield
Chief, Services
708-786-4955
Diana Lawal
Chief, Pharm/Dental
708-786-4949
Christine Szrom
Chief, Program Mgmt & Resource Support
708-786-4936
May 10, 2017

National Contract Service
8
Steven Thomas
Director National Contract Service
Frank Zacchigna
Chief, High Tech Medical Equipment
Division
Ronald Jenkins
Chief, Medical/Surgical
Program
Fran DeRosa
Chief, Pharmaceutical
Division
May 10, 2017

PHARMACY BENEFITS
MANAGEMENT SERVICES (PBM)
May 10, 20179
Oversees the formulary for the entire VA system
Manages pharmaceuticals and pharmaceutical-related policies Drug safety and efficacy evaluations
Pharmacologic management algorithms Criteria for drug use
Evidence-based practices promote, optimize, and assist VA providers with the safe and appropriate use of pharmaceuticals
Allow formulary decisions that can result in substantial cost savings
Standardize generic agents as well as specific drugs and drug classes for National Contracts
Established an outcomes research section to undertake quality-improvement and safety initiatives that ultimately monitor and determine the clinical impact of formulary decisions
Responsible for processing non-FAMP data to produce FCPs Authority to make covered drug determinations

PBM CENTRAL OFFICE
May 10, 201710
Michael A. Valentino -Chief Consultant for Pharmacy Benefits Management Services, Department of Veterans Affairs Central Office
Responsible for planning and directing Drug benefit design
Formulary management and pharmaceutical contracting
Automated prescription fulfillment
Professional pharmacy practice
Emergency pharmacy services
Drug therapy policy development
Virginia S. Torrise, Pharm. D. - Deputy Chief Consultant - PBM Professional Practice and Clinical Informatics VA’s formulary committees
Pharmacy residency training
Adverse drug event reporting
Medication safety reviews
Recruitment and retention initiatives
Emergency pharmacy preparedness and pharmacy informatics development
PBM HINES
May 10, 201711
Joseph J. Canzolino, R. Ph. – Deputy Chief Consultant - Formulary Management Pharmacy Benefits Management Services VAMedSafe/Outcomes Research Emergency Pharmacy Service.
Jennifer Zacher, Pharm. D. - Assistant Chief Consultant - PBM/EPS Management of VA National Formulary initiatives Advisor to the National Acquisitions Center on Pharmacy
Issues Emergency Preparedness
Ted Karnezis, RPh, Pharm. D. - Public Law Database Manager Management of Public Law Prices
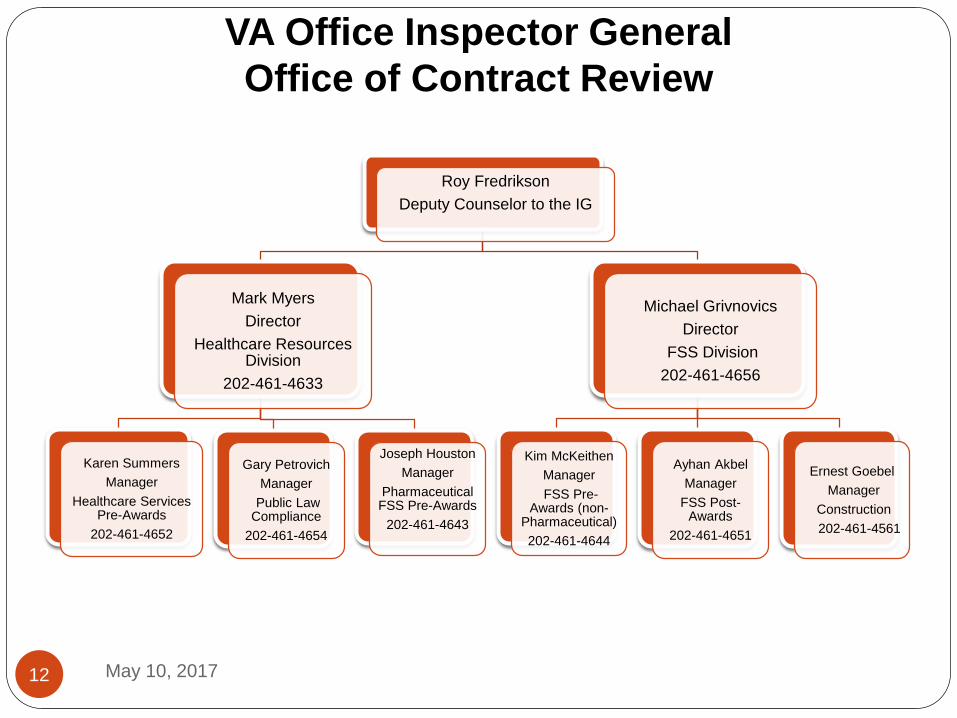
VA Office Inspector General
Office of Contract Review
12
Roy Fredrikson
Deputy Counselor to the IG
Mark Myers
Director
Healthcare Resources Division
202-461-4633
Karen Summers
Manager
Healthcare Services Pre-Awards
202-461-4652
Gary Petrovich
Manager
Public Law Compliance
202-461-4654
Joseph Houston
Manager
Pharmaceutical FSS Pre-Awards
202-461-4643
Michael Grivnovics
Director
FSS Division
202-461-4656
Kim McKeithen
Manager
FSS Pre-Awards (non-
Pharmaceutical)
202-461-4644
Ayhan Akbel
Manager
FSS Post-Awards
202-461-4651
Ernest Goebel
Manager
Construction
202-461-4561
May 10, 2017
OFFICE OF CONTRACT
REVIEW
May 10, 201713
Performs Pre- and Post-Award reviews of FSS
contracts awarded and administered at the
NAC
Pre-Award reviews are requested by and are
advisory to the Contracting Officer. All
pharmaceutical offers with estimated contract
values over $5 million will be subject to a Pre-
Award review.
Primary objective is to determine whether
CSP disclosures are accurate, complete and
current and whether the offered price is
reasonable.

OFFICE OF CONTRACT
REVIEW
May 10, 201714
Post-Award Reviews - compare disclosure
data with sales transaction data to
determine:
compliance with PL 102-585 section 603
billing at correct prices
compliance with FSS contract clauses including:
price adjustment clause, price reduction clause,
payment of IFF

COORDINATION OF NAC, PBM,
AND OIG
May 10, 201715
Preaward Reviews
NAC and OIG review CSPs and pricing schedules
OIG obtains current FCPs from PBM (if covered drugs are offered)
OIG conducts review and issues report to CO
CO negotiates contract with OIG advice as needed.
OIG coordinates with NAC Contracting Staff regarding any potential issues with offeror
Postaward Reviews
Can be initiated at the request of the CO, by the OIG, or in response to a voluntary disclosure
NAC and OIG will discuss unique issues
OIG report to CO with recommendations
OIG may obtain open market purchase data through PBM if a covered drug is not offered timely, or is removed from the schedule prematurely.

COORDINATION OF NAC, PBM,
AND OIG
May 10, 201716
Public Law Updates
PBM sends letter in October to contractors with
covered drugs
PBM reviews and calculates FCPs sends to
contractor for concurrence
PBM sends final FCPs to contractor and contracting
officer
If the contractor has concerns or disagrees with
final FCP, need to timely discuss and resolve with
PBM
Contractor submits modification request and CO
performs analysis (Max Cap and TC relationship)
Mod is processed for January 1 implementation

Best Practices
May 10, 201717
Understand what is required for submission for a
new contract, contract extension, FCP,
modification, price reduction and establish
policies, procedures, and processes that will:
Allow you to extract accurate, complete, and current
information needed to submit an offer or
modification, and calculate the FCP for each line
item.
Allow you to track information needed to ensure
contract compliance such as place of manufacture
and compliance with FDA laws and regulations.

Best Practices
May 10, 201718
Submit offers timely to ensure award at the time
you expect and before an existing contract
expires.
3 months or less in advance of your desired award
date will not be sufficient.
Allow at least one year for optimal results.
If you don’t get a response from the NAC, contact
them to determine the status.
Same goes for requests for modifications
Document progress, especially for addition for
covered drugs
Best Practices
May 10, 201719
Perform internal reviews periodically. If noncompliance issues are found, determine impact and if any, submit a voluntary disclosure to your CO with a copy to the OIG.
For offers that require a preaward review, follow-up with CO once the review is complete. No more than 60 days should pass between the completion of the review and the award of the contract/modification.
If the CO is not responsive, elevate concerns to the Chief and don’t hesitate to elevate to the Director level if necessary.
Disclose and negotiate. Don’t selectively disclose based on criteria of your choosing.
Single v. Dual Pricing
Ensure that you have the information needed to make
an informed decision whether to offer single or dual
pricing on the FSS for covered drugs.
May 10, 201720

Single v. Dual Pricing
May 10, 201721
“Covered drug” is a single-source or innovator multiple-source drug, marketed under a New Drug Application or a Biological License Agreement
Manufacturers must make VHCA “covered drugs” available for sale on an FSS contract at statutorily-capped pricing known as the Federal Ceiling Price (FCP) to be eligible for Medicaid and Medicare Part B reimbursement, and purchase by the “Big Four” Federal agencies: Big Four: VA, DoD, Public Health Service (PHS)
(including Indian Health Service) (IHS)), and Coast Guard
Other Government Agencies (OGAs) and other eligible FSS purchasers are not entitled to FCP, so VA allows manufacturers to decide whether to extend FCPs to the OGAs using the dual pricing option
Single v. Dual Pricing
May 10, 201722
Single Pricers Provide FCP (or lower) pricing to all FSS-eligible
purchasers as the FSS “contract price”
Maintain single price list
Dual Pricers Establish two prices:
Big Four price: capped at FCP
OGA: negotiated price that serves as the FSS “contract price”
Maintain two price lists
Single Pricing Pros and Cons
May 10, 201723
Pros: Simpler administratively: Only one price point to negotiate CSP disclosures will
be limited only to prices that are equal to or lower than
the FCP for offered products
Only one price list to maintain
Only one set of prices to monitor for compliance with the
Price Reductions Clause
Cons: Limitation on price increases Single pricing rules depress or inhibit increase in FCP in
dual calculation years

Dual Pricing Pros and Cons
May 10, 201724
Pros: Permits price increases and may limit other liabilities OGA price is usually higher than FCP
OGA price allows for FCP to increase more quickly over time relative to single pricers (OGA price is used as the FSS Max Cap in the FCP calculation)
Lower rebate liability under the TRICARE retail rebate program
Cons: More complicated administratively: Two price points to negotiate CSP disclosures will be more
involved to address FCP-based Big 4 price and the negotiated OGA price
Two price lists to maintain
Two sets of prices to monitor for compliance with the Price Reductions Clause

Dual Pricing – Considerations
May 10, 201725
Differential between MFC, Tracking Customer
Price and calculated FCP
Inflationary market could mean heavy
additional discounts which would favor dual
pricing
Deflationary market could mean there is a
potential for the Tracking Customer price to
become the permanent FSS price
Applies to all 42-2A products on contract.
Overall benefit should be evaluated.
Making/Changing the Election
May 10, 201726
The single/dual election is made at the time of contract award
The election applies to all covered drugs on contract
Vendor Response Document, Page 12, includes instructions, considerations and election form.
Established single pricers can change to dual pricing at any time during the contract period (DML dated 11/1/2013) If a company changes its election (from single to dual) during
the life of the contract, new CSP forms must be submitted to negotiate an FSS price
Trade Agreements Act
May 10, 201727
All VA FSS and other national contracts (other than small business set-asides) include the Trade Agreements Act clause.
The contractor has the responsibility to identify the country of origin, not the CO or the purchaser.
For pharmaceuticals, maintain documents showing the country of origin for the API.
For non-manufacturers, ensure that your subcontracts to obtain the products includes a provision that requiring your suppliers (both direct and indirect) to certify that the products provided are Trade Agreements Act compliant.
Blanket non-availability determination for 42-2A items only.
Top Related