






Languages
Pages
Legal


2025
Familial Lipoprotein Disorders in Patients WithPremature Coronary Artery Disease
Jacques J. Genest Jr., MD; Sarah S. Martin-Munley, PhD; Judith R. McNamara, MT;Jose M. Ordovas, PhD; Jennifer Jenner, BsC; Richard H. Myers, PhD; Steven R. Silberman, PhD;
Peter W.F. Wilson, MD; Deeb N. Salem, MD; and Ernst J. Schaefer, MD
Background. Genetic lipoprotein disorders have been associated with premature coronary artery disease(CAD).
Methods and Results. The prevalence of such disorders was determined in 102 kindreds (n=603 subjects)in whom the proband had significant CAD documented by angiography before the age of 60 years. Fastingplasma cholesterol, triglyceride, low density lipoprotein (LDL) cholesterol, apolipoprotein (apo) B, andlipoprotein (a) [Lp(a)] values above the 90th percentile and high density lipoprotein (HDL) cholesteroland apo A-I below the 10th percentile of age- and sex-specific norms were defined as abnormal. Anabnormality was noted in 73.5% of probands compared with 38.2% in age-matched controls (p<0.001),with a low HDL cholesterol level (hypoalphalipoproteinemia) being the most common abnormality (39.2%of cases). In these kindreds, 54% had a defined phenotypic familial lipoprotein or apolipoprotein disorder.The following frequencies were observed: Lp(a) excess, 18.6% (includes 12.7% with no other dyslipi-demias); hypertriglyceridemia with hypoalphalipoproteinemia, 14.7%; combined hyperlipidemia, 13.7%(11.7% with and 2.0%o without hypoalphalipoproteinemia); hyperapobetalipoproteinemia (elevated apo Bonly), 5%; hypoalphalipoproteinemia, 4%; hypercholesterolemia (elevated LDL only), 3%; hypertriglycer-idemia, 1%; decreased apo A-I only, 1%. Overall, 54% of the probands had a familial dyslipidemia;unclassifiable lipid disorders (spouse also affected) were found in 3%. No identifiable familial dyslipi-demia was noted in 43% of kindreds of those; nearly half (45%) had a sporadic lipid disorder.Parent-offspring and proband-spouse correlations for these biochemical variables revealed that lipopro-tein and apolipoprotein levels are in part genetically determined, with Lp(a) showing the highest degreeof parent-offspring correlation.
Conclusions. Our data indicate that more than half of patients with premature CAD have a familiallipoprotein disorder, with Lp(a) excess, hypertriglyceridemia with hypoalphalipoproteinemia, and com-
bined hyperlipidemia with hypoalphalipoproteinemia being the most common abnormalities. (Circulation1992;85:2025-2033)KEY WoRDs * coronary artery disease * lipids * lipoproteins * genetics
F amily history of myocardial infarction or suddendeath is a frequent finding in patients withpremature coronary artery disease (CAD) and
is considered a risk factor for the development of CAD.1Several familial lipid disorders, including familial hyper-
From the Lipid Metabolism Laboratory (J.J.G., S.S.M.-M.,J.R.M., J.M.O., J.J., E.J.S.), U.S.D.A. Human Nutrition ResearchCenter on Aging at Tufts University and Cardiology Division(D.N.S.), Department of Medicine, New England Medical CenterHospital, Boston; Department of Neurology (R.H.M.), BostonUniversity School of Medicine, Boston; Terumo Medical Corpo-ration (S.R.S.), Elkton, Md.; and the Framingham Heart Study(P.W.F.W.), Framingham, Mass.Supported by grant HL-35243 and subcontract HV-83-03 from
the National Heart, Lung, and Blood Institute, National Institutesof Health, and by contract 53-3K06-5-10 from the U.S. Departmentof Agriculture Research Service. J.J.G. was supported by a Centen-nial Fellowship of the Medical Research Council of Canada.
Presented in part at the 62nd Scientific Sessions of the Ameri-can Heart Association, New Orleans, November 1989.Address for correspondence: Ernst J. Schaefer, MD, Lipid
Metabolism Laboratory, U.S.D.A. Human Nutrition ResearchCenter on Aging, Tufts University, 711 Washington St., Boston,MA 02111.
cholesterolemia (FH),2 familial combined hyperlipid-emia (FCH),3-5 and familial hypoalphalipoproteinemia(FHA),6 have been associated with an increased risk ofpremature CAD. The role of plasma lipids and lipopro-teins in the development of CAD has been shown inlarge prospective7-8 and case-control studies.9-10 Theprotein content of low density lipoproteins (LDL) andthe main apolipoproteins of high density lipoproteins(HDL), i.e., apolipoprotein (apo) B and apo A-I,1-14 aswell as lipoprotein (a) [Lp(a)] and apo (a)15"6 have beenshown in some studies, but not all, to be better markersfor the presence of CAD than elevated LDL cholesterolor decreased HDL cholesterol levels. Elevation of LDLapo B with normal (or near-normal) lipid values (hyper-apobetalipoproteinemia) is associated with prematureCAD and has been shown to segregate in family mem-bers." Lp(a) excess also is associated with prematureCAD and is present in families of affected individuals.The modes of inheritance for many of these disorders isthought to be autosomal dominant or polygenic, withvarying degrees of penetrance and/or expression inadulthood. With the exception of FH,2 familial defectiveapo B-100,17 familial dysbetalipoproteinemia (type III
by guest on October 5, 2017
http://circ.ahajournals.org/D
ownloaded from

2026 Circulation Vol 85, No 6 June 1992
hyperlipoproteinemia),18 and rare disorders of the apoAI-CIII-AIV gene cluster,'9'20 the molecular defects ofmost familial lipoprotein disorders associated with pre-mature CAD are unknown. In FH, multiple disorders ofthe LDL receptor gene have been identified, and thedisease is transmitted in a Mendelian dominantfashion.21,22The prevalence of lipid disorders is increased in
patients with premature CAD. However, the type andprevalence of familial dyslipidemias have not been wellcharacterized since the description of FCH in CADpatients,3-5 which was based on measurements of totalcholesterol and triglyceride concentrations and the li-poprotein electrophoresis pattern.The purpose of the present study was to determine
the type and prevalence of dyslipidemias in patientswith premature coronary disease. The genetic contribu-tion of lipoprotein and apolipoprotein levels was as-sessed by comparing parental with offspring plasmalevels of various lipid parameters.
MethodsPatients
From July 1986 through December 1987, 259 consec-utive patients referred to our hospital for coronaryangiography were included in the study if they wereCaucasian and less than 60 years of age at the time ofangiography and had significant CAD, defined as >50%stenosis of one or more epicardial coronary artery.Patients with <50% stenosis were excluded (n=25), aswere patients older than 60 years and those receivinglipid-lowering medications (n = 1). All angiograms werereviewed by three cardiologists, including one of theauthors (J.J.G.). The other two cardiologists wereblinded to the study and scored the angiograms fordiagnostic purposes. The majority of the patients se-lected (97%) had severe two- or three-vessel disease.There were 214 men (83%) and 45 women (17%) in thegroup. The referral base of the New England MedicalCenter Hospital includes the greater Boston area andeastern Massachusetts. Information on use of lipid-lowering drugs, f3-adrenergic blocking agents, and di-uretics and history of hypertension, diabetes mellitus,and cigarette smoking was obtained.
All patients were seen in the hospital by one of theauthors (J.J.G.). Information on the presence of coro-nary disease was gathered on first-degree relatives,parents, and grandparents by history. The country oforigin of relatives also was determined. We attemptedto study all kindreds consisting of patients who had aminimum of two offspring and a genetically unrelatedspouse available for blood sampling. A letter confirmingthe appointment for family studies was sent, and tele-phone confirmation was made to ensure compliance. Of259 patients with premature CAD, 36 were unmarriedor had insufficient children for this study. Of the re-maining 223 families, 50 (22%) did not wish to take partin the study; 44 (20%) volunteered but were unable toparticipate; 21 (9%) were lost to follow-up; and 108families (49%) were sampled. In six families, notenough first-degree relatives were available for analysis,and these kindreds were excluded from the phenotypeanalysis. There were 87 men (85.3%) and 15 women
relatives (3.75 per proband, including 16 parents), 23second-degree relatives, and 96 genetically unrelatedspouses; 88.6% of offspring identified were sampled. Atotal of 603 subjects were studied. None of the womenprobands were on hormonal therapy at the time ofsampling. Data on the use of hormones were notobtained in first-degree relatives of the probands. In-formed consent was obtained from all participatingfamily members by using a protocol approved by theHuman Investigation Review Committee of the NewEngland Medical Center Hospital and Tufts UniversitySchool of Medicine. Parental consent was obtained forthose under 18 years of age.
ControlsTo classify values of probands and first-degree rela-
tives, we used the Lipid Research Clinics (LRC) database's 90th percentile age- and sex-specific values fortotal cholesterol, triglycerides, and LDL cholesterol andthe 10th percentile values for HDL cholesterol as cutoffpoints.23 No age or sex norms for apo A-I, apo B, andLp(a) are available from the LRC study; apo A-I and apoB were therefore measured on a sample of 3,541 partic-ipants in cycle 3 of the Framingham Offspring Study. Ageand sex distribution were used for the cutoff points(<10th percentile for apo A-I and >90th percentile forapo B) in the present study. Lp(a) was determined on1,240 men and 1,309 women, free of cardiovasculardisease, from the Framingham Offspring cohort. The90th percentile was determined to be 39 mg/dl in menand 39.5 mg/dl in women at a mean age of 50 years. Ascomparison groups for the probands, we used 901 healthymen aged 40-60 years (mean+SD age, 49+6 years) and1,125 healthy women aged 40-60 years (mean±SD age,49±6 years) from the Framingham Offspring Study whohad no evidence of cardiovascular disease. Triglyceridesand Lp(a) were log10-transformed to approximate thenormal distribution.
Lipid, Lipoprotein, and Apolipoprotein MeasurementsAll patients and relatives were sampled in the free-
living state at least 1 month after their diagnosticcatheterization and at least 6 weeks after major surgeryor myocardial infarction. The sampling took place in theMetabolic Research Unit of the U.S. Department ofAgriculture Human Nutrition Research Center on Ag-ing at Tufts University. Subjects were sampled after a12-14-hour overnight fast (morning medication, includ-ing insulin, was allowed); subjects were asked to refrainfrom alcohol consumption for 24 hours before thesampling. Blood sampling was carried out after subjectshad been in the sitting position for at least 10 minutesand after blood pressure measurements were per-formed. Thirty milliliters of blood was drawn from anantecubital vein in EDTA-containing tubes to a finalconcentration of 1.2 mg/ml and put on ice. Plasma wasisolated by centrifugation (2,500 rpm for 20 minutes at4°C), and multiple aliquots were stored immediately at-80°C for later apo A-I, apo B, and Lp(a) determina-tions. Blood cells were resuspended in 0.9% NaCI forsubsequent DNA isolation.
Plasma total cholesterol and triglyceride concentra-tions were determined enzymatically. HDL cholesterol
(14.7%) identified as probands, with 382 first-degree also was measured enzymatically after dextran-Mg`
by guest on October 5, 2017
http://circ.ahajournals.org/D
ownloaded from

Genest et al Genetic Lipoprotein Disorders and CAD 2027
precipitation.24'25 Our laboratory meets the perfor-mance criteria of the Centers for Disease Control-National Heart, Lung, and Blood Institute Lipid Stan-dardization program. In most subjects, LDL cholesterolwas estimated with the Friedewald formula.24-26 How-ever, in cases where the plasma triglyceride levels were>400 mg/dl, cholesterol was measured in the density> 1.006 g/ml infranate plasma after ultracentrifugation;LDL cholesterol was then calculated by subtractingHDL cholesterol from infranate cholesterol.23 Apo A-Iand apo B were determined by noncompetitive ELI-SAs.2728 These assays were standardized using aminoacid analysis of purified protein standards. Lp(a) wasmeasured using a commercially available ELISA (Ter-umo Medical Corp., Elkton, Md.), which uses twoantisera, one monoclonal antibody that does not cross-react with plasminogen, and a polyclonal antibody thatis specific for the apo (a) protein of Lp(a). The assay isstandardized with respect to the total Lp(a) particle.Results are expressed in milligrams per deciliter ofLp(a). Coefficients of variance for this assay were 2.46%for intrarun and 3.33% for interrun variations, respec-tively, and <10% for other apolipoprotein assays.
Lipoprotein AbnormalitiesTo classify lipid disorders, we defined hypertriglycer-
idemia as a plasma triglyceride level >90th percentilevalue of age- and sex-matched control subjects. Simi-larly, hypercholesterolemia was defined as a plasmalevel of LDL cholesterol >90th percentile, and hypoal-phalipoproteinemia was defined as a plasma level ofHDL cholesterol <10th percentile, based on the LRCpopulation study.23 The LRC data for lipid and lipopro-tein levels were used rather than the Framingham Studydata base because the former includes data on children.However, cutoff-point values for either sample werevery similar. We have avoided defining hyperlipopro-teinemias by types IV29; rather, we have used the termsas defined above.The criteria used to define a familial dyslipidemia are
as follows: Abnormalities found in probands alone andnot in any first-degree relatives were called "sporadic"and the family was considered "normal." In cases wherethe spouse was affected and the proband was not andsegregation was found in the children, the family waslabeled "normal" for the purposes of this study. If theproband was affected with a lipoprotein or apolipopro-tein abnormality and at least one first-degree relativehad a lipoprotein or apolipoprotein abnormality, thekindred was considered to have a familial lipoproteinabnormality. FH was defined as elevated LDL choles-terol only, regardless of the presence of xanthomas orxanthelasmas and the finding of this same abnormalityin one or more first-degree relatives. Familial hypertri-glyceridemia was defined as an elevated triglyceridelevel and the presence of the same abnormality in atleast one first-degree relative. FHA was defined as lowHDL cholesterol only and the presence of the sameabnormality in at least one first-degree relative. FamilialLp(a) excess was defined as an elevated Lp(a) level(>39 mg/dl for men, >39.5 mg/dl for women) in theproband and at least one first-degree relative. Familialhyperapo B was defined as apo B >90th percentile in
normal lipid and lipoprotein levels. Familial apo A-Ideficiency was defined as apo A-I levels < 10th percentilewith normal lipid values, including HDL cholesterol.FCH was defined as the finding of an elevated triglycer-ide level and/or an elevated LDL cholesterol level(>90th percentile) in the proband and at least onefirst-degree relative, with the stipulation that both abnor-malities had to be present in the kindred. Familialhypertriglyceridemia with hypoalphalipoproteinemia wasdefined as an elevated triglyceride level and/or a lowHDL cholesterol level (< 10th percentile) in the probandand at least one first-degree relative, with the stipulationthat both abnormalities had to be present within thekindred. We call this entity familial dyslipidemia.
Statistical AnalysisData were stored on a VAX 11/780 (Digital Equip-
ment Corp., Maynard, Mass.) on the data base RS/1(BBN Software, Cambridge, Mass.). The RPL languagewas used for all programming (BBN software); Z scores
were determined by using a built-in subroutine. Tocalculate correlation coefficients between parents andoffspring for biochemical variables, the Z score was
determined for each lipoprotein and apolipoproteinvariable to correct for age and sex differences. Pearson'smultiple regression analysis, using the SAS statisticalpackage (SAS Institute, Cary, N.C.) was used to deter-mine correlation coefficients between lipoprotein andapolipoprotein levels in proband-spouse, midparent-midoffspring, and proband (or spouse)-offspring com-binations. Because we did not observe age and sex
differences for Lp(a) levels in this study, we useduncorrected Lp(a) data for these correlation analyses.Differences in lipids, lipoproteins, and apolipoproteinswere analyzed by t tests, and differences in the fre-quency of lipid disorders were assessed by x2 analysis.Covariate analysis between cases and controls was per-formed using a general linear model (GLM) procedure.The data were adjusted for body mass index, sex, age,use of ,8-blockers, cigarette smoking, and hypertension.
ResultsThe mean age of the probands was 51±6 years (age
range, 34-59 years). When the CAD cases were com-pared with Framingham controls, prevalence rates forsmoking (within the past 2 years; 44% versus 28%,p<0.01), diabetes (11% versus 3%, p<0.001), and hy-pertension (45% versus 20%, p<0.01) were significantlyhigher in the CAD group than in the control group.Mean age in men with CAD was 51±6 years comparedwith 49±6 years in the male controls (p<0.05), andmean age in women with CAD was 51+3 years com-
pared with 49±6 years in the female controls (p=NS).Lipid, lipoprotein, and apolipoprotein levels in men
and women with CAD are shown in Table 1 and are
compared with levels of male and female controls fromthe Framingham Offspring Study, cycle 3. (3-Adrenergicantagonists (P-blockers) can alter lipid and lipoproteincholesterol levels, so we determined the effects ofp-blocker use on 236 patients from which the probandswere selected in whom }3-blocker data were available.For such comparisons, we assumed that patients receiv-ing ,-blockers did not differ significantly from those not
the proband and at least one first-degree relative, with receiving such medication. There were 94 patients not
by guest on October 5, 2017
http://circ.ahajournals.org/D
ownloaded from

2028 Circulation Vol 85, No 6 June 1992
TABLE 1. LApid, Lipoprotein, and Apolipoprotein Levels in Probands
Men Women
CAD FHS controls CAD FHS controlsLevels (mg/dl) (n=87) (n=901) (n=15) (n=1,125)Cholesterol 200±55 214±36t 241±96 215±43*Triglycerides 177+107 141±+ 104t 219±225 110±144*LDL cholesterol 139±55* 138±35 152+58 134±38HDL cholesterol 35±8 45+12t 41+7 57+15tApo B 126+37 108±33t 146±53 96+31tApo A-I 112±23 136±32t 137±28 160±39*Lp(a) 19±18 15±17t 19±19 14+14
CAD, coronary artery disease; FHS, Framingham Heart Study; LDL, low density lipoprotein; HDL, high densitylipoprotein; apo, apolipoprotein; Lp(a), lipoprotein (a).Values are given as mean±SD.*LDL cholesterol is estimated at 147±58 mg/dl in CAD patients once corrected for f-blocker use and diet effects.tp<0.005, *p<0.05.
receiving ,B-blockers and 142 who were. Total choles-terol (212±51 versus 211±60 mg/dl, p=0.893), triglyc-erides (169±90 versus 191± 120 mg/dl, p=0.345), LDLcholesterol (144±48 versus 136±45 mg/dl, p=0.197),HDL cholesterol (34±11 versus 33±9 mg/dl,p=0.378),apo B (123+±31 versus 127±39 mg/dl,p=0.408), apo A-I(111±25 versus 112+24 mg/dl, p=0.645), and Lp(a)(18±18 versus 19±23 mg/dl, p=0.718) did not differsignificantly between patients not receiving and thosereceiving ,-blockers. Analysis by ,B-blocker (proprano-lol, metoprolol, atenolol, and others) or sex did notaffect the results (data not shown).The results of a covariate analysis are presented in
Table 2. The data on lipids, lipoproteins, and apolipo-proteins were adjusted for sex, age, body mass index,smoking status, use of ,-blockers, and hypertension.This analysis revealed that triglycerides, LDL choles-terol, and apo B were no longer higher in the CADprobands after adjusting for covariates.With the criteria outlined in "Methods," the preva-
lence of lipoprotein and apolipoprotein abnormalitieswas determined in probands alone (Table 3) and withinthe familial context (Table 4). A lipoprotein or apolipo-protein abnormality was identified in 75 probands(73.5%). In 20 of these patients (19.6% of all CADindex cases), no clear familial segregation was identi-fied, and the proband was classified as having a sporadic
TABLE 2. Covariate Analysis of Lipid, Lipoprotein, andApolipoprotein Levels in Probands
CAD FHSprobands controls
Levels (mg/dl) (n=102) (n=901) pCholesterol 194± 1 214+6 0.0009Triglycerides 146±+17 145 +4 0.9598LDL cholesterol 129+5 138±1 0.0856HDL cholesterol 35±2 45±0.4 0.0001Apo B 119±5 108±1 0.1385Apo A-I 109±5 136±1 0.0001
CAD, coronary artery disease; FHS, Framingham Heart Study;LDL, low density lipoprotein; HDL, high density lipoprotein; apo,apolipoprotein.Data adjusted for age, sex, body mass index, hypertension,
smoking, and 3-blocker use.Values are given as mean±SEM.
lipid disorder (see "Methods"). Therefore, 53.9% of theCAD probands were documented as having a familiallipoprotein or apolipoprotein disorder as previouslydefined.
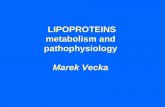
In the probands, the prevalence of lipoprotein andapolipoprotein abnormalities were hypoalphalipopro-teinemia, 39.2%; elevated apo B, 30.4%; reduced apoA-I, 28.4%; elevated triglyceride levels, 22.5%; Lp(a)excess, 18.6%; and hypercholesterolemia, 10.8% (thesegroups were not mutually exclusive). Our assay for apoB measures total plasma apo B. When family memberswere considered, the prevalence of familial lipoproteinabnormalities did not always follow the proband's phe-notype (Table 4). Isolated lipid disorders were infre-quent; combined lipoprotein disorders were frequent.The majority of probands with low HDL cholesterolalso had first-degree relatives with elevated triglycer-ides; similarly, many probands with a lipoprotein abnor-mality were part of families with combined disorders.The most common familial dyslipidemias were Lp(a)excess, seen in 19 families (18.6%), including 13(12.7%) with no other lipid abnormalities (Figure 1A);hypertriglyceridemia with low HDL cholesterol, 15 fam-ilies (14.7%) (Figure 1B); FCH (elevated triglyceridesand/or LDL cholesterol), 14 families (13.7%) with(11.7%) or without (2%) low HDL cholesterol (Figure1C); and FHA, four families (4%) (Figure 1D). FH wasseen in three families, two of whom had classic FH with
TABLE 3. Lipoprotein and Apolipoprotein Disorders* inProbands With Premature Coronary Artery Disease
Disorder No. of patients (%)Hypoalphalipoproteinemia 40 (39.2)Hyper apo Bt 31 (30.4)Decreased apo A-I 29 (28.4)Hypertriglyceridemia 23 (22.5)Lp(a) excess 19 (18.6)Hypercholesterolemia
(elevated LDL cholesterol) 11 (10.8)Normal 24 (23.5)
Apo, apolipoprotein; Lp(a), lipoprotein (a); LDL, low densitylipoprotein.
*Not mutually exclusive groups.tBased on total plasma apo B.
by guest on October 5, 2017
http://circ.ahajournals.org/D
ownloaded from

Genest et al Genetic Lipoprotein Disorders and CAD 2029
TABLE 4. Prevalence of Familial Lipid Disorders in 102 Familiesin Which the Proband Has Premature Coronary Artery Disease
Familial lipid disorder No. of families (%)Lp(a) (includes 5.9% with
dyslipidemias) 19 (18.6)Combined hyperlipidemia 14 (13.7)Hyper-apo B 5 (5.0)Hypertriglyceridemia with
hypoalphalipoproteinemia* 15* (14.7)Hypoalphalipoproteinemia 4 (4.0)Apo A-I deficiency 1 (1.0)Hypercholesterolemia* 3 (3.0)Hypertriglyceridemia 1 (1.0)Genetic dyslipidemiat 55 (53.9)Unclassified* 3 (3.0)Normal 44 (43.1)
*One patient has both familial hypercholesterolemia (LDLreceptor gene defect) and familial dyslipidemia (hypertriglyceri-demia with hypoalphalipoproteinemia).tOf the kindreds, 6.9% had two abnormalities; however, each
case was counted only once, and the overlaps are indicated.tBoth proband and spouse were dyslipidemic and children were
affected; therefore, the type of lipid disorder could not unequiv-ocally be assigned to the proband.
tendinous xanthomas. On Southern blot analysis, a10-kilobase (kb) deletion of the 5' end of the LDLreceptor was detected in one of the patients (French-Canadian mutation, H. Hobbs, Dallas, Tex., personalcommunication).2' This patient also had familial hyper-triglyceridemia combined with FHA. Another familyhad hypercholesterolemia without tendinous xantho-mas. One family had isolated familial hypertriglyceri-demia (1%).
< t$>~~~~~~L(a) Exc7ess
II 3 ~~~~~~~~~~~Lp(a)mgtdL
1 2 3 4 5 6
FAN 024
FCH
II
IIIb
T
xv TI T H
1 2 3 4 5 6 7 a 9
Levels of apo A-I and apo B further refined theanalysis; five kindreds (4.9%) had elevated apo B as thesole abnormality, and one kindred (1%) had decreasedapo A-I only. An additional three (3%) had an unclassi-fiable lipoprotein disorder. When Lp(a), apo B, and apoA-I were included in the analysis, 55 kindreds (53.9%)manifested a familial lipoprotein disorder, and 6.9% of allkindreds had more than one disorder (Table 4).There were 20 patients (19.6%) with dyslipidemia in
whom no familial segregation was observed; these caseswere defined as "sporadic" dyslipidemias. In 24 patients(23.5%), no lipid disorder was identified. Thus, of 44probands with no familial lipoprotein disorder, 20(43%) had a sporadic dyslipidemia. Ten of these indexcases were diabetic. In two, a pattern consistent withFCH was found; in two other subjects, Lp(a) excess wasidentified; in two additional subjects, a sporadic hyper-lipoproteinemia was found (both with low HDL choles-terol); and in the remaining four subjects, no lipopro-tein abnormality was identified.The lipoprotein and apolipoprotein levels in male
probands with the most common disorders are shown inTable 5 (there were too few women in each category formeaningful comparison). It is noteworthy that patientswith FHA as well as those with familial hypertriglycer-idemia with hypoalphalipoproteinemia and familialLp(a) excess had mean total cholesterol levels below200 mg/dl. Familial Lp(a) excess without other lipopro-tein abnormalities occurred in 13 kindreds. In thosefamilies, lipoprotein cholesterol levels were not signifi-cantly different from those of the control group.The genetic relations of the various lipid and apolipo-
protein parameters were assessed by calculating corre-lation coefficients for lipid, lipoprotein cholesterol, andapolipoprotein levels in proband-offspring, midparent-
II1
iii *
iv
III
FAM 060
Familial dyslipidemia
2 3 4 5
10 IV
1 2 3 4 5 6
FIGURE 1. Men are indicated by a square; women are indicated by a circle. Subjects sampled are shown in thick symbols.Deceased subjects are marked with a diagonal line. An asterisk indicates premature coronary artery disease. T, triglycerides >90thpercentile; L, low density lipoprotein cholesterol >90th percentile; H, high density lipoprotein cholesterol <1Oth percentile. Top leftpanel: Familial lipoprotein (a) [Lp(a)l excess. Values expressed in mgldl. Top right panel: Familial dyslipidemia. Bottom leftpanel: Familial combined hyperlipidemia. Bottom right panel: Familial hypoalphalipoproteinemia.
by guest on October 5, 2017
http://circ.ahajournals.org/D
ownloaded from

2030 Circulation Vol 85, No 6 June 1992
TABLE 5. Lipoprotein Levels in Probands (Men Only) With Common Dyslipidemias (mg/dl)
Totaln cholesterol Triglycerides LDL cholesterol HDL cholesterol Apo B Apo A-I Lp(a)
T+H 12 178+32* 225+128* 107+42* 29+6* 130+34t 99+20* 9+12tT+L±H 11 213±29 233+104* 135+31 32+6* 140±28* 113+17t 24+20tLp(a) 12 189±32t 168±142 117±37t 39+ 10t 105 18 121±20t 47±9*Apo B 4 222+23 226+135t 141±30 36+4 176±32* 120±12 11±15HDL 4 196+28 130+61 141+16 28+3* 127±28 90+11* 20±26Control 901 214±36 141±104 138+35 45±12 108±33 136±32 15±17
T, triglycerides >9Oth percentile; H, high density lipoprotein (HDL) cholesterol <lOth percentile; L, low density lipoprotein (LDL)>90th percentile; Lp(a), lipoprotein(a) >38 mg/dl.
pp<0.005, tp<0.05.
midoffspring, and spouse-offspring combinations andcomparing them with proband-spouse pairs. An indexof environmental influence, such as shared household or
diet, on lipid parameters can be gleaned from proband-spouse correlations. There was a significantly positivecorrelation for HDL cholesterol (r=0.127, p<O.05) andapo B (r=0.138, p<0.05) and an inverse correlation forLDL cholesterol (r=-0.158, p<O.O1) in proband-spouse comparisons. The correlation in triglycerideconcentrations between probands and spouses did notreach statistical significance (r=0.111, p>O.05). Therewas a significant correlation for total cholesterol(r=0.271, p<O.OO1), triglycerides (r=0.160, p<0.O1),very low density lipoprotein (VLDL) cholesterol(r=0.134, p<0.05), LDL cholesterol (r=0.289,p<O.OOl), HDL cholesterol (r=0.284, p<O.OO1), apo B(r=0.252, p<O.OO1), apo A-I (r=0.276, p<O.OO1), andLp(a) (r=0.614, p<O.OO1) between parents and off-spring. The correlation coefficients were somewhat lessfor proband-offspring or spouse-offspring but were stillsignificant for cholesterol, LDL cholesterol, HDL cho-lesterol, apo B, apo A-I, and Lp(a) (Table 6). Therewere no significant differences in Lp(a) levels betweenmen and women in the control groups, nor were theresignificant correlations between age and Lp(a) levels inthe control groups (men and women) or in the group ofpatients with CAD, their spouses, and their relatives.
DiscussionThe characterization of most familial lipid disorders
has been fraught with difficulties; in FCH, the pheno-typic expression of the disease may vary between sib-lings and the proband; FHA has been described fre-quently, but in many families, elevated triglycerideswere present.30 31 The expression of these lipid disordersmay not be evident until adulthood. The lack of speci-ficity in biochemical or molecular markers for eachdisorder has added to the difficulty in differentiatingpatients with various lipoprotein disorders. Plasma apo
B or VLDL apo B may be a marker for FCH, whereaselevated LDL apo B may be a marker for a normolipi-demic subset of FCH, i.e., familial hyperapobetali-poproteinemia232 Single-gene disorders leading to ex-
treme levels of lipoproteins are rare and do not accountfor much of the variability in plasma lipoprotein levelswithin a population. These disorders account for a smallfraction of lipid disorders within a group of patientswith CAD.33 Single-gene effects that lead to moderatevariation in lipoprotein parameters remain an impor-tant area of investigation.
In the present study, the most common disorders are
those in which there is combined elevation of apo
B-containing particles (VLDL, LDL, or both), oftenwith decreased HDL cholesterol. Because of the inter-relation among the various lipoproteins, classification ofeach disorder within a specific lipoprotein class (i.e.,VLDL, LDL, or HDL) or by hyperlipoproteinemia typeis impractical. The common lipoprotein disorders willbe discussed separately.
Familial HypertriglyceridemiaWith Hypoalphalipoproteinemia(Familial Dyslipidemia)There are several lines of evidence suggesting that
familial hypertriglyceridemia with hypoalphalipopro-teinemia (FTgH) is a distinct entity. The inverse rela-tion between triglycerides and HDL cholesterol haslong been known.34 The prevalence of hypertriglyceri-demia with hypoalphalipoproteinemia in the generalpopulation is higher than expected if the two variableswere independent. In previous studies of FHA, severalfamilies also had hypertriglyceridemia.3031 In the pres-ent study, FTgH was one of the most common familiallipid abnormalities in patients with premature CAD,being present in 14.7% of the probands (Table 4). It isof interest that the prevalence of FTg without hypoal-phalipoproteinemia was 1% in CAD families; the prev-
TABLE 6. Lipoprotein Correlations*
Total cholesterol Triglycerides VLDL LDL HDL Apo B Apo A-I Lp(a)t
Parents-offspring 0.271* 0.160§ 0.134§ 0.289* 0.284* 0.252: 0.276t 0.614*Proband-spouse 0.017 0.111 0.087 -0.158§ 0.127§ 0.138§ 0.077 -0.050Proband-offspring 0.2364: 0.146§ 0.109§ 0.228* 0.255* 0.148§ 0.137§ 0.4344Spouse-offspring 0.2854 0.074 0.090 0.3234: 0.174§ 0.217* 0.130§ 0.322§
*Corrected for age and sex, Z score.tNot corrected for age and sex.*p<O.005, §p<0.05.
by guest on October 5, 2017
http://circ.ahajournals.org/D
ownloaded from

Genest et al Genetic Lipoprotein Disorders and CAD 2031
alence of hypertriglyceridemia without low HDL cho-lesterol did not differ significantly between CADpatients and control subjects. This suggests that ele-vated triglyceride levels are important as a risk factoronly when associated with another lipoprotein abnor-mality (elevated LDL cholesterol or decreased HDLcholesterol). The etiology of FTgH is unknown. As inFCH, apo B levels were increased and HDL cholesterollevels were decreased (Table 5). Whether FTgH andFCH share a common metabolic etiology is uncertain;in FTg, hyperproduction of triglycerides has been doc-umented, whereas in FCH (or in familial hyperapobeta-lipoproteinemia), there is overproduction of apo B.34-36The importance of this disorder is its association with anormal total cholesterol. We suggest that this entity becalled familial dyslipidemia to distinguish it from FCH.
FCHFCH, as defined by elevated triglycerides, LDL cho-
lesterol, or both, was one of the most common dyslipi-demias found in the present study. This disorder wasseen in 13.7% of probands (2% with normal HDLcholesterol and 11.7% with decreased HDL cholesterollevels). In affected family members, increased hepaticapo B production rates have been reported.37 The apo Blevels were elevated (Table 5). A closely related disor-der, hyperapobetalipoproteinemia (elevated apo B lev-els in the presence of normal lipid levels), is probably avariant of FCH. In this study, five families (5%) hadelevated apo B without abnormal lipoprotein choles-terol levels. We did not, however, determine the prev-alence of hyperapobetalipoproteinemia as described bySniderman et a32 because our assay for apo B measurestotal plasma apo B but not LDL apo B."
FHAOnce thought to be a common lipid disorder, FHA is
most often associated with hypertriglyceridemia, includ-ing FCH. Patients with rare disorders of the apo A-I-C-III-A-IV gene cluster and those with Tangier diseaseand other unusual disorders of HDL metabolism38exhibit severely depressed HDL cholesterol levels.These cases are extremely rare. In this study, 4% of thefamilies had hypoalphalipoproteinemia, and 1% had adecreased apo A-I as the sole abnormality.
FHFH may be due to a variety of mechanisms. Although
LDL receptor defects underlie many severe hypercho-lesterolemic subjects, defective apo B-100 and disordersof hepatic overproduction of LDL particles may accountfor a substantial number of cases.39 The prevalence ofhypercholesterolemia was lower than that found byGoldstein et al.3 In one of our cases, hypertriglyceri-demia with hypoalphalipoproteinemia also was present.The prevalence of LDL receptor defects in this cohortwith CAD appears to be on the order of 3%. Othermechanisms may play a role in FH, such as defectswithin the apo B gene, which decrease binding to theLDL receptor'7 or overproduction of LDL particles.
Familial Lp(a) ExcessFamilial Lp(a) excess was seen in 18.6% of our
families. Elevated levels of Lp(a) appear to be inversely
correlated with the molecular weight of apo (a) and thenumber of kringlelike domains in the protein.40 Thepathogenic mechanisms by which Lp(a) enhances ath-erosclerosis may be related to its cholesterol estercontent or the antithrombolytic effects of the particle.40Lp(a) appears to be a highly heritable trait. Parent-offspring correlations indicate that this may be thelipoprotein disorder that has the strongest geneticdeterminant.The molecular basis for most of these disorders is
unknown. One approach in finding a genetic basis hasbeen the candidate gene approach, in which the genesfor the apolipoproteins found in abnormal amounts inthese disorders were investigated for genetic polymor-phisms.4' Thus, genetic variability within the apo B- andapo A-I-C-III-A-IV genes has been investigated byrestriction fragment-length polymorphisms (RFLP)analysis in patients with a variety of lipid disorders orvascular problems. Some RFLPs have been associatedwith altered lipid values in some but not all studies;these associations have, for the most part, not beenconsistent in various populations. In the present study,no RFLP of the apo B gene42 or the apo A-I-C-III-A-IV gene complex43 appeared to segregate with thelipoprotein disorders outlined above. A few rare disor-ders, including hypobetalipoproteinemia, familial defec-tive apo B-100,17 and defects of the apo A-I-C-III-A-IVgene complex,'1920 have been documented in the apo-lipoprotein genes; these have a profound effect onplasma lipid levels but do not contribute to any signifi-cant extent to plasma lipoprotein levels within a popu-lation because of their low frequency.44The cutoff points used in the present study, in which
we assumed that the 90th or 10th percentile of avariable constituted an abnormal level, may have led toan overestimation of familial lipoprotein disorders.There was no control for environmental influenceswithin individual families. The effect of diet was notcontrolled for, nor were other environmental variablessuch as exercise, body mass index, and cigarette smok-ing. Because most of our patients were referred fromcommunity hospitals, the sampling may be biased to-ward patients with more severe CAD. Therefore, theseresults may not be representative of the population atlarge. However, plasma lipoprotein cholesterol, apo A-Iand apo B, and Lp(a) were not significantly different inthese probands than in 321 men with premature CADon whom we reported previously.45 46Sampling patientswith cardiovascular events during the acute episode maylead to misclassification of lipid disorders. Waiting 6weeks after acute myocardial infarction is necessary tobest approximate lipoprotein cholesterol levels presentbefore the event (reviewed in Reference 47).The phenotypic assignment of individual families may
not precisely reflect accurate genotypes. Furthermore,it is likely that the disorders discussed above have apolygenic etiology, in which case the chance associationof several genetic variations will have an effect onplasma lipoprotein levels. This may explain in part thepatterns of inheritance of these disorders in which anaffected offspring may have inherited only one anomalyand thus may reveal a different lipid disorder than theproband. Phenotypic expression has been explained byincomplete penetrance, expression of the disorder inadults but not in children, or coexisting environmental
by guest on October 5, 2017
http://circ.ahajournals.org/D
ownloaded from

2032 Circulation Vol 85, No 6 June 1992
variables such as diet, exercise, hormonal status, orponderosity. One also must consider the inheritance ofseveral unlinked genetic disorders, each with an effecton plasma lipoprotein levels. Despite these caveats,familial dyslipidemias were identified in more than halfof the probands with premature CAD. Most of thesedisorders were associated with normal total cholesterolor LDL cholesterol levels.No single lipoprotein parameter will identify all pa-
tients at risk for CAD. From the data presented here, itappears that triglyceride, HDL cholesterol, apo B, andLp(a) levels are useful markers for the detection offamilial lipid disorders. LDL cholesterol elevation, al-though strongly associated with the development of CAD,is an infrequent finding in CAD probands. The highprevalence of lipid disorders in offspring and first-degreerelatives makes it mandatory to sample children of dyslip-idemic probands with premature CAD.
AcknowledgmentsThe authors wish to thank Pamella Miller, BSc, for her
computer programming skills; Lindsay A. Farrer, PhD, andDan Kiely, PhD, for their advice on statistical analysis ofgenetic traits; and Leah Zanotti, RN, and the nurses of theMetabolic Research Unit for their help in conducting thisstudy.
References1. Slack J, Evans KA: The increased risk of death from ischemic
heart disease in first degree relatives of 121 men and 96 womenwith ischemic heart disease. J Med Genet 1966;3:329
2. Goldstein JL, Hazzard WR, Schrott WR, Bierman EL, MotulskyAG, Levinski MJ, Campbell ED: Hyperlipidemia in coronary heartdisease: I. Lipid levels in 500 survivors of myocardial infarction.J Clin Invest 1973;52:1533-1543
3. Goldstein JL, Schrott HG, Hazzard WR, Bierman EL, MotulskyAG, Campbell ED, Levinski MJ: Hyperlipidemia in coronary heartdisease: II. Genetic analysis of lipid levels in 176 families anddelineation of a new inherited disorder, combined hyperlipidemia.J Clin Invest 1973;52:1544-1568
4. Nikkila EA, Aro A: Family study of serum lipids and lipoproteinsin coronary heart-disease. Lancet 1973;1:954-958
5. Rose HG, Kranz P, Weinstock M, Juliano J, Haft JI: Inheritanceof combined hyperlipoproteinemia: Evidence for a new lipoproteinphenotype. Am J Med 1973;54:148-160
6. Vergani C, Bettale G: Familial hypo-alpha-lipoproteinemia. ClinChim Acta 1981;114:45-52
7. Martin MJ, Hulley SB, Browner WS, Kuller LH, Wentworth D:Serum cholesterol, blood pressure, and mortality: Implicationsfrom a cohort of 361,662 men. Lancet 1986;2:933-936
8. Castelli WP, Garrison RJ, Wilson PWF, Abbott RD, Kalousdian S,Kannel WB: Incidence of coronary heart disease and lipoproteincholesterol levels: The Framingham Heart Study. JAMA 1986;256:2835-2838
9. Papadapoulos NM, Bedynek JL: Serum lipoprotein patterns inpatients with coronary atherosclerosis. Clin Chim Acta1973;44:153-156
10. Frick MH, Dahlen G, Berg K, Valle M, Hekali P: Serum lipids inangiographically assessed coronary atherosclerosis. Chest 1978;73:62-65
11. Sniderman AD, Shapiro S, Marpole D, Skinner B, Teng B, Kwiterov-ich PO: Association of coronary atherosclerosis with hyperapobeta-lipoproteinemia. Proc NatlAcad Sci USA 1980;77:604-608
12. Maciejko JJ, Holmes DR, Kottke BA, Zinsmeister AR, Dinh DM,Mao SJT: Apolipoprotein A-I as a marker of angiographicallyassessed coronary-artery disease. N EngI JMed 1983;309:385-389
13. Durrington PN, Hunt L, Ishola M, Kane J, Stephens WP: Serumapolipoproteins AI and B and lipoproteins in middle aged menwith and without previous myocardial infarction. Br Heart J1986;56:206-212
14. Kottke BA, Zinsmeister AR, Holmes DR Jr, Kneller RW, Halla-way BJ, Mao SIT: Apolipoproteins and coronary artery disease.Mayo Clin Proc 1986;61:313-320
15. Dahlen GH, Guyton JR, Attar M, Farmer JA, Kautz JA, GottoAM Jr: Association of levels of lipoprotein Lp(a), plasma lipids,and other lipoproteins with coronary artery disease documentedby angiography. Circulation 1986;74:758-765
16. Murai A, Miyahara T, Fujimoto N, Matsuda M, Kameyama M:Lp(a) lipoprotein as a risk factor for coronary heart disease andcerebral infarction. Atherosclerosis 1986;59:199-204
17. Soria LF, Ludwig EH, Clarke HRG, Vega GL, Grundy SM,McCarthy BJ: Association between a specific apolipoprotein Bmutation and familial defective apolipoprotein B-100. Proc NatlAcad Sci U S A 1989;86:587-591
18. Rall SC Jr, Weisgraber KH, Inneratity TL, Mahley RH: Structuralbasis for receptor binding heterogeneity of apolipoprotein E fromtype III hyperlipoproteinemic subjects. Proc Natl Acad Sci U S A1982;79:4696-4700
19. Karathanasis SK, Ferris E, Haddad IA: DNA inversion within theapolipoproteins AI/CIII/AIV-encoding gene cluster of certainpatients with premature atherosclerosis. Proc NatlAcad Sci U S A1987;84:7198-7202
20. Ordovas JM, Cassidy DK, Civiera F, Bisgaier CL, Schaefer EJ:Familial apolipoprotein A-I, C-III, and A-IV deficiency and pre-mature atherosclerosis due to a deletion of a gene complex onchromosome 11. 1 Biol Chem 1989;28:16349-16342
21. Russell DW, Esser V, Hobbs HH: Molecular basis of familialhypercholesterolemia. Arteriosclerosis 1989;9(suppl I):I-8-I-13
22. Brown MS, Goldstein JL: A receptor-mediated pathway for cho-lesterol homeostasis. Science 1986;232:34-47
23. The Lipid Research Clinics: Population Studies Data Book: Vol *:The Prevalence Study. Washington, DC, US Department of Healthand Human Services, NIH publication No. 80-1527, 1980
24. McNamara JR, Schaefer EJ: Automated enzymatic standardizedlipid analyses for plasma and lipoprotein fractions. C/in Chim Acta1987;166:1-8
25. Warnick GR, Benderson J, Albers JJ: Dextran sulfate-Mg2+precipitation procedure for quantitation of high-density lipopro-tein cholesterol. Clin Chem 1982;28:1379-1387
26. Friedewald WT, Levy RI, Fredrickson DS: Estimation of theconcentration of low density lipoprotein cholesterol in plasma,without use of the preparative ultracentrifuge. Clin Chem1972;18:499-502
27. Schaefer EJ, Ordovas JM: Metabolism of apolipoproteins A-I, A-IIand A-IV. Meth Enzymol 1986;129:420-443
28. Ordovas JM, Peterson JP, Santaniello P, Cohn JS, Wilson PWF,Schaefer EJ: Enzyme-linked immonosorbent assay for humanplasma apolipoprotein B. J Lipid Res 1987;28:1216-1224
29. Fredrickson DS, Levy RI, Lees RS: Fat transport in lipoproteins:An integrated approach to mechanisms and disorders. N Engl JMed 1967;276:34-44, 94-103, 215-225, 273-281
30. Third JLHC, Montag J, Flynn M, Freidel J, Laskarzewski P,Glueck CJ: Primary and familial hypoalphalipoproteinemia.Metabolism 1984;33:136-146
31. Borecki IB, Rao DC, Third JLHC, Laskarzewski PM, Glueck CJ:A major gene for primary hypoalphalipoproteinemia. Am J HumGenet 1986;38:373-381
32. Brunzell JD, Sniderman AD, Albers JJ, Kwiterovich PO Jr:Apoproteins B and A-I and coronary artery disease in humans.Arteriosclerosis 1984;4:79-83
33. Hopkins PN, Williams RR: Human genetics and coronary heartdisease: A public health perspective. Annu Rev Nutr 1989;9:303-345
34. Schaefer EJ, Lery RI, Anderson DW, Danner RN, Brewer HB Jr,Blackwelder WC: Plasma triglycerides in the regulation of HDL.Lancet 1978;2:391-393
35. Chait A, Albers JJ, Brunzell JD: Very low density lipoproteinoverproduction in genetic forms of hypertriglyceridemia. EurJClinInvest 1980;10:17-22
36. Sane T, Nikkila EA: Very low density lipoprotein triglyceridemetabolism in relatives of hypertriglyceridemic probands: Evi-dence for genetic control of triglyceride removal. Arteriosclerosis1988;8:217-226
37. Kissebah AH, Alfarsi S, Evans DJ: Low density lipoproteinmetabolism in familial combined hyperlipidemia: Mechanisms ofthe multiple phenotype lipoprotein phenotypic expression. Athero-sclerosis 1984;4:614-624
38. Schaefer EJ: Clinical, biochemical, and genetic features in familialdisorders of high density lipoprotein deficiency. Arteriosclerosis1984;4:303-322
39. Grundy SM, Vega GL: Causes of high blood cholesterol. Circula-tion 1990;81:412-427
40. Utermann G: The mysteries of lipoprotein (a). Science 1989;246:904-910
by guest on October 5, 2017
http://circ.ahajournals.org/D
ownloaded from

Genest et al Genetic Lipoprotein Disorders and CAD 2033
41. Lusis AJ: Genetic factors affecting blood lipoproteins: The candi-date gene approach. J Lipid Res 1988;29:397-429
42. Genest J Jr, Ordovas JM, Robbins AM, Salem DN, Wilson PWF,Masherain U, Frossard PM, Meade T, Cohn S, Schaefer EJ: DNApolymorphisms of the apolipoprotein B gene in patients withpremature coronary artery disease. Atherosclerosis 1990;82:7-17
43. Ordovas JM, Civeira F, Genest J Jr, Craig S, Robbins AM, MeadeT, Pocovi M, Frossard PM, Masharani U, Wilson PWF, Salem DN,Ward RH, Schaefer EJ: Restriction fragment-length polymor-phisms of the apolipoprotein AI-CIII-AIV gene locus, relation-ships with lipids, apolipoproteins, and premature coronary arterydisease. Atherosclerosis 1991;87:75-86
44. Breslow JL: Genetic basis of lipoprotein disorders. J Clin Invest1989;84:373-380
45. Genest J Jr, McNamara JR, Ordovas JM, Jenner JL, SilbermanSR, Anderson KM, Wilson PWF, Salem DN, Schaefer EJ: Lipo-protein cholesterol, apolipoproteins A-I and B, and lipoprotein (a)abnormalities in men with premature coronary artery disease.JAm Coil Cardiol 1992;19:792-802
46. Genest J Jr, McNamara JR, Upson B, Salem DN, Ordovas JM,Schaefer EJ, Malinow MR: Prevalence of familial hyperhomocyst-(e)inemia in men with premature coronary artery disease. ArterioThromb 1991;11:1129-1136
47. Genest J Jr, Corbett HM, McNamara JR, Schaefer MM, SalemDN, Schaefer EJ: Effect of hospitalization on high-density lipo-protein cholesterol in patients undergoing elective coronary angi-ography. Am J Cardiol 1986;61:998-1000
by guest on October 5, 2017
http://circ.ahajournals.org/D
ownloaded from

Silberman, P W Wilson, D N Salem and E J SchaeferJ J Genest, Jr, S S Martin-Munley, J R McNamara, J M Ordovas, J Jenner, R H Myers, S R
Familial lipoprotein disorders in patients with premature coronary artery disease.
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1992 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.85.6.2025
1992;85:2025-2033Circulation.
http://circ.ahajournals.org/content/85/6/2025the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on October 5, 2017
http://circ.ahajournals.org/D
ownloaded from
Top Related