







Languages
Pages
Legal


1
Factors Affecting Motivation and Retention of Primary
Level Health Care Workers in Three Disparate Regions in
Kenya

2
Factors Affecting Motivation and Retention of Primary-
Level Health Care Workers in Three Disparate Regions In
Kenya
AMREF Kenya Human Resources For Health Project
Operations Research Report – Conducted in Machakos, Kibera and Turkana
August 2012
© AMREF 2012

3
Table of Contents
List of Tables .................................................................................................................................. 4
List of Figures ................................................................................................................................. 4
List of Acronyms ............................................................................................................................ 5
ACKNOWLEDGMENTS .............................................................................................................. 6
EXECUTIVE SUMMARY ............................................................................................................ 7
CHAPTER ONE: BACKGROUND AND INTRODUCTION ...................................................... 9
CHAPTER TWO: PROBLEM STATEMENT, LITERATURE REVIEW AND OBJECTIVES 15
CHAPTER THREE: RESEARCH METHODOLOGY ............................................................... 20
CHAPTER FOUR: FINDINGS .................................................................................................... 24
4.1. Background Characteristics of Respondents .................................................................. 24
4.2. Service Characteristics and Distribution of Health Care Workers ................................. 25
4.3. Training .......................................................................................................................... 26
4.4. Comparison of Training Factors .................................................................................... 26
4.5. Preference for Where to Work ....................................................................................... 26
4.6. Work Environment ......................................................................................................... 27
4.7. Satisfaction Factors ........................................................................................................ 29
4.8. Remuneration ................................................................................................................. 30
4.9. Compensation Factors .................................................................................................... 31
4.10. Job Stability ................................................................................................................ 32
4.11. Insights from Qualitative Interviews .......................................................................... 34
CHAPTER FIVE: DISCUSSIONS, RECOMMENDATIONS AND CONCLUSIONS ............. 36
REFERENCES AND BIBLIOGRAPHY ..................................................................................... 41
APPENDIXES .............................................................................................................................. 45

4
List of Tables
Table 1: Background Characteristics of the Study Population ..................................................... 24
Table 2: Distribution of Types of Service Providers by Region ................................................... 25
Table 3: Training Characteristics of Professional Health Workers .............................................. 26
Table 4: Satisfaction Factors that differed across Facility Types ................................................. 30
Table 5: Percentage of Factors Related to Remuneration by Region ........................................... 31
Table 6: Percentage Distribution of Factors Related to Intention to Leave by Region ................ 33
Table 7: Summary of Thematic Issues Emanating from FGDs in the Three Regions ................. 35
List of Figures Figure 1: Preference of Working Institution ................................................................................. 27
Figure 2: Comparison of Work Environment Factors by Facility Type ....................................... 28
Figure 3: Importance of Compensation Factors............................................................................ 32
Figure 4: Proportion of Professional HCW who Changed Jobs in the last year by Region ......... 32

5
List of Acronyms
AMREF African Medical and Research Foundation
HCW Health Care worker
HRH Human Resources for Health
HRM Human Resource Management
HENNET Health NGOs Network
NGO Non-Governmental Organisation
FBO Faith-Based Organisation
GoK Government of Kenya
WHO World Health Organisation
6
ACKNOWLEDGMENTS
This operations research study was conducted by a small team of consultants and AMREF Kenya
staff under the Human Resources for Health (HRH) Project. We express our appreciation to the
many stakeholders, public and private, who provided in-depth information for the study. In
particular, the management and staff of the various health facilities in Turkana and Machakos
Counties and in Kibera informal settlement who were visited during the study.
Secondly, we acknowledge support and input from the AMREF Kenya Country Director, Dr.
Lennie Bazira; Programme Manger, Research Advocacy and Business Development Unit, Dr.
David Ojakaa; Research Officer, Hellen Gakuruh; immediate former Project Coordinator, Allan
Oginga; Project Officer, Abigael Lukhwaro; Project Coordinator, Susan Olang‟o.
AMREF Kenya acknowledges the partnership and collaboration of World Vision Kenya (WVK)
and the Health NGOs Network (HENNET) who are co-partners in the HRH project. This study
would not have been possible without financial support from the European Union and World
Vision Kenya.
Last but not least we thank the team of consultants who conducted the study; Millicent Muiru,
Francis Njiri, Mary Nandili and Jackson Nguriarengan.

7
EXECUTIVE SUMMARY
Background
Functional, effective, efficient and well distributed human resources for health (HRH) are
recognized by the World Health Organization and the Government of Kenya as critical
ingredients and determinants of better health for all. Within the HRH action framework, this
study was conducted in Turkana, Machakos and Nairobi counties, regions in which AMREF and
World Vision have been working in before.
Problem Statement
The health sector in Kenya is currently undergoing previously unprecedented reviews and
changes in policy and practice. However, motivation and retention of health workers especially
at the lower (primary) levels of health care persists as a serious challenge to better health for all
Kenyans.
Objectives
This study investigated the critical factors influencing motivation and retention of health workers
working in primary health care facilities in three different settings in Kenya.
Methodology
A cross-sectional survey was conducted among selected health care workers. A cluster sample
design was used to select 404 health care workers for interview. Data were collected using
structured questionnaires and a Focus Group Discussion guide. Data generated were analyzed
using bi-variate and multi-variate methods of the associations and determinants of health worker
motivation and retention.
Key Findings
A total 404 health service providers in 10 categories1 were interviewed. Of these, 234 were
females (57%), 264 were married (65%), the mean age was 34 years, while 324 (80.2%) had post
secondary school training. Overall, more than 13% of the respondents changed jobs in the last 12
months and less than 44% were satisfied with their jobs.2 Intention to leave was highest in
Turkana with 88% of respondents indicating they would leave their current job to work in a
different district and 82% would take up jobs outside the health facility if given the opportunity.
Family health care (87.4), salary (83.6), and terminal benefits (79.3) are important compensation
1 5 Medical Officers, 35 Clinical Officers, 93 Registered Nurses, 23 Enrolled Nurses, 32 Lab Technicians, 10
Nutritionists, 20 Counselors, 13 Pharmacists, 21 CHEWs and 152 Support Staff. 2 Percentages in the findings section (apart from demographics) represent those who agree or strongly agree with
the attributes.

8
factors closely linked to motivation and retention. About 76% of health care workers in
Machakos felt that they had unfair salary compared to 56%-Nairobi, 53% Turkana (p<0.0001).
About 91% of the respondents in Machakos felt that hardship allowance is important, while
71%-Nairobi, and 64%-Turkana (p<0.0001) felt the same. Inefficient and unreliable transport to
work (60%) and lack of electricity (85%) were the main de-motivational factors in Turkana,
while an appreciation of the local culture (86%) was a positive motivator3.
Turkana (28%) compared with Nairobi (45%) and Machakos (46%) had the lowest number of
diploma holders (p<0.0001). In comparison to the other areas, (52% - Machakos and 27% -
Turkana), Kibera registered a higher percentage (60%) of those who acknowledged receiving on-
the-job training.
Conclusion and Recommendations
The study findings demonstrate that there are distinct motivation and retention factors affecting
health workers in the three disparate regions. Insights from the study also show that the issues
(such as job satisfaction and conducive work environment) can be addressed. The findings of this
study should be used to strengthen HRH systems in the proposed county governments to
motivate and retain health care workers in the respective counties. The findings should also be
used to review the national Human Resources for Health policies and strategic plan. Specifically
there is need to:
1. Develop comprehensive and equitable continuous training programmes for health workers in
hard-to-reach regions.
2. Develop and implement gender mainstreaming strategies in the facilities to address the
gender issues identified in this study.
3. Develop and apply retention schemes specific to the three respective regions
4. Address job satisfaction factors such as adequate staff numbers, supervision, basic equipment
in the hard to reach areas in particular.
5. Tackle issues related to working conditions such as energy supply, equipment, and housing
in Turkana and Machakos regions in particular.
6. Decentralize HRH management system to the regions to address issues specific to regions
7. Develop competitive compensation packages for health staff particularly in hard to reach
areas to include family health care.
8. Develop strategies for career growth and promotion especially for higher cadre of health
workers such as doctors.
9. Develop and establish a model “HRH community” within selected NGO/FBO health
facilities in hard to reach areas.
3Deeper insight from the FGDs suggests that most of those interviewed in Turkana in comparison to Kibera and
Machakos are indigenous to the area.
9
CHAPTER ONE: BACKGROUND AND INTRODUCTION
1.1.1 Human Resources for Health: A Global Perspective
Human resources are the most important asset of any health system strengthening and consume a
major share of the resources allocation in the sector. Human Resources for Health (HRH) can be
defined as the different kinds of clinical and non-clinical staff responsible for public and
individual health intervention. The global shortage of health workers is estimated to be around
2.3 million physicians, nurses and midwives, and over 4 million health workers overall (WHO,
2009). Regional disparities exist between countries with sub-Saharan Africa requiring an almost
140% increase in the health workforce in order to overcome the crisis of the health workforce. A
statistically significant relationship has been established between health worker density and the
burden of disease, expressed in Disability Adjusted Life Years (DALYs) (Castillo-Laborde,
2011).
Increased investments in HRH produce many tangible benefits which include improving the
overall health of individuals and families. Moreover, investments in HRH would allow people to
enjoy a basic human right; and in this context therefore, HRH is not solely a health issue, but a
matter of economic development and social justice. An estimated $500 million is spent annually
on medical education of workers from Africa who will eventually emigrate to the developed
world and serve the populations in these countries (Chen L et al). The UN recognizes that MDGs
cannot be achieved in low resource settings without attention to population issues and access to
services4 (UNDP, 2005). Quick-win HRH interventions such as increasing the efficiency and
effectiveness of skilled care during and after labor and delivery can make the difference between
life and death for both women and their newborns.
A prerequisite for a well-functioning health system is a well-motivated staff. Low level of health
worker motivation has often been identified as a central problem in health service delivery
among existing human resources. Motivation and retention are major concerns in human
resources for health. Health workers are susceptible to push factors such as pay and working
conditions and pull factors such as job satisfaction and economic prospects. Ensuring staff
receive adequate pay for their work is key to retention. However it is not just salary that is
important. In many contexts, the low numbers of trained health staff in remote areas is due to the
lack of supporting infrastructure and opportunities for staff and their families. In fragile contexts,
these factors include poor living conditions, the lack of safety and security in the workplace, and
the absence of continuous professional development (Global Health Magazine July 2010).
4 UNDP 2005. Population, Reproductive Health and the Millenium Development Goals. Message from the UN Millenium Project Report. New York: UNDP.

10
Motivation is influenced by both financial and non-financial incentives. Though financial
incentives are important, increased salaries are by no means sufficient to solve the problem of
low motivation. More money does not automatically imply higher motivation. Low motivation
has a negative impact on individual performance, health facilities and generally the health
system. The results from a survey undertaken by the German Technical Cooperation, (GTZ)
among representatives of ministries of health and GTZ staff from 29 countries showed that low
motivation is the second most important health workforce problem after staff shortages.
1.1.2. The Place of Human Resources for Health (HRH) in the health system
The important role of the health workforce is universally recognized in the WHO health systems
framework (WHO, 2007). Together with service delivery, information, medical products,
financing, leadership and governance, human resources for health constitute the six building
blocks which are essential for promoting and maintaining health. The concern about the health
workforce is that it should be well-performing. In this regard, good performance of the health
workforce is assessed in terms of its adequacy in numbers, combination of the various cadres,
equitably distributed between the various regions of the country, competent, and productive.
1.1.3. The Human Resources for Health Action Framework
The Health Action Framework (MSH, 2009) is a useful perspective for showing how human
resources for health are linked to better health outcomes. It is also a tool that Governments and
programmes can use to address the HRH crisis. The health action framework shown below
consists of six elements which are described briefly below.

11
Source: http://www.capacityproject.org/framework/
Human Resource management systems include integrated use of data, policy and experience
from practice in order to adequately plan for, recruit, post, develop, and support health workers.
The second element focuses on leadership – the capacity to provide direction, organize people,
and mobilize resources. The third aspect – partnerships – involves linking stakeholders in order
to maximize use of human resources for health. The aspect on Finance focuses on sourcing,
sharing, and distributing funding for human resources for health. The fifth aspect of the action
framework – education - is producing and maintaining a skilled workforce. Policy is the sixth
and last element of the HRH action framework. It covers legislation, regulations, and
requirements for employment, working standards, and development of the health workers.
1.1.4. Human Resources for Health in Kenya
Several Kenyan policy documents articulate HRH issues. Two of these are the Kenya Health
Policy 2012-2030 and the Kenya Health Sector Strategic Plan July 2012-June 2017. In the health
policy, the health workforce is identified as one of the seven policy orientations which the health
12
sector will invest in and strive to attain. Under health workforce policy direction, the
Government intends to provide for adequate and equitable distribution of human resources. This
will be achieved through several strategies; one of them being enhancement of the management
of the health workforce by setting up or strengthening mechanisms for the attraction, retention,
and motivation of the workforce, particularly in the marginalized areas.
The health sector strategic plan divides the implementation of the health policy framework into
five years. As such, the current strategic plan (2012-2017) is the first of the five year plans of the
Kenya Health Policy 2012-2030. It is aligned to two key Government agenda: the 2010
Constitution and the Vision 2030. Several articles of the Kenya 2010 Constitution have a bearing
on health. One of these is Article 174 relating to the staffing of the respective county
Governments: establish and abolish offices, appointments, confirmations, and discipline of staff.
The strategic plan outlines the main issues related to the attraction and retention of human
resources for health in Kenya. These include high levels of attrition, unfavourable terms and
conditions of service, lack of incentives in hard to reach areas, disharmonized remuneration, low
levels of employee satisfaction, and stagnation due to unfavorable career guidelines.
The Government of Kenya (GOK) views human resource development in the health sector as an
essential component of the health system especially in the provision of basic health services.
There is growing recognition that HRH in the public sector are shrinking dramatically, thereby
affecting the delivery of services. Several studies have shown that the emergence and re-
emergence of infectious diseases, such as HIV/AIDS, tuberculosis, and malaria, have also
increased the demand for health services, putting enormous stress on the existing human
resources (ROK 2006).
Generally, the HRH function in Kenya can be observed from three broad lenses: availability of
the required health workforce to deliver quality health care services at all levels of health care;
equitable distribution of health workforce across the country irrespective of the nature of the
physical and social environment; and provision of quality health care services supported by
strong pillars of performance management, compensation and sensitivity to basic human
requirements that make service delivery in harsh environments possible. Kenya currently faces
several HRH related challenges. HRH ratios in Kenya fall below the WHO recommended
standards, for example, the WHO recommended staffing levels for key health workers (doctors,
nurses and midwives) is 2.3 per 1000 population as compared to Kenya‟s 1.5 per 1000
population. In 2008, the Ministry of Health had 33,317 filled positions out of the approved
required number of 47,247; an overall vacancy level of 29% as compared to 2006 when 35,627
positions were filled out of an establishment of 44,8135. Retirement has previously been cited as
5 „Human Resources for Health Strategic Plan 2009-2012‟-MoMS 2009
13
the major cause of attrition with the attendant imbalance in equitable distribution of HRH
especially in public sector. However with the increase of the public sector retirement age in
2007-2008 from 55 to 60 years there is hope that attrition due to retirement will improve,
although migration and „streamlining‟ of public sector employment in line with the new
constitution may present new challenges with regard to equitable distribution. With regard to
quality health care services, it is estimated that in Kenya, US$65,997 is spent educating one
medical doctor from primary school to university and for every doctor who emigrates
US$517,931 returns in investment are lost, seriously undermining the quality of HRH work force
(Kirigia J et al).
Kenya has been trying to improve the functioning of health care delivery system to ensure that
the general population receives quality services. Towards this end the Government launched the
first ever National Human Resources for Health Strategic Plan 2009-2012 in 2009. This
strategic plan has five projected outcomes: appropriate numbers and types of health workers in
post and equitably distributed, retention of health workers improved at all levels, improved
institutional and health worker performance, strengthened human resources development systems
and practices and strengthened human resources planning and management. The strategic plan
identifies retention as a major concern as health workers continue to leave the subsector and
sector especially the highly mobile cadres of doctors and nurses and the problem is more acute in
remote/hard to reach areas. The plan therefore prioritises improved attraction and retention of
health workers as one of the anticipated outcomes.
The Human Resources for Health Strategic Plan 2009-2012 (ROK, 2009) summarizes the
situation of the health workforce in Kenya. Out of a total establishment of 47,247 positions in
2008, the Ministry of Health had 33,317 positions occupied. Between 2004 and 2008 however
the number of staff employed by the Ministry of Health declined significantly. During the same
period, the population increased by 7%, implying a decline in coverage. A number of
development partners (such as the US-funded Capacity Project) have supported the recruitment
of the health workforce. This number of contract staff is significant – it represents the equivalent
of increasing the MOH workforce by 10%.
There is inadequate data on the health labour market. Informal data however indicate that there is
a large number of unemployed qualified health personnel in the country. This is mainly due to
the past freeze on public sector recruitment with a large number of people applying for a limited
number of positions. Other programmes that have attempted to rapidly absorb health workers are
the Emergency Hiring Programme (EHP) and the Economic Stimulus Package (ESP) which is
focused at the constituency level.
The Kenya HRH strategic plan has identified five strategic objectives to be addressed which are
based on five outcomes, one of which is retention of health workers improved at all levels. The

14
two objectives to be attained in order to reach this outcome are making health sector jobs more
attractive in order to improve staffing levels and reduce attrition, and making hard to reach areas
more attractive to health workers.
1.2. The Human Resources for Health Advocacy Project
The study was conducted as one of the deliverables of a HRH in Kenya advocacy project funded
by the European Union through World Vision Austria and locally implemented by World Vision
Kenya (WVK), Health NGOs Network (HENNET) and AMREF Kenya The project is to run
from January 2011- December 2013.
The HRH Health Advocacy Project seeks to enhance access to primary healthcare countrywide
through advocacy for increased human resources and effective community based demand side
including accountability from primary health delivery institutions. It is being delivered through a
three-pronged strategy based on the competencies of the three implementing partners. The
partners are to utilize their national presence and key strategic community presence to leverage
lobbying for better primary healthcare for poor communities. The community strategy
component is being implemented in six districts (also partner project areas) spread across three
regions. The sites are significantly varied and offer a wide scope for implementation, learning
and innovation. The remote and arid Turkana North district is a hardship area comprising
nomadic pastoralist livelihood group. Machakos, Yatta, Mwala, and Mutonguni districts are
agro-pastoralists falling within the relatively accessible rural Eastern region, while the informal
settlement of Kibera comprises the most socio-economically disadvantaged groups in Nairobi.

15
CHAPTER TWO: PROBLEM STATEMENT, LITERATURE REVIEW AND
OBJECTIVES
2.1. Problem Statement
As the 2010 Constitution is enacted and the devolved county governments take shape, a number
of issues related to the management of human resources at the sub-county level need to be
articulated. Motivated, functional and equitably distributed human resources for health (HRH)
are both essential for implementing the strategic plan at the sub-county level and ensuring
primary health care for all Kenyans. However, there are a number of critical factors that
contribute to the motivation and retention of staff, and these are not currently well-understood in
the Kenyan context. Moreover, Kenya is a diverse country both culturally and geographically,
and this diversity leads to different working conditions in different regions. Without a clear
understanding of the various factors that affect health care worker motivation and retention in
different environments, it is likely that communities will continue to face challenges in receiving
accessible and high quality primary health care. This study, therefore, will examine the factors
that lead to motivation and retention of health workers at the primary health care level in three
disparate regions of Kenya.
2.2. Literature Review
2.2.1. Motivation
Factors in the motivation and retention of health workers in developing countries have been
systematically reviewed. The major themes regarding motivation of health workers include:
finance in terms of salaries and allowances; career development (possibility to specialize or be
promoted); education (pre-service and in-service); infrastructure; work environment; resource
availability; management; and personal recognition or appreciation (Willis-Shattuck et al., 2008).
Studies on motivation address a number of issues. A ten item score developed to measure
motivation of health workers, motivation being an individual‟s degree of willingness to exert and
maintain an effort towards attaining organizational goals, may be useful to measure changes in
motivation over time or for rapid assessment of health worker motivation (Mbindyo, Blaauw,
Gilson, & English, 2009). Contextual factors are also important in the motivation of health
workers (Mbindyo, Gilson, Blaauw, & English, 2009). Measuring and managing the work
environment of the middle-level provider is equally important (McAuliffe et al., 2009). The
question of burnout of health workers has been addressed in Zambia (Kruse et al., 2009). In
Lusaka, overwork, illness and death are primary reasons for the attrition of health workers. The
study shows that programmes to improve access, acceptability and confidentiality of health
provider services and reduction of workplace stress could improve workforce stability.

16
Human resource leadership is important (O'Neil, 2008). Research findings (O'Neil, 2008) show
that the leadership development programme makes a profound difference in health managers‟
attitude towards their work. Rather than perceiving that one is defeated by a workplace
environment, people report that they are being mobilized to take action to change the status quo.
The lesson is that without this capacity at all levels, global policy and national human resources
for health strategies will fail to make a difference.
A survey conducted by the Ministry of Medical Services in Kenya (Republic of Kenya, 2009)
highlights some of the key issues related to the motivation and satisfaction of the health workers.
In a representative sample of 32 health facilities in the republic, the survey – on employee
satisfaction - sought information on several aspects such as job factors, compensation, work
environment, supervision, and promotion among health staff working at the level of sub-district,
district and provincial public health facilities. Background characteristics of the sampled
respondents provide insights into the profile of a typical health worker in a Kenyan health
facility. The mean age of employees was 40 years; the majority (62%) were female. Most (78%)
were married, and about three quarters of them (72%) had secondary education. The employees
had served in the Ministry for an average of 15 years.
The survey also gathered information on motivation of Kenyan health workers. With regard to
job satisfaction, although the majority of the staff (93%) reported that they liked their work, there
was also an increase in the proportion who indicated that they lacked the resources to accomplish
their tasks adequately. Over half of the employees have had training opportunities and the same
proportion have had openings for career advancement. Compared to results of a similar survey
conducted in 2007, there was an increase (by 5%) in the number of staff who felt that the current
remuneration package that they receive negatively affects their work. Most of the staff indicated
dissatisfaction with the civil service compensation package, compared to other people working
outside the service. The majority of the staff (69%) had not received feedback on their
performance in the last one month. Only 10% are satisfied with the promotion system.
2.2.2. Incentives
The question of incentives is prominent in the literature on motivation of health workers. Non
financial incentives and human resource management tools play important roles in increasing the
motivation of health professionals in Africa (Mathauer & Imhoff, 2006). This involves
acknowledging the professionalism of health workers and addressing professional goals such as
recognition, career development, and further education. The work environment should be
developed to enable health workers to meet their personal and organizational goals. Further,
financial incentive programmes for return of medical services in underserved areas can alleviate
labor shortages (Barnighausen & Bloom, 2009). Seven management functions essential for the
success of incentives comprise financing, promotion/marketing, selection, placement, support,

17
enforcement, and evaluation. However, they may not improve the working and living conditions
in underserved areas. Financial incentives, non-financial incentives, and compulsory service can
re-enforce each other. Literature also shows that several non financial incentives are in place
(Dambisya, 2007). These include training and career-path related incentives, incentives
addressing social needs, improved working conditions, human resource management (HRM) and
human resource information systems (HRIS). A new HRIS in Uganda has helped in tracking and
monitoring the health workforce (Spero, McQuide, & Matte, 2011).
Findings on a study on incentives for health worker retention in Kenya (Ndetei et al., 2007)
provide a number of insights. In public facilities, there are many unfilled positions. Primary
Health Care (PHC) facilities are severely understaffed. Management practices are also important,
but the strategic information needed for effective management is missing. Routine information
needed to assess impact of incentives is not accessible. The Government therefore needs to put in
place further national-level policies to retain health workers in rural areas. Other studies (Proper,
Deeg, & Beek, 2009) also show that measures which promote challenges at work, together with
financial stimuli, appear to hold promise in promoting longer workforce participation.
Lessons drawn from the implementation of health workers‟ salaries and benefits in South
America – Bolivia, Peru, and Chile - show that common problems related to the pay and
benefits of health workers include the shortage, distribution, working environment, and
inadequate knowledge of health workers (Gonzalo Urcullo, 2008). Wages of doctors in the three
Latin American countries increased significantly in the last 15 years relative to those of other
health workers. Salaries of health workers respond to a number of factors. While the basic salary
of a health worker represents a half to two thirds of the total income, the rest is made up of on the
job bonuses, allowances for working in remote areas, and adjustments following advanced
studies. Political and economic factors that play a role in the determination of salary levels
comprise the bargaining power of trade unions as well as professional bodies, economic growth,
and inflation. The public sector is the largest employer of health workers. However retention is
more difficult as the private sector provides better terms of service.
Literature reviewed from sub-Saharan Africa shows that salaries of health workers in the public
and private sectors are an important aspect in the functioning of the health system (David McCoy
2008). The study shows that pay structures not only vary between countries, but are also
constructed in complex ways. Pay and income of health workers, while varying between
countries, also differ by cost of living, and by sector – public and private. Health workers
supplement their salaries with other sources of income. The study concludes by highlighting the
need for policy interventions to address the pay and income of health workers. Fiscal constraints
to salary increments and non-financial incentives also need to be considered.

18
2.2.3. Retention
A study to determine policies to improve nurse recruitment and retention in rural Kenya
(Mudhune, 2009) has identified a number of job attributes that can be directly influenced by
health policy in order to increase attraction to rural postings. These include permanent contracts
linked to rural posts, allowances, opportunities for training and reduce years of experience before
being promoted. These results show that nurses place the highest value on attributes that would
be expected to have immediate monetary advantages such as salary enhancement or long term
factors (promotion, training and permanent contract). A study conducted in rural Ghana (Snow
et al., 2011) has investigated the factors related to low retention of health workers. For doctors,
although salary is important, it is more the career development concerns which keep them in
urban areas. The study also shows that short-term service in rural areas would be preferable if it
was linked to coaching and mentoring, as well as career growth.
In investigating reasons for poor recruitment and retention of nurses in rural Kenya (Mullei et al.,
2010) make a number of recommendations. These comprise additional rural allowances, and
allowing choice of rural location. Greater investment is needed on information to assess the
impact of such policies. Other studies (Lehmann, Dieleman, & Martineau, 2008) show that to
adequately staff remote areas, planning and decision-making on retention require multi-sectoral
collaboration. Findings from investigations on workforce stability (Buchan, 2010) conclude that
for policy and advocacy purposes, it is important to examine the interactions between staff
turnover and organizational performance.
A study by the Regional Network for Equity in Health in East and Southern Africa (EQUINET
sought to investigate the causes of migration of health professionals, the strategies used to retain
health professionals, how they are being implemented, monitored and evaluated, as well as their
impact, to make recommendations to enhance the monitoring, evaluation and management of
non-financial incentives for health worker retention. It revealed that all four countries studied
(Swaziland, Zimbabwe, Tanzania, Kenya) have put in place strategies to improve morale and
retain staff in the public health sector. Nevertheless it raised caution about approaches that target
specific groups. The study pointed to cadres that appear to have been excluded from incentive
strategies, particularly those cadres that work at community level and that form a bridge to other
actors who play a role in primary health care, such as traditional health providers and
community health workers (Dambisya, 2007).
Several reasons explain attrition of health workers in Kenya (Chankova, Muchiri, & Kombe,
2009). These include retirement, resignation, and death. Appropriate policies to retain staff in the
public health sector may need to be tailored for different cadres and level of health facility are
therefore required. An ethnographic study on attrition among community health workers in home
based care (HBC) programmes in Western Kenya (Olang'o, Nyamongo, & Aagaard-Hansen,
2010) reveals a number of underlying factors. The reasons for dropout included the cultural
environment within which CHWs operated; lack of adequate support from area NGOs; poor

19
selection criteria for CHWs; power differences between NGO officials and CHWs. This fostered
lack of transparency in the NGOs' operations. The study concludes that to achieve well
functioning and sustainable HBC services, factors which influence retention and dropout of
CHWs should be addressed. These should take into account the socio-cultural, programmatic,
and economic contexts within which CHW activities are implemented.
The question of retention of health workers has also been addressed in a study in Malawi
(Manafa et al., 2009). Results from the investigation show that continuous education and
progressive career growth are inadequate. Standard HRM practices such as performance
appraisal and job descriptions were not present. Health workers felt that they were inadequately
supervised, with no feedback on performance. However, managers did not perceive these
deficiencies as having an impact on motivation. The study concludes that a strong HRM unit
operating at the district level in Malawi is likely to improve worker motivation and performance.
2.2.4. Summary of Literature Review
A number of observations can be deduced from the literature review. First, in the developing
world as a whole and sub-Saharan Africa in particular, the salary and income of health workers
are important factors in their motivation. This aspect, as viewed from an overarching perspective
of the economics of the health care workforce – including related financial and non-financial
incentives - comprised an important variable examined in this study. Secondly, the literature
highlights the motivational concepts related to the health workforce. These motivational factors
are also considered in the conceptual framework of the study. Lastly, it is evident that there are
virtually no rigorous studies on the retention of health workers in Kenya, particularly in
underserved communities. This study seeks to bridge this knowledge gap.
2.3. Objectives
2.3.1. General:
The general objective of this study is to investigate critical factors related to the motivation and
retention of health workers in three settings in Kenya – remote areas, disadvantaged urban
informal settlements, and relatively accessible regions.
2.3.2. Specific Objectives:
1. Explore themes underlying motivation and retention of health workers in three Kenyan
settings
2. Explore the association between individual, motivation, and retention factors and the three
settings/regions
3. To determine the relationships (strength and direction) between identified factors and
motivation/retention

20
CHAPTER THREE: RESEARCH METHODOLOGY
3.1. Study Groups and framework
3.1.1. Study Groups
The study/population consisted of all health workers in the health facilities in the region
(Turkana, Greater Machakos, and Machakos). These health workers comprised technical plus
non technical health staff who included; doctors, nurses, clinical officers, laboratory officers, and
clerks, as well as support staff. The focus in the study was the effects of individual
characteristics, and context on the motivation and retention/drop out of the health workers.
Qualitative information related to motivation and retention was also collected through FGDs
conducted with groups of health workers (professional health workers; support staff in the
selected health facilities). The study was conducted in three districts in which AMREF already
has on-going projects. The three districts are the remote Turkana North district in the North Rift
Province (nomadic and hard-ship area), the relatively accessible Greater Machakos district in
Lower Eastern, and Kibera – a socio-economically disadvantaged slum district in Nairobi city.
3.1.2. Outcome Variables
Health worker motivation and drop out (attrition) was measured through face to face interviews
conducted during this baseline survey. They will be measured again 24 months later. The same
health facilities will be visited at the end of 24 months.
3.1.3. Other Factors and Potential Confounders
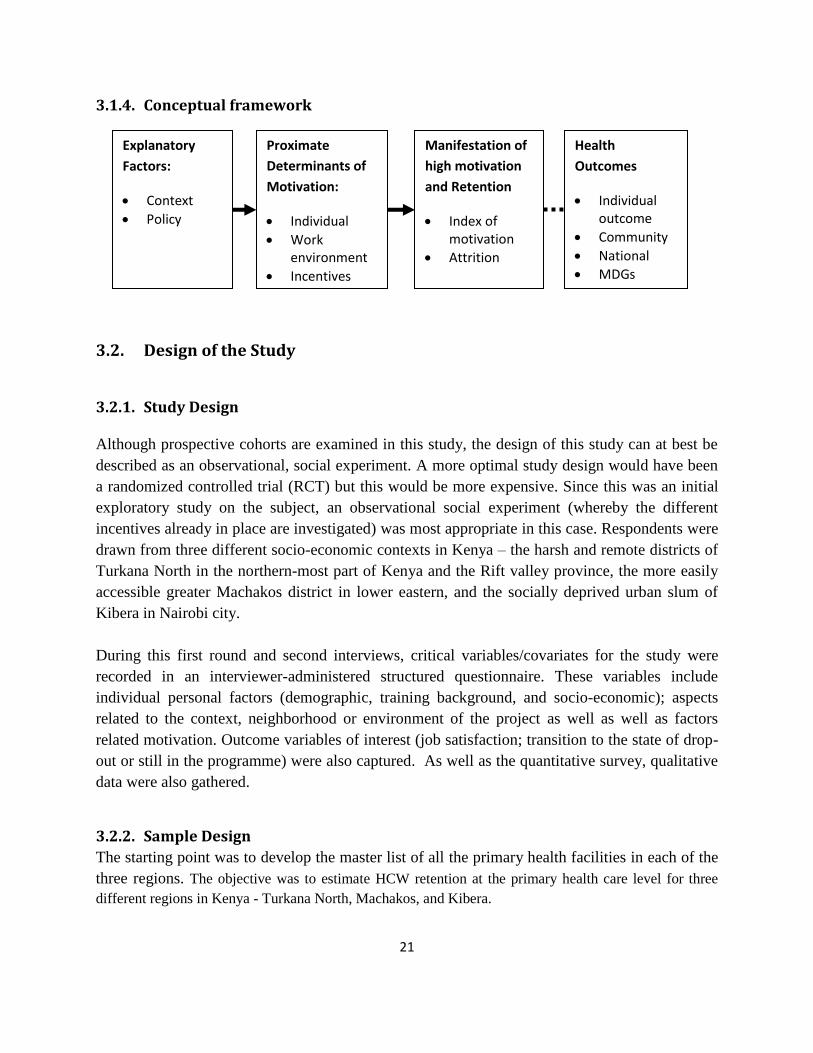
The diagram below shows a simple framework for health worker motivation and retention in the
three settings in Kenya. It consists of background factors, intermediate variables, and the
outcomes. Background factors include the policy environment and context/setting. Proximate
determinants of health worker motivation include individual factors and organizational climate.
Motivation is measured by a combination of ideas which include the level of satisfaction.
Motivated individuals contribute to higher retention rates. The combination of motivation and
high retention in turn result in better health outcomes at the individual, community, national and
international levels (e.g. attainment of Millenium Development Goals).
21
3.1.4. Conceptual framework
3.2. Design of the Study
3.2.1. Study Design
Although prospective cohorts are examined in this study, the design of this study can at best be
described as an observational, social experiment. A more optimal study design would have been
a randomized controlled trial (RCT) but this would be more expensive. Since this was an initial
exploratory study on the subject, an observational social experiment (whereby the different
incentives already in place are investigated) was most appropriate in this case. Respondents were
drawn from three different socio-economic contexts in Kenya – the harsh and remote districts of
Turkana North in the northern-most part of Kenya and the Rift valley province, the more easily
accessible greater Machakos district in lower eastern, and the socially deprived urban slum of
Kibera in Nairobi city.
During this first round and second interviews, critical variables/covariates for the study were
recorded in an interviewer-administered structured questionnaire. These variables include
individual personal factors (demographic, training background, and socio-economic); aspects
related to the context, neighborhood or environment of the project as well as well as factors
related motivation. Outcome variables of interest (job satisfaction; transition to the state of drop-
out or still in the programme) were also captured. As well as the quantitative survey, qualitative
data were also gathered.
3.2.2. Sample Design
The starting point was to develop the master list of all the primary health facilities in each of the
three regions. The objective was to estimate HCW retention at the primary health care level for three
different regions in Kenya - Turkana North, Machakos, and Kibera.
Explanatory
Factors:
Context
Policy
Proximate
Determinants of
Motivation:
Individual
Work environment
Incentives
Manifestation of
high motivation
and Retention
Index of motivation
Attrition
Health
Outcomes
Individual outcome
Community
National
MDGs

22
The Health Facility listing frame was constructed from the 3 blocks consisting only of Level 1-3 facilities
and private facilities that were operational in the divisions that were of interest. This consisted of 208
health facilities which were the “Primary Sampling Units” (PSU) – the clusters (Appendix 1). The HCWs
were in these facilities were the “Secondary Sampling Units” (SSU).
The number of clusters (health facilities) to be sampled was obtained using the formula below;
-------The Johns Hopkins University and Saifuddin Ahmed, 2009.
Where;
p represents the estimated retention rates (estimated at 80%), d is the level of precision (0.05), m
is the average cluster size (approx 7) and ρ is the intra-cluster correlation coefficient estimated at
0.25. This indicated that we required 45 clusters (health facilities). Adjusting for 30% non-
response and loss to follow up, we needed to visit 58 health facilities. The numbers of health
facilities in each of the regions were 72, 70 and 66 for Turkana, Langata and Machakos
respectively. The average numbers of HCWs for each facility in each of the regions were
estimated at 2, 10 and 8 for Turkana, Langata and Machakos respectively. We weighted each of
the 3 regions based on the number of health facilities and the number of HCWs in each facility
and used the weights to allocate the number of health facilities that should be visited for each
region.
Thus, the number of health facilities selected from each of the regions were; Turkana 26,
Langata 17 and Machakos 16. Given the low numbers of health workers usually posted to work
in level 2 and 3 health facilities, the study interviewed all staff found on site.
While health facilities were selected purposively to reduce costs and minimize inconvenience,
the selection process ensured that the selected sites were well distributed geographically.
3.2.3. Data Collection
This was a cross-sectional study aimed to explore the different incentives already in place
supporting staff performance as well as the contextual performance. Subsequent to the baseline,
a cohort study design shall follow with similar respondents re interviewed at 24 months. The

23
entire HRH study shall be expected to last at least 36 months. Approaches of this study
integrated observational and social experiment, best identified to determine change.
Data collection instruments were designed and developed by AMREF. Both quantitative as well
as qualitative tools were applied during the interviews. To ensure quality and validity of these
tools, a pre-test was conducted in health facilities out of the study site. Eighteen research
assistants were recruited from across the country to conduct interviews. The team was trained for
two days to facilitate proper use of tools. The tools were also translated in local languages to
ensure ease of use. Data were collected from every enrolled participant through a face-to face
interview following a structured quantitative questionnaire by a trained research assistant at each
of the respective three selected sites. In addition qualitative interviews were held through Focus
Group Discussions (FGDs) and in-depth interviews (2 in each study site). Representation was
drawn from both public and private health facilities with technical staff and support staff forming
forums. A sample size of 404 was calculated statistically of who were decided to undertake
interviews. All forms of biases were addressed from the beginning to end of study.
The study focused on the effects of individual characteristics, context, and incentives on the
motivation and retention/drop out of health workers. AMREF identified seven possible factors
suitable to measure outcome of interest. Dependent and independent variables were adequately
chosen as variables to determine the effects of interest on job satisfaction; transition to the state
of drop-out or still in the programme as part of different incentives. Key variables included;
Financial (salary, hardship allowance, and top-up) and non-financial incentives.
Three methods of data analysis were applied in this study. Qualitative data was managed and
analyzed in descriptive form as well as use of NVIVO software. Quantitative data was processed
using SPSS. Findings have been presented in form of tables, charts, graphs and percentages.
24
CHAPTER FOUR: FINDINGS
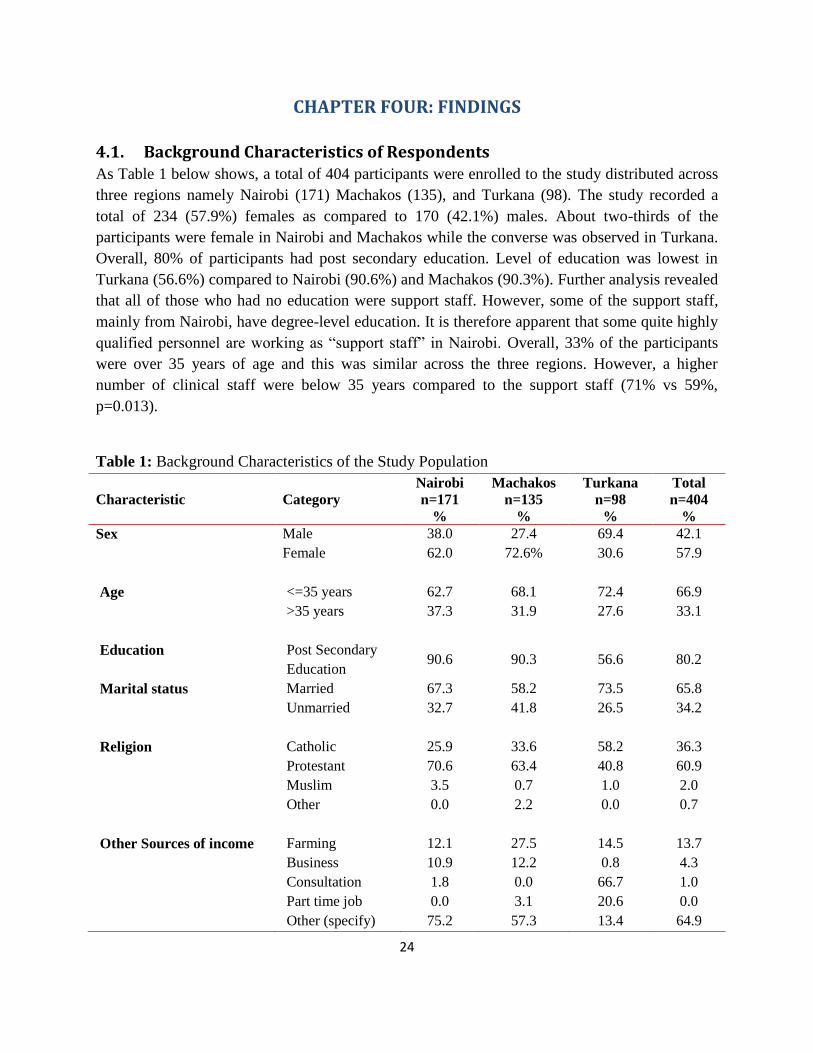
4.1. Background Characteristics of Respondents As Table 1 below shows, a total of 404 participants were enrolled to the study distributed across
three regions namely Nairobi (171) Machakos (135), and Turkana (98). The study recorded a
total of 234 (57.9%) females as compared to 170 (42.1%) males. About two-thirds of the
participants were female in Nairobi and Machakos while the converse was observed in Turkana.
Overall, 80% of participants had post secondary education. Level of education was lowest in
Turkana (56.6%) compared to Nairobi (90.6%) and Machakos (90.3%). Further analysis revealed
that all of those who had no education were support staff. However, some of the support staff,
mainly from Nairobi, have degree-level education. It is therefore apparent that some quite highly
qualified personnel are working as “support staff” in Nairobi. Overall, 33% of the participants
were over 35 years of age and this was similar across the three regions. However, a higher
number of clinical staff were below 35 years compared to the support staff (71% vs 59%,
p=0.013).
Table 1: Background Characteristics of the Study Population
Characteristic
Category
Nairobi
n=171
%
Machakos
n=135
%
Turkana
n=98
%
Total
n=404
%
Sex Male 38.0 27.4 69.4 42.1
Female 62.0
72.6%
30.6
57.9
Age <=35 years 62.7 68.1 72.4 66.9
>35 years
37.3
31.9
27.6
33.1
Education Post Secondary
Education 90.6 90.3 56.6 80.2
Marital status Married 67.3 58.2 73.5 65.8
Unmarried
32.7
41.8
26.5
34.2
Religion Catholic 25.9 33.6 58.2 36.3
Protestant 70.6 63.4 40.8 60.9
Muslim 3.5 0.7 1.0 2.0
Other
0.0
2.2
0.0
0.7
Other Sources of income Farming 12.1 27.5 14.5 13.7
Business 10.9 12.2 0.8 4.3
Consultation 1.8 0.0 66.7 1.0
Part time job 0.0 3.1 20.6 0.0
Other (specify) 75.2 57.3 13.4 64.9
25
Thirty four percent of all respondents were unmarried with Turkana having the lowest proportion
of unmarried respondents (26%). Respondents had an average of two living children with
significantly higher proportions observed in Turkana as compared to other sites (3 vs 2 in other
sites, p<0.0001). The majority of the respondents (97%) were Christians and religion did not
differ across public and private/mission owned health facilities. Other sources of income for the
health care workers were farming (14.5%), business (13.7%), consultation (0.8%) and part time
jobs (4.3%). While business was most preferred source of other income in Turkana (21%),
farming was more preferred in Machakos (27%) and Nairobi (12%). Only Nairobi had
consultancy as an alternative source of income (1.8%). As regards other sources of income
beside the salary, farming and business in Nairobi and Machakos are more practiced. However
52% of respondents in the three settings reported that the salary was the major source of income.
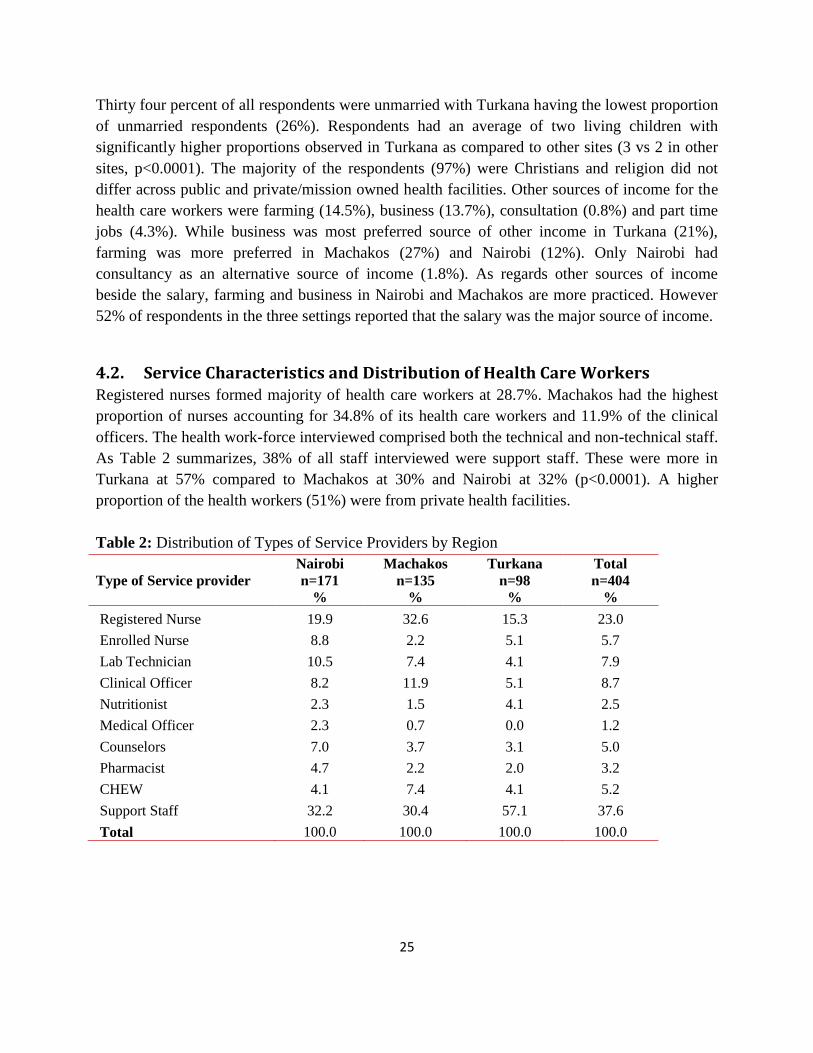
4.2. Service Characteristics and Distribution of Health Care Workers Registered nurses formed majority of health care workers at 28.7%. Machakos had the highest
proportion of nurses accounting for 34.8% of its health care workers and 11.9% of the clinical
officers. The health work-force interviewed comprised both the technical and non-technical staff.
As Table 2 summarizes, 38% of all staff interviewed were support staff. These were more in
Turkana at 57% compared to Machakos at 30% and Nairobi at 32% (p<0.0001). A higher
proportion of the health workers (51%) were from private health facilities.
Table 2: Distribution of Types of Service Providers by Region
Type of Service provider
Nairobi
n=171
%
Machakos
n=135
%
Turkana
n=98
%
Total
n=404
%
Registered Nurse 19.9 32.6 15.3 23.0
Enrolled Nurse 8.8 2.2 5.1 5.7
Lab Technician 10.5 7.4 4.1 7.9
Clinical Officer 8.2 11.9 5.1 8.7
Nutritionist 2.3 1.5 4.1 2.5
Medical Officer 2.3 0.7 0.0 1.2
Counselors 7.0 3.7 3.1 5.0
Pharmacist 4.7 2.2 2.0 3.2
CHEW 4.1 7.4 4.1 5.2
Support Staff 32.2 30.4 57.1 37.6
Total 100.0 100.0 100.0 100.0

26
4.3. Training As can be observed from Table 3 below, 52.8% of professional health workers had at least a
diploma level of training and these were higher in Machakos (55.8%) and Nairobi (52%) than
Turkana (48.2%), p<0.0001. Overall, 55.9% of respondents had attended an upgrading course. A
higher proportion of respondents working in greater Machakos (67.8%) had attended an
upgrading course compared to 52.3% in Nairobi and 40% in Turkana, p=0.014. More than half
of the respondents who had attended an upgrading course did so within the past 12 months. Sixty
seven percent of the participants went to a government institution for their first qualification
while 16.7% and 15.9% did so in a mission and private institution respectively.
Table 3: Training Characteristics of Professional Health Workers
Characteristic
Category
Nairobi
n=100
%
Machakos
n=68
%
Turkana
n=27
%
Total
n=195
%
Highest level of
training
<Diploma
Diploma
28
52
41.2
55.8
48.1
48.2
35.4
52.8
>Diploma 20 3 3.7 11.8
Attended upgrade
course
Yes
(n=111)
52.3
(n=87)
67.8
(n=40)
40
(n=238)
55.9
No 47.7 32.2 60 44.1
4.4. Comparison of Training Factors
A higher proportion of respondents who went to private training institutions also worked for
private institutions 41.9% compared to 22.2% among those trained in Government institutions
(p=0.004). Although the differences were not statistically different, private institutions had a
higher proportion of graduates than those in Government health facilities (12% vs 7.3%,
p=0.393) and had a higher proportion having attended an upgrading course (54.4% vs 53%,
p=0.358).
4.5. Preference for Where to Work
Looking at where the respondents would prefer to work (Figure 1 below) if given an opportunity,
50.9% of the respondents said they would prefer NGOs, 26.9% would prefer Government, 11.7%
out of the country, 6.3% in FBOs and 4.2% in private institutions. The preference to work in
NGOs was higher in Nairobi 56% compared to Machakos 47.8% and Turkana 46.7%. The
preference to work for Government was more common in Turkana 36.7% compared to
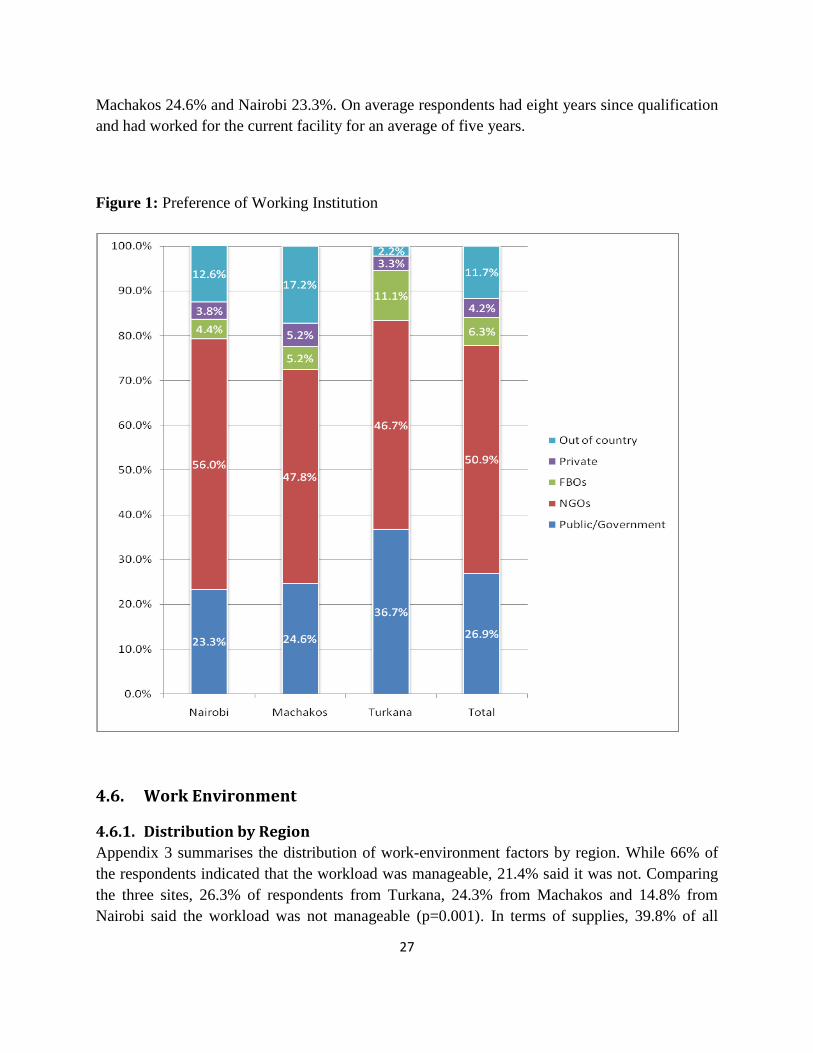
27
Machakos 24.6% and Nairobi 23.3%. On average respondents had eight years since qualification
and had worked for the current facility for an average of five years.
Figure 1: Preference of Working Institution
4.6. Work Environment
4.6.1. Distribution by Region
Appendix 3 summarises the distribution of work-environment factors by region. While 66% of
the respondents indicated that the workload was manageable, 21.4% said it was not. Comparing
the three sites, 26.3% of respondents from Turkana, 24.3% from Machakos and 14.8% from
Nairobi said the workload was not manageable (p=0.001). In terms of supplies, 39.8% of all

28
respondents did not indicate they had enough supplies overall but this was higher in Machakos
44% than Turkana 38.4% and Nairobi 29.2% (P<0.0001). Overall, 73.8% of respondents
indicated that they are allowed to go on leave but this proportion was 62.8% in Machakos, 70.1%
in Turkana and 83.9% in Nairobi (p<0.0001). When asked about their job security, 36.2% of the
respondents indicated they did not feel they had job security. This feeling was more common in
Machakos 45.2% compared to Turkana 28.4% and Nairobi 27.6% (p=0.042). A higher
proportion of respondents in Machakos 38.9% compared to 29.9% in Turkana and 14.6% from
Nairobi indicated that their children did not have access to good schooling (p<0.0001). Access to
safe water at the work place was a bigger problem in Machakos (45.1%) and Turkana (32.3%)
compared to Nairobi (17.6%), (p<0.0001).
4.6.2. Comparison of Work Environment factors by Type of Health Facility
The results in Figure 2 below indicate that in almost all aspects, respondents from private
institutions rated their environment better than those in government.
Figure 2: Comparison of Work Environment Factors by Facility Type

29
Among the most striking differences was adequacy of supplies (76.2% vs 43.1%, p<0.001), good
access to drugs (79.8% vs 57.9%, p<0.0001) and safe and clean water at work places (80.3% vs
57.9%).
4.7. Satisfaction Factors
As the results in Appendix 5 demonstrate, out of all interviewed respondents, 26.8% indicated
they were dissatisfied with their jobs. Although this was 24.5% in Nairobi, 31.1% in Machakos
and 25.2% in Turkana, the difference was not statistically significant (p=0.163). Only 11.1% of
the respondents felt that their supervisors did not provide support and encouragement. This
complaint was most common in Machakos at 12.6%, lesser at 11.3% in Nairobi and least in
Turkana at 9.1% (p=0.430). With respect to receiving training required for the current position,
46.5% of those interviewed felt they had been provided this training. This proportion was highest
in Nairobi at 70.2%, lesser in Machakos 43.7% and least in Turkana 27.3% (p<0.0001).
4.7.1. Satisfaction by Type of Health Facility
The results in Table 4 below show that compared to those working in Government, a higher
proportion of respondents from private institutions indicated they were not sure of what was
expected of them at work (2.4% vs 1.6%, p=0.009). However, morale levels were comparable
between private institutions and government (64% vs 63%). However, respondents working in
government institutions were less likely to encourage friends to seek care at their place of work
compared to those in private institutions (76.5% vs 80%, p=0.0045). Respondents from private
institutions were more likely to enjoy their work than those in government (56.2% vs 51.1%,
p=0.0037).

30
Table 4: Satisfaction Factors that differed across Facility Types
GoK
n=189
%
Private/NGO
n=211
%
p-value
When I come to work, I
know what is expected
of me
Strongly disagree 0.5 0.0 0.009
Disagree 1.1 2.4
Neutral 12.7 17.5
Agree 42.9 25.9
Strongly Agree 42.9 53.8
I find my work at this
facility to be enjoyable
Strongly disagree
2.6
5.2
0.037
Disagree 15.9 8.1
Neutral 30.2 28.4
Agree 34.9 33.6
Strongly Agree 16.4 24.6
I would encourage my
friends and family to
seek care here
n=166
%
n=180
%
Strongly disagree 4.2 2.8 0.045
Disagree 6.6 3.9
Neutral 12.7 13.3
Agree 42.8 31.1
Strongly Agree 33.7 48.9
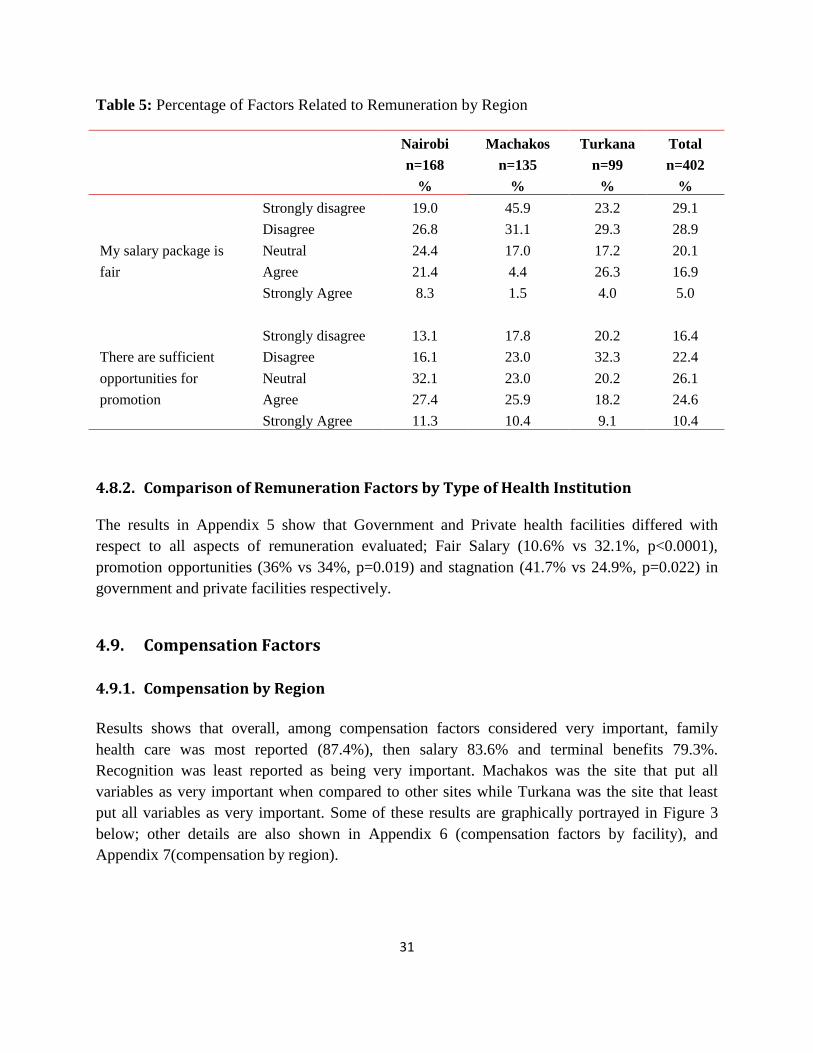
4.8. Remuneration
4.8.1. Distribution of Remuneration Factors by Region
Table 5 below shows that among the respondents, 21.9% agreed that their salary package was
fair. Turkana had the highest proportion of those agreeing that salary was fair at 30.3% followed
by Nairobi at 29.7% while Machakos had the lowest at 5.9% (p<0.0001). In terms of promotion
opportunities, 35% felt there were sufficient opportunities for this. This proportion was highest
in Nairobi at 38.7%, then Turkana at 27.3% and lowest in Machakos at 26.3% (p=0.039). While
39.5% felt there was no stagnation in their organizations, this proportion differed across sites –
Nairobi 33.2%, Machakos 36.6% and 55.6% in Turkana (p=0.016).
31
Table 5: Percentage of Factors Related to Remuneration by Region
Nairobi
n=168
%
Machakos
n=135
%
Turkana
n=99
%
Total
n=402
%
My salary package is
fair
Strongly disagree 19.0 45.9 23.2 29.1
Disagree 26.8 31.1 29.3 28.9
Neutral 24.4 17.0 17.2 20.1
Agree 21.4 4.4 26.3 16.9
Strongly Agree
8.3 1.5 4.0 5.0
There are sufficient
opportunities for
promotion
Strongly disagree 13.1 17.8 20.2 16.4
Disagree 16.1 23.0 32.3 22.4
Neutral 32.1 23.0 20.2 26.1
Agree 27.4 25.9 18.2 24.6
Strongly Agree 11.3 10.4 9.1 10.4
4.8.2. Comparison of Remuneration Factors by Type of Health Institution
The results in Appendix 5 show that Government and Private health facilities differed with
respect to all aspects of remuneration evaluated; Fair Salary (10.6% vs 32.1%, p<0.0001),
promotion opportunities (36% vs 34%, p=0.019) and stagnation (41.7% vs 24.9%, p=0.022) in
government and private facilities respectively.
4.9. Compensation Factors
4.9.1. Compensation by Region
Results shows that overall, among compensation factors considered very important, family
health care was most reported (87.4%), then salary 83.6% and terminal benefits 79.3%.
Recognition was least reported as being very important. Machakos was the site that put all
variables as very important when compared to other sites while Turkana was the site that least
put all variables as very important. Some of these results are graphically portrayed in Figure 3
below; other details are also shown in Appendix 6 (compensation factors by facility), and
Appendix 7(compensation by region).

32
Figure 3: Importance of Compensation Factors
4.10. Job Stability
Overall, 13% of health workers had changed jobs in the last one year. Figure 4 below shows that
the proportion of health care workers changing jobs was comparable in Machakos (15.6%) and
Nairobi (15%) but lower in Turkana at 6.1%.
Figure 4: Proportion of Professional HCW who Changed Jobs in the last year by Region
33
A higher proportion of those who changed jobs were professional health workers (85.7%) as
compared to support staff (14.3%). The results also show that among the professional health
workers, proportions are higher among registered nurses, and support staff. In both cases, these
people are based in Nairobi and Machakos and a very small proportion from Turkana
4.10.1. Factors in Leaving Previous Job
Respondents were requested to comment on several factors in leaving a job. The results are
shown in Appendix 4. Overall, 64% of those interviewed explained that low salary and
allowances are very important factors in leaving their jobs. This percentage was greatest in
Greater Machakos (77%), 68% in Turkana and least in Nairobi (47%). A similar pattern is
observed in the regions with regard to a number of other factors such as poor access to supplies
and equipment; limited opportunities for promotion; poor utilities; communication problems;
educational facilities; job security.
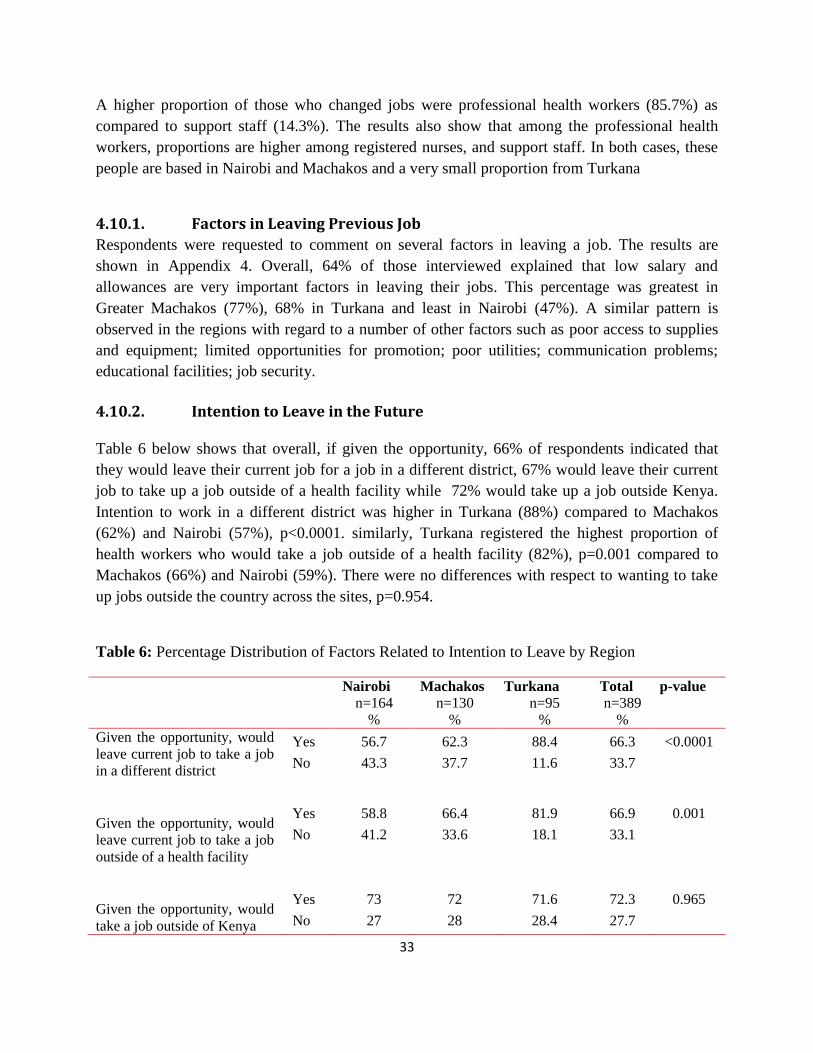
4.10.2. Intention to Leave in the Future
Table 6 below shows that overall, if given the opportunity, 66% of respondents indicated that
they would leave their current job for a job in a different district, 67% would leave their current
job to take up a job outside of a health facility while 72% would take up a job outside Kenya.
Intention to work in a different district was higher in Turkana (88%) compared to Machakos
(62%) and Nairobi (57%), p<0.0001. similarly, Turkana registered the highest proportion of
health workers who would take a job outside of a health facility (82%), p=0.001 compared to
Machakos (66%) and Nairobi (59%). There were no differences with respect to wanting to take
up jobs outside the country across the sites, p=0.954.
Table 6: Percentage Distribution of Factors Related to Intention to Leave by Region
Nairobi
n=164
%
Machakos
n=130
%
Turkana
n=95
%
Total
n=389
%
p-value
Given the opportunity, would
leave current job to take a job
in a different district
Yes
No
56.7
43.3
62.3
37.7
88.4
11.6
66.3
33.7
<0.0001
Given the opportunity, would
leave current job to take a job
outside of a health facility
Yes
No
58.8
41.2
66.4
33.6
81.9
18.1
66.9
33.1
0.001
Given the opportunity, would
take a job outside of Kenya
Yes
No
73
27
72
28
71.6
28.4
72.3
27.7
0.965

34
4.11. Factors Affecting Health Worker Motivation
Using Bivariate logistic regression, workload with an odds ratio of 5 (OR=5.062; CI=2.128 -
12.044) and Salary with Odds ratio of 13(OR=13.492; CI=4.315- 42.185) were the two
statistically significant factors that were found to affect job satisfaction which is a measure of
Motivation. The confidence intervals were however too wide to consider salary as statistically
significant. Hence, a larger sample size may be required in subsequent studies.
4.12. Factors Affecting Health Worker Retention
The duration health workers would stay in their current employment was measured against
several predictors using multinomial logistic regression. The factor that was of statistical
significance was: Salary with p value of 0.008.
4.13. Insights from Qualitative Interviews
The results from the qualitative interviews elaborated in table 10 reveal the following aspects:
i. Several partners are involved in hiring of HCWs:
a. Turkana: AMREF, Merlin, GOK/ESP/Capacity K, AIC, IRC; Kibera: AMREF,
NCC, Private; Machakos: mainly GoK
ii. Getting a job in Turkana is a strategy for gaining GoK employment with an intention to
move out to other regions later
iii. Inadequate staff, transport, inadequate supportive supervision, essentials (gloves)
contribute to dissatisfaction of HCWs
iv. Lack of housing, payment of support staff, physical state of health facilities contribute to
non-conducive environment for HCWs
v. Allowances (hardship, marriage, overtime), rest and recuperation are important
vi. Gender balance in nursing staff, cultural issues critical

35
Table 7: Summary of Thematic Issues Emanating from FGDs in the Three Regions
Kibera Machakos Turkana
1-Positive issues
about the current
work environment
General satisfaction with salary, and
job security
Positive response from patients Good connections, relations with the
community
2-Limitations Discrimination in training, Poor
Communication from superiors on Job
assignments; Tribalism.
Low/substandard housing, quality of
accommodation.
Limited choices for education facilities
for children of staff; language barrier
especially for non locals, unreliable
transport to work and lack of electricity.
3-Reasons for
leaving job
Stagnation on current job, rivalry
between different job cadres
especially between Clinical Officers
and Nurses
Poor commuter allowance, Huge
workload; Government bureaucracy (lack
of commodities and other supplies)
Harsh geographical and climatic
conditions
4-Retention: What
would keep you in
your job?
Regular training; good supervision Better salaries, on-the- job training; more
staff to support high workload
Hardship allowances; better
accommodation and infrastructure.
5-Compensation
factors
Increase allowances (medical, house,
overtime and leave allowances)
Need to increase salaries and to pay
salaries on time;
Lack of NSSF and retirement benefits
(For Private facilities);
6-Gender issues at
work
Increase duration of maternity leave Not very vocal on gender issues, though a
few muted voices of females felt that need
to increase duration of maternity leave
Men require paternity leave
7-Cultural issues Men control family planning and
especially reproductive health issues
sometimes to the detriment of women
A significant number of people believe in
witchcraft and use herbs and charms to
treat diseases
Women do not easily allow male nurses
to attend to them; Women are
encouraged to give birth in standing
position; New mothers do not breastfeed
for a while if they give birth at night.
8-Organizational
support
Multiple reporting lines and
supervision make it difficult to
coordinate work
In-charges are often significantly older
than those they supervise and do not fully
appreciate their younger colleagues.
Staff are committed to work in hardship
conditions
9- other comments Training should be based on
experiences and qualifications
Employ and deploy more staff

36
CHAPTER FIVE: DISCUSSIONS, RECOMMENDATIONS AND CONCLUSIONS
5.1. Summary of Findings
The general objective of this study was to analyse the critical factors which are related to the
motivation and retention of health workers at the primary level in three different settings in
Kenya. Related to this, the three specific objectives of the study are to determine important
themes underling motivation and retention in the three settings; explore the association between
individual, motivation and retention factors and the three settings; determine the relationship
between identified factors and motivation as well as retention. Below we summarise the findings
of the study with regard to these specific objectives.
Individual characteristics: Education and gender factors were lowest in Turkana compared
to Kibera and Machakos. There are more male health workers in Turkana than females.
Nationally, females are estimated to make up 50% of health workers compared to just 30% in
Turkana. This imbalance has cultural implications in the delivery of services.
Training. A smaller proportion of health workers in Turkana feel they have adequate
training for their jobs. This correlates with the findings on the low levels of education and
upgrading opportunities noted in Turkana. In the Uganda workforce study, health workers
disclosed that training was a significant reward and motivator.
Job stability: Overall, 13% had changed jobs in the last 12 months before the survey and
20% indicated that they could leave their current job within two years. Attrition rates are
highest in Machakos and Nairobi compared to Turkana. However a higher proportion of
health workers in Turkana would leave the job for another district signifying lower levels of
satisfaction and poor working conditions. This is similar to a study on motivation of health
workers in Uganda in which 20% indicated that they could leave within three years. In
Uganda however, the average number of years spent in the job was much higher than that
observed in this study. In Uganda, the average years of stay was ten years compared to five
years in Kenya. This was attributed to the high status accorded to health sector jobs, as well
as stable and reasonable compensation. Satisfaction among health workers is also correlated
with motivation. The study findings also indicate that salary is an important predictor of
health worker retention.
Working conditions: Inadequate access to electricity, equipment and transport most critical
in Turkana, as expected. Lack of housing, payment of support staff, physical state of the
health facility contribute to non-conducive environment for health workers. More than 30%
of health workers do not feel they have job security. A higher proportion of health workers in
Turkana feel their work load is not manageable. This could be related to the inadequate staff

37
in Turkana as observed in the findings. Working environment in the private facilities is rated
higher than that in government facilities.
Satisfaction: Satisfaction levels are considerably low among health workers in the three
regions. Inadequate staff, transport, inadequate supportive supervision, essentials (gloves)
contribute to dissatisfaction. Allowances (hardship, marriage, over-time), rest and
recuperation are also important aspects of satisfaction. Just as in the Uganda Workforce
study, this study identified adequate training, job security, salary, supervisor support and
manageable workload as critical satisfaction factors.
Remuneration: Remuneration is a critical factor of motivation and retention. A higher
proportion of health staff however feel their remuneration is not fair. This is highest in
Machakos district which also records the highest attrition rate. Opportunities for promotion
or career growth are key element of motivation.
Importance of compensation factors: Family health care, salary, and terminal benefits are
important compensation factors that are closely linked to motivation and retention. Health
workers place emphasis on family care; compensation is highly regarded if it has direct
benefit to dependants. Health care to families is even rated higher than salary among health
workers.
5.1.2. Relating Findings to the HRH Strategic Plan The findings of this study resonate well with the Kenya HRH strategic plan, 2009-2012.
Specifically, they relate directly to the second outcome - improving attraction and retention of
health workers. The two strategic objectives under this outcome are: 1) Making health sector
jobs more attractive; 2) Making hard to reach stations more attractive. Health sector jobs may
not be currently very attractive, with the majority of health workers preferring to be in the NGO
sector. This may be related with working conditions in health facilities, low satisfaction that
includes inadequate training and issues to do with remuneration packages. Hard-to-reach areas
such as Turkana are least attractive sites to work in with the majority of health staff indicating
desire to work in different districts. Health workers in these regions are more susceptible to
poorer working conditions compared to other regions. Satisfaction levels are lower in hard-to-
reach regions since majority of staff often miss out on training opportunities leaving them feeling
less equipped for their job. Furthermore, hard-to-reach areas such as Turkana record the lowest
number of health workers and levels of education. Incidentally, these are the regions with some
of the worst health indicators such as maternal and child mortality. With constant improvement
in health delivery packages, it is paramount that equity is exercised in training opportunities to
ensure hard-to-reach regions are adequately covered.
The HRH strategic plan outlines six strategies meant to improve attraction and retention of health
workers. These are: conduct periodic review of compensation packagers; lobby for improved

38
staff welfare; improve work climate; explore options for retention schemes; review and
disseminate schemes of service; develop and implement retention packages. The extent to which
these strategies are being or have been implemented remains unclear.
5.1.3. Policy Implications of the findings:
Individual characteristics: Gender imbalance exists in Turkana with more male health
workers in the district. Whereas this may be as a result of the harsh conditions that are
deemed unfavorable to women, this imbalance has cultural implications in the delivery of
services. One of the issues that women have cited for low skilled delivery (in health
facilities) includes unwillingness to be examined and delivered by a man. With more than
70% of health workers being male, cultural inhibitions are bound to continue. The observed
gender imbalance has policy implications on recruitment particularly in the hard-to-reach
regions.
Education and Training. A smaller proportion in Turkana feel they have adequate training
for their jobs. This compares to the low levels of education noted among health workers in
Turkana. Lower levels of education and inadequate opportunities for upgrading has potential
implications on the motivation of health workers in Turkana as majority feel they are not
adequately prepared for their tasks. Health workers consider training as a significant reward
and motivator. Inadequate skills among health workers therefore not only affects quality of
services provided, but has direct implications on the motivation and retention of health
workers. Education is identified as the fifth aspect of HRM systems in the HRH action
framework with a focus on maintaining a skilled workforce. A comprehensive and equitable
continuous training programme for health workers is therefore imperative.
Job stability: Previous studies have established a link between intent to leave and staff
turnover. This implies a staff turnover of about 20% within the next two years due to
resignations alone. Health workers are likely to move from government to NGOs, private
facilities and out of the country in search for better working environment.
Job satisfaction: Job satisfaction has been found to be predictive of staff turnover. This
means that motivation and retention factors when addressed in isolation may not
comprehensively address the high attrition rates.
Working conditions: Inadequate working conditions coupled with low job satisfaction and
stability are bound to de-motivate health workers and impact retention.
Compensation: The majority of health workers are in their mid-years and married with
children. Compensation to them transcends individual interest to include greater benefits for
dependants. This has potential policy implications on recruitment and compensation.

39
Model HRH community. Last but by no means least, the important insight one learns from
these findings is that there is need to demonstrate that addressing HRH issues such as those
related to the work environment and employee satisfaction works, and that indeed there are
solutions. Unlike the current practice where the focus is on the increase in the number of
service providers per population, there is need to link increased investment in human
resources for health to increased productivity and performance. As more health service
providers are recruited for each health facility, we should be able to see a corresponding
improvement in health indicators in the catchment of the facility.
5.2. Recommendations 1. Conduct in-depth but rapid review of gender dynamics in the primary health care facilities in
Turkana County in particular and the other regions as well; develop and implement gender
mainstreaming strategies in the facilities to address the health issues identified in this study.
2. Develop and implement tailor-made training package and strategies for hard-to-reach areas
like Turkana to address training gaps identified in this study. Above all, develop
comprehensive and equitable continuous training programmes for health workers in hard-to-
reach regions.
3. Develop and apply retention schemes specific to the three respective regions
4. Address job satisfaction factors such as adequate staff numbers, supervision, basic equipment
in the hard to reach areas in particular.
5. Tackle issues related to working conditions such as energy supply, equipment, and housing
in Turkana and Machakos regions in particular.
6. Decentralise HRH management system to the regions to address issues specific to regions
7. Develop competitive compensation packages for health staff particularly in hard to reach
areas to include family health care. These should be regularly reviewed to address changing
needs.
8. Develop strategies for career growth and promotion especially for higher cadre of health
workers such as doctors.
9. Develop and market a proposal to establish a model “HRH community” within selected
NGO/FBO health facilities in hard to reach areas.

40
5.3. Conclusion The findings from this study indeed confirm distinct issues related to motivation and retention in
each of the three settings that the study was conducted in. Secondly, motivation and retention in
the three regions is associated with particular background characteristics of health workers.
Thirdly, results of this study show that salary is an important predictor of motivation and
retention of health workers. Lastly, insights from this study show that there are solutions to HRH
issues such as those related to employee satisfaction and work environment. At least two current
national processes should be the focus of attention in the light of the findings and
recommendations of this study. These are the review of the Kenya HRH Strategic Plan and the
devolution to County Governments. The findings from this study should be used to strengthen
HRH systems in the proposed county governments (under the new constitution) to motivate and
retain health care workers in the respective counties. Findings should also be used in the review
of the national HRH Strategic Plan.
41
REFERENCES AND BIBLIOGRAPHY
Andrew A. Fisher, J. E. L., John.E.Stoekel, John.W.Townsend. 1998. Handbook for Family Planning
Operations Research Design. Population Council.
Barnighausen, T., & Bloom, D. 2009. Designing financial-incentive programmes for return of medical
service in underserved areas: seven management functions. Human Resources for Health, 7(1):
52.
Brugha, R., Kadzandira, J., Simbaya, J., Dicker, P., Mwapasa, V., & Walsh, A. 2010. Health workforce
responses to global health initiatives funding: a comparison of Malawi and Zambia. Human
Resources for Health, 8(1): 19.
Buchan, J. 2010. Reviewing The Benefits of Health Workforce Stability. Human Resources for Health,
8(1): 29.
Buchan, J., Fronteira, I., & Dussault, G. 2011. Continuity and change in human resources policies for
health: lessons from Brazil. Human Resources for Health, 9(1): 17.
Castillo-Laborde, C. 2011. Human resources for health and burden of disease: an econometric approach.
Human Resources for Health, 9(1): 4.
Chankova, S., Muchiri, S., & Kombe, G. 2009. Health workforce attrition in the public sector in Kenya: a
look at the reasons. Human Resources for Health, 7(1): 58.
Dambisya, Y. M. 2007. A review of non-financial incentives for health worker retention in east and
southern Africa. EQUITNET, ECSA-HA.
Dieleman, M., Shaw, D., & Zwanikken, P. 2011. Improving the implementation of health workforce
policies through governance: a review of case studies. Human Resources for Health, 9(1): 10.
Fauveau, V., Sherratt, D., & de Bernis, L. 2008. Human resources for maternal health: multi-purpose or
specialists? Human Resources for Health, 6(1): 21.
Gonzalo Urcullo, J. V. V., Carlos Ricse y Camilo Cid. 2008. Health Worker Salaries and Benefits:
Lessons from Bolivia, Peru
and Chile.
Hirschhorn, L., Oguda, L., Fullem, A., Dreesch, N., & Wilson, P. 2006. Estimating health workforce
needs for antiretroviral therapy in resource-limited settings. Human Resources for Health, 4(1):
1.
Kennedy, P. 2003. A Guide to Econometrics. MIT Press.
Kent Ranson, T. J. L., Sara Bennett. 2010. Establishing health systems financing research priorities in
developing countries
42
using a participatory methodology. Social Science & Medicine.
Kmenta, J. 1997. Elements of Econometrics,. University of Michigan Press.
Kruse, G., Chapula, B., Ikeda, S., Nkhoma, M., Quiterio, N., Pankratz, D., Mataka, K., Chi, B., Bond, V.,
& Reid, S. 2009. Burnout and use of HIV services among health care workers in Lusaka District,
Zambia: a cross-sectional study. Human Resources for Health, 7(1): 55.
Lehmann, U., Dieleman, M., & Martineau, T. 2008. Staffing remote rural areas in middle- and low-
income countries: A literature review of attraction and retention. BMC Health Services
Research, 8(1): 19.
Manafa, O., McAuliffe, E., Maseko, F., Bowie, C., MacLachlan, M., & Normand, C. 2009. Retention of
health workers in Malawi: perspectives of health workers and district management. Human
Resources for Health, 7(1): 65.
Mario A.Cleves, W. W. G., and Roberto G. Gutierrez. 2002. An Introduction to Survival Analysis Using
Stata. The Stata Journal
Mathauer, I., & Imhoff, I. 2006. Health worker motivation in Africa: the role of non-financial incentives
and human resource management tools. Human Resources for Health, 4(1): 24.
Mbindyo, P., Blaauw, D., Gilson, L., & English, M. 2009. Developing a tool to measure health worker
motivation in district hospitals in Kenya. Human Resources for Health, 7(1): 40.
Mbindyo, P., Gilson, L., Blaauw, D., & English, M. 2009. Contextual influences on health worker
motivation in district hospitals in Kenya. Implementation Science, 4(1): 43.
McAuliffe, E., Bowie, C., Manafa, O., Maseko, F., MacLachlan, M., Hevey, D., Normand, C., & Chirwa,
M. 2009. Measuring and managing the work environment of the mid-level provider - the
neglected human resource. Human Resources for Health, 7(1): 13.
Mudhune, S. 2009. Identifying policies to improve nurse recruitment and retention in rural Kenya:
Results of a discrete choice experiment. Researching interventions to address the human
resources for health crisis - an application of discrete choice experiments in Kenya, Thailand
and South Africa.
Mullei, K., Mudhune, S., Wafula, J., Masamo, E., English, M., Goodman, C., Lagarde, M., & Blaauw, D.
2010. Attracting and retaining health workers in rural areas: investigating nurses' views on rural
posts and policy interventions. BMC Health Services Research, 10(Suppl 1): S1.
Ndetei, D., , F. O., , V. M., , M. K., , L. K., & , D. K. 2007. The challenges of human resources
in mental health in Kenya. African Journal online(10): 33-36.
Newman, C., de Vries, D., d'Arc Kanakuze, J., & Ngendahimana, G. 2011. Workplace violence and
gender discrimination in Rwanda's health workforce: Increasing safety and gender equality.
Human Resources for Health, 9(1): 19.
43
O'Neil, M. L. 2008. Human Resource Leadership:the Key to Improved Results in Health. Human
Resources for Health.
Ojakaa, D. 2008. Trends and Determinants of Unmet Need for Family Planning in Kenya. Demographic
and Health Research. DHS Working Paper No. 56, Macro International Inc. USAID
MEASURE DHS Project. .
Olang'o, C. O., Nyamongo, I. K., & Aagaard-Hansen, J. 2010. Staff attrition among community health
workers in home-based care programmes for people living with HIV and AIDS in western Kenya.
Health Policy, 97(2-3): 232-237.
Peters, D., Chakraborty, S., Mahapatra, P., & Steinhardt, L. 2010. Job satisfaction and motivation of
health workers in public and private sectors: cross-sectional analysis from two Indian states.
Human Resources for Health, 8(1): 27.
Proper, K., Deeg, D., & Beek, A. 2009. Challenges at work and financial rewards to stimulate longer
workforce participation. Human Resources for Health, 7(1): 70.
Republic of Kenya. 2010. National Human Resources for Health Annual report.
Rolfe, B., Leshabari, S., Rutta, F., & Murray, S. F. 2008. The crisis in human resources for health care
and the potential of a „retired‟ workforce: case study of the independent midwifery sector in
Tanzania. Health Policy and Planning, 23(2): 137-149.
Rowe, S. Y., Kelly, J. M., Olewe, M. A., Kleinbaum, D. G., McGowan, J. J. E., McFarland, D. A.,
Rochat, R., & Deming, M. S. 2007. Effect of multiple interventions on community health
workers' adherence to clinical guidelines in Siaya district, Kenya. Transactions of the Royal
Society of Tropical Medicine and Hygiene, 101(2): 188-202.
Snow, R., Asabir, K., Mutumba, M., Koomson, E., Gyan, K., Dzodzomenyo, M., Kruk, M., & Kwansah,
J. 2011. Key factors leading to reduced recruitment and retention of health professionals in
remote areas of Ghana: a qualitative study and proposed policy solutions. Human Resources for
Health, 9(1): 13.
Spero, J., McQuide, P., & Matte, R. 2011. Tracking and monitoring the health workforce: a new human
resources information system (HRIS) in Uganda. Human Resources for Health, 9(1): 6.
The First Global Forum on Human Resources for Health. 2008. Health Workers for all and all for Health
Workers. Global Health Workforce Alliance.
Tjoa, A., Kapihya, M., Libetwa, M., Schroder, K., Scott, C., Lee, J., & McCarthy, E. 2010. Meeting
human resources for health staffing goals by 2018: a quantitative analysis of policy options in
Zambia. Human Resources for Health, 8(1): 15.
Tulloch, L. N. H. a. J. 2008. Incentives for Retaining and Motivating Health Workers in Pacific na Asian
Countries. Human Resources for Health.

44
Varpilah, S. T., Safer, M., Frenkel, E., Baba, D., Massaquoi, M., & Barrow, G. 2011. Rebuilding human
resources for health: a case study from Liberia. Human Resources for Health, 9(1): 11.
Vian, T., Richards, S., McCoy, K., Connelly, P., & Feeley, F. 2007. Public-private partnerships to build
human capacity in low income countries: findings from the Pfizer program. Human Resources
for Health, 5(1): 8.
Willis-Shattuck, M., Bidwell, P., Thomas, S., Wyness, L., Blaauw, D., & Ditlopo, P. 2008. Motivation
and retention of health workers in developing countries: a systematic review. BMC Health
Services Research, 8(1): 247.
Wonnacott, W. a. 1995. Statistique: Economie-Gestion-Sciences-Medicine (avec exercises d‟application).
. ECONOMICA. 49, rue Héricat. 75015 Paris, Traduction du livre publié par John Wiley and
Sons New York.
WHO (2007). Everybody‟s Business: strengthening health systems to improve health outcomes: WHO‟s
framework for action. NLM classification: W 84.3. Available at www.who.int/healthsystems/strategy/
everybodys_business.pdf
World Health Organization, 2008.The World Health Report, 2008 – primary health care (Now more than
ever).World health Organization, Geneva.
Zurn, P., Vujicic, M., Lemiere, C., Juquois, M., Stormont, L., Campbell, J., Rutten, M., & Braichet, J.-M.
2011. A technical framework for costing health workforce retention schemes in remote and rural
areas. Human Resources for Health, 9(1): 8.

45
APPENDIXES
APPENDIX 1: List of Health Facilities Visited
Kibera Machakos
Turkana
Nairobi South Medical
Centre
1 Kalama dispensary 1 Jawabu Medical Clinic
2 Uhuru camp medical centre 2 St Michael Catholic
Dispensary
2 AIC Health Centre
3 AMREF Kibera 3 Muumandu Health Centre 3 Kakuma Mission Hospital
4 Langata Women Prison 4 Kaani sub health 4 Makutano Model Health
5 Karen Health Centre 5 Ithaeni Dispensary 5 Kanakurudio
7 Dreams Centre 6 Family care clinic 6 Kaeris Health Facilities
9 Lang‟ata Health centre 7 Tunawanjali clinic 7 Kaaleng Dispensary
10 MSF Kibera South 8 Mbiuni Health Centre 8 Kaikor Health Center
11 Kibera D.O 9 Mwala District Hospital 9 Koyasa
12 Family health options 10 Approved School Dispensary 10 Lorus Dispensaries
13 Tabitha Medical clinic 11 Kimutwa Dispensary 11 Lokitaung District Hospital
14 Ushirika Medical clinic 12 APDK Dispensary 12 Lokitaung District Hospital
15 Frepals Nursing home 13 Mutituni Dispensary 13 Oropoi Dispensary.
16 Silanga Dispensary 14 St. Assisi Sisters of Mary
Immaculate Nursing Home
14 AIC Health Centre
18 Saola-managed 15 Nzaikoni Sacred Heart
Dispensary 19 Lea Toto community center 16 Mitaboni Health center 20 Family Health Options 17 Kaviani Dispensary 21 Kibera D.O 18 Wamunyu Health Centre 22 AMREF Kibera 19 Masii Health Centre

46
APPENDIX 2: Survey Instruments
QUESTIONNAIRE
SERVICE PROVIDER
Title of the Study: Motivation and Retention of Health Workers in Three Kenyan Settings
Module I: Identification
101. County: ……………………………………………………………………….
102. District: ………………………………………………………………………..
103. Division: ………………………………………………………………………..
104. Facility Name: ………………………………………………………………………
105. Type of Service provider:…………………………………..………………...
(Nurse – Specify level, lab technician, clinical officer, CHEW, nutritionist, morgue assistant, driver)
106. Job title: ……………………………………………………………………..……..
FOR OFFICIAL USE ONLY
Questionnaire No.
Date Checked.
Interviewer Code.
Supervisor Code.
Date of Interview.
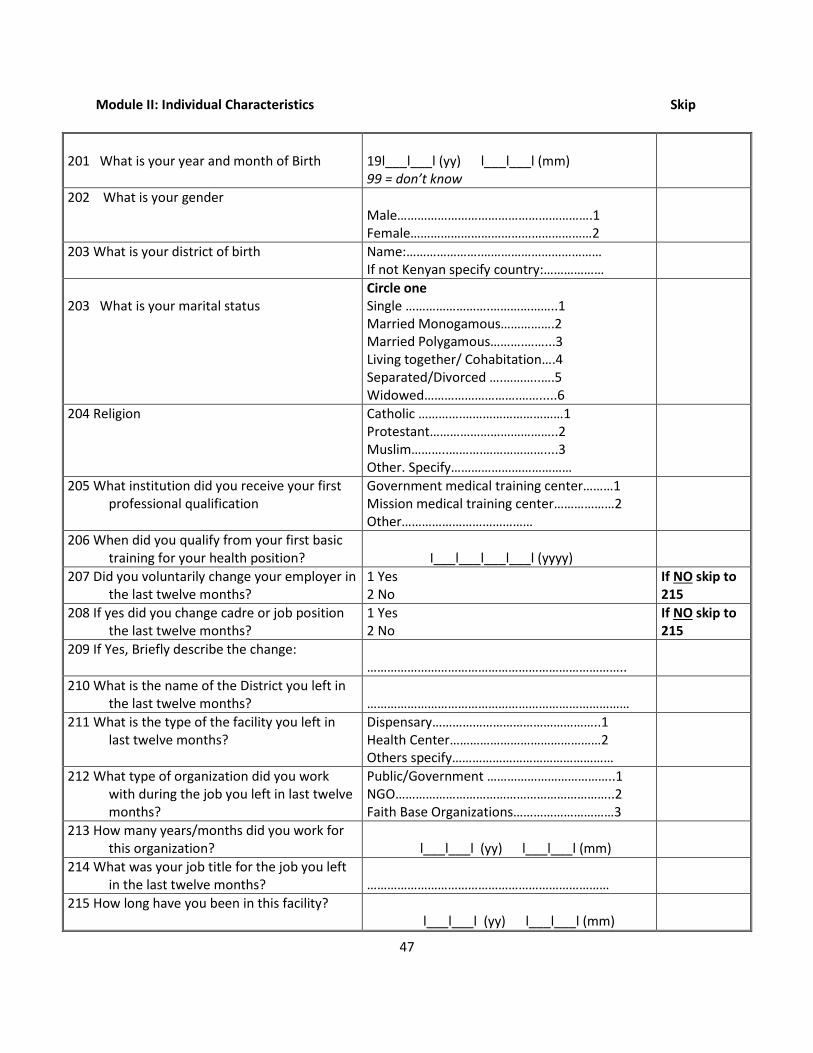
47
Module II: Individual Characteristics Skip
201 What is your year and month of Birth
19l___l___l (yy) l___l___l (mm) 99 = don’t know
202 What is your gender Male………………………………………………….1 Female………………………………………………2
203 What is your district of birth Name:………………….……………………………… If not Kenyan specify country:………………
203 What is your marital status
Circle one Single …………………….………………..1 Married Monogamous…………….2 Married Polygamous……….……...3 Living together/ Cohabitation….4 Separated/Divorced ….………..….5 Widowed……………………….…….....6
204 Religion Catholic ………….…………………………1 Protestant………………………………..2 Muslim………..……….………………....3 Other. Specify………………………………
205 What institution did you receive your first professional qualification
Government medical training center………1 Mission medical training center………………2 Other…………………………………
206 When did you qualify from your first basic training for your health position?
I___l___l___l___l (yyyy)
207 Did you voluntarily change your employer in the last twelve months?
1 Yes 2 No
If NO skip to 215
208 If yes did you change cadre or job position the last twelve months?
1 Yes 2 No
If NO skip to 215
209 If Yes, Briefly describe the change: …………………………………………………………………..
210 What is the name of the District you left in the last twelve months?
……………………………………………………………………
211 What is the type of the facility you left in last twelve months?
Dispensary…………………………………………..1 Health Center………………………………………2 Others specify…………………………………………
212 What type of organization did you work with during the job you left in last twelve months?
Public/Government ………………………………..1 NGO………………………………………………………..2 Faith Base Organizations…………………………3
213 How many years/months did you work for this organization?
l___l___l (yy) l___l___l (mm)
214 What was your job title for the job you left in the last twelve months?
………………………………………………………………
215 How long have you been in this facility? l___l___l (yy) l___l___l (mm)

48
16 Highest Level of Education
Circle one None ……………………………………………….…....1 Primary Incomplete …………….………….……..2 Primary Complete……………………………..…..3 Secondary Incomplete ………….……………..4 Secondary Complete ……………….……….……5 Polytechnic/College………………………….……6 Undergraduate…. …………..………………………7 Postgraduate……………………..…………..……..8
217 How many children do you have? l___l___l
218 How many people are there in your household (include all those sleeping in the dwelling for at least three of the last 12 months, including children and adults)?
l___l___l
219 What are the other sources of your income apart from the current job?
Circle one Farming ……………..…………………….1 Business ……………..……………………2 Consultation…………..…………………3 None…………………………………………4 Other (specify)………………………...
If NONE, skip to question 220
220 What proportion of your total income does
your salary comprise?
Circle answer It is the only income …….……………….……..…1 Partially contributes to the household income…………………………………….…………..….2 Largest part of the household income…………………………………….………..…….3
Module III: WORK ENVIRONMENT
The following questions refer to your working conditions at your current facility. Please circle the appropriate response
# To what extent do you agree with the following statement?
5 = Strongly
Agree
4 = Agree
3 = Neutral
2 = Disagree
1 = Strongly disagree
301 The workload is manageable. 5 4 3 2 1
302 I have the supplies I need to do my job well and safely (gloves, needles, bandages, etc).
5 4 3 2 1
303 I have the equipment I need to do my job well and efficiently e.g. ultrasound, x-ray, blood pressure cuffs.
5 4 3 2 1
304 This facility has good access to drugs and medications.
5 4 3 2 1
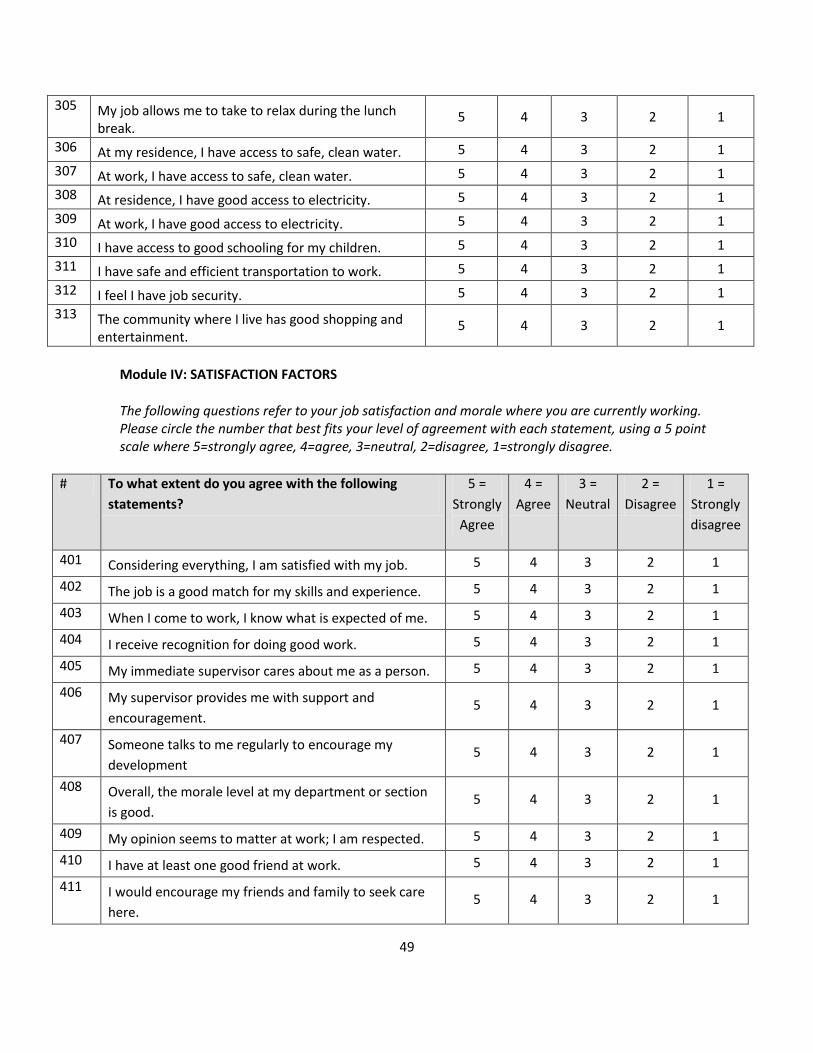
49
305 My job allows me to take to relax during the lunch break.
5 4 3 2 1
306 At my residence, I have access to safe, clean water. 5 4 3 2 1
307 At work, I have access to safe, clean water. 5 4 3 2 1
308 At residence, I have good access to electricity. 5 4 3 2 1
309 At work, I have good access to electricity. 5 4 3 2 1
310 I have access to good schooling for my children. 5 4 3 2 1
311 I have safe and efficient transportation to work. 5 4 3 2 1
312 I feel I have job security. 5 4 3 2 1
313 The community where I live has good shopping and entertainment.
5 4 3 2 1
Module IV: SATISFACTION FACTORS
The following questions refer to your job satisfaction and morale where you are currently working. Please circle the number that best fits your level of agreement with each statement, using a 5 point scale where 5=strongly agree, 4=agree, 3=neutral, 2=disagree, 1=strongly disagree.
# To what extent do you agree with the following
statements?
5 =
Strongly
Agree
4 =
Agree
3 =
Neutral
2 =
Disagree
1 =
Strongly
disagree
401 Considering everything, I am satisfied with my job. 5 4 3 2 1
402 The job is a good match for my skills and experience. 5 4 3 2 1
403 When I come to work, I know what is expected of me. 5 4 3 2 1
404 I receive recognition for doing good work. 5 4 3 2 1
405 My immediate supervisor cares about me as a person. 5 4 3 2 1
406 My supervisor provides me with support and
encouragement. 5 4 3 2 1
407 Someone talks to me regularly to encourage my
development 5 4 3 2 1
408 Overall, the morale level at my department or section
is good. 5 4 3 2 1
409 My opinion seems to matter at work; I am respected. 5 4 3 2 1
410 I have at least one good friend at work. 5 4 3 2 1
411 I would encourage my friends and family to seek care
here. 5 4 3 2 1

50
412 I have flexibility to balance the demands of my
workplace and my personal life. 5 4 3 2 1
413 I find my work at this facility to be enjoyable. 5 4 3 2 1
414 My supervisors are kind to me; they do not verbally,
physically or emotionally abuse me. 5 4 3 2 1
415 My peers are kind to me; they do not verbally,
physically or emotionally abuse me. 5 4 3 2 1
416 My patients and their family members are kind to me;
they do not verbally, physically or emotionally abuse
me.
5 4 3 2 1
417 I have been provided the training needed to succeed in
my position. 5 4 3 2 1
418 The organization takes specific measures to protect me
against HIV/AIDS and TB. 5 4 3 2 1
419 I consider myself a part of this community. 5 4 3 2 1
420 I am fairly evaluated on my work. 5 4 3 2 1
421 The in charge here is competent and committed. 5 4 3 2 1
422 I am actively involved in helping to make this a great
health care facility. 5 4 3 2 1
Module V: Remuneration Package Please indicate your level of agreement with the following questions by marking the appropriate
response with a circle.
# To what extent do you agree with the following statements?
5 = Strongly
Agree
4 = Agree
3 = Neutral
2 = Disagree
1 = Strongly disagree
501 My salary package is fair. 5 4 3 2 1
502 I feel there are sufficient opportunities for promotion with this employer.
5 4 3 2 1
Module VI: Importance of Compensation Factors
Please indicate how important the following compensation factors are for you when choosing a job.
No How important are the following compensation factors offered by an organization to you?
3 = Very
important
2= Somewhat important
1= Not
important
601 Salary. 3 2 1

51
602 Terminal benefits (retirement, pension, etc) 3 2 1
603 Receiving a housing allowance or allocation of a house to stay in.
3 2 1
604 Assistance with transportation. 3 2 1
605 Health care for my family. 3 2 1
606 Hardship allowance or top-up salary. 3 2 1
MODULE VII: Factors in leaving previous job (If still on current job for over 12 months skip to MODULE
VIII)
Please indicate how important the following factors were in your decision to leave your previous job.
# How important were the following factors in your decision to leave your previous job?
3 = Very
important
2= Somewhat important
1= Not
important
701 Low pay/salary/allowances 3 2 1
702 High workload 3 2 1
703 Poor access to supplies & equipment at work 3 2 1
704 Limited opportunities for promotion 3 2 1
705 Social conflicts in the workplace 3 2 1
706 Poor supervision and management 3 2 1
707 Transport problems 3 2 1
708 Poor/lack of utilities (water, electricity) at residence 3 2 1
709 Poor/lack of utilities (water, electricity) at work 3 2 1
710 Lack of housing facilities 3 2 1
711 Communication problems e.g. telephones, internet 3 2 1
712 High cost of living 3 2 1
713 Poor educational facilities for children 3 2 1
714 Poor access to advanced training and education for myself
3 2 1
715 Work is far from home. 3 2 1
716 Other__________________________ 3 2 1
Module VIII: These are open-ended questions about your current work place.
801. Please identify three things that you like about working for this organization:
802. Please identify three things you don’t like about working here:

52
803 Which of the following statements is true for you? 1= I would leave this job as soon as possible. 2= I would leave this job within a year from now. 3= I would leave this job one to two years from now. 4= I would leave this job three to five years from now. 5= I plan to stay in this job indefinitely. 6= Other (Specify): l___l___l years
804 If given the opportunity, would you leave your current job to take a job in a different district?
1=Yes 2=No
805 If given the opportunity, would you leave your current job to take a job outside of a health facility?
1=Yes 2=No
806 If given the opportunity, would you take a job outside of Kenya?
1=Yes 2=No
807. What would you change in this job to help you stay longer?
a. ____________________________________________________________________________
b. ____________________________________________________________________________
c. ____________________________________________________________________________
808. Other comments:
THANK YOU FOR YOUR SUPPORT AND COLLABORATION

53
QUESTIONNAIRE
IN-CHARGE QUESTIONNAIRE
Title of the study: Motivation and Retention of Health Workers in Three Kenyan Settings
Module I: Identification
101. County: ………………………………………………………………………………
102. District: ………………………………………………………………………………
103. Division: ……………………………………………………………………………….
104. Facility Name:……………………………………………………………………………
105. Type of Service provider (In-charge):………………………………………….
(Nurse – Specify level, clinical officer,)
106. Job title: …………………………………………………………………………………
FOR OFFICIAL USE ONLY
Questionnaire No.
Date Checked.
Interviewer Code.
Supervisor Code.
Date of Interview.

54
Module II: Individual Characteristics Skip
201 What is your year and month of Birth
19l___l___l (yy) l___l___l (mm) 99 = don’t know
202 What is your gender Male………………………………………….1 Female………………………………………2
203 What is your district of birth Name:……………………………………… If not Kenyan specify country……………………………………
204 What is your marital status
Circle one Single ………….…………………….……..1 Married Monogamous……………....2 Married Polygamous….……………...3 Living together/ Cohabitation…….4 Separated/Divorced ……………..….5 Widowed……..………..…………….....6
205 Religion Catholic ……………………………..……1 Protestant………………………………..2 Muslim……………..……………….…....3 Other. Specify………………………………
206 What institution did you receive your first professional qualification
Government medical training center……..1 Mission medical training center………………2 Other……………………………………………………….
207 When did you qualify from your first basic training for your health position?
I___l___l___l___l (yyyy)
208 Did you voluntarily change your employer in the last twelve months?
1 Yes 2 No
If NO skip to 216
209 If yes did you change cadre or job position the last twelve months?
1 Yes 2 No(skip)
If NO skip to 216
210 If Yes, Briefly describe the change: ………………………………………………………………..
211 What is the name of the District you left in the last twelve months?
……………………………………………………..
212 What is the type of the facility you left in last twelve months?
Dispensary………..………………..1 Health Center………………………2 Others specify………………………
213 What type of organization did you work with during the job you left in last twelve months?
Public/Government .…………………..1 NGO………………….………………………..2 Faith Base Organizations……………..3
214 How many years/months did you work for this organization?
I___l___l (yy) l___l___l (mm)

55
215 What was your job title for the job you left in the last twelve months?
………………………………………………………….
216 How long have you been in this facility? I___l___l (yy) l___l___l (mm)
217 For how many years have you been the in-charge?
I___l___l (yy)
18 Highest Level of Education
Circle one None ……………..…………………....1 Primary Incomplete ………….…..2 Primary Complete…………….……3 Secondary Incomplete……….…..4 Secondary Complete ……….……5 Polytechnic/College………….……6 Undergraduate ………………….…7 Postgraduate………………..……..8
219 How many children do you have? l___l___l
220 How many people are there in your household (include all those sleeping in the dwelling for at least three of the last 12 months, including children and adults)?
l___l___l
221 What are the other sources of your income apart from the current job?
Circle one Farming ……………………………….1 Business ………………………………2 Consultation…………………………3 None……………………………………4 Other (specify)………………………...
If NONE skip to 222
222 What proportion of your total income does
your salary comprise?
Circle answer It is the only income ……………..……………..…1 Partially contributes to the household income………………………………………………..….2 Largest part of the household income……………………………………………..…….3
Module III: Work Environment in the Facility/District
To what extent do you agree with each of the following statements on the working conditions in the facility? Please circle the appropriate response both “for yourself” and “for employees in your facility.”

56
# To what extent do you agree with the following statement?
For myself For employees in my facility
5 = Strongly
agree
4 = Agree
3= Neutral
2 = Disagree
1 = Strongly disagree
5 = Strongly
agree
4 = Agree
3 = Neutral
2 = Disagree
1 = Strongly disagree
301 The workload is manageable.
5 4 3 2 1 5 4 3 2 1
302 Supplies (gloves, needles, bandages, etc) are available to do our work well.
5 4 3 2 1 5 4 3 2 1
303 The equipment (x-ray, ultrasound, blood pressure cuffs) is available to help us do our jobs well
5 4 3 2 1 5 4 3 2 1
304 There is adequate access to safe, clean water at residence
5 4 3 2 1 5 4 3 2 1
305 Safe, clean water available at work 5 4 3 2 1 5 4 3 2 1
306 Access to electricity is good at residence
5 4 3 2 1 5 4 3 2 1
307 Access to electricity is good at work
5 4 3 2 1 5 4 3 2 1
308 Good schooling is available for the children of the people who work here.
5 4 3 2 1 5 4 3 2 1

57
# To what extent do you agree with the following statement?
For myself For employees in my facility
5 = Strongly
agree
4 = Agree
3= Neutral
2 = Disagree
1 = Strongly disagree
5 = Strongly
agree
4 = Agree
3 = Neutral
2 = Disagree
1 = Strongly disagree
309
There is safe and efficient transportation to work.
5 4 3 2 1 5 4 3 2 1
Module IV: Performance Factors Evaluate each factor related to job satisfaction by rating both how important you think each factor is to
your employees and how well the organization performs on each factor. Circle the appropriate response.
# How important do you think this is important to your employees?
How well does your organization perform on this factor?
3=Very important
2= Somewhat important
1=Not important
3=We perform very well
2=We have adequate performance
1=We don’t perform well
401 Overall job satisfaction. 3 2 1 3 2 1
402 Placing people in jobs for which they are suited.
3 2 1 3 2 1
403 Having clear job descriptions. 3 2 1 3 2 1
404 Recognizing & rewarding good work.
3 2 1 3 2 1
405 Supervisors who care about their staff and offer support.
3 2 1 3 2 1
406 Talking to staff regularly to encourage their development.
3 2 1 3 2 1
407 Overall morale. 3 2 1 3 2 1
408 Valuing and respecting each worker.
3 2 1 3 2 1
409 Creating a climate in which people get along and have friendship at work.
3 2 1 3 2 1
410 Creating flexibility to balance the demands of the workplace and personal lives.
3 2 1 3 2 1

58
411 Making the workplace an enjoyable and stimulating place.
3 2 1 3 2 1
412 Preventing harassment by supervisors.
3 2 1 3 2 1
413 Preventing harassment by peers. 3 2 1 3 2 1
414 Preventing harassment by patients or their friends and family.
3 2 1 3 2 1
415 Preventing harassment while traveling to and from work.
3 2 1 3 2 1
416 Offering the training needed for staff to succeed at their jobs.
3 2 1 3 2 1
417 Taking specific measures to protect workers against HIV/AIDS and other infections.
3 2 1 3 2 1
418 Connecting staff with the community.
3 2 1 3 2 1
419 Using appropriate methods & standards to measure job performance.
3 2 1 3 2 1
Module V: Ranking of compensation factors
# How important is the following compensation factor to employees in your workplace?
3= Very
important
2= Somewhat important
1= Not
important
501 Salary. 3 2 1
502 Terminal benefits (retirement, pension, etc) 3 2 1
503 Receiving a housing allowance or allocation of a house. 3 2 1
504 Assistance with transportation. 3 2 1
505 Health care for dependents. 3 2 1
506 Hardship or top-up allowance. 3 2 1
Module IV: Remuneration Package
To what extent do you agree with each of the following statements on work compensation in the facility?
Please circle the appropriate response both for yourself and for employees in your facility, using a scale
of 1-5 where 1=Strongly disagree; 2=Disagree; 3=Neutral; 4=Agree; and 5=Strongly agree.
# To what extent do you agree with the following statement?
For myself For my employees
5 = Strongly
agree
4 = Agree
3 = Neutral
2 = Disagre
e
1 = Strongly disagree
5 = Strongly
agree
4 = Agree
3 = Neutral
2 = Disagree
1 = Strongly disagree

59
601 The salary package is fair.
5 4 3 2 1 5 4 3 2 1
602 There are sufficient opportunities for promotion with this employer.
5 4 3 2 1 5 4 3 2 1
Module VII: Factors related to leaving
The following questions are about employees who left this facility for another employer (Leavers) in the
last twelve months. Please indicate, to your best knowledge, the degree of importance of each of the
factors below in employees’ decision to leave this facility in the last twelve months.
# How important is the following factor in making the people leave employment with your facility/district in the last year?
3= Very
important
2= Somewhat important
1= Not
important
701 Low pay/salary/allowances 3 2 1
702 High workload 3 2 1
703 Limited access to supplies & equipment (gloves, bandages, x-ray machines, etc.) at work
3 2 1
704 Limited opportunities for promotion 3 2 1
705 Social conflicts in the workplace 3 2 1
706 Poor supervision and management 3 2 1
707 Transport problems 3 2 1
708 Poor/lack of utilities (water, electricity) 3 2 1
709 Lack of housing facilities 3 2 1
710 Communication problems e.g. telephones 3 2 1
711 High cost of living 3 2 1
712 Lack of educational facilities for children 3 2 1
713 Lack of access to education and additional training for themselves
3 2 1
714 Work was far from home. 3 2 1
715 Other………………………………………………………………… 3 2 1
Section VIII: These are open-ended questions about your position.
801. Please identify three things that you like about working for this organization:
802. Please identify three things you don’t like about working for this organization.
803. Other comments:
THANK YOU FOR YOUR PARTICIPATION.

60
Focus Group Discussion Guide
Focus Group Discussion Guide for 10-12 service providers in health facility
Date (day/month/year):____/____/____ Time focus-group discussion began: _:____
Name of facilitator: ______________Time focus-group discussion ended: ___:____
Name of recorder: ______:_______
Gender of group: male: _____ female: ______
Introduction
Please identify a private setting for the FGDs. Ask/assist each of the participants to complete the background
information form. .
I would like to thank each of you for agreeing to be a part of this focus group discussion. My name is
………………. . I will be leading the discussion session.
My colleague here is called …………………; will help by taking notes about the discussion.
We also request you to allow the session to be audio-taped so that we do not miss writing down any of
the ideas. The purpose of conducting this discussion is to know how health workers view their jobs and
how satisfied they are with the working conditions. The information collected will be useful in helping
the Ministry of Public Health and Sanitation in improving the working conditions and other factors
related to the retention of health workers in Kenya. There are no wrong or right answers. Please be
assured that your personal details or what you say as a person will not be used at any time. What you say
is therefore confidential and anonymous. We shall be tape-recording the discussion. This will help us in
ensuring that we captured all the important information discussed. We will ensure confidentiality with
regard to all the information discussed and in particular, the information in the tapes will be destroyed
after analysis. This discussion will also be anonymous – your names will not be recorded in the notes;
rather we shall assign codes to the names. You are therefore encouraged to participate actively and to
feel free during the discussion.
Do you have questions at this point about this discussion? Ask each participant to introduce himself or
herself in turn. After the introductions, open up the discussion by asking the questions below.
1. Positive things about the work environment
1. Let’s start the discussion by talking about what makes this health centre a good place to work. What are some of the positive aspects of working here at this facility?
2. Limitations What are some things that aren’t so good about here as a place to work?
3. Leaving Have you considered leaving your job here? If so, why? What factors contributed to your decision to
want to leave and to your decision to stay?

61
4. Retention What would keep you in this job longer? What suggestions do you have to improve the working
environment here so that you would want to stay in your job?
Probe/discuss the following:
Salary
Benefits
Culture o Local culture, Relationships, camaraderie
Safety & Health protection o Protective measures (e.g., gloves) o Abuse issues on the job
Working conditions o Access to supplies, equipment, drugs
Respect/recognition from management or others
Opportunity, achievement, growth o Advancement, further education, responsibility
Management and supervision
Is there a sense of ownership of the outcomes here? o Work content, responsibility
Standards of living o Cost of living o Housing o Electricity o Water o Transportation
Education for children
Work/life (home) balance 5. Please feel free to make any other comment about the introduction of a new malaria vaccine in the
immunization programme.
AT THE END
We would like to thank you for sharing your thoughts and opinions; the information you have provided will be used
in the malaria control programme. We have come to the end of our discussions.
After the focus groupImmediately after the discussion, note-taker and/or facilitator: debrief together; look over the
forms with the participants‟ background information; make a note of suggested changes in the way the group or
interview should be conducted or in the technical aspects of the logistics; revise, edit and complete gestures and
consensus notes.

62
Appendix 3: Distribution of Factors Related to the Work Environment by Region
County
Nairobi Machakos Turkana Total
n % n % n % n % P value
The workload is
manageable.
Strongly disagree 4 2.4% 16 12.0% 5 5.1% 25 6.2% 0.001
Disagree 21 12.4% 19 14.3% 21 21.2% 61 15.2
%
Neutral 25 14.7% 22 16.5% 4 4.0% 51 12.7
%
Agree 92 54.1% 57 42.9% 47 47.5% 196 48.8
%
Strongly Agree 28 16.5% 19 14.3% 22 22.2% 69 17.2
%
Adequate supplies
(gloves, needles,
bandages, etc).
Strongly disagree 6 3.5% 17 12.6% 12 12.1% 35 8.6% <0.0001
Disagree 18 10.5% 33 24.4% 16 16.2% 67 16.5
%
Neutral 26 15.2% 23 17.0% 10 10.1% 59 14.6
%
Agree 53 31.0% 36 26.7% 29 29.3% 118 29.1
%
Strongly Agree 68 39.8% 26 19.3% 32 32.3% 126 31.1
%
Equipment available Strongly disagree 18 11.3% 28 21.1% 32 32.7% 78 19.9
%
<0.0001
Disagree 19 11.9% 42 31.6% 30 30.6% 91 23.3
%
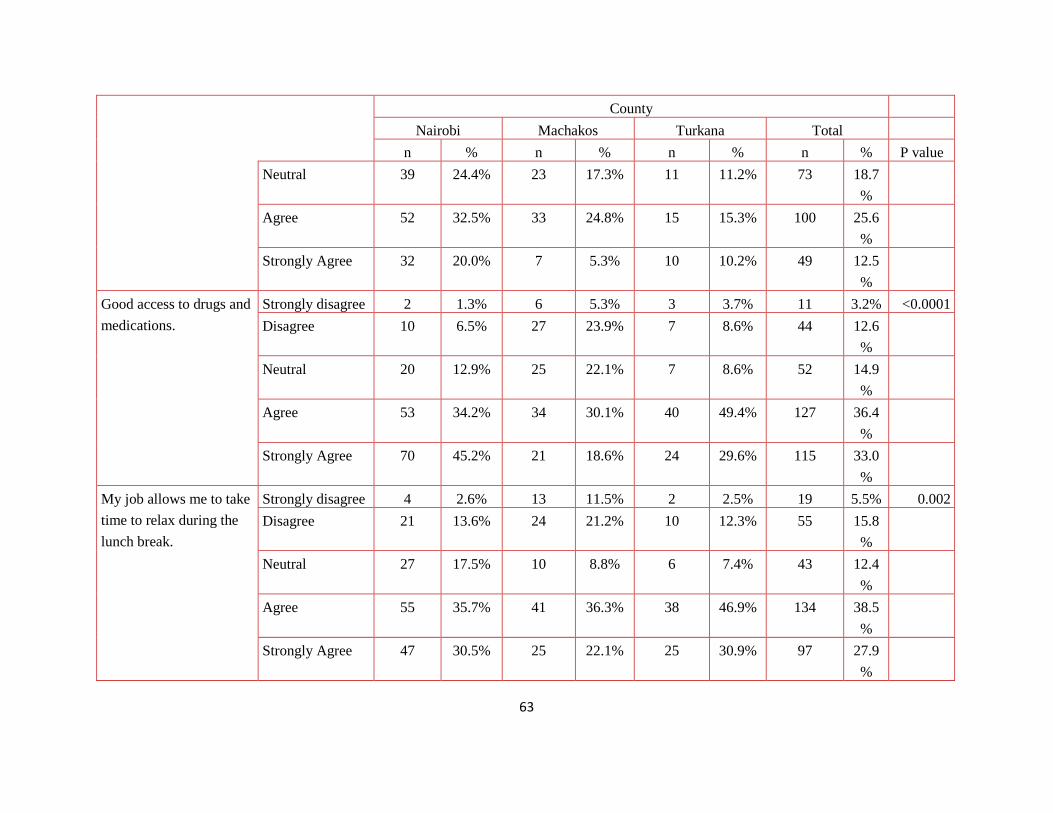
63
County
Nairobi Machakos Turkana Total
n % n % n % n % P value
Neutral 39 24.4% 23 17.3% 11 11.2% 73 18.7
%
Agree 52 32.5% 33 24.8% 15 15.3% 100 25.6
%
Strongly Agree 32 20.0% 7 5.3% 10 10.2% 49 12.5
%
Good access to drugs and
medications.
Strongly disagree 2 1.3% 6 5.3% 3 3.7% 11 3.2% <0.0001
Disagree 10 6.5% 27 23.9% 7 8.6% 44 12.6
%
Neutral 20 12.9% 25 22.1% 7 8.6% 52 14.9
%
Agree 53 34.2% 34 30.1% 40 49.4% 127 36.4
%
Strongly Agree 70 45.2% 21 18.6% 24 29.6% 115 33.0
%
My job allows me to take
time to relax during the
lunch break.
Strongly disagree 4 2.6% 13 11.5% 2 2.5% 19 5.5% 0.002
Disagree 21 13.6% 24 21.2% 10 12.3% 55 15.8
%
Neutral 27 17.5% 10 8.8% 6 7.4% 43 12.4
%
Agree 55 35.7% 41 36.3% 38 46.9% 134 38.5
%
Strongly Agree 47 30.5% 25 22.1% 25 30.9% 97 27.9
%

64
County
Nairobi Machakos Turkana Total
n % n % n % n % P value
I am allowed to go on
leave
Strongly disagree 5 3.2% 16 14.2% 6 7.5% 27 7.8% <0.0001
Disagree 8 5.2% 14 12.4% 14 17.5% 36 10.3
%
Neutral 12 7.7% 12 10.6% 4 5.0% 28 8.0%
Agree 40 25.8% 31 27.4% 29 36.3% 100 28.7
%
Strongly Agree 90 58.1% 40 35.4% 27 33.8% 157 45.1
%
At my residence, I have
access to safe, clean
water.
Strongly disagree 4 2.3% 16 11.9% 12 12.2% 32 7.9% <0.0001
Disagree 17 9.9% 28 20.7% 13 13.3% 58 14.4
%
Neutral 16 9.4% 10 7.4% 11 11.2% 37 9.2%
Agree 56 32.7% 45 33.3% 36 36.7% 137 33.9
%
Strongly Agree 78 45.6% 35 25.9% 26 26.5% 139 34.4
%
34 0 .0% 1 .7% 0 .0% 1 .2%
At work, I have access to
safe, clean water.
Strongly disagree 7 4.1% 14 10.4% 10 10.1% 31 7.7% <0.0001
Disagree 8 4.7% 36 26.7% 12 12.1% 56 13.8
%
Neutral 15 8.8% 11 8.1% 10 10.1% 36 8.9%
Agree 57 33.3% 43 31.9% 37 37.4% 137 33.8
%
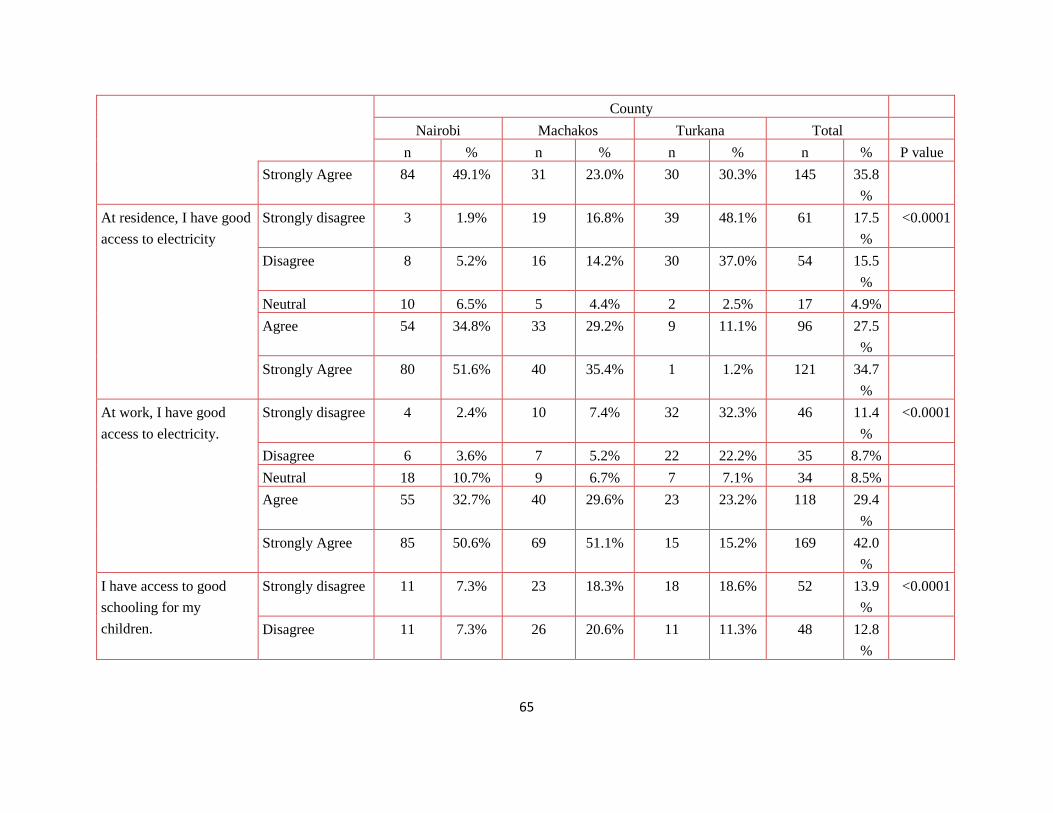
65
County
Nairobi Machakos Turkana Total
n % n % n % n % P value
Strongly Agree 84 49.1% 31 23.0% 30 30.3% 145 35.8
%
At residence, I have good
access to electricity
Strongly disagree 3 1.9% 19 16.8% 39 48.1% 61 17.5
%
<0.0001
Disagree 8 5.2% 16 14.2% 30 37.0% 54 15.5
%
Neutral 10 6.5% 5 4.4% 2 2.5% 17 4.9%
Agree 54 34.8% 33 29.2% 9 11.1% 96 27.5
%
Strongly Agree 80 51.6% 40 35.4% 1 1.2% 121 34.7
%
At work, I have good
access to electricity.
Strongly disagree 4 2.4% 10 7.4% 32 32.3% 46 11.4
%
<0.0001
Disagree 6 3.6% 7 5.2% 22 22.2% 35 8.7%
Neutral 18 10.7% 9 6.7% 7 7.1% 34 8.5%
Agree 55 32.7% 40 29.6% 23 23.2% 118 29.4
%
Strongly Agree 85 50.6% 69 51.1% 15 15.2% 169 42.0
%
I have access to good
schooling for my
children.
Strongly disagree 11 7.3% 23 18.3% 18 18.6% 52 13.9
%
<0.0001
Disagree 11 7.3% 26 20.6% 11 11.3% 48 12.8
%

66
County
Nairobi Machakos Turkana Total
n % n % n % n % P value
Neutral 34 22.5% 29 23.0% 14 14.4% 77 20.6
%
Agree 57 37.7% 34 27.0% 33 34.0% 124 33.2
%
Strongly Agree 38 25.2% 14 11.1% 21 21.6% 73 19.5
%
I have safe and efficient
transportation to work
Strongly disagree 18 11.0% 22 16.3% 23 23.7% 63 15.9
%
<0.0001
Disagree 21 12.9% 38 28.1% 35 36.1% 94 23.8
%
Neutral 42 25.8% 21 15.6% 12 12.4% 75 19.0
%
Agree 54 33.1% 35 25.9% 14 14.4% 103 26.1
%
Strongly Agree 28 17.2% 19 14.1% 13 13.4% 60 15.2
%
I feel I have job security Strongly disagree 23 13.8% 27 20.0% 18 18.2% 68 17.0
%
0.042
Disagree 23 13.8% 34 25.2% 20 20.2% 77 19.2
%
Neutral 35 21.0% 25 18.5% 16 16.2% 76 19.0
%
Agree 61 36.5% 26 19.3% 27 27.3% 114 28.4
%

67
County
Nairobi Machakos Turkana Total
n % n % n % n % P value
Strongly Agree 25 15.0% 23 17.0% 18 18.2% 66 16.5
%
I feel there is adequate
security at my residence
and within the
surrounding
Strongly disagree 14 9.2% 14 12.4% 12 14.8% 40 11.5
%
0.004
Disagree 24 15.7% 31 27.4% 14 17.3% 69 19.9
%
Neutral 45 29.4% 12 10.6% 12 14.8% 69 19.9
%
Agree 46 30.1% 40 35.4% 24 29.6% 110 31.7
%
Strongly Agree 24 15.7% 16 14.2% 19 23.5% 59 17.0
%
The community where I
live has good shopping
areas and entertainment.
Strongly disagree 10 6.6% 17 15.0% 12 15.0% 39 11.3
%
0.008
Disagree 23 15.2% 24 21.2% 19 23.8% 66 19.2
%
Neutral 46 30.5% 13 11.5% 15 18.8% 74 21.5
%
Agree 47 31.1% 43 38.1% 24 30.0% 114 33.1
%
Strongly Agree 25 16.6% 16 14.2% 10 12.5% 51 14.8
%
I understand and
appreciate the cultural
Strongly disagree 5 3.0% 6 4.5% 1 1.0% 12 3.0% <0.0001
Disagree 14 8.3% 15 11.2% 1 1.0% 30 7.5%

68
County
Nairobi Machakos Turkana Total
n % n % n % n % P value
values within the
surrounding community
Neutral 42 25.0% 21 15.7% 11 11.2% 74 18.5
%
Agree 69 41.1% 64 47.8% 41 41.8% 174 43.5
%
Strongly Agree 38 22.6% 28 20.9% 44 44.9% 110 27.5
%

69
Appendix 4: Distribution of factors in leaving Job by Region
County
Nairobi Machakos Turkana Total
n % n % n % n % P value
Low
pay/salary/allowances
Not important 7 20.6% 4 10.3% 3 15.8% 14 15.2% 0.127
Somewhat important 11 32.4% 4 10.3% 3 15.8% 18 19.6%
Very important 16 47.1% 30 76.9% 13 68.4% 59 64.1%
4 0 .0% 1 2.6% 0 .0% 1 1.1%
High workload Not important 11 35.5% 10 27.8% 6 31.6% 27 31.4% 0.122
Somewhat important 8 25.8% 13 36.1% 1 5.3% 22 25.6%
Very important 12 38.7% 13 36.1% 12 63.2% 37 43.0%
Poor access to supplies &
equipment at work
Not important 11 35.5% 9 25.0% 6 31.6% 26 30.2% 0.905
Somewhat important 10 32.3% 12 33.3% 6 31.6% 28 32.6%
Very important 10 32.3% 15 41.7% 7 36.8% 32 37.2%
Limited opportunities for
promotion
Not important 10 32.3% 5 13.9% 2 10.5% 17 19.8% 0.066
Somewhat important 7 22.6% 8 22.2% 9 47.4% 24 27.9%
Very important 14 45.2% 23 63.9% 8 42.1% 45 52.3%
Social conflicts in the
workplace
Not important 16 51.6% 19 52.8% 9 47.4% 44 51.2% 0.997
Somewhat important 6 19.4% 7 19.4% 4 21.1% 17 19.8%
Very important 9 29.0% 10 27.8% 6 31.6% 25 29.1%
Insecurity within the
surrounding community
Not important 8 44.4% 5 25.0% 5 100.0% 18 41.9% 0.024
Somewhat important 6 33.3% 5 25.0% 0 .0% 11 25.6%
Very important 4 22.2% 10 50.0% 0 .0% 14 32.6%
Poor supervision and
management
Not important 14 46.7% 16 44.4% 10 52.6% 40 47.1% 0.423
Somewhat important 5 16.7% 11 30.6% 2 10.5% 18 21.2%
Very important 11 36.7% 9 25.0% 7 36.8% 27 31.8%
Transport problems Not important 13 41.9% 13 36.1% 7 36.8% 33 38.4% 0.674

70
County
Nairobi Machakos Turkana Total
n % n % n % n % P value
Somewhat important 5 16.1% 11 30.6% 6 31.6% 22 25.6%
Very important 13 41.9% 12 33.3% 6 31.6% 31 36.0%
Poor/lack of utilities
(water, electricity) at
residence
Not important 15 48.4% 10 27.8% 9 47.4% 34 39.5% 0.094
Somewhat important 8 25.8% 7 19.4% 1 5.3% 16 18.6%
Very important 8 25.8% 19 52.8% 9 47.4% 36 41.9%
Poor/lack of utilities
(water, electricity) at
work
Not important 9 50.0% 4 20.0% 3 60.0% 16 37.2% 0.277
Somewhat important 3 16.7% 5 25.0% 1 20.0% 9 20.9%
Very important 6 33.3% 11 55.0% 1 20.0% 18 41.9%
Inadequate housing
facilities
Not important 10 32.3% 12 33.3% 7 36.8% 29 33.7% 0.952
Somewhat important 8 25.8% 11 30.6% 4 21.1% 23 26.7%
Very important 13 41.9% 13 36.1% 8 42.1% 34 39.5%
Communication problems
e.g. telephones, internet
Not important 14 46.7% 9 25.0% 8 42.1% 31 36.5% 0.454
Somewhat important 7 23.3% 12 33.3% 5 26.3% 24 28.2%
Very important 9 30.0% 15 41.7% 6 31.6% 30 35.3%
High cost of living Not important 6 20.0% 5 13.9% 4 21.1% 15 17.6% 0.405
Somewhat important 8 26.7% 4 11.1% 4 21.1% 16 18.8%
Very important 16 53.3% 27 75.0% 11 57.9% 54 63.5%
Poor educational
facilities for children
Not important 13 41.9% 10 28.6% 6 31.6% 29 34.1% 0.757
Somewhat important 8 25.8% 9 25.7% 6 31.6% 23 27.1%
Very important 10 32.3% 16 45.7% 7 36.8% 33 38.8%
Poor access to advanced
training and education for
myself
Not important 9 30.0% 7 20.0% 7 36.8% 23 27.4% 0.332
Somewhat important 9 30.0% 6 17.1% 4 21.1% 19 22.6%
Very important 12 40.0% 22 62.9% 8 42.1% 42 50.0%
Work is far from home. Not important 10 32.3% 8 22.9% 8 42.1% 26 30.6% 0.580

71
County
Nairobi Machakos Turkana Total
n % n % n % n % P value
Somewhat important 11 35.5% 13 37.1% 4 21.1% 28 32.9%
Very important 10 32.3% 14 40.0% 7 36.8% 31 36.5%
Inadequate socialization Not important 9 50.0% 6 33.3% 5 100.0% 20 48.8% 0.115
Somewhat important 5 27.8% 5 27.8% 0 .0% 10 24.4%
Very important 4 22.2% 7 38.9% 0 .0% 11 26.8%
Job security Not important 5 27.8% 3 15.0% 2 40.0% 10 23.3% 0.628
Somewhat important 4 22.2% 3 15.0% 1 20.0% 8 18.6%
Very important 9 50.0% 14 70.0% 2 40.0% 25 58.1%
Other Not important 1 11.1% 1 12.5% 1 50.0% 3 15.8% 0.391
Somewhat important 1 11.1% 3 37.5% 0 .0% 4 21.1%
Very important 7 77.8% 4 50.0% 1 50.0% 12 63.2%

72
Appendix 5: Percentage Distribution of Job Satisfaction Factors by Region
County
Nairobi Machakos Turkana Total
n % n % n % n %
P
value
Considering everything, I
am satisfied with my job.
Strongly
disagree
10 6.0% 13 9.6% 2 2.0% 25 6.2% 0.163
Disagree 31 18.5% 29 21.5% 23 23.2% 83 20.6%
Neutral 49 29.2% 44 32.6% 23 23.2% 116 28.9%
Agree 44 26.2% 31 23.0% 31 31.3% 106 26.4%
Strongly
Agree
34 20.2% 18 13.3% 20 20.2% 72 17.9%
The job is a good match
for my skills and
experience.
Strongly
disagree
5 3.0% 9 6.8% 1 1.0% 15 3.8% 0.028
Disagree 20 11.9% 25 18.8% 7 7.1% 52 13.0%
Neutral 33 19.6% 18 13.5% 23 23.5% 74 18.5%
Agree 65 38.7% 53 39.8% 46 46.9% 164 41.1%
Strongly
Agree
45 26.8% 28 21.1% 21 21.4% 94 23.6%
When I come to work, I
know what is expected of
me.
Strongly
disagree
1 .6% 0 .0% 0 .0% 1 .2% 0.002
Disagree 1 .6% 4 3.0% 3 3.0% 8 2.0%
Neutral 22 13.0% 22 16.4% 17 17.2% 61 15.2%
Agree 39 23.1% 54 40.3% 43 43.4% 136 33.8%
Strongly
Agree
105 62.1% 54 40.3% 36 36.4% 195 48.5%
33 1 .6% 0 .0% 0 .0% 1 .2%
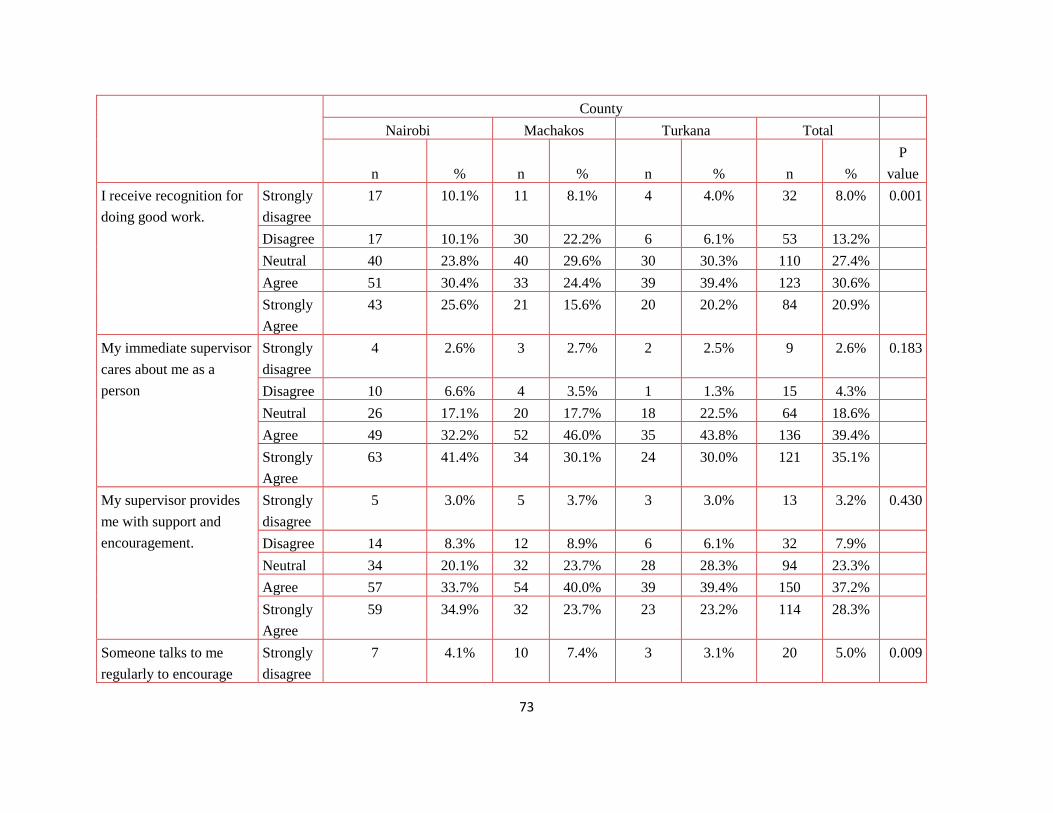
73
County
Nairobi Machakos Turkana Total
n % n % n % n %
P
value
I receive recognition for
doing good work.
Strongly
disagree
17 10.1% 11 8.1% 4 4.0% 32 8.0% 0.001
Disagree 17 10.1% 30 22.2% 6 6.1% 53 13.2%
Neutral 40 23.8% 40 29.6% 30 30.3% 110 27.4%
Agree 51 30.4% 33 24.4% 39 39.4% 123 30.6%
Strongly
Agree
43 25.6% 21 15.6% 20 20.2% 84 20.9%
My immediate supervisor
cares about me as a
person
Strongly
disagree
4 2.6% 3 2.7% 2 2.5% 9 2.6% 0.183
Disagree 10 6.6% 4 3.5% 1 1.3% 15 4.3%
Neutral 26 17.1% 20 17.7% 18 22.5% 64 18.6%
Agree 49 32.2% 52 46.0% 35 43.8% 136 39.4%
Strongly
Agree
63 41.4% 34 30.1% 24 30.0% 121 35.1%
My supervisor provides
me with support and
encouragement.
Strongly
disagree
5 3.0% 5 3.7% 3 3.0% 13 3.2% 0.430
Disagree 14 8.3% 12 8.9% 6 6.1% 32 7.9%
Neutral 34 20.1% 32 23.7% 28 28.3% 94 23.3%
Agree 57 33.7% 54 40.0% 39 39.4% 150 37.2%
Strongly
Agree
59 34.9% 32 23.7% 23 23.2% 114 28.3%
Someone talks to me
regularly to encourage
Strongly
disagree
7 4.1% 10 7.4% 3 3.1% 20 5.0% 0.009

74
County
Nairobi Machakos Turkana Total
n % n % n % n %
P
value
my development Disagree 33 19.5% 23 17.0% 3 3.1% 59 14.7%
Neutral 49 29.0% 34 25.2% 38 38.8% 121 30.1%
Agree 49 29.0% 46 34.1% 38 38.8% 133 33.1%
Strongly
Agree
31 18.3% 22 16.3% 16 16.3% 69 17.2%
Overall, the morale level
at my department or
section is good.
Strongly
disagree
7 4.2% 8 5.9% 4 4.0% 19 4.7% 0.600
Disagree 19 11.3% 25 18.5% 19 19.2% 63 15.7%
Neutral 48 28.6% 36 26.7% 28 28.3% 112 27.9%
Agree 65 38.7% 49 36.3% 31 31.3% 145 36.1%
Strongly
Agree
29 17.3% 17 12.6% 17 17.2% 63 15.7%
My opinion seems to
matter at work; I am
respected.
Strongly
disagree
2 1.2% 4 3.0% 4 4.1% 10 2.5% 0.213
Disagree 16 9.7% 19 14.1% 3 3.1% 38 9.5%
Neutral 46 27.9% 33 24.4% 28 28.6% 107 26.9%
Agree 72 43.6% 52 38.5% 44 44.9% 168 42.2%
Strongly
Agree
29 17.6% 27 20.0% 19 19.4% 75 18.8%
I have at least one good
friend at work.
Strongly
disagree
1 .6% 4 3.0% 1 1.0% 6 1.5% 0.030
Disagree 10 6.0% 7 5.2% 1 1.0% 18 4.5%
Neutral 21 12.7% 27 20.0% 20 20.2% 68 17.0%

75
County
Nairobi Machakos Turkana Total
n % n % n % n %
P
value
Agree 65 39.2% 52 38.5% 51 51.5% 168 42.0%
Strongly
Agree
69 41.6% 45 33.3% 26 26.3% 140 35.0%
I would encourage my
friends and family to seek
care here.
Strongly
disagree
3 2.0% 7 6.2% 2 2.5% 12 3.5% 0.023
Disagree 6 3.9% 8 7.1% 4 4.9% 18 5.2%
Neutral 26 17.1% 13 11.5% 6 7.4% 45 13.0%
Agree 45 29.6% 41 36.3% 41 50.6% 127 36.7%
Strongly
Agree
72 47.4% 44 38.9% 28 34.6% 144 41.6%
I have flexibility to
balance the demands of
my workplace and my
personal life.
Strongly
disagree
2 1.2% 9 6.7% 3 3.0% 14 3.5% 0.137
Disagree 29 17.4% 22 16.3% 11 11.1% 62 15.5%
Neutral 41 24.6% 37 27.4% 27 27.3% 105 26.2%
Agree 66 39.5% 48 35.6% 34 34.3% 148 36.9%
Strongly
Agree
29 17.4% 19 14.1% 24 24.2% 72 18.0%
I find my work at this
facility to be enjoyable.
Strongly
disagree
7 4.2% 6 4.5% 4 4.0% 17 4.2% 0.628
Disagree 18 10.7% 17 12.7% 12 12.1% 47 11.7%
Neutral 40 23.8% 43 32.1% 34 34.3% 117 29.2%
Agree 67 39.9% 40 29.9% 30 30.3% 137 34.2%

76
County
Nairobi Machakos Turkana Total
n % n % n % n %
P
value
Strongly
Agree
36 21.4% 28 20.9% 19 19.2% 83 20.7%
My supervisors are kind
to me; they do not
verbally, physically or
emotionally abuse
Strongly
disagree
3 1.8% 5 3.7% 1 1.0% 9 2.2% 0.013
Disagree 7 4.2% 9 6.7% 3 3.0% 19 4.7%
Neutral 30 17.9% 31 23.0% 35 35.4% 96 23.9%
Agree 60 35.7% 45 33.3% 40 40.4% 145 36.1%
Strongly
Agree
68 40.5% 44 32.6% 20 20.2% 132 32.8%
31 0 .0% 1 .7% 0 .0% 1 .2%
My peers are kind to me;
they do not verbally,
physically or emotionally
abuse me.
Strongly
disagree
3 1.8% 2 1.5% 0 .0% 5 1.2% 0.232
Disagree 11 6.5% 10 7.4% 3 3.0% 24 6.0%
Neutral 32 18.9% 28 20.7% 29 29.3% 89 22.1%
Agree 60 35.5% 49 36.3% 42 42.4% 151 37.5%
Strongly
Agree
63 37.3% 46 34.1% 25 25.3% 134 33.3%
My patients and their
family members are kind
to me; they do not
verbally, physically or
Strongly
disagree
6 3.6% 2 1.5% 2 2.0% 10 2.5% 0.584
Disagree 18 10.7% 10 7.4% 4 4.0% 32 8.0%
Neutral 34 20.2% 30 22.2% 27 27.3% 91 22.6%
Agree 62 36.9% 54 40.0% 38 38.4% 154 38.3%

77
County
Nairobi Machakos Turkana Total
n % n % n % n %
P
value
Strongly
Agree
48 28.6% 39 28.9% 28 28.3% 115 28.6%
I have been provided the
training needed to
succeed in my
position.(on the job
Strongly
disagree
7 4.2% 14 10.4% 15 15.2% 36 9.0% <0.00
01
Disagree 27 16.1% 29 21.5% 25 25.3% 81 20.1%
Neutral 32 19.0% 33 24.4% 32 32.3% 97 24.1%
Agree 52 31.0% 37 27.4% 10 10.1% 99 24.6%
Strongly
Agree
49 29.2% 22 16.3% 17 17.2% 88 21.9%
33 1 .6% 0 .0% 0 .0% 1 .2%
The organization takes
specific measures to
protect me against
HIV/AIDS and TB.
Strongly
disagree
6 3.6% 12 9.0% 7 7.1% 25 6.2% 0.313
Disagree 15 8.9% 14 10.4% 8 8.1% 37 9.2%
Neutral 37 21.9% 36 26.9% 27 27.3% 100 24.9%
Agree 58 34.3% 45 33.6% 35 35.4% 138 34.3%
Strongly
Agree
53 31.4% 27 20.1% 22 22.2% 102 25.4%
I consider myself a part
of this community.
Strongly
disagree
0 .0% 1 .7% 0 .0% 1 .2% 0.805
Disagree 7 4.2% 8 5.9% 4 4.0% 19 4.7%
Neutral 35 20.8% 30 22.2% 20 20.2% 85 21.1%
Agree 68 40.5% 46 34.1% 34 34.3% 148 36.8%

78
County
Nairobi Machakos Turkana Total
n % n % n % n %
P
value
Strongly
Agree
57 33.9% 50 37.0% 41 41.4% 148 36.8%
32 1 .6% 0 .0% 0 .0% 1 .2%
I am fairly evaluated on
my work.
Strongly
disagree
0 .0% 7 5.3% 7 7.1% 14 3.5% 0.002
Disagree 10 6.0% 16 12.1% 2 2.0% 28 7.1%
Neutral 39 23.5% 33 25.0% 27 27.3% 99 24.9%
Agree 70 42.2% 51 38.6% 45 45.5% 166 41.8%
Strongly
Agree
47 28.3% 25 18.9% 18 18.2% 90 22.7%
The in charge here is
competent and
committed.
Strongly
disagree
1 .7% 6 5.3% 3 3.7% 10 2.9% 0.060
Disagree 7 4.6% 7 6.2% 1 1.2% 15 4.3%
Neutral 13 8.6% 9 8.0% 12 14.8% 34 9.9%
Agree 61 40.4% 38 33.6% 38 46.9% 137 39.7%
Strongly
Agree
69 45.7% 53 46.9% 27 33.3% 149 43.2%
I am actively involved in
helping to make this a
great health care facility.
Strongly
disagree
1 .7% 2 1.8% 1 1.2% 4 1.2% 0.426
Disagree 3 2.0% 6 5.3% 0 .0% 9 2.6%
Neutral 13 8.5% 7 6.2% 7 8.6% 27 7.8%
Agree 60 39.2% 50 44.2% 36 44.4% 146 42.1%

79
County
Nairobi Machakos Turkana Total
n % n % n % n %
P
value
Strongly
Agree
76 49.7% 48 42.5% 37 45.7% 161 46.4%
Appendix 6: Comparison of Compensation Factors by Type of Facility
Government Private/NGO
n % n % P value
My salary package is fair.
Strongly disagree 67 35.4% 49 23.1% <0.0001
Disagree 68 36.0% 48 22.6%
Neutral 34 18.0% 47 22.2%
Agree 14 7.4% 54 25.5%
Strongly Agree 6 3.2% 14 6.6%
I feel there are sufficient
opportunities for promotion with this
employer.
Strongly disagree 34 18.0% 32 15.1% 0.019
Disagree 51 27.0% 39 18.4%
Neutral 36 19.0% 68 32.1%
Agree 51 27.0% 48 22.6%
Strongly Agree 17 9.0% 25 11.8%
I feel there is no stagnation in the
Ministry/organization
Strongly disagree 32 19.6% 23 12.7% 0.022
Disagree 36 22.1% 22 12.2%
Neutral 39 23.9% 56 30.9%
Agree 37 22.7% 56 30.9%
Strongly Agree 19 11.7% 24 13.3%

80
Appendix 7: Importance of Compensation factors by Region
Nairobi Machakos Turkana Total
n % n % n % n % P value
Salary Not important 3 1.8% 1 .8% 11 11.2% 15 3.8% <0.0001
Somewhat important 32 19.4% 11 8.3% 7 7.1% 50 12.6%
Very important 130 78.8% 121 91.0% 80 81.6% 331 83.6%
Terminal benefits
(retirement, pension, etc)
Not important 5 3.0% 2 1.5% 27 27.6% 34 8.5% <0.001
Somewhat important 31 18.5% 5 3.8% 11 11.2% 47 11.8%
Very important 132 78.6% 126 94.7% 60 61.2% 318 79.7%
Receiving a housing
allowance or allocation of
a house to stay in.
Not important 14 8.5% 6 4.5% 25 25.5% 45 11.4% <0.0001
Somewhat important 23 14.0% 8 6.0% 9 9.2% 40 10.1%
Very important 127 77.4% 118 88.7% 64 65.3% 309 78.2%
Assistance with
transportation/commuter
allowance.
Not important 16 9.6% 7 5.3% 32 32.7% 55 13.9% <0.0001
Somewhat important 27 16.3% 8 6.0% 10 10.2% 45 11.3%
Very important 121 72.9% 117 88.0% 56 57.1% 294 74.1%
Health care for my
family.
Not important 9 5.4% 2 1.5% 5 5.1% 16 4.0% 0.250
Somewhat important 17 10.2% 8 6.0% 9 9.2% 34 8.6%
Very important 140 84.3% 123 92.5% 84 85.7% 347 87.4%
Hardship allowance or
top-up salary.
Not important 15 9.0% 5 3.8% 27 27.6% 47 11.8% <0.0001
Somewhat important 32 19.3% 7 5.3% 8 8.2% 47 11.8%
Very important 119 71.7% 121 91.0% 63 64.3% 303 76.3%
Recognition and awards
scheme
Not important 14 8.3% 8 6.1% 24 24.5% 46 11.6% <0.0001
Somewhat important 43 25.6% 13 9.8% 20 20.4% 76 19.1%
Very important 108 64.3% 103 78.0% 49 50.0% 260 65.3%
Measure of motivation
instituted at the facility
level
Not important 12 8.2% 3 3.6% 10 12.7% 25 8.1% 0.002
Somewhat important 27 18.5% 3 3.6% 15 19.0% 45 14.6%

1
Partner Profiles
AMREF was founded in 1957 as the Flying Doctors Service of East Africa and remains one of the
continents leading health development and research organisations. Headquartered in Nairobi Kenya,
AMREF's vision is for lasting health change in Africa: communities with the knowledge,
skills and means to maintain their good health and break the cycle of poor health and
poverty. AMREF believes that the power for lasting transformation of Africa‟s health lies within its
communities there by working side by side with the people in these communities to build their
knowledge, skills and means to transform health outcomes. AMREF believes that by focusing on
the health of women and children, the health of the whole community can be improved. Our main
areas of intervention are maternal and child health; HIV and Tuberculosis; safe water and sanitation;
malaria; and essential clinical care. AMREF is a winner of the Gates Award for Global Health.
World Vision Kenya (WVK) is a Christian Based Non-Profit making Relief Organisation,
motivated by our faith in Jesus Christ, and serves alongside the poor and oppressed without
partiality as a demonstration of God‟s unconditional love for all people. It is a child focused
organisation and therefore prioritizes the needs of children, especially the poorest and most
vulnerable, and empowers them together with their families and communities to improve their well
being.
Health NGOs Network (HENNET) is a national membership organisation founded in 2005 to
fill in a longstanding coordination and networking gap among health related CSOs. It has since
provided a forum for CSOs dealing with health issues for collaboration, experience sharing and
advocacy. It brings together different health NGOs under the common vision of a “healthy Kenyan
society”.
For more information, contact
Country Director, AMREF Kenya
P.O Box 30125-00100, Nairobi, kenya
Tel: +254 20 699 4000; Fax:
Email:
www.amref.org
Top Related