






Languages
Pages
Legal

Eye, Ear & Maxillofacial Pathologies
Kimberly Lakhan, PA-C
SMDC ENT
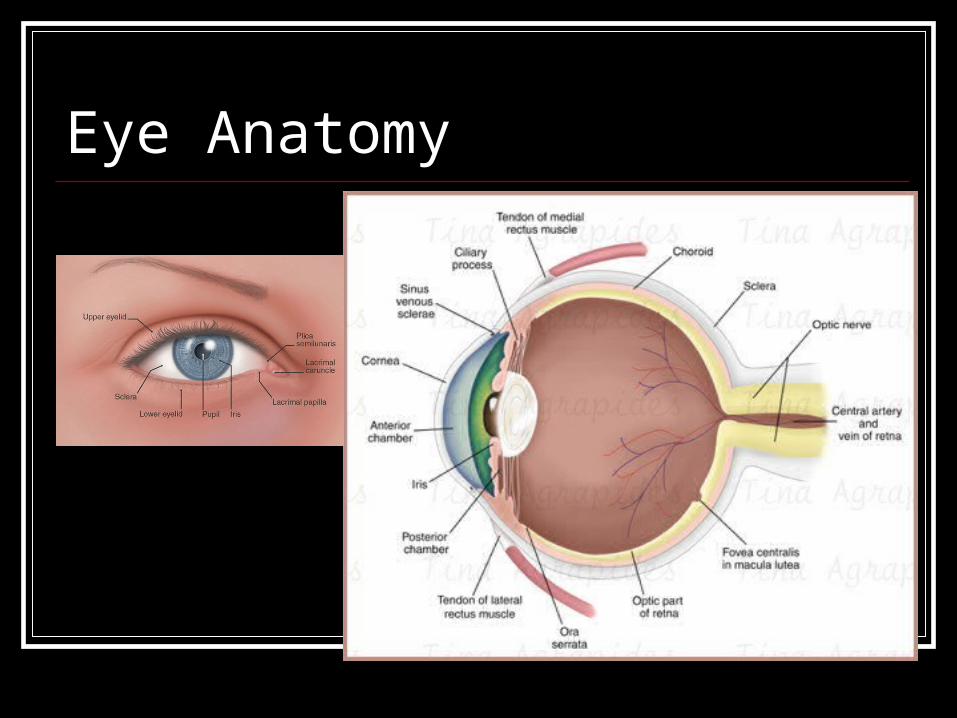
Eye Anatomy
How to Use a Ophthalmoscope
Preparing your Equipment Check the battery Cover off Familiarize self with dials & levers, set all to
“0” Light should be bright, round, white Turn light down, dim
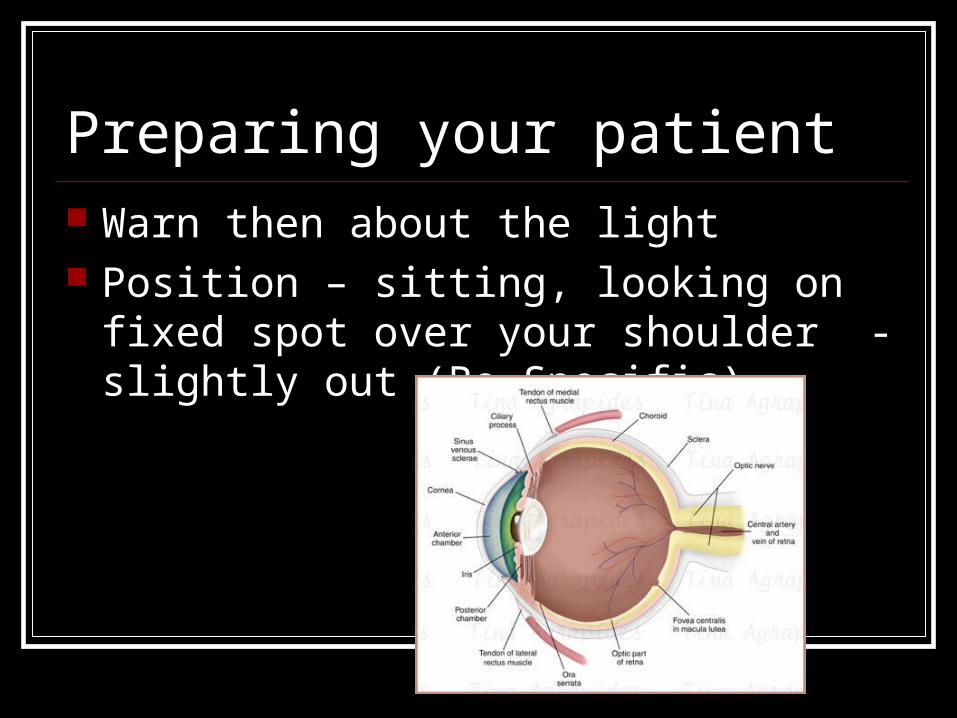
Preparing your patient Warn then about the light Position – sitting, looking on fixed spot over
your shoulder - slightly out (Be Specific)
Your Position Eye to Eye (Left to left, Right to Right) Try and keep your other eye open Begin at arm’s length by shining light into
the patient’s pupil. Continue to move forward until your
forehead rests on your thumb. The closer you are the wider your field of view.
Turn dial to focus on disc
What am I looking for? Red reflex
Optic disc
Vessels
Macula
Eye Pathology Conjunctivitis Hyphema Lacerated Eye Lid Corneal Abrasion Orbital Fx Ruptured Globe Detached Retina Strabismus Aniscoria Stye Raccoon Eyes
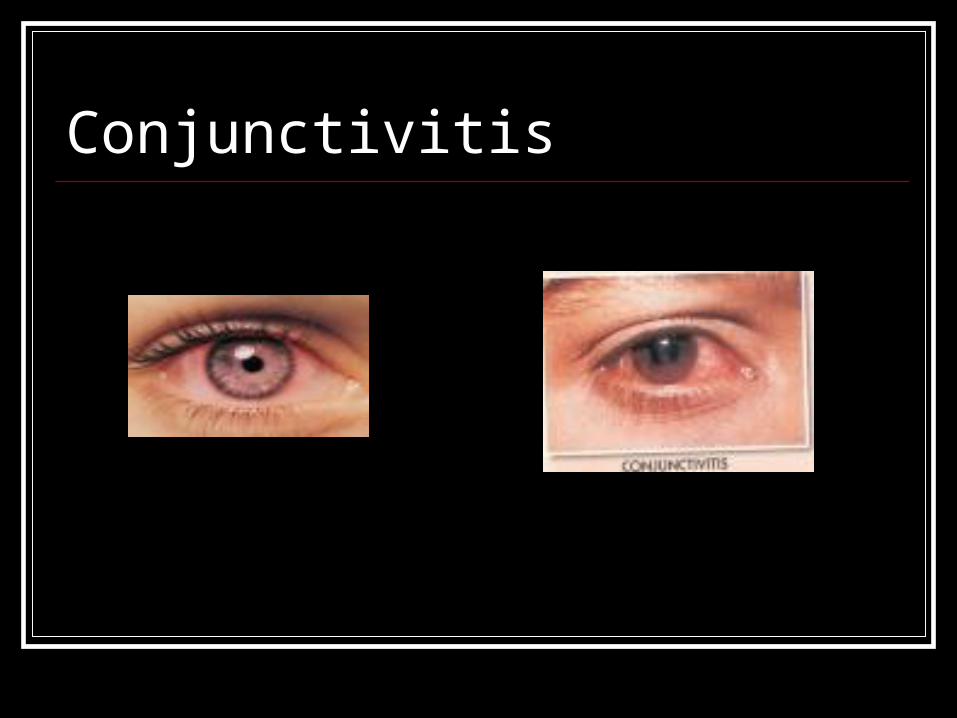
Conjunctivitis
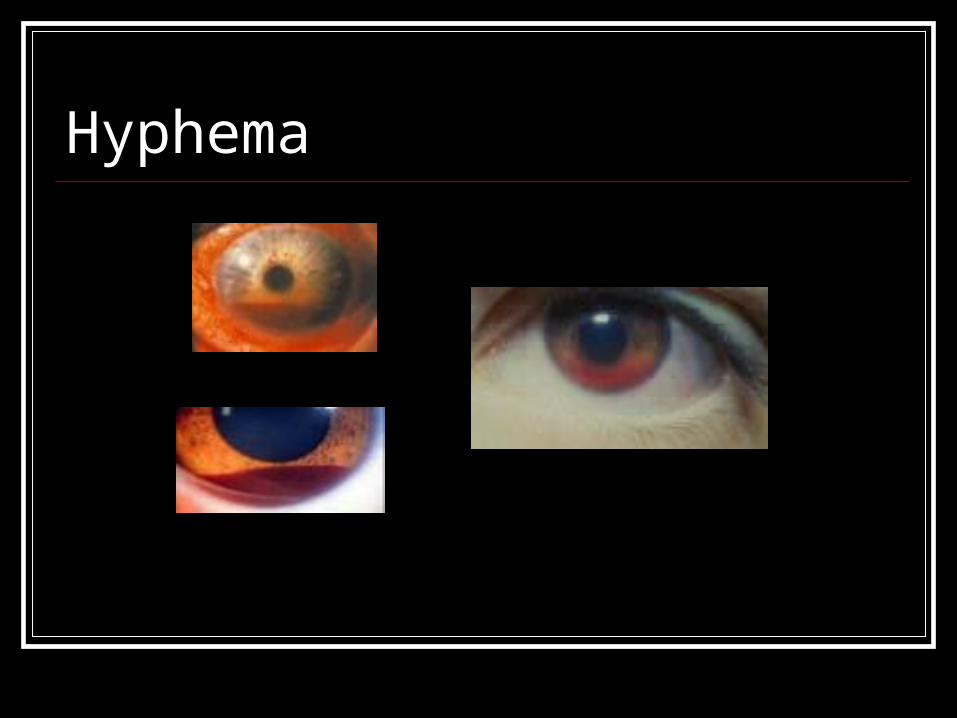
Hyphema
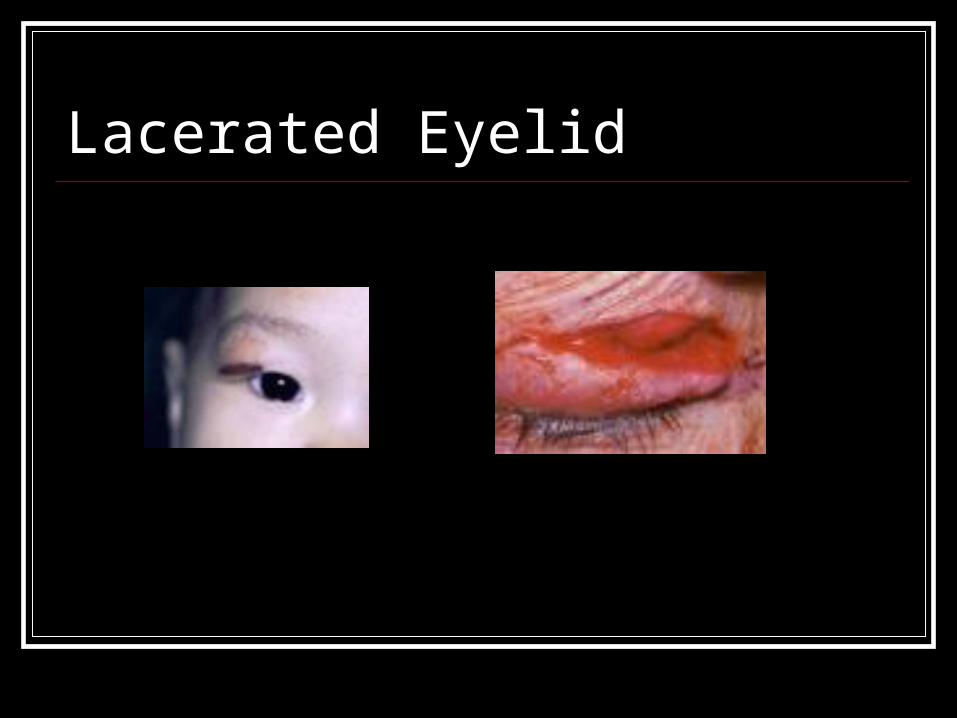
Lacerated Eyelid
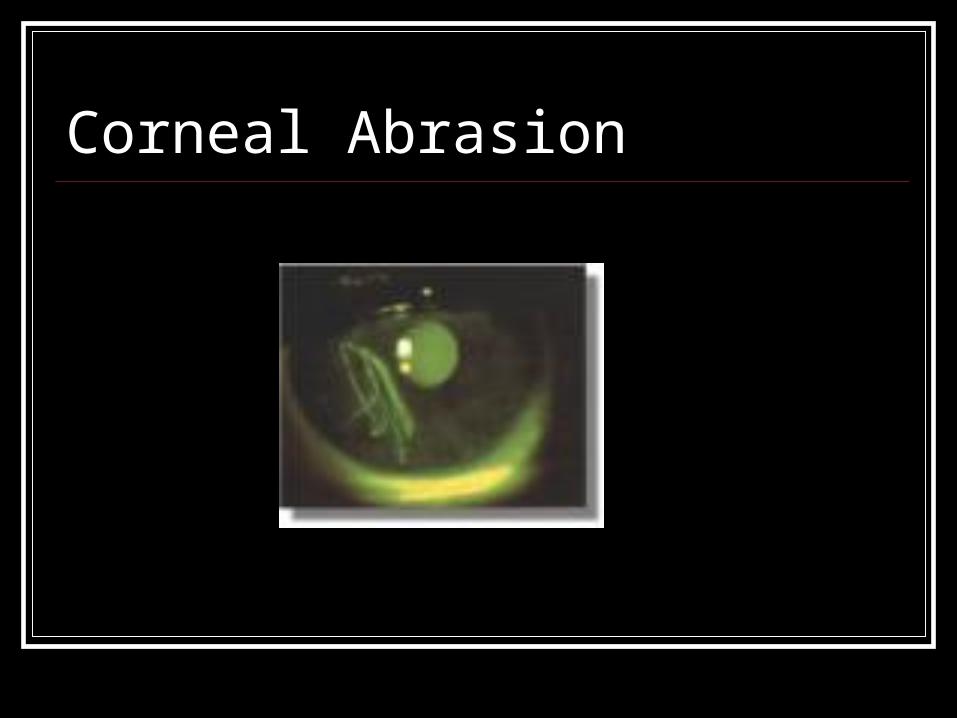
Corneal Abrasion
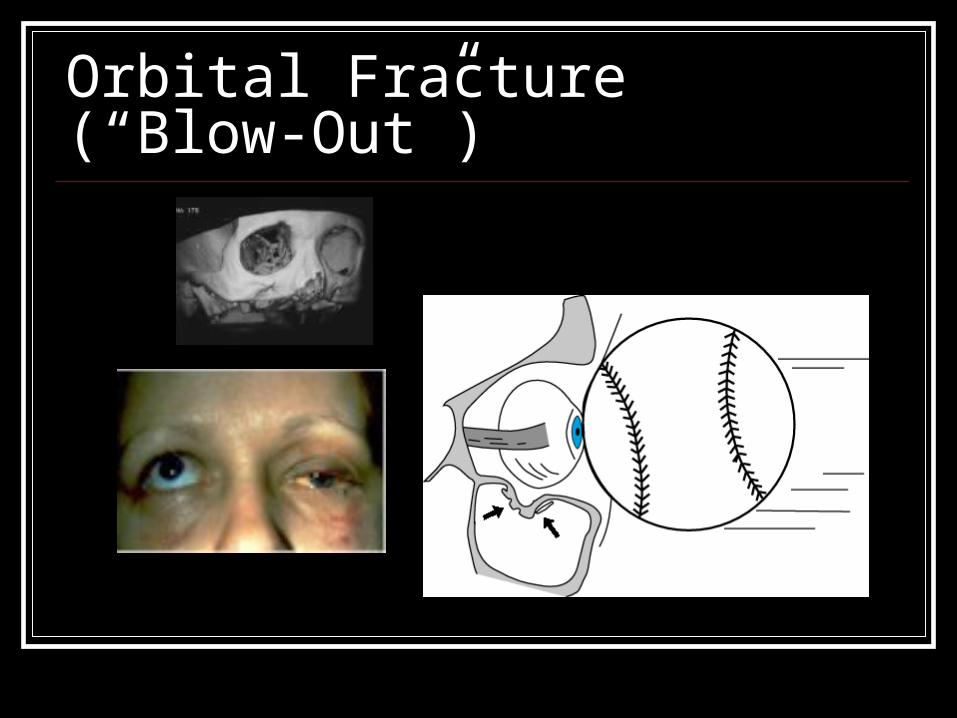
Orbital Fracture (“Blow-Out”)
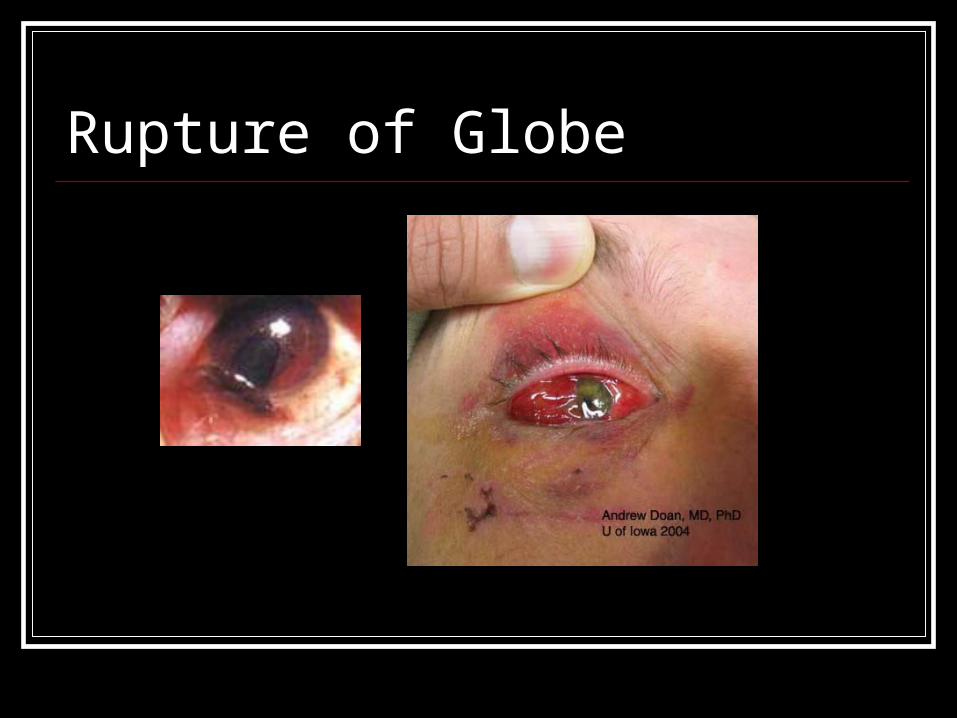
Rupture of Globe
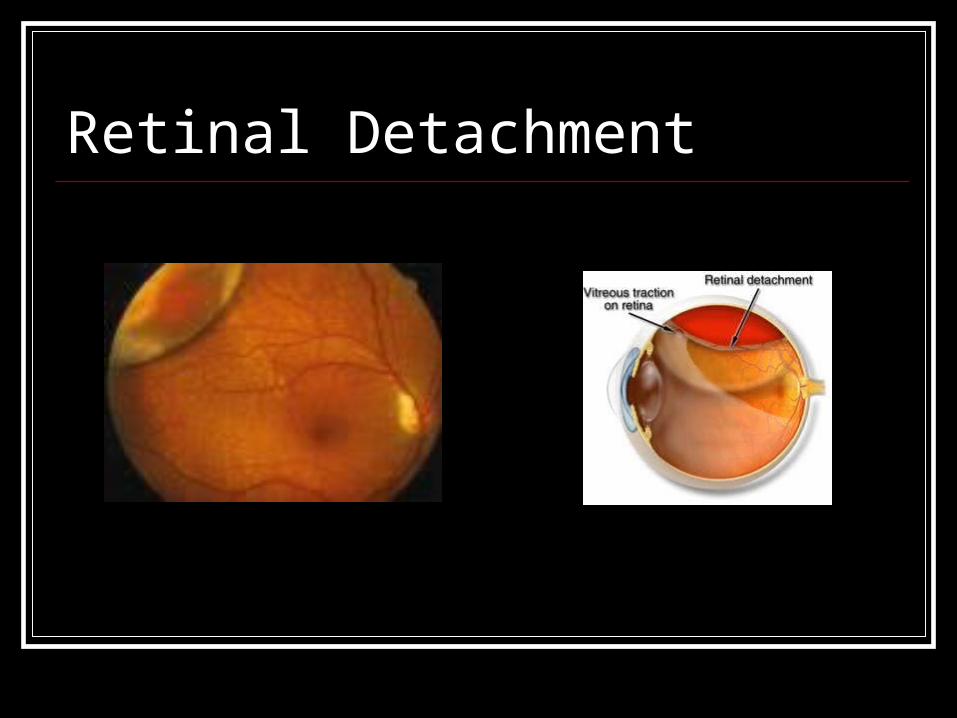
Retinal Detachment
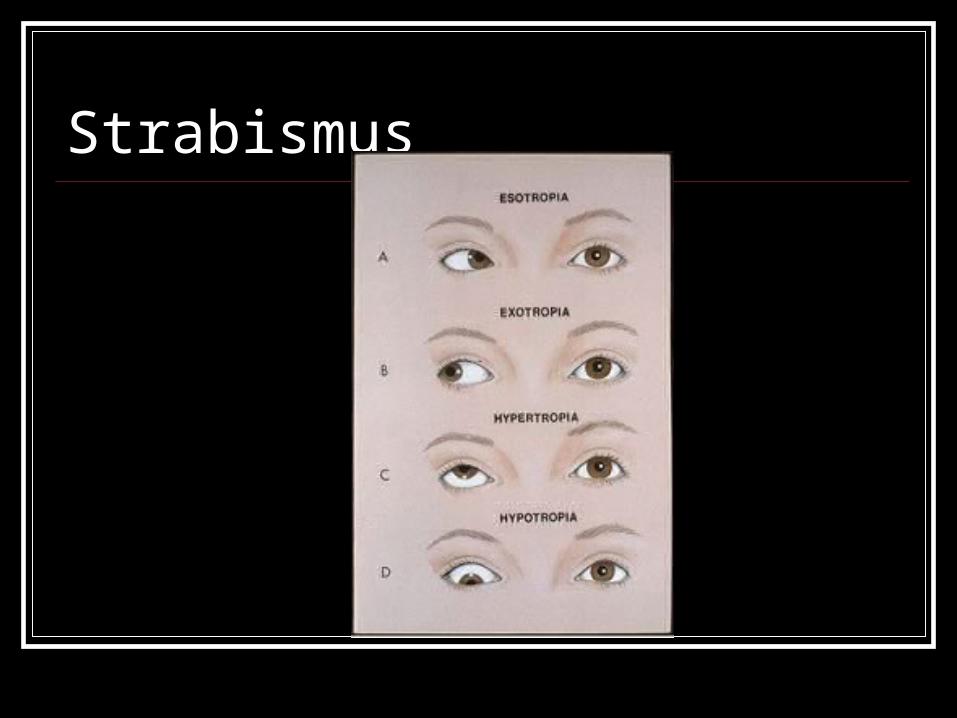
Strabismus
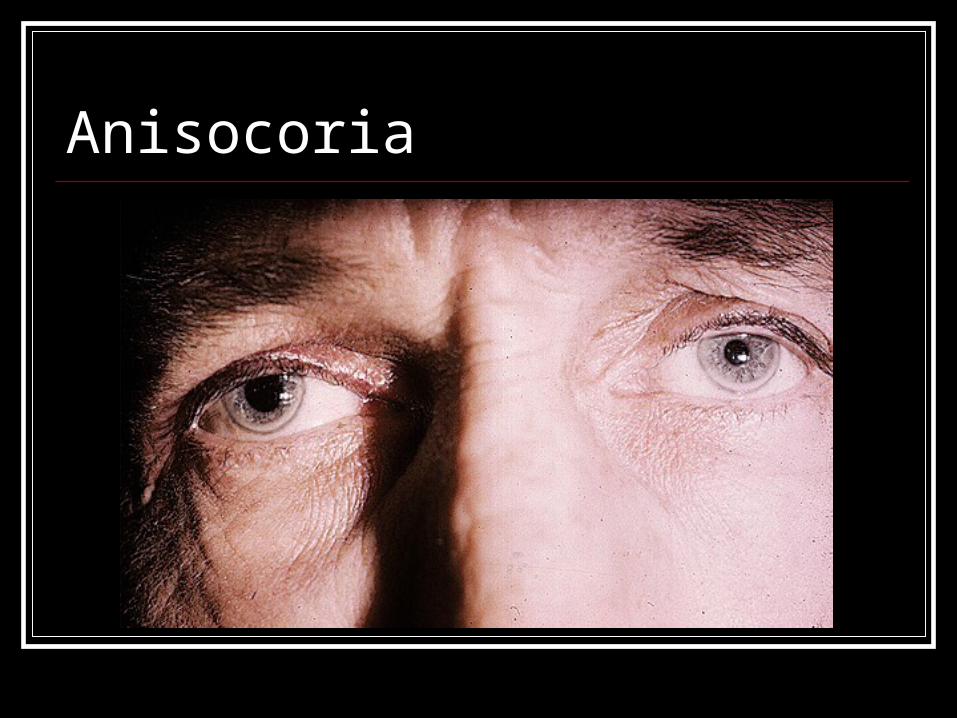
Anisocoria
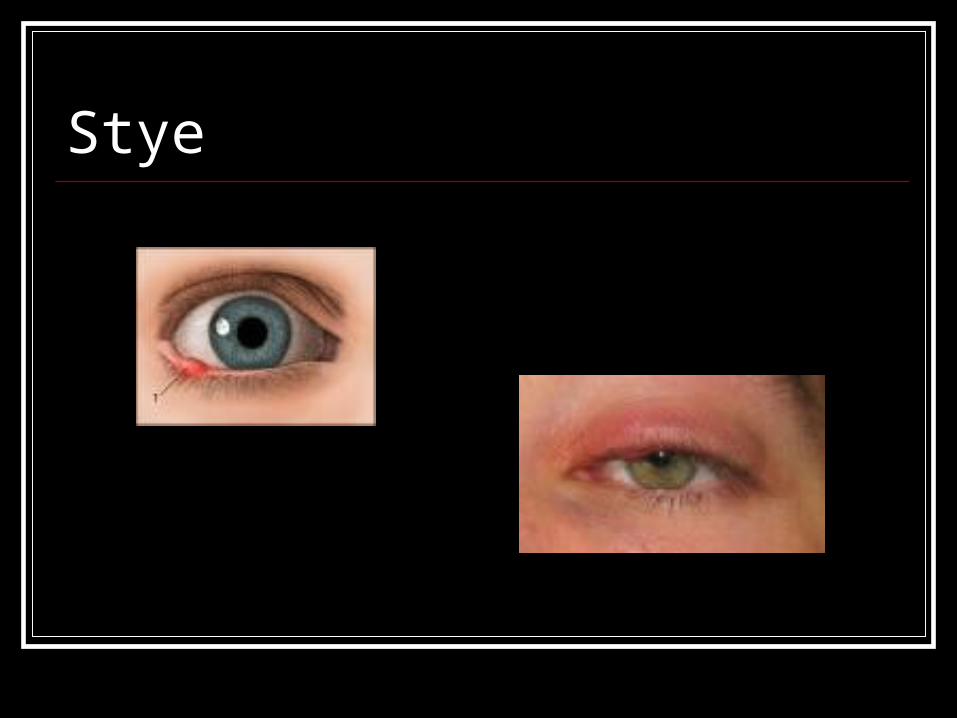
Stye
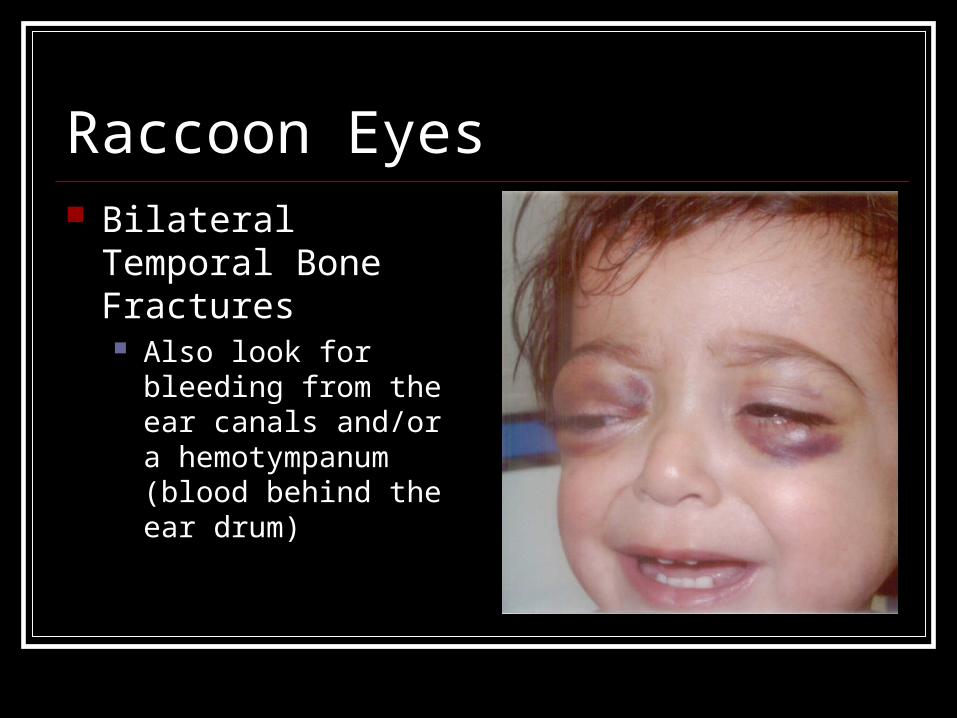
Raccoon Eyes Bilateral Temporal
Bone Fractures Also look for bleeding
from the ear canals and/or a hemotympanum (blood behind the ear drum)
Eye Referral Embedded object Decreased or partial vision Hyphema Diplopia Laceration of eyelid Strabismus Nystagmus Inverted or everted eye Eye swollen shut Abnormal pupil size
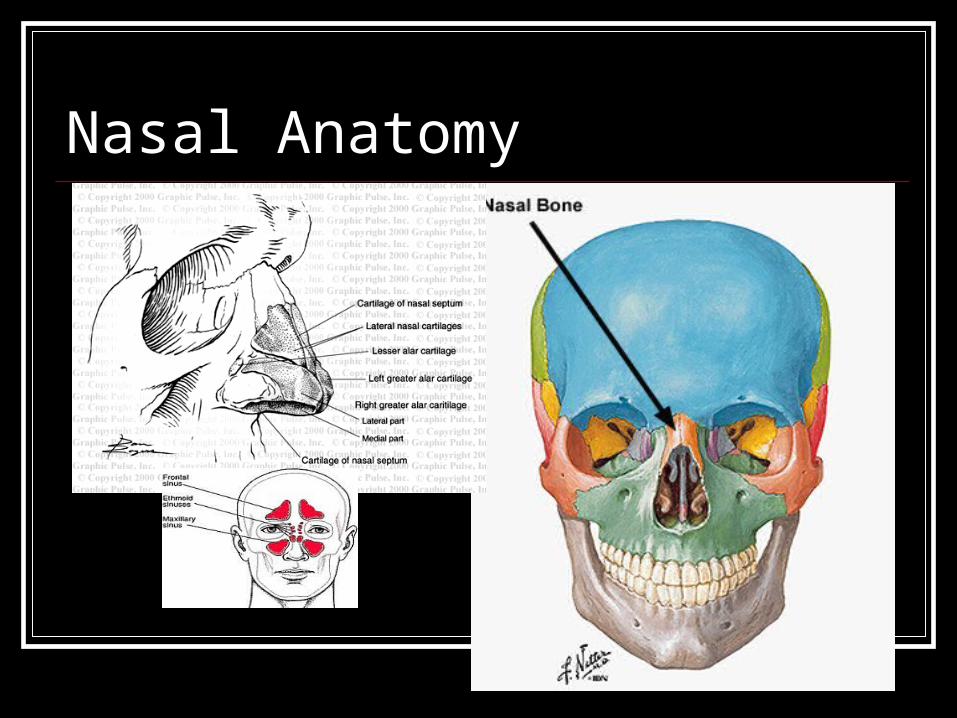
Nasal Anatomy
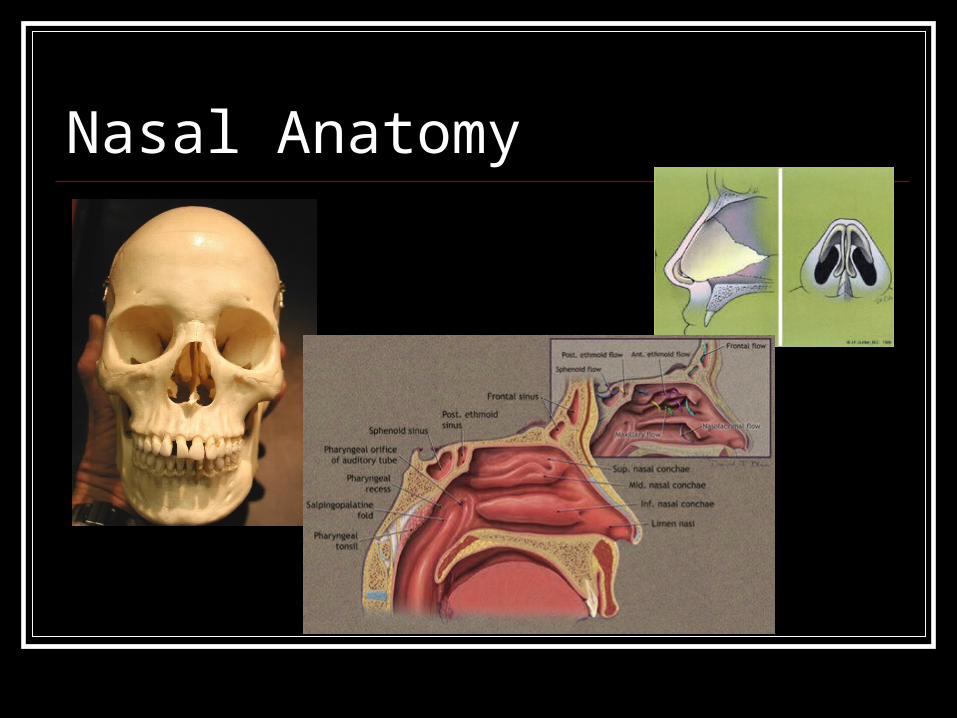
Nasal Anatomy
Nasal Pathology Epistaxis Nasal Fracture Deviated septum Perforated septum Polyps
Epistaxis
Control the bleeding
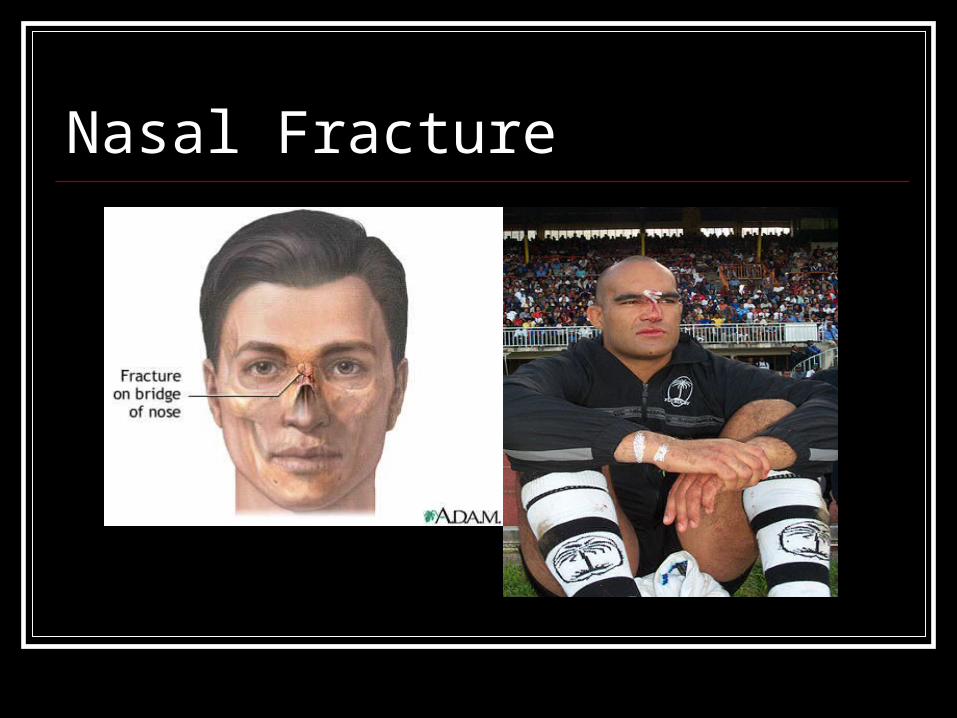
Nasal Fracture
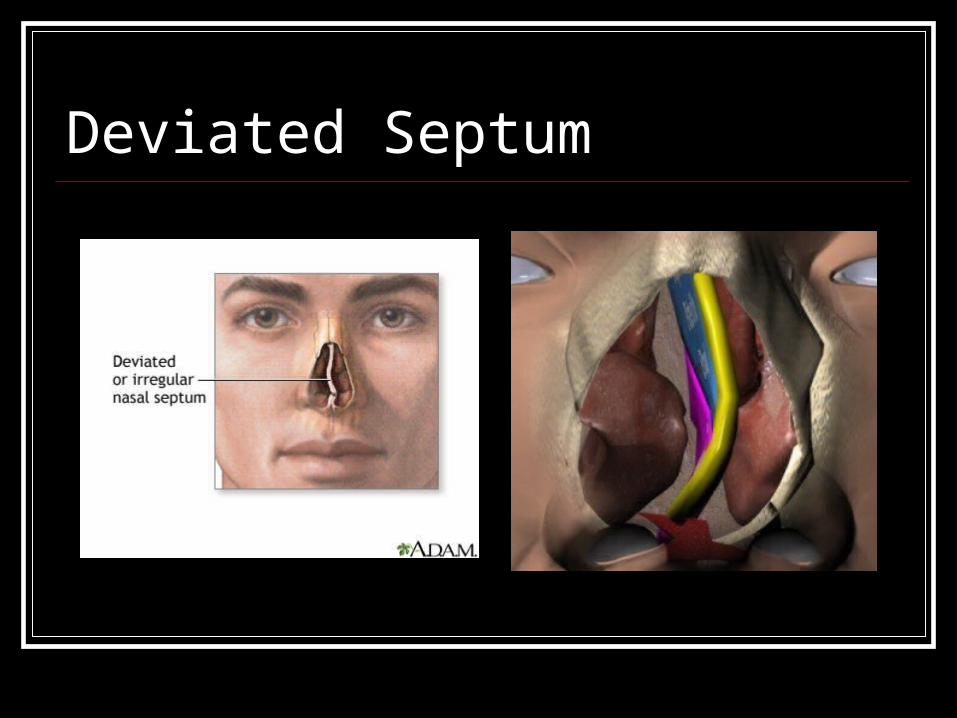
Deviated Septum
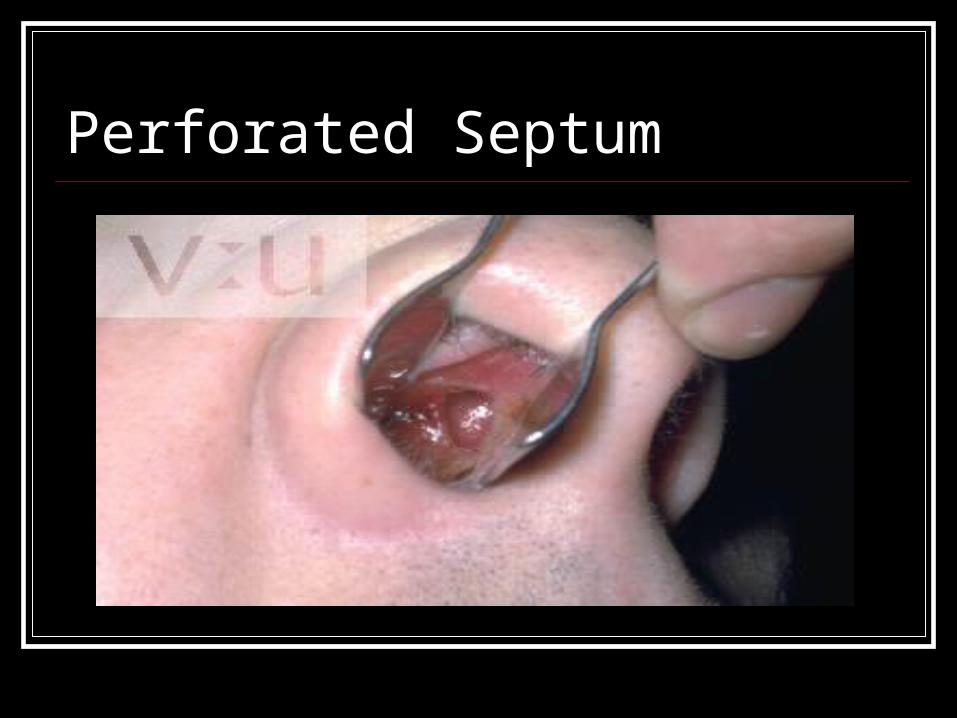
Perforated Septum
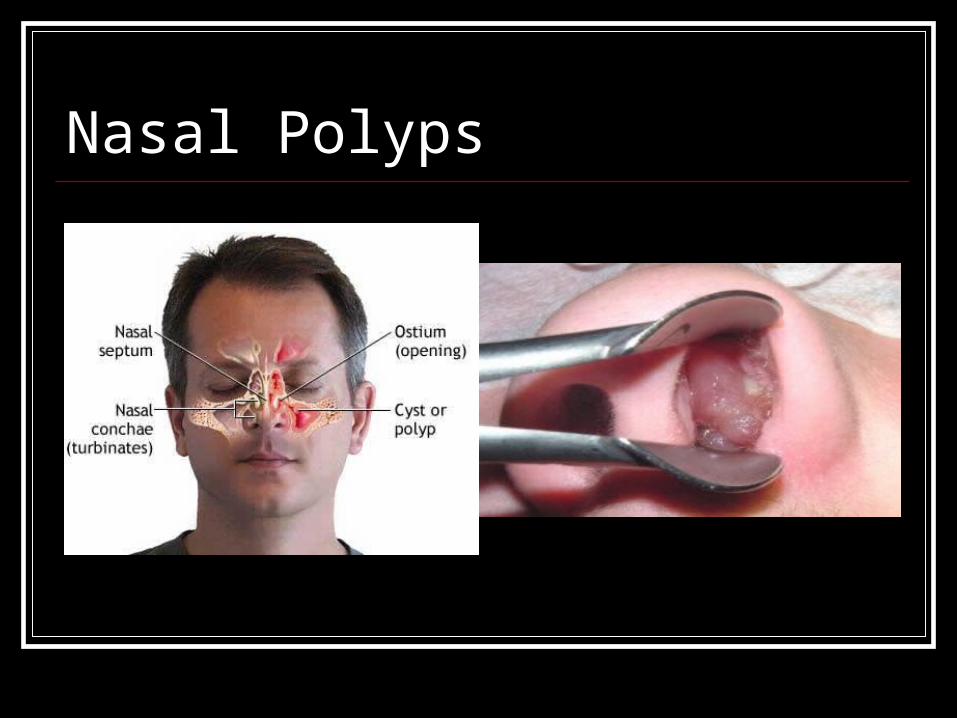
Nasal Polyps
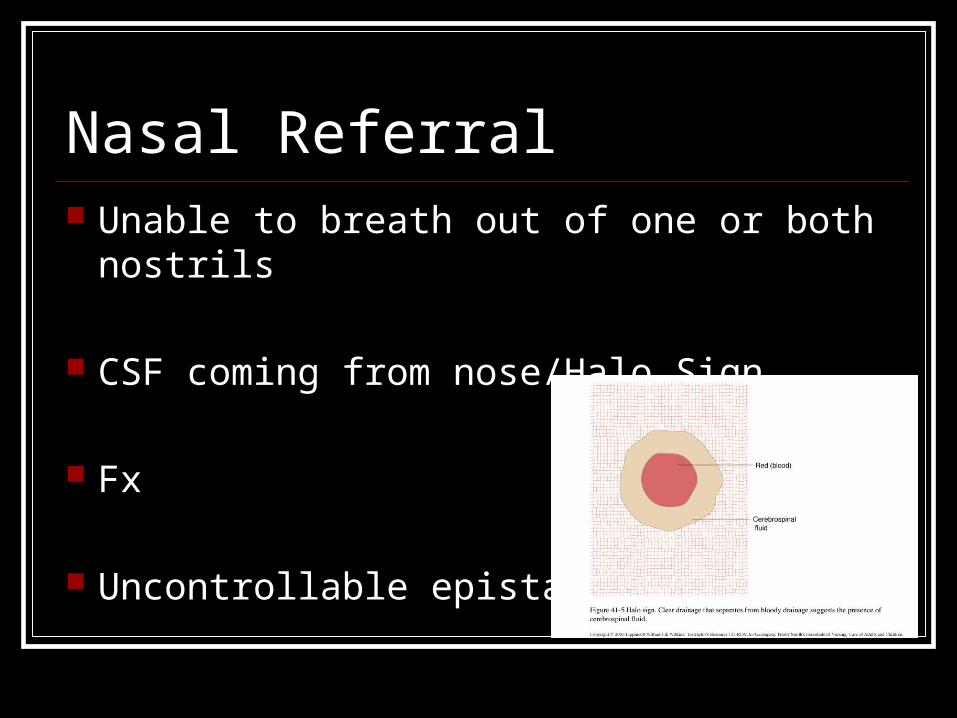
Nasal Referral Unable to breath out of one or both nostrils
CSF coming from nose/Halo Sign
Fx
Uncontrollable epistaxis
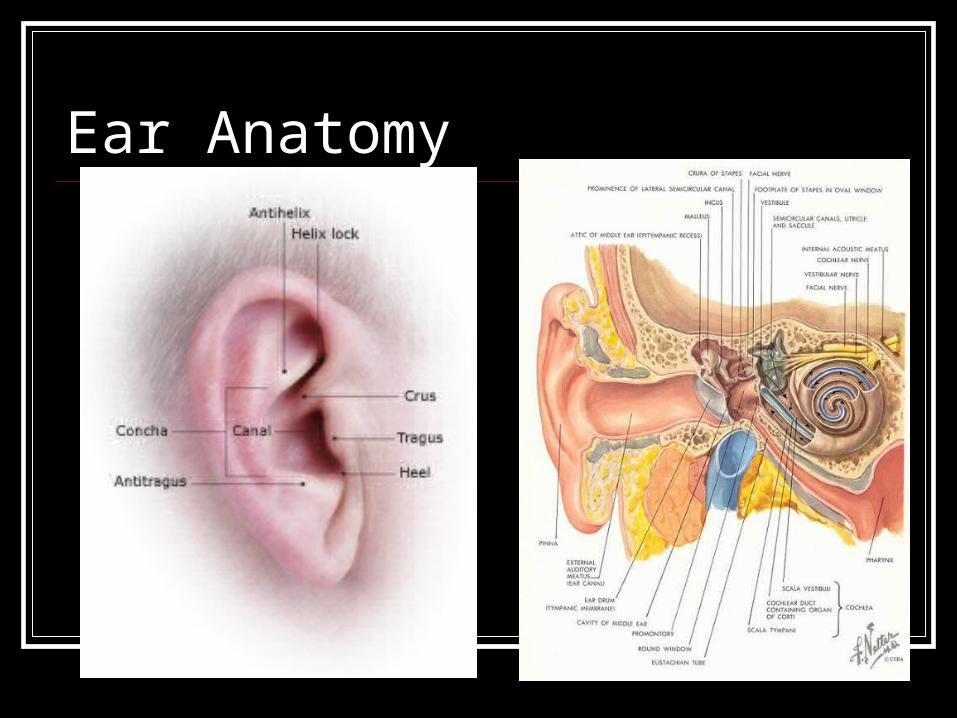
Ear Anatomy
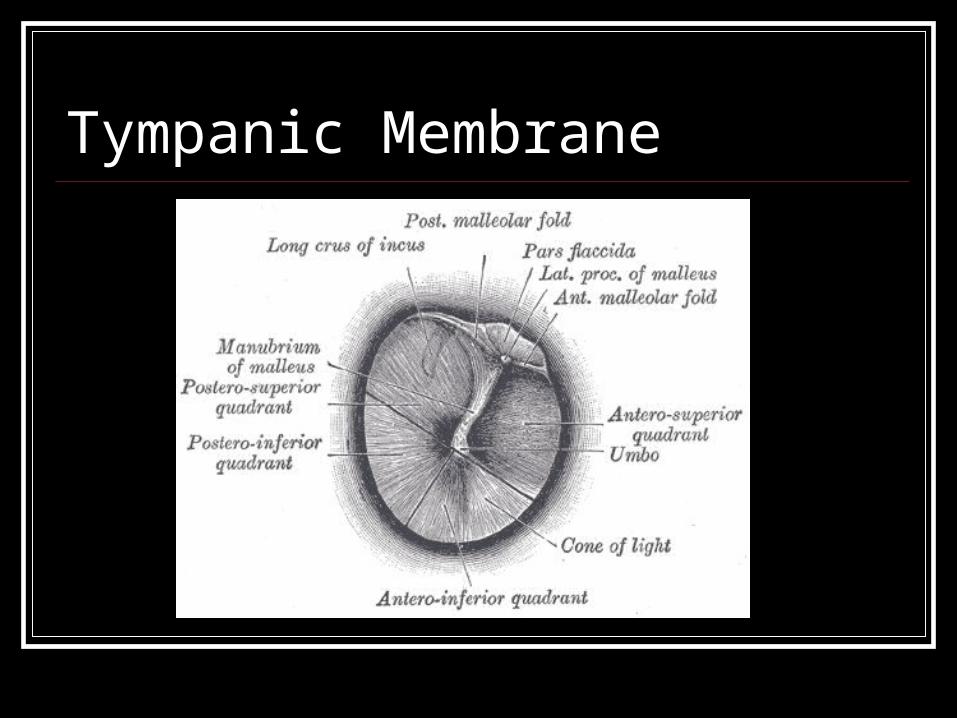
Tympanic Membrane
Use of the Otoscope in Athletic Use of the Otoscope in Athletic TrainingTraining
Objectives Briefly discuss the types and features of the
otoscope Provide an overview of otoscopic assessment
procedures Present a clinical teaching model for teaching
your students to properly use the otoscope Provide educational resources for teaching
otoscopy
Types & Features of the OtoscopeTypes & Features of the Otoscope
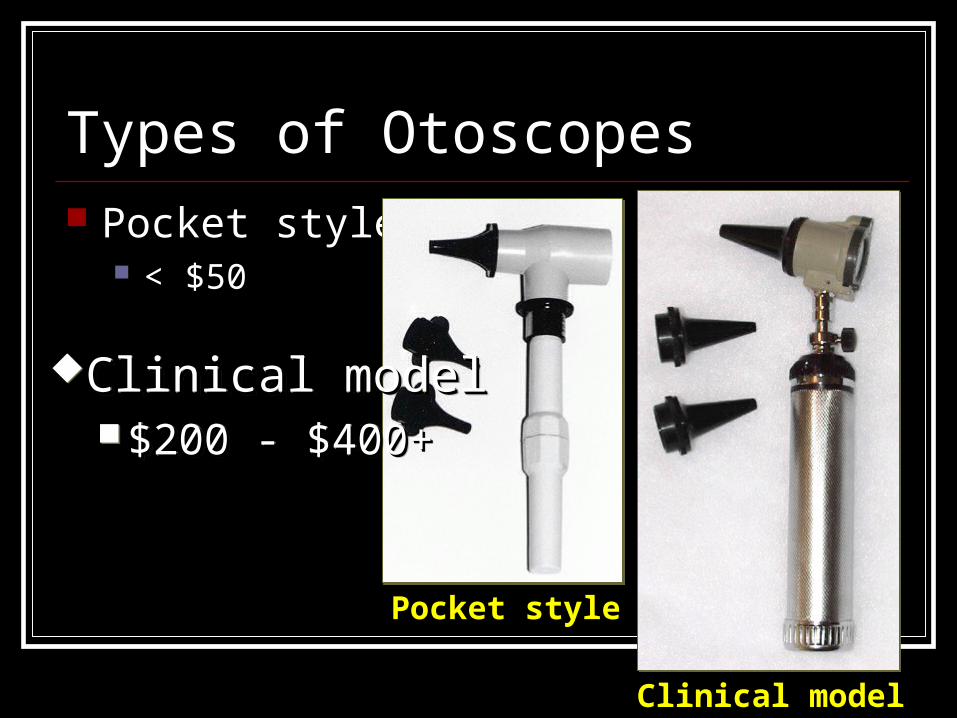
Types of Otoscopes Pocket style
< $50
Pocket stylePocket style
Clinical modelClinical model
Clinical modelClinical model $200 - $400+$200 - $400+
Clinical modelClinical model $200 - $400+$200 - $400+
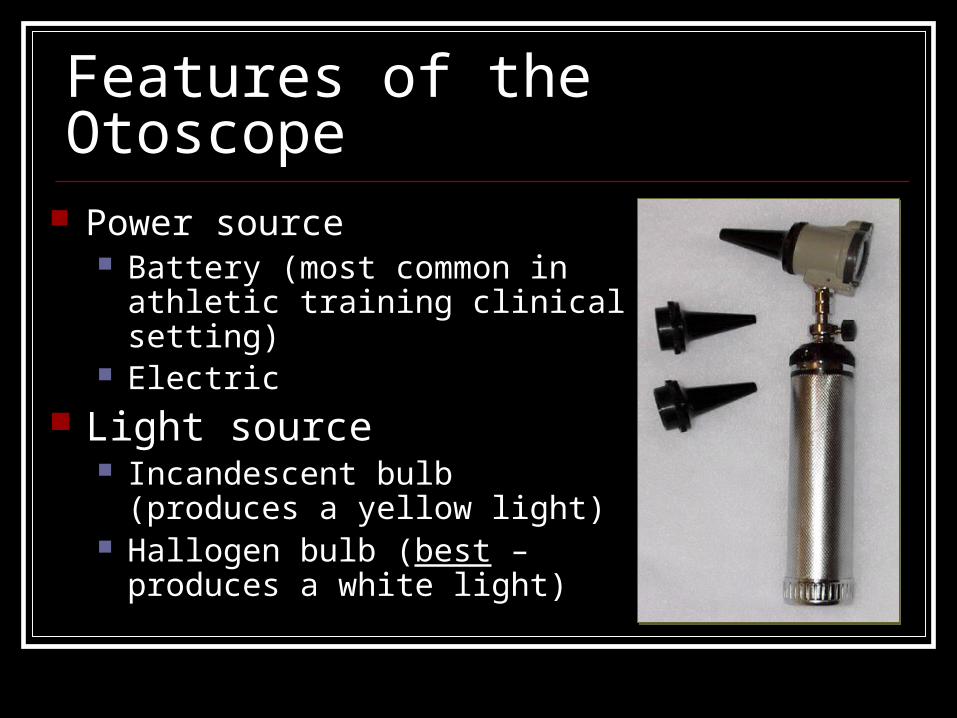
Features of the Otoscope Power source
Battery (most common in athletic training clinical setting)
Electric
Light source Incandescent bulb (produces a
yellow light) Hallogen bulb (best – produces a
white light)
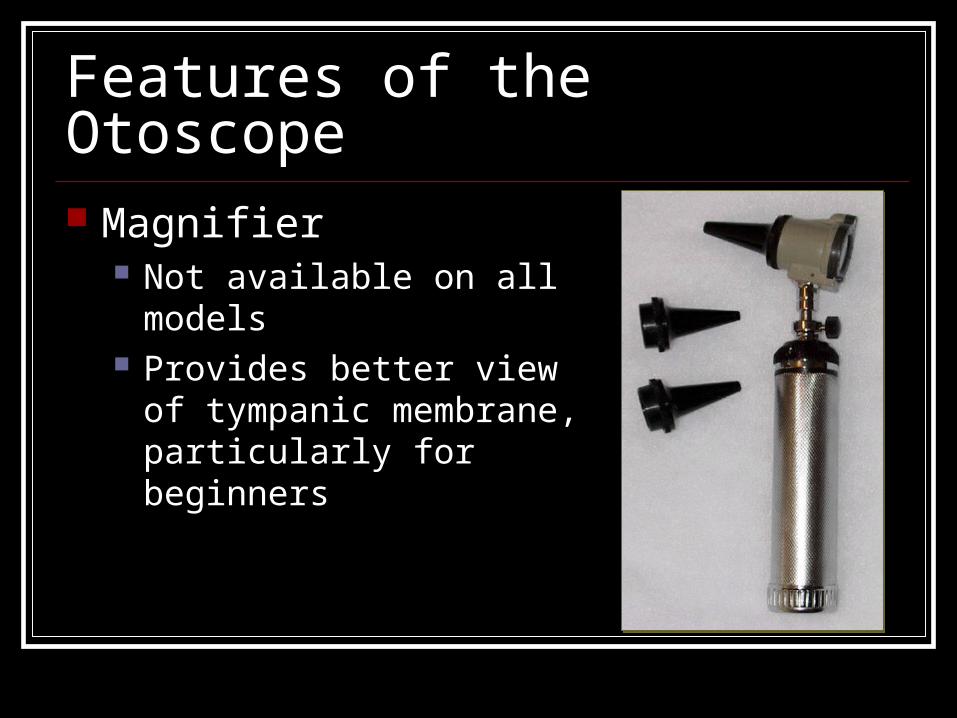
Features of the Otoscope Magnifier
Not available on all models Provides better view of
tympanic membrane, particularly for beginners

Features of the Otoscope Speculum
Variety of sizes Reusable or disposable
Overview of Otoscopic AssessmentOverview of Otoscopic Assessment
Examination of the EarExamination of the Ear History Observation Palpation
Special tests Otoscopic assessment
Examination of the EarExamination of the Ear History
Trauma Allergies, colds, sinus drainage Changes in pressure (flying, diving) Dizziness Changes in hearing Duration of symptoms

Examination of the Ear Observation
Redness Swelling Drainage Foreign object Cuts, scrapes,
bruises
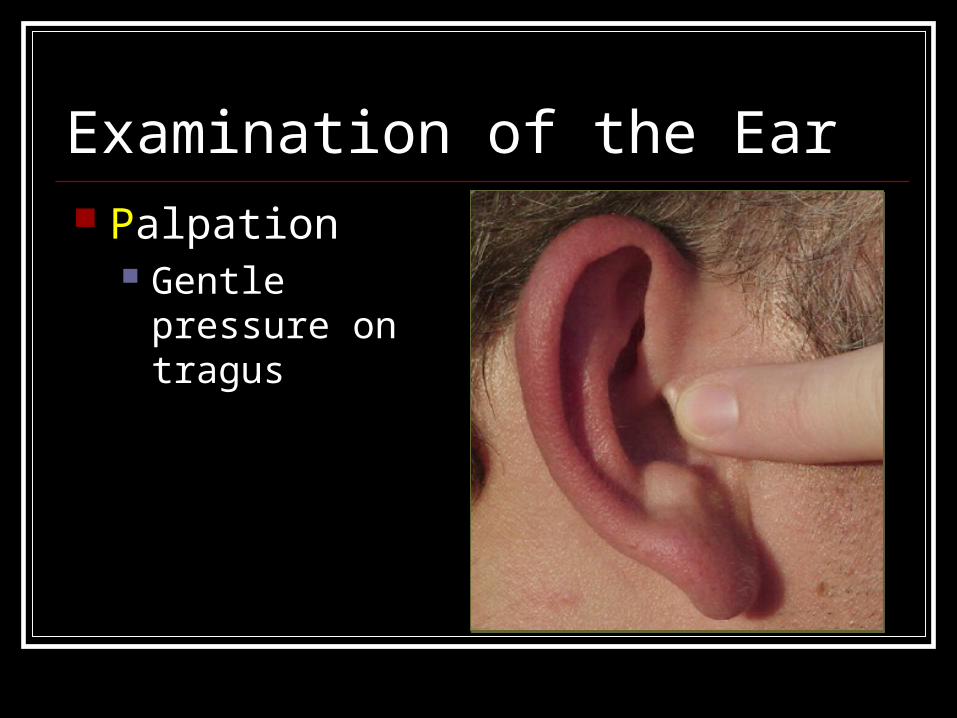
Examination of the Ear Palpation
Gentle pressure on tragus
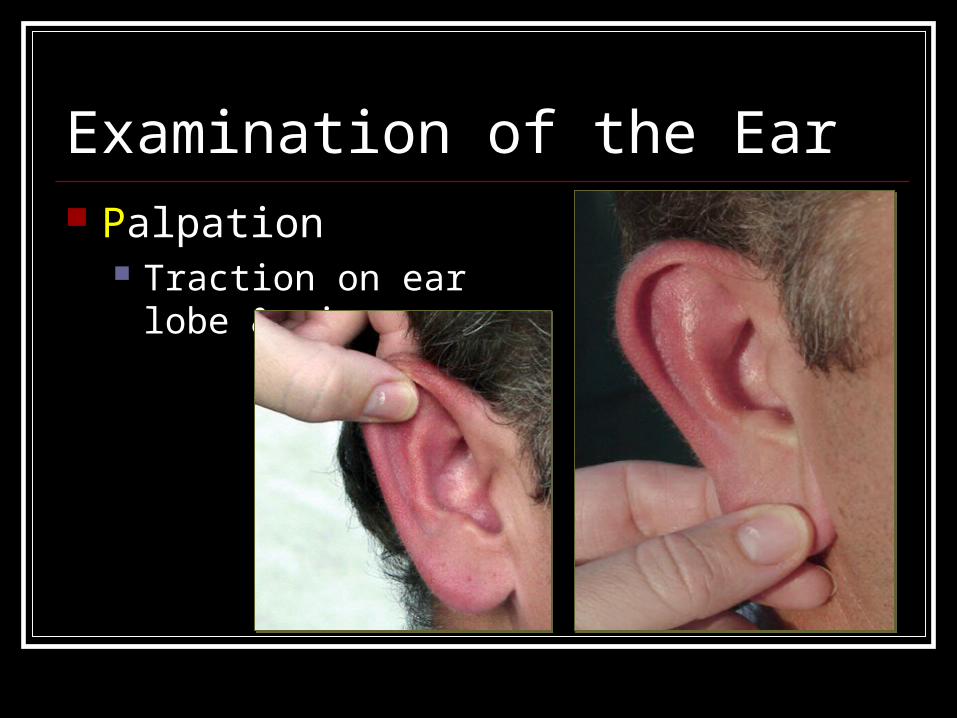
Examination of the Ear Palpation
Traction on ear lobe & pinna
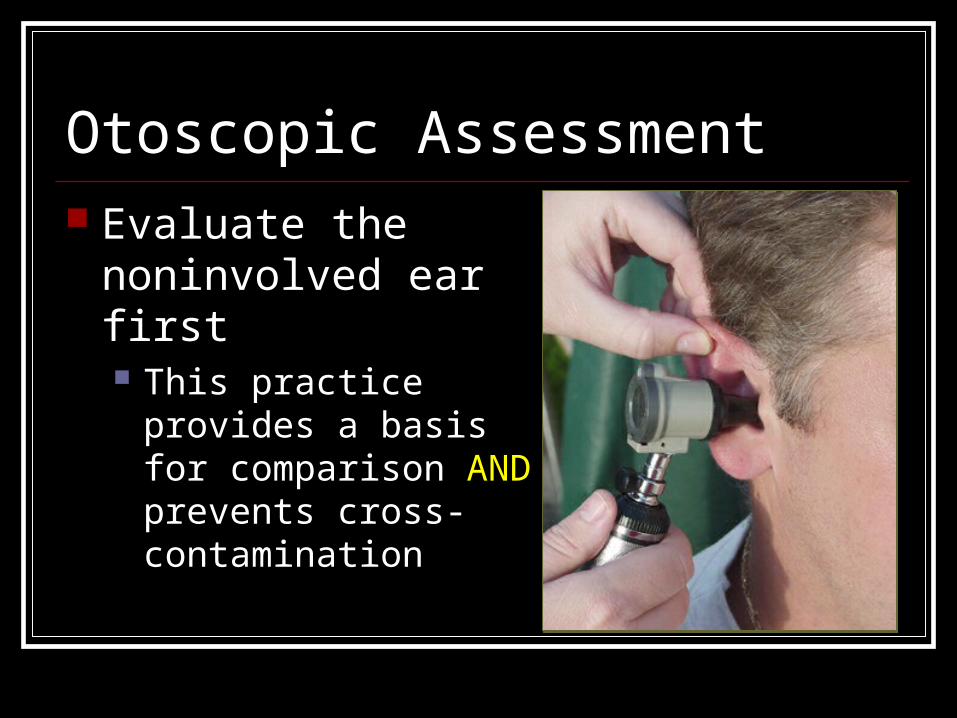
Otoscopic Assessment Evaluate the
noninvolved ear first This practice provides a
basis for comparison AND prevents cross-contamination
Otoscopic Assessment Step 1:
Place your patient in a seated position with his/her head turned slightly downward and away from the ear to be examined
Otoscopic Assessment Step 1 (cont.):
the “puppy position” (puppies always cock their heads to the side when you talk to them)
Otoscopic Assessment Step 2:
Select the largest possible speculum that can be comfortably inserted into the ear
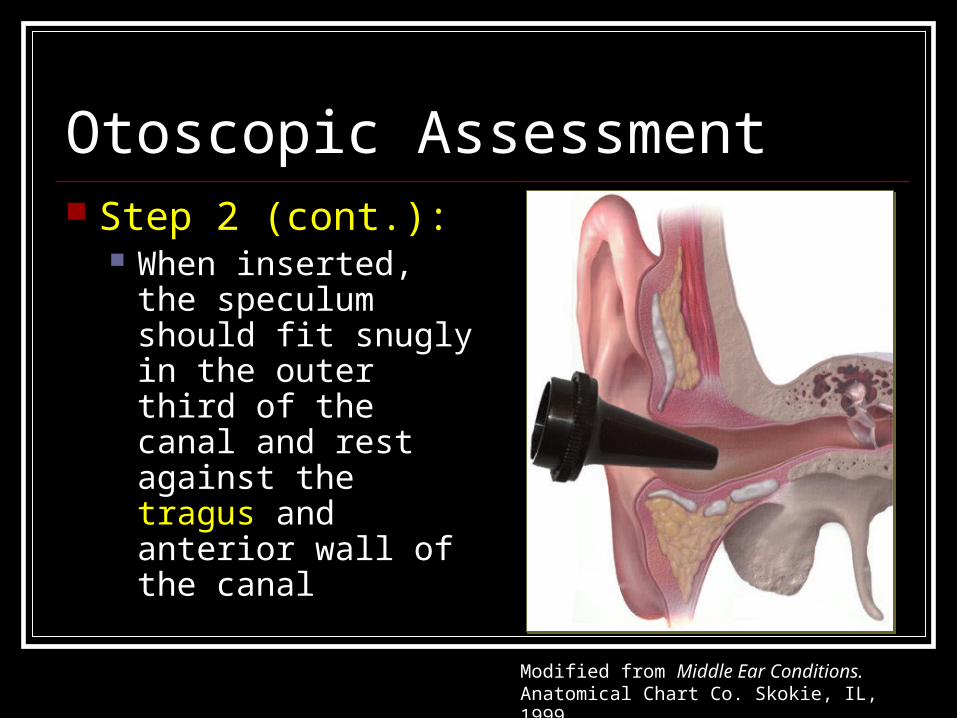
Otoscopic Assessment Step 2 (cont.):
When inserted, the speculum should fit snugly in the outer third of the canal and rest against the tragus and anterior wall of the canal
Modified from Middle Ear Conditions. Anatomical Chart Co. Skokie, IL, 1999.
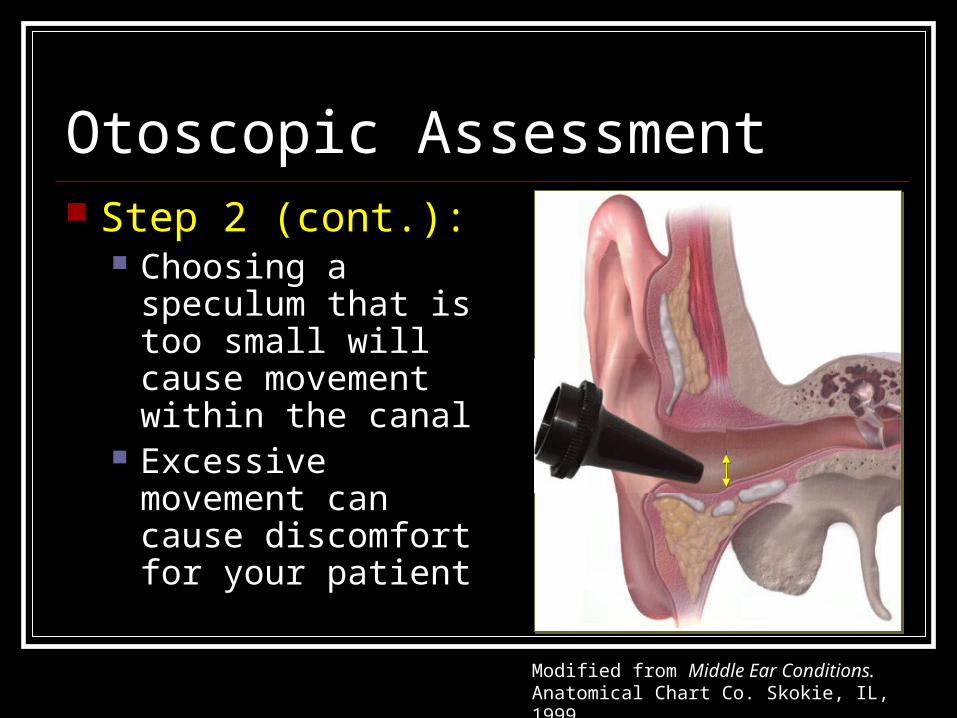
Otoscopic Assessment Step 2 (cont.):
Choosing a speculum that is too small will cause movement within the canal
Excessive movement can cause discomfort for your patient
Modified from Middle Ear Conditions. Anatomical Chart Co. Skokie, IL, 1999.
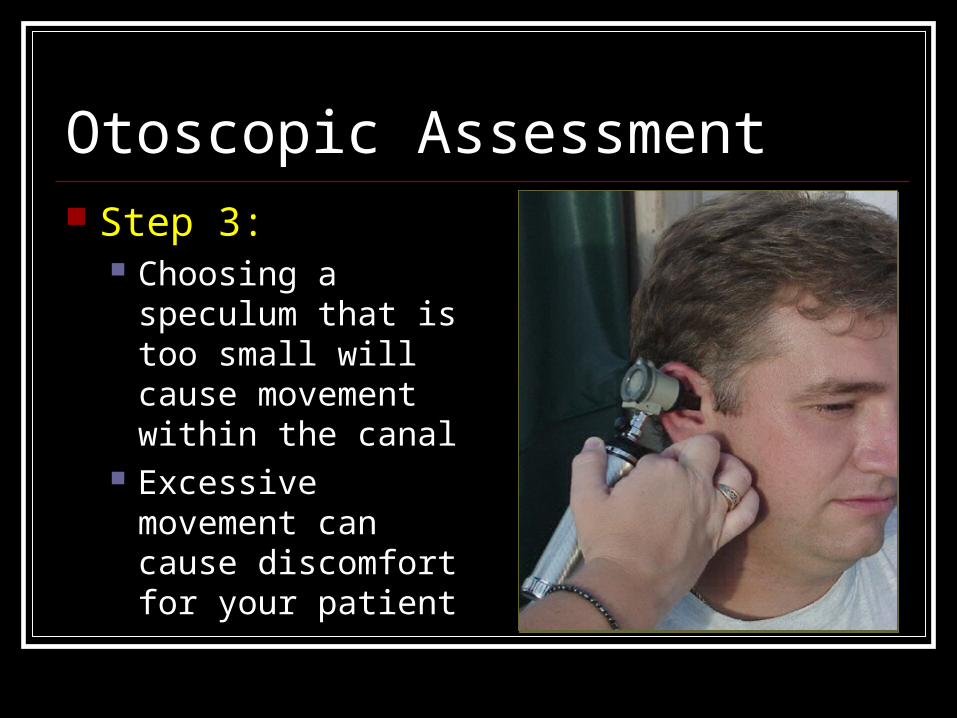
Otoscopic Assessment Step 3:
Choosing a speculum that is too small will cause movement within the canal
Excessive movement can cause discomfort for your patient
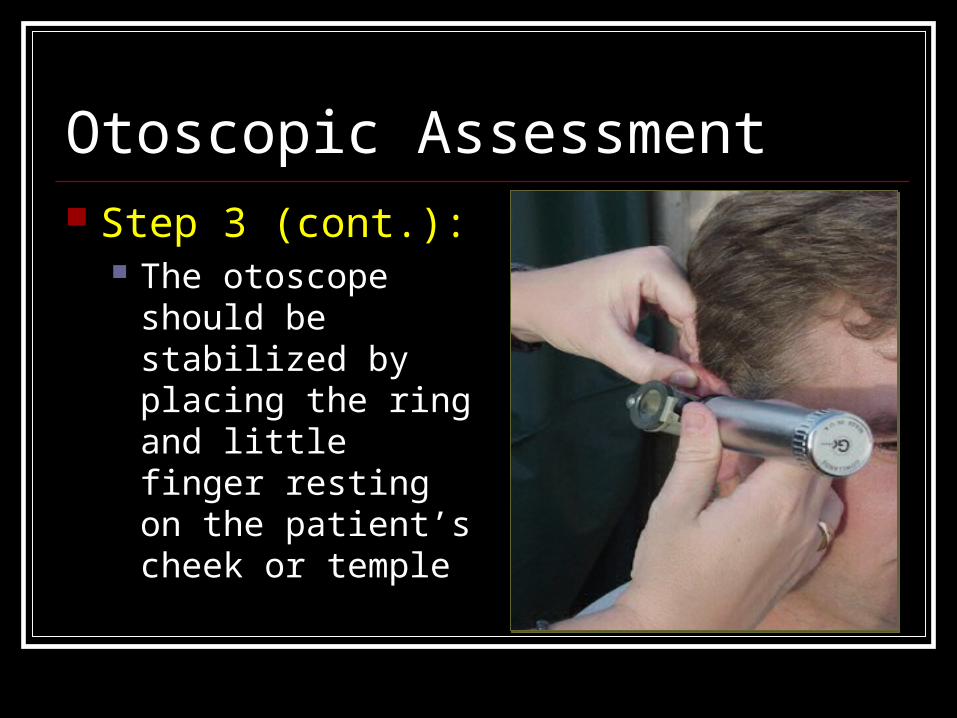
Otoscopic Assessment Step 3 (cont.):
The otoscope should be stabilized by placing the ring and little finger resting on the patient’s cheek or temple
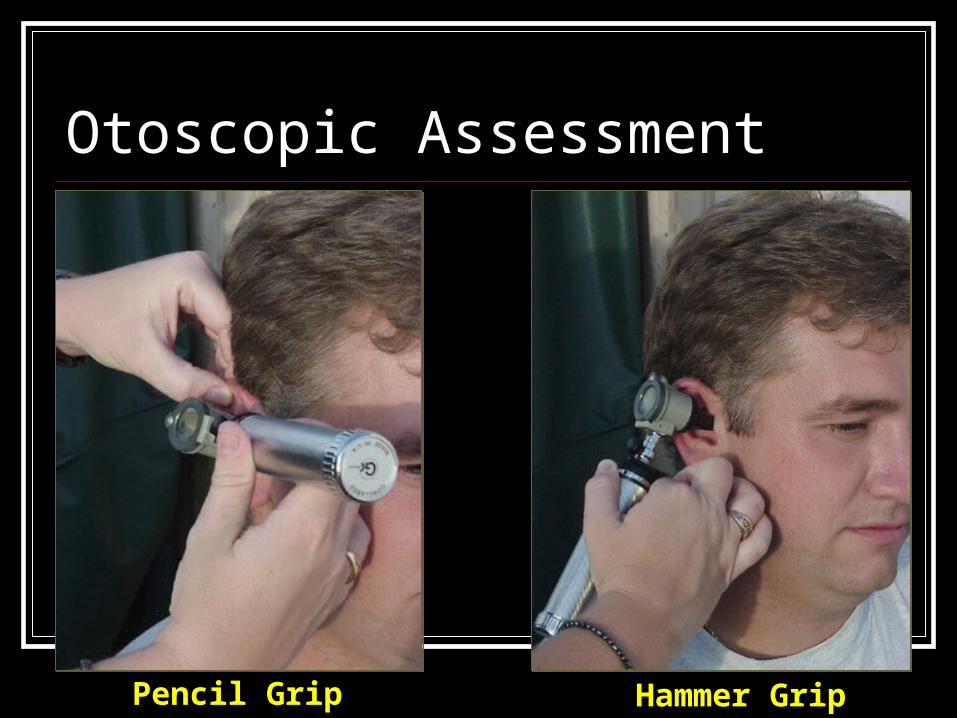
Otoscopic Assessment
Pencil Grip Hammer Grip
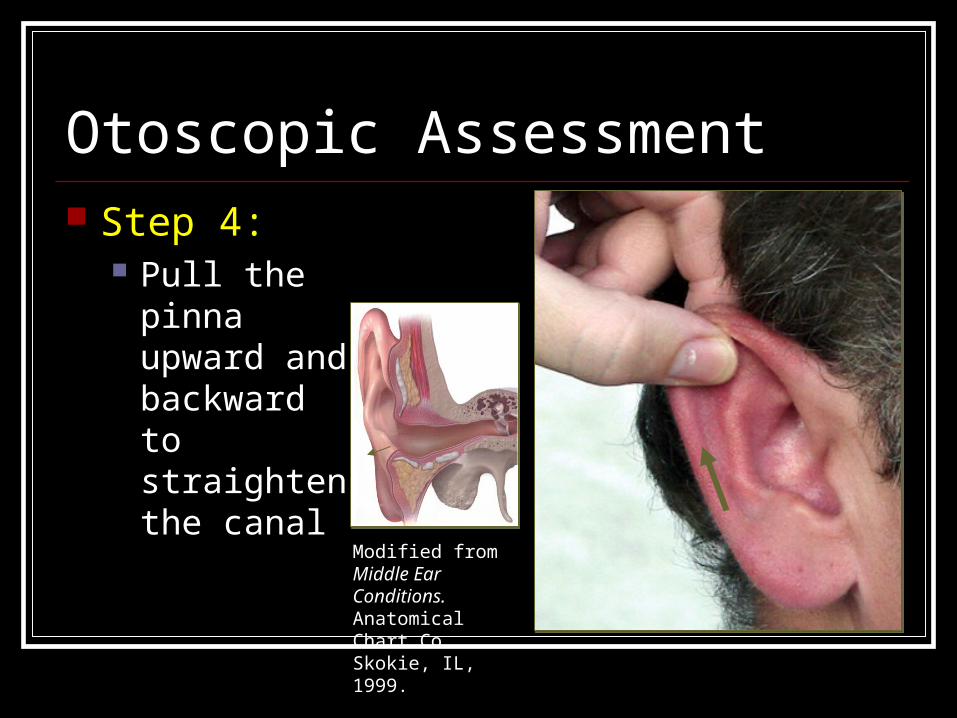
Otoscopic Assessment Step 4:
Pull the Pull the pinna pinna upward and upward and backward to backward to straighten straighten the canalthe canal
Modified from Middle Ear Conditions. Anatomical Chart Co. Skokie, IL, 1999.
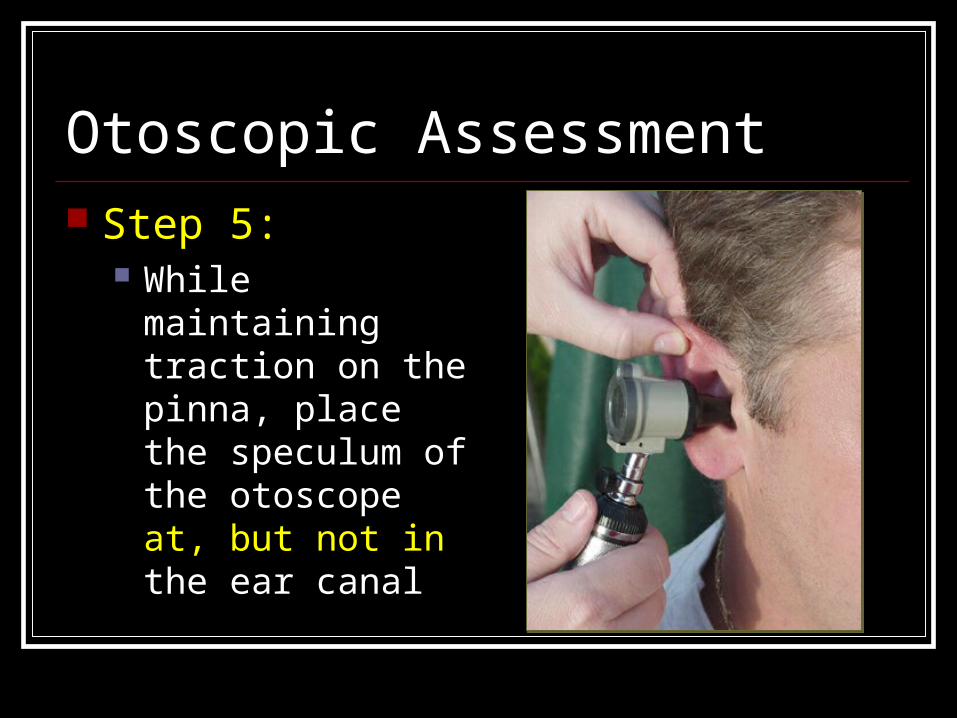
Otoscopic Assessment Step 5:
While maintaining traction on the pinna, place the speculum of the otoscope at, but not in the ear canal
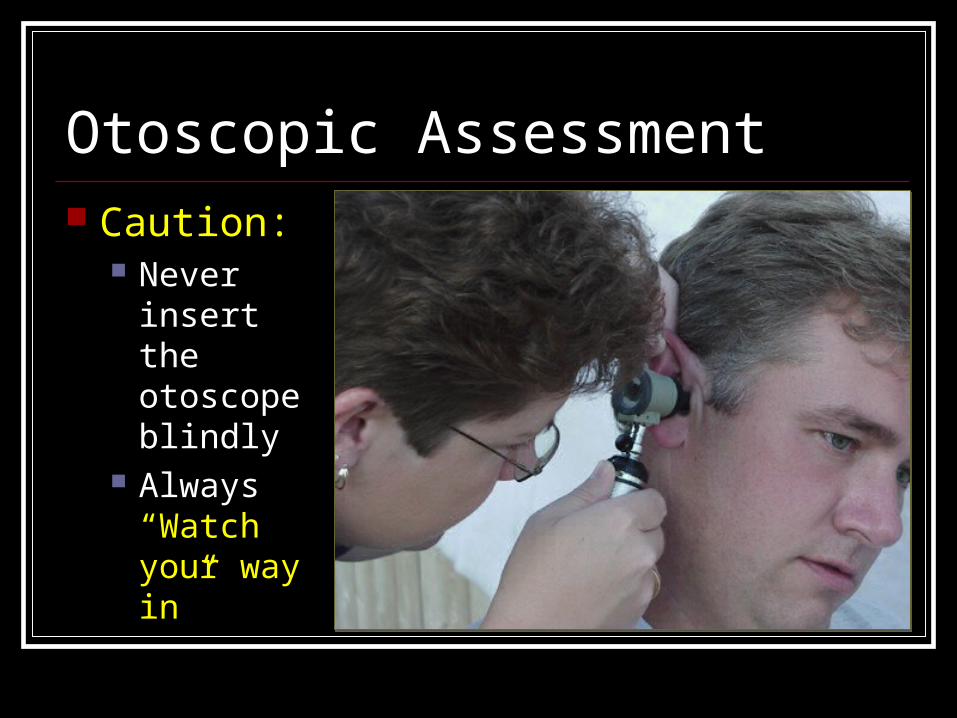
Otoscopic Assessment Caution:
Never insert the otoscope blindly
Always“Watch your way in”
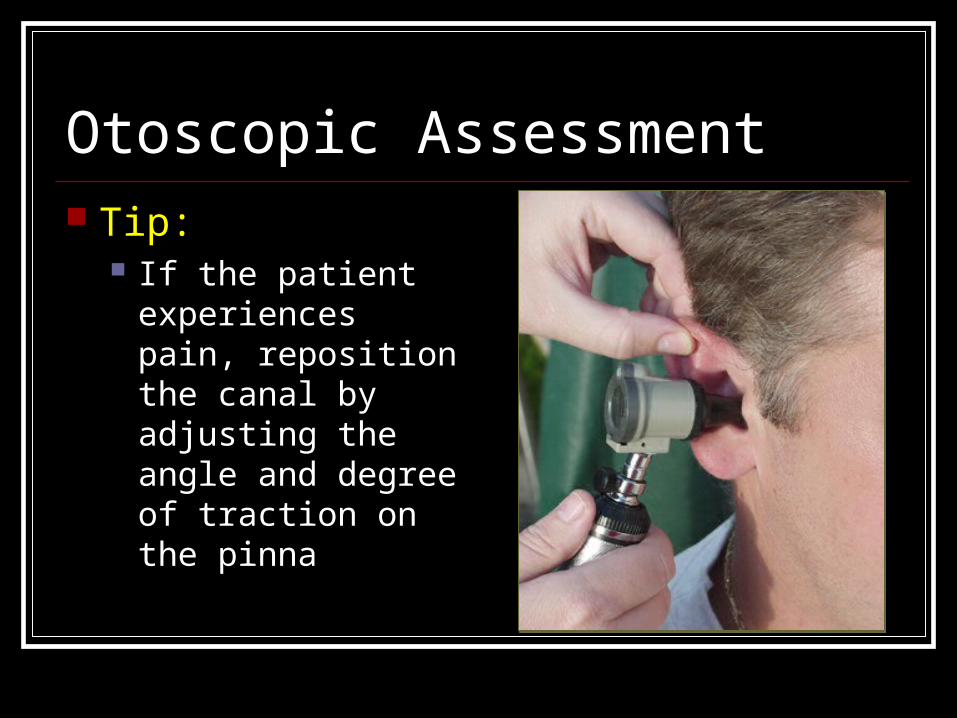
Otoscopic Assessment Tip:
If the patient experiences pain, reposition the canal by adjusting the angle and degree of traction on the pinna
Otoscopic Assessment Caution:
If the patient’s If the patient’s discomfort persists discomfort persists even after even after readjustment of the readjustment of the canal, halt the canal, halt the examination and examination and refer the patient to refer the patient to a physician.a physician.
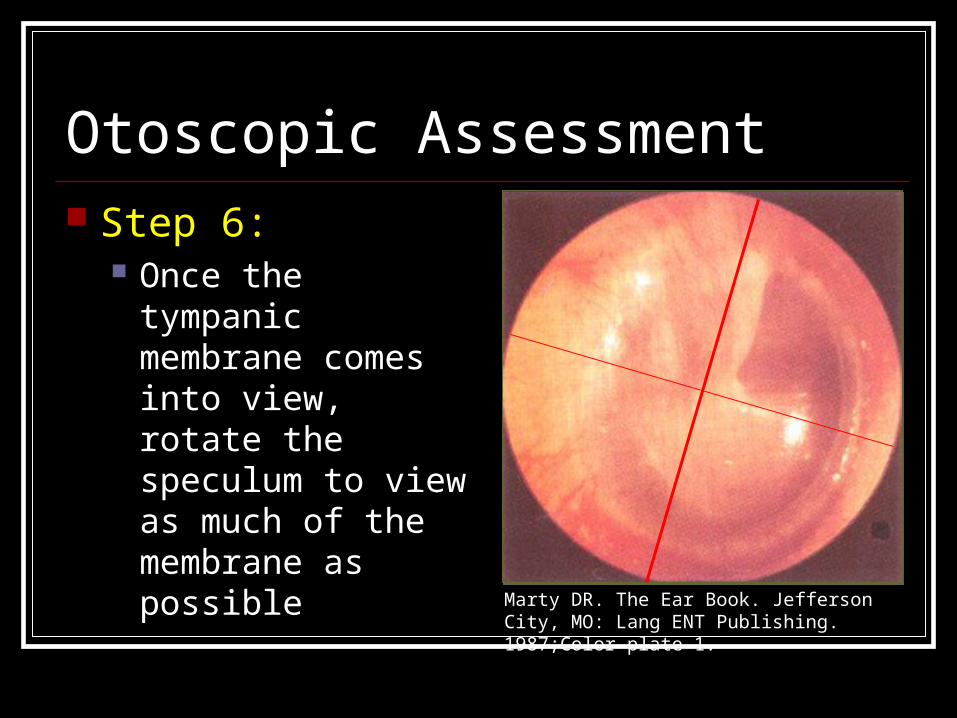
Otoscopic Assessment Step 6:
Once the tympanic membrane comes into view, rotate the speculum to view as much of the membrane as possible
Marty DR. The Ear Book. Jefferson City, MO: Lang ENT Publishing. 1987;Color plate 1.
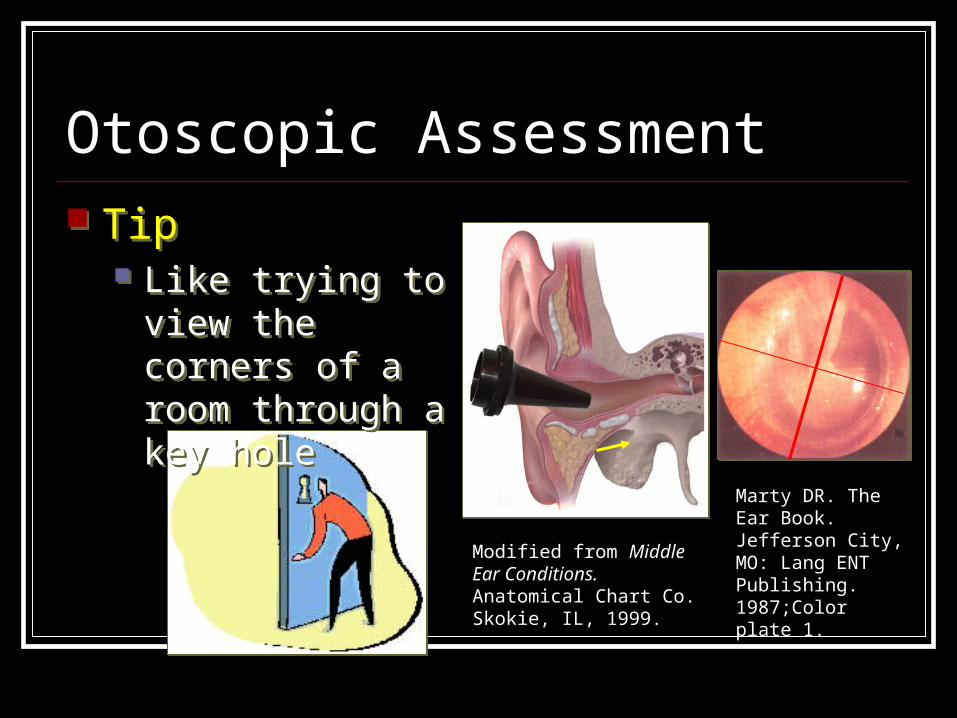
Otoscopic Assessment Tip
Like trying to view the corners of a room through a key hole
Tip Like trying to view
the corners of a room through a key hole
Marty DR. The Ear Book. Jefferson City, MO: Lang ENT Publishing. 1987;Color plate 1.
Modified from Middle Ear Conditions. Anatomical Chart Co. Skokie, IL, 1999.
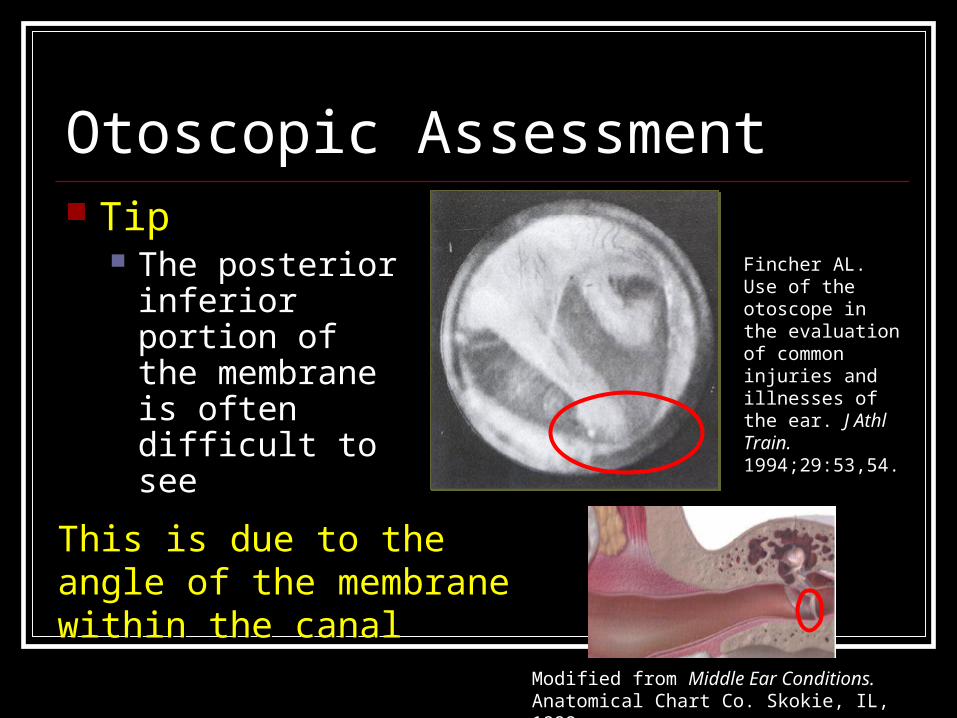
This is due to the angle of the This is due to the angle of the membrane within the canalmembrane within the canal
Otoscopic Assessment Tip
The posterior inferior portion of the membrane is often difficult to see
Fincher AL. Use of the otoscope in the evaluation of common injuries and illnesses of the ear. J Athl Train. 1994;29:53,54.
Modified from Middle Ear Conditions. Anatomical Chart Co. Skokie, IL, 1999.
Otoscopic Assessment
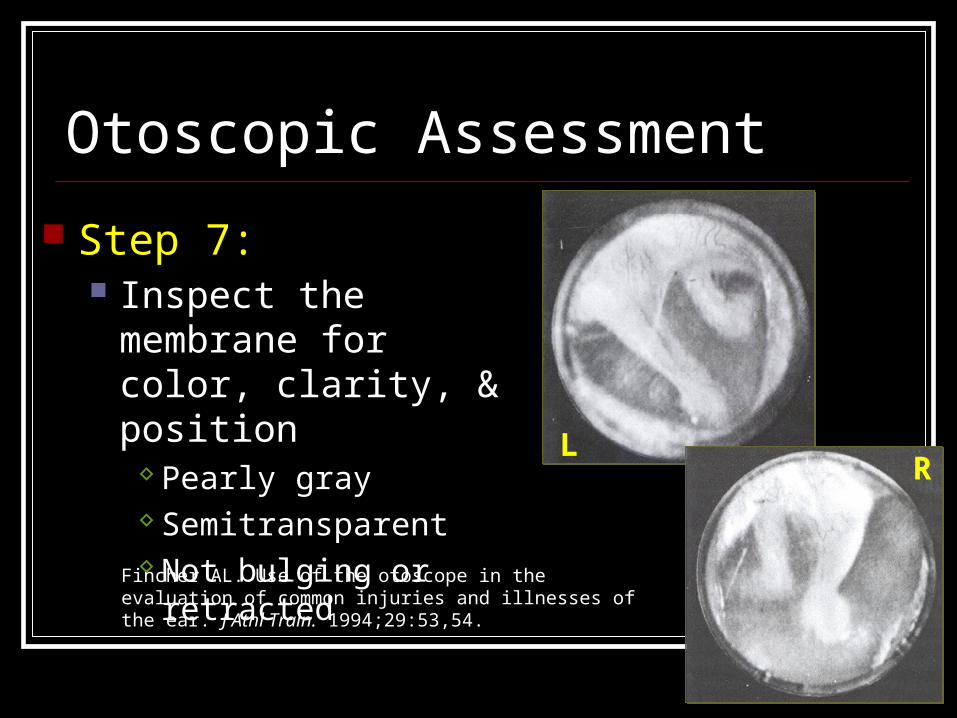
Step 7: Inspect the membrane
for color, clarity, & position
Pearly gray Semitransparent Not bulging or retracted
LR
Fincher AL. Use of the otoscope in the evaluation of common injuries and illnesses of the ear. J Athl Train. 1994;29:53,54.

Otoscopic Assessment
Step 8: Identify key landmarks
LR
Umbo
Short processMalleusMalleus
• ManubriumManubrium• Short process Short process • UmboUmbo
• ManubriumManubrium• Short process Short process • UmboUmbo
Light reflexLight reflex
Fincher AL. Use of the otoscope in the evaluation of common injuries and illnesses of the ear. J Athl Train. 1994;29:53,54.
Otoscopic Assessment
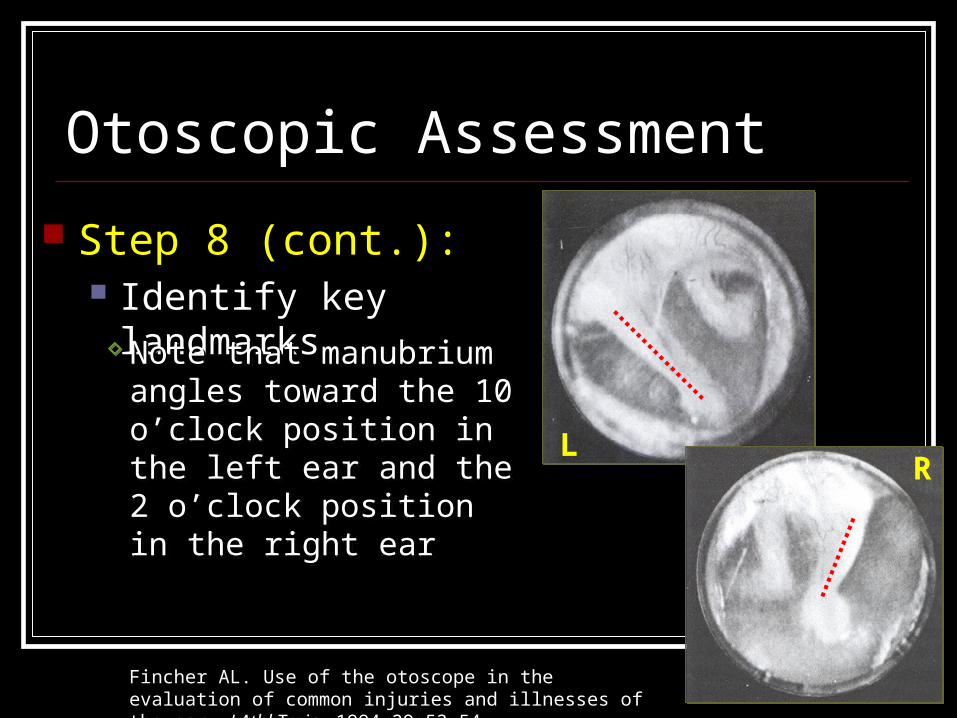
Step 8 (cont.): Identify key landmarks
LR
Note that manubrium Note that manubrium angles toward the 10 angles toward the 10 o’clock position in the left o’clock position in the left ear and the 2 o’clock ear and the 2 o’clock position in the right earposition in the right ear
Note that manubrium Note that manubrium angles toward the 10 angles toward the 10 o’clock position in the left o’clock position in the left ear and the 2 o’clock ear and the 2 o’clock position in the right earposition in the right ear
Fincher AL. Use of the otoscope in the evaluation of common injuries and illnesses of the ear. J Athl Train. 1994;29:53,54.
Otoscopic Assessment
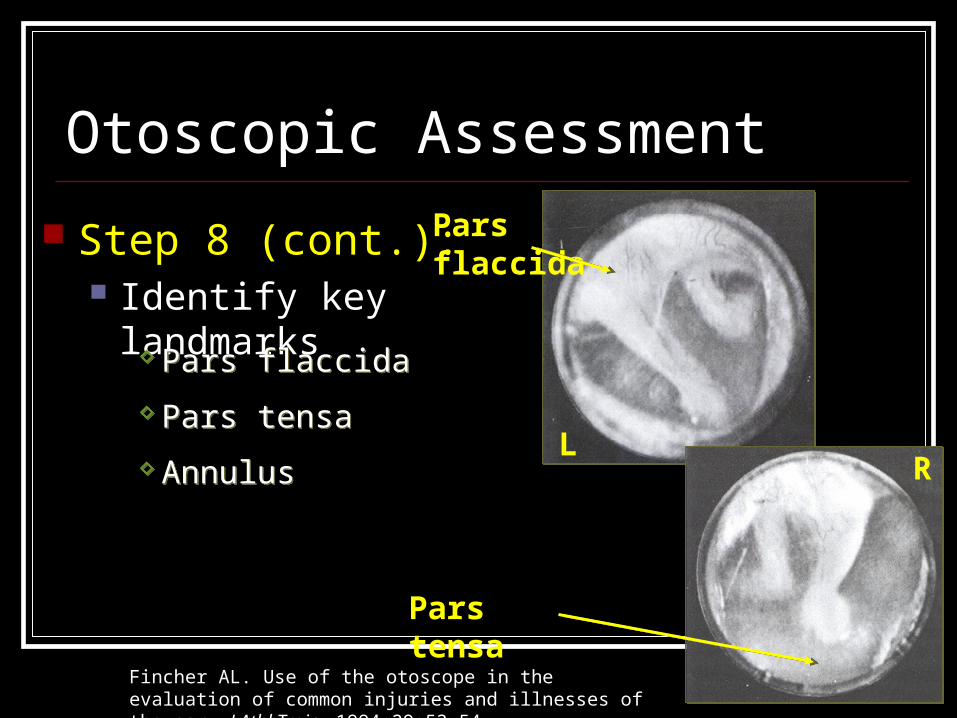
Step 8 (cont.): Identify key landmarks
LR
Pars tensa
Pars flaccida Pars flaccida
Pars tensa Pars tensa
Annulus Annulus
Pars flaccida
Fincher AL. Use of the otoscope in the evaluation of common injuries and illnesses of the ear. J Athl Train. 1994;29:53,54.
Otoscopic Assessment
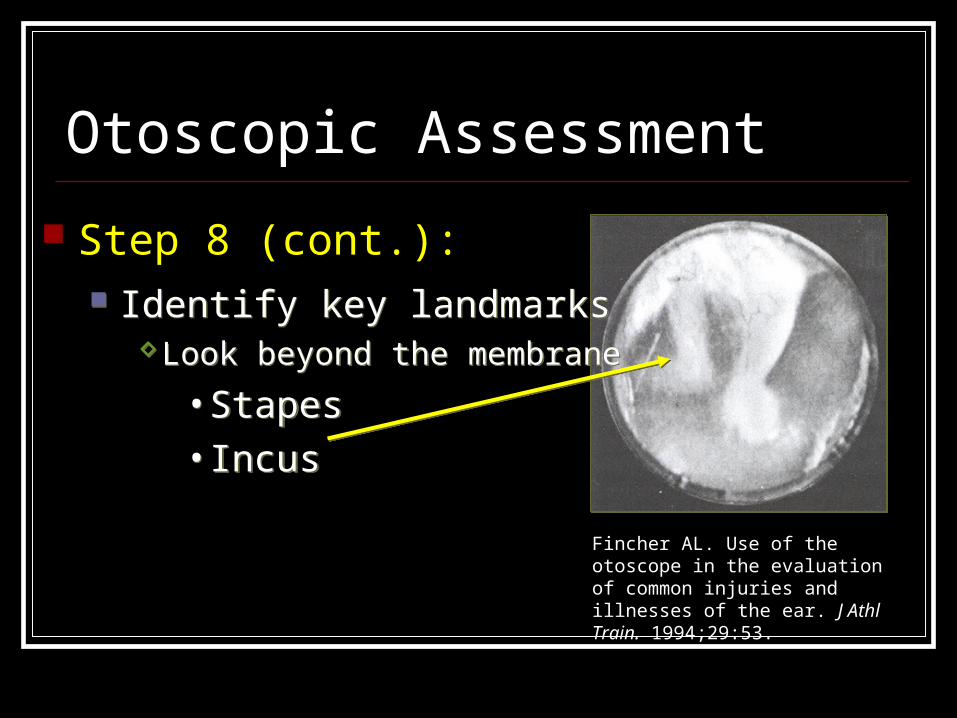
Step 8 (cont.): Identify key landmarks
Look beyond the membrane
• Stapes• Incus
Identify key landmarksLook beyond the membrane
• Stapes• Incus
Fincher AL. Use of the otoscope in the evaluation of common injuries and illnesses of the ear. J Athl Train. 1994;29:53.
Otoscopic Assessment
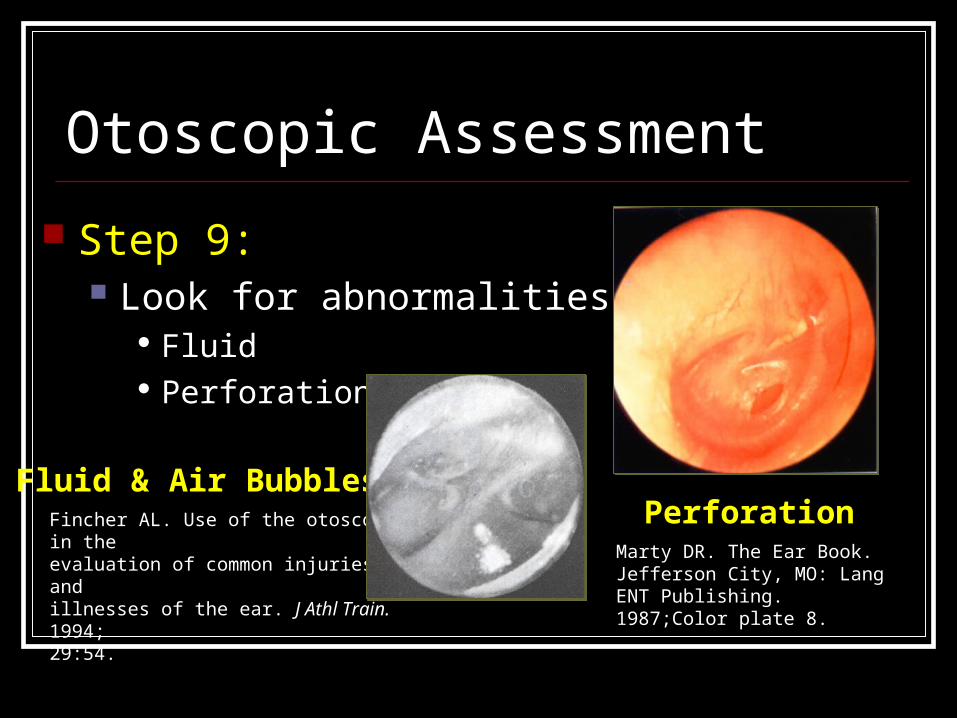
Step 9: Look for abnormalities
Fluid Perforations
PerforationMarty DR. The Ear Book. Jefferson City, MO: Lang ENT Publishing. 1987;Color plate 8.
Fluid & Air BubblesFincher AL. Use of the otoscope in the evaluation of common injuries andillnesses of the ear. J Athl Train. 1994;29:54.
Otoscopic Assessment
Step 10: Work with your team physician to develop
your confidence and skill
PRACTICE, PRACTICE, PRACTICE !!!
You must look at many ears to develop to become comfortable with “normal”
Ear Pathology Hematoma Auris Otitis Externa Otitis Media Perforated/ruptured tympanic membrane
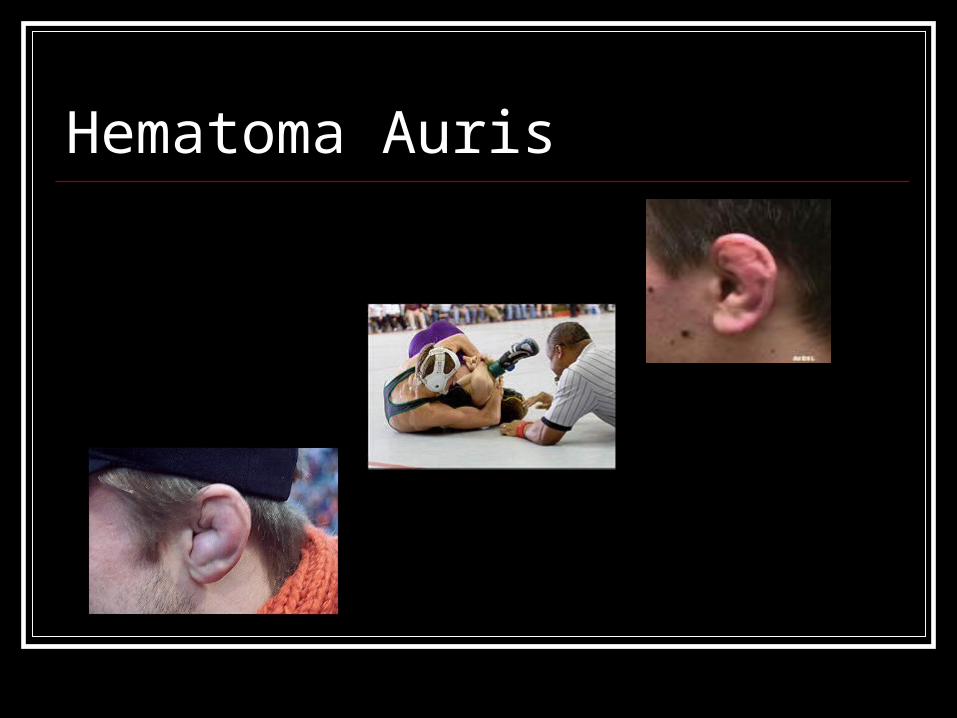
Hematoma Auris
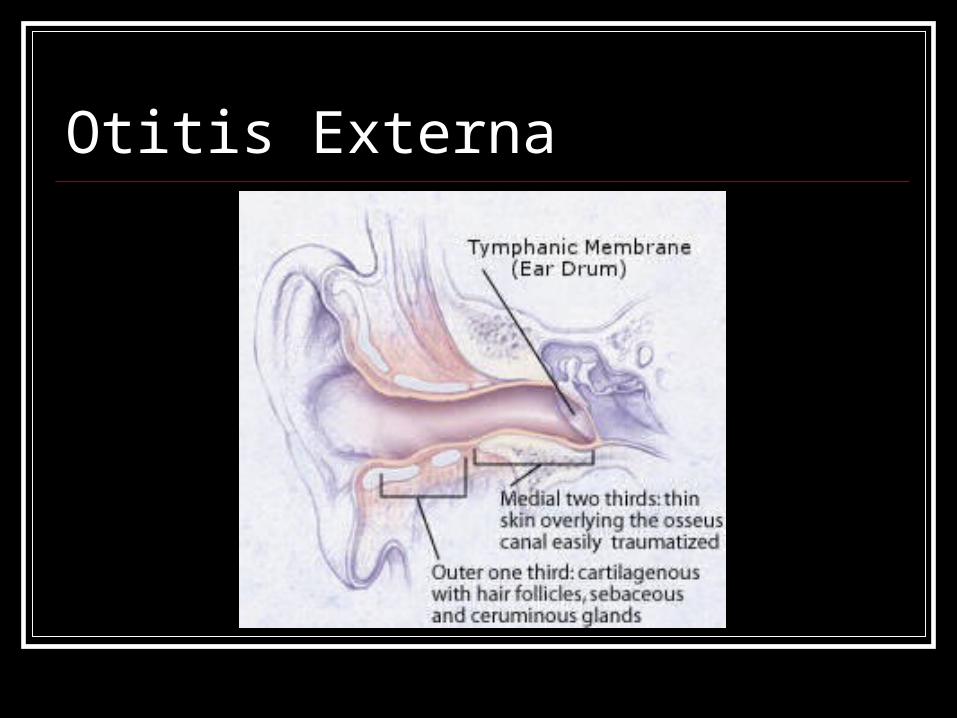
Otitis Externa
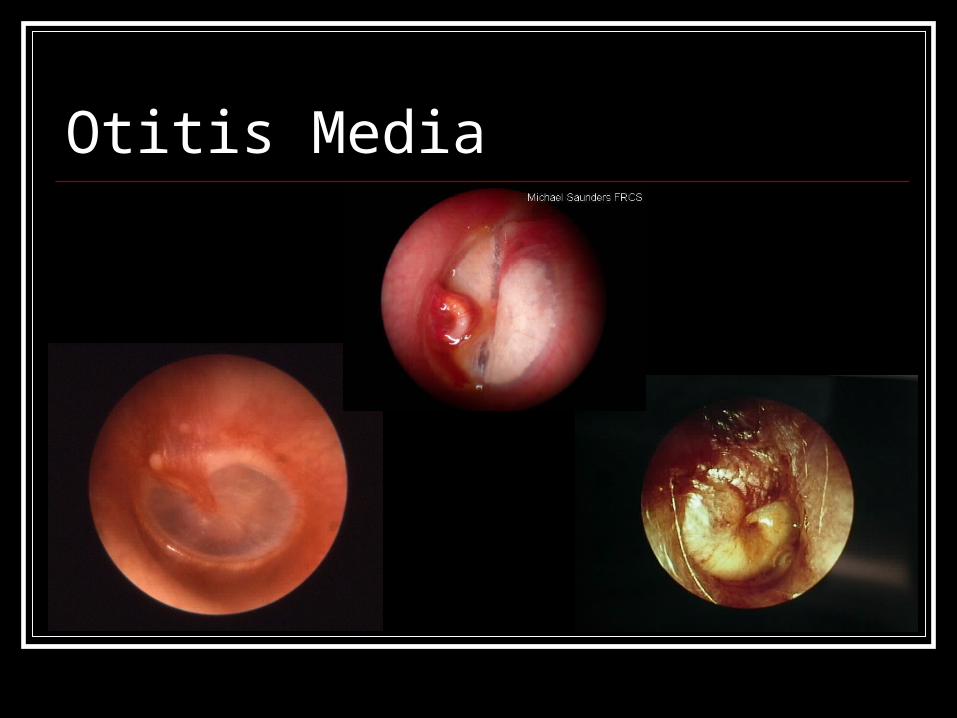
Otitis Media
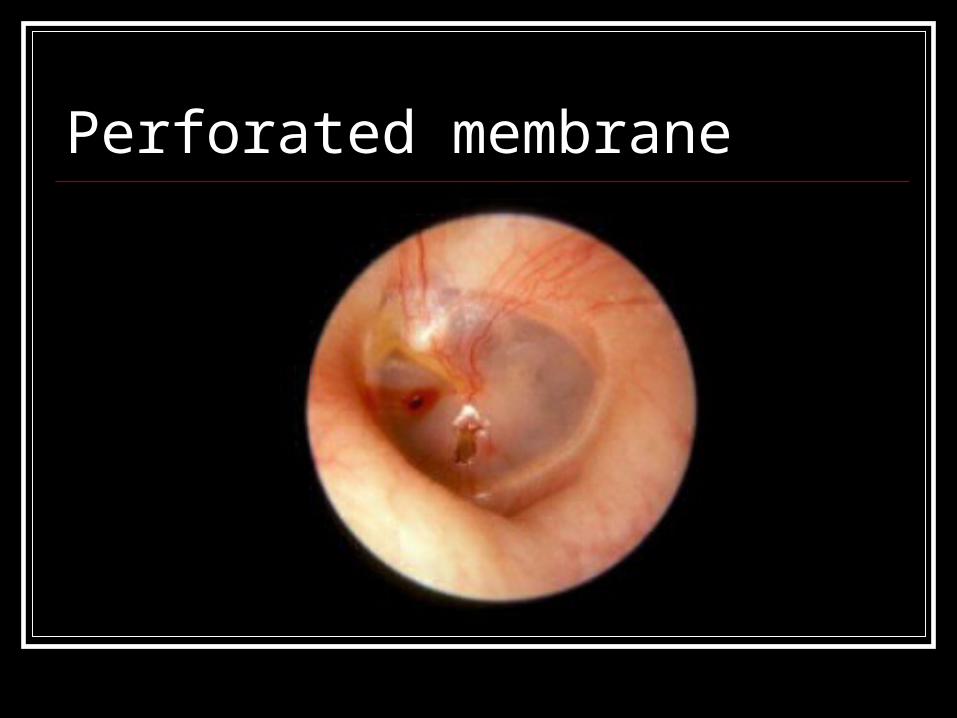
Perforated membrane
Ear Referral Blood or CSF coming from ear
Battle’s sign
Hearing loss or diminished in one or both ears
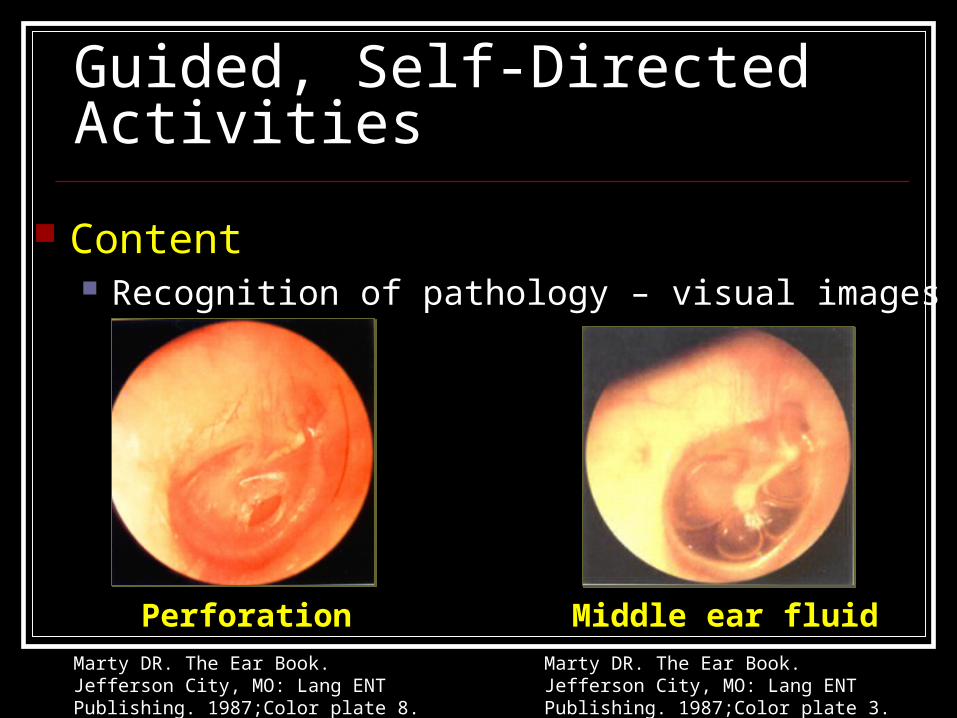
Guided, Self-Directed Activities
Content Recognition of pathology – visual images
PerforationMarty DR. The Ear Book. Jefferson City, MO: Lang ENT Publishing. 1987;Color plate 8.
Middle ear fluidMarty DR. The Ear Book. Jefferson City, MO: Lang ENT Publishing. 1987;Color plate 3.
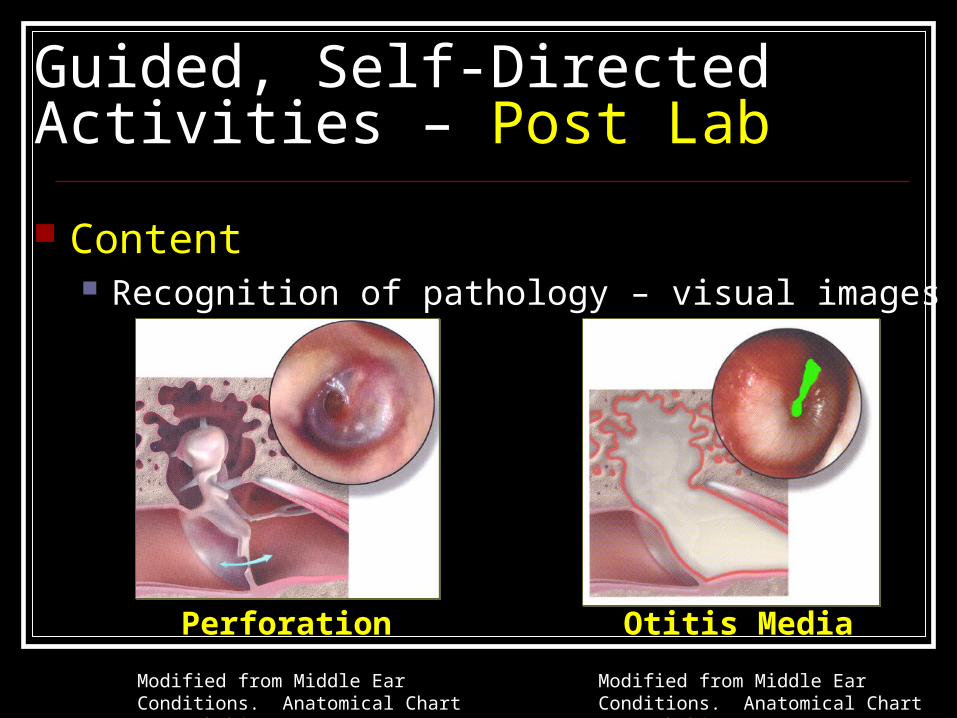
Guided, Self-Directed Activities – Post Lab
Content Recognition of pathology – visual images
Perforation
Modified from Middle Ear Conditions. Anatomical Chart Co., Skokie, IL. 1999.
Otitis Media
Modified from Middle Ear Conditions. Anatomical Chart Co., Skokie, IL. 1999.
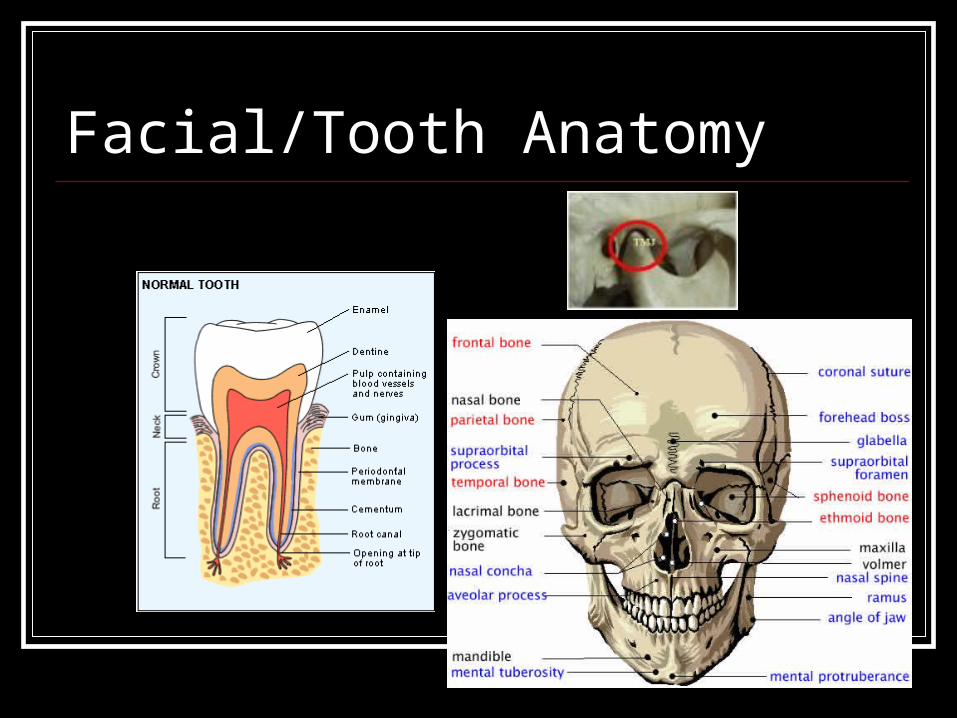
Facial/Tooth Anatomy
Tooth Pathology Tooth Fx Jaw Fx Tooth Intrusion Tooth Luxation Tooth Extrusion
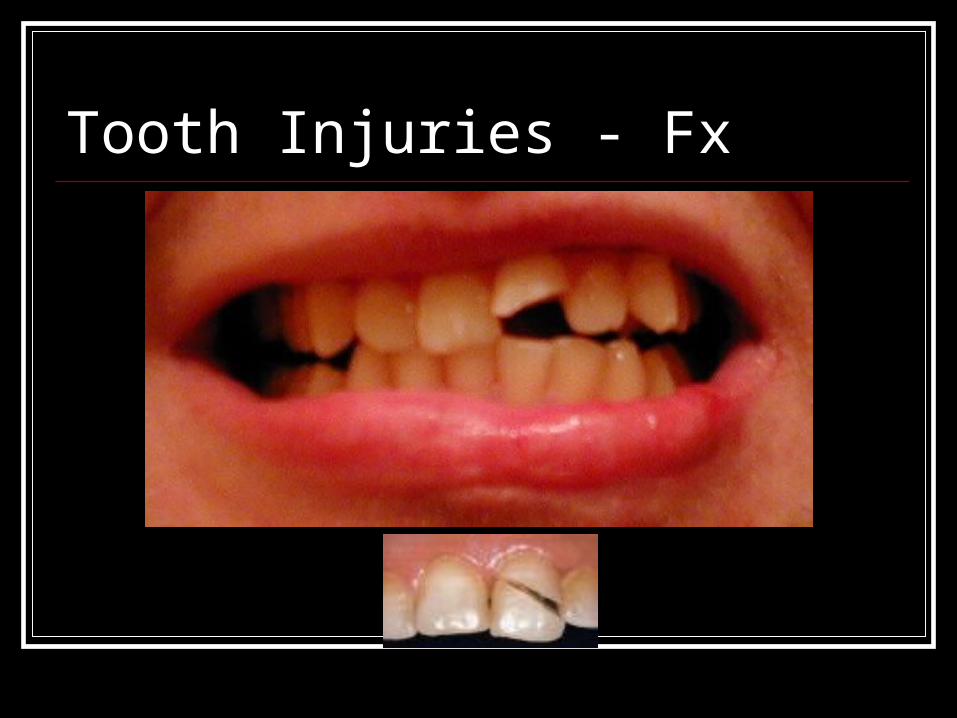
Tooth Injuries - Fx

Jaw Fx
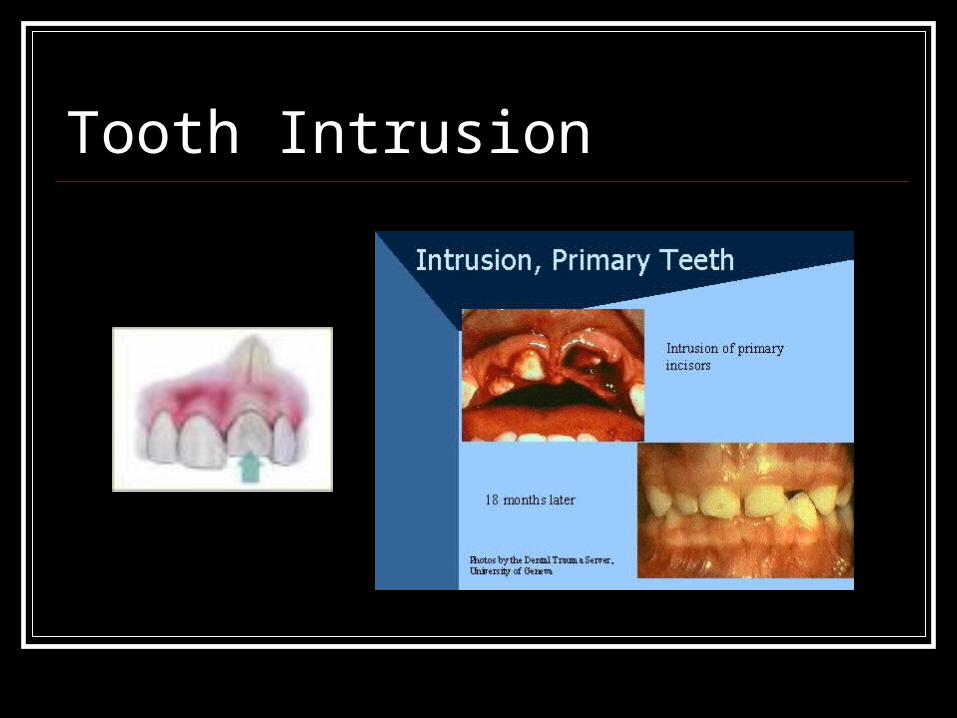
Tooth Intrusion
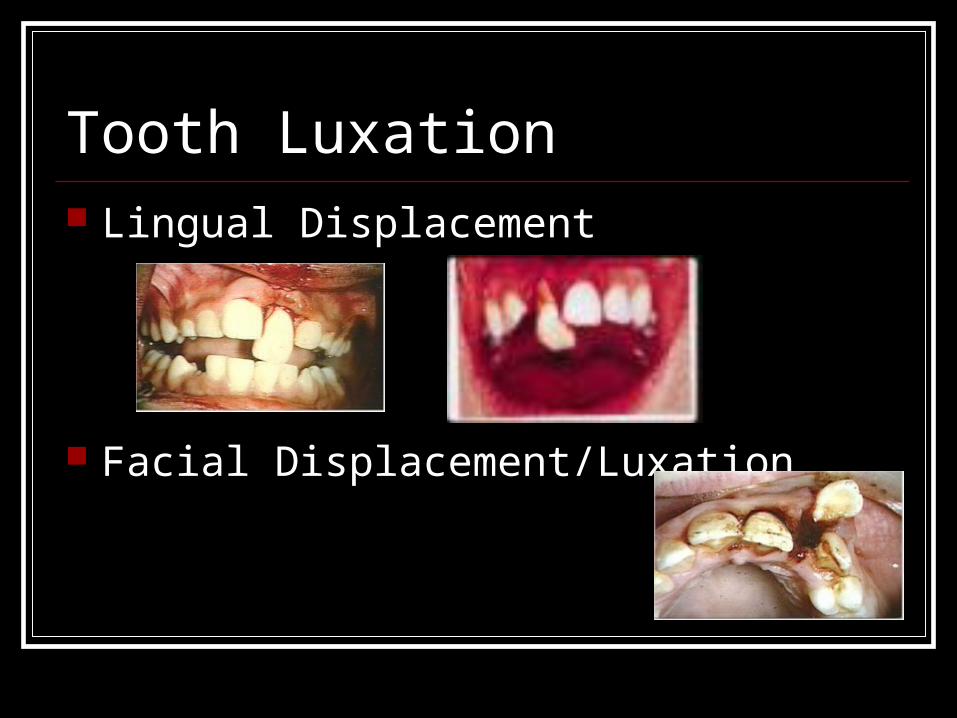
Tooth Luxation Lingual Displacement
Facial Displacement/Luxation
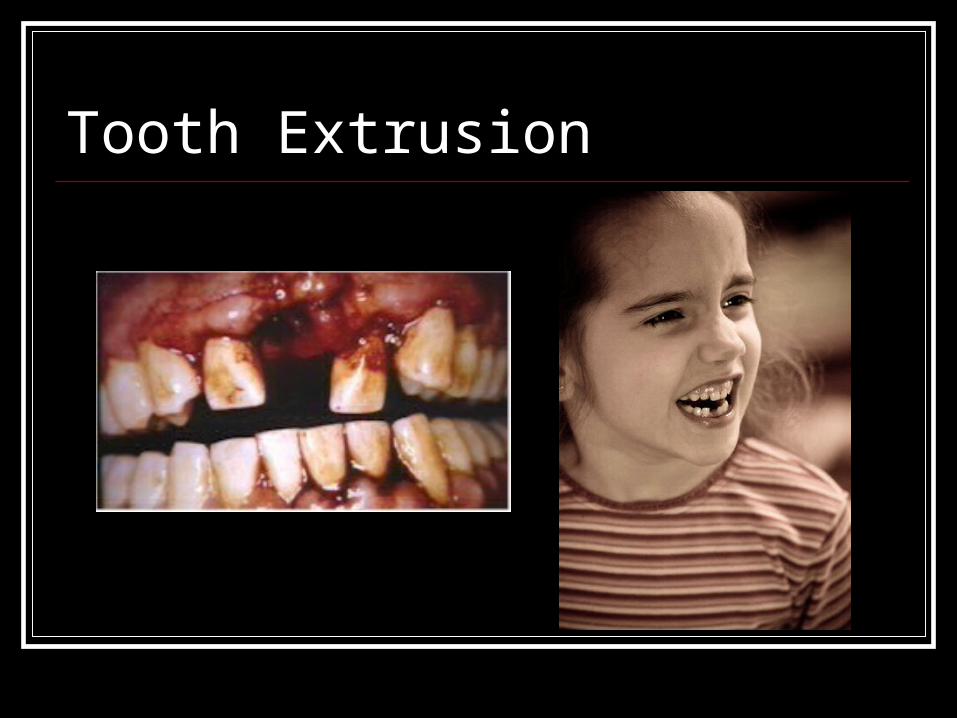
Tooth Extrusion

Facial Lacerations/Stitches
Tooth/Facial referral Suspected Fx Lacerations that need stitches Fx Tooth Avulsed tooth Malocclusion P c breathing TMJ dislocation When accompanied by closed head injury
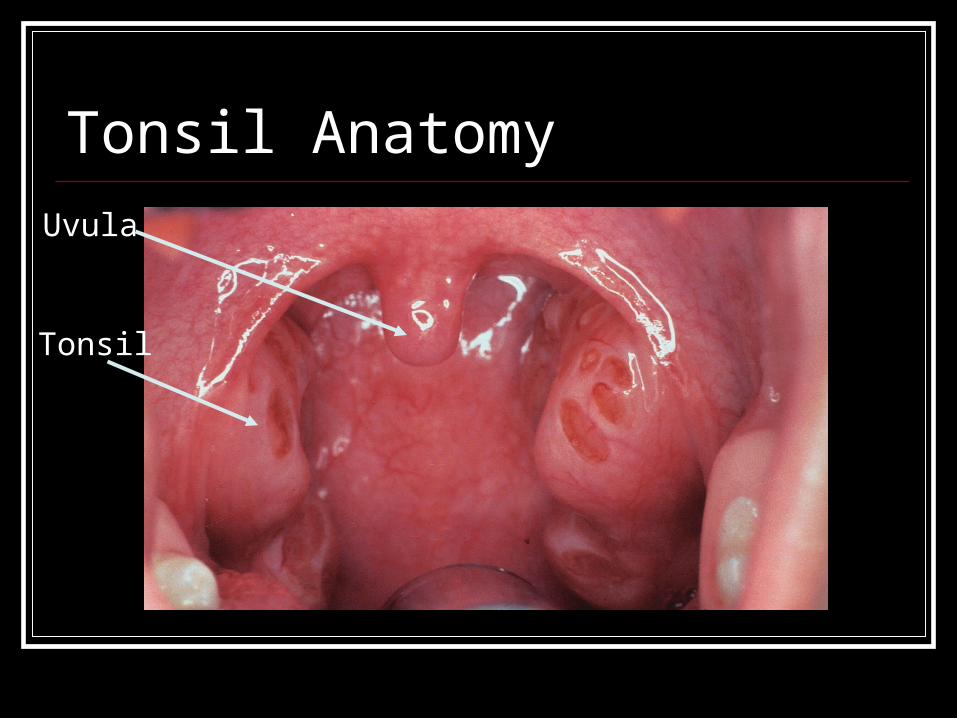
Tonsil Anatomy
Tonsil
Uvula
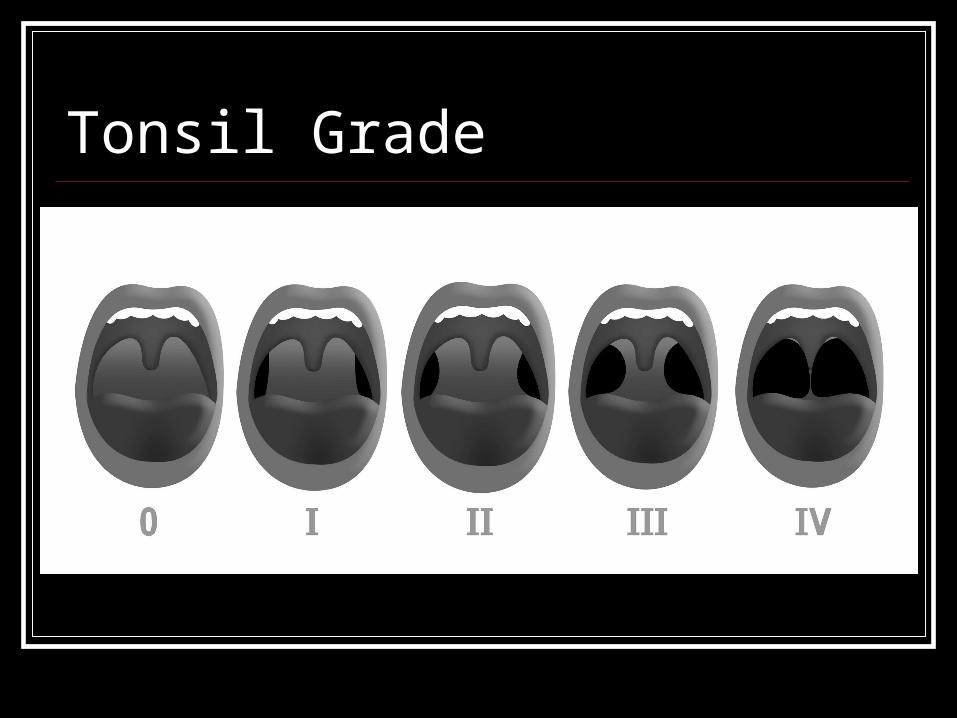
Tonsil Grade
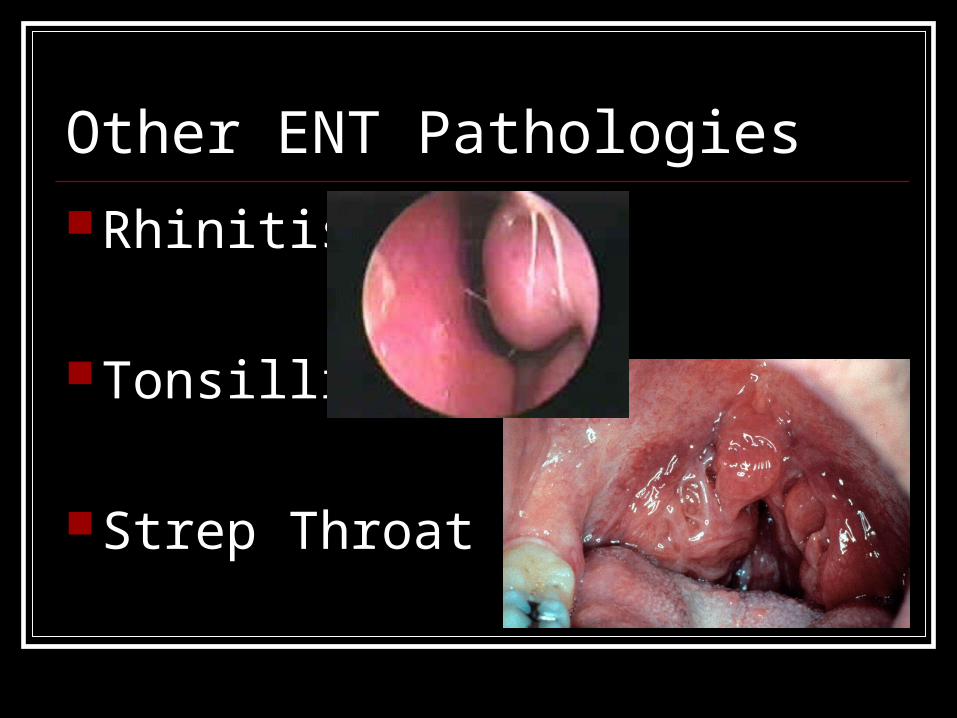
Other ENT Pathologies
Rhinitis
Tonsillitis
Strep Throat
Other ENT Pathologies Laryngitis
Pharyngitis
Sinusitis
Antibiotics and URIs Difficult to determine if Viral or Bacteria
cause Many physicians treat with antibiotics
regardless
Summary A directed history and thorough physical
exam are key.