







Languages
Pages
Legal


Special Commission of Inquiry into the Ruby Princess
EXHIBIT 33
Epidemiology Reports re COVID-19 of Communicable Diseases Intelligence, Department of Health - Numbers 1 to 9

Special Commission of Inquiry into the Ruby Princess
Index to bundle of documents relating to CDI epidemiology reports
(As at 10 June 2020)
Tab Description Date
1. 2019-nCoV acute respiratory disease, Australia: Epidemiology Report 1
Reporting week 26 January–1 February 2020
2. COVID-19, Australia: Epidemiology Report 2 Reporting week ending 19:00 AEDT 8 February 2020
3. COVID-19, Australia: Epidemiology Report 3 Reporting week ending 19:00 AEDT 15 February 2020
4. COVID-19, Australia: Epidemiology Report 4 Reporting week ending 19:00 AEDT 22 February 2020
5. COVID-19, Australia: Epidemiology Report 5 Reporting week ending 19:00 AEDT 29 February 2020
6. COVID-19, Australia: Epidemiology Report 6 Reporting week ending 1900 AEDT 7 March 2020
7. COVID-19, Australia: Epidemiology Report 7 Reporting week ending 19:00 AEDT 14 March 2020
8. COVID-19, Australia: Epidemiology Report 8 Reporting period from 19:00 AEDT 14 March to 23:59 AEDT 22 March 2020
9. COVID-19, Australia: Epidemiology Report 9 Reporting week ending 23:59 AEDT 29 March 2020

2 0 2 0 V o l u m e 4 4https://doi.org/10.33321/cdi.2020.44.13
2019-nCoV acute respiratory disease, Australia Epidemiology Report 1 Reporting week 26 January – 1 February 20202019-nCoV National Incident Room Surveillance Team

Communicable Diseases Intelligence ISSN: 2209-6051 Online
This journal is indexed by Index Medicus and Medline.
Creative Commons Licence - Attribution-NonCommercial-NoDerivatives CC BY-NC-ND
© 2020 Commonwealth of Australia as represented by the Department of Health
This publication is licensed under a Creative Commons Attribution- Non-Commercial NoDerivatives 4.0 International Licence from https://creativecommons.org/licenses/by-nc-nd/4.0/legalcode (Licence). You must read and understand the Licence before using any material from this publication.
Restrictions The Licence does not cover, and there is no permission given for, use of any of the following material found in this publication (if any):
• the Commonwealth Coat of Arms (by way of information, the terms under which the Coat of Arms may be used can be found at www.itsanhonour.gov.au);
• any logos (including the Department of Health’s logo) and trademarks;
• any photographs and images;
• any signatures; and
• any material belonging to third parties.
Disclaimer Opinions expressed in Communicable Diseases Intelligence are those of the authors and not necessarily those of the Australian Government Department of Health or the Communicable Diseases Network Australia. Data may be subject to revision.
Enquiries Enquiries regarding any other use of this publication should be addressed to the Communication Branch, Department of Health, GPO Box 9848, Canberra ACT 2601, or via e-mail to: [email protected]
Communicable Diseases Network Australia Communicable Diseases Intelligence contributes to the work of the Communicable Diseases Network Australia. http://www.health.gov.au/cdna
Communicable Diseases Intelligence (CDI) is a peer-reviewed scientific journal published by the Office of Health Protection, Department of Health. The journal aims to disseminate information on the epidemiology, surveillance, prevention and control of communicable diseases of relevance to Australia.
Editor Cindy Toms
Deputy Editor Simon Petrie
Design and Production Kasra Yousefi
Editorial Advisory Board David Durrheim, Mark Ferson, John Kaldor, Martyn Kirk and Linda Selvey
Website http://www.health.gov.au/cdi
Contacts Communicable Diseases Intelligence is produced by: Health Protection Policy Branch Office of Health Protection Australian Government Department of Health GPO Box 9848, (MDP 6) CANBERRA ACT 2601
Email: [email protected]
Submit an Article You are invited to submit your next communicable disease related article to the Communicable Diseases Intelligence (CDI) for consideration. More information regarding CDI can be found at: http://health.gov.au/cdi.
Further enquiries should be directed to: [email protected].

1 of 8 health.gov.au/cdi Commun Dis Intell (2018) 2020;44(https://doi.org/10.33321/cdi.2020.44.13) Epub 6/2/2020
Weekly epidemiological report
2019-nCoV acute respiratory disease, Australia Epidemiology Report 1
Reporting week 26 January – 1 February 2020
2019-nCoV National Incident Room Surveillance Team
Summary
This is the first epidemiological report of novel coronavirus (2019-nCoV) acute respiratory disease infections reported in Australia at 19:00 Australian Eastern Daylight Time [AEDT] 1 February 2020. It includes data on Australian cases notified during the week 26 January to 1 February 2020 and in the previous week (19 to 25 January 2020), the international situation and current information on the severity, transmission and spread of the 2019-nCoV infection.
Keywords: novel coronavirus (2019-nCoV); respiratory disease; case definition; epidemiology; Australia
The following epidemiological data are subject to change both domestically and internationally due to the rapidly evolving situation. Australian cases are still under active investigation. While every effort has been made to standardise the investigation of cases nationally, there may be some differences between jurisdictions.
In Australia:
• A total of twelve cases of 2019-nCoV infection were notified up until 1 Febru-ary 2020;
• All twelve cases reported a travel history to China, and 92% (11/12) had a travel history to Wuhan, Hubei Province, China;
• The majority of cases (92%, 11/12) developed mild to moderate symptoms, with one case (8%, 1/12) admitted to intensive care;
• Zero deaths were reported; and
• Two days elapsed since the onset of ill-ness in the latest confirmed case and the date of this report.
Internationally:
• Case numbers are increasing rapidly with 11,953 infections confirmed glob-ally; and
• The majority of confirmed infections (11,821) were reported in China, as well as 259 deaths.

2 of 8 health.gov.au/cdiCommun Dis Intell (2018) 2020;44(https://doi.org/10.33321/cdi.2020.44.13) Epub 6/2/2020
Domestic cases
There were twelve confirmed cases reported in Australia as at 19:00 AEDT 1 February 2020 (Table 1). Cases were reported in New South Wales (n = 4), Victoria (n = 4), Queensland (n = 2) and South Australia (n = 2). The first onset of signs and symptoms in a case occurred on 13 January 2020 (Figure 1). The majority of cases (92%, 11/12) had a travel history to Wuhan. The remaining case had direct contact with a confirmed case from Wuhan while travelling in China. All cases acquired their infection in China, which resulted in many close contacts requiring investigation. The median age of cases was 45 (range 21–66) years. The male-to-female ratio was 1.4:1. All cases (12/12) reported fever and/or chills and 83% (10/12) reported cough. Two cases were reported with pneumonia (Figure 2). Approximately 75% (9/12) of cases were hospitalised for clinical management and infection control, including one patient who was admitted to an Intensive Care Unit (ICU). The clinical course of infection was unavailable from these preliminary data. There were no deaths associated with the outbreak in Australia. The median time between onset of illness and col-lection of a specimen was 1 day (range 0–9 days).
International status report
As at 19:00 AEST 1 February 2020 the number of confirmed 2019-nCoV cases was 11,953 globally (Table 2). Mainland China reported the majority of cases (11,791) and all of the 259 deaths.1
Background
The World Health Organization (WHO) declared the outbreak of 2019-nCoV a Public Health Emergency of International Concern (PHEIC) on 30 January 2020.2 Cases were ini-tially associated with exposure to a wet market – located in Wuhan, Hubei Province, China – indicating a possible zoonotic source. Sustained human-to-human transmission is now likely to be occurring in the majority of provinces out-side of Hubei Province in China. Additionally, limited instances of human-to-human trans-mission were observed in a number of countries outside mainland China.3, 4
As of 1 February 2020, mainland China had reported 11,791 confirmed 2019-nCoV cases and 259 deaths.5
As of 1 February 2020, countries and Special Administrative Regions outside of mainland China reported 162 confirmed 2019-nCoV cases and zero deaths.
The current estimates on epidemiological param-eters including severity, transmissibility and incubation period are uncertain. Estimates are likely to change as more information becomes available.
Severity
Patients with 2019-nCoV infection present with a wide range of symptoms. Most seem to have
Table 1: Cumulative notified cases of confirmed 2019-nCoV by jurisdiction, Australia, 2020This week Last week Total cases
(26 Jan to 1 Feb) (19 to 25 Jan) (as of 1 Feb 2020)
Jurisdiction No. of cases No. of cases No. of cases
NSW 0 4 4
Vic 2 2 4
Qld 2 0 2
WA 0 0 0
SA 2 0 2
Tas 0 0 0
NT 0 0 0
ACT 0 0 0
Total cases 6 6 12

3 of 8 health.gov.au/cdi Commun Dis Intell (2018) 2020;44(https://doi.org/10.33321/cdi.2020.44.13) Epub 6/2/2020
Figure 1: Confirmed cases of 2019-nCoV infection by date of illness onset, Australia 2020
0
1
2
3
4
5
Num
ber o
f con
firm
ed 2
019-
nCoV
case
s
Date of illness onset
NSW VIC QLD SA
Figure 2: Signs and symptoms reported by 2019-nCoV cases in Australia, 2020 (n = 12)
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Fever/chills
Cough
Runny nose
Sore throat
Diarrhoea
Fatigue
Headache
Pneumonia
Nausea/vomiting
Shortness of breath
Irritability/confusion
Abdominal
Chest
Joint
Muscular
Pain
Percentage of 2019-nCoV cases with symptoms
Sym
ptom
s

4 of 8 health.gov.au/cdiCommun Dis Intell (2018) 2020;44(https://doi.org/10.33321/cdi.2020.44.13) Epub 6/2/2020
Table 2: Cumulative confirmed cases of 2019-nCoV globally, excluding Australia, 2019–2020
Country / SpecialAdministrative Region
This reporting week(26 Jan to 1 Feb 2020)
Total cases(from Dec 2019)1
Cambodia 1 1
Canada 4 4
mainland China 10,504 11,791
Finland 1 1
France 3 6
Germany 7 7
Hong Kong 8 13
India 1 1
Italy 2 2
Japan 14 17
Macau 5 7
Malaysia 8 8
Nepal 0 1
Philippines 1 1
Republic of South Korea 10 12
Russian Federation 2 2
Singapore 13 16
Spain 1 1
Sri Lanka 1 1
Sweden 1 1
Taiwan 7 10
Thailand 15 19
United Arab Emirates 4 4
United Kingdom 2 2
United States of America 5 7
Vietnam 4 6

5 of 8 health.gov.au/cdi Commun Dis Intell (2018) 2020;44(https://doi.org/10.33321/cdi.2020.44.13) Epub 6/2/2020
mild disease, and about 20% appear to progress to severe disease, including pneumonia, respira-tory failure and in some cases death.6
Transmission
The exact nature of transmission is poorly understood. WHO report ‘during previous outbreaks due to other coronavirus (Middle-East Respiratory Syndrome (MERS) and Severe Acute Respiratory Syndrome (SARS)), human-to-human transmission occurred through droplets, contact and fomites, suggesting that the trans-mission mode of the 2019-nCoV can be similar’.7 Sustained human-to-human transmission is likely to be now occurring in the majority of provinces in mainland China. The basic repro-ductive number, R0, indicates how contagious an infectious disease is and is defined as the average expected number of secondary cases produced by a single infection in a completely susceptible population. Chinese authorities reported a pre-liminary R0 of 1.4–2.5 on 23 January 2020 to the WHO International Health Regulations (2005) Emergency Committee.8 On 31 January 2020, Thailand reported its first instance of close com-munity human-to-human transmission (not within a household setting).9 Other instances were reported in Japan, Germany and Vietnam.4
Incubation period
Current estimates of the incubation period of 2019-nCoV from the WHO range from 2 to 10 days, with these estimates to be refined as more data become available.7 A recently-published article characterising the first 425 cases in Wuhan, Hubei Province China estimated the mean incubation period to be 5.2 days (95% confidence interval, 4.1–7.0).10
Recommendations for control
The WHO recommends the general public reduce their exposure and transmission to 2019-nCoV by:
• Frequently cleaning hands by using alcohol-based hand rub or soap and water;
• When coughing and sneezing cover mouth and nose with flexed elbow or tissue – throw tissue away immediately and wash hands;
• Avoid close contact with anyone who has fever and cough;
• If you have a fever, cough and difficulty breathing seek medical care early and share previous travel history with your health care provider.
Treatment
Currently there is no specific medication rec-ommended for 2019-nCoV. Antibiotics are not effective against viruses. Some antiviral medi-cations have shown promise in treating MERS and are now being tested for their effectiveness against 2019-nCoV.11 Experimental vaccines are also in development. Clinical care of suspected patients with 2019-nCoV should focus on early recognition, immediate isolation, implementa-tion of appropriate infection prevention and control measures and provision of optimised supportive care.6
Methods
Data for this report were current as at 19:00 hours AEDT, 1 February 2020.
This report outlines what is known epidemio-logically on 2019-nCoV in Australia and from publicly available data from WHO Situation Reports, other countries’ official updates and the scientific literature. Data on domestic cases in this report were collected from National Notifiable Diseases Surveillance System (NNDSS) and state and territory case investi-gation reports. The Communicable Diseases Network Australia (CDNA) developed the case definition for suspected and confirmed cases, which was modified at different time points in the epidemic (23 January and 27 January 2020) (Table 3). CDNA developed national guidance on investigating suspected and confirmed cases of 2019-nCoV. Based on this guidance, state and territory health department investigators con-

6 of 8 health.gov.au/cdiCommun Dis Intell (2018) 2020;44(https://doi.org/10.33321/cdi.2020.44.13) Epub 6/2/2020
ducted interviews of suspected cases to collect core and enhanced data for inclusion in NNDSS. Data were analysed using Stata to describe the epidemiology of infections in Australia and the progress of the epidemic.
Data for the international reports of 2019-nCoV case numbers by country were compiled from a range of sources. Case definitions for these case counts varied considerably making comparisons difficult. Rapid reviews of the current state of knowledge on 2019-nCoV were conducted from the literature using PubMed.
Acknowledgements
This report represents surveillance data reported through CDNA as part of the nationally coordi-nated response to 2019-nCoV. We thank public health staff from incident emergency operations centres in state & territory health departments,
and the Australian Government Department of Health; along with state and territory public health laboratories.
Author details
Corresponding author
Liz J Walker NIR Surveillance Team, Communicable Disease Epidemiology and Surveillance Section, Health Protection Policy Branch, Australian Government Department of Health, GPO Box 9484, MDP 14, Canberra, ACT 2601. Telephone: +61 2 6289 1512. Email: [email protected]
Table 3: Australian 2019-nCoV case definition as of 1 February 202012
Date of development Suspected Cases Confirmed Cases
27 January 2020 As the full clinical spectrum of illness is not known, clinical and public health judgement should also be used to determine the need for testing in patients who do not meet the clinical criteria below. If the patient satisfies epidemiological and clinical criteria, they are classified as a suspect case.
Epidemiological criteria• Travel to Hubei Province, China in the 14 days before the
onset of illness.a
OR• Travel to agreed areas of human-to-human transmission, or a
declared outbreak, within 14 days before onset of illness.OR• Close contact in 14 days before illness onset with a case of
2019-nCoV.
Clinical criteria• Fever or history of fever (≥38 °C) and acute respiratory
infection (sudden onset of respiratory infection with at least one of: shortness of breath, cough or sore throat).
OR• Severe acute respiratory infection requiring admission to
hospital with clinical or radiological evidence of pneumonia or acute respiratory distress syndrome (i.e. even if no evidence of fever).
A person who tests positive to a specific 2019-nCoV PCR test (when available) or has the virus identified by electron microscopy or viral culture, at a reference laboratory.
a The previous case definition developed on 23 January 2020 required that suspected cases had travelled to the city of Wuhan.

7 of 8 health.gov.au/cdi Commun Dis Intell (2018) 2020;44(https://doi.org/10.33321/cdi.2020.44.13) Epub 6/2/2020
References
1. World Health Organization (WHO). Novel coronavirus (2019-nCoV) situ-ational report-12: 1 February 2020. Ge-neva: WHO; 2020. [Accessed on 1 Febru-ary 2020.] Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200201-sitrep-12-ncov.pdf?sfvrsn=273c5d35_2.
2. WHO. Statement on the second meeting of the International Health Regulations (2005) Emergency Committee regarding the outbreak of novel coronavirus (2019-nCoV). [Internet.] Geneva: WHO; 2020. [Accessed on 31 January 2020.] Available from: https://www.who.int/news-room/detail/30-01-2020-statement-on-the-sec-ond-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavi-rus-(2019-ncov).
3. Rothe C, Schunk M, Sothmann P, Bretzel G, Froeschl G, Wallrauch C et al. Trans-mission of 2019-nCoV infection from an asymptomatic contact in Germany. N Engl J Med. 2020. https://doi.org/10.1056/NE-JMc2001468.
4. Phan LT, Nguyen TV, Luong QC, Nguyen TV, Nguyen HT, Le HQ et al. Importation and human-to-human transmission of a novel coronavirus in Vietnam. N Engl J Med. 2020. https://doi.org/10.1056/nejmc2001272.
5. National Health Commission, China. Update on pneumonia of new coronavirus infection as of 21:00 on January 31 2020. [Internet.] Beijing, China: National Health Commission; 2020. [Accessed on 1 February 2020.] Avail-able from: http://www.nhc.gov.cn/yjb/s7860/202002/84faf71e096446fdb1ae44939ba5c528.shtml.
6. WHO. Novel coronavirus (2019-nCoV) situational report-8: 28 January 2020. Ge-neva: WHO; 2020. [Accessed on 29 January
2020.] Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200128-sitrep-8-ncov-cleared.pdf?sfvrsn=8b671ce5_2.
7. WHO. Novel coronavirus (2019-nCoV) situational report-7: 27 January 2020. Ge-neva: WHO; 2020. [Accessed on 28 January 2020.] Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200127-sitrep-7-2019--ncov.pdf?sfvrsn=98ef79f5_2.
8. WHO. Statement on the meeting of the International Health Regulations (2005) Emergency Committee regarding the out-break of novel coronavirus (2019-nCoV). [Internet.] Geneva: WHO; 2020. [Ac-cessed on 24 January 2020.] Available from: https://www.who.int/news-room/detail/23-01-2020-statement-on-the-meet-ing-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavirus-(2019-ncov).
9. Department of Disease Control, Ministry of Public Health, Thailand. Ministry of Public Health reports that group of experts confirm five additional cases and invites people to carry surgical masks to protect themselves. [Internet.] Mueang Nonthaburi, Thailand: Department of Disease Control, Ministry of Public Health; 2020. [Accessed on 1 Febru-ary 2020.] Available from: https://ddc.moph.go.th/viralpneumonia/eng/file/news/news_no8_310163_1.pdf.
10. Li Q, Guan X, Wu P, Wang X, Zhou L, Tong Y et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N Engl J Med. 2020. https://doi.org/10.1056/NEJMoa2001316.
11. Paules CI, Marston HD, Fauci AS. Coronavi-rus infections—more than just the common cold. JAMA. 2020. https://doi.org/10.1001/jama.2020.0757.
12. Australian Government Department of

8 of 8 health.gov.au/cdiCommun Dis Intell (2018) 2020;44(https://doi.org/10.33321/cdi.2020.44.13) Epub 6/2/2020
Health. Novel coronavirus 2019 (2019-nCoV) - CDNA national guidelines for public health units 2020. [Internet.] Canber-ra: Australian Government Department of Health; 2020. [Accessed on 1 February 2020.] Available from: https://www1.health.gov.au/internet/main/publishing.nsf/Content/cdna-song-novel-coronavirus.htm.

2 0 2 0 V o l u m e 4 4https://doi.org/10.33321/cdi.2020.44.14
COVID-19, Australia: Epidemiology Report 2
COVID-19 National Incident Room Surveillance Team
Reporting week ending 19:00 AEDT 8 February 2020

Communicable Diseases Intelligence ISSN: 2209-6051 Online
This journal is indexed by Index Medicus and Medline.
Creative Commons Licence - Attribution-NonCommercial-NoDerivatives CC BY-NC-ND
© 2020 Commonwealth of Australia as represented by the Department of Health
This publication is licensed under a Creative Commons Attribution- Non-Commercial NoDerivatives 4.0 International Licence from https://creativecommons.org/licenses/by-nc-nd/4.0/legalcode (Licence). You must read and understand the Licence before using any material from this publication.
Restrictions The Licence does not cover, and there is no permission given for, use of any of the following material found in this publication (if any):
• the Commonwealth Coat of Arms (by way of information, the terms under which the Coat of Arms may be used can be found at www.itsanhonour.gov.au);
• any logos (including the Department of Health’s logo) and trademarks;
• any photographs and images;
• any signatures; and
• any material belonging to third parties.
Disclaimer Opinions expressed in Communicable Diseases Intelligence are those of the authors and not necessarily those of the Australian Government Department of Health or the Communicable Diseases Network Australia. Data may be subject to revision.
Enquiries Enquiries regarding any other use of this publication should be addressed to the Communication Branch, Department of Health, GPO Box 9848, Canberra ACT 2601, or via e-mail to: [email protected]
Communicable Diseases Network Australia Communicable Diseases Intelligence contributes to the work of the Communicable Diseases Network Australia. http://www.health.gov.au/cdna
Communicable Diseases Intelligence (CDI) is a peer-reviewed scientific journal published by the Office of Health Protection, Department of Health. The journal aims to disseminate information on the epidemiology, surveillance, prevention and control of communicable diseases of relevance to Australia.
Editor Cindy Toms
Deputy Editor Simon Petrie
Design and Production Kasra Yousefi
Editorial Advisory Board David Durrheim, Mark Ferson, John Kaldor, Martyn Kirk and Linda Selvey
Website http://www.health.gov.au/cdi
Contacts Communicable Diseases Intelligence is produced by: Health Protection Policy Branch Office of Health Protection Australian Government Department of Health GPO Box 9848, (MDP 6) CANBERRA ACT 2601
Email: [email protected]
Submit an Article You are invited to submit your next communicable disease related article to the Communicable Diseases Intelligence (CDI) for consideration. More information regarding CDI can be found at: http://health.gov.au/cdi.
Further enquiries should be directed to: [email protected].

1 of 12 health.gov.au/cdi Commun Dis Intell (2018) 2020;44(https://doi.org/10.33321/cdi.2020.44.14) Epub 12/2/2020
Weekly epidemiological report
COVID-19, Australia: Epidemiology Report 2Reporting week ending 19:00 AEDT 8 February 2020
COVID-19 National Incident Room Surveillance Team
Summary
This is the second epidemiological report for coronavirus disease 2019 (COVID-19), previously known as novel coronavirus (2019-nCoV), reported in Australia as at 19:00 Australian Eastern Daylight Time [AEDT] 8 February 2020. It includes data on Australian cases notified during the week ending 19:00 AEDT 8 February 2020, the international situation and current information on the severity, transmission and spread of the COVID-19 infection.
Keywords: novel coronavirus; 2019-nCoV; COVID-19; acute respiratory disease; case definition; epidemiology; Australia
The following epidemiological data are subject to change both domestically and internationally due to the rapidly evolving situation. Australian cases are still under active investigation. While every effort has been made to standardise the investigation of cases nationally, there may be some differences between jurisdictions.
In Australia:
• A total of fifteen cases of COVID-19 infec-tion were notified up until 19:00 AEDT 8 February 2020;
• All fifteen cases reported a travel history to China, and 80% (12/15) had a travel history to Wuhan, Hubei Province, China;
• All five Queensland cases were in a small tour group of nine people;
• The three Queensland cases reported this week are consistent with secondary trans-mission from the index Queensland case prior to isolation;
• Isolation and quarantine actions undertak-en for the Queensland cases appear to have successfully prevented further transmission
from the isolated tour group;
• Zero deaths were reported; and
• Three days elapsed since the onset of illness in the latest confirmed case at the date of this report.
Internationally:
• Case numbers are increasing rapidly with 34,886 infections confirmed globally;
• The majority of confirmed infections (34,546) were reported in mainland China, as well as 721 deaths; and
• Two deaths were reported outside mainland China, one each in Hong Kong and the Philippines.

2 of 12 health.gov.au/cdiCommun Dis Intell (2018) 2020;44(https://doi.org/10.33321/cdi.2020.44.14) Epub 12/2/2020
Domestic cases
There were fifteen confirmed cases reported in Australia at 19:00 AEDT 8 February 2020 (Table 1). Cases were reported in New South Wales (n = 4), Victoria (n = 4), Queensland (n = 5) and South Australia (n = 2). The first onset of signs and symptoms in a case occurred on 13 January 2020 (Figure 1). The median age of cases was 43 (range 8–66) years. The male-to-female ratio was 1.5:1. 93% of cases (14/15) reported fever and/or chills and 73% (11/15) reported cough. Two cases were reported with pneumo-nia (Figure 2). Approximately 73% (11/15) of cases were hospitalised for clinical management and infection control. The remaining cases, in accordance with infection control procedures, were assessed to be well enough to self-isolate at home. One case, previously reported as admit-ted to an Intensive Care Unit (ICU), was actu-ally admitted to a negative pressure isolation room in an ICU for infection control reasons.
The clinical course of infection was unavailable from these preliminary data. No deaths were reported.
A travel history to Wuhan, Hubei Province, China was reported in 80% of cases (12/15). The remaining three cases from mainland China were epidemiologically linked to labo-ratory-confirmed cases from Wuhan. The five laboratory-confirmed cases from Queensland were all part of a tour group of nine people from mainland China. The index case was isolated on presentation to hospital and all others within the tour group were quarantined. Four of those in quarantine were subsequently confirmed as cases, one of whom was a co-primary case, who like the index case had been in Wuhan, Hubei Province during the 14 days prior to illness onset. The other three cases were consistent with secondary transmission from the index case prior to isolation.
Table 1: Cumulative notified cases of confirmed COVID-19 by jurisdiction, Australia, 2020
JurisdictionThis week
(to 19:00 AEDT 8 Feb) No. of cases
Last week (to 19:00 AEDT 1 Feb)
No. of cases
Total cases (to 19:00 AEDT 8 Feb
2020) No. of cases
NSW 0 0 4
Vic 0 2 4
Qld 3 2 5
WA 0 0 0
SA 0 2 2
Tas 0 0 0
NT 0 0 0
ACT 0 0 0
Total cases 3 6 15

3 of 12 health.gov.au/cdi Commun Dis Intell (2018) 2020;44(https://doi.org/10.33321/cdi.2020.44.14) Epub 12/2/2020
Figure 1: Confirmed cases of COVID-19 infection by date of illness onset, Australia 2020 (n = 15)a
0
1
2
3
4
5
Num
ber o
f con
firm
ed C
OVI
D-19
case
s
Date of illness onset
NSW VIC QLD SA
a Date of illness onset for South Australian cases has been corrected since Epidemiology Report 1.1
Figure 2: Signs and symptoms reported by COVID-19 cases in Australia, 2020 (n = 15)
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Fever/chills
Cough
Sore throat
Diarrhoea
Runny nose
Fatigue
Headache
Pneumonia
Nausea/vomiting
Shortness of breath
Irritability/confusion
Abdominal
Chest
Joint
Muscular
Pain
Percentage of COVID-19 cases with symptoms
Sym
ptom
s

4 of 12 health.gov.au/cdiCommun Dis Intell (2018) 2020;44(https://doi.org/10.33321/cdi.2020.44.14) Epub 12/2/2020
The isolation and quarantine actions under-taken at identification of the index case appear to have successfully limited further transmis-sion to the isolated tour group. No further cases were identified amongst close contacts who had travelled on the same flight, all of whom have now completed a 14 day quarantine period.
International cases
As at 19:00 AEDT 8 February 2020, the num-ber of confirmed COVID-19 cases was 34,886 globally (Table 2).2 Mainland China reported 99% of cases (34,546) and 721 deaths. Twenty-seven countries and Special Administrative Regions outside of mainland China reported 276 confirmed COVID-19 cases. Two deaths were reported outside of mainland China, a 44-year-old male Wuhan resident in the Philippines and a 39-year-old male Hong Kong resident with recent travel to Wuhan. A cruise ship with approximately 3,700 passengers and crew quar-antined in Japanese territorial waters reported 64 confirmed COVID-19 cases.
Background
The World Health Organization (WHO) declared the outbreak of COVID-19 a Public Health Emergency of International Concern (PHEIC) on 30 January 2020.3
Cases were initially associated with exposure to a wet market – located in Wuhan, Hubei Province, China – indicating a possible zoonotic source. Sustained human-to-human transmis-sion is now likely to be occurring in the majority of provinces outside of Hubei Province in China. Eleven countries (France, Germany, Japan, Malaysia, Republic of Korea, Singapore, Spain, Thailand, the UK, USA and Vietnam) report possible or confirmed transmission in close contact settings outside of China.2,4 There is no evidence of widespread sustained community transmission in these countries.
In an effort to contain the spread of the virus, Chinese authorities imposed a lockdown on the city of Wuhan on 23 January 2020, suspending all
public transport including international flights.5 The measure was extended to neighbouring cities in Hubei Province over subsequent days, quarantining an estimated 50 million people.6
Following advice from the Australian Health Protection Principle Committee (AHPPC) to substantially reduce the volume of travellers coming from mainland China, additional border measures were implemented in Australia. From 1 February 2020, Australia has denied entry to anyone who had left or transited through main-land China, with the exception of Australian citizens, permanent residents and their imme-diate family and air crew who have been using appropriate personal protective equipment.7 Australia implemented these measures to slow the spread of COVID-19 into the country and to prepare healthcare services and laboratories for a targeted response.
The current estimates on epidemiological param-eters including severity, transmissibility and incubation period are uncertain. Estimates are likely to change as more information becomes available.
Severity
Patients with COVID-19 infection present with a wide range of symptoms. Most seem to have mild disease, and about 18% appear to progress to severe disease, including pneumonia, respira-tory failure and in some cases death.2,8 Fever, dry non-productive cough and fatigue are common symptoms.
Reports from China on the clinical presentation are limited to novel coronavirus-infected pneu-monia (NCIP) patients. Of patients with NCIP, 30% develop difficulty breathing five days after onset of illness (range 1–10 days).9, 10 The median time from onset of illness to hospitalisation for NCIP patients was seven days (range 4–8 days), with acute respiratory distress syndrome (ARDS) experienced on day eight (range 6–12 days).10 Of 138 NCIP patients, approximately a quarter required ICU admission (2% receiving high-flow oxygen, 11% non-invasive ventilation,

5 of 12 health.gov.au/cdi Commun Dis Intell (2018) 2020;44(https://doi.org/10.33321/cdi.2020.44.14) Epub 12/2/2020
Table 2: Cumulative confirmed cases of COVID-19 globally, 2019–2020
Country / Special Administrative Region This reporting week (to 19:00 AEDT 8 Feb 2020) Total cases (from Dec 2019)a
Mainland China 22,755 34,546
Cruise ship 64 64
Singapore 17 33
Thailand 13 32
Hong Kong 13 26
Japan 8 25
Republic of South Korea 12 24
Taiwan 6 16
Australia 3 15
Malaysia 7 15
Germany 7 14
Vietnam 7 13
United States of America 5 12
Macau 3 10
Canada 3 7
United Arab Emirates 3 7
France 0 6
India 2 3
Italy 1 3
Philippines 2 3
United Kingdom 1 3
Russian Federation 0 2
Belgium 1 1
Cambodia 0 1
Finland 0 1
Nepal 0 1
Spain 0 1
Sri Lanka 0 1
Sweden 0 1
Total 22,933 34,886
a Data taken from WHO Situation Reports.

6 of 12 health.gov.au/cdiCommun Dis Intell (2018) 2020;44(https://doi.org/10.33321/cdi.2020.44.14) Epub 12/2/2020
9% invasive ventilation and 3% extracorpor-eal membrane oxygenation (ECMO)).10 ICU patients were typically older than 65 years and had a greater number of comorbidities.
The true fatality rate for COVID-19 cannot be presently calculated. Diagnosis of COVID-19 will precede death or recovery by days to weeks. The number of deaths should be compared to past confirmed cases, taking into account this lag period and estimating the fraction of mild under-reported disease.11 Spatio-temporal variations of the crude fatality rate (deaths/confirmed cases) are seen in Hubei Province, 2.8% (699/24,953) compared to other provinces in China, 0.2% (23/9593) and may reflect a focus in Hubei Province on diagnosing and treating severe disease and/or a health system struggling to provide supportive care to a large volume of patients during the epidemic.
Transmission
The exact nature of transmission is poorly under-stood. The WHO has reported ‘during previous outbreaks due to other coronavirus (Middle-East Respiratory Syndrome (MERS) and Severe Acute Respiratory Syndrome (SARS)), human-to-human transmission occurred through droplets, contact and fomites, suggesting that the transmission mode of the 2019-nCoV can be similar’.12 The basic reproductive number, R0, indicates the contagiousness of an infec-tious disease and is defined as the average expected number of secondary cases produced by a single infection in a completely susceptible population. Chinese authorities reported a pre-liminary R0 of 1.4–2.5 on 23 January 2020 to the WHO International Health Regulations (2005) Emergency Committee.13 On 31 January 2020, Thailand reported its first instance of close com-munity human-to-human transmission (not within a household setting).14
China and France have reported hospital-related transmission.10,15 In one study from Wuhan, of 138 NCIP patients 41% were presumed infected in the hospital, including 40 healthcare work-ers.10 Media have reported shortages of masks
and personal protective equipment in Hubei Province due to the quarantine measures which may have exacerbated the high proportion of hospital-related infections in this study.16 A reverse transcription polymerase chain reaction (RT-PCR)-confirmed asymptomatic child was described with radiological signs of pneumonia reported from a family cluster in Shenzhen, although onward transmission from this case was not documented.17 A report describing a suspected asymptomatic transmission in Germany was proven inaccurate once health officials interviewed the patient directly.
Incubation period
Current estimates of the incubation period of COVID-19 from the WHO range from 2 to 10 days, with these estimates to be refined as more data become available.12 A recently-published article characterising the first 425 cases in Wuhan, Hubei Province China estimated the mean incubation period to be 5.2 days (95% confidence interval, 4.1–7.0 days) with the 95th percentile of the distribution at 12.5 days.18 A modelling paper using known travel history to and from Wuhan and symptom onset date in 88 exported cases calculated the mean incubation period to be 6.4 days (95% confidence interval, 5.6–7.7 days) ranging from 2.1 to 11.1 days (2.5th and 97.5th percentile).19 Both reports support the use of 14 days as the upper limit of the incubation period used in the Australian interim advice.20
Recommendations for control
The WHO recommends the general public reduce their exposure and transmission to COVID-19 by:
• Frequently cleaning hands by using alco-hol-based hand rub or soap and water;
• When coughing and sneezing cover mouth and nose with flexed elbow or tissue – throw tissue away immediately and wash hands;
• Avoid close contact with anyone who has

7 of 12 health.gov.au/cdi Commun Dis Intell (2018) 2020;44(https://doi.org/10.33321/cdi.2020.44.14) Epub 12/2/2020
fever and cough; and
• If you have a fever, cough and difficulty breathing seek medical care early and share previous travel history with your health care provider.
Treatment
Currently there is no specific medication recommended for COVID-19. Antibiotics are not effective against viruses. A number of antiviral medications will be trialled to assess whether they can be used to treat COVID-19. Experimental vaccines are also in development.
Clinical care of suspected patients with COVID-19 should focus on early recognition, immediate isolation, implementation of appropriate infec-tion prevention and control measures and provi-sion of optimised supportive care.8
Methods
Data for this report were current as at 19:00 hours AEDT, 8 February 2020.
This report outlines what is known epidemio-logically on COVID-19 in Australia and from publicly available data from WHO Situation Reports, other countries’ official updates and the scientific literature. Data on domestic cases in this report were collected from National Notifiable Diseases Surveillance System (NNDSS) and state and territory case investigation reports. The Communicable Diseases Network Australia (CDNA) developed the case definition for sus-pected and confirmed cases, which was modi-fied at different time points in the epidemic (23 and 27 January and 2, 4, 6 and 7 February 2020) (Table 3). CDNA developed national guidance on investigating suspected and confirmed cases of COVID-19. Based on this guidance, state and territory health department investigators con-ducted interviews of suspected cases to collect core and enhanced data for inclusion in NNDSS. Data were analysed using Stata to describe the epidemiology of infections in Australia and the progress of the epidemic.
Previous case definitions are provided in Appendix A.
Data for the international cases of COVID-19 by country were compiled from the latest WHO Situational Report. Case definitions may vary by country making comparisons difficult. Rapid reviews of the current state of knowledge on COVID-19 were conducted from the literature using PubMed.
Acknowledgements
This report represents surveillance data reported through CDNA as part of the nationally coordi-nated response to COVID-19. We thank public health staff from incident emergency operations centres in state & territory health departments, and the Australian Government Department of Health; along with state and territory public health laboratories.
Author details
Corresponding author
Liz J Walker
NIR Surveillance Team, Communicable Disease Epidemiology and Surveillance Section, Health Protection Policy Branch, Australian Government Department of Health, GPO Box 9484, MDP 14, Canberra, ACT 2601. Telephone: +61 2 6289 1512. Email: [email protected]

8 of 12 health.gov.au/cdiCommun Dis Intell (2018) 2020;44(https://doi.org/10.33321/cdi.2020.44.14) Epub 12/2/2020
Table 3: Australian COVID-19 case definition as of 8 February 202020
Version Date of development Suspected Cases Confirmed Cases
1.5 7 February 2020 As the full clinical spectrum of illness is not known, clinical and public health judgement should also be used to determine the need for testing in patients who do not meet the clinical criteria below. If the patient satisfies epidemiological and clinical criteria, they are classified as a suspect case.
Epidemiological criteria• Travel to (including transit through)
mainland China in the 14 days before the onset of illness.
OR• Close or casual contact in 14 days before
illness onset with a confirmed case of COVID-19.
Clinical criteria• FeverOR• Acute respiratory infection (e.g. shortness
of breath or cough) with or without fever
A person who tests positive to a specific COVID-19 PCR test (when available) or has the virus identified by electron microscopy or viral culture, at a reference laboratory.

9 of 12 health.gov.au/cdi Commun Dis Intell (2018) 2020;44(https://doi.org/10.33321/cdi.2020.44.14) Epub 12/2/2020
References
1. 2019-nCoV National Incident Room Surveil-lance Team. 2019-nCoV acute respiratory disease, Australia: Epidemiology Report 1. Reporting week 26 January – 1 February 2020. Commun Dis Intell (2018). 2020;44. doi: https://doi.org/10.33321/cdi.2020.44.13.
2. World Health Organization (WHO). Novel coronavirus (2019-nCoV) situa-tion report-19: 8 February 2020. Geneva: WHO; 2020. [Accessed on 9 February 2020.] Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200208-sitrep-19-ncov.pdf?sfvrsn=6e091ce6_2.
3. WHO. Statement on the second meeting of the International Health Regulations (2005) Emergency Committee regarding the outbreak of novel coronavirus (2019-nCoV). [Internet.] Geneva: WHO; 2020. [Accessed on 31 January 2020.] Available from: https://www.who.int/news-room/detail/30-01-2020-statement-on-the-sec-ond-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavi-rus-(2019-ncov).
4. Patel A, Jernigan D, 2019-nCoV CDC Response Team. Initial public health re-sponse and interim clinical guidance for the 2019 novel coronavirus outbreak—United States, December 31, 2019–February 4, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(5):140–6.
5. Reuters. Wuhan lockdown ‘unprededented’, shows commitment to contain virus: WHO representative in China 2020. [Internet.] London: Reuters; 23 January 2020. [Accessed on 7 February 2020.] Available from: https://www.reuters.com/article/us-china-health-who-idUSKBN1ZM1G9.
6. The New York Times. China tightens Wuhan lockdown in ‘wartime’ battle with coronavi-
rus. [Internet.] New York: New York Times; 6 February 2020. [Accessed on 7 February 2020.] Available from: https://www.nytimes.com/2020/02/06/world/asia/coronavirus-china-wuhan-quarantine.html.
7. Australian Government Department of Health. Australian Health Protection Princi-pal Committee (AHPPC) novel coronavirus statement on 1 February 2020. [Internet.] Canberra: Australian Government Depart-ment of Health; 2020 [Accessed on 7 Feb-ruary 2020.] Available from: https://www.health.gov.au/news/australian-health-protec-tion-principal-committee-ahppc-novel-coro-navirus-statement-on-1-february-2020.
8. WHO. Novel coronavirus (2019-nCoV) situation report-8: 28 January 2020. Ge-neva: WHO; 2020. [Accessed on 29 January 2020.] Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200128-sitrep-8-ncov-cleared.pdf?sfvrsn=8b671ce5_2.
9. Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y et al. Epidemiological and clinical charac-teristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descrip-tive study. Lancet. 2020. doi: https://doi.org/10.1016/S0140-6736(20)30211-7.
10. Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J et al. Clinical characteristics of 138 hospi-talized patients with 2019 novel coronavi-rus–infected pneumonia in Wuhan, China. JAMA. 2020. doi: https://doi.org/10.1001/jama.2020.1585.
11. Battegay M, Kuehl R, Tschudin-Sutter S, Hirsch HH, Widmer AF, Neher RA. 2019-novel coronavirus (2019-nCoV): esti-mating the case fatality rate - a word of cau-tion. Swiss Med Wkly. 2020;150:w20203.
12. WHO. Novel coronavirus (2019-nCoV) situation report-7: 27 January 2020. Ge-neva: WHO; 2020 [Accessed on 28 January

10 of 12 health.gov.au/cdiCommun Dis Intell (2018) 2020;44(https://doi.org/10.33321/cdi.2020.44.14) Epub 12/2/2020
2020.] Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200127-sitrep-7-2019--ncov.pdf?sfvrsn=98ef79f5_2.
13. WHO. Statement on the meeting of the International Health Regulations (2005) Emergency Committee regarding the out-break of novel coronavirus (2019-nCoV). [Internet.] Geneva: WHO; 2020. [Ac-cessed on 24 January 2020.] Available from: https://www.who.int/news-room/detail/23-01-2020-statement-on-the-meet-ing-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavirus-(2019-ncov).
14. Department of Disease Control, Ministry of Public Health, Thailand. Ministry of Public Health reports that group of experts confirm five additional cases and invites people to carry surgical masks to protect themselves. [Internet.] Mueang Nonthaburi, Thailand: Department of Disease Control, Ministry of Public Health; 2020. [Accessed on 1 Febru-ary 2020.] Available from: https://ddc.moph.go.th/viralpneumonia/eng/file/news/news_no8_310163_1.pdf.
15. WHO. Novel coronavirus (2019-nCoV) situation report-12: 1 February 2020. Ge-neva: WHO; 2020. [Accessed on 1 Febru-ary 2020.] Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200201-sitrep-12-ncov.pdf?sfvrsn=273c5d35_2.
16. Reuters. China’s coronavirus-hit Hubei says medical supply tightness easing, shortages persist. [Internet.] London: Reuters; 9 Feb-ruary 2020. [Accessed on 9 February 2020.] Available from: https://www.reuters.com/ar-ticle/us-china-health-hubei/chinas-coronavi-rus-hit-hubei-says-medical-supply-tightness-easing-shortages-persist-idUSKBN2020MF.
17. Chan JF, Yuan S, Kok KH, To KK, Chu H, Yang J et al. A familial cluster of pneumonia associated with the 2019 novel coronavi-
rus indicating person-to-person transmis-sion: a study of a family cluster. Lancet. 2020. doi: https://doi.org/10.1016/S0140-6736(20)30154-9.
18. Li Q, Guan X, Wu P, Wang X, Zhou L, Tong Y et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N Engl J Med. 2020. doi: https://doi.org/10.1056/NEJMoa2001316.
19. Backer JA, Klinkenberg D, Wallinga J. In-cubation period of 2019 novel coronavirus (2019-nCoV) infections among travellers from Wuhan, China, 20–28 January 2020. Eurosurveillance. 2020;25(5):2000062.
20. Australian Government Department of Health. Novel coronavirus 2019 (2019-nCoV) – CDNA national guidelines for public health units. [Internet.] Canberra: Australian Government Department of Health; 2020. [Accessed on 1 February 2020.] Available from: https://www1.health.gov.au/internet/main/publishing.nsf/Content/cdna-song-novel-coronavirus.htm.

11 of 12 health.gov.au/cdi Commun Dis Intell (2018) 2020;44(https://doi.org/10.33321/cdi.2020.44.14) Epub 12/2/2020
Appendix A – Previous case definitions and contact definitions
Version Date of development
Suspected Cases Confirmed Cases
As the full clinical spectrum of illness is not known, clinical and public health judgement should also be used to determine the need for testing in patients who do not meet the clinical criteria below. If the patient satisfies epidemiological and clinical criteria, they are classified as a suspect case.
A person who tests positive to a specific COVID-19 PCR test (when available) or has the virus identified by electron microscopy or viral culture, at a reference laboratory.
1.4 6 February 2020 Epidemiological criteria
• Travel to (including transit through) mainland China in the 14 days before the onset of illness.
OR• Close or casual contacta in 14 days
before illness onset with a confirmed or suspected case of COVID-19.
Clinical criteria• Fever.OR• Acute respiratory infection (e.g.
shortness of breath or cough) with or without fever.
1.3 4 February 2020 Epidemiological criteria
• Travel to (including transit through) mainland China in the 14 days before the onset of illness.
OR• Close contacta in 14 days before
illness onset with a confirmed or suspected case of COVID-19.
Clinical criteria• Fever.OR• Acute respiratory infection (e.g.
shortness of breath or cough) with or without fever.
1.2 2 February 2020 Epidemiological criteria
• Travel to (including transit through) mainland China in the 14 days before the onset of illness.
OR• Close contacta in the 14 days before
illness onset with a confirmed or suspected case of COVID-19.
Clinical criteria• Acute respiratory infection (sudden
onset of respiratory infection with at least one of: shortness of breath, cough or sore throat) with or without fever or history of fever.

12 of 12 health.gov.au/cdiCommun Dis Intell (2018) 2020;44(https://doi.org/10.33321/cdi.2020.44.14) Epub 12/2/2020
Version Date of development
Suspected Cases Confirmed Cases
1.1 27 January 2020 Epidemiological criteria
• Travel to Hubei Province, China in the 14 days before the onset of illness.
OR• Travel to agreed areas of human-to-
human transmission, or a declared outbreak, within 14 days before onset of illness
OR• Close contacta in 14 days before
illness onset with a case of COVID-19.Clinical criteria• Fever or history of fever (≥38 °C) and
acute respiratory infection (sudden onset of respiratory infection with at least one of: shortness of breath, cough or sore throat)
OR• Severe acute respiratory infection
requiring admission to hospital with clinical or radiological evidence of pneumonia or acute respiratory distress syndrome (i.e. even if no evidence of fever)
1.0 23 January 2020 Epidemiological criteria
• Travel to Wuhan City (Hubei Province, China) in the 14 days before the onset of illness.
OR• Travel to an area with evidence
of sustained human-to-human transmission, or a declared outbreak, within 14 days before onset of illness.
OR• Close contacta in 14 days before
illness onset with a case of COVID-19.
Clinical criteria
• Fever or history of fever (≥38 °C) and acute respiratory infection (sudden onset of respiratory infection with at least one of: shortness of breath, cough or sore throat).
OR• Severe acute respiratory infection
requiring admission to hospital with clinical or radiological evidence of pneumonia or acute respiratory distress syndrome (i.e. even if no evidence of fever).
a Full details on the definition of a close contact are available on the Australian Government Department of Health CDNA National
Guidelines for Public Health Units 2019-nCoV.20

2 0 2 0 V o l u m e 4 4https://doi.org/10.33321/cdi.2020.44.15
COVID-19, Australia: Epidemiology Report 3:Reporting week ending 19:00 AEDT 15 February 2020
COVID-19 National Incident Room Surveillance Team

Communicable Diseases Intelligence ISSN: 2209-6051 Online
This journal is indexed by Index Medicus and Medline.
Creative Commons Licence - Attribution-NonCommercial-NoDerivatives CC BY-NC-ND
© 2020 Commonwealth of Australia as represented by the Department of Health
This publication is licensed under a Creative Commons Attribution- Non-Commercial NoDerivatives 4.0 International Licence from https://creativecommons.org/licenses/by-nc-nd/4.0/legalcode (Licence). You must read and understand the Licence before using any material from this publication.
Restrictions The Licence does not cover, and there is no permission given for, use of any of the following material found in this publication (if any):
• the Commonwealth Coat of Arms (by way of information, the terms under which the Coat of Arms may be used can be found at www.itsanhonour.gov.au);
• any logos (including the Department of Health’s logo) and trademarks;
• any photographs and images;
• any signatures; and
• any material belonging to third parties.
Disclaimer Opinions expressed in Communicable Diseases Intelligence are those of the authors and not necessarily those of the Australian Government Department of Health or the Communicable Diseases Network Australia. Data may be subject to revision.
Enquiries Enquiries regarding any other use of this publication should be addressed to the Communication Branch, Department of Health, GPO Box 9848, Canberra ACT 2601, or via e-mail to: [email protected]
Communicable Diseases Network Australia Communicable Diseases Intelligence contributes to the work of the Communicable Diseases Network Australia. http://www.health.gov.au/cdna
Communicable Diseases Intelligence (CDI) is a peer-reviewed scientific journal published by the Office of Health Protection, Department of Health. The journal aims to disseminate information on the epidemiology, surveillance, prevention and control of communicable diseases of relevance to Australia.
Editor Cindy Toms
Deputy Editor Simon Petrie
Design and Production Kasra Yousefi
Editorial Advisory Board David Durrheim, Mark Ferson, John Kaldor, Martyn Kirk and Linda Selvey
Website http://www.health.gov.au/cdi
Contacts Communicable Diseases Intelligence is produced by: Health Protection Policy Branch Office of Health Protection Australian Government Department of Health GPO Box 9848, (MDP 6) CANBERRA ACT 2601
Email: [email protected]
Submit an Article You are invited to submit your next communicable disease related article to the Communicable Diseases Intelligence (CDI) for consideration. More information regarding CDI can be found at: http://health.gov.au/cdi.
Further enquiries should be directed to: [email protected].

1 of 14 health.gov.au/cdi Commun Dis Intell (2018) 2020;44(https://doi.org/10.33321/cdi.2020.44.15) Epub 20/2/2020
Weekly epidemiological report
COVID-19, Australia: Epidemiology Report 3:Reporting week ending 19:00 AEDT 15 February 2020
COVID-19 National Incident Room Surveillance Team
Summary
This is the third epidemiological report for coronavirus disease 2019 (COVID-19), previously known as novel coronavirus (2019-nCoV), from the virus now known as SARS-CoV-2, reported in Australia as at 19:00 Australian Eastern Daylight Time [AEDT] 15 February 2020. It includes data on the COVID-19 Australian cases, the international situation and current information on the severity, transmission and spread.
Keywords: SARS-CoV-2; novel coronavirus; 2019-nCoV; coronavirus disease 2019; COVID-19; acute respiratory disease; case definition; epidemiology; Australia
The following epidemiological data are subject to change both domestically and internationally due to the rapidly evolving situation. Australian cases are still under active investigation. While every effort has been made to standardise the investigation of cases nationally, there may be some differences between jurisdictions.
In Australia:
• A total of fifteen COVID-19 cases werenotified up until 19:00 AEDT 15 Febru-ary 2020;
• All fifteen cases reported a travel historyto China;
• Zero deaths were reported;
• At the conclusion of this report’s cover-age, eleven days have elapsed since theonset of illness in the latest confirmedcase; and
• On 13 February 2020, the AustralianHealth Protection Principal Committee(AHPPC) issued a statement on resolu-tion on travel restrictions and COVID-9recommending that the current travelrestrictions remain in place.
Internationally:
• Case numbers are increasing rapidlywith 67,102 infections confirmed glob-ally;
• The majority of confirmed infections(66,492) were reported in mainlandChina, as well as 1,523 deaths;
• On 12 February 2020 the case diagnosisclassification in Hubei Province waschanged to include clinically diagnosedcases in addition to laboratory-con-firmed cases.
• As of 15 February 2020, Hubei Provincereported 54,406 cases, of which 30%(16,522) were clinically diagnosed; and
• Three deaths were reported outsidemainland China, one each in HongKong, Japan and the Philippines.

2 of 14 health.gov.au/cdiCommun Dis Intell (2018) 2020;44(https://doi.org/10.33321/cdi.2020.44.15) Epub 20/2/2020
Domestic cases
There were fifteen confirmed cases reported in Australia at 19:00 AEDT 15 February 2020 (Table 1). Cases were reported in New South Wales (n = 4), Victoria (n = 4), Queensland (n = 5) and South Australia (n = 2). The first onset of signs and symptoms in a case occurred on 13 January 2020 (Figure 1). The median age of cases was 43 (range 8–66) years. The male-to-female ratio was 1.5:1. Fourteen of the 15 cases (93%) reported fever and/or chills and 73% (11/15) reported cough. Two cases reported with pneu-monia. Approximately 73% (11/15) of cases were hospitalised for clinical management and infec-tion control. The remaining cases, in accordance with infection control procedures, were assessed to be well enough to self-isolate at home. The clinical course of infection was unavailable from these preliminary data. No deaths were reported.
The five laboratory-confirmed cases from Queensland were all part of a tour group of nine people from mainland China. The index case was isolated on presentation to hospital and all others within the tour group were quarantined. Four of those in quarantine were subsequently confirmed as cases, one of whom was a co-primary case, who like the index case had been in Wuhan, Hubei Province during the 14 days prior to illness onset. The other three cases were consistent with secondary transmission from the index case prior to isolation.
International cases
On 12 February 2020 the General Office of the National Health Commission of the People’s Republic of China and the Office of the State Administration of Traditional Chinese Medicine added clinical diagnosis to the case diagnosis classification in Hubei Province. This change was issued through the ‘Diagnosis and Treatment Plan for Pneumonia of New Coronavirus (Version)’ to ensure that patients can receive standardised treatment according to confirmed cases as early as possible to further improve the success rate of treatment.2 This is
the first time China has reported clinically diag-nosed cases in addition to laboratory-confirmed cases.3 The number of clinically-diagnosed cases in Hubei Province will be included in the num-ber of confirmed cases for publication from 12 February 2020 onwards.2
As at 19:00 AEDT 15 February 2020, the num-ber of confirmed COVID-19 cases was 67,102 globally, including 16,522 clinically-diagnosed cases from Hubei Province, China (Table 2).4 Mainland China reported 99% of cases (66,492) and 1,523 deaths. Twenty-eight countries and Special Administrative Regions outside of mainland China reported 392 confirmed COVID-19 cases. Three deaths were reported outside of mainland China, a 44-year-old male Wuhan resident in the Philippines, a 39-year-old male Hong Kong resident with recent travel to Wuhan and a female in her 80s from Kanagawa Prefecture near Tokyo, Japan who had no recent travel history to China. A cruise ship with approximately 3,700 passengers and crew quar-antined in Japanese territorial waters reported 218 confirmed COVID-19 cases.
Background
The World Health Organization (WHO) declared the outbreak of COVID-19 a Public Health Emergency of International Concern (PHEIC) on 30 January 2020.5
Cases were initially associated with exposure to a wet market – located in Wuhan, Hubei Province, China – indicating a possible zoonotic source. Sustained human-to-human transmission is now occurring in the majority of provinces outside of Hubei Province in China. Fourteen countries (Australia, Egypt, France, Germany, Japan, Malaysia, Republic of Korea, Singapore, Spain, Thailand, UAE, UK, USA and Vietnam) report possible or confirmed transmission in close contact settings outside of China.4,6,7 There is no evidence of widespread sustained commu-nity transmission in these countries.

3 of 14 health.gov.au/cdi Commun Dis Intell (2018) 2020;44(https://doi.org/10.33321/cdi.2020.44.15) Epub 20/2/2020
Table 1: Cumulative notified cases of confirmed COVID-19 by jurisdiction, Australia, 2020
JurisdictionThis week
(to 19:00 AEDT 15 Feb) No. of cases
Last week (to 19:00 AEDT 8 Feb)
No. of cases
Total cases (to 19:00 AEDT 15 Feb 2020)
No. of cases
NSW 0 0 4
Vic 0 0 4
Qld 0 3 5
WA 0 0 0
SA 0 0 2
Tas 0 0 0
NT 0 0 0
ACT 0 0 0
Total cases 0 3 15
In an effort to contain the spread of the virus, Chinese authorities imposed a lockdown on the city of Wuhan on 23 January 2020, suspending all public transport including international flights.8 The measure was extended to neighbouring cities in Hubei Province over subsequent days, quarantining an estimated 50 million people.9
Following advice from the Australian Health Protection Principle Committee (AHPPC) to substantially reduce the volume of travellers coming from mainland China, additional border measures were implemented in Australia. From 1 February 2020, Australia has denied entry to anyone who had left or transited through main-land China, with the exception of Australian citizens, permanent residents and their imme-diate family and air crew who have been using appropriate personal protective equipment.10 Australia implemented these measures to slow the spread of COVID-19 into the country and to prepare healthcare services and laboratories for a targeted response.
On 13 February 2020, AHPPC released a state-ment on the resolution on travel restrictions and coronavirus (COVID-19) recommending current travel restrictions remain in place.11
AHPPC noted approximately 70% reduction in entry to Australia of people who have been in mainland China, contributing to a much more
manageable program of self-isolation of recent arrivals. Border measures to screen flights and vessels from mainland China and for people who have come from or transited through main-land China in the past 14 days should continue as should the policy of requiring isolation for 14 days after leaving mainland China.11
The WHO continues to reiterate its concern for high-risk nations with weaker health systems that may lack the facilities to identify and man-age COVID-19 cases.12
The current estimates on epidemiological param-eters including severity, transmissibility and incubation period are uncertain. Estimates are likely to change as more information becomes available.
Severity
COVID-19 is a respiratory illness. Patients pre-sent with a wide range of symptoms. Most seem to have mild disease, and about 18% appear to progress to severe disease, including pneumonia, respiratory failure and in some cases death.13 Fever, dry non-productive cough and fatigue are common symptoms. Atypical features include dizziness, headache, vomiting and abdominal pain.14

4 of 14 health.gov.au/cdiCommun Dis Intell (2018) 2020;44(https://doi.org/10.33321/cdi.2020.44.15) Epub 20/2/2020
Table 2: Cumulative confirmed cases of COVID-19 globally, 2019–2020
Country / Special Administrative Region
This reporting week (to 19:00 AEDT 15 Feb 2020) Total cases (from Dec 2019)a
Mainland China (laboratory confirmed) 15,424 49,970
Hubei Province (clinically diagnosed) 16,522 16,522
Cruise ship quarantined in Japanese waters 154 218
Singapore 34 67
Hong Kong 30 56
Japan 16 41
Thailand 2 34
Republic of South Korea 4 28
Malaysia 6 21
Taiwan 2 18
Germany 2 16
Vietnam 3 16
Australia 0 15
United States of America 3 15
France 5 11
Macau 0 10
United Kingdom 6 9
United Arab Emirates 1 8
Canada 0 7
India 0 3
Italy 0 3
Philippines 0 3
Russian Federation 0 2
Spain 1 2
Belgium 0 1
Cambodia 0 1
Egypt 1 1
Finland 0 1
Nepal 0 1
Sri Lanka 0 1
Sweden 0 1
Total 32,216 67,102
a Data taken from WHO Situation Reports.

5 of 14 health.gov.au/cdi Commun Dis Intell (2018) 2020;44(https://doi.org/10.33321/cdi.2020.44.15) Epub 20/2/2020
Figure 1: Confirmed cases of COVID-19 infection by date of illness onset, Australia 2020 (n = 15)a
0
1
2
3
4
5
10/0
1/20
20
11/0
1/20
20
12/0
1/20
20
13/0
1/20
20
14/0
1/20
20
15/0
1/20
20
16/0
1/20
20
17/0
1/20
20
18/0
1/20
20
19/0
1/20
20
20/0
1/20
20
21/0
1/20
20
22/0
1/20
20
23/0
1/20
20
24/0
1/20
20
25/0
1/20
20
26/0
1/20
20
27/0
1/20
20
28/0
1/20
20
29/0
1/20
20
30/0
1/20
20
31/0
1/20
20
1/02
/202
0
2/02
/202
0
3/02
/202
0
4/02
/202
0
5/02
/202
0
6/02
/202
0
7/02
/202
0
8/02
/202
0
9/02
/202
0
10/0
2/20
20
11/0
2/20
20
12/0
2/20
20
13/0
2/20
20
14/0
2/20
20
15/0
2/20
20
Num
ber o
f con
firm
ed C
OVI
D-19
case
s
Date of illness onset
NSW VIC QLD SA
a Date of illness onset for New South Wales, Queensland and Victorian cases has been corrected since Epidemiology Report 2.1
Reports from China on the clinical presentation are limited to novel coronavirus-infected pneu-monia (NCIP) patients. Of patients with NCIP, 30% develop difficulty breathing five days after onset of illness (range 1–10 days).14,15 The median time from onset of illness to hospitalisation for NCIP patients was seven days (range 4–8 days), with acute respiratory distress syndrome (ARDS) experienced on day eight (range 6–12 days).14 Of 138 NCIP patients, approximately a quarter required ICU admission (2% receiving high-flow oxygen, 11% non-invasive ventilation, 9% invasive ventilation and 3% extracorpor-eal membrane oxygenation (ECMO)).14 ICU patients were typically older than 65 years and had a greater number of comorbidities. The first case report from the US described the clinical course and management of a case, including the patient’s initial mild symptoms that progressed to pneumonia on day 9 of illness.6 These studies suggests clinicians should be prepared for some
individuals, who initially present with mild-to-moderate symptoms, to deteriorate over subse-quent days to severe disease.
Evidence on COVID-19 in pregnant women and children is limited. Concern was raised when a baby 30 hours after birth was confirmed with COVID-19; however, close contact history can-not be excluded.16,17 In a small study evaluating the clinical characteristics of nine pregnant women with confirmed COVID-19, no evidence of transplacental or perinatal viral transmission was detected.15 No women developed pneumo-nia or died. Delivery of nine live births by cae-sarean was employed to reduce risk of vertical transmission or due to pre-existing conditions. It is premature to consider a caesarean delivery a universal prevention approach.18 Larger stud-ies with longer duration are needed to confirm these results. According to a recent review, children (ranging from 1 month to 17 years) made up 0.3% (28/9682) of all confirmed cases in Wuhan City by 30 January 2020.19

6 of 14 health.gov.au/cdiCommun Dis Intell (2018) 2020;44(https://doi.org/10.33321/cdi.2020.44.15) Epub 20/2/2020
Cases presented with mild clinical manifesta-tions with some asymptomatic infections.19 No deaths were reported.
The true fatality rate for COVID-19 cannot be presently calculated. Diagnosis of COVID-19 will precede death or recovery by days to weeks. The number of deaths should be compared to past confirmed cases, taking into account this lag period and estimating the fraction of mild under-reported disease.20 In a pre-print, non-peer-reviewed study of 4,021 cases with laboratory-confirmed COVID-19 where approx-imately 48% were aged over 50 years, the case fatality rate (CFR) was 3.06%.21 When stratified by sex and age, male patients had a CFR of 4.45 compared to 1.25 in females, and those ≥ 60 years had a CFR of 5.30 versus those < 60 years of 1.43. This emphasises the importance of early detection in elderly patients, particularly males, to pre-empt clinical deterioration.
Transmission
The exact nature of transmission is poorly under-stood. The WHO has reported ‘during previous outbreaks due to other coronavirus (Middle-East Respiratory Syndrome (MERS) and Severe Acute Respiratory Syndrome (SARS)), human-to-human transmission occurred through droplets, contact and fomites, suggesting that the transmission mode of the 2019-nCoV can be similar’.22 The basic reproductive number, R0, indicates the contagiousness of an infec-tious disease and is defined as the average expected number of secondary cases produced by a single infection in a completely susceptible population. Chinese authorities reported a pre-liminary R0 of 1.4–2.5 on 23 January 2020 to the WHO International Health Regulations (2005) Emergency Committee.23 On 13 February a review of 12 studies which estimated the R0 was published. It found the mean R0 to be 3.28 and median R0 to be 2.79, which exceeds the WHO preliminary R0 of 1.4–2.5 (average 1.95).24 Models using stochastic and statistical methods, such as exponential growth were reasonably
comparable, while mathematical methods pro-duced estimates on the higher side. R0 in more recent studies has stabilised around 2–3.
China and France have reported hospital-related transmission.14,25 In one study from Wuhan, of 138 NCIP patients 41% were presumed infected in the hospital, including 40 healthcare work-ers.14 Media have reported shortages of masks and personal protective equipment in Hubei Province due to the quarantine measures which may have exacerbated the high proportion of hospital-related infections in this study.26 On 14 February China confirmed 1,716 medical staff infected, 87.5% (1502/1716) from Hubei Province, and six deaths.27
Asymptomatic and pre-symptomatic infection has been reported.4,28 A reverse transcription polymerase chain reaction (RT-PCR)-confirmed asymptomatic child was described with radio-logical signs of pneumonia reported from a family cluster in Shenzhen, although onward transmission from this case was not docu-mented.29 On 15 February Egypt confirmed an asymptomatic COVID-19 case. The case was identified through contact screening of an index case who travelled from China to Egypt.30 A report describing a suspected asymptomatic transmission in Germany was proven inaccu-rate once health officials interviewed the patient directly.31
Incubation period
Current estimates of the incubation period of COVID-19 from the WHO range from 2 to 10 days, with these estimates to be refined as more data become available.22 A recently-published article characterising the first 425 cases in Wuhan, Hubei Province China estimated the mean incubation period to be 5.2 days (95% confidence interval, 4.1–7.0 days) with the 95th percentile of the distribution at 12.5 days.32 A modelling paper using known travel history to and from Wuhan and symptom onset date in 88 exported cases calculated the mean incubation period to be 6.4 days (95% confidence interval, 5.6–7.7 days) ranging from 2.1 to 11.1 days (2.5th

7 of 14 health.gov.au/cdi Commun Dis Intell (2018) 2020;44(https://doi.org/10.33321/cdi.2020.44.15) Epub 20/2/2020
and 97.5th percentile).33 Both reports support the use of 14 days as the upper limit of the incubation period used in the Australian interim advice.34 Using 50 patients with well-defined exposure periods Jiang et al. applied various statistical models to the dataset and inferred the mean incubation period was 4.9 days (95% confidence interval, 4.4–5.5 days).35
A pre-print non-peer-reviewed article posted on 9 February retrospectively described the clinical characteristics of 1,099 patients with laboratory-confirmed COVID-19 acute respiratory disease (ARD) from 552 hospitals in 31 provinces in China. The results suggested that the median incubation period was 3 days, ranging from 0 to 24 days.36 The researchers relied on clini-cal records and did not conduct active contact tracing. This study was refuted by two Canadian medical experts who described the reports of patients with 24-day incubation periods as ‘out-liers’ that should be studied further and do not represent a significant shift in thinking around the virus.37
Recommendations for control
The WHO recommends the general public reduce their exposure and transmission to COVID-19 by:
• Frequently cleaning hands by using alcohol-based hand rub or soap and water;
• When coughing and sneezing cover mouth and nose with flexed elbow or tissue – throw tissue away immediately and wash hands;
• Avoid close contact with anyone who has fever and cough; and
• If you have a fever, cough and difficulty breathing seek medical care early and share previous travel history with your health care provider.
Treatment
Currently there is no specific medication recommended for COVID-19. Antibiotics are not effective against viruses. A number of antiviral medications will be trialled to assess whether they can be used to treat COVID-19. Experimental vaccines are also in development.
Clinical care of suspected patients with COVID-19 should focus on early recognition, immediate isolation, implementation of appropriate infec-tion prevention and control measures and provi-sion of optimised supportive care.8
Virology
SARS-CoV-2, the virus that causes COVID-19, is 96% identical to the whole genome sequence of a known bat coronavirus (BATCoV RaTG13) and 79.5% identical to SARS-CoV-1.38 Like SARS-CoV-1, it attaches its spike (S) protein to the angiotensin-converting enzyme 2 (ACE-2) to enter and infect host cells located in the lower respiratory tract.38 Progressive respiratory fail-ure is due to alveolar damage.38
Methods
Data for this report were current as at 19:00 hours AEDT, 15 February 2020.
This report outlines what is known epidemio-logically on COVID-19 in Australia and from publicly available data from WHO Situation Reports, other countries’ official updates and the scientific literature. Data on domestic cases in this report were collected from National Notifiable Diseases Surveillance System (NNDSS) and state and territory case investigation reports. The Communicable Diseases Network Australia (CDNA) developed the case definition for sus-pected and confirmed cases, which was modified at different time points in the epidemic (23 and 27 January and 2, 4, 6, 7 and 14 February 2020) (Table 3). CDNA developed national guidance on investigating suspected and confirmed cases of COVID-19. Based on this guidance, state and territory health department investigators con-

8 of 14 health.gov.au/cdiCommun Dis Intell (2018) 2020;44(https://doi.org/10.33321/cdi.2020.44.15) Epub 20/2/2020
Table 3: Australian COVID-19 case definition as of 15 February 202034
Version Date of development Suspected Cases Confirmed Cases
1.6a 14 February 2020 As the full clinical spectrum of illness is not known, clinical and public health judgement should also be used to determine the need for testing in patients who do not meet the clinical criteria below. If the patient satisfies epidemiological and clinical criteria, they are classified as a suspect case. Epidemiological criteria• Travel to (including transit through)
mainland China in the 14 days before the onset of illness.
OR• Close or casual contact in 14 days before
illness onset with a confirmed case of COVID-19.
Clinical criteria• FeverOR• Acute respiratory infection (e.g.
shortness of breath or cough) with or without fever
A person who tests positive to a specific COVID-19 PCR test (when available) or has the virus identified by electron microscopy or viral culture, at a reference laboratory.
a Version 1.6 includes updated information about personal protective equipment.
ducted interviews of suspected cases to collect core and enhanced data for inclusion in NNDSS. Data were analysed using Stata to describe the epidemiology of infections in Australia and the progress of the epidemic.
Previous case definitions are provided in Appendix A.
Data for the international cases of COVID-19 by country were compiled from the latest WHO Situation Report. Case definitions may vary by country making comparisons difficult. Rapid reviews of the current state of knowledge on COVID-19 were conducted from the literature using PubMed.
Acknowledgements
This report represents surveillance data reported through CDNA as part of the nationally-coordi-nated response to COVID-19. We thank public health staff from incident emergency operations centres in state & territory health departments,
and the Australian Government Department of Health; along with state and territory public health laboratories.
Author details
Corresponding author
Malinda Chea NIR Surveillance Team, Communicable Disease Epidemiology and Surveillance Section, Health Protection Policy Branch, Australian Government Department of Health, GPO Box 9484, MDP 14, Canberra, ACT 2601. Telephone: +61 2 6289 1512. Email: [email protected]
References
1. COVID-19 National Incident Room Surveil-lance Team. COVID-19, Australia: Epide-miology Report 2. Reporting week ending 19:00 AEDT 8 February 2020. Commun Dis Intell (2018). 2020;44. doi: https://doi.org/10.33321/cdi.2020.44.14.
9 of 14 health.gov.au/cdi Commun Dis Intell (2018) 2020;44(https://doi.org/10.33321/cdi.2020.44.15) Epub 20/2/2020
2. Health Commission of Hubei Province. Epidemic situation of new coronavirus pneumonia in Hubei Province on February 12, 2020. [Internet.] Hubei Province: Health Commission of Hubei Province; 2020. [Ac-cessed on 13 February 2020.] Available from: http://wjw.hubei.gov.cn/fbjd/dtyw/202002/t20200213_2025581.shtml.
3. World Health Organization (WHO). Coro-navirus disease 2019 (COVID-19) situa-tion report-24: 13 February 2020. Geneva: WHO; 2020. [Accessed on 13 February 2020.] Available from: https://www.who.int/docs/default-source/coronaviruse/situa-tion-reports/20200213-sitrep-24-covid-19.pdf?sfvrsn=9a7406a4_4.
4. WHO. Coronavirus disease 2019 (COV-ID-19) situation report-26: 15 February 2020. Geneva: WHO; 2020. [Accessed on 16 Febru-ary 2020.] Available from: https://www.who.int/docs/default-source/coronaviruse/situa-tion-reports/20200215-sitrep-26-covid-19.pdf?sfvrsn=a4cc6787_2.
5. WHO. Statement on the second meeting of the International Health Regulations (2005) Emergency Committee regarding the outbreak of novel coronavirus (2019-nCoV). [Internet.] Geneva: WHO; 2020. [Accessed on 31 January 2020.] Available from: https://www.who.int/news-room/detail/30-01-2020-statement-on-the-sec-ond-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavi-rus-(2019-ncov).
6. Holshue ML, DeBolt C, Lindquist S, Lofy KH, Wiesman J, Bruce H et al. First case of 2019 novel coronavirus in the United States. N Engl J Med. 2020. doi: https://10.1056/NEJ-Moa2001191.
7. Yoo JH, Hong ST. The outbreak cases with the novel coronavirus suggest upgraded quaran-tine and isolation in Korea. J Korean Med Sci. 2020;35(5):e62.
8. Reuters. Wuhan lockdown ‘unprededented’, shows commitment to contain virus: WHO representative in China. [Internet.] London: Reuters; 23 January 2020. [Accessed on 7 February 2020.] Available from: https://www.reuters.com/article/us-china-health-who-idUSKBN1ZM1G9.
9. The New York Times. China tightens Wuhan lockdown in ‘wartime’ battle with coronavi-rus. [Internet.] New York: New York Times; 6 February 2020. [Accessed on 7 February 2020.] Available from: https://www.nytimes.com/2020/02/06/world/asia/coronavirus-china-wuhan-quarantine.html.
10. Australian Government Department of Health. Australian Health Protection Princi-pal Committee (AHPPC) novel coronavirus statement on 1 February 2020. [Internet.] Canberra: Australian Government Depart-ment of Health; 2020. [Accessed on 7 Feb-ruary 2020.] Available from: https://www.health.gov.au/news/australian-health-protec-tion-principal-committee-ahppc-novel-coro-navirus-statement-on-1-february-2020.
11. Australian Government Department of Health. Australian Health Protection Princi-pal Committee (AHPPC) resolution on travel restrictions and coronavirus (COVID-19). [Internet.] Canberra: Australian Government Department of Health; 2020. [Accessed on 14 February 2020.] Available from: https://www.health.gov.au/news/australian-health-protec-tion-principal-committee-ahppc-resolution-on-travel-restrictions-and-coronavirus-covid-19.
12. WHO. Munich Security Conference. [Inter-net.] Geneva: WHO; 2020. [Accessed on 15 February 2020.] Available from: https://www.who.int/dg/speeches/detail/munich-security-conference.
13. WHO. Novel coronavirus (2019-nCoV) situation report-8: 28 January 2020. Ge-neva: WHO; 2020. [Accessed on 29 January 2020.] Available from: https://www.who.int/

10 of 14 health.gov.au/cdiCommun Dis Intell (2018) 2020;44(https://doi.org/10.33321/cdi.2020.44.15) Epub 20/2/2020
docs/default-source/coronaviruse/situation-reports/20200128-sitrep-8-ncov-cleared.pdf?sfvrsn=8b671ce5_2.
14. Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J et al. Clinical characteristics of 138 hos-pitalized patients with 2019 novel coro-navirus–infected pneumonia in Wuhan, China. JAMA. 2020. https://doi.org/10.1001/jama.2020.1585.
15. Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y et al. Epidemiological and clini-cal characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020.doi: https://doi.org/10.1016/S0140-6736(20)30211-7.
16. National Health Commission, China. Transcript of press conference on February 7, 2020. [Internet.] Beijing: National Health Commission; 2020. [Accessed on 15 Febru-ary 2020.] Available from: http://www.nhc.gov.cn/xcs/s3574/202002/5bc099fc9144445297e8776838e57ddc.shtml.
17. Qiao J. What are the risks of COVID-19 infection in pregnant women? Lancet. 2020. doi: https://doi.org/10.1016/S0140-6736(20)30365-2.
18. Wald A. COVID-19 infection during preg-nancy’s third trimester. [Internet.] Waltham, MA: Massachusetts Medical Society; 2020. [Accessed on 15 February 2020.] Available from: https://www.jwatch.org/na50916/2020/02/14/covid-19-infection-during-pregnancys-third-trimester.
19. Shen K, Yang Y, Wang T, Zhao D, Jiang Y, Jin R et al. Diagnosis, treatment, and prevention of 2019 novel coronavirus infection in chil-dren: experts’ consensus statement. World J Pediatr. 2020. https://doi.org/10.1007/s12519-020-00343-7.
20. Battegay M, Kuehl R, Tschudin-Sutter S, Hirsch HH, Widmer AF, Neher RA. 2019-novel coronavirus (2019-nCoV): esti-
mating the case fatality rate - a word of cau-tion. Swiss Med Wkly. 2020;150:w20203.
21. Yang Y, Lu Q, Liu M, Wang Y, Zhang A, Jalali N et al. Epidemiological and clinical features of the 2019 novel coronavirus out-break in China. medRxiv. 2020. doi: https://doi.org/10.1101/2020.02.10.20021675.
22. WHO. Novel coronavirus (2019-nCoV) situation report-7: 27 January 2020. Ge-neva: WHO; 2020. [Accessed on 28 January 2020.] Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200127-sitrep-7-2019--ncov.pdf?sfvrsn=98ef79f5_2.
23. WHO. Statement on the meeting of the International Health Regulations (2005) Emergency Committee regarding the out-break of novel coronavirus (2019-nCoV). [Internet.] Geneva: WHO; 2020. [Ac-cessed on 24 January 2020.] Available from: https://www.who.int/news-room/detail/23-01-2020-statement-on-the-meet-ing-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavirus-(2019-ncov).
24. Liu Y, Gayle AA, Wilder-Smith A, Rocklöv J. The reproductive number of COVID-19 is higher compared to SARS coronavi-rus. J Travel Med. 2020. doi: https://doi.org/10.1093/jtm/taaa021.
25. WHO. Novel coronavirus (2019-nCoV) situation report-12: 1 February 2020. Ge-neva: WHO; 2020. [Accessed on 1 Febru-ary 2020.] Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200201-sitrep-12-ncov.pdf?sfvrsn=273c5d35_2.
26. Reuters. China’s coronavirus-hit Hubei says medical supply tightness easing, shortages persist. [Internet.] London: Reuters; 9 Feb-ruary 2020. [Accessed on 9 February 2020.] Available from: https://www.reuters.com/ar-ticle/us-china-health-hubei/chinas-coronavi-

11 of 14 health.gov.au/cdi Commun Dis Intell (2018) 2020;44(https://doi.org/10.33321/cdi.2020.44.15) Epub 20/2/2020
rus-hit-hubei-says-medical-supply-tightness-easing-shortages-persist-idUSKBN2020MF.
27. Center for Infectious Disease Research and Policy. COVID-19 sickens over 1,700 health workers in China, killing 6. [Internet.] Minneapolis: CIDRAP – Center for Infec-tious Disease Research and Policy; 2020. [Accessed on 16 February 2020.] Available from: http://www.cidrap.umn.edu/news-perspective/2020/02/covid-19-sickens-over-1700-health-workers-china-killing-6.
28. Chang D, Xu H, Rebaza A, Sharma L, Dela Cruz CS. Protecting health-care work-ers from subclinical coronavirus infection. Lancet Respir Med. 2020. doi: https://doi.org/10.1016/S2213-2600(20)30066-7.
29. Chan JF, Yuan S, Kok KH, To KK, Chu H, Yang J et al. A familial cluster of pneumonia associated with the 2019 novel coronavi-rus indicating person-to-person transmis-sion: a study of a family cluster. Lancet. 2020. doi: https://doi.org/10.1016/S0140-6736(20)30154-9.
30. WHO. Update on COVID-19 in the Eastern Mediterranean Region. [Internet.] Cairo: Re-gional Office for the Eastern Mediterranean, WHO; 2020. Available from: http://www.emro.who.int/media/news/update-on-covid-19-in-the-eastern-mediterranean-region.html.
31. Wilson ME. Clarification: Asymptomatic 2019-nCoV Transmission in Germany. [In-ternet.] Waltham, MA: New England Journal of Medicine, NEJM Group; 2020. [Accessed on 16 February 2020.] Available from: htt-ps://www.jwatch.org/na50871/2020/02/07/clarification-asymptomatic-2019-ncov-trans-mission-germany.
32. Li Q, Guan X, Wu P, Wang X, Zhou L, Tong Y et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N Engl J Med. 2020. doi: https://doi.org/10.1056/NEJMoa2001316.
33. Backer JA, Klinkenberg D, Wallinga J. In-cubation period of 2019 novel coronavirus (2019-nCoV) infections among travellers from Wuhan, China, 20–28 January 2020. Eurosurveillance. 2020;25(5):2000062.
34. Australian Government Department of Health. Coronavirus disease 2019 (COV-ID-19) - CDNA national guidelines for pub-lic health units. [Internet.] Canberra: Aus-tralian Government Department of Health; 2020. [Accessed on 14 February 2020.] Available from: https://www1.health.gov.au/internet/main/publishing.nsf/Content/cdna-song-novel-coronavirus.htm.
35. Jiang X, Rayner S, Luo MH. Does SARS‐CoV‐2 has a longer incubation period than SARS and MERS? J Med Virol. 2020. doi: https://doi.org/10.1002/jmv.25708.
36. 36. Guan W-j, Ni Z-y, Hu Y, Liang W-h, Ou C-q, He J-x et al. Clinical characteristics of 2019 novel coronavirus infection in China. medRxiv. doi: https://doi.org/10.1101/2020.02.06.20020974.
37. CTVNews. Experts skeptical of report sug-gesting some coronavirus patients don’t show symptoms for 24 days. [Internet.] Toronto: Bell Media; 2020. [Accessed on 14 February 2020.] Available from: https://www.ctvnews.ca/world/experts-skeptical-of-report-sug-gesting-some-coronavirus-patients-don-t-show-symptoms-for-24-days-1.4807571.
38. Zhou P, Yang X-L, Wang X-G, Hu B, Zhang L, Zhang W et al. A pneumonia outbreak associated with a new coronavirus of prob-able bat origin. Nature. 2020. doi: https://doi.org/10.1038/s41586-020-2012-7.

12 of 14 health.gov.au/cdiCommun Dis Intell (2018) 2020;44(https://doi.org/10.33321/cdi.2020.44.15) Epub 20/2/2020
App
endi
xA
ppen
dix
A –
Pre
viou
s cas
e de
finiti
ons a
nd co
ntac
t defi
nitio
nsa
c fici n e
o a
sp) oe rtl cb ea lli t a
e t av y e
, avn
a eti d b ri ue
os e tfih lti u
s p w l c.yn r
s t t ( e a os s de r te e i as s i ra o
tR
tu r v o
C h C ri
d y o
e lab
n w 9 P e v p e
m o1o -s
th ccr n
onfi sr DI a os ee rV
A p eO r h
rci feC C o m r
e . s9 a1
e f - f t D d c
n e r t o
y a I r t o e .re e e e t e
m cs v s
e t th V
O ve, t
h ne f C n ee e
g e t f e o sp t fd e o
e o u u u
th ju t m
ai o or s r se aoo
n t e th
th e th
thr ii rl r o o d o
a f d c i
f ee l co
d ee r w e r wa
th o m
c h c s b m ri r s b
fili h n y fi y th o
bu s w
d p t d
cli nn i ia a
) w4 d
4 d
h
n e 1
u e 1
th a
co
th a
co ) whn n g ge l a uti
l a a oa ig n th oca t w r c r cc n th
ii
t w
i n p
o a i en g
i l so n n th o a i esnn th
o
, cli n i ii hti m h
ss o a
d C e ss
o a
d C en r rs ew e d ei f b e f bo r t n n lnpn a ln a lo
t k s e ll n ss
o
d f n ss
o l e i
i e i
e i re a r ea oo es
n ) m
o ne ) m
nfi ff t t
e n s e r e rti o o
s i a h s b hh s b
hg gs y ue e th t s . s yu a . sn a
ln o g ge .l n ei tif i 4 d or . re 4 d
m n (
m o
a t th
t th
r i n 1
o i n 1 n (
s se . n t i n tit e p o iti a
u ert f th es ia a c cca r e ia ta c
o d r er a f a
. I t c g t r ft n tc nn g t
ned
t w
l sp c it
en o it
en or y
i
o e i y i
r i
e l c d l c r c d l c r
s e sp o
se
s a ta alu u a alc clu
ia r clu oa t
iaa i e u
a b uic . a
no
b s a
s ic rn s r i n s ig i ii ait
e sp g a -19 r
C r oe l o ( o sp
d l cli r c e l o (
r c Dt I ite
es i l t r
te
. c .l r l t rV cu l d a
mio e ss e o r e r
mio ss r e
r
c l c e e o .
O
e e f d a e tv ala ve
te v eufi e e ac os al C vel os ua cp
s th u c i ln ic ln icis ss d r l r l fT li C Ti Fe A d l
n i C o
u a p p lin
Ao i Fe
R lin R R RhS A s cli
cl E O C O E O • • • • • • C • O •
t 20 20n 20
20
y yr ra af pme
e o lo u ur r
e b bt v e ea e F FD d 7 6
noisrVe
5 4
1. 1.

13 of 14 health.gov.au/cdi Commun Dis Intell (2018) 2020;44(https://doi.org/10.33321/cdi.2020.44.15) Epub 20/2/2020
sesa Cde
mron
fiC
l a
f n cii g f f f :
t o
f th of . lr e o
t o s i o e o
e e e o
e o )e a .s
d c rs , w t i cv f n a d nen e n k t o o a e
e o s
e o v a ra t f de t o e e h r r
d c u vc f f
it s e
e th
ra so
y o tb ne e e
t
l oe r at th t l u o c o e
r c i e th
rr sp . n o
o e o o ssf d o r s
iu ne f n
e r wsp
f t e d
th o e r s th
asi e . n
i
r du ln 9 h o
s b
s b
d o i
n w r h 1 el a
f i th c
li
r s
- u g vsy i y cl Da o r o
u i
a
d o
) w
e
t o e I n ( o . e
4 d
4 d m Vti e l wr oc v e O , c ea .ie h fi ti t
e 1 m e 1 se eg in f n r a
d
f C c th e (
u o n
e o , o e o mn os
p
n th
r t f e a
fi o
n th
th a
c y i f eu n r on oo r c o s rro y
i
th e th a f b
h o i o
h d
a i
th a
c a i rt ii ss na
r w
r i o yn trt n i oi aa f ss o n t
i oh h r e i
d C i e t w sp
th o e smn th
a c
i nt ss
t w d C
s b i ss
s
r e e
t w sp e
f b
s a in f r rri ey o mrtn esl ss
o n eaa a n t
t o ) w sl ss o e r sh d i
n an n tt n : s
e fi
ss o ei e a u y
d
s 4 d
m g a
a c
hu
nn ln
) m
n il ss o ra o ort te r e
1
e o
) m o e i an rh n o re d a i- uh ln o ln n il h r e qg g o e
th
ld n th t
e i . s r - t o e spu u f o ) an se d e i
eao r g Co a i
.
s b r s a n
r
o r u rr ns i ss o 8 ° e
t th f e m
t th
h o f t l o e
r
e n ( ey h te 3 ti u
s b a n
(
ln ci o i ≥ c
4 d o gs s , C
n th a eti e f hu
l s b
y ti u f i r ( fn y
ia ia o ia c i n r aa a c a
e 1 c ear
4 d e r e , c n s
o
r rg
t r if a t ov a o
g t fn n e eo r s 4 d v y
i
e n w
ite
ite th ite r
f f
i
n 1
n 1 o o
y i n r ti r i y i nn a n tir r oa c d r i c n
th
cd r e c d a
rs
clu o i o i P y
oe i
a
f b
e ett e o i m
alse
ua al clu ra a rt ft a al b e tr o nc spic c ia ic c ia ic r o ia t er r u ea n a r i n a i g f a sr r ng i nt .
ite sp g C o ite e y
i
o ( i nt sp ss o g i
o ( .
-19 ro -19 o nt e
r
l r h oo e e tl f pd o o
mio r
mio r e l o
H
o a
ite
. c e r l t . s
b
l t e r n
mio l t
t u
te . c l t y c r ass D c r ss D c c ce e I e e r e o
t e e a eal ve
I t r o
al r al
it
e a
4 d e
sp
cc v e s V s u v su v e V ve o v ne a ln o O e a ln oic O ic e a a oc c )p d r r h r r icT li C Fe d C A T Ti Cl A T li Cl d 1s i s i Cl e r eer ervu p lin
eF
R p R lin
dR p R R lin R i ve vS E • O • C • O • E • O E • C • • O • O • C • O S e fe
t 20 20 02n 20
20 0
f pme y y y 2
r r ra a a
e o lo u ur r nue b b at v e ea e F F 7
J
D d 4 2 2
noisrVe
3 2 .11. 1. 1
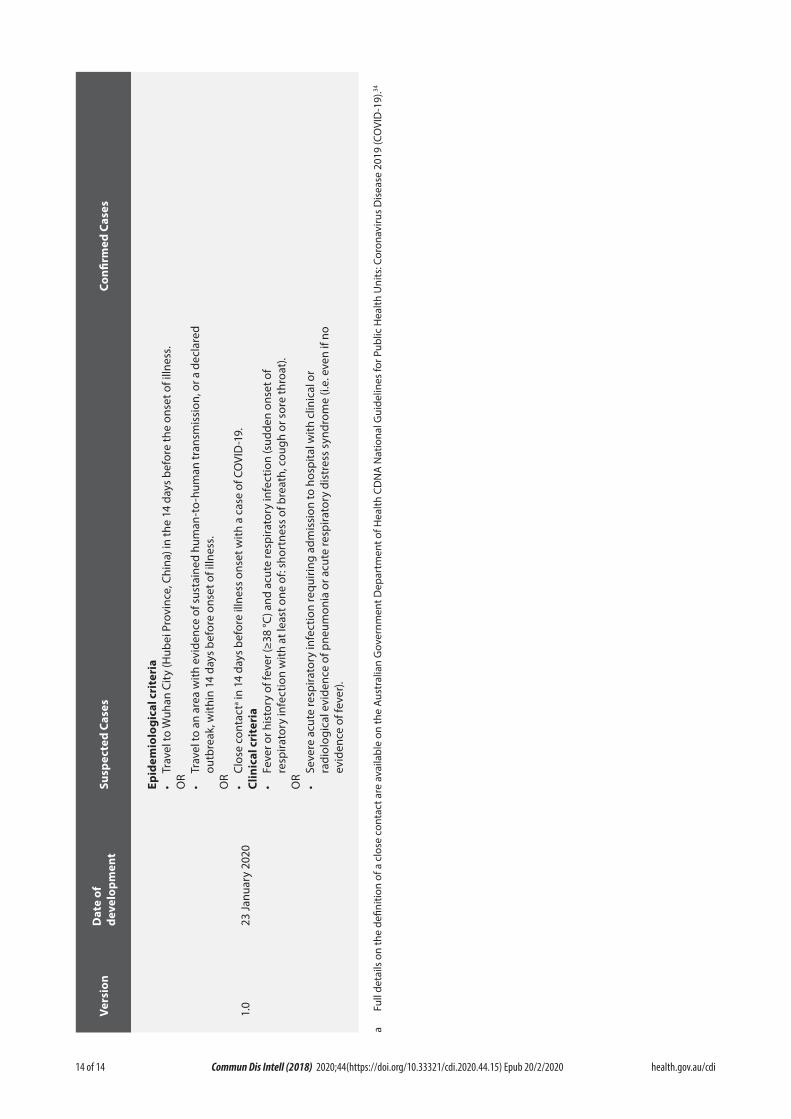
14 of 14 health.gov.au/cdiCommun Dis Intell (2018) 2020;44(https://doi.org/10.33321/cdi.2020.44.15) Epub 20/2/2020
sesa Cde
mron
fiC
d o era f n.ss cl n i
e e .
r a d
) e
ln t vf a r l o . ef i t o r l o e
t o , o e h a .
sne e t cn i e (i
ns on i n o ro
th c
li m
ss
e o oi e r s r
sm
. dd h o d
e th 9 i n1n - u yga l wD sr r n
( u ao
n t I oV ti ss
s
f ee O o , ca ti osp r
s b th t
m f C sc i
ya hu- e o e af en y d
4 d r o
h
so a y i
n t ro
e 1 t f b
ss o
t-
th a
c r oo an i rt
n th
a ss ia
m r e ii. spn m
ss
i
) i t w sp et dre e o e r
a d hu
ln e t
ni e r h g
aue l s nth f i n i cn : su ri ia c u r a, C
f
t t o qe s e ss o
e o
u ec s d a
n e a o
n f s n ln ni n r inlv t os oo e
o ) ae i o
r e o
r r C a ti m
i P c eo o c un f f 8 °
t l e eee e e 3
bu s b s b ≥
y y r ( th a f nndiv f p
H
th e i y
i
ia e ra a v e o
y (
ei n w or t
ite a cti 4
d
4 d
a w f f n
n 1
n 1 o r
n C i .
y o ti sp e )r c di er c ia e i e e vs al th r v
se
ar fh t o n feic cu i t e r
n a ia l ea
o W , w a s t fr ag
o a nt ite i y
i
u C r hr c oo ck o i ed l oe e
a g
te
mio
a
l t l t
t c r a o c r le e r e r o ric v tb os ev al e ie e a a o v sp v dr r u ic e iden
c
p e vd e aT T o Cllin
F r S r es iu p R R R
S E • O • O C O • • •
0t 2
n 0
pme y 2
raf e
o lo nue at va e 3 J
D d 2
noisrVe
01.
a Fu
ll de
tails
on
the
defin
ition
of a
clo
se c
onta
ct a
re a
vaila
ble
on th
e Au
stra
lian
Gov
ernm
ent D
epar
tmen
t of H
ealth
CD
NA
Nat
iona
l Gui
delin
es fo
r Pub
lic H
ealth
Uni
ts: C
oron
aviru
s D
isea
se 2
019
(CO
VID
-19)
.34

2 0 2 0 V o l u m e 4 4https://doi.org/10.33321/cdi.2020.44.17
COVID-19, Australia: Epidemiology Report 4:Reporting week ending 19:00 AEDT 22 February 2020
COVID-19 National Incident Room Surveillance Team

Communicable Diseases Intelligence ISSN: 2209-6051 Online
This journal is indexed by Index Medicus and Medline.
Creative Commons Licence - Attribution-NonCommercial-NoDerivatives CC BY-NC-ND
© 2020 Commonwealth of Australia as represented by the Department of Health
This publication is licensed under a Creative Commons Attribution- Non-Commercial NoDerivatives 4.0 International Licence from https://creativecommons.org/licenses/by-nc-nd/4.0/legalcode (Licence). You must read and understand the Licence before using any material from this publication.
Restrictions The Licence does not cover, and there is no permission given for, use of any of the following material found in this publication (if any):
• the Commonwealth Coat of Arms (by way of information, the terms under which the Coat of Arms may be used can be found at www.itsanhonour.gov.au);
• any logos (including the Department of Health’s logo) and trademarks;
• any photographs and images;
• any signatures; and
• any material belonging to third parties.
Disclaimer Opinions expressed in Communicable Diseases Intelligence are those of the authors and not necessarily those of the Australian Government Department of Health or the Communicable Diseases Network Australia. Data may be subject to revision.
Enquiries Enquiries regarding any other use of this publication should be addressed to the Communication Branch, Department of Health, GPO Box 9848, Canberra ACT 2601, or via e-mail to: [email protected]
Communicable Diseases Network Australia Communicable Diseases Intelligence contributes to the work of the Communicable Diseases Network Australia. http://www.health.gov.au/cdna
Communicable Diseases Intelligence (CDI) is a peer-reviewed scientific journal published by the Office of Health Protection, Department of Health. The journal aims to disseminate information on the epidemiology, surveillance, prevention and control of communicable diseases of relevance to Australia.
Editor Cindy Toms
Deputy Editor Simon Petrie
Design and Production Kasra Yousefi
Editorial Advisory Board David Durrheim, Mark Ferson, John Kaldor, Martyn Kirk and Linda Selvey
Website http://www.health.gov.au/cdi
Contacts Communicable Diseases Intelligence is produced by: Health Protection Policy Branch Office of Health Protection Australian Government Department of Health GPO Box 9848, (MDP 6) CANBERRA ACT 2601
Email: [email protected]
Submit an Article You are invited to submit your next communicable disease related article to the Communicable Diseases Intelligence (CDI) for consideration. More information regarding CDI can be found at: http://health.gov.au/cdi.
Further enquiries should be directed to: [email protected].

1 of 11 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.17) Epub 26/2/2020
Weekly epidemiological report
COVID-19, Australia: Epidemiology Report 4:Reporting week ending 19:00 AEDT 22 February 2020
COVID-19 National Incident Room Surveillance Team
Summary
This is the fourth epidemiological report for coronavirus disease 2019 (COVID-19), reported in Australia as at 19:00 Australian Eastern Daylight Time [AEDT] 22 February 2020. It includes data on COVID-19 cases diagnosed in Australia, the international situation and a review of current evidence.
Keywords: SARS-CoV-2; novel coronavirus; 2019-nCoV; coronavirus disease 2019; COVID-19; acute respiratory disease; case definition; epidemiology; Australia
The following epidemiological data are subject to change both domestically and internationally due to the rapidly evolving situation. Australian cases are still under active investigation. While every effort has been made to standardise the investigation of cases nationally, there may be some differences between jurisdictions.
In Australia:
• 22 COVID-19 cases were notified up until19:00 AEDT 22 February 2020;
• The first 15 cases are all considered to havehad a direct or indirect link to Wuhan, HubeiProvince, China;
• The seven most recent cases were among the‘Diamond Princess’ passengers repatriatedon a flight from Japan to the Northern Terri-tory on 20 February 2020;
• Zero deaths were reported; and
• On 20 February 2020, the AustralianHealth Protection Principal Committee(AHPPC) issued a statement recommend-ing that the current travel restrictions formainland China remain in place for a furtherseven days.
Internationally:
• 77,794 infections have been confirmed glob-ally, with 2,359 deaths;
• The majority of confirmed infections (98%;n = 76,288) and deaths (99%; n = 2,345) havebeen reported in mainland China;
• On 19 February 2020, the case reportingfrom Hubei Province was revised to removecases that have been diagnosed clinicallywithout laboratory confirmation;
• Fourteen deaths were reported outside main-land China – four in Iran (Islamic Republicof), two each in Hong Kong SAR, Republicof Korea and from the ‘Diamond Princess’cruise ship, and one each in France, Japan,the Philippines and Taiwan; and
• Republic of Korea has reported a substantialincrease in confirmed cases. There were 318confirmed cases in the current reportingweek compared to four cases reported in thepreceding week.

2 of 11 health.gov.au/cdiCommun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.17) Epub 26/2/2020
Domestic cases
There were 22 confirmed cases reported in Australia as at 19:00 AEDT 22 February 2020 (Table 1). Seven of the 22 confirmed cases were among the ‘Diamond Princess’ passengers (n = 164) repatriated on a flight from Japan to the Northern Territory on 20 February 2020. The remaining cases were reported in New South Wales (n = 4), Victoria (n = 4), Queensland (n = 5) and South Australia (n = 2).
As at 19:00 AEDT 22 February 2020, details were not available for the seven cases from the ‘Diamond Princess’. The following is therefore a summary of the first 15 cases reported in Australia. The first case in Australia reported onset of signs and symptoms on 13 January 2020 (Figure 1). The median age of cases was 43 years (range 8–66 years). The male-to-female ratio was 1.5:1. Fourteen cases (93%) reported fever and/or chills, 11 cases (73%) reported cough, and two cases were reported to have pneumonia. Eleven (73%) of the 15 cases were hospitalised for clinical management and infection control. The remaining cases were assessed to be well enough to self-isolate at home. At the time of reporting, ten of these cases were reported to have recovered. No deaths were reported.
Evidence of limited secondary transmission of COVID-19 in Australia is thought to have occurred for three cases who were part of a five person cluster identified in Queensland. The cluster of confirmed COVID-19 cases were part of a small group of nine people from mainland China that had been travelling together. The initial case among this group was isolated upon presentation to hospital, and all others in the travel group were also quarantined. Four mem-bers of this group were subsequently confirmed as cases. Of these, three cases were consistent with secondary transmission from the initial case due to their close contact prior to isolation. The remaining case had been in Wuhan, Hubei Province during the 14 days prior to illness onset and was considered a co-primary case.
International cases
On 19 February 2020, the National Health Commission of the People’s Republic of China removed the case classification of ‘clinically diagnosed’ that had previously been used for cases reported in Hubei Province. Confirmed cases are those testing positive by RT-PCR or gene sequencing.1 This change in reporting has meant that some cases that had previously been clinically diagnosed would now be removed as they have since tested negative. This has resulted
Table 1: Cumulative notified cases of confirmed COVID-19 by jurisdiction, Australia, 2020 (n = 22)
JurisdictionThis week
(to 19:00 AEDT 22 Feb) No. of cases
Last week (to 19:00 AEDT 15 Feb)
No. of cases
Total cases (to 19:00 AEDT 22 Feb
2020) No. of cases
NSW 0 0 4
Vic 0 0 4
Qld 0 0 5
WA 0 0 0
SA 0 0 2
Tas 0 0 0
NT 0 0 0
ACT 0 0 0
Repatriation (Diamond Princess) 7 0 7
Total cases 7 0 22

3 of 11 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.17) Epub 26/2/2020
Figure 1: Confirmed cases of COVID-19 by date of illness onset, Australia 2020 (n = 15)a
0
1
2
3
4
5
10/0
1/20
2011
/01/
2020
12/0
1/20
2013
/01/
2020
14/0
1/20
2015
/01/
2020
16/0
1/20
2017
/01/
2020
18/0
1/20
2019
/01/
2020
20/0
1/20
2021
/01/
2020
22/0
1/20
2023
/01/
2020
24/0
1/20
2025
/01/
2020
26/0
1/20
2027
/01/
2020
28/0
1/20
2029
/01/
2020
30/0
1/20
2031
/01/
2020
1/02
/202
02/
02/2
020
3/02
/202
04/
02/2
020
5/02
/202
06/
02/2
020
7/02
/202
08/
02/2
020
9/02
/202
010
/02/
2020
11/0
2/20
2012
/02/
2020
13/0
2/20
2014
/02/
2020
15/0
2/20
2016
/02/
2020
17/0
2/20
2018
/02/
2020
19/0
2/20
2020
/02/
2020
21/0
2/20
2022
/02/
2020
Num
ber o
f con
firm
ed 2
019-
nCoV
case
s
Date of illness onset
NSW VIC QLD SA Limited local transmission
a Cases from the ‘Diamond Princess’ (n = 7) were not included.
in an apparent slowing of reported cases, especially from Hubei Province in the current reporting week.
As at 19:00 AEDT 22 February 2020, the number of confirmed COVID-19 cases was 77,794 glob-ally (Table 2). Mainland China reported 98% of cases (n = 76,288) and 2,345 deaths. Thirty-one countries and Special Administrative Regions outside of mainland China reported 872 con-firmed COVID-19 cases. An additional 634 confirmed cases were associated with the cruise ship ‘Diamond Princess’. Fourteen deaths were reported outside mainland China: four in Iran (Islamic Republic of), two each in Hong Kong SAR, Republic of Korea and from the ‘Diamond Princess’ cruise ship, and one each in France, Japan, the Philippines and Taiwan.2 Seventeen countries (Australia, Egypt, France, Germany, Iran, Israel, Italy, Japan, Malaysia, Republic of Korea, Singapore, Spain, Thailand, UAE, UK, USA and Vietnam) reported possible or con-firmed limited local transmission.2
There is growing evidence of sustained local transmission in some countries. Over the reporting week, the Republic of Korea had a large increase in confirmed cases from 4 to 318.3 Cases were primarily from two clusters, one linked to a church group and the other linked to a hospital.4 Japan also reported an increase in confirmed cases over the reporting week, with the majority not linked to travel to Hubei Province.5 Since the last reporting week, three new countries (Lebanon, Iran and Israel) have reported cases of COVID-19. Iran reported 18 cases and four deaths.2
Background
The World Health Organization (WHO) declared the outbreak of COVID-19 a Public Health Emergency of International Concern (PHEIC) on 30 January 2020.6 Cases were ini-tially associated with exposure to a wet market, located in Wuhan, Hubei Province, China, indicating a possible zoonotic source. Sustained

4 of 11 health.gov.au/cdiCommun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.17) Epub 26/2/2020
Tabl
e 2:
Cum
ulat
ive
confi
rmed
cas
es o
f CO
VID
-19
glob
ally
, 201
9–20
20
Coun
try
/ Spe
cial
Adm
inis
trat
ive
Regi
onTh
is re
port
ing
wee
k (t
o 19
:00
AED
T 22
Feb
202
0)La
st re
port
ing
wee
k (t
o 19
:00
AED
T 15
Fe
b 20
20)
Tota
l cas
es (f
rom
Dec
201
9)a
Mai
nlan
d Ch
ina
9,79
631
,946
b76
,288
Crui
se s
hip
quar
antin
ed in
Japa
nese
wat
ers
416
154
634
Repu
blic
of K
orea
318
434
6
Japa
n64
1610
5
Sing
apor
e19
3486
Hon
g Ko
ng12
3068
Thai
land
12
35
Uni
ted
Stat
es o
f Am
eric
a20
335
Taiw
an8
226
Mal
aysi
a1
622
Aus
tral
ia6c
021
c
Iran
(Isla
mic
Rep
ublic
of)
180
18
Ger
man
y0
216
Viet
nam
03
16
Fran
ce1
512
Uni
ted
Ara
b Em
irate
s3
111
Mac
au0
010
Italy
60
9
Uni
ted
King
dom
06
9
Cana
da1
08
Indi
a0
03
Phili
ppin
es0
03
Russ
ian
Fede
ratio
n0
02

5 of 11 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.17) Epub 26/2/2020
Coun
try
/ Spe
cial
Adm
inis
trat
ive
Regi
onTh
is re
port
ing
wee
k (t
o 19
:00
AED
T 22
Feb
202
0)La
st re
port
ing
wee
k (t
o 19
:00
AED
T 15
Fe
b 20
20)
Tota
l cas
es (f
rom
Dec
201
9)a
Spai
n0
12
Belg
ium
00
1
Cam
bodi
a0
01
Egyp
t0
11
Finl
and
00
1
Isra
el1
01
Leba
non
10
1
Nep
al0
01
Sri L
anka
00
1
Swed
en0
01
Tota
l10
,692
32,2
1677
,794
a D
ata
take
n fr
om W
HO
Situ
atio
n Re
port
s.b
Incl
udes
clin
ical
ly d
iagn
osed
cas
es (n
= 1
6,52
2) in
Hub
ei P
rovi
nce,
Chi
na.
c Th
is is
diff
eren
t to
the
case
num
bers
repo
rted
in p
revi
ous
sect
ions
of t
his
repo
rt (i
.e. T
able
1),
whi
ch m
ay b
e du
e to
the
inte
rnal
cut
-off
times
use
d by
WH
O fo
r rep
ortin
g.

6 of 11 health.gov.au/cdiCommun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.17) Epub 26/2/2020
human-to-human transmission is now occur-ring in the majority of provinces outside of Hubei Province in China. In an effort to contain the spread of the virus, Chinese authorities imposed a lockdown on the city of Wuhan on 23 January 2020 – suspending all public transport including international flights – and extended the measure to neighbouring cities in Hubei Province over subsequent days.7
Following advice from the Australian Health Protection Principal Committee (AHPPC) to substantially reduce the volume of travellers coming from mainland China, additional border measures were implemented in Australia. From 1 February 2020, Australia denied entry to any-one who had left or transited through mainland China, with the exception of Australian citizens, permanent residents and their immediate family and air crew who have been using appropriate personal protective equipment.8 On 20 February 2020, AHPPC released a statement recommend-ing current travel restrictions remain in place for a further seven days.9 AHPPC noted the con-tinuing growth in COVID-19 cases and deaths in the Hubei Province of China, and acknowl-edged that, while there has been an apparent slowing in case numbers in other provinces of mainland China, it is unclear whether this slow-ing will continue as Chinese employees return to work after the holiday period. Border meas-ures to screen flights and vessels from mainland China and for people who have come from or transited through mainland China were also recommended to continue.9
The current estimates on epidemiological param-eters including severity, transmissibility and incubation period are uncertain. Estimates are likely to change as more information becomes available.
Severity
COVID-19 is a respiratory illness. The most commonly reported symptoms are fever, cough, fatigue and difficulty with breathing (dysp-noea).10–12 A large study of 44,672 confirmed cases in China found that 80.9% had mild dis-
ease, with no pneumonia or mild pneumonia.13 The disease appeared to affect primarily adults, with children aged less than 19 years making up only 2–3% of reported cases.10,13 Children also appeared to present with less severe disease.13
The case fatality rate (CFR) for China has been calculated at 2.3%, based on 44,672 laboratory-confirmed cases up to 11 February 2020. The calculated CFR was much higher in Hubei Province (2.9%) than in all other provinces (0.4%). The CFR increased with increasing age group, with the highest CFR observed among those aged 80 years or older at 14.8%. No deaths were reported in children aged less than 10 years. The CFR was calculated at 0.9% in those reporting no comorbidities and 10.5% in cases with cardiovascular disease; however, data on comorbidities was missing for 53% of confirmed cases. Cases classified as critical (respiratory failure, septic shock, and/or multi-organ failure) had a CFR of 49.0%.13 Critically ill patients who died have been shown to be older and more likely to have chronic comorbidities.12 CFR estimates for regions outside mainland China are gener-ally low; however, the clinical outcome for the majority of these cases is not yet known.14
There are increasing reports of COVID-19 cases who did not display any symptoms at the time of testing.13,15-17 However, it is not always clear how many continued to be asymptomatic. Among a cohort of travellers repatriated to Germany on 1 February 2020, two travellers who were tested positive for SARS-CoV-2 showed no symptoms at the time of testing. On review one was found to have a faint rash and mild sore throat (pharyn-gitis). Both remained well and with no fever (afe-brile) for seven days following isolation.16 Fifty-one per cent (n = 318) of the confirmed cases on board the ‘Diamond Princess’ cruise ship as of 21 February 2020 showed no symptoms at time of specimen collection.17 Information about the development of symptoms in these cases after disembarkation was not available.

7 of 11 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.17) Epub 26/2/2020
Transmission
The exact nature of transmission of SARS-CoV-2 is not well understood. Human-to-human transmission is currently suspected to be via droplets, contact and fomites, which is con-sistent with other coronaviruses.18 There have been multiple reports of clusters within family and closed social groups, which would support this hypothesis.10,15,17 The WHO has recently released protocols for research into community, household and health facility transmission and surface contamination to help further define transmission patterns of SARS-CoV-2.2
There continues to be a large variation in the basic reproductive number (R0) calculated in various studies depending on the assumptions made and data set used. A recent review of 12 studies estimated the mean basic reproductive number (R0) to be 3.28 and median R0 to be 2.79, which exceeded the WHO preliminary R0 of 1.4–2.5 (average 1.95).19,20
A small study analysing viral load in nasal and throat swabs from 17 confirmed cases in Guangdong, China found higher viral loads detected soon after symptom onset, and in nasal compared to throat swabs.21 This is a shedding pattern similar to influenza illness rather than SARS-CoV. Whilst there is currently no pub-lished evidence of SARS-CoV-2 transmission from an asymptomatic case, there is some evi-dence of potential infectivity of asymptomatic cases based on viral load studies. For example, the viral load detected in an asymptomatic patient, from the Chinese cohort of 17 discussed above, was similar to that in the symptomatic patients.21 SARS-CoV-2 was also isolated from samples in cell culture from asymptomatic German nationals.16 The role played by asymp-tomatic cases in SARS-CoV-2 transmission is still unclear.
While diarrhoea has been reported as an uncom-mon symptom of COVID-19, a stool sample of a US case tested positive for SARS-CoV-2.10,22
Should confirmation of enteric infection and faecal excretion of SARS-CoV-2 be confirmed, it may have implications for transmission control.
Incubation period
WHO has revised the key epidemiologic parameters of COVID-19 in collaboration with an international network of statisticians and mathematical modellers. These parameters were calculated using data captured from COVID-19 surveillance activities and early investigations. Preliminary estimates of median incubation period, based on seven published studies, are 5 to 6 days (ranging from 0 to 14 days).14 Patients with long incubation periods do occasionally occur and have been reported, however medical experts have described these patients as ‘outli-ers’ who should be studied further and do not represent a significant shift in thinking about the virus.
Recommendations for control
The Australian Government Department of Health and WHO recommend the general pub-lic reduce their exposure to and transmission of COVID-19 by:
• Frequently cleaning hands with soap and water or by using alcohol-based hand rub.
• When coughing and sneezing cover mouth and nose with flexed elbow or tissue – throw tissue away immediately and wash hands.
• Avoid close contact with anyone who has fever and cough.
• If you have a fever, cough and difficulty breathing seek medical care early and share previous travel history with your health care provider.
Treatment
Current clinical management of COVID-19 cases focuses on early recognition, isolation, appropri-ate infection control measures and provision of

8 of 11 health.gov.au/cdiCommun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.17) Epub 26/2/2020
Table 3: Australian COVID-19 case definition as of 22 February 202026
Version Date of development Suspect Case Confirmed Case
1.9a 21 February 2020 If the patient satisfies epidemiological and clinical criteria, they are classified as a suspect case.
Epidemiological criteria• Travel to (including transit through) mainland
China in the 14 days before the onset of illness.OR• Close or casual contact in 14 days before illness
onset with a confirmed case of COVID-19. Clinical criteria• FeverOR• Acute respiratory infection (e.g. shortness of
breath or cough) with or without fever.
A person who tests positive to a validated specific SARS-CoV-2 nucleic acid test or has the virus identified by electron microscopy or viral culture.
a Version 1.9 update includes revised guidance on infectious period, contact management, and in special situation (cruise ship).
supportive care.23 Whilst there is no specific antiviral treatment currently recommended for patients with suspected or confirmed SARS-CoV-2 infection, multiple drugs are being inves-tigated. Experimental vaccines are also in devel-opment. University of Queensland researchers recently reported making significant advances towards a vaccine against SARS-CoV-2.24
Virology
SARS-CoV-2, the virus that causes COVID-19, is 96% identical to the whole genome sequence of a known bat coronavirus (BATCoV RaTG13) and 79.5% identical to SARS-CoV-1. Like SARS-CoV-1, it attaches its spike (S) protein to the angiotensin-converting enzyme 2 (ACE-2) to enter and infect host cells located in the lower respiratory tract, with progressive respiratory failure due to alveolar damage.25
Methods
Data for this report were current as at 19:00 hours AEDT, 22 February 2020.
This report outlines what is known epidemio-logically on COVID-19 in Australia and from publicly available data from WHO Situation Reports, other countries’ official updates and the scientific literature. Data on domestic cases
in this report were collected from the National Notifiable Diseases Surveillance System (NNDSS) and state and territory case investi-gation reports. The Communicable Diseases Network Australia (CDNA) developed the case definition for suspected and confirmed cases, which was modified at different time points in the epidemic (Table 3). CDNA developed national guidance on investigating suspected and confirmed cases of COVID-19. Based on this guidance, state and territory health department investigators conducted interviews of suspected cases to collect core and enhanced data for inclu-sion in the NNDSS. Data was analysed using Stata to describe the epidemiology of infections in Australia and the progress of the epidemic.
Data for the international cases of COVID-19 by country were compiled from the latest WHO Situation Report. Case definitions may vary by country making comparisons difficult. Rapid reviews of the current state of knowledge on COVID-19 were conducted from the literature using PubMed.
Acknowledgements
This report represents surveillance data reported through CDNA as part of the nationally-coordi-nated response to COVID-19. We thank public health staff from incident emergency operations

9 of 11 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.17) Epub 26/2/2020
centres in state and territory health departments, and the Australian Government Department of Health; along with state and territory public health laboratories.
Author details
Corresponding author
Tracy Tsang
NIR Surveillance Team, Communicable Disease Epidemiology and Surveillance Section, Health Protection Policy Branch, Australian Government Department of Health, GPO Box 9484, MDP 14, Canberra, ACT 2601. Email: [email protected]
References
1. National Health Commission of the Peo-ple’s Republic of China. Interpretation of new coronavirus pneumonia diagnosis and treatment plan (trial version 6). [Internet.] Beijing: National Health Commission of the People’s Republic of China; 2020. [Accessed on 22 February 2020.] Available from: http://www.nhc.gov.cn/yzygj/s7652m/202002/54e1ad5c2aac45c19eb541799bf637e9.shtml.
2. World Health Organization(WHO). Coro-navirus disease 2019 (COVID-19) situa-tion report – 33: 22 February 2020. Geneva: WHO; 2020. [Accessed on 23 February 2020.]. Available from: https://www.who.int/docs/default-source/coronaviruse/situa-tion-reports/20200222-sitrep-33-covid-19.pdf?sfvrsn=c9585c8f_2.
3. COVID-19 National Incident Room Surveil-lance Team. 2019-nCoV acute respiratory disease, Australia: Epidemiology Report 3. Reporting week ending 19:00 AEDT 15 February 2020. Commun Dis Intell (2018). 2020;44. doi: https://doi.org/10.33321/cdi.2020.44.15.
4. Centers for Disease Control and Preven-tion. Coronavirus infection-19 domestic
outbreak (February 22, regular briefing). [Internet.] Osong, South Korea: Centers for Disease Control & Prevention; 2020. [Accessed on 23 February 2020.]. Avail-able from: https://www.cdc.go.kr/board/board.es?mid=a20501000000&bid=0015&list_no=366298&act=view.
5. Ministry of Health Labor and Welfare. About coronavirus disease 2019 (COVID-19). [Internet.] Tokyo: Ministry of Health, Labor and Welfare; 2020. [Accessed on 23 Febru-ary 2020.] Available from: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/new-page_00032.html.
6. WHO. Statement on the second meeting of the International Health Regulations (2005) Emergency Committee regarding the outbreak of novel coronavirus (2019-nCoV). [Internet.] Geneva: WHO; 2020. [Accessed on 31 January 2020.] Available from: https://www.who.int/news-room/detail/30-01-2020-statement-on-the-sec-ond-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavi-rus-(2019-ncov).
7. The New York Times. China tightens Wuhan lockdown in ‘wartime’ battle with coronavi-rus. [Internet.] New York: New York Times; 6 February 2020. [Accessed on 7 February 2020.] Available from: https://www.nytimes.com/2020/02/06/world/asia/coronavirus-china-wuhan-quarantine.html.
8. Australian Government Department of Health. Australian Health Protection Princi-pal Committee (AHPPC) novel coronavirus statement on 1 February 2020. [Internet.] Canberra: Australian Government Depart-ment of Health; 2020. [Accessed on 7 Feb-ruary 2020.] Available from: https://www.health.gov.au/news/australian-health-protec-tion-principal-committee-ahppc-novel-coro-navirus-statement-on-1-february-2020.
9. Australian Government Department of

10 of 11 health.gov.au/cdiCommun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.17) Epub 26/2/2020
Health. Australian Health Protection Prin-cipal Committee (AHPPC) recommenda-tion on travel restrictions and coronavirus (COVID-19). [Internet.] Canberra: Austral-ian Government Department of Health; 2020. [Accessed on 22 February 2020.] Avail-able from: https://www.health.gov.au/news/australian-health-protection-principal-com-mittee-ahppc-recommendation-on-travel-restrictions-and-coronavirus-covid-19.
10. Xu XW, Wu XX, Jiang XG, Xu KJ, Ying LJ, Ma CL et al. Clinical findings in a group of patients infected with the 2019 novel corona-virus (SARS-CoV-2) outside of Wuhan, Chi-na: retrospective case series. BMJ. 2020;368. doi: https://doi.org/10.1136/bmj.m606.
11. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506.
12. Yang X, Yu Y, Xu J, Shu H, Xia J, Liu H et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospec-tive, observational study. Lancet Respir Med. 2020. doi: https://doi.org/10.1016/S2213-2600(20)30079-5.
13. The Novel Coronavirus Pneumonia Emer-gency Response Epidemiology Team. The epidemiological characteristics of an out-break of 2019 novel coronavirus diseases (COVID-19) – China, 2020. China CDC Weekly. 2020;2(8):113–22.
14. WHO. Coronavirus disease 2019 (COV-ID-19) situation report – 29: 18 February 2020. Geneva: WHO; 2020. [Accessed on 22 February 2020.] Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200218-sitrep-29-cov-id-19.pdf?sfvrsn=6262de9e_2.
15. Pan X, Chen D, Xia Y, Wu X, Li T, Ou X et al. Asymptomatic cases in a family cluster with SARS-CoV-2 infection. Lancet Infect
Dis. 2020. doi: https://doi.org/10.1016/S1473-3099(20)30114-6.
16. Hoehl S, Berger A, Kortenbusch M, Cinatl J, Bojkova D, Rabenau H et al. Evidence of SARS-CoV-2 infection in returning travelers from Wuhan, China. N Eng J Med. 2020. doi: https://doi.org/10.1056/NEJMc2001899.
17. National Institute of Infectious Diseases. Field briefing: Diamond Princess COVID-19 cases, 20 Feb update. [Internet.] Tokyo: Na-tional Institute of Infectious Diseases; 2020. [Accessed on 23 February 2020.] Available from: https://www.niid.go.jp/niid/en/2019-ncov-e/9417-covid-dp-fe-02.html.
18. WHO. Novel coronavirus (2019-nCoV) situation report – 7: 27 January 2020. Ge-neva: WHO; 2020. [Accessed on 28 January 2020.] Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200127-sitrep-7-2019--ncov.pdf?sfvrsn=98ef79f5_2.
19. Liu Y, Gayle AA, Wilder-Smith A, Rocklöv J. The reproductive number of COVID-19 is higher compared to SARS coronavirus.J Travel Med. 2020. doi: https://doi.org/10.1093/jtm/taaa021.
20. WHO. Statement on the meeting of the International Health Regulations (2005) Emergency Committee regarding the out-break of novel coronavirus (2019-nCoV). [Internet.] Geneva: WHO; 2020. [Ac-cessed on 24 January 2020.] Available from: https://www.who.int/news-room/detail/23-01-2020-statement-on-the-meet-ing-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavirus-(2019-ncov).
21. Zou L, Ruan F, Huang M, Liang L, Huang H, Hong Z et al. SARS-CoV-2 viral load in upper respiratory specimens of infected patients. N Eng J Med. 2020. doi: https://doi.org/10.1056/NEJMc2001737.

11 of 11 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.17) Epub 26/2/2020
22. Holshue ML, DeBolt C, Lindquist S, Lofy KH, Wiesman J, Bruce H, et al. First case of 2019 novel coronavirus in the United States. N Engl J Med. 2020. https://doi.org/10.1056/NEJMoa2001191.
23. WHO. Clinical management of severe acute respiratory infection when novel coronavirus (nCoV) infection is suspected. [Internet.] Geneva: WHO; 2020. [Accessed on 23 Febru-ary 2020.] Available from: https://www.who.int/publications-detail/clinical-management-of-severe-acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-sus-pected.
24. University of Queensland. ‘Significant step’ in COVID-19 vaccine quest. [Internet.] Brisbane: University of Queensland Aus-tralia; 2020. [Accessed on 23 February 2020.] Available from: https://www.uq.edu.au/news/article/2020/02/significant-step%E2%80%99-covid-19-vaccine-quest.
25. Zhou P, Yang X-L, Wang X-G, Hu B, Zhang L Zhang W, et al. A pneumonia outbreak associated with a new coronavirus of prob-able bat origin. Nature. 2020. doi: https://doi.org/10.1038/s41586-020-2012-7.
26. Australian Government Department of Health. Coronavirus disease 2019 (COV-ID-19) - CDNA national guidelines for pub-lic health units. [Internet.] Canberra: Aus-tralian Government Department of Health; 2020. [Accessed on 22 February 2020.] Available from: https://www1.health.gov.au/internet/main/publishing.nsf/Content/cdna-song-novel-coronavirus.htm.

2 0 2 0 V o l u m e 4 4https://doi.org/10.33321/cdi.2020.44.20
COVID-19, Australia: Epidemiology Report 5:Reporting week ending 19:00 AEDT 29 February 2020
COVID-19 National Incident Room Surveillance Team

Communicable Diseases Intelligence ISSN: 2209-6051 Online
This journal is indexed by Index Medicus and Medline.
Creative Commons Licence - Attribution-NonCommercial-NoDerivatives CC BY-NC-ND
© 2020 Commonwealth of Australia as represented by the Department of Health
This publication is licensed under a Creative Commons Attribution- Non-Commercial NoDerivatives 4.0 International Licence from https://creativecommons.org/licenses/by-nc-nd/4.0/legalcode (Licence). You must read and understand the Licence before using any material from this publication.
Restrictions The Licence does not cover, and there is no permission given for, use of any of the following material found in this publication (if any):
• the Commonwealth Coat of Arms (by way of information, theterms under which the Coat of Arms may be used can be found atwww.itsanhonour.gov.au);
• any logos (including the Department of Health’s logo) andtrademarks;
• any photographs and images;
• any signatures; and
• any material belonging to third parties.
Disclaimer Opinions expressed in Communicable Diseases Intelligence are those of the authors and not necessarily those of the Australian Government Department of Health or the Communicable Diseases Network Australia. Data may be subject to revision.
Enquiries Enquiries regarding any other use of this publication should be addressed to the Communication Branch, Department of Health, GPO Box 9848, Canberra ACT 2601, or via e-mail to: [email protected]
Communicable Diseases Network Australia Communicable Diseases Intelligence contributes to the work of the Communicable Diseases Network Australia. http://www.health.gov.au/cdna
Communicable Diseases Intelligence (CDI) is a peer-reviewed scientific journal published by the Office of Health Protection, Department of Health. The journal aims to disseminate information on the epidemiology, surveillance, prevention and control of communicable diseases of relevance to Australia.
Editor Cindy Toms
Deputy Editor Simon Petrie
Design and Production Kasra Yousefi
Editorial Advisory Board David Durrheim, Mark Ferson, John Kaldor, Martyn Kirk and Linda Selvey
Website http://www.health.gov.au/cdi
Contacts Communicable Diseases Intelligence is produced by: Health Protection Policy Branch Office of Health Protection Australian Government Department of Health GPO Box 9848, (MDP 6) CANBERRA ACT 2601
Email: [email protected]
Submit an Article You are invited to submit your next communicable disease related article to the Communicable Diseases Intelligence (CDI) for consideration. More information regarding CDI can be found at: http://health.gov.au/cdi.
Further enquiries should be directed to: [email protected].

1 of 14 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.20) Epub 4/3/2020
Weekly epidemiological report
COVID-19, Australia: Epidemiology Report 5:Reporting week ending 19:00 AEDT 29 February 2020
COVID-19 National Incident Room Surveillance Team
Summary
This is the fifth epidemiological report for coronavirus disease 2019 (COVID-19), reported in Australia as at 19:00 Australian Eastern Daylight Time [AEDT] 29 February 2020. It includes data on COVID-19 cases diagnosed in Australia, the international situation and a review of current evidence.
Keywords: SARS-CoV-2; novel coronavirus; 2019-nCoV; coronavirus disease 2019; COVID-19; acute respiratory disease; case definition; epidemiology; Australia
The following epidemiological data are subject to change both domestically and internationally due to the rapidly evolving situation. Australian cases are still under active investigation. While every effort has been made to standardise the investigation of cases nationally, there may be some differences between jurisdictions.
In Australia:
• 25 COVID-19 cases were notified up until 19:00 AEDT 29 February 2020;
• The first 15 cases are all considered to have had a direct or indirect link to Wuhan, HubeiProvince, China;
• Nine cases were among the ‘Diamond Princess’ cruise ship passengers repatriated from Japanto the Northern Territory on 20 February 2020;
• The most recent case in Queensland had travelled from Iran;
• There were zero deaths at time of reporting;
• On 27 February 2020, the Australian Health Protection Principal Committee (AHPPC)recommended that the current travel restrictions for mainland China remain in place for afurther seven days; and
• On 29 February 2020, travel restrictions were announced for travellers from Iran.

2 of 14 health.gov.au/cdiCommun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.20) Epub 4/3/2020
Internationally:
• 85,403 infections have been confirmed globally, with 2,924 deaths;
• The majority of confirmed infections (93%; n = 79,251) and deaths (97%; n = 2,835) havebeen reported in mainland China;
• On 26 February 2020, the number of cases reported in a 24 hour period from outside main-land China exceeded the number of cases from mainland China for the first time;
• All passengers from the ‘Diamond Princess’ cruise ship have now disembarked and remain-ing staff will complete 14 days quarantine in Japan;
• Eighty-nine deaths were reported outside mainland China – 34 in Iran (Islamic Republic of),21 in Italy, 17 in Republic of Korea, six associated with the ‘Diamond Princess’, five in Japan,two each in Hong Kong and France and one each in the Philippines and Taiwan; and
• Republic of Korea, Italy and Iran are now reporting high levels of transmission.
Domestic cases
There were 25 confirmed cases reported in Australia as at 19:00 AEDT 29 February 2020 (Table 1). Nine (36.0%) of the 25 confirmed cases were among the ‘Diamond Princess’ cruise ship passengers repatriated from Japan (n=164) to the Northern Territory on 20 February 2020. The remaining cases were reported in New South Wales (n = 4), Victoria (n = 4), Queensland (n = 6) and South Australia (n = 2). The first 15 casesall had direct or indirect links to Wuhan. Themost recent case in Queensland had returnedfrom Iran and was the first Australian case notlinked to the outbreaks in Wuhan or on the‘Diamond Princess’.1
The first case in Australia reported onset of symptoms on 13 January 2020 (Figure 1). The median age of all 25 reported Australian cases was 53 years (range 8–79 years) with a male-to-female ratio of 1:1.3. The following analysis involves 23 out of 25 cases who had detailed data available at the time of reporting. Sixteen cases (69.6%) reported fever, 12 cases (52.2%) reported cough, and nine (39.1%) had a sore throat. Two cases (8.7%) were reported to have pneumonia and five (21.7%) reported diarrhoea. Four cases
had no symptoms recorded. Seven cases were reported as having no comorbidities and one case was reported as having diabetes. The first 15 cases have been reported to have recovered, and no deaths were recorded at time of reporting.
Twenty cases had recorded onset of symptoms prior to laboratory testing. The median time between onset of symptoms and testing in these cases was 2 days (range 0–10 days). From these cases, those associated with the ‘Diamond Princess’ (n = 6) had a median time between onset of symptoms and testing of 2 days (range 0–5 days), whilst the remaining cases (n=14) had a median time of 2.5 days (range 0–10 days) between onset of symptoms and testing. The slightly shorter time from symptom onset to testing in the ‘Diamond Princess’ cohort may be because they were under active surveillance for COVID-19. Two cases were tested prior to recorded onset of symptoms and one case did not have a date of symptom onset or any symp-toms recorded.
No cases have been detected among Australians who have returned from mainland China since 1 February 2020 or among students from mainland China.2 Evidence of limited second-

3 of 14 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.20) Epub 4/3/2020
Table 1: Cumulative notified cases of confirmed COVID-19 by jurisdiction, Australia, 2020 (n = 25)
JurisdictionThis week
(to 19:00 AEDT 29 Feb) No. of cases
Last week (to 19:00 AEDT 22 Feb)
No. of cases
Total cases (to 19:00 AEDT 29
Feb 2020) No. of cases
NSW 0 0 4
Vic 0 0 4
Qld 1 0 6
WA 0 0 0
SA 0 0 2
Tas 0 0 0
NT 0 0 0
ACT 0 0 0
Repatriation (Diamond Princess) 2 7 9
Total cases 3 7 25
ary transmission of COVID-19 in Australia is thought to have occurred for three cases who were part of a five-person cluster identified in Queensland. There is currently no evidence of community transmission within Australia.
International cases
As at 19:00 AEDT 29 February 2020, the num-ber of confirmed COVID-19 cases reported to the World Health Organization (WHO) was 85,403 globally (Table 2). Whilst mainland China reported 92.8% of cases (n = 79,251), this is a decrease from 98.1% on 22 February 2020 as the proportion of new cases reported from outside of mainland China increased over the last week. On 26 February 2020, the number of new cases outside of mainland China exceeded the number reported from mainland China for the first time and this trend has continued to date (Figure 2). Fifty-six countries and Special Administrative Regions outside of mainland China have reported a total of 5,447 confirmed COVID-19 cases. There were an additional 705 confirmed cases on the cruise ship ‘Diamond Princess’. Republic of Korea reported 51.2% of all cases outside of mainland China (n = 3,150), Italy reported 14.4% (n = 888), Iran (Islamic Republic of) 6.3% (n = 388) and Japan 3.7% (n = 230).3
Twenty-five new countries or Member States (Afghanistan, Algeria, Austria, Bahrain, Belarus, Brazil, Croatia, Denmark, Estonia, Georgia, Greece, Iraq, Kuwait, Lithuania, Mexico, Netherlands, New Zealand, Nigeria, Norway, North Macedonia, Oman, Pakistan, Romania, San Marino, Switzerland) reported cases of COVID-19 in the past seven days. Eastern Mediterranean and European regions had the greatest growth in number of new coun-tries reporting cases. The first African and South American countries reported cases over the last seven days. Two new countries (Croatia and San Marino) have reported possible or confirmed limited local transmission since the last report on 22 February 2020. Reports suggest sustained local transmission is evident in Republic of Korea, Italy and Iran. Vietnam, Philippines, Cambodia, Russia, Belgium, India, Nepal, Sri Lanka, and Egypt have not reported any new cases for at least 14 days.3
Globally, 2,924 deaths have been reported, with 93.3% (n = 2,727) reported from Hubei Province, China. Eighty-nine deaths were reported out-side mainland China: 34 in Iran, 21 in Italy, 17 in Republic of Korea, six from the ‘Diamond Princess’, five in Japan, two each in Hong Kong and France and one each in the Philippines and Taiwan.3

4 of 14 health.gov.au/cdiCommun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.20) Epub 4/3/2020
Tabl
e 2:
Cum
ulat
ive
confi
rmed
cas
es o
f CO
VID
-19
glob
ally
, 201
9–20
20
a )910c
2e
m D
o 35
)7r 28 17 21 6 34 5 0 2 0 2 0 0 0 1 0 0 0 0 0 0 0 0f ,7
s ( ,2 2
htael datoT
a )910c
2e
m D
51 37 0 5 82 3,, 15 30 bo 2r , 888
70 38 98 94 62 57 57 45 4 39 38 32 24 24 20 19 16 14f 9 6 2
s ( 37 6
esal catoT
0 0:9o
1 )0t 2k
( 0e b 2
g w
e 6 8e 9 8 6
2 F 4 8
31 6 1 64 19 12 20 1 0 0 1 8 0 0 6 1 0 3 0 17 0 1, 49,n 9itr T 2
o Dp Ee At rsaL
)02 0kee b 2
wT
29 F
eng 3 4i 0 0 5t 83 96 8 87 71 12 26 27 45 1,9 8 4, 37 12 45 7 13 38 30 11or
3 2 8 0 6
D 2 2 2,p E res 0
Ai 0h :9T
o 1
t(
pih se ) an f
io s c
l) i o i
g a ru
rc e seel ot
i
c l ma ai ub
t
R at s ( s r
c e e e pa f A
iv e
hin r m
nc
c ee mi
o np t i R s o o E
f K gd
y / S
a vi r ec ab
ist r c o tr C o P e a nd d r t
r P oli n lam
i
ong
ny
idn ia ai K Ar
i at a e bn min l d
S
b u ain
u y mo ap
ss K n le a tI c m lan
a e ( an
i a d d
ay d
ain e a r e
an
g t n ip r w ain t t tu w hr
Jap li i tn
ameo d l a in n a aH e a e i n n
C A M Di ii on
g
u ha a p us ana
( R It rI S H U Fr G K T Ta B S A M U U V C

5 of 14 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.20) Epub 4/3/2020
a )910c
2e
m D
or 0 0 0 0 0 0 0 0 0 0 0 1 0 0 0 0 0 0 0 0 0 0 0 0fs
(htae
l datoTa )910
c 2
em
Do 12 10 10 8 6 6 5 5 5 3 3 3 3 2 2 2 2 2 2 2 2 1 1 1rf
s (
esal catoT
0 0:9o
1 )0t 2k
( 0e b 2
g w
e e2
F 0 0 0 0 0 0 0 0 1 0 0 0 0 0 0 0 1 0 0 0 0 0 0 0
nitr T 2
o Dp Ee At rsaL
)02 0kee b 2
w ein
gt T
29 F
11or
0 10 8 6 6 5 5 4 3 0 0 3 2 1 2 1 2 2 2 0 1 1 1
Dp E
res 0 A
i 0h :9To
1t(
niogel na R oic e it
iv ae rp t e
y / S
a dla
n s ds dris
t e e annrkr in
min
n r ia a d non ta F s
ay nia a io lre an nia at e pn au
e suz w an l er t ip ad mc t rgi c ti iat a e a hu se i ia sxq r ee
c
mo us
i
d mw r hil nlan oa ta a o e lar
o en
Sw ro d e ei eb ak us ghan
M sr n M
f geri
l eC A S rI N O A C I G I P R D F G L N P R A A B
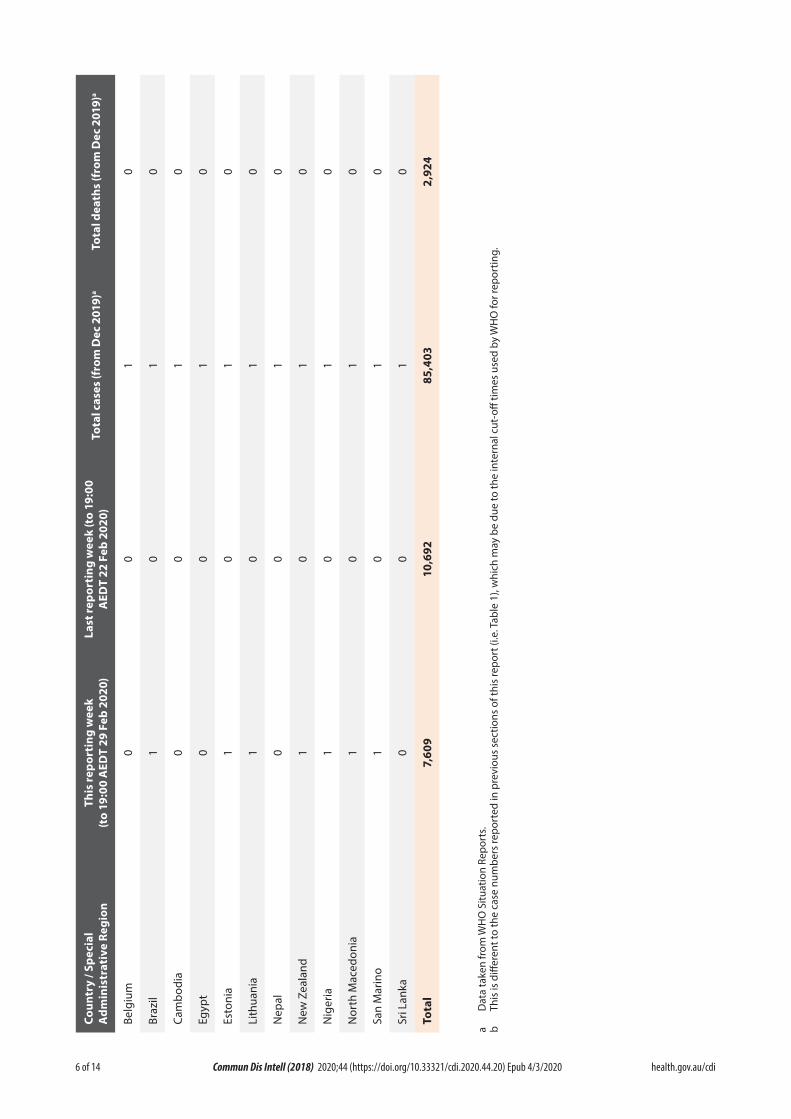
6 of 14 health.gov.au/cdiCommun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.20) Epub 4/3/2020
a )910c
2e
m D
o 24r 0 0 0 0 0 0 0 0 0 0 0 0f ,9
s ( 2
htael datoT
a )910c
2e
m D 30o 1 1 1 1 1 1 1 1 1 1 1 1 4rf
s ( 85
,
esal catoT
0 0:9o
1 )0t 2k
( 0e b 2
g w
e 2
e 9
2 F 0 0 0 0 0 0 0 0 0 0 0 0 6,
ni 10tr T 2
o Dp Ee At rsaL
)02 0kee b 2
wT
29 F
eng 9it 0
or
0 1 0 0 1 1 0 1 1 1 1 0 6D 7,p E res 0
Ai 0h :9T
o 1
t(n
iogel ai Rc e ni
a
e iv op t d d
y / S
ar oa
alan ec
ist
di a n
um
i artm
in o nia
nia e a M ar
n l b t a l ha Zzi
am
p u ank
l
o t M au gil y h p w r Ld ao te geri
sC A i anB Br C Eg
t
E L Ne te ii o
N N N rS S To
a D
ata
take
n fr
om W
HO
Situ
atio
n Re
port
s.b
This
is d
iffer
ent t
o th
e ca
se n
umbe
rs re
port
ed in
pre
viou
s se
ctio
ns o
f thi
s re
port
(i.e
. Tab
le 1
), w
hich
may
be
due
to th
e in
tern
al c
ut-o
ff tim
es u
sed
by W
HO
for r
epor
ting.

7 of 14 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.20) Epub 4/3/2020
Figure 1: Confirmed cases of COVID-19 infection by date of illness onset, Australia 2020 (n = 22)a
0
1
2
3
4
5
10/0
1/20
20
12/0
1/20
20
14/0
1/20
20
16/0
1/20
20
18/0
1/20
20
20/0
1/20
20
22/0
1/20
20
24/0
1/20
20
26/0
1/20
20
28/0
1/20
20
30/0
1/20
20
1/02
/202
0
3/02
/202
0
5/02
/202
0
7/02
/202
0
9/02
/202
0
11/0
2/20
20
13/0
2/20
20
15/0
2/20
20
17/0
2/20
20
19/0
2/20
20
21/0
2/20
20
23/0
2/20
20
25/0
2/20
20
27/0
2/20
20
29/0
2/20
20
Num
ber o
f con
firm
ed C
OVI
D-19
case
s
Date of illness onset
NSW VIC QLD SA Limited local transmission Diamond Princess
a Date of symptom onset not available for three cases.
Background
On 31 December 2019, the World Health Organization (WHO) were notified about a large number of cases of pneumonia of unknown origin in Wuhan City, Hubei Province, China. Chinese authorities isolated and identified a novel coronavirus on 7 January 2020.4 WHO declared the outbreak of COVID-19 a Public Health Emergency of International Concern (PHEIC) on 30 January 2020.5 From 1 February 2020, Australia denied entry to anyone who had left or transited through mainland China, with the exception of Australian citizens, permanent residents and their immediate family and air crew who have been using appropriate personal protective equipment.6 The Australian Health Protection Principal Committee (AHPPC) have reviewed these restrictions weekly, and on 27 February 2020, they released a state-ment recommending current travel restric-tions remain in place for a further seven days.2
AHPPC acknowledged that while there has been
a decrease in number of cases being reported in mainland China (outside of Hubei Province), there is an increasing risk of sustained trans-mission being established in several other countries.2 On the same day, the Australian Prime Minister announced the activation of the Australian Health Sector Emergency Response Plan for Novel Coronavirus (COVID-19).7 On the 29 February 2020, the Minister for Health announced travel restrictions for travellers coming from Iran. From 1 March 2020 those who are neither Australian citizens nor perma-nent residents will be prevented from coming to Australia until 14 days after leaving Iran. Australian citizens, permanent residents and their immediate family will be required to self-isolate on return from Iran.8
The current estimates on epidemiological param-eters including severity, transmissibility and incubation period are uncertain. Estimates are likely to change as more information becomes available.

8 of 14 health.gov.au/cdiCommun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.20) Epub 4/3/2020
Country in focus: Republic of Korea
Republic of Korea notified their first confirmed case of COVID-19 on 20 January 2020. Of the first 30 cases, 10 had direct links to Wuhan and 13 were close or family contacts of confirmed cases. On 19 February 2020, 20 new cases were notified. Fifteen of these had an epidemiologi-cal link through the Shincheonji Church of Jesus to a case identified the day prior. From then, reported cases in Republic of Korea rose rapidly with an increase of nearly twentyfive-fold over the next week to 26 February 2020 (n = 1,261).9
Cases have been concentrated in Daegu city, primarily linked to the Shincheonji Church of Jesus. As of 29 February 2020, 66.0% of cases in Daegu city were directly associated with the Shincheonji Church of Jesus and 53.1% of all confirmed cases in Republic of Korea were associ-ated with this church.10 The Shincheonji Church of Jesus is reported to have over 1,000 churches across the Republic of Korea. Church services are reported to involve close physical proximity to others and frequent loud calling out, which may contribute to the rapid spread of COVID-19 amongst members. There are media reports that the church is secretive and members may be unlikely to disclose their membership to contacts, making contact tracing difficult.11
There have been clusters associated with the Cheongdo Daenam Hospital, an Israel pilgrimage, the Busan Onchun church, and community centres and shelters in Gyeong-buk Province. Only 1.1% of cases reported up until 29 February 2020 in Republic of Korea have been attributed to imported disease.10
The first death in Republic of Korea was reported on 20 February 2020.12 As of 29 February 2020, 17 deaths had been reported.13 Epidemiological analysis of the first 16 reported fatal cases conducted by Korean Centers for Disease Control and Prevention (KCDC) found 14 (87.5%) were aged over 50 years (range 35–93 years). The ratio of males to females was 1:0.6. All cases were reported as having comorbid conditions, such as hypertension, chronic liver or kidney disease and cancer. The seven cases associated with Cheongdo Daenam hospital cluster were all long term admissions in the mental health ward which the KCDC felt might have contributed to poor health and susceptibility to severe COVID-19.10
Republic of Korea has tested over 85,000 people for SARS-CoV-2. This extensive testing effort has likely contributed to the identification of large numbers of COVID-19 cases. On 24 February 2020, the Republic of Korea government raised the alert level to the highest level in prepara-tion for possible nationwide transmission.14 The KCDC has made recommendations to avoid large gatherings, particularly for those aged over 65 years. Potential contacts are encouraged to self-isolate with testing once they become symptomatic. Now with large numbers of cases and sustained community transmission, the KCDC has advised that medical resources need to focus on those with comorbid conditions and the elderly to minimise fatalities. Local governments have now taken over epidemiological investigations and quarantine measures from the KCDC.10

9 of 14 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.20) Epub 4/3/2020
Figure 2. Cases of COVID-19 reported to WHO and number of countries and SARs reporting outside mainland China from 21 January to 29 February 202015
0
10
20
30
40
50
60
0
500
1000
1500
2000
2500
3000
3500
4000
4500
21-Ja
n22
-Jan
23-Ja
n24
-Jan
25-Ja
n26
-Jan
27-Ja
n28
-Jan
29-Ja
n30
-Jan
31-Ja
n1-
Feb
2-Fe
b3-
Feb
4-Fe
b5-
Feb
6-Fe
b7-
Feb
8-Fe
b9-
Feb
10-F
eb11
-Feb
12-F
eb13
-Feb
14-F
eb15
-Feb
16-F
eb17
-Feb
18-F
eb19
-Feb
20-F
eb21
-Feb
22-F
eb23
-Feb
24-F
eb25
-Feb
26-F
eb27
-Feb
28-F
eb29
-Feb
Num
ber o
f cou
ntrie
s and
SAR
s out
side
of m
ainl
and
Chin
a
Num
ber o
f rep
orte
d ca
ses
Date of repor ng
Mainland China Outside of mainland China Number of countries and SARs outside of mainland China repor ng casesti
ti
a WHO declares the outbreak of COVID-19 a Public Health Emergency of International Concern
b WHO start reporting both laboratory confirmed and clinically diagnosed cases from Hubei Province
c Hubei Province cease reporting clinically diagnosed cases
Severity
Ongoing evidence from China supports previous research that COVID-19 presents as mild illness in the majority of cases with fever and cough the most commonly reported symptoms. Severe or fatal outcomes tend to occur in the elderly or those with comorbid conditions.16 Reports from cases in Republic of Korea suggest that their experience is similar.9 Examination of cases in China found the median time from onset to resolution of symptoms was two weeks for those with mild disease and three to six weeks for severe or critical disease. Severe disease tended to develop one week after onset of symptoms and in fatal cases, time from onset of symptoms to death was two to eight weeks.16
Calculated case fatality rates (CFR) have varied depending on location across China and in
countries outside China. Ji et al found a sig-nificant correlation between mortality rate and population case load in China. They discussed that the high and rapid escalation of disease may have quickly overwhelmed health services and been a contributing factor to Hubei’s high case fatality rate (CFR).17 In the wealthy and developed province of Zhejiang, the zero fatality rate despite the large number of cases might be due to well-resourced and accessible healthcare facilities.17 These findings suggest that delay-ing the onset of the outbreak and slowing the escalation of cases may allow health authorities in countries not yet reporting sustained com-munity transmission to better prepare for and adapt to manage increasing numbers of cases. However, resource–limited regions might be overwhelmed earlier and at a lower number of cases.

10 of 14 health.gov.au/cdiCommun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.20) Epub 4/3/2020
A small case series from China has described four cases who tested positive for SARS-CoV-2 five to 13 days after meeting the criteria for hospital discharge. The criteria for hospital discharge included: normal temperature for at least 3 days; resolved respiratory symptoms; substantially improved acute exudative lesions on chest computed tomography (CT scan); and reverse transcription polymerase chain reaction (RT-PCR) negative on at least two consecutive specimens separated by at least one day. Three repeat RT-PCR tests were performed in the next four to five days for each patient, all of whom remained asymptomatic, and all returned positive.18 The Australian Series of National Guidelines for COVID-19 acknowledges that a small proportion of people may have an illness that has completely resolved but their respira-tory specimens remain persistently PCR posi-tive. The guideline recommends that a decision to release these patients from isolation should be made on a case-by-case basis and that a follow up should take place seven days after release from isolation for clinical review to ensure full symptom resolution.19
Transmission
Human-to-human transmission of SARS-CoV-2 is via droplets and fomites from an infected person to a close contact.16 Reports from China, Republic of Korea and Australia of clusters within family and close social groups support this.16,20 Current evidence does not support air-borne or faecal-oral spread as major factors in transmission.16
Incubation period
No new research has been published on the incubation period for COVID-19. Please refer to COVID-19, Australia: Epidemiology Report 4.21
Recommendations for control
The Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19) made
the following major recommendations for coun-tries with imported cases and/or outbreaks of COVID-19:16
1. Immediately activate the highest level ofnational Response Management protocols toensure the all-of-government and all-of-so-ciety approach needed to contain COVID-19with non-pharmaceutical public healthmeasures;
2. Prioritise active, exhaustive case finding andimmediate testing and isolation, painstakingcontact tracing and rigorous quarantine ofclose contacts;
3. Fully educate the general public on theseriousness of COVID-19 and their role inpreventing its spread;
4. Immediately expand surveillance to detectCOVID-19 transmission chains, by test-ing all patients with atypical pneumonias,conducting screening in some patients withupper respiratory illnesses and/or recentCOVID-19 exposure, and adding testing forthe COVID-19 virus to existing surveillancesystems (e.g. systems for influenza-like-illness); and
5. Conduct multi-sector scenario planning andsimulations for the deployment of even morestringent measures to interrupt transmis-sion chains as needed (e.g. the suspensionof large-scale gatherings and the closure ofschools and workplaces).
Treatment
Current clinical management of COVID-19 cases focuses on early recognition, isolation, appropriate infection control measures and provision of supportive care.22 Whilst there is no specific antiviral treatment currently recom-mended for patients with suspected or confirmed SARS-CoV-2 infection, there are multiple clini-cal trials underway in China and the US have

11 of 14 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.20) Epub 4/3/2020
Table 3: Australian COVID-19 case definition as of 29 February 202019
Date of Version Suspect Case Confirmed Casedevelopment
1.13 28 February 2020 If the patient satisfies epidemiological A person who tests positive to a and clinical criteria, they are classified as validated specific SARS-CoV-2 nucleic a suspect case. acid test or has the virus identified by Epidemiological criteria electron microscopy or viral culture.• Travel to (including transit through)
mainland China in the 14 days before the onset of illness.
OR• Close or casual contact in 14 days
before illness onset with a confirmed case of COVID-19.
Clinical criteria• FeverOR• Acute respiratory infection (e.g.
shortness of breath or cough) with or without fever.
begun a clinical trial evaluating Remdesivir, an antiviral developed for the treatment of Ebola virus disease.23
Testing
The North West London National Health Service (NHS) Trust has implemented a pilot program of home testing of potential cases. Those identi-fied as potential cases by general practitioners, emergency departments or via the NHS hotline are referred to the program. Cases are triaged over the phone before a trained healthcare pro-fessional in personal protective equipment goes to the person’s house to collect the specimen and provide education on self-isolation, advice on what to do if they deteriorate and an emergency contact number. The potential case is then con-tacted with the results and if the result is posi-tive they are admitted to hospital.24 The aim of the program is to reduce the risk of ambulance services and emergency waiting rooms being overwhelmed with potential cases and reduce the risk of disease transmission to potentially vulnerable populations within healthcare set-tings whilst still allowing for early identification and isolation of cases.
Virology
Several countries have isolated and sequenced the genome for SARS-CoV-2 from cases with COVID-19. Analysis of the genetic diversity of these samples found few mutations, suggest-ing that following initial animal-to-human transmission from a single source, spread has resulted from human-to-human transmission over a limited period of time. Based on model-ling, researchers estimate that initial human infection was in November to early December 2019. Groups of sequences with the same muta-tions are being identified, confirming human-to-human transmission and linking cases across countries.25 Ongoing surveillance of sequences and shared mutations will assist with under-standing of the global spread of the virus.
Methods
Data for this report were current as at 19:00 hours AEDT, 29 February 2020.
This report outlines what is known epidemio-logically on COVID-19 in Australia and from publicly available data from WHO Situation Reports, other countries’ official updates and the scientific literature. Data on domestic cases in this report were collected from the National Notifiable Diseases Surveillance
12 of 14 health.gov.au/cdiCommun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.20) Epub 4/3/2020
System (NNDSS) and state and territory health department media releases. The Communicable Diseases Network Australia (CDNA) developed the case definition for suspected and confirmed cases, which was modified at different time points in the epidemic (Table 3). Based on this guidance, state and territory health department investigators conducted interviews of suspected cases to collect core and enhanced data for inclu-sion in the NNDSS. Data was analysed using Stata to describe the epidemiology of COVID-19 in Australia and the progress of the epidemic.
Data for the international cases of COVID-19 by country were compiled from the latest WHO Situation Report. Case definitions may vary by country making comparisons difficult. Rapid reviews of the current state of knowledge on COVID-19 were conducted from the literature using PubMed.
Acknowledgements
This report represents surveillance data reported through CDNA as part of the nationally-coordi-nated response to COVID-19. We thank public health staff from incident emergency operations centres in state and territory health departments, and the Australian Government Department of Health; along with state and territory public health laboratories.
Author details
Corresponding author
Olivia Williams
NIR Surveillance Team, Communicable Disease Epidemiology and Surveillance Section, Health Protection Policy Branch, Australian Government Department of Health, GPO Box 9484, MDP 14, Canberra, ACT 2601.
Email: [email protected]
References
1. Queensland Health. Novel coronavirus alert.
[Internet.] Brisbane: Queensland Health; 2020. [Accessed on 1 March 2020.] Available from: https://www.health.qld.gov.au/news-events/health-alerts/novel-coronavirus.
2. Australian Government Department ofHealth. Australian Health Protection Prin-cipal Committee (AHPPC) statement oncoronavirus (COVID-19). [Internet.] Can-berra: Australian Government Departmentof Health; 2020. [Accessed on 28 February2020.] Available from: https://www.health.gov.au/news/australian-health-protection-principal-committee-ahppc-statement-on-coronavirus-covid-19-0.
3. World Health Organization (WHO). Coro-navirus disease 2019 (COVID-19) situa-tion report – 40: 29 February 2020. Geneva:WHO; 2020. [Accessed on 1 March 2020.]Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200229-sitrep-40-covid-19.pdf.
4. WHO. Novel coronavirus (2019-nCoV)situation report – 1: 21 January 2020. Ge-neva: WHO; 2020. [Accessed on 22 January2020.] Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200121-sitrep-1-2019-ncov.pdf.
5. WHO. Statement on the second meetingof the International Health Regulations(2005) Emergency Committee regardingthe outbreak of novel coronavirus (2019-nCoV). [Internet.] Geneva: WHO; 2020.[Accessed on 31 January 2020.] Availablefrom: https://www.who.int/news-room/detail/30-01-2020-statement-on-the-sec-ond-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavi-rus-(2019-ncov).
6. Australian Government Department ofHealth. Australian Health Protection Princi-pal Committee (AHPPC) novel coronavirusstatement on 1 February 2020. [Internet.]Canberra: Australian Government De-

13 of 14 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.20) Epub 4/3/2020
partment of Health; 2020. [Accessed on 7 February 2020.] Available from: https://www.health.gov.au/news/australian-health-protection-principal-committee-ahppc-novel-coronavirus-statement-on-1-febru-ary-2020.
7. Australian Government Department ofHealth. Australian Health Sector EmergencyResponse Plan for novel coronavirus (COV-ID-19). [Internet.] Canberra: AustralianGovernment Department of Health; 2020.[Accessed on 1 March 2020.] Available from:https://www.health.gov.au/sites/default/files/documents/2020/02/australian-health-sector-emergency-response-plan-for-novel-coronavirus-covid-19_1.pdf.
8. Australian Government Department ofHealth. Press conference about coronavirus(COVID-19) with the Chief Medical Officer.[Internet.] Canberra: Australian GovernmentDepartment of Health; 2020. [Accessed on1 March 2020.] Available from: https://www.health.gov.au/ministers/the-hon-greg-hunt-mp/media/press-conference-about-coronavi-rus-covid-19-with-the-chief-medical-officer.
9. Korea Centers for Disease Control & Preven-tion (KCDC). The updates of COVID-19 inRepublic of Korea as of 26 February, 2020.[Internet.] Osong, Republic of Korea: KCDC;2020. [Accessed on 1 March 2020.] Availablefrom: https://www.cdc.go.kr/board/board.es?mid=a30402000000&bid=0030&act=view&list_no=366352.
10. KCDC. The updates of COVID-19 in Koreaas of 29 Feb. 2020. [Internet.] Osong, Re-public of Korea: KCDC; 2020. [Accessed on1 March 2020.] Available from: https://www.cdc.go.kr/board/board.es?mid=a30402000000&bid=0030&act=view&list_no=366406.
11. Cable News Network (CNN). How novelcoronavirus spread through the Shincheonjireligious group in South Korea. [Internet.]Atlanta: CNN; 2020. [Accessed on 1 March2020.] Available from: https://edition.cnn.
com/2020/02/26/asia/shincheonji-south-korea-hnk-intl/index.html.
12. KCDC. The updates of COVID-19 in Re-public of Korea. [Internet.] Osong, Repub-lic of Korea: KCDC; 2020. [Accessed on1 March 2020.] Available from: https://www.cdc.go.kr/board/board.es?mid=a30402000000&bid=0030&act=view&list_no=366363.
13. KCDC. Press release – 219 additional casesare confirmed. [Internet.] Osong, Republic ofKorea: KCDC; 2020. [Accessed on 3 March2020.] Available from: https://www.cdc.go.kr/board/board.es?mid=a30402000000&bid=0030&act=view&list_no=366407.
14. KCDC. The updates of COVID-19 in Re-public of Korea as of 24 February, 2020.[Internet.] Osong, Republic of Korea: KCDC;2020. [Accessed on 1 March 2020.] Availablefrom: https://www.cdc.go.kr/board/board.es?mid=a30402000000&bid=0030&act=view&list_no=366328.
15. WHO. Coronavirus disease 2019 (COV-ID-19) situation reports. [Internet.] Geneva:WHO; 2020. [Accessed on 3 March 2020.]Available from: https://www.who.int/emer-gencies/diseases/novel-coronavirus-2019/situation-reports/.
16. WHO. Report of the WHO-China jointmission on coronavirus disease 2019 (COV-ID-19). [Internet.] Geneva: WHO; 2020.[Accessed on 1 March 2020.] Available from:https://www.who.int/docs/default-source/coronaviruse/who-china-joint-mission-on-covid-19-final-report.pdf.
17. Ji Y, Ma Z, Peppelenbosch MP, Pan Q.Potential association between COVID-19mortality and healthcare resource availability.Lancet Glob Health. 2020. doi: https://doi.org/10.1016/S2214-109X(20)30068-1.
18. Lan L, Xu D, Ye G, Xia C, Wang S, Li Y, etal. Positive RT-PCR test results in patientsrecovered from COVID-19. JAMA. 2020. doi:

14 of 14 health.gov.au/cdiCommun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.20) Epub 4/3/2020
https://doi.org/10.1001/jama.2020.2783.
19. Australian Government Department ofHealth. Novel coronavirus 2019 (2019-nCoV) - CDNA national guidelines for pub-lic health units. [Internet.] Canberra: Aus-tralia Government Department of Health;2020. [Accessed on 28 February 2020.]Available from: https://www1.health.gov.au/internet/main/publishing.nsf/Content/cdna-song-novel-coronavirus.htm.
20. Queensland Health. Queensland coronavi-rus update. [Internet.] Brisbane: QueenslandHealth; 2020. [Accessed on 1 March 2020.]Available from: https://www.health.qld.gov.au/news-events/doh-media-releases/releases/queensland-coronavirus-update5.
21. COVID-19 National Incident Room Surveil-lance Team. COVID-19, Australia: Epide-miology Report 4. Reporting week ending19:00 AEDT 22 February 2020. CommunDis Intell (2018). 2020;44. doi: https://doi.org/10.33321/cdi.2020.44.17.
22. WHO. Clinical management of severe acuterespiratory infection when novel coronavi-rus (nCoV) infection is suspected. [Inter-net.] Geneva: WHO; 2020. [Accessed on23 February 2020.] Available from: https://www.who.int/publications-detail/clinical-management-of-severe-acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-suspected.
23. Chinese Clinical Trial Registry. Trial search.[Internet.] Sichuan: Chinese Clinical TrialRegistry; 2020. [Accessed on 1 March 2020.]Available from: http://www.chictr.org.cn/searchprojen.aspx.
24. Mahase E. Coronavirus: home testing pilotlaunched in London to cut hospital visits andambulance use. BMJ;368:m621. 2020. doi:http://doi.org/10.1136/bmj.m621.
25. Bedford T, Neher R, Hadfield J, HodcroftE, Ilcisin M, Müller N. Genomic analysis
of nCOV spread. Situation report 2020-01-30. [Internet.] 2020. Available from:https://nextstrain.org/narratives/ncov/sit-rep/2020-01-30.

2 0 2 0 V o l u m e 4 4https://doi.org/10.33321/cdi.2020.44.21
COVID-19, Australia: Epidemiology Report 6:Reporting week ending 1900 AEDT 7 March 2020
COVID-19 National Incident Room Surveillance Team

Communicable Diseases Intelligence ISSN: 2209-6051 Online
This journal is indexed by Index Medicus and Medline.
Creative Commons Licence - Attribution-NonCommercial-NoDerivatives CC BY-NC-ND
© 2020 Commonwealth of Australia as represented by the Department of Health
This publication is licensed under a Creative Commons Attribution- Non-Commercial NoDerivatives 4.0 International Licence from https://creativecommons.org/licenses/by-nc-nd/4.0/legalcode (Licence). You must read and understand the Licence before using any material from this publication.
Restrictions The Licence does not cover, and there is no permission given for, use of any of the following material found in this publication (if any):
• the Commonwealth Coat of Arms (by way of information, the terms under which the Coat of Arms may be used can be found at www.itsanhonour.gov.au);
• any logos (including the Department of Health’s logo) and trademarks;
• any photographs and images;
• any signatures; and
• any material belonging to third parties.
Disclaimer Opinions expressed in Communicable Diseases Intelligence are those of the authors and not necessarily those of the Australian Government Department of Health or the Communicable Diseases Network Australia. Data may be subject to revision.
Enquiries Enquiries regarding any other use of this publication should be addressed to the Communication Branch, Department of Health, GPO Box 9848, Canberra ACT 2601, or via e-mail to: [email protected]
Communicable Diseases Network Australia Communicable Diseases Intelligence contributes to the work of the Communicable Diseases Network Australia. http://www.health.gov.au/cdna
Communicable Diseases Intelligence (CDI) is a peer-reviewed scientific journal published by the Office of Health Protection, Department of Health. The journal aims to disseminate information on the epidemiology, surveillance, prevention and control of communicable diseases of relevance to Australia.
Editor Cindy Toms
Deputy Editor Simon Petrie
Design and Production Kasra Yousefi
Editorial Advisory Board David Durrheim, Mark Ferson, John Kaldor, Martyn Kirk and Linda Selvey
Website http://www.health.gov.au/cdi
Contacts Communicable Diseases Intelligence is produced by: Health Protection Policy Branch Office of Health Protection Australian Government Department of Health GPO Box 9848, (MDP 6) CANBERRA ACT 2601
Email: [email protected]
Submit an Article You are invited to submit your next communicable disease related article to the Communicable Diseases Intelligence (CDI) for consideration. More information regarding CDI can be found at: http://health.gov.au/cdi.
Further enquiries should be directed to: [email protected].

1 of 15 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.21) Epub 11/3/2020
Weekly epidemiological report
COVID-19, Australia: Epidemiology Report 6:Reporting week ending 1900 AEDT 7 March 2020
COVID-19 National Incident Room Surveillance Team
Summary
This is the sixth epidemiological report for coronavirus disease 2019 (COVID-19), reported in Australia as at 19:00 Australian Eastern Daylight Time [AEDT] 7 March 2020. It includes data on COVID-19 cases diagnosed in Australia, the international situation and a review of current evidence.
Keywords: SARS-CoV-2; novel coronavirus; 2019-nCoV; coronavirus disease 2019; COVID-19; acute respiratory disease; case definition; epidemiology; Australia
The following epidemiological data are subject to change both domestically and internationally due to the rapidly evolving situation. Australian cases are still under active investigation. While every effort has been made to standardise the investigation of cases nationally, there may be some differences between jurisdictions.
In Australia:
• Seventy-one COVID-19 cases, including two deaths, were notified up until 19:00 AEDT 7 March 2020;
◦ Sixteen cases had direct or indirect links to mainland China;
◦ Ten cases, including one death, were among the ‘Diamond Princess’ cruise ship passen-gers repatriated from Japan;
◦ Sixteen cases had direct or indirect links to the Islamic Republic of Iran;
◦ Fourteen had a recent travel history to other countries;
◦ Fifteen cases, including one death, had no recent history of overseas travel;
• On 4 March 2020, the Australian Health Protection Principal Committee (AHPPC) recom-mended that the current travel restrictions for mainland China and the Islamic Republic of Iran remain in place for a further seven days; and
• On 5 March 2020, travel restrictions were announced for travellers from Republic of Korea and enhanced health screening for travellers from Italy.

2 of 15 health.gov.au/cdiCommun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.21) Epub 11/3/2020
Internationally:
• 101,927 infections have been confirmed globally, with 3,486 deaths;
• The majority of confirmed infections (79%; n = 80,651) and deaths (88%; n = 3,070) have been reported in mainland China;
• Outside of mainland China, cases (n = 21,276) have been reported in 96 countries, territories and areas, with approximately 78% of those cases reported from three countries: Italy, the Islamic Republic of Iran and Republic of Korea; and
• Outside of mainland China, 416 deaths were reported by 16 countries, territories and areas.
Domestic cases
There were 71 confirmed cases, including two deaths, reported in Australia as at 19:00 AEDT 7 March 2020 (Table 1). Of the 71 confirmed cases, 10 (14%) were among the ‘Diamond Princess’ cruise ship passengers repatriated from Japan (n = 164) to the Northern Territory on 20 February 2020. The remaining cases were reported in New South Wales (n = 33), Victoria (n = 8), Queensland (n = 12), Western Australia (n = 1), South Australia (n = 6) and Tasmania (n = 1) (Figure 1).
Of the 71 confirmed cases, 16 (23%) had direct or indirect links to mainland China, 10 (14%) were associated with the ‘Diamond Princess’ cruise ship, 16 (23%) had direct or indirect links to the Islamic Republic of Iran, 14 (20%) had a recent travel history to other countries and 15 (21%) had no recent history of overseas travel. Of the 15 cases who had no recent history of over-seas travel, these were all reported in New South Wales. Twelve of the cases were associated with an aged care facility, including four residents, three staff members and several close contacts outside of the facility. A further two cases were associated with a workshop and the source of infection/exposure for the remaining case was under investigation at the time of writing. The identification of COVID-19 clusters in New South Wales with no recent history of overseas
travel in any of the primary/index cases suggests that there has potentially been some very limited local transmission within New South Wales.
The median age of all 71 reported Australian cases was 45 years (range 0–94 years), with the highest proportion of cases aged 50–59 years (Table 2). Male-to-female ratio was approxi-mately 1:1. Twenty-two cases have been reported to have cleared their infections, and two cases were reported to have died. Of the two cases that died, both were aged over 65 years.
Of the 71 confirmed cases, 34 (48%) had symp-toms recorded. Cough was the most commonly reported symptom (Table 3) and no cases reported irritability/confusion, abdominal pain or acute respiratory disease.
International cases
As at 19:00 AEDT 7 March 2020, the number of confirmed COVID-19 cases reported to the World Health Organization (WHO) was 101,927 globally.1 The proportion of new cases reported from mainland China has continued to decrease, from 98% on 22 February 2020 to 79% (n = 80,651) on 7 March 2020.1,2 On 26 February 2020, the number of new cases outside of mainland China exceeded the number reported from mainland China for the first time and this trend has continued to date (Figure 2). The total number of confirmed COVID-19 cases reported by 96 countries, territories and areas outside of
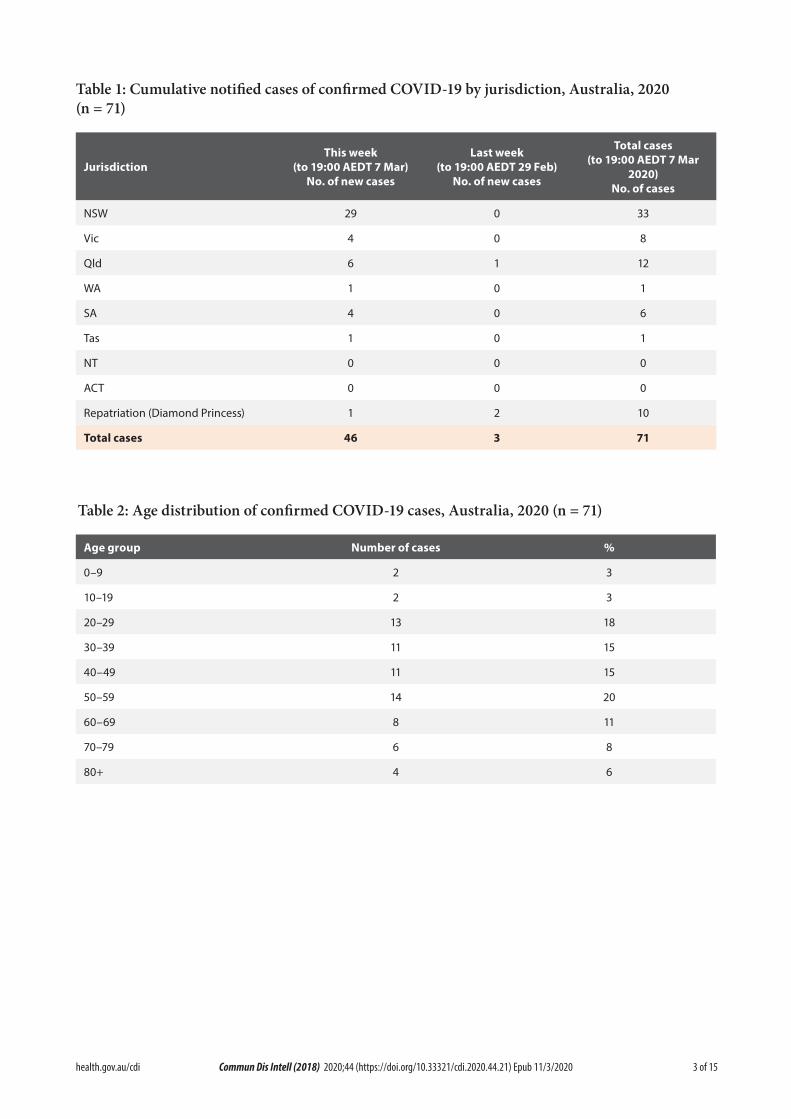
3 of 15 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.21) Epub 11/3/2020
Table 1: Cumulative notified cases of confirmed COVID-19 by jurisdiction, Australia, 2020 (n = 71)
JurisdictionThis week
(to 19:00 AEDT 7 Mar) No. of new cases
Last week (to 19:00 AEDT 29 Feb)
No. of new cases
Total cases (to 19:00 AEDT 7 Mar
2020) No. of cases
NSW 29 0 33
Vic 4 0 8
Qld 6 1 12
WA 1 0 1
SA 4 0 6
Tas 1 0 1
NT 0 0 0
ACT 0 0 0
Repatriation (Diamond Princess) 1 2 10
Total cases 46 3 71
Table 2: Age distribution of confirmed COVID-19 cases, Australia, 2020 (n = 71)
Age group Number of cases %
0–9 2 3
10–19 2 3
20–29 13 18
30–39 11 15
40–49 11 15
50–59 14 20
60–69 8 11
70–79 6 8
80+ 4 6
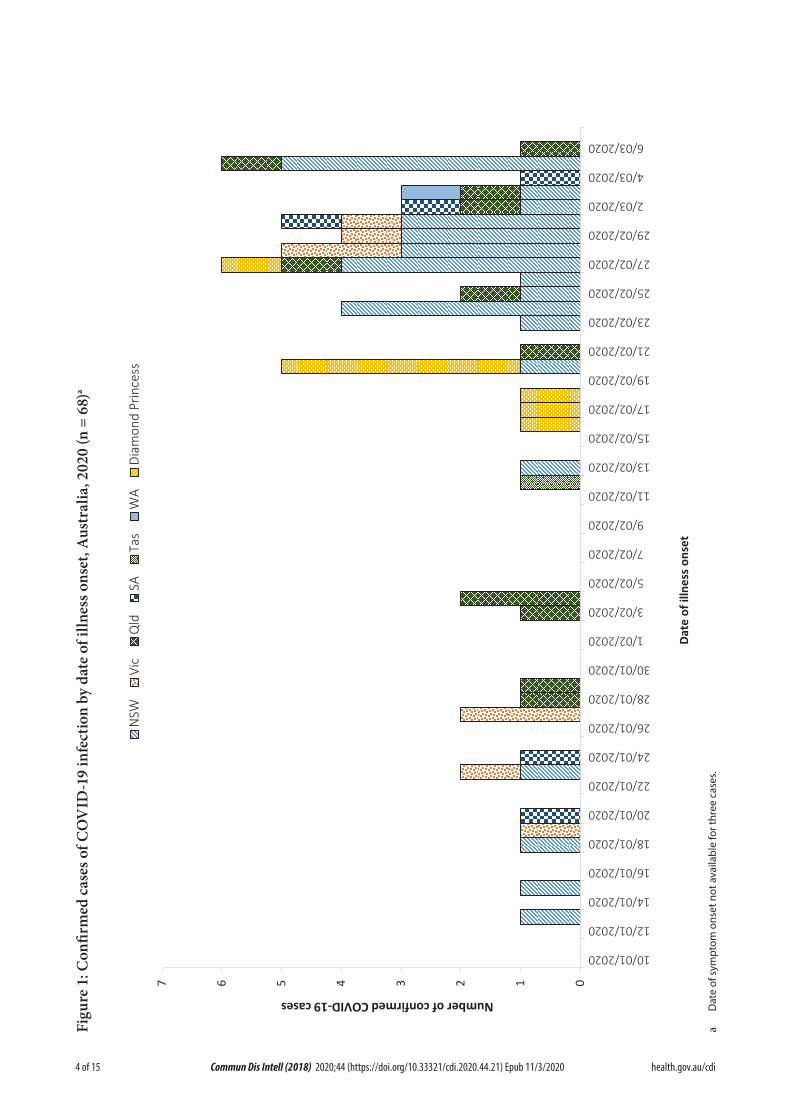
4 of 15 health.gov.au/cdiCommun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.21) Epub 11/3/2020
Figu
re 1
: Con
firm
ed c
ases
of C
OV
ID-1
9 in
fect
ion
by d
ate
of il
lnes
s ons
et, A
ustr
alia
, 202
0 (n
= 6
8)a
0123456710/01/2020
12/01/2020
14/01/2020
16/01/2020
18/01/2020
20/01/2020
22/01/2020
24/01/2020
26/01/2020
28/01/2020
30/01/2020
1/02/2020
3/02/2020
5/02/2020
7/02/2020
9/02/2020
11/02/2020
13/02/2020
15/02/2020
17/02/2020
19/02/2020
21/02/2020
23/02/2020
25/02/2020
27/02/2020
29/02/2020
2/03/2020
4/03/2020
6/03/2020
Number of confirmed COVID-19 cases
Date
of i
llnes
s on
set
NSW
Vic
Qld
SATa
sW
ADi
amon
d Pr
ince
ss
a D
ate
of s
ympt
om o
nset
not
ava
ilabl
e fo
r thr
ee c
ases
.

5 of 15 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.21) Epub 11/3/2020
Table 3: Symptoms of confirmed COVID-19 cases, Australia, 2020 (n = 34)
Symptom Number of cases %
Cough 24 71
Fever 22 65
Sore throat 17 50
Headache 12 35
Runny nose 10 29
Diarrhoea 9 26
Muscular pain 6 18
Joint pain 6 18
Shortness of breath 3 9
Nausea/vomiting 2 6
Chest pain 2 6
Pneumonia 2 6
mainland China in the current reporting week have increased almost four-fold (n = 21,276) compared to the preceding week (n = 5,447), where 696 confirmed cases were associated with the cruise ship ‘Diamond Princess’.1,3 The Republic of Korea reported 33% (n = 6,767) of all cases outside of mainland China, Italy reported 23% (n = 4,636), the Islamic Republic of Iran 23% (n = 4,747) and Japan 2% (n = 408). Thirty-five new countries, territories and areas reported cases of COVID-19 in the past seven days. Of all the countries, territories and areas outside of mainland China with known transmission clas-sification (n = 87), 45 (52%) have reported local transmission of COVID-19. Cambodia, Nepal and Sri Lanka have not reported any new cases for at least 14 days.1
Globally, 3,486 deaths have been reported, with 85% (n = 2,959) reported from Hubei Province, China and 111 deaths reported from elsewhere within mainland China. The remaining 416 deaths were reported by 16 countries, territories and areas outside of mainland China.1

6 of 15 health.gov.au/cdiCommun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.21) Epub 11/3/2020
Figu
re 2
. Cas
es o
f CO
VID
-19
repo
rted
to W
HO
; and
num
ber o
f cou
ntri
es, t
erri
tori
es a
nd a
reas
repo
rtin
g ou
tsid
e m
ainl
and
Chi
na fr
om 2
1 Ja
nuar
y to
7 M
arch
202
04
020406080100
120
0
500
1,00
0
1,50
0
2,00
0
2,50
0
3,00
0
3,50
0
4,00
0
4,50
0
21/01/2020
23/01/2020
25/01/2020
27/01/2020
29/01/2020
31/01/2020
02/02/2020
04/02/2020
06/02/2020
08/02/2020
10/02/2020
12/02/2020
14/02/2020
16/02/2020
18/02/2020
20/02/2020
22/02/2020
24/02/2020
26/02/2020
28/02/2020
01/03/2020
03/03/2020
05/03/2020
07/03/2020
Number of countries, territories and areas outside of mainland China
Number of reported cases
Date
of r
epor
ting
Mai
nlan
d Ch
ina
Out
side
of m
ainl
and
Chin
aN
umbe
r of c
ount
ries,
terr
itorie
s and
are
as o
utsid
e of
mai
nlan
d Ch
ina
a
b
c
a W
HO
dec
lare
s th
e ou
tbre
ak o
f CO
VID
-19
a Pu
blic
Hea
lth E
mer
genc
y of
Inte
rnat
iona
l Con
cern
b W
HO
sta
rts
repo
rtin
g bo
th la
bora
tory
con
firm
ed a
nd c
linic
ally
dia
gnos
ed c
ases
from
Hub
ei P
rovi
nce
c H
ubei
Pro
vinc
e ce
ase
repo
rtin
g cl
inic
ally
dia
gnos
ed c
ases

7 of 15 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.21) Epub 11/3/2020
Country in focus: the Islamic Republic of Iran
Data on confirmed cases of COVID-19 in the Islamic Republic of Iran have not been made publicly available. The following is therefore a brief summary based on information obtained from WHO situation reports.
The Islamic Republic of Iran reported its first confirmed case of COVID-19 on 20 February 2020. From then, reported cases in the Islamic Republic of Iran increased rapidly, from two confirmed cases on 20 February 2020 to 4,747 on 7 March 2020. Among the cases reported as at 7 March 2020, 30% (n = 1,413) were reported in Tehran, 11% (n = 523) in Qom and 9% (n = 424) in Gilan. The Islamic Republic of Iran is one of the countries outside of mainland China with the most rapid growth of COVID-19 cases (Figure 3).
Based on confirmed cases up to 7 March 2020, the case fatality rate (CFR) for the Islamic Republic of Iran has been calculated at 2.6%. As the outbreak continues, the confirmed CFR may change. The current calculated CFR does not include the number of cases with mild infections that may be missed from current surveillance, nor does it account for the recently confirmed cases that may subsequently develop severe disease and die.
Background
On 31 December 2019, the World Health Organization (WHO) was notified about a large number of cases of pneumonia of unknown origin in Wuhan City, Hubei Province, China. Chinese authorities isolated and identified a novel coronavirus on 7 January 2020.5 WHO declared the outbreak of COVID-19 a Public Health Emergency of International Concern (PHEIC) on 30 January 2020.6
From 1 February 2020, Australia denied entry to anyone who had left or transited through main-land China, with the exception of Australian citizens, permanent residents and their imme-diate family and air crew who have been using appropriate personal protective equipment (Figure 4).7 The Australian Health Protection Principal Committee (AHPPC) have reviewed these restrictions weekly, and on 4 March 2020, they released a statement recommending cur-rent travel restrictions for mainland China and the Islamic Republic of Iran remain in place for a further seven days.8 On 5 March 2020, the Prime Minister announced new travel restrictions for travellers coming from Republic of Korea, and implementation of enhanced health screening
for arrivals from Italy. From 5 March 2020, for-eign nationals (excluding permanent residents of Australia) will be prevented from coming to Australia until 14 days after leaving Republic of Korea.9
The AHPPC acknowledged that Australia’s bor-der measures may no longer be able to prevent the importation of COVID-19, and the primary focus should now be directed at domestic con-tainment and preparedness.8 Local transmis-sion of COVID-19 has occurred in Australia, highlighting the need of effective containment measures to limit spread. Early isolation of iden-tified cases and quarantine of suspected cases and close contacts is a key measure to minimise transmission of COVID-19 in the community. However, as COVID-19 presents as mild illness in the majority of cases, early identification and isolation of cases may be difficult to achieve.
The current estimates on epidemiological param-eters including severity, transmissibility and incubation period are uncertain. Estimates are likely to change as more information becomes available.
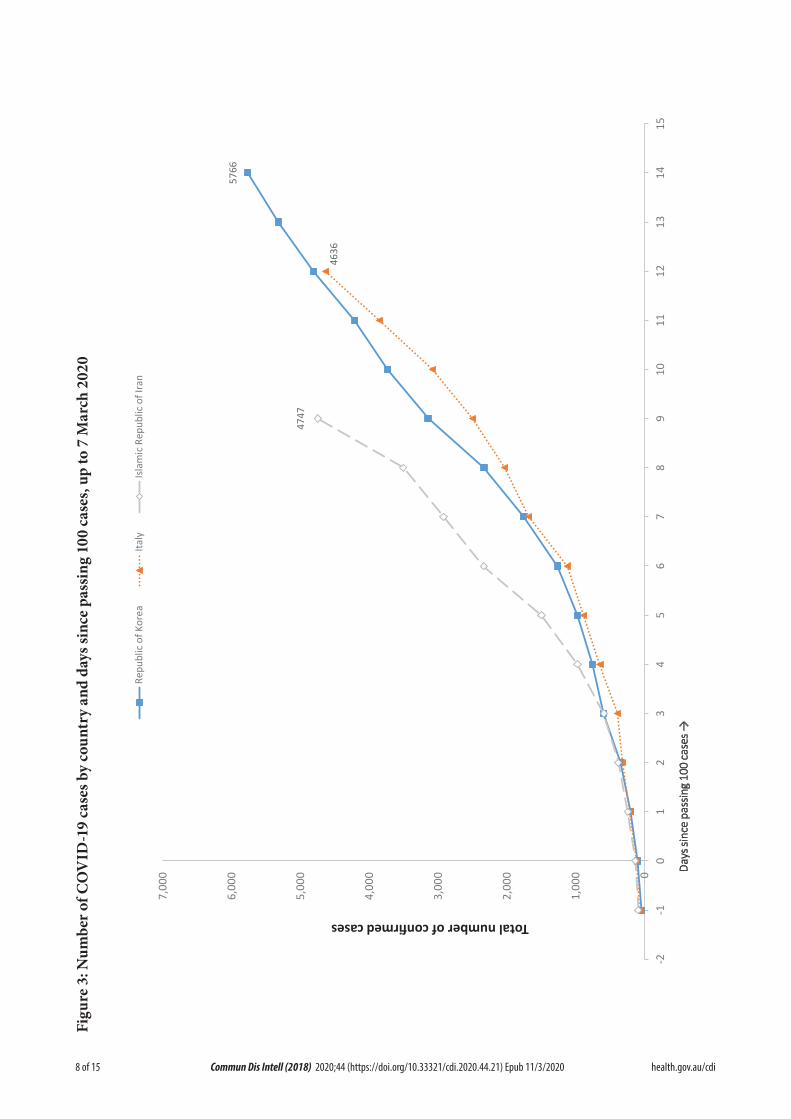
8 of 15 health.gov.au/cdiCommun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.21) Epub 11/3/2020
Figu
re 3
: Num
ber o
f CO
VID
-19
case
s by
coun
try
and
days
sinc
e pa
ssin
g 10
0 ca
ses,
up to
7 M
arch
202
0
5766
4636
4747
0
1,00
0
2,00
0
3,00
0
4,00
0
5,00
0
6,00
0
7,00
0
-2-1
01
23
45
67
89
1011
1213
1415
Total number of confirmed cases
Day
s sin
ce p
assin
g 10
0 ca
ses →
Repu
blic
of K
orea
Italy
Isla
mic
Rep
ublic
of I
ran

9 of 15 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.21) Epub 11/3/2020
Figu
re 4
: A ti
mel
ine
of k
ey e
vent
s in
the
COVI
D-1
9 ou
tbre
ak, A
ustr
alia
, up
to 7
Mar
ch 2
020

10 of 15 health.gov.au/cdiCommun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.21) Epub 11/3/2020
Severity
Ongoing evidence, including a recently pub-lished meta-analysis, supports previous research that COVID-19 presents as mild illness in the majority of cases with fever and cough being the most commonly reported symptoms. Severe or fatal outcomes tend to occur in the elderly or those with comorbid conditions.10,11 Examination of cases and their close contacts in China found an association between age and time from symptom onset to recovery. Median time to recovery was estimated to be 27 days in 20–29 year olds, 32 days in 50–59 year olds, and 36 days in those aged over 70 years. The study also found an association between clinical sever-ity and time from symptom onset to recovery. Compared to people with mild disease, those with moderate and severe disease were associ-ated with a 19% and 58% increase in recovery time, respectively.12
Transmission
Human-to-human transmission of SARS-CoV-2 is via droplets and fomites from an infected person to a close contact.10 Examination of cases and their close contacts in China supports this. Household contacts and those who travelled with a confirmed COVID-19 case were strongly associated with an increased risk of infection.12 The study also examined the average time from symptom onset to disease confirmation and isolation among cases identified through symptom-based (i.e. symptomatic screening at airports, community fever monitoring and testing of hospital patients) and contact-based (i.e. monitoring and testing of close contacts of confirmed COVID-19 cases) surveillance. Compared to cases identified through symp-tom-based surveillance, cases identified through contact-based surveillance were associated with a 2.3 day decrease from symptom onset to dis-ease confirmation, and a 1.9 day decrease from symptom onset to isolation. Based on modelling, researchers have found that effective contact tracing increases the probability of control.12
Current evidence does not support airborne or faecal-oral spread as major factors in transmis-sion.10
Incubation period
No new research has been published on the incubation period for COVID-19. Please refer to COVID-19, Australia: Epidemiology Report 4 for the most recently published summary.13
Treatment
Current clinical management of COVID-19 cases focuses on early recognition, isolation, appropriate infection control measures and provision of supportive care.14 Whilst there is no specific antiviral treatment currently rec-ommended for patients with suspected or con-firmed SARS-CoV-2 infection, multiple clinical trials are underway to evaluate a number of therapeutic agents, including remdesivir and lopinavir/ritonavir.15
Virology
Based on modelling, researchers estimated that initial human SARS-CoV-2 infection was in November to early December 2019.16 An analysis based on 86 genomic sequences of SARS-CoV-2, obtained from the Global Initiative on Sharing All Influenza Data (GISAID), found many mutations.17 This suggests that SARS-CoV-2 has rapidly evolved since the outbreak occurred. Ongoing surveillance of sequences and shared mutations will assist with understanding of the global spread of the virus.
Comparison between COVID-19, SARS and MERS
Coronaviruses are a group of viruses that can cause upper respiratory tract infections in humans. Coronaviruses can occasionally cause severe diseases such as Middle East Respiratory Syndrome (MERS), Severe Acute Respiratory Syndrome (SARS) and more recently COVID-19. Similar to MERS and SARS, COVID-19 is thought to have originated from bats, and trans-

11 of 15 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.21) Epub 11/3/2020
mitted to humans via an intermediate animal host. The intermediate animal host is currently unknown.18 Table 4 provides an overview of characteristics of COVID-19, MERS and SARS.
Public health response
The Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19) describes some of the key aspects associated with the evolving outbreak in mainland China, including the outbreaks transmission dynam-ics, disease progression and severity, mainland China’s response and knowledge gaps. As part of the report, the following major recommenda-tions were made for countries with imported cases and/or outbreaks of COVID-19:10
1. Immediately activate the highest level of national Response Management protocols to ensure the all-of-government and all-of-so-ciety approach needed to contain COVID-19 with non-pharmaceutical public health measures;
2. Prioritise active, exhaustive case finding and immediate testing and isolation, painstaking contact tracing and rigorous quarantine of close contacts;
3. Fully educate the general public on the seriousness of COVID-19 and their role in preventing its spread;
4. Immediately expand surveillance to detect COVID-19 transmission chains, by test-ing all patients with atypical pneumonias, conducting screening in some patients with upper respiratory illnesses and/or recent COVID-19 exposure, and adding testing for the COVID-19 virus to existing surveillance systems (e.g. systems for influenza-like-illness); and
5. Conduct multi-sector scenario planning and simulations for the deployment of even more stringent measures to interrupt transmis-sion chains as needed (e.g. the suspension of large-scale gatherings and the closure of
schools and workplaces).
Methods
Data for this report were current as at 19:00 hours AEDT, 7 March 2020.
This report outlines what is known epidemio-logically on COVID-19 in Australia and from publicly available data from WHO Situation Reports, other countries’ official updates and the scientific literature. Data on domestic cases in this report were collected from the National Notifiable Diseases Surveillance System (NNDSS) and jurisdictional health department media releases. The Communicable Diseases Network Australia (CDNA) developed the case definition for suspect and confirmed cases, which was modified at different time points during the outbreak (Table 5). Data was ana-lysed using Stata to describe the epidemiology of COVID-19 in Australia and the progress of the epidemic.
Data for the international cases of COVID-19 by country were compiled from the latest WHO Situation Report. Case definitions may vary by country making comparisons difficult. Rapid reviews of the current state of knowledge on COVID-19 were conducted from the literature using PubMed.
Acknowledgements
This report represents surveillance data reported through CDNA as part of the nationally-coordi-nated response to COVID-19. We thank public health staff from incident emergency operations centres in state and territory health departments, and the Australian Government Department of Health, along with state and territory public health laboratories.

12 of 15 health.gov.au/cdiCommun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.21) Epub 11/3/2020
Tabl
e 4:
Cha
ract
eris
tics o
f CO
VID
-19,
MER
S an
d SA
RS19
–21
COV
ID-1
9M
ERS
SARS
Med
ian
incu
batio
n pe
riod
5–6
days
5 da
ys4–
5 da
ys
Mod
e of
tran
smis
sion
Resp
irato
ry d
ropl
et, c
lose
con
tact
, fom
ites
Resp
irato
ry d
ropl
et, c
lose
con
tact
Resp
irato
ry d
ropl
et, c
lose
con
tact
, fom
ites
Sym
ptom
sFe
ver,
coug
h, fa
tigue
and
diffi
culty
with
br
eath
ing
(dys
pnoe
a)Fe
ver,
coug
h an
d sh
ortn
ess
of b
reat
hFe
ver,
mal
aise
, mya
lgia
, hea
dach
e, d
iarr
hoea
an
d sh
iver
ing
(rigo
rs)
Num
ber o
f cou
ntrie
s an
d re
gion
s aff
ecte
d97
2729
Regi
ons
seve
rely
affe
cted
Mai
nlan
d Ch
ina,
Rep
ublic
of K
orea
, Ita
ly a
nd
Isla
mic
Rep
ublic
of I
ran
Saud
i Ara
bia
Mai
nlan
d Ch
ina,
Hon
g Ko
ng S
AR,
Tai
wan
, Ca
nada
, Sin
gapo
re
Num
ber o
f cas
es g
loba
lly10
1,92
72,
519
8,42
2
Num
ber o
f dea
ths
glob
ally
3,48
686
691
6
Glo
bal c
ase
fata
lity
rate
3.4%
34.3
%10
.9%
Prop
hyla
xis
avai
labl
eN
oN
oN
o
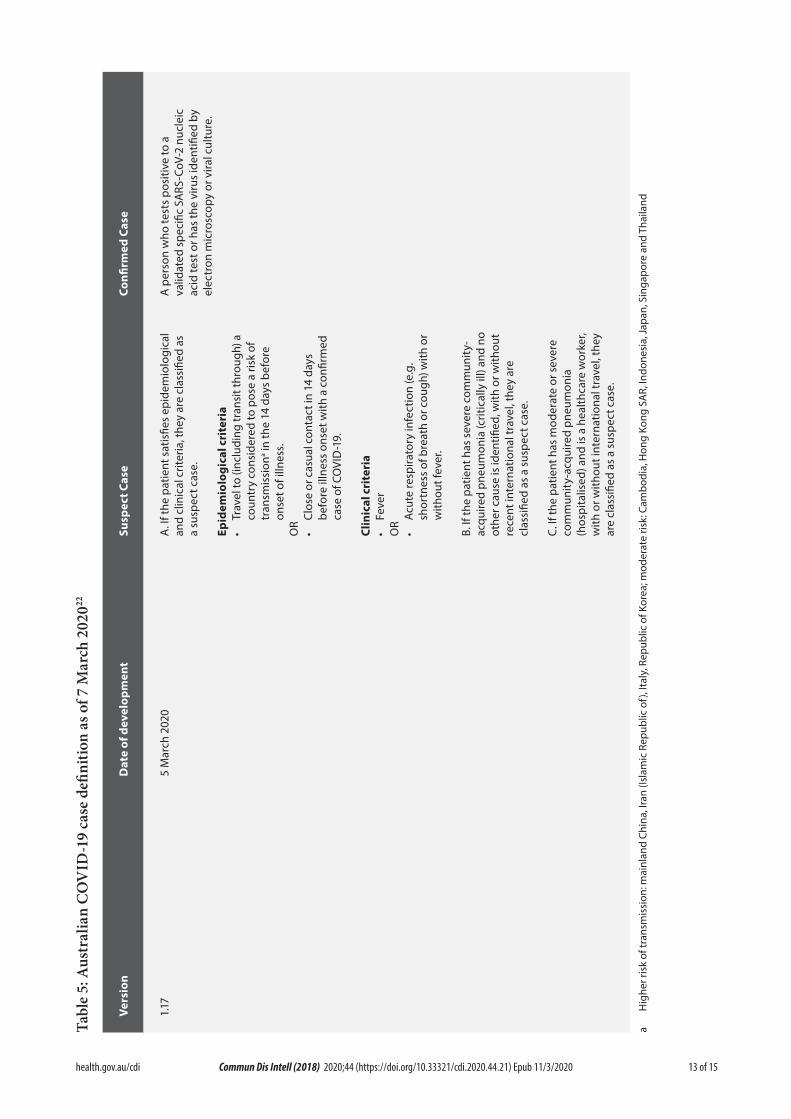
13 of 15 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.21) Epub 11/3/2020
Tabl
e 5:
Aus
tral
ian
CO
VID
-19
case
defi
nitio
n as
of 7
Mar
ch 2
02022
Vers
ion
Dat
e of
dev
elop
men
tSu
spec
t Cas
eCo
nfirm
ed C
ase
1.17
5 M
arch
202
0A
. If t
he p
atie
nt s
atis
fies
epid
emio
logi
cal
and
clin
ical
crit
eria
, the
y ar
e cl
assi
fied
as
a su
spec
t cas
e.
Epid
emio
logi
cal c
rite
ria
• Tr
avel
to (i
nclu
ding
tran
sit t
hrou
gh) a
co
untr
y co
nsid
ered
to p
ose
a ris
k of
tr
ansm
issi
ona in
the
14 d
ays
befo
re
onse
t of i
llnes
s.O
R•
Clos
e or
cas
ual c
onta
ct in
14
days
be
fore
illn
ess
onse
t with
a c
onfir
med
ca
se o
f CO
VID
-19.
Clin
ical
cri
teri
a•
Feve
rO
R•
Acu
te re
spira
tory
infe
ctio
n (e
.g.
shor
tnes
s of
bre
ath
or c
ough
) with
or
with
out f
ever
.
B. If
the
patie
nt h
as s
ever
e co
mm
unity
-ac
quire
d pn
eum
onia
(crit
ical
ly il
l) an
d no
ot
her c
ause
is id
entifi
ed, w
ith o
r with
out
rece
nt in
tern
atio
nal t
rave
l, th
ey a
re
clas
sifie
d as
a s
uspe
ct c
ase.
C. I
f the
pat
ient
has
mod
erat
e or
sev
ere
com
mun
ity-a
cqui
red
pneu
mon
ia
(hos
pita
lised
) and
is a
hea
lthca
re w
orke
r, w
ith o
r with
out i
nter
natio
nal t
rave
l, th
ey
are
clas
sifie
d as
a s
uspe
ct c
ase.
A p
erso
n w
ho te
sts
posi
tive
to a
va
lidat
ed s
peci
fic S
ARS
-CoV
-2 n
ucle
ic
acid
test
or h
as th
e vi
rus
iden
tified
by
elec
tron
mic
rosc
opy
or v
iral c
ultu
re.
a H
ighe
r ris
k of
tran
smis
sion
: mai
nlan
d Ch
ina,
Iran
(Isl
amic
Rep
ublic
of)
, Ita
ly, R
epub
lic o
f Kor
ea; m
oder
ate
risk:
Cam
bodi
a, H
ong
Kong
SA
R, In
done
sia,
Japa
n, S
inga
pore
and
Tha
iland

14 of 15 health.gov.au/cdiCommun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.21) Epub 11/3/2020
Author details
Corresponding author
Tracy Tsang
NIR Surveillance Team, Communicable Disease Epidemiology and Surveillance Section, Health Protection Policy Branch, Australian Government Department of Health, GPO Box 9484, MDP 14, Canberra, ACT 2601.
Email: [email protected]
References
1. World Health Organization (WHO). Coro-navirus disease 2019 (COVID-19) situa-tion report – 47: 07 March 2020. Geneva: WHO; 2020. [Accessed on 8 March 2020.] Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200307-sitrep-47-covid-19.pdf.
2. WHO. Coronavirus disease 2019 (COV-ID-19) situation report – 33: 22 February 2020. Geneva: World Health Organization; 2020. [Accessed on 23 February 2020.] Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200222-sitrep-33-covid-19.pdf.
3. WHO. Coronavirus disease 2019 (COV-ID-19) situation report – 40: 29 February 2020.. Geneva: WHO; 2020. [Accessed on 1 March 2020.] Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200229-sitrep-40-cov-id-19.pdf.
4. WHO. Coronavirus disease 2019 (COV-ID-19) situation reports. [Internet.] Geneva: WHO; 2020. [Accessed on 3 March 2020.] Available from: https://www.who.int/emer-gencies/diseases/novel-coronavirus-2019/situation-reports/.
5. WHO. Novel coronavirus (2019-nCoV) situation report – 1: 21 January 2020. Ge-
neva: WHO; 2020. [Accessed on 22 January 2020.] Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200121-sitrep-1-2019-ncov.pdf.
6. WHO. Statement on the second meeting of the International Health Regulations (2005) Emergency Committee regarding the outbreak of novel coronavirus (2019-nCoV). [Internet.] Geneva: WHO; 2020. [Accessed on 31 January 2020.] Available from: https://www.who.int/news-room/detail/30-01-2020-statement-on-the-sec-ond-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavi-rus-(2019-ncov).
7. Australian Government Department of Health. Australian Health Protection Princi-pal Committee (AHPPC) novel coronavirus statement on 1 February 2020. [Internet.] Canberra: Australian Government Depart-ment of Health; 2020. [Accessed on 7 Feb-ruary 2020.] Available from: https://www.health.gov.au/news/australian-health-protec-tion-principal-committee-ahppc-novel-coro-navirus-statement-on-1-february-2020.
8. Australian Government Department of Health. Australian Health Protection Prin-cipal Committee (AHPPC) coronavirus (COVID-19) statement on 4 March 2020. [Internet.] Canberra: Australian Government Department of Health; 2020. [Accessed on 7 March 2020.] Available from: https://www.health.gov.au/news/australian-health-protec-tion-principal-committee-ahppc-coronavi-rus-covid-19-statement-on-4-march-2020.
9. Australian Government Department of the Prime Minister and Cabinet. Update on novel coronavirus (COVID-19) in Australia. [Internet.] Canberra: Australian Govern-ment Department of the Prime Minister and Cabinet; 2020. [Accessed on 7 March 2020.] Available from: https://www.pm.gov.au/media/update-novel-coronavirus-covid-19-australia-0.

15 of 15 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.21) Epub 11/3/2020
10. WHO. Report of the WHO-China joint mission on coronavirus disease 2019 (COV-ID-19). Geneva: World Health Organization; 2020. [Accessed on 1 March 2020.] Available from: https://www.who.int/docs/default-source/coronaviruse/who-china-joint-mis-sion-on-covid-19-final-report.pdf.
11. Sun P, Qie S, Liu Z, Ren J, Xi JJ. Clinical characteristics of 50466 patients with 2019-nCoV infection. medRxiv. 2020. doi: https://doi.org/10.1101/2020.02.18.20024539.
12. Bi Q, Wu Y, Mei S, Ye C, Zou X, Zhang Z et al. Epidemiology and transmission of COVID-19 in Shenzhen China: analysis of 391 cases and 1286 of their close contacts. medRxiv. 2020. doi: https://doi.org/10.1101/2020.03.03.20028423.
13. COVID-19 National Incident Room Surveil-lance Team. COVID-19, Australia: Epide-miology Report 4. Reporting week ending 19:00 AEDT 22 February 2020. Commun Dis Intell (2018). 2020;44. doi: https://doi.org/10.33321/cdi.2020.44.17.
14. WHO. Clinical management of severe acute respiratory infection when novel coronavirus (nCoV) infection is suspected. [Internet.] Geneva: WHO; 2020. [Accessed on 23 Febru-ary 2020.] Available from: https://www.who.int/publications-detail/clinical-management-of-severe-acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-sus-pected.
15. WHO. Coronavirus disease 2019 (COV-ID-19) situation report – 41: 01 March 2020. Geneva: WHO; 2020. [Accessed on 7 March 2020.] Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200301-sitrep-41-covid-19.pdf.
16. Bedford T, Neher R, Hadfield J, Hodcroft E, Ilcisin M, Müller N. Genomic analysis of nCOV spread. Situation report 2020-01-30. [Internet.] 2020. Available from: https://nextstrain.org/narratives/ncov/sit-
rep/2020-01-30.
17. Phan T. Genetic diversity and evolu-tion of SARS-CoV-2. Infect Genet Evol. 2020. doi: https://doi.org/10.1016/j.meegid.2020.104260.
18. WHO. Novel coronavirus (2019-nCoV) situation report – 22: 11 February 2020. Ge-neva: WHO; 2020. [Accessed on 12 February 2020.] Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200211-sitrep-22-ncov.pdf.
19. World Health Organization Regional Of-fice for the Eastern Mediterranean. MERS situation update, January 2020. [Internet.] Egypt: World Health Organization Regional Office for the Eastern Mediterranean; 2020. [Accessed on 7 March 2020.] Available from: http://www.emro.who.int/pandemic-epidem-ic-diseases/mers-cov/mers-situation-update-january-2020.html.
20. Centers for Disease Control and Prevention. MERS clinical features. [Internet.] Atlanta: CDC; 2019. [Accessed on 7 March 2020.] Available from: https://www.cdc.gov/corona-virus/mers/clinical-features.html.
21. WHO. Consensus document on the epi-demiology of severe acute respiratory syn-drome (SARS). [Internet.] Geneva: WHO; 2003. [Accessed on 7 March 2020.] Available from: https://www.who.int/csr/sars/WHOc-onsensus.pdf?ua=1.
22. Australian Government Department of Health. Novel coronavirus 2019 (2019-nCoV) - CDNA national guidelines for pub-lic health units. [Internet.] Canberra: Aus-tralian Government Department of Health; 2020. [Accessed on 28 February 2020.] Available from: https://www1.health.gov.au/internet/main/publishing.nsf/Content/cdna-song-novel-coronavirus.htm.

2 0 2 0 V o l u m e 4 4https://doi.org/10.33321/cdi.2020.44.23
COVID-19, Australia: Epidemiology Report 7: Reporting week ending 19:00 AEDT 14 March 2020
COVID-19 National Incident Room Surveillance Team

Communicable Diseases Intelligence ISSN: 2209-6051 Online
This journal is indexed by Index Medicus and Medline.
Creative Commons Licence - Attribution-NonCommercial-NoDerivatives CC BY-NC-ND
© 2020 Commonwealth of Australia as represented by the Department of Health
This publication is licensed under a Creative Commons Attribution- Non-Commercial NoDerivatives 4.0 International Licence from https://creativecommons.org/licenses/by-nc-nd/4.0/legalcode (Licence). You must read and understand the Licence before using any material from this publication.
Restrictions The Licence does not cover, and there is no permission given for, use of any of the following material found in this publication (if any):
• the Commonwealth Coat of Arms (by way of information, the terms under which the Coat of Arms may be used can be found at www.itsanhonour.gov.au);
• any logos (including the Department of Health’s logo) and trademarks;
• any photographs and images;
• any signatures; and
• any material belonging to third parties.
Disclaimer Opinions expressed in Communicable Diseases Intelligence are those of the authors and not necessarily those of the Australian Government Department of Health or the Communicable Diseases Network Australia. Data may be subject to revision.
Enquiries Enquiries regarding any other use of this publication should be addressed to the Communication Branch, Department of Health, GPO Box 9848, Canberra ACT 2601, or via e-mail to: [email protected]
Communicable Diseases Network Australia Communicable Diseases Intelligence contributes to the work of the Communicable Diseases Network Australia. http://www.health.gov.au/cdna
Communicable Diseases Intelligence (CDI) is a peer-reviewed scientific journal published by the Office of Health Protection, Department of Health. The journal aims to disseminate information on the epidemiology, surveillance, prevention and control of communicable diseases of relevance to Australia.
Editor Tanja Farmer
Deputy Editor Simon Petrie
Design and Production Kasra Yousefi
Editorial Advisory Board David Durrheim, Mark Ferson, John Kaldor, Martyn Kirk and Linda Selvey
Website http://www.health.gov.au/cdi
Contacts Communicable Diseases Intelligence is produced by: Health Protection Policy Branch Office of Health Protection Australian Government Department of Health GPO Box 9848, (MDP 6) CANBERRA ACT 2601
Email: [email protected]
Submit an Article You are invited to submit your next communicable disease related article to the Communicable Diseases Intelligence (CDI) for consideration. More information regarding CDI can be found at: http://health.gov.au/cdi.
Further enquiries should be directed to: [email protected].

1 of 17 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.23) Epub 19/3/2020
Weekly epidemiological report
COVID-19, Australia: Epidemiology Report 7:Reporting week ending 19:00 AEDT 14 March 2020
COVID-19 National Incident Room Surveillance Team
Summary
This is the seventh epidemiological report for coronavirus disease 2019 (COVID-19), reported in Australia as at 19:00 Australian Eastern Daylight Time [AEDT] 14 March 2020. It includes data on COVID-19 cases diagnosed in Australia, the international situation and a review of current evidence.
Keywords: SARS-CoV-2; novel coronavirus; 2019-nCoV; coronavirus disease 2019; COVID-19; acute respiratory disease; case definition; epidemiology; Australia
The following epidemiological data are subject to change both domestically and internationally due to the rapidly evolving situation. Australian cases are still under active investigation. While every effort has been made to standardise the investigation of cases nationally, there may be some differences between jurisdictions.
Domestic cases
There were 295 confirmed cases, including three deaths, reported in Australia as at 19:00 AEDT 14 March 2020 (Table 1). Of the 295 confirmed cases, 51.5% (n = 152) were reported in NSW, 18.6% (n = 55) from Qld, 15.6% (n = 46) from Vic, 7.1% (n = 21) from SA, 4.7% (n = 14) from WA, 2% (n = 6) from Tas, and 0.3% (n = 1) from ACT (Figure 1).
Of the 295 confirmed cases reported in the National Notifiable Diseases Surveillance System (NNDSS), 86% (n = 253) reported a place of acquisition and 14% (n = 42) remain under investigation. Of reported place of acquisition, 66% (n = 166) had a recent travel history and 34% (n = 87) were locally acquired. Of cases that reported recent travel history, 22% (n = 36) have a direct link to USA, 11% (n = 18) have a direct link to Italy, 9% (n = 15) have a direct link to Iran, 8% (n = 13) have a direct link to the UK, 8% (n = 13) have a direct link to China, 6% (n = 10) were passengers on the ‘Diamond Princess’
cruise ship repatriated from Japan, and 37% (n = 61) have a recent travel history to other coun-tries.
Of the 34% (n = 87) of cases that were locally acquired, 75% (n = 65) were from NSW, 9% (n = 8) from Qld, 9% (n = 8) from SA, 2% (n = 2) from WA, 2% (n = 2) from Vic, 1% (n = 1) from ACT and 1% (n = 1) from Tas.
There were three reported deaths as of 14 March 2020, one associated with the ‘Diamond Princess’ cruise ship, and two who were part of the same aged care facility cluster in NSW.
The median age of all 295 reported Australian cases was 47 years (range 0–94 years), with the highest proportion of cases aged 50–59 and 60–69 years (Figure 2). The male-to-female ratio was approximately 1:1. All three cases that were reported to have died were aged over 70 years.
Of the 295 confirmed cases, 76% (n = 225) had hospitalisation data reported (Figure 3). Of those

2 of 17 health.gov.au/cdiCommun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.23) Epub 19/3/2020
In Australia:
• 295 COVID-19 cases, including three deaths, were notified up until 19:00 AEDT 14 March 2020;
◦ In the National Notifiable Diseases Surveillance System (NNDSS), 86% (n = 253) of all cases have a reported place of acquisition and 14% (n = 42) remain under investigation;
◦ Of reported places of acquisition, 66% (n = 166) had a recent overseas travel history and 34% (n = 87) were locally acquired. 14% (n = 42) are pending investigation;
◦ Of reported recent overseas travel history:
◦ 22% (n = 36) have a direct link to USA;
◦ 11% (n = 18) have a direct link to Italy;
◦ 9% (n = 15) have a direct link to Iran;
◦ 8% (n = 13) have a direct link to the UK;
◦ 8% (n = 13) have a direct to China;
◦ 6% (n = 10) are associated with the ‘Diamond Princess’ cruise ship passengers repatriated from Japan;
◦ 37% (n = 61) have a recent travel history to other countries;
• Of the three reported deaths, one was associated with the ‘Diamond Princess’ cruise ship, and two were part of the same aged care facility cluster; and
• Since the last report, AHPPC have provided further recommendations on public events, travel restrictions, work restrictions for health and aged care workers, and public gatherings and testing.
Internationally:
• 142,539 infections have been confirmed globally, with 5,393 deaths;
• The majority of confirmed infections (57%; n = 81,021) and deaths (59%; n = 3,194) have been reported in mainland China;
• Outside of mainland China, cases (n = 61,518) have been reported in 134 countries, territories and areas, with approximately 60% of those cases reported from three countries: Italy, the Islamic Republic of Iran and Republic of Korea;
• Outside of mainland China, 2,199 deaths were reported by 35 countries, territories and areas; and
• The number of daily new cases reported in mainland China has continued to decrease as cases increase in other countries, territories and areas globally.

3 of 17 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.23) Epub 19/3/2020
Table 1: Cumulative notified cases of confirmed COVID-19 by jurisdiction, Australia, 2020 (n = 295)
Jurisdictiona
This weekb (19:00 AEDT 7 March to 14 March
2020) No. of new cases
Total casesb (to 19:00 AEDT 14 March 2020)
NSW 74 152
Vic 20 46
Qld 35 55
WA 6 14
SA 8 21
Tas 4 6
NT 0 0
ACT 1 1
Total cases 148 295
a NSW = New South Wales, Vic = Victoria, Qld = Queensland, WA = Western Australia, SA = South Australia, Tas = Tasmania, NT = Northern
Territory, ACT = Australian Capital Territory.
b Case totals for this report, and ongoing, use data in the NNDSS to ensure systematic management of information. There may be
differences in case numbers from last week due to changes in reporting methods for this report and future reports.
cases, 36% (n = 80) were hospitalised, 43% (n = 97) were not hospitalised, and hospitalisation status for 21% (n = 48) was unknown. The 60–64 age group reported the highest proportion of hospitalisation at 13% (n = 10), followed by the 30–34 and 35–39 age groups both reporting 11% (n = 9), and the 40–44 and 50–54 age groups both reporting 10% (n = 8).
Of the 295 confirmed cases, 53% (n = 156) reported symptoms (Table 2). A total of fifteen symptoms were reported with fever being the most commonly reported by 69% of cases (n = 108). Fifty-four percent (n = 84) reported cough, 46% (n = 72) reported sore throat, 35% (n = 55) reported shortness of breath, and 31% (n = 48) reported diarrhoea. Only 1% of all cases reported either joint pain, pneumonia or acute respiratory disease (ARD).
Of the 295 confirmed cases, 14% (n = 42) did not report place of acquisition and 2% (n = 5) reported overseas acquisition but with country unknown. Of the 248 cases with reported place of acquisition and country level data, 65% (n = 161) were overseas acquired. Table 3 shows the
most common places of acquisition for returned travellers were from countries in the European Region (n = 54), Region of the Americas (n = 39) and Western Pacific Region (n = 33). No place of acquisition was reported from the African Region. 4% of cases were acquired from the ‘Diamond Princess’ cruise ship under interna-tional conveyance.
Eighty-seven cases in Australia (35%) were locally acquired.

4 of 17 health.gov.au/cdiCommun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.23) Epub 19/3/2020
Figu
re 1:
Con
firm
ed ca
ses o
f CO
VID
-19
infe
ctio
n by
dat
e of i
llnes
s ons
et, A
ustr
alia
, 202
0 (n
= 2
95)a,
b
051015202530
12/01/2020
14/01/2020
16/01/2020
18/01/2020
20/01/2020
22/01/2020
24/01/2020
26/01/2020
28/01/2020
30/01/2020
1/02/2020
3/02/2020
5/02/2020
7/02/2020
9/02/2020
11/02/2020
13/02/2020
15/02/2020
17/02/2020
19/02/2020
21/02/2020
23/02/2020
25/02/2020
27/02/2020
29/02/2020
2/03/2020
4/03/2020
6/03/2020
8/03/2020
10/03/2020
12/03/2020
14/03/2020
Number of cases
Date
of i
llnes
s on
set
ACT
NSW
NT
QLD
SATA
SVI
CW
A
a D
iagn
osis
dat
e us
ed fo
r eig
ht c
ases
whe
re d
ate
of il
lnes
s on
set i
s un
avai
labl
e.b
Case
s as
soci
ated
with
the
Dia
mon
d Pr
ince
ss c
ruis
e sh
ip re
patr
iatio
n ar
e in
clud
ed w
ith th
eir r
espe
ctiv
e ju
risdi
ctio
ns.
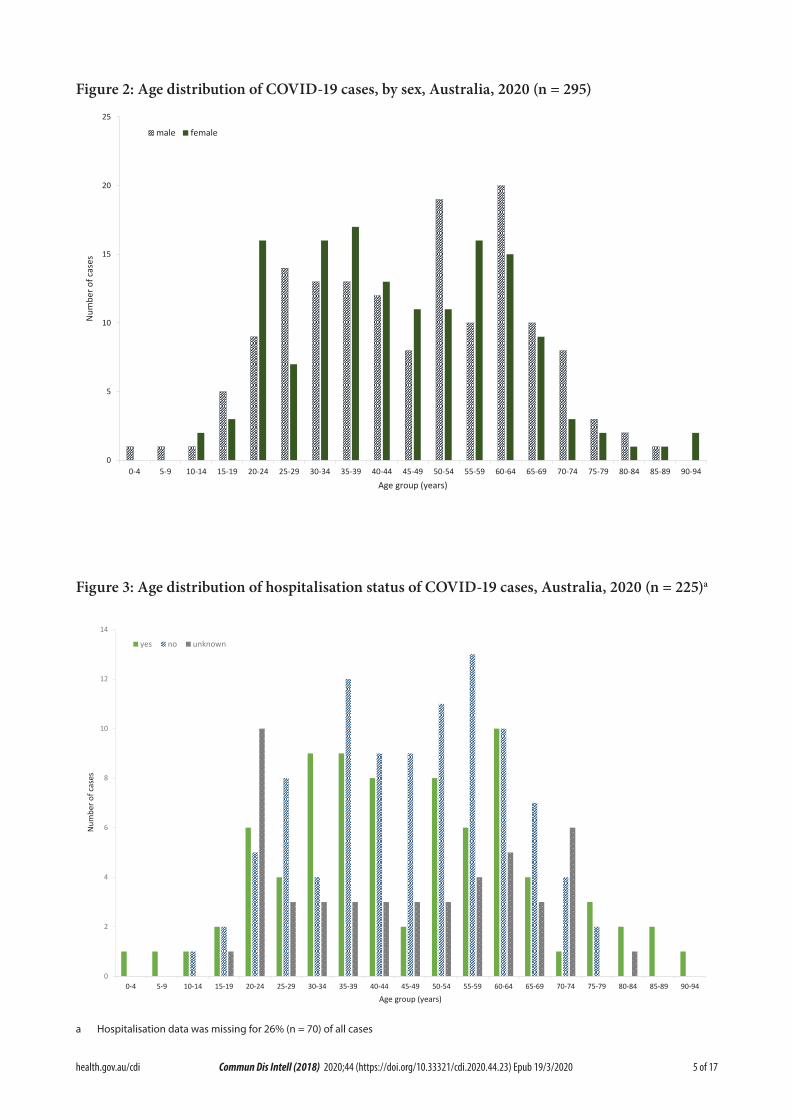
5 of 17 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.23) Epub 19/3/2020
Figure 2: Age distribution of COVID-19 cases, by sex, Australia, 2020 (n = 295)
0
5
10
15
20
25
0-4 5-9 10-14 15-19 20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74 75-79 80-84 85-89 90-94
Num
ber o
f cas
es
Age group (years)
male female
Figure 3: Age distribution of hospitalisation status of COVID-19 cases, Australia, 2020 (n = 225)a
0
2
4
6
8
10
12
14
0-4 5-9 10-14 15-19 20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74 75-79 80-84 85-89 90-94
Num
ber o
f cas
es
Age group (years)
yes no unknown
a Hospitalisation data was missing for 26% (n = 70) of all cases

6 of 17 health.gov.au/cdiCommun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.23) Epub 19/3/2020
Table 2: COVID-19 symptoms in confirmed cases in Australia, 2020 (n = 156)
Symptom n %
Fever 108 69%
Cough 84 54%
Sore throat 72 46%
Runny nose 62 40%
Shortness of breath 55 35%
Diarrhoea 48 31%
Nausea/vomiting 34 22%
Headache 31 20%
Irritability/confusion 27 17%
Muscular pain 22 14%
Chest pain 9 6%
Abdominal pain 6 4%
Joint pain 1 1%
Pneumonia 1 1%
Acute respiratory disease (ARD) 1 1%
Table 3: Place of acquisition of confirmed COVID-19 cases in Australia, by WHO regions, international conveyance, and local acquisition, 2020 (n = 248)a
WHO regions % n
European Region (EURO) 22% 54
Region of the Americas (PAHO) 16% 39
Western Pacific Region (WPRO) 13% 33
Eastern Mediterranean Region (EMRO) 6% 16
South-East Asia Region (SEARO) 4% 9
International conveyance 4% 10
African Region (AFRO) 0% 0
Locally acquired 35% 87
Total 100% 248
a Five cases that reported overseas travel to an unknown country are included as under investigation.

7 of 17 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.23) Epub 19/3/2020
Figu
re 4
. Cas
es o
f CO
VID
-19
repo
rted
to W
HO
; and
num
ber o
f cou
ntri
es, t
erri
tori
es a
nd a
reas
from
21
Janu
ary
to 1
4 M
arch
202
01
020406080100
120
140
160
0
2,00
0
4,00
0
6,00
0
8,00
0
10,0
00
12,0
00
20/01/2020
22/01/2020
24/01/2020
26/01/2020
28/01/2020
30/01/2020
01/02/2020
03/02/2020
05/02/2020
07/02/2020
09/02/2020
11/02/2020
13/02/2020
15/02/2020
17/02/2020
19/02/2020
21/02/2020
23/02/2020
25/02/2020
27/02/2020
29/02/2020
02/03/2020
04/03/2020
06/03/2020
08/03/2020
10/03/2020
12/03/2020
14/03/2020
Number of countries, territories and areas
Number of reported cases
Date
of r
epor
ting
Mai
nlan
d Ch
ina
Out
side
of m
ainl
and
Chin
aN
umbe
r of c
ount
ries,
terr
itorie
s
ab
c
a W
HO
dec
lare
s th
e ou
tbre
ak o
f CO
VID
-19
a Pu
blic
Hea
lth E
mer
genc
y of
Inte
rnat
iona
l Con
cern
(30/
01/2
020)
b W
HO
sta
rt re
port
ing
both
labo
rato
ry c
onfir
med
and
clin
ical
ly d
iagn
osed
cas
es fr
om H
ubei
Pro
vinc
e (1
7/02
/202
0)c
Hub
ei P
rovi
nce
ceas
e re
port
ing
clin
ical
ly d
iagn
osed
cas
es (2
0/02
/202
0)

8 of 17 health.gov.au/cdiCommun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.23) Epub 19/3/2020
International cases
As at 19:00 AEDT 14 March 2020, the number of confirmed COVID-19 cases reported to the World Health Organization (WHO) was 142,539 globally.1 The proportion of total cases reported from mainland China has continued to decrease, from 79% on 7 March 2020 to 57% (n = 81,021) on 14 March 2020.1,2 On 26 February 2020, the number of new cases reported outside of mainland China (n = 459) exceeded the num-ber reported from mainland China (n = 412) for the first time and this trend has continued to date (Figure 4). The total number of confirmed COVID-19 cases reported by 134 countries, ter-ritories and areas outside of mainland China in the current reporting week has increased almost threefold (n = 61,518) compared to the preced-ing week (n = 21,110).1,3 Italy reported 29% (n = 17,660) of all cases outside of mainland China; the Islamic Republic of Iran reported 18% (n = 11,364); the Republic of Korea reported 13% (n = 8,086) and Spain reported 7% (n = 4,231). Thirty-eight countries, territories and areas reported cases of COVID-19 for the first time in the past seven days. Of all the countries, territories and areas outside of mainland China with known transmission classification (n = 134), fifty-eight percent (n = 78) have reported local transmis-sion of COVID-19.
Globally, 5,393 deaths have been reported, with 57% (n = 3,075) reported from Hubei Province, China and 119 deaths reported from elsewhere within mainland China. The remaining 2,199 deaths were reported by 35 countries, territories and areas outside of mainland China.1
The current estimates on epidemiological param-eters including severity, transmissibility and incubation period are uncertain. Estimates are likely to change as more information becomes available.
Country in focus: Italy
Data on confirmed cases of COVID-19 in Italy have not been made publicly available. The following is therefore a brief summary based on information obtained from WHO situation reports and the Italian Ministry of Health.
Italy reported its first two confirmed cases of COVID-19 on 31 January 2020.4 Cases increased rapidly with 6 new cases reported on 22 February 2020 up to 17,660 cases on 14 March 2020. Reported deaths increased more than sixfold (n = 197) on 7 March to 1268 on 14 March 2020.1,2 Among the cases reported as at 14 March 2020, 51% (n = 9,059) were reported in Lombardia, 13% (n = 2,349) in Emilia Romagna and 10% (n = 1,775) in Veneto.5 Italy is now the epicentre outside of mainland China with the most rapid growth of COVID-19 cases, surpass-ing the Republic of Korea and the Islamic Republic of Iran (Figure 5).
Based on confirmed cases up to 14 March 2020, the case fatality rate (CFR) for Italy has been calculated at 7.8%. As the out-break continues, the confirmed CFR may change. The current calculated CFR does not include the number of cases with mild infections that may be missed from current surveillance, nor does it account for the recently confirmed cases that may subse-quently develop severe disease and die.
On 9 March 2020, Italy became the first European country to place a nationwide travel ban from all travel unless certi-fied as justified on professional or health grounds.6 The nationwide restrictions will be in effect until 3 April 2020. On 11 March 2020, the Italian Prime Minister imposed new restrictions by closing non-essential commercial activities in the country, with the exception of basic necessities and phar-macies. The new restrictions will be valid for two weeks.7

9 of 17 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.23) Epub 19/3/2020
Figu
re 5:
Num
ber o
f CO
VID
-19
case
s by c
ount
ry an
d da
ys si
nce p
assin
g 100
case
s, up
to 14
Mar
ch 2
020
7755
7869
7979
8086
1059
0
1246
2
1511
3
1766
0
8042
9000
1007
5
1136
4
0
2,00
0
4,00
0
6,00
0
8,00
0
10,0
00
12,0
00
14,0
00
16,0
00
18,0
00
20,0
00
01
23
45
67
89
1011
1213
1415
1617
1819
2021
2223
Total number of confirmed cases
Day
s sin
ce p
assin
g 10
0 ca
ses
Repu
blic
of K
orea
Italy
Isla
mic
Rep
ublic
of I
ran

10 of 17 health.gov.au/cdiCommun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.23) Epub 19/3/2020
Transmission
Human-to-human transmission of SARS-CoV-2 is via droplets and fomites from an infected per-son to a close contact.8 A study of cases and their close contacts in China supports this. Household contacts and those who travelled with a con-firmed COVID-19 case were strongly associated with an increased risk of infection.9 The study also examined the average time from symptom onset to disease confirmation among cases who were identified through symptom-based surveil-lance (i.e. symptomatic screening at airports, community fever monitoring and testing of hos-pital patients) and contact-based surveillance (i.e. monitoring and testing of close contacts of confirmed COVID-19 cases). Compared to cases identified through symptom-based surveillance, cases identified through contact-based surveil-lance were associated with a 2.3 day decrease from symptom onset to disease confirmation, and a 1.9 day decrease from symptom onset to isolation. Based on modelling, researchers have found that effective contact tracing increases the probability of control.9 A virological analysis of nine hospitalised cases found proof of active virus replication in upper respiratory tract tis-sues, with pharyngeal virus shedding very high during the first week of symptoms.10 COVID-19 can often present as a common cold-like illness where the virus is shed for a prolonged time after symptoms end, including in stools.10 This may have implications for current case definitions and re-evaluation of the prospects of outbreak containment.10
Current evidence does not support airborne or faecal-oral spread as major factors in transmis-sion.8
Incubation period
Estimates of median incubation period, based on seven published studies, are 5 to 6 days (ranging from 0 to 14 days).11 Patients with long incubation periods do occasionally occur and have been reported, however medical experts
have described these patients as ‘outliers’ who should be studied further and do not represent a significant shift in thinking about the virus.11
Clinical features
Ongoing evidence, including a recently pub-lished meta-analysis, supports previous research that COVID-19 presents as mild illness in the majority of cases with fever and cough being the most commonly reported symptoms. Severe or fatal outcomes tend to occur in the elderly or those with comorbid conditions.8,12 Some COVID-19 patients show neurological signs such as headache, nausea and vomiting. A study identified increasing evidence that coronavi-ruses are not always confined to the respiratory tract and may also invade the central nervous system inducing neurological symptoms.13 As such, it is likely that the potential invasion of SARS-CoV2 to the central nervous system is partially responsible for the acute respiratory failure of COVID-19 patients.13 Examination of cases and their close contacts in China found a positive association between age and time from symptom onset to recovery. Median time to recovery was estimated to be 27 days in 20–29 year olds, 32 days in 50–59 year olds, and 36 days in those aged over 70 years. The study also found an association between clinical sever-ity and time from symptom onset to time to recovery. Compared to people with mild disease, those with moderate and severe disease were associated with a 19% and 58% increase in time to recovery, respectively.9 A retrospective cohort study looking at risk factors for mortality among patients with COVID-19 who have experienced a definite outcome found an increase in the odds of in-hospital death associated with older age, higher sequential organ failure assessment score and elevated blood d-dimer levels on admis-sion.14 Detectable SARS-CoV-2 RNA persisted for a median of 20 days in survivors and sus-tained until death in non-survivors.14
Molecular epidemiology
Based on modelling, researchers estimated that initial human SARS-CoV-2 infection was in

11 of 17 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.23) Epub 19/3/2020
November to early December 2019.15 An analysis based on 86 genomic sequences of SARS-CoV-2, obtained from the Global Initiative on Sharing All Influenza Data (GISAID), found many muta-tions.16 This suggests that SARS-CoV-2 will con-tinue to evolve as the outbreak occurs. Ongoing surveillance of sequences and shared mutations will assist with understanding the spread of the virus globally and within Australia.
Treatment
Current clinical management of COVID-19 cases focuses on early recognition, isolation, appropriate infection control measures and provision of supportive care.17 Whilst there is no specific antiviral treatment currently recom-mended for patients with suspected or confirmed SARS-CoV-2 infection, multiple clinical trials are underway to evaluate a number of thera-peutic agents, including remdesivir, lopinavir/ritonavir, and chloroquine.18
Comparison between COVID-19, SARS and MERS
Coronaviruses are a group of viruses that can cause upper respiratory tract infections in humans. Coronaviruses can occasionally cause severe diseases such as Middle East Respiratory Syndrome (MERS), Severe Acute Respiratory Syndrome (SARS) and more recently COVID-19. Similar to MERS-CoV and SARS-CoV, SARS-CoV-2 is thought to have originated from bats, and to have been transmitted to humans via an intermediate animal host. The intermediate ani-mal host responsible for COVID-19 is currently unknown.19 Table 4 provides an overview of characteristics of COVID-19, MERS and SARS.
Public health response
The Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19) describes some of the key aspects associated with the evolving outbreak in mainland China, includ-ing transmission dynamics, disease progression and severity, mainland China’s response and knowledge gaps. As part of the report, the fol-
lowing major recommendations were made for countries with imported cases and/or outbreaks of COVID-19:8
1. Immediately activate the highest level of national Response Management protocols to ensure the all-of-government and all-of-so-ciety approach needed to contain COVID-19 with non-pharmaceutical public health measures;
2. Prioritise active, exhaustive case finding and immediate testing and isolation, painstaking contact tracing and rigorous quarantine of close contacts;
3. Fully educate the general public on the seriousness of COVID-19 and their role in preventing its spread;
4. Immediately expand surveillance to detect COVID-19 transmission chains, by test-ing all patients with atypical pneumonias, conducting screening in some patients with upper respiratory illnesses and/or recent COVID-19 exposure, and adding testing for the COVID-19 virus to existing surveillance systems (e.g. systems for influenza-like-illness); and
5. Conduct multi-sector scenario planning and simulations for the deployment of even more stringent measures to interrupt transmis-sion chains as needed (e.g. the suspension of large-scale gatherings and the closure of schools and workplaces).

12 of 17 health.gov.au/cdiCommun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.23) Epub 19/3/2020
Tabl
e 4:
Cha
ract
eris
tics o
f CO
VID
-19,
MER
S an
d SA
RS20
–22
COV
ID-1
9M
ERS
SARS
Med
ian
incu
batio
n pe
riod
5–6
days
5 da
ys4–
5 da
ys
Mod
e of
tran
smis
sion
Resp
irato
ry d
ropl
et, c
lose
con
tact
, fom
ites
Resp
irato
ry d
ropl
et, c
lose
con
tact
Resp
irato
ry d
ropl
et, c
lose
con
tact
, fom
ites
Sym
ptom
sFe
ver,
coug
h, fa
tigue
and
diffi
culty
with
br
eath
ing
(dys
pnoe
a)Fe
ver,
coug
h an
d sh
ortn
ess
of b
reat
hFe
ver,
mal
aise
, mya
lgia
, hea
dach
e, d
iarr
hoea
an
d sh
iver
ing
(rigo
rs)
Num
ber o
f cou
ntrie
s an
d re
gion
s aff
ecte
d13
427
29
Regi
ons
seve
rely
affe
cted
Mai
nlan
d Ch
ina,
Rep
ublic
of K
orea
, Ita
ly a
nd
Isla
mic
Rep
ublic
of I
ran
Saud
i Ara
bia
Mai
nlan
d Ch
ina,
Hon
g Ko
ng S
AR,
Tai
wan
, Ca
nada
, Sin
gapo
re
Num
ber o
f cas
es g
loba
lly14
2,53
92,
519
8,42
2
Num
ber o
f dea
ths
glob
ally
5,39
386
691
6
Glo
bal c
ase
fata
lity
rate
3.8%
34.3
%10
.9%
Prop
hyla
xis
avai
labl
eN
oN
oN
o

13 of 17 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.23) Epub 19/3/2020
Background
On 31 December 2019, the World Health Organization (WHO) was notified about a large number of cases of pneumonia of unknown origin in Wuhan City, Hubei Province, China. Chinese authorities isolated and identified a novel coronavirus on 7 January 2020.23 WHO declared the outbreak of COVID-19 a Public Health Emergency of International Concern (PHEIC) on 30 January 2020.8
From 1 February 2020, Australia denied entry to anyone who had left or transited through main-land China, with the exception of Australian citizens, permanent residents and their imme-diate family and air crew who have been using appropriate personal protective equipment (Figure 4).24 The Australian Health Protection Principal Committee (AHPPC) have reviewed these restrictions weekly, and on 4 March 2020, they released a statement recommending cur-rent travel restrictions for mainland China and the Islamic Republic of Iran remain in place for a further seven days.25 On 5 March 2020, the Prime Minister announced new travel restric-tions for travellers coming from the Republic of Korea, and implementation of enhanced health screening for arrivals from Italy. From 5 March 2020, foreign nationals (excluding permanent residents of Australia) will be prevented from coming to Australia until 14 days after leav-ing the Republic of Korea.26 On 8 March 2020, AHPPC recommended that people who have been a close contact of a confirmed COVID-19 case, or who returned from or transited through a listed higher risk country*, must not attend public gatherings until 14 days after leaving the country or having contact with a confirmed case even if they are completely symptom free.27 Those undergoing COVID-19 testing also must not attend public gatherings until they have received their result.27 On March 11, AHPPC recommended that the government continue to direct primary focus toward domestic contain-ment and preparedness of COVID-19, and that enhanced border measures and travel restric-tions be maintained for a further 7 days.28 On March 12, AHPPC provided recommendations
on testing and work restriction for health and aged care workers. In addition to the other sus-pect case criteria, AHPPC recommended testing for any health care worker (HCW) who provides direct care AND who has a fever (> 37.5 ° C) AND an acute respiratory infection (e.g. shortness of breath, cough, coryza, and/or sore throat), are classified as a suspect case and should be tested for COVID-19. Recommendations for exclusion from work for HCW were also provided.29 On 13 March, AHPPC provided recommendations for public gatherings and testing by putting in place social distancing measures to mitigate spread.30 This includes:
• Limiting non-essential organised gatherings to fewer than 500 people;
• Limiting non-essential meetings or confer-ences of critical workforce e.g. healthcare professionals and emergency services;
• Encouraging all Australians to exercise personal responsibility for social distancing measures; and
• Initiating measures to protect vulnerable populations, such as reducing visitors to all residential care facilities and remote Aborigi-nal and Torres Strait Islander communities.
AHPPC acknowledges that diagnostic testing issues are related to an emerging global short-age and are reviewing the case definition. The current situation emphasises the need for testing to be limited to the current recommendations.30
AHPPC acknowledged that Australia’s border measures may no longer be able to prevent the importation of COVID-19, and the primary focus should now be directed at domestic con-tainment and preparedness.24 Local transmis-sion of COVID-19 has occurred in Australia, highlighting the need of effective containment measures to limit spread. Early isolation of iden-tified cases and quarantine of suspected cases and close contacts is a key measure to minimise transmission of COVID-19 in the community.

14 of 17 health.gov.au/cdiCommun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.23) Epub 19/3/2020
Table 5: Australian COVID-19 case definition as of 14 March 202031
Version Date of development Suspect Case Confirmed Case
1.18 13 March 2020 A. If the patient satisfies epidemiological and clinical criteria, they are classified as a suspect case. Epidemiological criteria• International travel in the 14 days before illness onset.OR• Close contact in 14 days before illness onset with a
confirmed case of COVID-19.Clinical criteria• FeverOR• Acute respiratory infection (e.g. shortness of breath,
cough, sore throat) with or without fever. B. If the patient has severe community-acquired pneumonia (critically ill) and no other cause is identified, with or without recent international travel, they are classified as a suspect case. C. If any healthcare worker with direct patient contact has a fever (≥ 37.5°C) AND an acute respiratory infection (e.g. shortness of breath, cough, sore throat), they are classified as a suspect case.
A person who tests positive to a validated specific SARS-CoV-2 nucleic acid test or has the virus identified by electron microscopy or viral culture.
However, as COVID-19 presents as mild illness in the majority of cases, early identification and isolation of cases may be difficult to achieve.
Methods
Data for this report were current as at 19:00 hours AEDT, 14 March 2020.
This report outlines what is known epidemio-logically on COVID-19 in Australia and from publicly available data from WHO Situation Reports, other countries’ official updates and the scientific literature. Data on domestic cases in this report were collected from the National Notifiable Diseases Surveillance System (NNDSS) and jurisdictional health department media releases. The Communicable Diseases Network Australia (CDNA) developed the case definition for suspect and confirmed cases, which was modified at different time points during the outbreak (Table 5). Data were ana-lysed using Stata to describe the epidemiology of COVID-19 in Australia and the progress of the epidemic.
Data for the international cases of COVID-19 by country were compiled from the latest WHO Situation Report. Case definitions may vary by country making comparisons difficult. Rapid reviews of the current state of knowledge on COVID-19 were conducted from the literature using PubMed.
Acknowledgements
This report represents surveillance data reported through CDNA as part of the nationally-coordi-nated response to COVID-19. We thank public health staff from incident emergency operations centres in state and territory health departments, and the Australian Government Department of Health, along with state and territory public health laboratories.

15 of 17 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.23) Epub 19/3/2020
Author details
Corresponding author
Malinda V Chea
NIR Surveillance Team, Communicable Disease Epidemiology and Surveillance Section, Health Protection Policy Branch, Australian Government Department of Health, GPO Box 9484, MDP 14, Canberra, ACT 2601.
Email: [email protected]
References
1. World Health Organization (WHO). Coro-navirus disease 2019 (COVID-19) situa-tion report – 54: 14 March 2020. Geneva: WHO; 2020. [Accessed on 15 March 2020.] Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200314-sitrep-54-covid-19.pdf.
2. WHO. Coronavirus disease 2019 (COV-ID-19) situation report – 47: 07 March 2020. Geneva: WHO; 2020. [Accessed on 15 March 2020.] Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200307-sitrep-47-covid-19.pdf.
3. WHO. Coronavirus disease 2019 (COV-ID-19) situation report – 40: 29 February 2020. Geneva: WHO; 2020. [Accessed on 15 March 2020.] Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200229-sitrep-40-cov-id-19.pdf.
4. WHO. Novel Coronavirus (2019-nCoV) situ-ation report – 11: 31 January 2020. Geneva: WHO; 2020. [Accessed on 15 March 2020.] Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200131-sitrep-11-ncov.pdf.
5. Ministry of Health. COVID-19 cases in Italy at 6 pm on March 14th. [Internet.] Rome: Ital-ian Government Ministry of Health; 2020.
[Accessed on 15 March 2020.] Available from: http://www.salute.gov.it/imgs/C_17_pagineAree_5351_12_file.pdf.
6. Ministry of Health. COVID-19 COVID-19, closed cinemas, pubs, discos throughout Italy. [Internet.] Rome: Italian Government Ministry of Health; 2020. [Accessed on 12 March 2020.] Available from: http://www.salute.gov.it/portale/news/p3_2_1_1_1.jsp?lingua=italiano&menu=notizie&p=dalministero&id=4175.
7. Ministry of Health. COVID-19, close non-essential commercial activities. [Internet.] Rome: Italian Government Ministry of Health; 2020. [Accessed on 12 March 2020.] Available from: http://www.salute.gov.it/por-tale/news/p3_2_1_1_1.jsp?lingua=italiano&menu=notizie&p=dalministero&id=4212.
8. WHO. Report of the WHO-China joint mission on coronavirus disease 2019 (COV-ID-19). Geneva: WHO; 2020. [Accessed on 1 March 2020.] Available from: https://www.who.int/docs/default-source/coronaviruse/who-china-joint-mission-on-covid-19-final-report.pdf.
9. Bi Q, Wu Y, Mei S, Ye C, Zou X, Zhang Z et al. Epidemiology and transmission of COVID-19 in Shenzhen China: analysis of 391 cases and 1286 of their close contacts. medRxiv. 2020. doi: https://doi.org/10.1101/2020.03.03.20028423.
10. Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z et al. Clinical course and risk factors for mor-tality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020. doi: https://doi.org/10.1016/S0140-6736(20)30566-3.
11. WHO. Coronavirus disease 2019 (COV-ID-19) situation report – 29: 18 February 2020. Geneva: WHO; 2020. [Accessed on 15 March 2020.] Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200218-sitrep-29-cov-

16 of 17 health.gov.au/cdiCommun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.23) Epub 19/3/2020
id-19.pdf.
12. Sun P, Qie S, Liu Z, Ren J, Xi JJ. Clinical characteristics of 50466 patients with 2019-nCoV infection. medRxiv. 2020. doi: https://doi.org/10.1101/2020.02.18.20024539.
13. Li Y, Bai W, Hashikawa T. The neuroinvasive potential of SARS-CoV2 may be at least par-tially responsible for the respiratory failure of COVID-19 patients. J. Med. Virol. 2020. doi: https://doi.org/10.1002/jmv.25728.
14. Woelfel R, Corman VM, Guggemos W, Seil-maier M, Zange S, Mueller MA et al. Clini-cal presentation and virological assessment of hospitalized cases of coronavirus disease 2019 in a travel-associated transmission clus-ter. medRxiv. 2020. doi: https://doi.org/10.1101/2020.03.05.20030502.
15. Bedford T, Neher R, Hadfield J, Hodcroft E, Ilcisin M, Müller N. Genomic analysis of nCOV spread. Situation report 2020-01-30. [Internet.] 2020. Available from: https://nextstrain.org/narratives/ncov/sit-rep/2020-01-30.
16. Phan T. Genetic diversity and evolu-tion of SARS-CoV-2. Infect Genet Evol. 2020. doi: https://doi.org/10.1016/j.meegid.2020.104260.
17. WHO. Clinical management of severe acute respiratory infection when novel coronavirus (nCoV) infection is suspected. [Internet.] Geneva: WHO; 2020. [Accessed on 23 Febru-ary 2020.] Available from: https://www.who.int/publications-detail/clinical-management-of-severe-acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-sus-pected.
18. Harrison, C. Coronavirus puts drug re-purposing on the fast track. Nat Biotechnol. 2020. doi: https://doi.org/10.1038/d41587-020-00003-1.
19. WHO. Novel coronavirus (2019-nCoV)
situation report – 22: 11 February 2020. Ge-neva: WHO; 2020. [Accessed on 12 February 2020.] Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200211-sitrep-22-ncov.pdf.
20. World Health Organization Regional Of-fice for the Eastern Mediterranean. MERS situation update, January 2020. [Internet.] Egypt: World Health Organization Regional Office for the Eastern Mediterranean; 2020. [Accessed on 7 March 2020.] Available from: http://www.emro.who.int/pandemic-epidem-ic-diseases/mers-cov/mers-situation-update-january-2020.html.
21. Centers for Disease Control and Prevention (CDC). MERS clinical features. [Internet.] Atlanta: United States Department of Health and Human Services, CDC; 2019. [Accessed on 7 March 2020.] Available from: https://www.cdc.gov/coronavirus/mers/clinical-features.html.
22. WHO. Consensus document on the epi-demiology of severe acute respiratory syn-drome (SARS). [Internet.] Geneva: WHO; 2003. [Accessed on 7 March 2020.] Available from: https://www.who.int/csr/sars/WHOc-onsensus.pdf.
23. WHO. Novel coronavirus (2019-nCoV) situation report – 1: 21 January 2020. Ge-neva: WHO; 2020. [Accessed on 22 January 2020.] Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200121-sitrep-1-2019-ncov.pdf.
24. Australian Government Department of Health. Australian Health Protection Princi-pal Committee (AHPPC) novel coronavirus statement on 1 February 2020. [Internet.] Canberra: Australian Government Depart-ment of Health; 2020. [Accessed on 7 Feb-ruary 2020.] Available from: https://www.health.gov.au/news/australian-health-protec-tion-principal-committee-ahppc-novel-coro-navirus-statement-on-1-february-2020.

17 of 17 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.23) Epub 19/3/2020
25. Australian Government Department of Health. Australian Health Protection Prin-cipal Committee (AHPPC) coronavirus (COVID-19) statement on 4 March 2020. [Internet.] Canberra: Australian Government Department of Health; 2020. [Accessed on 7 March 2020.] Available from: https://www.health.gov.au/news/australian-health-protec-tion-principal-committee-ahppc-coronavi-rus-covid-19-statement-on-4-march-2020
26. Australian Government Department of the Prime Minister and Cabinet. Update on novel coronavirus (COVID-19) in Australia. [Internet.] Canberra: Australian Govern-ment Department of the Prime Minister and Cabinet; 2020. [Accessed on 7 March 2020.] Available from: https://www.pm.gov.au/media/update-novel-coronavirus-covid-19-australia-0.
27. Australian Government Department of Health. Australian Health Protection Prin-cipal Committee (AHPPC) coronavirus (COVID-19) statement on 8 March 2020. [Internet.] Canberra: Australian Government Department of Health; 2020. [Accessed on 11 March 2020.] Available from: https://www.health.gov.au/news/australian-health-protec-tion-principal-committee-ahppc-coronavi-rus-covid-19-statement-on-8-march-2020.
28. Australian Government Department of Health. Australian Health Protection Prin-cipal Committee (AHPPC) coronavirus (COVID-19) statement on 11 March 2020. [Internet.] Canberra: Australian Government Department of Health; 2020. [Accessed on 13 March 2020.] Available from: https://www.health.gov.au/news/australian-health-protec-tion-principal-committee-ahppc-coronavi-rus-covid-19-statement-on-11-march-2020.
29. Australian Government Department of Health. Australian Health Protection Prin-cipal Committee (AHPPC) coronavirus (COVID-19) statement on 12 March 2020. [Internet.] Canberra: Australian Government Department of Health; 2020. [Accessed on 15
March 2020.] Available from: https://www.health.gov.au/news/australian-health-protec-tion-principal-committee-ahppc-coronavi-rus-covid-19-statement-on-12-march-2020.
30. Australian Government Department of Health. Australian Health Protection Prin-cipal Committee (AHPPC) coronavirus (COVID-19) statement on 13 March 2020. [Internet.] Canberra: Australian Government Department of Health; 2020. [Accessed on 15 March 2020.] Available from: https://www.health.gov.au/news/australian-health-protec-tion-principal-committee-ahppc-coronavi-rus-covid-19-statement-on-13-march-2020.
31. Australian Government Department of Health. Novel coronavirus 2019 (2019-nCoV) - CDNA national guidelines for public health units. [Internet.] Canberra: Australian Government Department of Health; 2020. [Accessed on 15 March 2020.] Available from: https://www1.health.gov.au/internet/main/publishing.nsf/Content/7A8654A8CB144F5FCA2584F8001F91E2/$File/interim-COVID-19-SoNG-v2.0.pdf.

2 0 2 0 V o l u m e 4 4https://doi.org/10.33321/cdi.2020.44.28
COVID-19, Australia: Epidemiology Report 8:Reporting period from 19:00 AEDT 14 March to 23:59 AEDT 22 March 2020
COVID-19 National Incident Room Surveillance Team

Communicable Diseases Intelligence ISSN: 2209-6051 Online
This journal is indexed by Index Medicus and Medline.
Creative Commons Licence - Attribution-NonCommercial-NoDerivatives CC BY-NC-ND
© 2020 Commonwealth of Australia as represented by the Department of Health
This publication is licensed under a Creative Commons Attribution- Non-Commercial NoDerivatives 4.0 International Licence from https://creativecommons.org/licenses/by-nc-nd/4.0/legalcode (Licence). You must read and understand the Licence before using any material from this publication.
Restrictions The Licence does not cover, and there is no permission given for, use of any of the following material found in this publication (if any):
• the Commonwealth Coat of Arms (by way of information, the terms under which the Coat of Arms may be used can be found at www.itsanhonour.gov.au);
• any logos (including the Department of Health’s logo) and trademarks;
• any photographs and images;
• any signatures; and
• any material belonging to third parties.
Disclaimer Opinions expressed in Communicable Diseases Intelligence are those of the authors and not necessarily those of the Australian Government Department of Health or the Communicable Diseases Network Australia. Data may be subject to revision.
Enquiries Enquiries regarding any other use of this publication should be addressed to the Communication Branch, Department of Health, GPO Box 9848, Canberra ACT 2601, or via e-mail to: [email protected]
Communicable Diseases Network Australia Communicable Diseases Intelligence contributes to the work of the Communicable Diseases Network Australia. http://www.health.gov.au/cdna
Communicable Diseases Intelligence (CDI) is a peer-reviewed scientific journal published by the Office of Health Protection, Department of Health. The journal aims to disseminate information on the epidemiology, surveillance, prevention and control of communicable diseases of relevance to Australia.
Editor Tanja Farmer
Deputy Editor Simon Petrie
Design and Production Kasra Yousefi
Editorial Advisory Board David Durrheim, Mark Ferson, John Kaldor, Martyn Kirk and Linda Selvey
Website http://www.health.gov.au/cdi
Contacts Communicable Diseases Intelligence is produced by: Health Protection Policy Branch Office of Health Protection Australian Government Department of Health GPO Box 9848, (MDP 6) CANBERRA ACT 2601
Email: [email protected]
Submit an Article You are invited to submit your next communicable disease related article to the Communicable Diseases Intelligence (CDI) for consideration. More information regarding CDI can be found at: http://health.gov.au/cdi.
Further enquiries should be directed to: [email protected].
1 of 19 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.28) Epub 27/03/2020
Weekly epidemiological report
COVID-19, Australia: Epidemiology Report 8:Reporting period from 19:00 AEDT 14 March to 23:59 AEDT 22 March 2020
COVID-19 National Incident Room Surveillance Team
Erratum: An error occurred in Figure 1 (Confirmed cases of COVID-19 infection, Australia, by date of illness onset) as originally published, which
inadvertently transposed the numbers of reported cases for Western Australia and Victoria. This has now been amended.
Summary
This is the eighth epidemiological report for coronavirus disease 2019 (COVID-19), reported in Australia as at 23:59 Australian Eastern Daylight Time [AEDT] 22 March 2020. It includes data on COVID-19 cases diagnosed in Australia, the international situation and a review of current evidence.
Keywords: SARS-CoV-2; novel coronavirus; 2019-nCoV; coronavirus disease 2019; COVID-19; acute respiratory disease; case definition; epidemiology; Australia
The following epidemiological data are subject to change both domestically and internationally due to the rapidly evolving situation. Australian cases are still under active investigation. While every effort has been made to standardise the investigation of cases nationally, there may be some differences between jurisdictions.
Australian situation
As at 23:59 AEDT 22 March 2020, there were 1,765 confirmed cases, including seven deaths, in Australia, reported to the National Notifiable Diseases Surveillance System (NNDSS)i (Table 1, Figure 1). Of the 1,765 confirmed cases, 43% (n = 766) were reported in NSW, 21% (n = 362) from Qld, 18% (n = 313) from Vic, 8% (n = 137) from SA, 7% (n = 130) from WA, 2% (n = 32) from ACT, 1% (n = 21) from Tas, and 0.2% (n = 4) from NT (Figure 2). The rate of cases in Australia per 100,000 population was 7.0; this varied across jurisdictions with NSW 9.5, SA 7.8, ACT 7.5, Qld 7.1, WA 5.0, Vic 4.8, Tas 3.9 and NT 1.6. Of the cases with a usual residence
i Data were extracted on 24 March 2020 with data reported
to 22 March 2020. Due to the dynamic nature of the NNDSS,
data in this extract are subject to retrospective revision and
may vary from data published in previous reports and reports
of notification data by states and territories.
in Australia, most cases are reported to reside within major metropolitan areas, with a small number of cases reported outside these areas (Figure 2).
During the current reporting period a total of 1,143 cases were reported. NSW (38%) reported the largest number of new cases, followed by Queensland (24%).
The median age of all 1,795 reported Australian cases was 48 years (range 0–94 years), with the highest proportion of cases aged between 20–29 and 60–69 years (Figure 3). Confirmed case rates within a given age cohort were highest for both males and females aged 60–69 years (Figure 4). There continue to be very few cases reported among children. The male-to-female ratio was approximately 1:1 overall.
Of the 1,765 confirmed cases, 51% (n = 907) had data on symptoms. Of the symptoms reported, cough (69%; n=628) was the most common.

2 of 19 health.gov.au/cdiCommun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.28) Epub 27/03/2020
In Australia:
• There have been 1,765 confirmed cases, including seven deaths, reported in Australia as at 23:59 AEDT 22 March 2020. Of confirmed cases, 43% were reported from NSW, 21% from Qld, 18% from Vic, 8% from SA, 7% from WA, 2% from ACT, 1% from Tas, and 0.2% from NT;
• Sixty-five percent of the total number of reported cases so far have been during the current reporting period;
• Hospitalisation status was recorded for 717 cases, of which 26% (n = 190) were reported to have been hospitalised due to their COVID-19 infection. Of these hospitalised cases, ICU (Intensive Care Unit) status was recorded for 87 cases, of which 20% (n = 17) were were ad-mitted to an ICU, with two cases requiring ventilation; and
• Virus genome sequences currently available from Australian cases indicate introductions from China, Iran, Europe and the USA, reflecting global diversity of SARS-COV-2 and cor-roborating field epidemiology.
Internationally:
• 292,142 infections have been confirmed globally, with 12,784 deaths;
• Cases have so far been reported in 175 countries, territories and areas globally;
• So far, the largest number of confirmed infections (29%; n = 81,498) within any country has been reported in mainland China, with the largest number of deaths (38%; n = 4,827) in Italy;
• The number of daily new cases reported in mainland China has continued to decrease. Cases have continued to increase in other countries, territories and areas globally, with the greatest increases currently occurring in the European Region; and
• Approximately 52% (n = 151,293) of all cases have been reported from the European Region, predominately from Italy, Spain, Germany and France.

3 of 19 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.28) Epub 27/03/2020
Fifty percent (n = 454) reported fever, 46% (n = 415) reported sore throat, 36% (n = 329) reported headache, and 28% (n = 251) reported muscular pain. Only 2% or fewer of all cases reported either abdominal pain, pneumonia or acute respiratory disease (ARD). An analysis of symptom combinations highlights that cough is the predominant clinical presentation in combi-nation with fever and/or sore throat (Figure 5).
Hospitalisation status was recorded for 717 cases of which 26% (n = 190) were reported to have been hospitalised due to their COVID-19 infec-tion. Of these hospitalised cases, ICU (Intensive Care Unit) status was recorded for 87 cases of which 20% (n = 17) were recorded being admit-ted to an ICU, with two cases requiring ventila-tion.
Seven COVID-19 deaths were confirmed in Australia up to 22 March 2020. The median age of deceased individuals was 81 years (range 78 to 94 years). Three of these deaths were from an aged care facility, one was associated with a cruise ship repatriation and the other three cases were acquired in the community. Three of the cases were male and four were female. The period between the date of illness onset and death ranged from 0 to 12 days.
Of cases with a reported place of acquisition (1,281 of 1,765), sixty-eight percent (n = 872) had a recent international travel history and 32% (n = 409) were locally acquired (Figure 6). The majority of recent overseas acquired cases reported a travel history to the European Region or the Americas Region. Of the locally acquired cases the majority were considered to be con-tacts of a confirmed case, with a very small number of cases not able to be epidemiologically linked to a confirmed case. For the remainder of cases where a place of acquisition has not been reported, these cases are currently under public health investigation.
Virus genome sequences currently available from Australian cases indicate introductions from China, the Islamic Republic of Iran, Europe
and the USA, reflecting the global diversity of SARS-COV-2 and corroborating field epidemi-ology (Figure 7).
International situation
As at 23:59 AEDT 22 March 2020, the number of confirmed COVID-19 cases reported to the World Health Organization (WHO) was 292,142 globally.1 The proportion of total cases reported from mainland China has continued to decrease, from 57% on 14 March, to 29% on 22 March 2020.1,2
The number of new cases reported outside of mainland China has continued or rapidly increase. The total number of confirmed COVID-19 cases reported by 174 countries, ter-ritories and areas outside mainland China in the current reporting week has increased more than threefold (n = 210,644) compared to the preced-ing week (n = 61,518).1,2 Italy reported 25% (n = 53,578) of all cases outside of mainland China; Spain reported 12% (n = 24,926); Germany reported 10% (n = 21,463); the US reported 7% (n = 15,219); and the Islamic Republic of Iran reported 5% (n = 10,610). Forty countries, ter-ritories and areas reported cases of COVID-19 for the first time in the past seven days. Of all the countries, territories and areas outside of mainland China with known transmission clas-sification (n = 174), 59% (n = 103) have reported local transmission of COVID-19.
Globally, there are very different epidem-ics occurring in different countries, with the trajectories of different countries’ outbreaks after their first 100 cases showing remarkable variation. Figure 8 highlights that for a number of countries outside of mainland China which have reported more than 100 cases, their rates of increase continue to be quite substantial, particularly Italy, Spain and the United States of America. For several other countries or regions including Singapore, Japan and Hong Kong there continues to be a slow rate of increase in their number of new cases, with the Republic of Korea reporting very few new cases each day.

4 of 19 health.gov.au/cdiCommun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.28) Epub 27/03/2020
Figu
re 1
: Con
firm
ed c
ases
of C
OV
ID-1
9 in
fect
ion,
Aus
tral
ia, b
y da
te o
f illn
ess o
nset
a
050100
150
200
250
12-Jan-20
14-Jan-20
16-Jan-20
18-Jan-20
20-Jan-20
22-Jan-20
24-Jan-20
26-Jan-20
28-Jan-20
30-Jan-20
1-Feb-20
3-Feb-20
5-Feb-20
7-Feb-20
9-Feb-20
11-Feb-20
13-Feb-20
15-Feb-20
17-Feb-20
19-Feb-20
21-Feb-20
23-Feb-20
25-Feb-20
27-Feb-20
29-Feb-20
2-Mar-20
4-Mar-20
6-Mar-20
8-Mar-20
10-Mar-20
12-Mar-20
14-Mar-20
16-Mar-20
18-Mar-20
20-Mar-20
22-Mar-20
Number of cases
Date
of i
llnes
s on
set
NSW
VIC
SAQ
LDW
ATA
SAC
TN
T
a Re
cent
ly re
port
ed c
ases
sho
wn
in th
e gr
aph
shou
ld b
e in
terp
rete
d w
ith c
autio
n as
ther
e ca
n be
del
ays
in re
port
ing.

5 of 19 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.28) Epub 27/03/2020
Fig
ure
2: C
onfir
med
cas
es o
f CO
VID
-19,
Aus
tral
ia, b
y lo
catio
n of
usu
al re
siden
ce a
nd st
atis
tical
are
a le
vel 3
a
a Re
pres
ents
the
usua
l loc
atio
n of
resi
denc
e of
a c
ase,
whi
ch d
oes
not n
eces
saril
y m
ean
that
this
is th
e pl
ace
whe
re th
ey a
cqui
red
thei
r inf
ectio
n or
wer
e di
agno
sed.
Ove
rsea
s re
side
nts
who
do
not h
ave
a us
ual p
lace
of r
esid
ence
in A
ustr
alia
are
not
sho
wn.

6 of 19 health.gov.au/cdiCommun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.28) Epub 27/03/2020
Table 1: Cumulative notified cases of confirmed COVID-19 and diagnostic tests performed, Australia, by jurisdiction
Jurisdictiona Number of new cases this
reporting periodb (19:00 AEDT 14 March to 23:59 AEDT 22 March
2020)
Total casesb (to 23:59 AEDT 22
March 2020)
Cases per 100,000
population
Cumulative number of tests
performed(proportion of
tests positive %)
NSW 445 766 9.5 59,131 (1.3%)
Vic 90 313 4.8 24,813 (1.3%)
Qld 273 362 7.1 31,868 (1.1%)
WA 169 130 5.0 9,498 (1.4%)
SA 117 137 7.8 13,000 (1.1%)
Tas 19 21 3.9 1,020 (2.1%)
NT 3 4 1.6 1,098 (0.4%)
ACT 27 32 7.5 2,628 (1.2%)
Total 1,143 1,765 7.0 143,056 (1.2%)
a NSW = New South Wales, Vic = Victoria, Qld = Queensland, WA = Western Australia, SA = South Australia, Tas = Tasmania, NT = Northern
Territory, ACT = Australian Capital Territory.
b Due to the dynamic nature of the NNDSS, data in this extract is subject to retrospective revision and may vary from data reported in
previously published reports and reports of notification data by states and territories.

7 of 19 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.28) Epub 27/03/2020
Figu
re 3
: Age
dis
trib
utio
n of
CO
VID
-19
case
s, A
ustr
alia
, by
sex
050100
150
200
250
0-9
10-1
920
-29
30-3
940
-49
50-5
960
-69
70-7
980
-89
90+
Number of cases
Age
grou
p (y
ears
)
mal
efe
mal
e

8 of 19 health.gov.au/cdiCommun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.28) Epub 27/03/2020
Figu
re 4
: Cas
e ra
tes o
f CO
VID
-19
case
s, A
ustr
alia
, by
age
and
sex
02468101214
0-9
10-1
920
-29
30-3
940
-49
50-5
960
-69
70-7
980
-89
90+
Number of cases per 100,000
Age
grou
p (y
ears
)
mal
e ra
tefe
mal
e ra
te
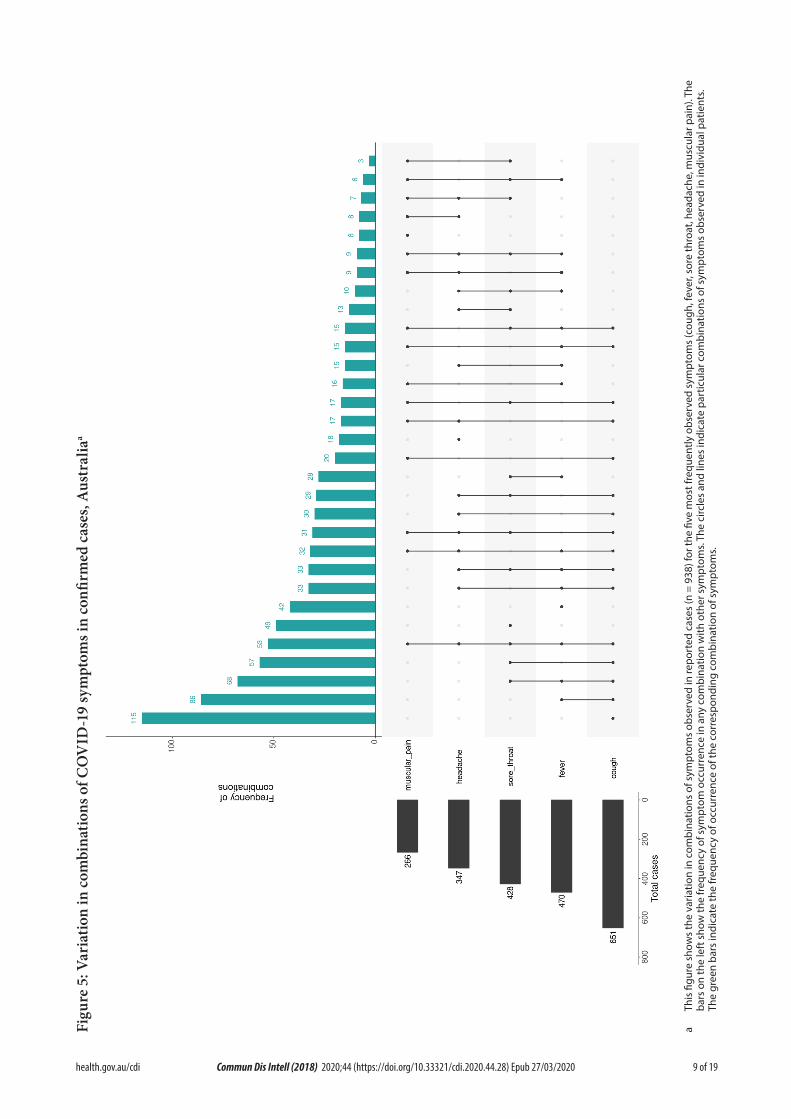
9 of 19 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.28) Epub 27/03/2020
Figu
re 5
: Var
iatio
n in
com
bina
tions
of C
OV
ID-1
9 sy
mpt
oms i
n co
nfirm
ed c
ases
, Aus
tral
iaa
a Th
is fi
gure
sho
ws
the
varia
tion
in c
ombi
natio
ns o
f sym
ptom
s ob
serv
ed in
repo
rted
cas
es (n
= 9
38) f
or th
e fiv
e m
ost f
requ
ently
obs
erve
d sy
mpt
oms
(cou
gh, f
ever
, sor
e th
roat
, hea
dach
e, m
uscu
lar p
ain)
. The
ba
rs o
n th
e le
ft s
how
the
freq
uenc
y of
sym
ptom
occ
urre
nce
in a
ny c
ombi
natio
n w
ith o
ther
sym
ptom
s. Th
e ci
rcle
s an
d lin
es in
dica
te p
artic
ular
com
bina
tions
of s
ympt
oms
obse
rved
in in
divi
dual
pat
ient
s. Th
e gr
een
bars
indi
cate
the
freq
uenc
y of
occ
urre
nce
of th
e co
rres
pond
ing
com
bina
tion
of s
ympt
oms.

10 of 19 health.gov.au/cdiCommun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.28) Epub 27/03/2020
Figu
re 6
: Num
ber o
f CO
VID
-19
case
s by
plac
e of
acq
uisit
ion
over
tim
e, A
ustr
alia
(n =
1,7
65)a
020406080100
120
140
160
180
12-Jan-20
14-Jan-20
16-Jan-20
18-Jan-20
20-Jan-20
22-Jan-20
24-Jan-20
26-Jan-20
28-Jan-20
30-Jan-20
1-Feb-20
3-Feb-20
5-Feb-20
7-Feb-20
9-Feb-20
11-Feb-20
13-Feb-20
15-Feb-20
17-Feb-20
19-Feb-20
21-Feb-20
23-Feb-20
25-Feb-20
27-Feb-20
29-Feb-20
2-Mar-20
4-Mar-20
6-Mar-20
8-Mar-20
10-Mar-20
12-Mar-20
14-Mar-20
16-Mar-20
18-Mar-20
20-Mar-20
22-Mar-20
Number of cases
Date
of i
llnes
s on
set
Ove
rsea
s acq
uire
d Lo
cally
acq
uire
d-cl
ose
cont
act
U
nder
inve
stig
atio
n Lo
cally
acq
uire
d, n
ot e
pi li
nked
a Re
cent
ly re
port
ed c
ases
sho
wn
in th
e gr
aph
shou
ld b
e in
terp
rete
d w
ith c
autio
n as
ther
e ca
n be
del
ays
in re
port
ing.

11 of 19 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.28) Epub 27/03/2020
Figu
re 7
: Con
firm
ed c
ases
of o
vers
eas a
cqui
red
CO
VID
-19
infe
ctio
n (n
= 8
72) b
y W
HO
regi
on o
f ori
gina
010203040506070
13-Jan-20
15-Jan-20
17-Jan-20
19-Jan-20
21-Jan-20
23-Jan-20
25-Jan-20
27-Jan-20
29-Jan-20
31-Jan-20
2-Feb-20
4-Feb-20
6-Feb-20
8-Feb-20
10-Feb-20
12-Feb-20
14-Feb-20
16-Feb-20
18-Feb-20
20-Feb-20
22-Feb-20
24-Feb-20
26-Feb-20
28-Feb-20
1-Mar-20
3-Mar-20
5-Mar-20
7-Mar-20
9-Mar-20
11-Mar-20
13-Mar-20
15-Mar-20
17-Mar-20
19-Mar-20
21-Mar-20
Number of cases
Date
of i
llnes
s on
set
Nor
th-E
ast A
siaN
orth
Afr
ica
and
the
Mid
dle
East
Euro
pe
Sout
h-Ea
st A
siaN
ew Z
eala
nd a
nd P
acifi
cAm
eric
as
Sout
hern
and
Cen
tral
Asia
Sub-
Saha
ran
Afric
aSo
uthe
rn a
nd C
entr
al A
sia
a Re
cent
ly re
port
ed c
ases
sho
wn
in th
e gr
aph
shou
ld b
e in
terp
rete
d w
ith c
autio
n as
ther
e ca
n be
del
ays
in re
port
ing.
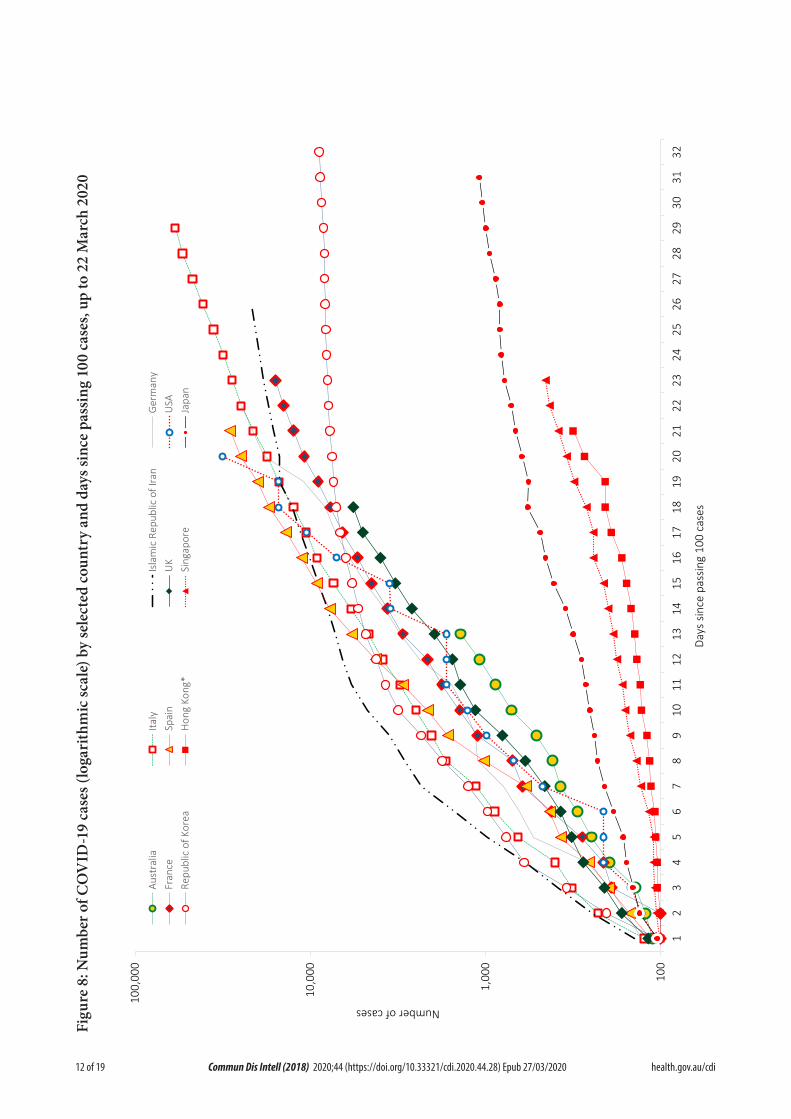
12 of 19 health.gov.au/cdiCommun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.28) Epub 27/03/2020
Figu
re 8
: Num
ber o
f CO
VID
-19
case
s (lo
gari
thm
ic sc
ale)
by
sele
cted
coun
try
and
days
sinc
e pa
ssin
g 10
0 ca
ses,
up to
22
Mar
ch 2
020
100
1,00
0
10,0
00
100,
000
12
34
56
78
910
1112
1314
1516
1718
1920
2122
2324
2526
2728
2930
3132
Number of cases
Days
sin
ce p
assin
g 10
0 ca
ses
Aust
ralia
Italy
Isla
mic
Rep
ublic
of I
ran
Ger
man
yFr
ance
Spai
nU
KU
SARe
publ
ic o
f Kor
eaH
ong
Kong
*Si
ngap
ore
Japa
n

13 of 19 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.28) Epub 27/03/2020
Globally, 12,783 deaths have been reported. Almost three-quarters (74%; n = 9,517) of global deaths have been reported by 174 countries, territories and areas outside of mainland China. Of the deaths reported outside of mainland China, 51% (n = 4,827) were reported in Italy, 16% (n = 1,556) in the Islamic Republic of Iran, and 14% (n = 1,326) in Spain.1 The global proportion of cases that are reported to have died is 4.4%. This proportion is likely to be an overestimate due to the likely variable levels of under-ascertainment of cases, especially those with mild infections. There is wide variation in this proportion globally, with countries such as Italy (9.0%), the Islamic Republic of Iran (7.5%) and Spain (5.3%) reporting substantially higher proportions.
Epidemiological features of COVID-19
The current estimates on epidemiological param-eters including severity, transmissibility and incubation period are uncertain. Estimates are likely to change as more information becomes available.
Transmission
Human-to-human transmission of SARS-CoV-2 is via droplets and fomites from an infected person to a close contact.3 COVID-19 can often present as a common cold-like illness where the virus is shed for a prolonged time after symp-toms end, including in stools.4 A virological analysis of nine hospitalised cases found active virus replication in upper respiratory tract tis-sues, with pharyngeal virus shedding very high during the first week of symptoms.4 However, current evidence does not support airborne or faecal-oral spread as major factors in transmis-sion.3
A study in China showed household contacts and those who travelled with a confirmed COVID-19 case were strongly associated with an increased risk of infection.5 The study also examined the average time from symptom onset to disease confirmation among cases who were identified through contact-based surveillance
(i.e. monitoring and testing of close contacts of confirmed COVID-19 cases) and symptom-based surveillance (i.e. symptomatic screening at airports, community fever monitoring and testing of hospital patients). Cases identified through contact-based surveillance were associ-ated with a 2.3 day decrease from symptom onset to disease confirmation and a 1.9 day decrease from symptom onset to isolation, compared to cases found by symptom-based surveillance. Modelling studies suggest that undocumented infections are the source for over three-quarters of documented cases and effective contact trac-ing increases the probability of control.5,6
Infection of a dog with SARS-CoV-2 has been reported to the International Organisation for Animal Health (OIE) on two occasions since the outbreak began.7 Both dogs were in Hong Kong and had close contact with owners with COVID-19. Neither dog showed clinical signs of infection and there is no evidence that dogs play a role in disease spread. Further studies are underway to understand if and how different animal species could be affected by COVID-19.
Incubation period
Estimates of median incubation period, based on seven published studies, are 5 to 6 days (ranging from 0 to 14 days).8 Patients with long incubation periods do occasionally occur, how-ever they are likely to be ‘outliers’ who should be studied further but are unlikely to represent a change in epidemiology of the virus.8
Molecular epidemiology
The initial COVID-19 cases were reported in late December 2019 following the discovery of a cluster of pneumonia cases at the Huanan Seafood Market in Wuhan China. However, subsequent work has identified SARS-CoV-2 cases as early as 1 December 2019 in Wuhan.9 Additionally, a phylogenetic analysis of whole genome sequences has dated the emergence of SARS-CoV-2 infection in humans to between late November and early December 2019.10 Since December 2019, the virus has diversified into

14 of 19 health.gov.au/cdiCommun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.28) Epub 27/03/2020
Figu
re 9
: Phy
loge
ny o
f glo
bal S
AR
S-C
oV-2
gen
ome
sequ
ence
sa
a Pu
blic
ly a
vaila
ble
high
qua
lity,
who
le g
enom
e se
quen
ces
wer
e do
wnl
oade
d fr
om w
ww
.gis
aid.
org,
alig
ned
and
anal
ysed
usi
ng a
phy
loge
netic
app
roac
h w
ith P
hyM
L (n
= 5
94 a
s of
21
Mar
ch 2
020)
. Ind
ivid
ual
sequ
ence
s ar
e sh
own
as c
ircle
s an
d co
lour
ed b
y co
untr
y or
regi
on a
s pe
r the
key
pro
vide
d. G
loba
lly, S
ARS
-CoV
-2 h
as d
iver
sifie
d in
to m
ultip
le li
neag
es w
ith s
ome
geog
raph
ic c
lust
erin
g ap
pare
nt. A
ustr
alia
n st
rain
s ar
e ge
nera
lly d
ispe
rsed
acr
oss
the
glob
al p
hylo
geny
alth
ough
not
able
clu
ster
s in
clud
e on
e of
retu
rned
trav
elle
rs fr
om th
e Is
lam
ic R
epub
lic o
f Ira
n. T
he s
cale
is p
ropo
rtio
nal t
o th
e nu
mbe
r of s
ubst
itu-
tions
per
site
.

15 of 19 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.28) Epub 27/03/2020
multiple lineages as it has spread globally with some degree of geographical clustering (Figure 9). The whole genome sequences currently avail-able from Australian cases (n=25) are mostly in returned travellers from China, the Islamic Republic of Iran, Europe and the USA, and thereby reflect this global diversity (Figure 9). Recent work describes an emerging clade linked to the epidemic in the Islamic Republic of Iran,11 which highlights how genomic epidemiology can shed light on un-sampled locations. The high number of independent introduction events within Australia from Europe is also striking. Continuing these analyses as more data from Australia become available will corroborate and query field data on the epidemiological links among clusters within and between jurisdic-tions.
Clinical features
A recently published meta-analysis supports previous research that COVID-19 presents as mild illness in the majority of cases with fever and cough being the most commonly reported symptoms. Severe or fatal outcomes tend to occur in the elderly or those with comorbid conditions.3,12
Some COVID-19 patients show neurological signs such as headache, nausea and vomiting. There is evidence that SARS-CoV-2 viruses are not always confined to the respiratory tract and may invade the central nervous system inducing neurological symptoms.13 As such, it is possible that invasion of the central nervous system is partially responsible for the acute respiratory failure of COVID-19 patients.13
Examination of cases and their close contacts in China found a positive association between age and time from symptom onset to recovery. Median time to recovery was estimated to be 27 days in 20–29 year olds, 32 days in 50–59 year olds, and 36 days in those aged over 70 years. The study also found an association between clinical severity and time from symptom onset to time to recovery. Compared to people with
mild disease, those with moderate and severe disease were associated with a 19% and 58% increase in time to recovery, respectively.5
A retrospective cohort study looking at risk fac-tors for mortality among patients with COVID-19 who have experienced a definite outcome found an increase in the odds of in-hospital death associated with older age, higher sequen-tial organ failure assessment score and elevated blood d-dimer levels on admission.14 Detectable SARS-CoV-2 RNA persisted for a median of 20 days in survivors and until death in non-survivors.14
Treatment
Current clinical management of COVID-19 cases focuses on early recognition, isolation, appropriate infection control measures and provision of supportive care.15 Whilst there is no specific antiviral treatment currently recom-mended for patients with suspected or confirmed SARS-CoV-2 infection, multiple clinical trials are underway to evaluate a number of thera-peutic agents, including remdesivir, lopinavir/ritonavir, and chloroquine.16
Public health response
A summary of the key events that have been associated with the emergence of COVID-19, including Australia’s public health response activities is provided at Figure 10. Since COVID-19 first emerged internationally, public health responses in Australia have continued to evolve with the changing body of knowledge and epi-demiological profile, both from overseas and in Australia. During the current reporting period, the Australian Health Protection Principal Committee have issued advice to inform the national public health response to the pandemic including the broadening of the 14-day quaran-tine requirement for all travellers from overseas, regardless of the country, as well as physical distancing measures.17

16 of 19 health.gov.au/cdiCommun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.28) Epub 27/03/2020
Figu
re 1
0. T
imel
ine
of C
OV
ID-1
9 re
late
d ev
ents
, inc
ludi
ng A
ustr
alia
n pu
blic
hea
lth re
spon
se a
ctiv
ities
31-D
ec-1
9No
tifica
tion t
oW
HO pn
eum
onia
of un
know
n orig
in7-Ja
n-20
SARS
-CoV
-2 id
entif
ied
11-F
eb-2
0W
HO an
noun
ced a
nam
e for
the
new
coro
navir
us di
seas
e: CO
VID-
19
21-M
ar-2
0Ql
d, W
A, N
T and
SA cl
ose b
orde
rsto
non-
esse
ntial
trav
eller
s
20-M
ar-2
0Ta
sman
ia clo
ses b
orde
rsto
non-
esse
ntial
trav
eller
s
18-M
ar-2
0DF
AT ra
ises t
rave
l adv
ice fo
r all o
verse
asde
stina
tions
to Le
vel 4
'Do N
ot Tr
avel'
18-M
ar-2
0AH
PPC r
ecom
men
dsth
e con
tinua
tion o
f a 14
day
quar
antin
e req
uirem
ent
for a
ll ret
urni
ng tr
avell
ers
11-M
ar-2
0W
HO ch
arac
teris
esCO
VID-
19 as
pand
emic
13-M
ar-2
0AH
PPC p
rovid
es re
com
men
datio
ns fo
rpu
blic g
athe
rings
, tes
ting a
nd so
cial d
istan
cing
12-M
ar-2
0AH
PPC p
rovid
es re
com
men
datio
nsfo
r hea
lthca
re an
d age
care
wor
kers
8-M
ar-2
0AH
PPC r
ecom
men
ds re
strict
ions o
nCO
VID-
19 co
ntac
ts an
d tra
velle
rsfro
m lis
ted h
igher
risk c
ount
ries
5-M
ar-2
0Re
strict
ions o
n tra
vel
from
Repu
blic
of Ko
rea
1-M
ar-2
0Re
strict
ions o
n tra
vel
from
Islam
ic Re
publi
c of Ir
an
1-Fe
b-20
Restr
iction
s on t
rave
lfro
m Ch
ina im
plem
ente
d
30-Ja
n-20
WHO
decla
res P
ublic
Hea
lthEm
erge
ncy o
f Inte
rnat
ional
Conc
ern

17 of 19 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.28) Epub 27/03/2020
Table 2: Australian COVID-19 case definition as of 22 March 202018
Version Date of development Suspect Case Confirmed Case
2.2 21 March 2020 A. If the patient satisfies epidemiological and clinical criteria, they are classified as a suspect case.Epidemiological criteriaInternational travel in the 14 days before illness onset.ORClose contact in 14 days before illness onset with a confirmed case of COVID-19.Clinical criteriaFever (≥ 38 °C) or history of fever (e.g. night sweats, chills).ORAcute respiratory infection (e.g. shortness of breath, cough, sore throat) with or without fever.
B. If the patient has bilateral community-acquired pneumonia (critically ill) and no other cause is identified, with or without recent international travel, they are classified as a suspect case.
C. If any healthcare worker with direct patient contact has a fever (≥ 38 °C) or history of fever (e.g. night sweats, chills) AND an acute respiratory infection (e.g. shortness of breath, cough, sore throat), they are classified as a suspect case.
A person who tests positive to a validated specific SARS-CoV-2 nucleic acid test or has the virus identified by electron microscopy or viral culture.
Methods
Data for this report were current as at 23:59 hours AEDT, 22 March 2020.
This report outlines what is known epidemio-logically on COVID-19 in Australia and from publicly available data from WHO Situation Reports, other countries’ official updates and the scientific literature. Data on domestic cases in this report were collected from the NNDSS and additionally informed by jurisdictional health department media releases. The Communicable Diseases Network Australia (CDNA) developed the case definition for suspect and confirmed cases, which was modified at different time points during the outbreak (Table 2). Data were analysed using Stata to describe the epidemiol-ogy of COVID-19 in Australia and the progress of the epidemic. Data for the international cases of COVID-19 by country were compiled from the latest WHO Situation Report. Case defini-tions may vary by country making comparisons difficult. Rapid reviews of the current state of knowledge on COVID-19 were conducted from the literature using PubMed.
Acknowledgements
This report represents surveillance data reported through CDNA as part of the nationally-coordinated response to COVID-19. We thank public health staff from incident emergency operations centres in state and territory health departments, and the Australian Government Department of Health, along with state and ter-ritory public health laboratories. We thank John Grewar for providing the R-code to produce Figure 5. We also thank John-Sebastian Eden and Eddie Holmes (University of Sydney and Westmead Institute for Medical Research) for graciously allowing the use of their phylogenetic tree (Figure 9).

18 of 19 health.gov.au/cdiCommun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.28) Epub 27/03/2020
Author details
Corresponding author
Andrew C. Breed
NIR Surveillance Team, Communicable Disease Epidemiology and Surveillance Section, Health Protection Policy Branch, Australian Government Department of Health, GPO Box 9484, MDP 14, Canberra, ACT 2601.
Email: [email protected]
References
1. World Health Organization (WHO). Coronavirus disease 2019 (COVID-19) situation report – 54: 22 March 2020. Geneva: WHO; 2020. [Accessed on 24 March 2020.] Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200322-sitrep-62-covid-19.pdf.
2. WHO. Coronavirus disease 2019 (COVID-19) situation report – 47: 14 March 2020. Geneva: WHO; 2020. [Accessed on 24 March 2020.] Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200314-sitrep-54-covid-19.pdf.
3. WHO. Report of the WHO-China joint mission on coronavirus disease 2019 (COVID-19). Geneva: WHO; 2020. [Accessed on 1 March 2020.] Available from: https://www.who.int/docs/default-source/coronaviruse/who-china-joint-mission-on-covid-19-final-report.pdf.
4. Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020. doi: https://doi.org/10.1016/S0140-6736(20)30566-3.
5. Bi Q, Wu Y, Mei S, Ye C, Zou X, Zhang Z et al. Epidemiology and transmission of
COVID-19 in Shenzhen China: analysis of 391 cases and 1286 of their close contacts. medRxiv. 2020. doi: https://doi.org/10.1101/2020.03.03.20028423.
6. Li R, Pei S, Chen B, Song Y, Zhang T, Yang W et al. Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus (SARS-CoV2). Science. 2020. doi: https://doi.org/10.1126/science.abb3221.
7. World Organisation for Animal Health (OIE). Questions and Answers on the 2019 coronavirus disease (COVID-19). [Internet.] Paris, OIE; 2020. [Accessed on 26 March 2020.] Available from: https://www.oie.int/en/scientific-expertise/specific-information-and-recommendations/questions-and-answers-on-2019novel-coronavirus/.
8. WHO. Coronavirus disease 2019 (COVID-19) situation report – 29: 18 February 2020. Geneva: WHO; 2020. [Accessed on 15 March 2020.] Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200218-sitrep-29-covid-19.pdf.
9. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y et al. Clinical features of patients infected with novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497-506. doi: https://doi.org/10.1016/S0140-6736(20)30183-5.
10. Bedford T, Neher R, Hadfield J, Hodcroft E, Ilcisin M, Müller N. Genomic analysis of nCOV spread. Situation report 2020-01-30. [Internet.] 2020. Available from: https://nextstrain.org/narratives/ncov/sit-rep/2020-01-30.
11. Eden JS, Rockett R, Carter I, Rahman H, de Ligt J, Hadfield J et al. An emergent clade of SARS-CoV-2 linked to returned travellers from Iran. bioRxiv. 2020. doi: https://doi.org/10.1101/2020.03.15.992818.
12. Sun P, Qie S, Liu Z, Ren J, Xi JJ. Clinical

19 of 19 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.28) Epub 27/03/2020
characteristics of 50466 patients with 2019-nCoV infection. medRxiv. 2020. doi: https://doi.org/10.1101/2020.02.18.20024539.
13. Li Y, Bai W, Hashikawa T. The neuroinvasive potential of SARS-CoV2 may be at least partially responsible for the respiratory failure of COVID-19 patients. J Med Virol. 2020. doi: https://doi.org/10.1002/jmv.25728.
14. Woelfel R, Corman VM, Guggemos W, Seilmaier M, Zange S, Mueller MA et al. Clinical presentation and virological assessment of hospitalized cases of coronavirus disease 2019 in a travel-associated transmission cluster. medRxiv. 2020. doi: https://doi.org/10.1101/2020.03.05.20030502.
15. WHO. Clinical management of severe acute respiratory infection when novel coronavirus (nCoV) infection is suspected. [Internet.] Geneva: WHO; 2020. [Accessed on 23 February 2020.] Available from: https://www.who.int/publications-detail/clinical-management-of-severe-acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-suspected.
16. Harrison, C. Coronavirus puts drug repurposing on the fast track. Nat Biotechnol. 2020. doi: https://doi.org/10.1038/d41587-020-00003-1.
17. Australian Government Department of Health. Latest statement from the Australian Health Protection Principal Committee (AHPPC) on coronavirus (COVID-19). [Internet.] Canberra: Australian Government Department of Health; 21 March 2020. [Accessed on 24 March 2020.] Available from: https://www.health.gov.au/news/latest-statement-from-the-australian-health-protection-principal-committee-ahppc-on-coronavirus-covid-19.
18. Australian Government Department of Health. Novel coronavirus 2019 (2019-nCoV) - CDNA national guidelines for
public health units. [Internet.] Canberra: Australian Government Department of Health; 2020. [Accessed on 24 March 2020.] Available from: https://www1.health.gov.au/internet/main/publishing.nsf/Content/7A8654A8CB144F5FCA2584F8001F91E2/$File/interim-COVID-19-SoNG-v2.2.pdf.

2 0 2 0 V o l u m e 4 4https://doi.org/10.33321/cdi.2020.44.29
COVID-19, Australia: Epidemiology Report 9: Reporting week ending 23:59 AEDT 29 March 2020COVID-19 National Incident Room Surveillance Team
Communicable Diseases Intelligence ISSN: 2209-6051 Online
This journal is indexed by Index Medicus and Medline.
Creative Commons Licence - Attribution-NonCommercial-NoDerivatives CC BY-NC-ND
© 2020 Commonwealth of Australia as represented by the Department of Health
This publication is licensed under a Creative Commons Attribution- Non-Commercial NoDerivatives 4.0 International Licence from https://creativecommons.org/licenses/by-nc-nd/4.0/legalcode (Licence). You must read and understand the Licence before using any material from this publication.
Restrictions The Licence does not cover, and there is no permission given for, use of any of the following material found in this publication (if any):
• the Commonwealth Coat of Arms (by way of information, the terms under which the Coat of Arms may be used can be found at www.itsanhonour.gov.au);
• any logos (including the Department of Health’s logo) and trademarks;
• any photographs and images;
• any signatures; and
• any material belonging to third parties.
Disclaimer Opinions expressed in Communicable Diseases Intelligence are those of the authors and not necessarily those of the Australian Government Department of Health or the Communicable Diseases Network Australia. Data may be subject to revision.
Enquiries Enquiries regarding any other use of this publication should be addressed to the Communication Branch, Department of Health, GPO Box 9848, Canberra ACT 2601, or via e-mail to: [email protected]
Communicable Diseases Network Australia Communicable Diseases Intelligence contributes to the work of the Communicable Diseases Network Australia. http://www.health.gov.au/cdna
Communicable Diseases Intelligence (CDI) is a peer-reviewed scientific journal published by the Office of Health Protection, Department of Health. The journal aims to disseminate information on the epidemiology, surveillance, prevention and control of communicable diseases of relevance to Australia.
Editor Tanja Farmer
Deputy Editor Simon Petrie
Design and Production Kasra Yousefi
Editorial Advisory Board David Durrheim, Mark Ferson, John Kaldor, Martyn Kirk and Linda Selvey
Website http://www.health.gov.au/cdi
Contacts Communicable Diseases Intelligence is produced by: Health Protection Policy Branch Office of Health Protection Australian Government Department of Health GPO Box 9848, (MDP 6) CANBERRA ACT 2601
Email: [email protected]
Submit an Article You are invited to submit your next communicable disease related article to the Communicable Diseases Intelligence (CDI) for consideration. More information regarding CDI can be found at: http://health.gov.au/cdi.
Further enquiries should be directed to: [email protected].

1 of 24 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.29) Epub 3/4/2020
Weekly epidemiological report
COVID-19, Australia: Epidemiology Report 9:Reporting week ending 23:59 AEDT 29 March 2020
COVID-19 National Incident Room Surveillance Team
An error occurred in the legend for Figure 8 (Confirmed cases of overseas acquired COVID-19 infection (n = 2,352) by Standard Australian
Classification of Countries) as originally published, which inadvertently omitted the key depicting the confirmed cases from Sub-Saharan Africa.
This has now been amended.
Summary
This is the ninth epidemiological report for coronavirus disease 2019 (COVID-19), reported in Australia as at 23:59 Australian Eastern Daylight Time [AEDT] 29 March 2020. It includes data on COVID-19 cases diagnosed in Australia, the international situation and a review of current evidence.
Keywords: SARS-CoV-2; novel coronavirus; 2019-nCoV; coronavirus disease 2019; COVID-19; acute respiratory disease; case definition; epidemiology; Australia
The following epidemiological data are subject to change both domestically and internationally due to the rapidly evolving situation. Australian cases are still under active investigation. While every effort has been made to standardise the investigation of cases nationally, there may be some differences between jurisdictions. For further information relating to the data incorporated in this series of reports, please refer to the Frequently Asked Questions addressed within the appendix to this report.
Australian situation
As at 23:59 AEDT 29 March 2020, there were 4,159 confirmed cases, including 15 deaths in Australia, reported to the National Notifiable Diseases Surveillance System (NNDSS)i (Table 1, Figure 1). Of the 4,159 confirmed cases, 48% were reported in NSW, 18% from Qld, 16% from Vic, 8% from WA, 7% from SA, 2% from ACT, 1% from Tas, and 0.3% from NT (Figures 2, 3). The rate of cases in Australia per 100,000 population was 16.4; in comparison, the rate per 100,000 population was 7.0 in the previous reporting period. Most cases are reported to
i Data were extracted on 30 March 2020 with data reported
to 29 March 2020. Due to the dynamic nature of the NNDSS,
data in this extract are subject to retrospective revision and
may vary from data published in previous reports and reports
of notification data by states and territories.
reside within major metropolitan areas, with a small number of cases reported outside these areas (Figures 2, 3).
During the current reporting week, 2,355 cases were reported; this is a 136% increase from cases reported during the previous reporting period. The median time between onset of symptoms and laboratory testing was two days (range 0–32 days).
The median age of notified cases in Australia was 48 years (range 0–98 years), with the largest number of cases in the 20–29 years age group (Figure 4). The highest rate of disease was among those in the 60–69 years age group (Figure 4). Notifications by gender were approximately equal, although there was some variation across age groups.

2 of 24
Weekly epidemiological report
Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.29) Epub 3/4/2020 health.gov.au/cdi
In Australia:
• There have been 4,159 confirmed cases, including 15 deaths, reported in Australia up to23:59 AEDT 29 March 2020. Of confirmed cases, the highest proportion of cases have beenfrom New South Wales (48%), followed by Queensland (18%) and Victoria (16%);
• Forty-two percent of the total number of cases reported so far have been during the currentreporting week;
• Hospitalisation status was recorded for 2,129 cases, of which 19% were reported to have beenhospitalised due to their COVID-19 infection. Of these hospitalised cases, ICU (IntensiveCare Unit) status was recorded for 176 cases, of which 22% (n = 38) were admitted to anICU, with five cases requiring ventilation; and
• The rate of increase in cases has lowered over the reporting week. Whilst the effects of borderand recently-introduced social distancing measures are likely having an effect, it is too soonto tell whether this trend will be sustained.
Internationally:
• A total of 634,813 cases have been reported globally across 189 countries, territories andregions;
• The USA has overtaken Italy as the country with most reported cases (n = 103,321), however,the European Region continues to be the most heavily affected, with Italy, Spain and Ger-many accounting for 60% (n = 217,267) of all cases in the region; and
• A total of 29,891 deaths have been reported globally with over 70% (n = 21,427) reported inthe European Region.
Of the symptoms reported, cough (70%) was the most common. Forty-nine percent reported headache, 47% reported fever, 45% reported sore throat, and 34% reported runny nose (Figure 5). Only 2% or fewer of all cases reported either pneumonia or acute respiratory disease (ARD). An analysis of symptom combinations high-lights that cough is the predominant clinical presentation in combination with fever and/or sore throat (Figure 6).
Hospitalisation status was recorded for 2,129 cases, of which 18.9% (n = 402) were reported to have been hospitalised due to their COVID-19 infection. The median age of hospitalised cases was 58 years (range 0–98 years), with the high-est proportion of cases in the 60–69 years age
group. The most commonly reported comorbid condition among hospitalised cases was diabetes (6.2%), followed by cardiac disease (6.0%). Of these hospitalised cases, ICU (Intensive Care Unit) status was recorded for 176 cases of which 22% (n = 38) were recorded being admitted to an ICU, with five cases requiring ventilation.
Fifteen COVID-19 deaths were confirmed in Australia up to 29 March 2020. The median age was 81 years (range 67–94 years). Four of these deaths were in an aged care facility, four were associated with cruise ships and the other seven cases were acquired in the community. Seven of the cases were male and eight were female. The period between the date of illness onset and death ranged from 0 to 12 days. Of the 15

3 of 24
Weekly epidemiological report
health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.29) Epub 3/4/2020
confirmed deaths, three reported having comor-bidities, including diabetes, chronic respiratory conditions and stroke.
Of cases with a reported place of acquisition (2,964 of 4,159), 79% (n = 2,352) had a recent international travel history and 21% (n = 612) were considered to have been locally acquired (Figure 7). The majority of overseas-acquired cases (Figure 8) reported a travel history to the European Region, the Americas Region or on board cruise ships. Of the locally-acquired cases, the majority were considered to be contacts of a confirmed case, with a very small number of cases not able to be epidemiologically linked to a confirmed case. For the remainder of cases where a place of acquisition has not been reported, these cases are currently under public health investigation. The distribution of the source of infection for cases varied by jurisdiction.
Of the 4,159 confirmed cases, 27 cases (0.6%) were reported in Aboriginal and Torres Strait Islander persons. These 27 cases have been reported across several jurisdictions with the majority of cases reported in areas classified as ‘major cities of Australia’ based on the case’s usual place of residence. Completeness of the Indigenous status field was approximately 73%, with 11% of cases with a reported value of unknown.
Cluster and outbreak investigations
Investigations are taking place in states and ter-ritories in relation to a number of clusters and outbreaks of COVID-19. To date the largest out-breaks have been associated with cruise ships.
Closed environments, close contact between travellers from various countries, and crew transfers between voyages make cruise ships a unique environment for rapid disease transmis-sion.1 Cruise ships account for a substantial proportion of COVID-19 cases in Australia. Of cases with a reported place of acquisition, 23% (n = 670) were considered to have acquired their infection at sea.
During the period 7 to 23 February 2020, the largest outbreak of COVID-19 cases outside of mainland China occurred on the Diamond Princess cruise ship. Of the 3,711 passengers and crew, 712 (19.2%) were confirmed as having COVID-19 including 56 residents of Australia.
Between 7 and 29 March 2020, at least 17 cruise ships have docked in Australia and 9 have con-firmed cases of COVID-19.ii This includes the Ruby Princess which docked on 19 March 2020 and at the time of reporting was associated with 215 cases.
ii Data obtained on 1 April 2020.
Clusters:
• The term ‘cluster’ in relation to COVID-19 refers to two or more cases that are epidemiologi-cally related in time, place or person where a common source (such as an event or within a community) of infection is suspected but not yet established.
Outbreaks:
• The term ‘outbreak’ in relation to COVID-19 refers to two or more cases among a specific group of people and/or over a specific period of time where illness is associated with a com-mon source (such as an event or within a community).

4 of 24
Weekly epidemiological report
Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.29) Epub 3/4/2020 health.gov.au/cdi
International situation
As at 23:59 AEDT 29 March 2020, the number of confirmed COVID-19 cases reported to the World Health Organization (WHO) was 634,813 globally.2 57% (n = 361,031) of all reported cases are from the European Region, 19% (n = 120,792) are from the Region of the Americas, and 16% (n = 102,788) are from the Western Pacific Region. The most affected countries with the highest number of reported cases across these regions are respectively Italy (n = 92,672), the United States of America (n = 103,321) and China, including special administrative regions (n = 82,341).
The number of new cases reported globally has continued to increase. As of the last reporting week, 15 countries, territories and areas reported cases of COVID-19 for the first time, bringing the total to 189 countries, territories and areas globally. The USA has now overtaken Italy as the country with most reported cases; however, the European Region continues to be the most heavily affected, with Italy, Spain and Germany accounting for 60% (n = 217,267) of all cases in the region. Of all the countries, territories and areas with known transmission classification (n = 189), 79% (n = 149) have reported local trans-mission of COVID-19.
The reported epidemiology varies by country with the trajectory of different countries’ out-breaks after their first 100 cases showing vari-ation. Figure 9 highlights that for a number of countries outside of mainland China which have reported more than 100 cases, their rates of increase continue to be high, particularly USA, Italy and Spain. For several other countries or regions including Singapore, Japan and Hong Kong there continues to be a slow rate of increase in their number of new cases, with the Republic of Korea reporting very few new cases each day. Reported case numbers will be influenced by rates of testing, case definition, and case detec-tion as well as overall health system capacity.
Border measures such as travel bans and man-datory 14-day quarantine for all return travel-lers have been put in place to reduce the risk of imported cases into Australia.
Globally, 29,891 deaths have been reported. Over 70% of deaths (n = 21,427) have been reported in the European Region, followed by 12% (n = 3,626) in the Western Pacific Region, and 9% (n = 2,668) in the Eastern Mediterranean Region. Italy, Spain, France and the United Kingdom have reported over 1,000 deaths in each respec-tive country, contributing to a combined total of 89% (n = 19,043) of deaths reported in the region. In the Western Pacific Region, 91% (n = 3,306) of all deaths are reported from China. Iran accounts for 94% (n = 2,517) of all deaths in the Eastern Mediterranean Region. The global proportion of cases that are reported to have died is 4.7%. This proportion is likely to be an overestimate due to variable levels of under-ascertainment of cases, especially those with mild infections. For several other countries or regions including the Republic of Korea, there continues to be a slow increase in their number of deaths, with few new deaths reported in the Republic of Korea each day (Figure 10).
Epidemiological features of COVID-19
The current estimates on epidemiological param-eters including severity, transmissibility and incubation period are uncertain. Estimates are likely to change as more information becomes available.
Transmission
Human-to-human transmission of SARS-CoV-2 is via droplets and fomites from an infected person to a close contact.3 COVID-19 can often present as a common cold-like illness, including in stools.4 A virological analysis of nine hospital-ised cases found active virus replication in upper respiratory tract tissues, with pharyngeal virus shedding during the first week of symptoms.4 However, current evidence does not support airborne or faecal-oral spread as major factors in transmission.3

5 of 24
Weekly epidemiological report
health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.29) Epub 3/4/2020
A study in China showed household contacts and those who travelled with a confirmed COVID-19 case was associated with an increased risk of infection.5 The study also examined the average time from symptom onset to disease confirma-tion among cases who were identified through contact-based surveillance (i.e. monitoring and testing of close contacts of confirmed COVID-19 cases) and symptom-based surveillance (i.e. symptomatic screening at airports, community fever monitoring and testing of hospital patients). Cases identified through contact-based surveil-lance were associated with a 2.3 day decrease from symptom onset to disease confirmation and a 1.9 day decrease from symptom onset to isolation, compared to cases found by symptom-based surveillance. Modelling studies suggest that undocumented infections are the source for over three-quarters of documented cases and effective contact tracing increases the probabil-ity of control.5,6
Incubation period
Estimates of median incubation period, based on seven published studies, are 5 to 6 days (ranging from 0 to 14 days).7 Patients with long incubation periods do occasionally occur, how-ever they are likely to be ‘outliers’ who should be studied further but are unlikely to represent a change in epidemiology of the virus.7
Molecular epidemiology
Since December 2019, the virus has diversified into multiple lineages as it has spread globally with some degree of geographical clustering. The whole genome sequences currently available from Australian cases are mostly in returned travellers from China, the Islamic Republic of Iran, Europe and the USA, and thereby reflect this global diversity. Recent work describes an emerging clade linked to the epidemic in the Islamic Republic of Iran.8
Clinical features
A recently published meta-analysis supports previous research that COVID-19 presents as
mild illness in the majority of cases with fever and cough being the most commonly reported symptoms. Severe or fatal outcomes tend to occur in the elderly or those with comorbid conditions.3,9
Some COVID-19 patients show neurological signs such as headache, nausea and vomiting. There is evidence that SARS-CoV-2 viruses are not always confined to the respiratory tract and may invade the central nervous system inducing neurological symptoms.10 As such, it is possible that invasion of the central nervous system is partially responsible for the acute respiratory failure of COVID-19 patients.10
Examination of cases and their close contacts in China found a positive association between age and time from symptom onset to recovery. Median time to recovery was estimated to be 27 days in 20–29 year olds, 32 days in 50–59 year olds, and 36 days in those aged over 70 years. The study also found an association between clinical severity and time from symptom onset to time to recovery. Compared to people with mild disease, those with moderate and severe disease were associated with a 19% and 58% increase in time to recovery, respectively.5
A retrospective cohort study looking at risk fac-tors for mortality among patients with COVID-19 who have experienced a definite outcome found an increase in the odds of in-hospital death associated with older age, higher sequen-tial organ failure assessment score and elevated blood d-dimer levels on admission.11 Detectable SARS-CoV-2 RNA persisted for a median of 20 days in survivors and until death in non-survivors.11
Several studies have identified cardiovascular implications resulting from COVID-19 infec-tion.12–14 Vascular inflammation has been observed in a number of cases and may be a potential mechanism for myocardial injury which can result in cardiac dysfunction and arrhythmias.
6 of 24
Weekly epidemiological report
Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.29) Epub 3/4/2020 health.gov.au/cdi
Treatment
Current clinical management of COVID-19 cases focuses on early recognition, isolation, appropriate infection control measures and provision of supportive care.15 Whilst there is no specific antiviral treatment currently recom-mended for patients with suspected or confirmed SARS-CoV-2 infection, multiple clinical trials are underway to evaluate a number of thera-peutic agents, including remdesivir, lopinavir/ritonavir, and chloroquine.16
Public health response
A summary of the key events that have been associated with the emergence of COVID-19, including Australia’s public health response activities is provided at Figures 11 and 12. Since COVID-19 first emerged internationally, public health responses in Australia have continued to evolve with the changing body of knowledge and epidemiological profile, both from overseas and in Australia. During the current report-ing period, the Australian Health Protection Principal Committee have issued advice to inform the national public health response to the pandemic including suspension of all non-urgent elective surgery in both public and private sectors, scaling up of social distancing measures, limits to both indoor and outdoor public gatherings, and mandatory 14-day quar-antine in their port of arrival for all travellers entering Australia.17–19
Methods
Data for this report were current as at 23:59 hours AEDT, 29 March 2020.
This report outlines what is known epidemio-logically on COVID-19 in Australia and from publicly available data from WHO Situation Reports, other countries’ official updates and the scientific literature. Data on domestic cases in this report were collected from the NNDSS and additionally informed by jurisdictional health department media releases. The Communicable Diseases Network Australia (CDNA) developed
the case definition for probable, suspect and confirmed cases, which was modified at differ-ent time points during the outbreak (Table 2). Data were analysed using SAS to describe the epidemiology of COVID-19 in Australia and the progress of the epidemic. Data for the interna-tional cases of COVID-19 by country were com-piled from the latest WHO Situation Report. Case definitions may vary by country making comparisons difficult. Rapid reviews of the current state of knowledge on COVID-19 were conducted from the literature using PubMed.
Acknowledgements
This report represents surveillance data reported through CDNA as part of the nationally-coordi-nated response to COVID-19. We thank public health staff from incident emergency operations centres in state and territory health departments, and the Australian Government Department of Health, along with state and territory public health laboratories. We thank John Grewar for providing the R-code to produce Figure 6.
Author details
Corresponding author
COVID-19 National Incident Room Surveillance Team, Communicable Disease Epidemiology and Surveillance Section, Health Protection Policy Branch, Australian Government Department of Health, GPO Box 9484, MDP 14, Canberra, ACT 2601.
Email: [email protected]

7 of 24
Weekly epidemiological report
health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.29) Epub 3/4/2020
Figu
re 1
: Con
firm
ed c
ases
of C
OV
ID-1
9 in
fect
ion,
Aus
tral
ia, b
y da
te o
f illn
ess o
nset
a
050100
150
200
250
300
350
400
13-Jan-20
15-Jan-20
17-Jan-20
19-Jan-20
21-Jan-20
23-Jan-20
25-Jan-20
27-Jan-20
29-Jan-20
31-Jan-20
2-Feb-20
4-Feb-20
6-Feb-20
8-Feb-20
10-Feb-20
12-Feb-20
14-Feb-20
16-Feb-20
18-Feb-20
20-Feb-20
22-Feb-20
24-Feb-20
26-Feb-20
28-Feb-20
1-Mar-20
3-Mar-20
5-Mar-20
7-Mar-20
9-Mar-20
11-Mar-20
13-Mar-20
15-Mar-20
17-Mar-20
19-Mar-20
21-Mar-20
23-Mar-20
25-Mar-20
27-Mar-20
29-Mar-20
Number of cases
Dat
e of
illn
ess o
nset
ACT
NSW
NT
QLD
SATA
SVI
CW
A
a Re
cent
ly re
port
ed c
ases
sho
wn
in th
e gr
aph
shou
ld b
e in
terp
rete
d w
ith c
autio
n as
ther
e ca
n be
del
ays
in re
port
ing.

8 of 24
Weekly epidemiological report
Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.29) Epub 3/4/2020 health.gov.au/cdi
Figu
re 2
: Con
firm
ed c
ases
of C
OV
ID-1
9, A
ustr
alia
, by
loca
tion
of u
sual
resid
ence
and
stat
istic
al a
rea
leve
l 3, a
s at 2
3 M
arch
202
0a
a Re
pres
ents
the
usua
l loc
atio
n of
resi
denc
e of
a c
ase,
whi
ch d
oes
not n
eces
saril
y m
ean
that
this
is th
e pl
ace
whe
re th
ey a
cqui
red
thei
r inf
ectio
n or
wer
e di
agno
sed.
Ove
rsea
s re
side
nts
who
do
not h
ave
a us
ual p
lace
of r
esid
ence
in A
ustr
alia
are
not
sho
wn.

9 of 24
Weekly epidemiological report
health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.29) Epub 3/4/2020
Figu
re 3
: Con
firm
ed c
ases
of C
OV
ID-1
9, A
ustr
alia
, by
loca
tion
of u
sual
resid
ence
and
stat
istic
al a
rea
leve
l 3, a
s at 1
Apr
il 20
20a
a Re
pres
ents
the
usua
l loc
atio
n of
resi
denc
e of
a c
ase,
whi
ch d
oes
not n
eces
saril
y m
ean
that
this
is th
e pl
ace
whe
re th
ey a
cqui
red
thei
r inf
ectio
n or
wer
e di
agno
sed.
Ove
rsea
s re
side
nts
who
do
not h
ave
a us
ual p
lace
of r
esid
ence
in A
ustr
alia
are
not
sho
wn.

10 of 24
Weekly epidemiological report
Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.29) Epub 3/4/2020 health.gov.au/cdi
Tabl
e 1:
Cum
ulat
ive
notifi
ed c
ases
of c
onfir
med
CO
VID
-19
and
diag
nost
ic te
sts p
erfo
rmed
, Aus
tral
ia, b
y ju
risd
ictio
n
Juri
sdic
tion
a
Num
ber o
f new
cas
es th
is
repo
rtin
g pe
riod
b (W
eek
endi
ng 2
3:59
AED
T 29
M
arch
202
0)
Tota
l cas
esb
(to
23:5
9 A
EDT
29 M
arch
202
0)Ca
ses
per 1
00,0
00 p
opul
atio
nCu
mul
ativ
e nu
mbe
r of t
ests
pe
rfor
med
(pro
port
ion
of te
sts
posi
tive
%)
NSW
1,21
51,
981
24.5
91,3
08 (2
.2%
)
Vic
360
673
10.2
28,9
41 (2
.3%
)
Qld
376
738
14.5
45,1
07 (1
.6%
)
WA
144
313
11.9
13,3
37 (2
.3%
)
SA16
730
417
.424
,737
(1.2
%)
Tas
3859
11.0
1,72
0 (3
.4%
)
NT
1014
5.7
1,88
1 (0
.7%
)
ACT
4577
18.0
4,23
0 (1
.8%
)
Tota
l 2,
355
4,15
916
.421
1,26
1 (2
.0%
)
a N
SW =
New
Sou
th W
ales
, Vic
= V
icto
ria, Q
ld =
Que
ensl
and,
WA
= W
este
rn A
ustr
alia
, SA
= S
outh
Aus
tral
ia, T
as =
Tas
man
ia, N
T =
Nor
ther
n Te
rrito
ry, A
CT
= Au
stra
lian
Capi
tal T
errit
ory.
b D
ue to
the
dyna
mic
nat
ure
of th
e N
ND
SS, d
ata
in th
is e
xtra
ct a
re s
ubje
ct to
retr
ospe
ctiv
e re
visi
on a
nd m
ay v
ary
from
dat
a re
port
ed in
pre
viou
sly
publ
ishe
d re
port
s an
d re
port
s of
not
ifica
tion
data
by
stat
es
and
terr
itorie
s.

11 of 24
Weekly epidemiological report
health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.29) Epub 3/4/2020
Figu
re 4
: Cas
e nu
mbe
rs a
nd ra
tes o
f CO
VID
-19
case
s, A
ustr
alia
, by
age
and
sex
05101520253035
050100
150
200
250
300
350
400
450
500
0–9
10–1
920
–29
30–3
940
–49
50–5
960
–69
70–7
980
–89
90+
Rate per 100,000
Number of cases
Age
grou
p (y
ears
)
Mal
eFe
mal
eM
ale
rate
Fem
ale
rate
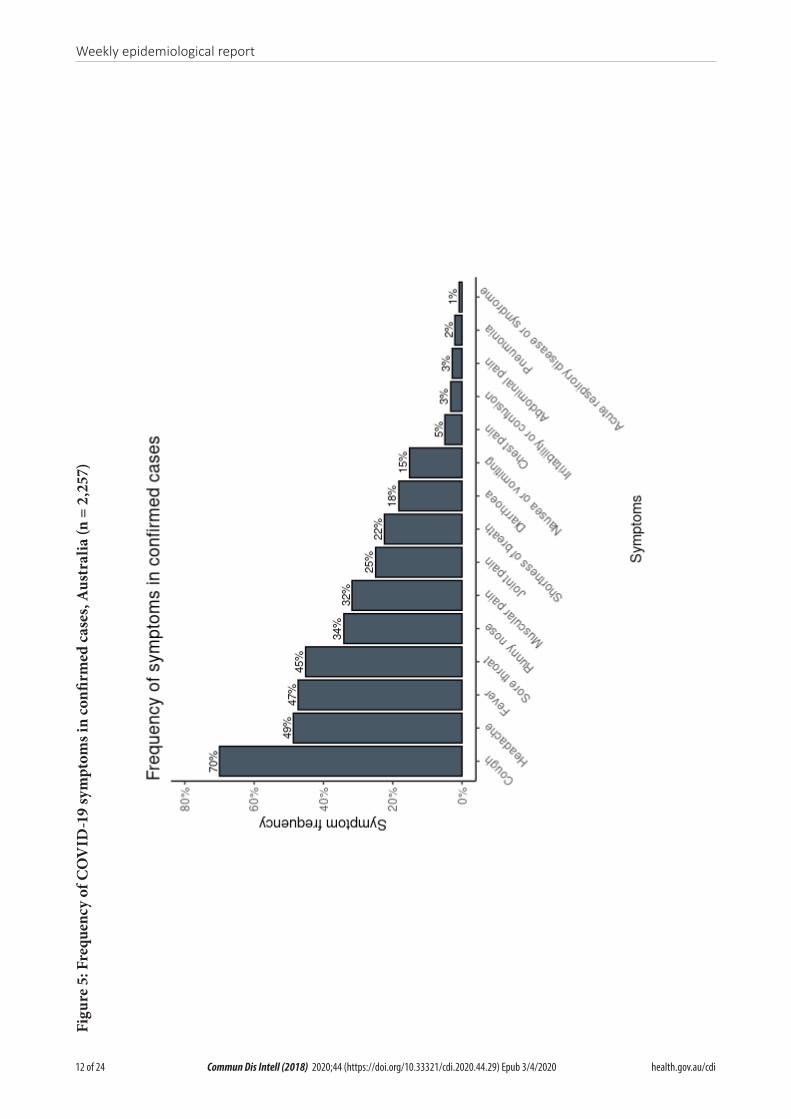
12 of 24
Weekly epidemiological report
Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.29) Epub 3/4/2020 health.gov.au/cdi
Figu
re 5
: Fre
quen
cy o
f CO
VID
-19
sym
ptom
s in
confi
rmed
cas
es, A
ustr
alia
(n =
2,2
57)

13 of 24
Weekly epidemiological report
health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.29) Epub 3/4/2020
Figu
re 6
: Var
iatio
n in
com
bina
tions
of C
OV
ID-1
9 sy
mpt
oms i
n co
nfirm
ed c
ases
, Aus
tral
iaa
a Th
is fi
gure
sho
ws
the
varia
tion
in c
ombi
natio
ns o
f sym
ptom
s ob
serv
ed in
repo
rted
cas
es (n
= 2
,257
) for
the
five
mos
t fre
quen
tly o
bser
ved
sym
ptom
s (c
ough
, hea
dach
e, fe
ver,
sore
thro
at, r
unny
nos
e). T
he
horiz
onta
l bar
s on
the
left
sho
w th
e fr
eque
ncy
of s
ympt
om o
ccur
renc
e in
any
com
bina
tion
with
oth
er s
ympt
oms.
The
circ
les
and
lines
indi
cate
par
ticul
ar c
ombi
natio
ns o
f sym
ptom
s ob
serv
ed in
indi
vidu
al
patie
nts.
The
vert
ical
gre
en b
ars
indi
cate
the
freq
uenc
y of
occ
urre
nce
of th
e co
rres
pond
ing
com
bina
tion
of s
ympt
oms.

14 of 24
Weekly epidemiological report
Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.29) Epub 3/4/2020 health.gov.au/cdi
Figu
re 7
: Num
ber o
f CO
VID
-19
case
s by
plac
e of
acq
uisit
ion
over
tim
e, A
ustr
alia
(n =
4,1
59)a
050100
150
200
250
300
350
400
13-Jan-20
15-Jan-20
17-Jan-20
19-Jan-20
21-Jan-20
23-Jan-20
25-Jan-20
27-Jan-20
29-Jan-20
31-Jan-20
2-Feb-20
4-Feb-20
6-Feb-20
8-Feb-20
10-Feb-20
12-Feb-20
14-Feb-20
16-Feb-20
18-Feb-20
20-Feb-20
22-Feb-20
24-Feb-20
26-Feb-20
28-Feb-20
1-Mar-20
3-Mar-20
5-Mar-20
7-Mar-20
9-Mar-20
11-Mar-20
13-Mar-20
15-Mar-20
17-Mar-20
19-Mar-20
21-Mar-20
23-Mar-20
25-Mar-20
27-Mar-20
29-Mar-20
Number of cases
Date
of i
llnes
s ons
et
Loca
lly a
cqui
red,
not
epi
link
ed
Loca
lly a
cqui
red-
clos
e co
ntac
t of a
con
firm
ed c
ase
Ove
rsea
s acq
uire
d
Und
er in
vest
igat
ion
a Re
cent
ly re
port
ed c
ases
sho
wn
in th
e gr
aph
shou
ld b
e in
terp
rete
d w
ith c
autio
n as
ther
e ca
n be
del
ays
in re
port
ing.

15 of 24
Weekly epidemiological report
health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.29) Epub 3/4/2020
Figu
re 8
: Con
firm
ed c
ases
of o
vers
eas a
cqui
red
CO
VID
-19
infe
ctio
n (n
= 2
,352
) by
Stan
dard
Aus
tral
ian
Cla
ssifi
catio
n of
Cou
ntri
es (S
ACC)
a
050100
150
200
250
13-Jan-20
15-Jan-20
17-Jan-20
19-Jan-20
21-Jan-20
23-Jan-20
25-Jan-20
27-Jan-20
29-Jan-20
31-Jan-20
2-Feb-20
4-Feb-20
6-Feb-20
8-Feb-20
10-Feb-20
12-Feb-20
14-Feb-20
16-Feb-20
18-Feb-20
20-Feb-20
22-Feb-20
24-Feb-20
26-Feb-20
28-Feb-20
1-Mar-20
3-Mar-20
5-Mar-20
7-Mar-20
9-Mar-20
11-Mar-20
13-Mar-20
15-Mar-20
17-Mar-20
19-Mar-20
21-Mar-20
23-Mar-20
25-Mar-20
27-Mar-20
29-Mar-20
Number of cases
Date
of i
llnes
s ons
et
Amer
icas
At se
a (c
ruise
ship
s)Eu
rope
New
Zea
land
and
Pac
ific
Nor
th A
fric
a an
d th
e M
iddl
e Ea
stN
orth
-Eas
t Asia
Sout
h-Ea
st A
siaSo
uthe
rn a
nd C
entr
al A
siaSu
b-Sa
hara
n Af
rica
a Re
cent
ly re
port
ed c
ases
sho
wn
in th
e gr
aph
shou
ld b
e in
terp
rete
d w
ith c
autio
n as
ther
e ca
n be
del
ays
in re
port
ing.

16 of 24
Weekly epidemiological report
Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.29) Epub 3/4/2020 health.gov.au/cdi
Figu
re 9
: Num
ber o
f CO
VID
-19
case
s (lo
gari
thm
ic sc
ale)
by
sele
cted
coun
try
and
days
sinc
e pa
ssin
g 10
0 ca
ses,
up to
29
Mar
ch 2
020
100
1,00
0
10,0
00
100,
000
1,00
0,00
0
01
23
45
67
89
1011
1213
1415
1617
1819
2021
2223
2425
2627
2829
3031
3233
3435
3637
38
Number of cases (log scale)
Days
sin
ce p
assi
ng 1
00 c
ases
Aust
ralia
Italy
Isla
mic
Rep
ublic
of I
ran
Ger
man
yFr
ance
Spai
nU
KU
SARe
publ
ic o
f Kor
eaHo
ng K
ong*
Sing
apor
eJa
pan
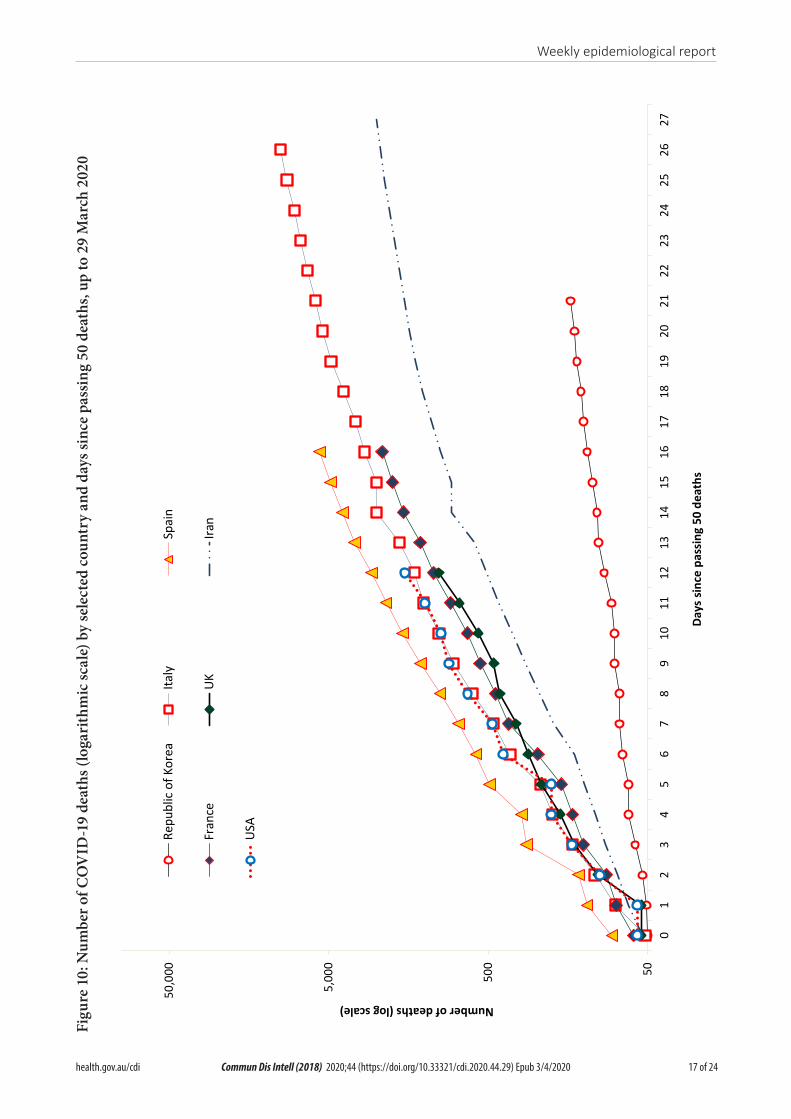
17 of 24
Weekly epidemiological report
health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.29) Epub 3/4/2020
Figu
re 1
0: N
umbe
r of C
OV
ID-1
9 de
aths
(log
arith
mic
scal
e) b
y se
lect
ed co
untr
y an
d da
ys si
nce
pass
ing
50 d
eath
s, up
to 2
9 M
arch
202
0
50500
5,00
0
50,0
00
01
23
45
67
89
1011
1213
1415
1617
1819
2021
2223
2425
2627
Number of deaths (log scale)
Days
sin
ce p
assi
ng 5
0 de
aths
Repu
blic
of K
orea
Italy
Spai
n
Fran
ceU
KIra
n
USA

18 of 24
Weekly epidemiological report
Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.29) Epub 3/4/2020 health.gov.au/cdi
Figu
re 1
1. T
imel
ine
of C
OV
ID-1
9 re
late
d ev
ents
, inc
ludi
ng A
ustr
alia
n pu
blic
hea
lth re
spon
se a
ctiv
ities
, fro
m 3
1 D
ecem
ber 2
019
to 1
5 M
arch
202
0
31 D
ecem
ber 2
019
15 M
arch
2020
31-D
ec-1
9No
tifica
tion t
oW
HO pn
eum
onia
of un
know
n orig
in
7-Ja
n-20
SARS
-CoV
-2 id
entif
ied
11-F
eb-2
0W
HO an
noun
ced a
nam
e for
the
new
coro
navir
us di
seas
e: CO
VID-
19
11-M
ar-2
0W
HO ch
arac
teris
esCO
VID-
19 as
pand
emic
13-M
ar-2
0AH
PPC p
rovid
es re
com
men
datio
ns fo
rpu
blic g
athe
rings
, tes
ting a
nd so
cial d
istan
cing
12-M
ar-2
0AH
PPC p
rovid
es re
com
men
datio
nsfo
r hea
lthca
re an
d age
care
wor
kers
8-M
ar-2
0AH
PPC r
ecom
men
ds re
strict
ions o
nCO
VID-
19 co
ntac
ts an
d tra
velle
rsfro
m lis
ted h
igher
risk c
ount
ries
5-M
ar-2
0Re
strict
ions o
n tra
vel
from
Repu
blic
of Ko
rea
1-M
ar-2
0Re
strict
ions o
n tra
vel
from
Islam
ic Re
publi
c of Ir
an
1-Fe
b-20
Restr
iction
s on t
rave
lfro
m Ch
ina im
plem
ente
d
30-Ja
n-20
WHO
decla
res P
ublic
Hea
lthEm
erge
ncy o
f Inte
rnat
ional
Conc
ern

19 of 24
Weekly epidemiological report
health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.29) Epub 3/4/2020
Figu
re 1
2. T
imel
ine
of C
OV
ID-1
9 re
late
d ev
ents
, inc
ludi
ng A
ustr
alia
n pu
blic
hea
lth re
spon
se a
ctiv
ities
, fro
m 1
5 to
29
Mar
ch 2
020
15 M
arch
2020
29 M
arch
2020
20-M
ar-2
0Ta
sman
ia clo
ses b
orde
rsto
non-
esse
ntial
trav
eller
s
18-M
ar-2
0DF
AT ra
ises t
rave
l adv
ice fo
r all o
verse
asde
stina
tions
to Le
vel 4
'Do N
ot Tr
avel' 18
-Mar
-20
AHPP
C rec
omm
ends
the c
ontin
uatio
n of a
14 da
yqu
aran
tine r
equir
emen
tfo
r all r
etur
ning
trav
eller
s
21-M
ar-2
0Ql
d, W
A, N
T and
SA cl
ose b
orde
rsto
non-
esse
ntial
trav
eller
s
24-M
ar-2
0–
AHPP
C rec
omm
ends
tem
pora
ry su
spen
sion o
f all n
on-u
rgen
t e
lectiv
e pro
cedu
res i
n bot
h the
publi
c and
priva
te se
ctor.
– AH
PPC r
ecom
men
ds pr
ogre
ssive
scale
up of
socia
l dist
ancin
g m
easu
res w
ith st
rong
er m
easu
res i
n rela
tion t
o non
-esse
ntial
gat
herin
gs, a
nd co
nside
ratio
ns of
furth
er m
ore i
nten
se op
tions
. –
Aged
care
prov
iders
limits
visit
s to a
max
imum
of tw
o visi
tors
at o
ne ti
me p
er da
y
25-M
ar-2
0- A
HHPC
reco
mm
ends
that
scho
ol-ba
sed i
mm
unisa
tion
pro
gram
s, wi
th th
e exc
eptio
n of t
he de
liver
y of m
ening
ococ
cal
ACW
Y vac
cine,
are p
ause
d at t
he cu
rrent
tim
e.–A
ustra
lian c
itize
ns an
d Aus
tralia
n per
man
ent r
eside
nts a
re re
strict
ed f
rom
trav
ellin
g ove
rseas
.
26-M
ar-2
0Re
strict
ed m
ovem
ent i
nto c
erta
in re
mot
e are
asto
prot
ect c
omm
unity
mem
bers
from
COVI
D-19
28-M
ar-2
0Al
l peo
ple e
nter
ing A
ustra
lia re
quire
d to u
nder
take
a man
dato
ry 14
-day
quar
antin
e at d
esign
ated
facil
ities
(e.g
. hot
els) i
n the
ir por
t of a
rriva
l.
29-M
ar-2
0Bo
th in
door
and o
utdo
or pu
blic
gath
ering
s lim
ited t
o two
perso
ns on
ly

20 of 24 health.gov.au/cdiCommun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.29) Epub 3/4/2020
Tabl
e 2:
Aus
tral
ian
CO
VID
-19
case
defi
nitio
n20 a
s of 2
9 M
arch
202
0Ve
rsio
n: 2
.4D
ate
of d
evel
opm
ent:
26
Mar
ch 2
020
Confi
rmed
cas
eA
per
son
who
test
s po
sitiv
e to
a v
alid
ated
spe
cific
SA
RS-C
oV-2
nuc
leic
aci
d te
st o
r has
the
viru
s id
entifi
ed b
y el
ectr
on m
icro
scop
y or
vira
l cul
ture
.
Prob
able
cas
e A
per
son
with
feve
r (38
°C) o
r his
tory
of f
ever
(e.g
. nig
ht s
wea
ts, c
hills
) OR
acut
e re
spira
tory
infe
ctio
n (e
.g. c
ough
, sho
rtne
ss o
f bre
ath,
sor
e th
roat
) AN
D w
ho is
a
hous
ehol
d co
ntac
t of a
con
firm
ed o
r pro
babl
e ca
se o
f CO
VID
-19,
whe
re te
stin
g ha
s no
t bee
n co
nduc
ted.
Susp
ect c
ase
A p
erso
n w
ho m
eets
the
follo
win
g ep
idem
iolo
gica
l and
clin
ical
crit
eria
:
Epid
emio
logi
cal c
rite
ria
Clin
ical
cri
teri
aA
ctio
n
Very
hig
h ri
sk
• Cl
ose
cont
act i
n 14
day
s be
fore
illn
ess
onse
t with
a c
onfir
med
or p
roba
ble
case
• In
tern
atio
nal t
rave
l in
the
14 d
ays
prio
r to
illne
ss o
nset
• Cr
uise
shi
p pa
ssen
gers
and
cre
w w
ho h
ave
trav
elle
d in
the
14 d
ays
prio
r to
illne
ss o
nset
Feve
r (≥
38 °C
) or h
isto
ry o
f fe
ver
OR
Acu
te re
spira
tory
infe
ctio
n (e
.g. c
ough
, sho
rtne
ss o
f br
eath
, sor
e th
roat
)
Test
Hig
h ri
sk
1. T
wo
or m
ore
case
s of
illn
ess
clin
ical
ly c
onsi
sten
t with
CO
VID
-19
in th
e fo
llow
ing
sett
ings
:
• A
ged
care
and
oth
er re
side
ntia
l car
e fa
cilit
ies
• M
ilita
ry o
pera
tiona
l set
tings
• Bo
ardi
ng s
choo
ls•
Corr
ectio
nal f
acili
ties
• D
eten
tion
cent
res
• A
borig
inal
rura
l and
rem
ote
com
mun
ities
, in
cons
ulta
tion
with
the
loca
l PH
U•
Sett
ings
whe
re C
OVI
D-1
9 ou
tbre
aks
have
occ
urre
d, in
con
sulta
tion
with
the
loca
l PH
U
2. In
divi
dual
pat
ient
s w
ith il
lnes
s cl
inic
ally
con
sist
ent w
ith C
OVI
D-1
9 in
a g
eogr
aphi
cally
loca
lised
are
a w
ith
elev
ated
risk
of c
omm
unity
tran
smis
sion
, as
defin
ed b
y PH
Us
Feve
r (≥
38 °C
) or h
isto
ry
of fe
ver (
e.g.
nig
ht s
wea
ts,
chill
s)
OR
Acu
te re
spira
tory
infe
ctio
n (e
.g. c
ough
, sho
rtne
ss o
f br
eath
, sor
e th
roat
)
Test
(on
site
fo
r age
d ca
re
resi
dent
s, w
here
fe
asib
le)

21 of 24 health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.29) Epub 3/4/2020
Vers
ion:
2.4
Dat
e of
dev
elop
men
t: 2
6 M
arch
202
0
Mod
erat
e ri
sk•
Hea
lthca
re w
orke
rs, a
ged
or re
side
ntia
l car
e w
orke
rsFe
ver (
≥ 38
°C) o
r his
tory
of
feve
r (e.
g. n
ight
sw
eats
, ch
ills)
OR
Acu
te re
spira
tory
infe
ctio
n (e
.g. c
ough
, sho
rtne
ss o
f br
eath
, sor
e th
roat
)
Test
Back
grou
nd ri
sk(N
o ep
idem
iolo
gica
l ris
k fa
ctor
s)H
ospi
talis
ed p
atie
nts
with
fe
ver (
≥ 38
°C)
AN
D
Acu
te re
spira
tory
sym
ptom
s (e
.g. c
ough
, sho
rtne
ss o
f br
eath
, sor
e th
roat
) of a
n un
know
n ca
se
Test

22 of 24
Weekly epidemiological report
Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.29) Epub 3/4/2020 health.gov.au/cdi
References
1. Moriarty LF, Plucinski MM, Marston BJ, Kur-batova EV, Knust B, Murray EL et al. Public health responses to COVID-19 outbreaks on cruise ships – worldwide, February–March 2020. MMWR Morb Mortal Wkly Rep. 2020;69(12):347–52.
2. World Health Organization (WHO). Coro-navirus disease 2019 (COVID-19) situa-tion report – 69: 29 March 2020. Geneva: WHO; 2020. [Accessed on 30 March 2020.] Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200329-sitrep-69-covid-19.pdf.
3. WHO. Report of the WHO-China joint mission on coronavirus disease 2019 (COV-ID-19). Geneva: WHO; 2020. [Accessed on 1 March 2020.] Available from: https://www.who.int/docs/default-source/coronaviruse/who-china-joint-mission-on-covid-19-final-report.pdf.
4. Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z et al. Clinical course and risk factors for mortal-ity of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020. doi: https://doi.org/10.1016/S0140-6736(20)30566-3.
5. Bi Q, Wu Y, Mei S, Ye C, Zou X, Zhang Z et al. Epidemiology and transmission of COVID-19 in Shenzhen China: analysis of 391 cases and 1286 of their close contacts. medRxiv. 2020. doi: https://doi.org/10.1101/2020.03.03.20028423.
6. Li R, Pei S, Chen B, Song Y, Zhang T, Yang W et al. Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus (SARS-CoV2). Science. 2020. doi: https://doi.org/10.1126/science.abb3221.
7. WHO. Coronavirus disease 2019 (COV-ID-19) situation report – 29: 18 February 2020. Geneva: WHO; 2020. [Accessed on 15 March 2020.] Available from: https://www.
who.int/docs/default-source/coronaviruse/situation-reports/20200218-sitrep-29-cov-id-19.pdf.
8. Eden JS, Rockett R, Carter I, Rahman H, de Ligt J, Hadfield J et al. An emergent clade of SARS-CoV-2 linked to returned travellers from Iran. bioRxiv. 2020. doi: https://doi.org/10.1101/2020.03.15.992818.
9. Sun P, Qie S, Liu Z, Ren J, Xi JJ. Clinical char-acteristics of 50466 patients with 2019-nCoV infection. medRxiv. 2020. doi: https://doi.org/10.1101/2020.02.18.20024539.
10. Li Y, Bai W, Hashikawa T. The neuroinvasive potential of SARS-CoV2 may be at least par-tially responsible for the respiratory failure of COVID-19 patients. J Med Virol. 2020. doi: https://doi.org/10.1002/jmv.25728.
11. Woelfel R, Corman VM, Guggemos W, Seil-maier M, Zange S, Mueller MA et al. Clini-cal presentation and virological assessment of hospitalized cases of coronavirus disease 2019 in a travel-associated transmission clus-ter. medRxiv. 2020. doi: https://doi.org/10.1101/2020.03.05.20030502.
12. Inciardi RM, Lupi L, Zaccone G, Italia L, Raffo M, Tomasoni D et al. Cardiac in-volvement in a patient with coronavirus disease 2019 (COVID-19). JAMA Cardiol. 2020. doi: https://doi.org/10.1001/jamacar-dio.2020.1096.
13. Guo T, Fan Y, Chen M, Wu X, Zhang L, He T et al. Cardiovascular implications of fatal outcomes of patients with coronavirus disease 2019 (COVID-19). JAMA Cardiol. 2020. doi: https://doi.org/10.1001/jamacar-dio.2020.1017.
14. Madjid M, Safavi-Naeini P, Solomon SD, Vardeny O. Potential effects of coronaviruses on the cardiovascular system: a review. JAMA Cardiol. 2020. doi: https://doi.org/10.1001/jamacardio.2020.1286.

23 of 24
Weekly epidemiological report
health.gov.au/cdi Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.29) Epub 3/4/2020
15. WHO. Clinical management of severe acute respiratory infection when novel coronavirus (nCoV) infection is suspected. [Internet.] Geneva: WHO; 2020. [Accessed on 23 Febru-ary 2020.] Available from: https://www.who.int/publications-detail/clinical-management-of-severe-acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-sus-pected.
16. Harrison, C. Coronavirus puts drug re-purposing on the fast track. Nat Biotechnol. 2020. doi: https://doi.org/10.1038/d41587-020-00003-1.
17. Australian Government Department of Health. Australian Health Protection Princi-pal Committee (AHPPC) advice to National Cabinet on 24 March 2020: a statement from the Australian Health Protection Principal Committee about the temporary suspension of all non-urgent elective surgery. [Internet.] Canberra: Australian Government Depart-ment of Health; 24 March 2020. [Accessed on 1 April 2020.] Available from: https://www.health.gov.au/news/australian-health-protec-tion-principal-committee-ahppc-advice-to-national-cabinet-on-24-march-2020.
18. Australian Government Department of Health. Read the latest statements from the Australian Health Protection Principal Committee (AHPPC) about coronavirus (COVID-19). [Internet.] Canberra: Austral-ian Government Department of Health; 24 March 2020. [Accessed on 1 April 2020.] Available from: https://www.health.gov.au/news/australian-health-protection-principal-committee-ahppc-advice-to-national-cabi-net-on-24-march-2020-0.
19. Australian Government Department of Home Affairs. COVID-19 and the border: airline industry and passengers. [Internet.] Canberra: Australian Government Depart-ment of Home Affairs; 2020. [Accessed on 1 April 2020.] Available from: https://covid19.homeaffairs.gov.au/airline-industry-and-passengers.
20. Australian Government Department of Health. Novel coronavirus 2019 (2019-nCoV) - CDNA national guidelines for public health units. [Internet.] Canberra: Australian Government Department of Health; 2020. [Accessed on 24 March 2020.] Available from: https://www1.health.gov.au/internet/main/publishing.nsf/Content/7A8654A8CB144F5FCA2584F8001F91E2/$File/interim-COVID-19-SoNG-v2.4.pdf.

24 of 24
Weekly epidemiological report
Commun Dis Intell (2018) 2020;44 (https://doi.org/10.33321/cdi.2020.44.29) Epub 3/4/2020 health.gov.au/cdi
Appendix A: Frequently asked questions
Q: Can I request access to the COVID-19 data behind your CDI weekly reports?
A: National notification data on COVID-19 con-firmed cases is collated in the National Notifiable Disease Surveillance System (NNDSS) based on notifications made to state and territory health authorities under the provisions of their relevant public health legislation.
Normally, requests for the release of data from the NNDSS requires agreement from states and ter-ritories via the Communicable Diseases Network Australia, and, depending on the sensitivity of the data sought and proposed, ethics approval may also be required.
Due to the COVID-19 response, unfortunately, spe-cific requests for NNDSS data have been put on hold. We are currently looking into options to be able to respond to data requests in the near future.
We will continue to publish regular summaries and analyses of the NNDSS dataset and recommend the following resources be referred to in the meantime:
• NNDSS summary tables: http://www9.health.gov.au/cda/source/cda-index.cfm
• Daily case summary of cases: https://www.health.gov.au/news/health-alerts/novel-coronavirus-2019-ncov-health-alert/coronavirus-covid-19-current-situation-and-case-numbers
• Communicable Diseases Intelligence COVID-19 weekly epidemiology report: https://www1.health.gov.au/internet/main/publishing.nsf/Content/novel_coronavirus_2019_ncov_weekly_epidemiology_reports_australia_2020.htm
• State and territory public health websites.
Q: Can I request access to data at post-code level of confirmed cases?
A: Data at this level cannot be released without eth-ics approval and permission would need to be sought from all states and territories via the Communicable Diseases Network Australia. As noted above, specific requests for NNDSS data are currently on hold.
A GIS/mapping analysis of cases will be included in each Communicable Diseases Intelligence COVID-19 weekly epidemiology report. In order to protect privacy of confirmed cases, data in this map will be presented at SA3 level.
Q. Where can I find more detailed data on COVID-19 cases?
A: We are currently looking into ways to provide more in-depth epidemiological analyses of COVID-19 cases, with regard to transmission and severity, including hospitalisation. These analyses will continue to be built upon in future iterations of the weekly Communicable Diseases Intelligence report.
Top Related