







Languages
Pages
Legal


ETIOLOGY OF PERIODONTAL
DISEASE
ETIOLOGY OF PERIODONTAL DISEASE
• The clinical manifestations of periodontal disease result form a complex interplay between bacteria found in dental plaque and the host tissues.
• Etiological factors in periodontal disease are classified into two broad categories, depending on their specific origin.

Primary Local Factors (dental plaque Secondary (plaque retention factors)
Systemic factors (modify the response of the gingiva to local factor)
ETIOLOGY
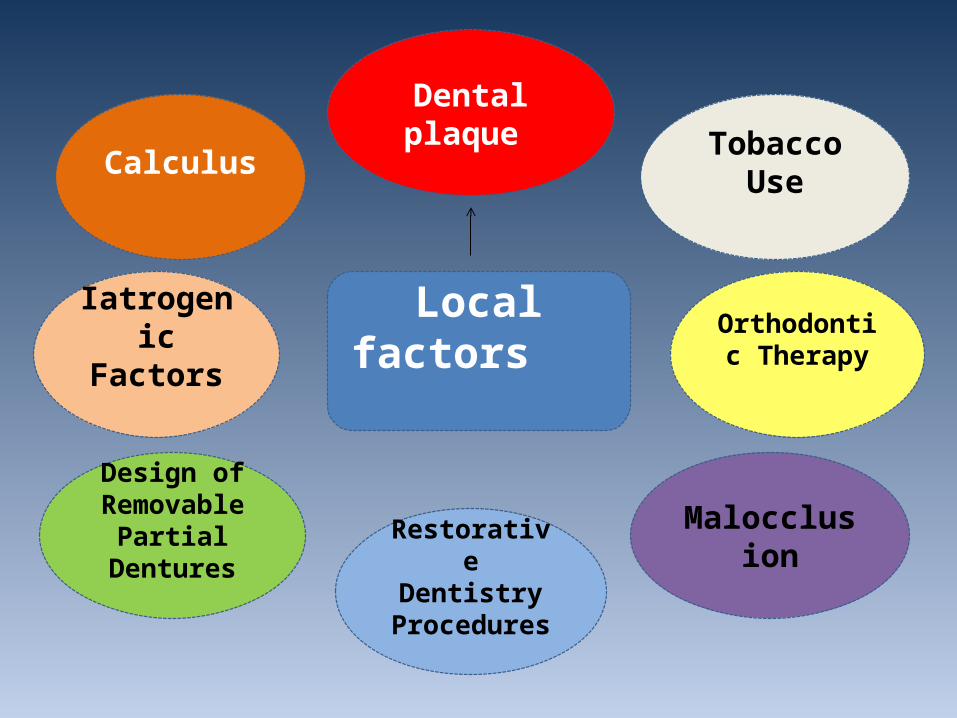
Local factors
Dental plaque
Tobacco UseCalculus
Orthodontic Therapy
Iatrogenic Factors
Restorative Dentistry
Procedures
Malocclusion
Design of Removable
Partial Dentures
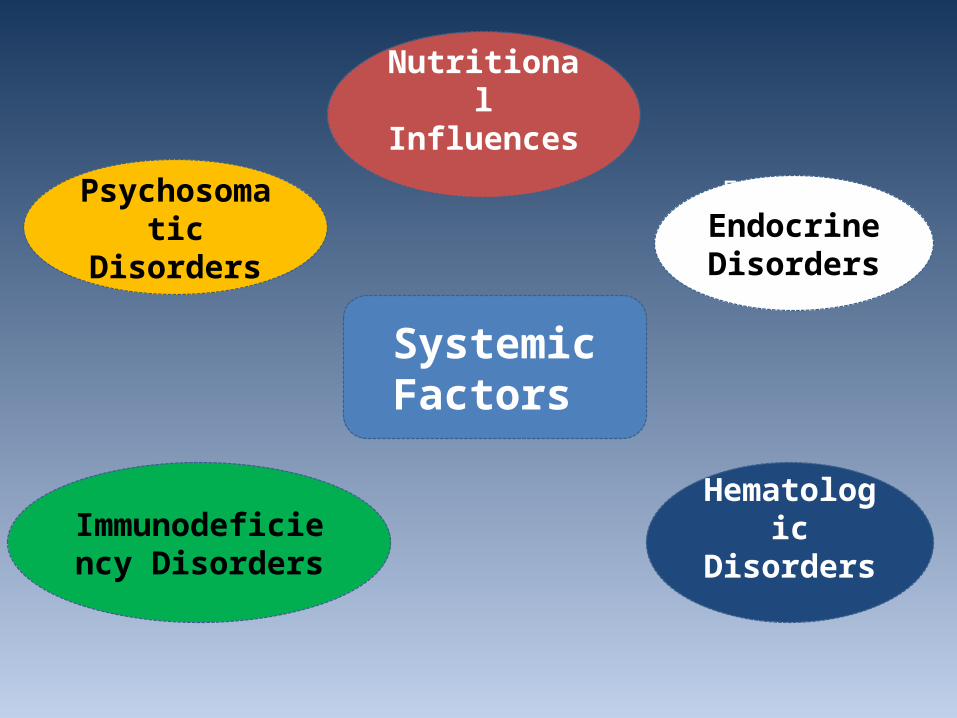
Systemic Factors
Nutritional Influences
Endocrine EndocrineDisorders
Psychosomatic Disorders
Immunodeficiency Disorders
Hematologic Disorders

Dental Plaque
Dental plaque can be defined as the soft deposits that form the biofilom adhering to the tooth surface or other hard surfaces in the oral cavity, including removable and fixed restorations.

Supragingival plaque Sub gingival plaque
Marginal plaque

• The different regions of plaque are significant to different processes associated with diseases of the teeth and periodontum.
Plaque Composition1_Microorganisms which exits within an intercellular
matrix. Gram positive: S. sanguis, A. viscousus. (initial colonizers)
Gram negative: P. intermedia, F.nucleatum.(secondary colonizers)
Plaque Composition2_The intercellular matrix consists of : • Organic constituents of the matrix include
polysaccharides, proteins, glycoproteins and lipid material.
• Inorganic component of plaque is predominately calcium and phosphorus and other minerals such as sodium, potassium and fluoride

• White, greyish or yellow in colour.• Globular appearance.• ON gingival third of the tooth surface.
Clinical fissure

Plaque Formation
• Dental pellicle.• Initial colonization( G. positive)• The plaque mass matures (colonization and growth of
additional species)• G .negative anaerobic.
• Dental plaque may be visualized on teeth after 1 or 2 days without oral hygiene measures.

Association between plaque microorganisms and Periodontal Diseases.
a. Nonspecific plaque hypothesis : that periodontal disease results from the elaboration of noxious products by the entire plaque flora.
b. Specific Plaque Hypothesis: that only certain plaque is pathogenic and its pathogenicity depends on the presence or increase in specific microorganisms.
Predisposing Factors
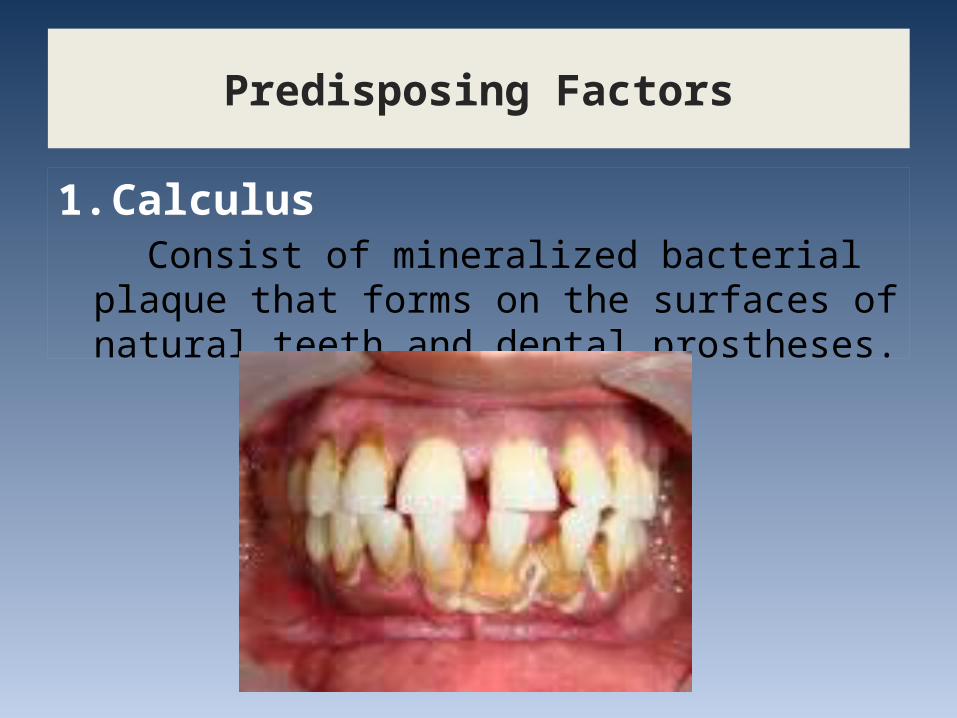
1. Calculus Consist of mineralized bacterial plaque that forms on
the surfaces of natural teeth and dental prostheses.

Supragingival Calculus
Sub gingival Calculus

Supra gingival calculus mostly formed in the buccal surfaces of the maxillary molars and the lingual surfaces of the mandibular anterior teeth.
When the gingival tissues recede, sub gingival
calculus becomes exposed.

Formation of calculus
Between the first and 14th days of plaque formation(4 to 8 hours).
Saliva supra gingival calculus G. Fluid sub gingival calculus.
Calcification begins along the inner surface of the plaque.
Etiologic Significance
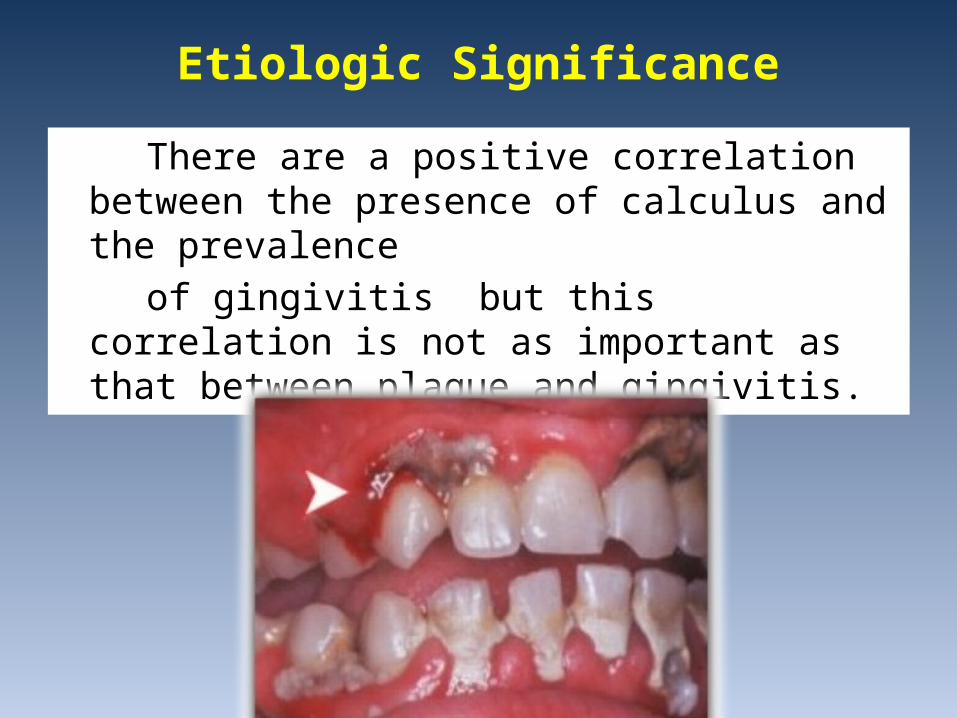
There are a positive correlation between the presence of calculus and the prevalence
of gingivitis but this correlation is not as important as that between plaque and gingivitis.
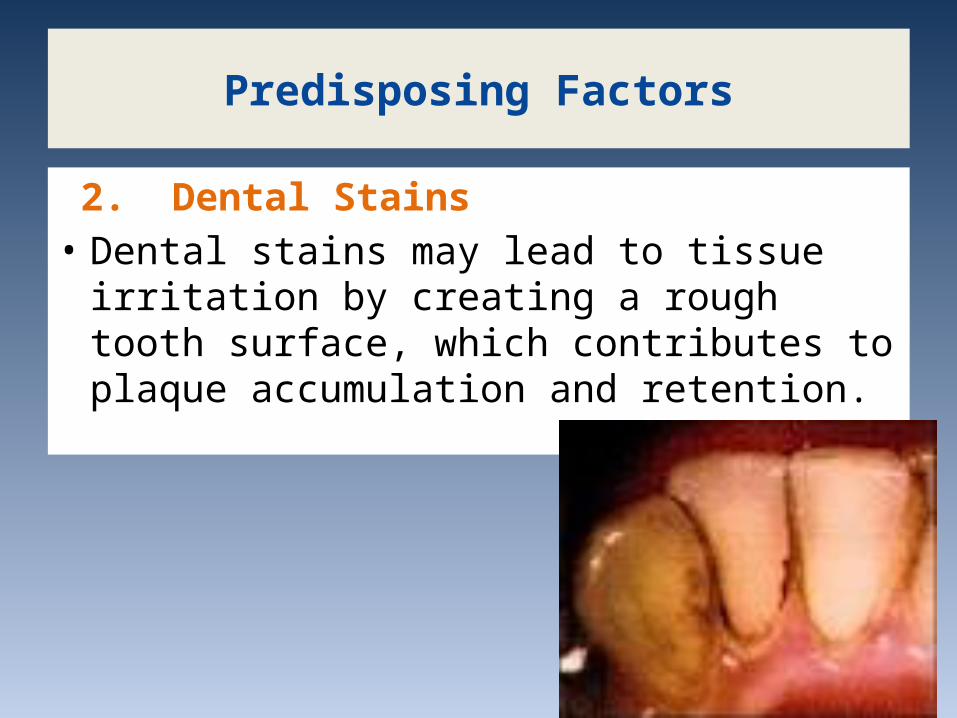
2. Dental Stains• Dental stains may lead to tissue irritation by
creating a rough tooth surface, which contributes to plaque accumulation and retention.
Predisposing Factors
3. Iatrogenic Factors Deficiencies in the quality of dental
restorations or prostheses are contributing factors for gingival inflammation and periodontal destruction.
Predisposing Factors

a. Over hanging Margins of Restorations .
Iatrogenic Factors

Iatrogenic Factors
b. Over contoured crown : Over contoured crowns and restorations
tend to accumulate plaque possibly prevent the self- cleaning mechanisms of the adjacent cheek, lips and tongue.

Iatrogenic Factors c. Open Contacts:• Food particles create a favourable environment
for plaque accumulation. • Acts as a direct mechanical irritant to the tissue.

Predisposing Factors
4 .Design of removable partial dentures

5. Restoratives dentistry procedures
Predisposing Factors
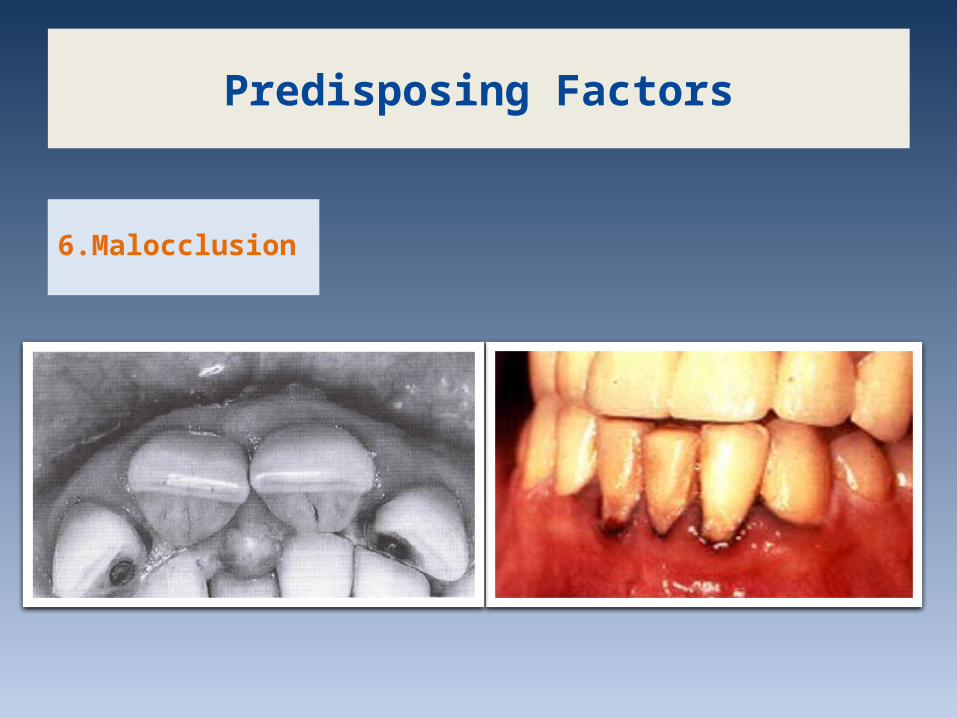
6.Malocclusion
Predisposing Factors
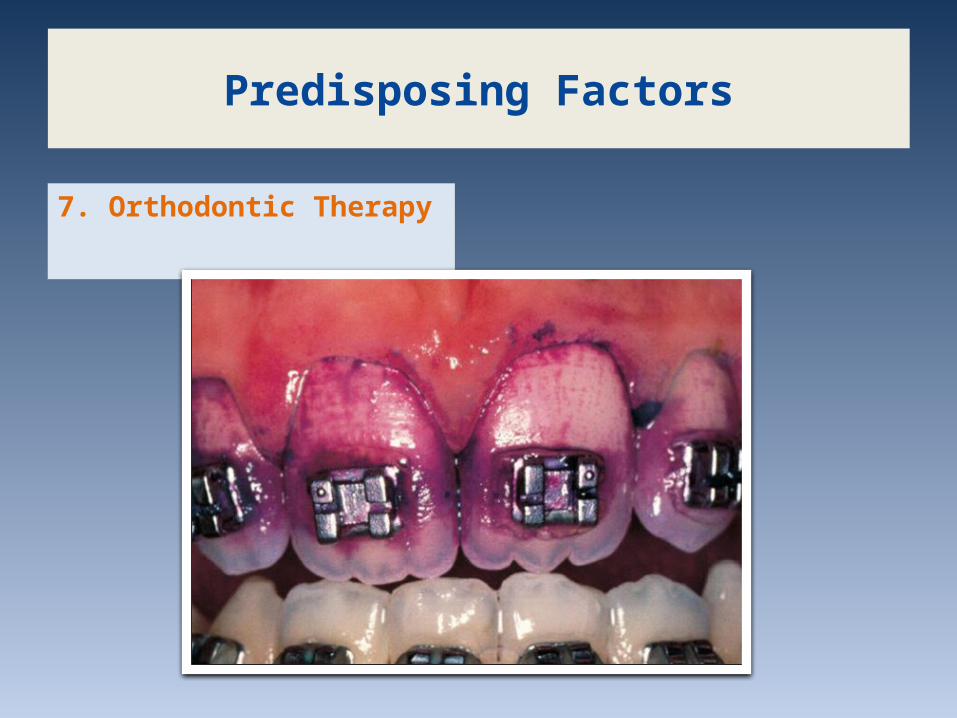
7. Orthodontic Therapy
Predisposing Factors

8. Tooth Brush Trauma
Predisposing Factors

9. Tobacco usethe smokers had more sites with:Deep pockets Greater attachment loss and severe periodontal disease.
Predisposing Factors

Effects of tobacco use:
• Diminish host response and increase disease susceptibility. • Less numbers of T- lymphocytes and less antibody
production and serum levels of IgG. • Reduce serum IgG antibobies to P. intermedia and F.
nucleatum.
• Diminish neutrophils chemotaxis, phagocytosis or both.
• Nicotina decrease gingival blood flow.
Bibliography
Carranza´s. Clinical Periodontology. 9th ed. 2003. pg:15-55.
Gururaja R. Textbook of Periodontology. 2nd ed. pg: 6. Klaus H. Color Atlas of Dental Medicine.
Periodontology. Vol 1. 1989. pg: 1- 10.
Top Related