






Languages
Pages
Legal


Epstein-Barr associated acute cerebellar ataxia in an adult
Adam N Hofer, MD, MPH; Joan Addington-White, MD University of Wisconsin-Hospitals & Clinics
Introduction
Case Description
Acute&cerebellar&ataxia&(ACA)&is&a&rare,&o3en&self6limi8ng,&inflammatory&disease&that&can&be&triggered&by&both&infec8ous&and&non6infec8ous&processes.&ACA&is&one&of&several&known¢ral&nervous&system&(CNS)&complica8ons&of&an&Ebstein6Barr&viral&(EBV)&infec8on.&Here,&we&present&a&case&of&ACA&as&the&primary&manifesta8on&of&a&primary&EBV&infec8on&without&the&classical&features&of&infec8ous&mononucleosis.&&
A&706year6old&ac8ve&and&generally&healthy&woman&presented&to&her&primary&care&physician&with&a&26week&history&of&progressive&gait&disturbance.&Her&symptoms&began&following&the&onset&of&a&self6limi8ng&diarrheal&illness&while&traveling&to&New&York&City.&Her&unsteadiness&worsened&to&the&point&that&she&had&several&falls&and&required&assistance&for&ambula8on.&She&had&no&other&localizing&infec8ous&symptoms&and&denied&changes&in&mental&status.&She&had&a&history&of&hypertension&and&osteoporosis.&There&had&been&no&recent&medica8on&changes.&She&had&no&family&history&of&ataxia&or&other&neurological&disorders.&&&&On&examina8on,&she&was&afebrile&(36.3°&C)&and&hemodynamically&stable.&Cardiopulmonary&and&abdominal&examina8ons&were&normal.&There&was&no&cervical&lymphadenopathy&or&tonsillar&exudates.&She&had&no&dysarthria&or&nystagmus.&She&had&a&wide6based,&unsteady&gait&and&was&unable&to&walk&without&assistance.&She&also&had&mild&dysdiadochokinesia&on&finger6to6nose&tes8ng.&Romberg&test&was&nega8ve.&&&&Complete&blood&count&was¬able&for&a&leukocytosis&(11.5&K/uL),&lymphocytosis&(6580/uL),&and&mild&thrombocytosis&(430&K/uL).&A&blood&smear&demonstrated&reac8ve&lymphocytes.&A&basic&metabolic&panel&was&normal.&C6reac8ve&protein&was&mildly&elevated&(2&mg/dL);&ESR&was&normal.&B12&and&TSH&were&normal.&An&MRI&of&the&brain&was¬able&for&ventriculomegaly,&le3&greater&than&right;&of¬e,&there&was&no&cerebellar&enhancement.&Due&to&concern&for&an&atypical&presenta8on&of&normal&pressure&hydrocephalus&(NPH),&she&underwent&lumbar&puncture&(LP)&with&cerebrospinal&fluid&(CSF)&removal.&She&did¬&have&significant&improvement&in&her&ataxia&following&lumbar&puncture&per&physical&therapy.&CSF&analysis&subsequently&revealed&only&two&nucleated&cells,&elevated&protein&at&59&mg/dl&(15645),&and&posi8ve&EBV&qualita8ve&PCR&(Table&1).&As&such,&serum&EBV&serology&was&ordered&and¬able&for&posi8ve&EBV&viral&capsid&an8gen&(VCA)&IgM&confirming´&EBV&infec8on&(Table&2).&Given&lack&of&significant&improvement&in&ataxia&with&CSF&removal&and&posi8ve&EBV&serology,&it&was&felt&that&her&presenta8on&was&most&consistent&with&EBV6associated&ACA.&&&Her&ataxia&improved&gradually&with&non6pharmacologic&therapy&and&had&completely&resolved&within&ten&weeks&at&8me&of&outpa8ent&follow6up.&&&
Discussion
We&report&a&case&of´&cerebellar&ataxia&(ACA)&as&the&primary&manifesta8on&of´&Epstein6Barr&virus&(EBV)&infec8on&in&a&706year6old&female.&In&retrospect,&the&pa8ent&in&our&case&reported&mild&fa8gue&and&a&sore&throat&at&the&onset&of&her&symptoms.&However,&while&rare,&ACA&can&present&without&the&systemic&manifesta8ons&of&infec8ous&mononucleosis&(IM)&such&as&fever,&pharyngi8s,&lymphadenopathy,&and&fa8gue.1&ACA&is&one&of&several&known&neurological&complica8ons&of&EBV&(Table&3),&which&can&be&seen&in&up&to&7.3&percent&of&pa8ents&with&EBV.2&&&&ACA&is&rare&(incidence&1&in&1006500k)&and&most&commonly&affects&children.&In&adults,&ACA&has&a&male&predominance&and&typically&affects&pa8ents&less&than&30&years&of&age.3,4&However,&as&in&our&case,&ACA&has&been&documented&in&pa8ents&in&their&70s.5&The&pathogenesis&is&incompletely&understood,&however,&two&mechanisms&have&been&speculated:&(1)&a&delayed&post6infec8ous&autoimmune&process,&(2)&direct&viral&infec8on&of&the&cerebellum.1,2,5&&The&detec8on&of&viral&DNA&in&CSF&in&our&case&would&support&the&laher.&&&The&differen8al&diagnosis&for&ACA&in&an&adult&is&broad,&and&includes&infec8ous,&neoplas8c,¶neoplas8c,&inflammatory,&and&toxic&e8ologies&(Table&4).1&In&this&case,´&EBV&infec8on&was&concluded&to&be&the&causa8ve&agent&based&on&posi8ve&EBV&viral&capsid&an8gen&IgM&in&the&serum.&Repeat&EBV&serology&approximately&10&weeks&a3er&diagnosis&was¬able&for&nega8ve&EBV&VCA&IgM&and&posi8ve&EBV&VCA&IgG,&consistent&with&resolving´&infec8on&(Table&2).&&&&MRI&is&the&most&commonly&performed&imaging&modality&in&pa8ents&with´&ataxia&and&may&demonstrate&bilateral&or&unilateral&diffuse&cerebellar&abnormali8es&(Figure&2);&however,&brain&MRI&is&unrevealing&in&the&majority&of&pa8ents&with&ACA&and&abnormal&imaging&lacks&both&specificity&and&prognos8c&value.6,7&Our&pa8ent&was¬ed&to&have&ventriculomegaly,&thus&ini8ally&raising&concern&for&normal&pressure&hydrocephalus&(NPH).&However,&hydrocephalus&has&been&reported&in&up&to&42&percent&of&pa8ents&in&one&case&series.6&&&&ACA&secondary&to&EBV&infec8on&is&usually&a&benign,&self6limi8ng&inflammatory&condi8on&that&can&most&o3en&be&treated&with&suppor8ve&therapy.&Complete&recovery&is&most&o3en&seen&within&3613&weeks.8&However,&obstruc8ve&hydrocephalus&and&chronic&cerebellar&atrophy&have&been&reported.6&&Treatment&has&commonly&included&cor8costeroids&and/or&an86viral&though&there&is¤tly&insufficient&evidence&to&support&the&use&of&either&in&the&treatment&of&ACA.2,9&Our&pa8ent&was&treated&with&suppor8ve&therapy&and&made&a&complete&recovery&a3er&approximately&ten&weeks.&&
References 1. McCarthy&CL,&McColgan&P,&Mar8n&P.&Acute&cerebellar&ataxia&due&to&Epstein6Barr&virus.&Pract&Neurol.&2012&Aug;12(4):238640.&doi:&10.1136/practneurol620116000115.&No&
abstract&available.&Erratum&in:&Pract&Neurol.&2012&Dec;12(6):399.&&2. Ali&K,&Lawthom&C.&Epstein6Barr&virus6associated&cerebellar&ataxia.&BMJ&Case&Rep.&2013&Apr&22;2013.&doi:pii:&bcr2013009171.&10.1136/bcr620136009171.&&3. Davis&DP,&Marino&A.&Acute&cerebellar&ataxia&in&a&toddler:&case&report&and&literature&review.&J&Emerg&Med.&2003&Apr;24(3):28164.&Review.&&4. Klockgether&T,&Döller&G,&Wüllner&U,&Petersen&D,&Dichgans&J.&Cerebellar&encephali8s&in&adults.&J&Neurol.&1993&Jan;240(1):17620.&&5. Fujimoto&H,&Asaoka&K,&Imaizumi&T,&Ayabe&M,&Shoji&H,&Kaji&M.&Epstein6Barr&virus&infec8ons&of&the¢ral&nervous&system.&Intern&Med.&2003&Jan;42(1):33640.&&6. De&Bruecker&Y,&Claus&F,&Demaerel&P,&Ballaux&F,&Sciot&R,&Lagae&L,&Buyse&G,&Wilms&G.&MRI&findings&in´&cerebelli8s.&Eur&Radiol.&2004&Aug;14(8):1478683.&Epub&2004&Feb&
13.&Review.&&7. Park&KM,&Kim&SE,&Kim&SE.&An&elderly&case&of´&cerebelli8s&a3er&alleged&vaccina8on.&J&Mov&Disord.&2012&May;5(1):2163.&doi:&10.14802/jmd.12006.&Epub&2012&May&30.&&8. Erzurum&S,&Kalavsky&SM,&Watanakunakorn&C.&Acute&cerebellar&ataxia&and&hearing&loss&as&ini8al&symptoms&of&infec8ous&mononucleosis.&Arch&Neurol.&1983&Nov;40(12):
76062.&&9. Van&Lierde&A,&Righini&A,&Tremola8&E.&Acute&cerebelli8s&with&tonsillar&hernia8on&and&hydrocephalus&in&Epstein6Barr&virus&infec8on.&Eur&J&Pediatr.&2004&Nov;163(11):
689691.&Epub&2004&Aug&12.&&
Conclusions
• Acute&Cerebellar&Ataxia&(ACA)&is&a&rare,&usually&self6limi8ng&inflammatory&syndrome&characterized&by&cerebellar&dysfunc8on&(e.g.,&gait&disturbance,&dysmetria)&
• EBV&may&cause&ACA&in&adults&and&ataxia&may&be&the&sole&manifesta8on&of&a&primary&EBV&infec8on&
• Conven8onal&MRI&is&o3en&normal&during&an´&infec8on&though&may&demonstrate&cerebellar&swelling&or&hydrocephalus&
• Treatment&is&suppor8ve;&there&is¤tly&insufficient&evidence&to&support&the&rou8ne&use&of&cor8costeroids&or&an86viral&medica8ons&&&
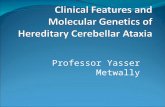
Figure&1:&Axial&T16weighted&sec8on&MRI&image&showing&ventriculomegaly&in&our&pa8ent&
A&
P&
Table 2: EBV Serology Day 0 Day 77
EBV VCA IgM + - EBV VCA IgG - + EBV EA IgG - - EBNA - - VCA, viral capsid antigen; EA, early antigen; EBNA, EBV nuclear antigen
Table 4: Causes of Acute Cerebellar Ataxia Vascular Infarction, hemorrhage, Vasculitis
Inflammatory MS, Acute disseminated encephalomyelitis
Toxic Alcohol, Drugs Neoplastic Posterior fossa space occupying lesions
Paraneoplastic Anti-Yo, Anti-Hu, Anti-Ri, anti-Tr, anti-VGCC, anti-Ma, Anti-Ta/M2, anti-CRMPS/CV2, anti-mGluRi
Infectious
EBV, VZV, mumps, Mycoplasma pneumonia, Japanese encephalitis virus, Legionella, Coxsackie virus, HIV, poliovirus
Genetic Episodic ataxia 1 and 2 MS, Mutliple sclerosis, EBV, Epstein-Barr Virus; VZV, varicella zoster virus (Source: McCarthy et al, 2012)
Table 1: Results of LP & CSF analysis
Opening pressure 18 cm H2O Closing pressure 9 cm H2O Removed CSF volume 28 mL
Protein 59 mg/dL (15-45) Glucose 52 mg/dL (40-80) Nucleated Cells 2 /uL CSF Culture Negative EBV PCR Positive Enterovirus PCR Negative HSV PCR Negative Paraneoplastic Autoantibodies Negative EBV, Ebstein-barr Virus; HSV, Herpes-simplex virus
1479
Case 2
A 4-year-old girl was admitted to the hospital with a 3-week histo-ry of headache, fever and neck stiffness. Blood examinationshowed 6,750 leucocytes/mm3 and a CRP of 0.2 mg/dl. Serologi-cal tests were negative. CSF analysis revealed an elevated proteinconcentration (463 mg/l) and 15 leucocytes/mm3. A bronchus as-pirate was positive for influenza virus. Brain CT revealed a lesionin the left cerebellar hemisphere. MRI on day 7 showed abnormal-ities in both cerebellar hemispheres and in the vermis (Fig. 2),with a subtle pial contrast enhancement. The influenza virus(blood titer >1/128) was thought to have triggered the acute cere-bellitis. A follow-up MR examination performed 2 months latershowed residual changes in the left cerebellar hemisphere and aslight dilatation of the fourth ventricle.
Case 3
An 11-year-old girl was referred to the emergency departmentwith a 1-week history of progressive generalized weakness, fever,diarrhea and a productive cough. Cerebellar signs consist of a dys-arthric speech, dysmetria, an ataxic gait and horizontal nystagmus.CT was normal. Blood examination showed an elevated CRP(6.2 mg/dl). Serological tests were negative. Analysis of the CSFshowed an elevated protein content (566 mg/l) and 51 leuco-cytes/mm3. MRI, performed 6 days after admission, was normal,but 1 month later a slight dilatation of the fourth ventricle could beseen (Fig. 3). The patient was discharged 45 days after admissionwith persistent dysarthria and ataxia. Follow-up MRI, 1 year afterthe initial presentation, revealed widening of the folia and thefourth ventricle, indicating severe cerebellar atrophy (Fig. 3).
Case 4
A 26-year-old woman with severe headache and fever was re-ferred to the emergency department. She developed intermittent
diplopia, an ataxic gait and dysarthric speech. Blood examinationdisclosed 21,200 leucocytes/mm3 and a CRP of 6.2 mg/dl. CSFanalysis showed an increased protein concentration (800 mg/l) and138 leucocytes/mm3. Serological tests were negative. Brain CTwas normal. She was treated with antibiotics. One week after ad-mission, an acute neurological deterioration was observed and shebecame unconscious. Fundoscopy revealed bilateral papilledema.CRP had risen up to 13.5 mg/dl. Because of progressive swellingof the cerebellum and acute obstructive hydrocephalus, a ventricu-lostomy was performed. MRI revealed diffuse increased signal inboth cerebellar hemispheres (Fig. 4a) with a diffuse pial contrastenhancement (Fig. 4b). A posterior fossa decompression was nec-essary and a biopsy of the right cerebellar hemisphere and menin-ges was performed (Fig. 4c). Dura mater, arachnoidea and cerebel-lar parenchyma were infiltrated by a predominantly lymphocyticinflammatory infiltrate. MRI, 9 days after the posterior fossa de-compression, showed residual T2-signal alterations in both cere-bellar hemispheres and a normalization of the ventricles. Therewas a clinical improvement with only mild cerebellar signs 2months later.
Discussion
Acute cerebellitis (AC) is characterized by an acute orsubacute onset of cerebellar ataxia following an infectionor vaccination. Most common presenting symptoms in-clude truncal ataxia, dysmetria and headache. To ourknowledge, MR findings for 29 patients with acute cere-bellitis, in the absence of cerebral or brainstem lesions,have been reported in the literature. Table 1 illustratesthose 29 patients, including the four cases of thismanuscript [4–25]. The mean and median age at the timeof diagnosis of the 33 patients was, respectively, 13 and11 years (range 1–64 years). Varicella, measles, mumps
Fig. 1 Axial T2-weighted image at initial presentation shows in-creased signal intensity in the left cerebellar hemisphere
Fig. 2 Axial T2-weighted image at initial presentation showsmarked abnormal areas of increased signal intensity in both cere-bellar hemispheres and the vermis
Figure&2:&Axial&T26weighted&image&showing&increased&signal&intensity&in&bilateral&cerebellar&hemispheres&and&vermis.6&(Source:&D&Bruecker&et&al,&2004)&
1&
2&
Table 3: Neurological Complications of EBV Meningitis Encephalitis Mononeuritis Guillain-Barre Syndrome Ophthalmoplegia Optic neuritis Acute demyelinating encephalomyelitis (ADEM) Acute Cerebellar Ataxia (Source: Ali & Lawthom, 2013)
P&
Top Related