






Languages
Pages
Legal

EPILEPSY SURGERY
WORKSHOP
K.B.Das
Master Class July 2012
Young Epilepsy
Aim
To discuss presurgical evaluation through some
illustrative case studies
To highlight practical issues
The dilemma
The removal of or modification of a part of the
brain with the aim of alleviating seizures
Epilepsy Surgery

Case 1
The jerking girl
History
15.6 yr girl
Normal birth, development
Well until 9 yrs of age
Mainstream school
9yrs
1st seizure: aged 9 yrs, x 1hr GTC
Admitted to local hospital
Rx Lorazepam, Phenytoin,
intubated, Thiopentone
No definite fever, rash
Few days before-episode of staring, fidgeting of
hands, confusion
Course in hospital
? Encephalitis
CT normal
CSF 17 WBC
Rx –Aciclovir,Antibiotics
Seizures controlled on carbamazepine
Stable when discharged, ? behaviour not normal

Progress
9 - 10 yrs : Recurrent attacks
Left arm posturing,staring,dysphasia,
tachycardia lasting 30-90 secs x 12/hr
Repeated episodes of status
No focal deficits on examination
MRI- Normal
What is the problem?
?Sequelae of encephalitis
?Neurodegenerative disease
?Seizure disorder
?

What is the next step?
EEG right slow
Sz onset right hemisphere
History (contd.)
Recurrent focal sz
At times transient weakness of left face & leg,speech disturbances
Frequent jerking of left leg
Resistant to various drugs (valproate,clobazam,lorazepam,
phenytoin,steroids)
Repeat CSF-normal
Progress
Left side clumsy
Dysphasia
Struggling in school
Uninhibited behaviour, aggressive,
hyperactive
What next ?

MRI
?
Rasmussen’s Encephalitis (Rt)
April 2006
Right functional Hemispherotomy
Dense Lt hemiplegia
Weaning Phenobarbitone
Reducing steroids gradually

July 2006
Recurrence of sz post op
‘Stretches’
Rt sided jerking – several /day

Any thoughts?
Rasmussen’s encephalitis (Kozhevnikov-Rasmussen Syndrome)
“A severe, probably acquired, neurological
neocortical disorder characterized by intractable
mainly motor focal seizures, epilepsia partialis
continua and progressive neuropsychiatric
deterioration with hemiparesis and mental deficits.” (Panayiotopoulos)

Rasmussen’s encephalitis
Peak onset around 5 - 6 years
Sex incidence equal
Rare
Progressive initially and then gradually burns out

Rasmussen’s encephalitis
Aetiology:
Unknown
?Chronic viral infection
?Autoimmune - T cell mediated
Pathology:
Inflammatory process – initially localized then spreading
Mainly a cortical process

Rasmussen’s encephalitis
EEG:
May be normal initially
Later unilateral, focal slow activity
Often progresses to bilateral slowing
Progressive loss of normal rhythms over affected
hemisphere
Interictal spikes/sharp waves common
– unilateral/bilateral
Imaging
Progressive hemi-atrophy
Commonly starts in temporo-insular region with
enlargement of temporal horn and sylvian fissure
Temporal & Frontal lobes chiefly affected
Involvement of Caudate nucleus
Management
Immunomodulation
IVIG
Methylprednisolone
Prednisolone
Azathioprine
Anticonvulsants
Definitive therapy
Hemispherotomy
Timing critical
Case 2
The baby who wouldn't leave hospital !
11 wk boy
Forceps delivery, no AN problems
Sz from D1
Twitching of right arm, leg ,few secs x multiple
Eye flickering, pupillary dilatation, cycling of arms
D6 : Rt sided jerking – left , bilateral convulsive sz
Frequent attacks, needing rescue meds
Never left hospital from birth
PICU X 2 for iv clonazepam at 5 wk , 10 wk

11 wk
Subtle behavioural changes, eye flickering and
deviation to right and sometime right upper limb
jerking and stiffening.
It may involve right leg and left hand
Duration: 20 to 60 seconds
Frequency: 50 to100 / day

Medications
Previous
Phenobarbitone
Sodium Valproate
Phenytoin
Carbamazepine
Clobazam
Clonazepam infusion: partial
control
Midazolam (rescue)
Paraldehyde (rescue)
Current
Vigabatrin 150 mg/kg/day
Levetiracetam 50 mg/kg/d
Clonazepam
Paraldehyde 5 ml (50:50mix)

Development : fixing and following at 10 wks (when well)
Family History : Nil relevant
O/E:
OFC 47.5 cms
No dysmorphic features
No neurocutaneous markers
Spontaneous movements Lt> Rt
Brisk reflexes Rt UL & both LL
Truncal and axial hypotonia
Ophthalmology -normal
EEG (Local)
Numerous seizures have been documented.
All have a stereotyped appearance though the clinical onset and termination are difficult to define precisely.
There is increased rhythmic jerking of the eyelids and deviation of the eyes (with a slightly dysconjugate gaze) to one or other side or often downwards. No jerking of the limbs is seen.
All are associated with epileptiform rhythmic activity appearing over the left centro-temporal and posterior temporal region with slightly variable emphasis between these two electrode locations.
EEG (GOSH )
Prolonged EEG recording (15 hours) with 78 electro-clinical seizures captured:
Asymmetry in the background with excess of slow activity over the left.
Very frequent epileptiform discharges seen over the left central and posterior temporal regions
Infrequent independent discharges over the right central region
Stereotypical electrographic seizures arising from the left centro-temporal regions and
spreading to the right central region. These are associated with rapid bilateral eye blinking, head turn to the right and reduced right arm movements. The seizures vary in duration from 20-60seconds with the shortest interval between seizures being 20seconds.
When compared to the previous EEG (20/05/2011), the site of seizure onset has not changed. There is slight improvement in the background activity over the left hemisphere however this could be partially state (sleep/wake) related.
What next ?
Any thoughts?
?

Echo: cardiac rhabdomyomas
Summary
11 week old infant with clinical diagnosis of Tuberous sclerosis
He has symptomatic focal refractory epilepsy onset from
Day 1 of life
Seizure semiology: stereotypical, left hemisphere origin
Focal deficit right upper limb (frequent seizures)
MRI Brain: Bilateral changes with possible dominant tuber /
area of cortical abnormality in left parietal region
Telemetry: left centro-temporal region

Outcome
12 wks:
Urgent discussion at MDT
Resection of left parietal cortical tuber with ECoG
(Electrocorticography)
Seizure free post-op
Recently: ? Recurrence of events ,for re-evaluation

Case 3
Sz from the wrong side !
8 yr old boy
Birth History: Born 42 weeks
15 hours of age, apnoeic. SCBU
Blood sugar of 1.2 mmol /L
Responded to a bolus of Glucose but had 2 further right sided fits, within 24 hrs
Early Development : Normal

History
First seizure: <1 year old
Subsequent seizures: Age 5 years, complaining of ‘sore head’ Then started to see animals and dinosaurs Subsequently, would wander, laugh inappropriately, staring Drowsy or hyperactive afterwards x 10/day Current seizures: With hallucinations Parents alerted by shouting Often sees dinosaurs Shouts “Dynamite” Is found pale, staring and looking afraid

Where is the seizure coming from ?
Hypothesis
What next ?
?

Invasive Monitoring

Conclusion
Sz onset over left hemisphere
Rapid spread to right
Progress
Left occipital resection done
Post-op sz free
In quest of the holy grail ! (Lesion)
Case 4
The Jigsaw puzzle !
History :
7 yr old boy
Seizure onset at 3 years
Head turning to left
Drooling
Trance-like
Quickly evolved to clusters of multiple seizure types
including tonic seizures, drop attacks and jerks
x 20/ a day lasting 30 seconds
No response to medications

Current seizures
Type 1 (aura) - says “Mum seizure feeling”, buries his head/face
for a couple of seconds. Sometimes associated with repeated
blinking
Frequent events every day, some not recognised completely.
No loss of consciousness
Type 2 (Drop attacks): grabs on to nearby persons/furniture for
support, takes a gasping breath
Suddenly loses tone, drops to the floor, rubs his nose on the floor
and retains partial awareness
Hyper-motor, repetitive movements arms/legs. Day and night.
There can be facial flushing
Whole episode 10-15 seconds x 9-14 per day
Previous
Medication:
Carbamazepine, sodium valproate, clonazepam,
phenytoin, phenobarbitone, topiramate.
Current Medication: Lamotrigine 5mg bd
Schooling/
behaviour:
Mainstream primary school, no learning difficulties
identified
Family: No significant illnesses. No history of nocturnal
seizures.
Examination: Normal examination. Right handed.
Past medical history Normal birth history. No meningitis or prolonged febrile
seizures.
Seizures fairly stereotyped
Short events
Behavioural arrest
Leans to side and grabs parents
Long events
Behavioural arrest
Rubbing nose in the pillow
Flipping over
Thrashing movements

Imaging
1.5 T x 2 epilepsy protocol
3T MRI
All negative

Any ideas?
?
MEG
Synchronous neuronal
currents produce weak
magnetic fields
Analogous to EEG
Good for convexity
Mainly inter-ictal
Clusters of dipoles

Able right handed 6-year-old boy with high average intellect.
Some difficulties with attention and concentration.
Neuropsychiatry Concerns about impact of epilepsy on school life.
Neuropsychology

Summary Seizure semiology Frontal, not clinically lateralising
Temporal - significance of aura?
Examination Normal ,Right handed
MRI March 2011
SPECT March 2010
PET July 2010
MEG Feb 2011
Negative (3T)
Lateralises to the right but does not localise (short seizure)
right mid frontal / right anterior temporal region.
Right frontal
Right frontal
Telemetry March 2010 Inter-ictal: right frontal
Ictal: Right frontal and anterior temporal slowing (F8, F10)
Neuropsychology Able right handed 6-year-old boy with high average intellect. Some
difficulties with attention and concentration
Neuropsychiatry Concerns about impact of epilepsy on school life
Reasons for
Invasive/ECoG
Hypothesis
Localise ictal onset. Map motor cortex
Depth into MEG lesion
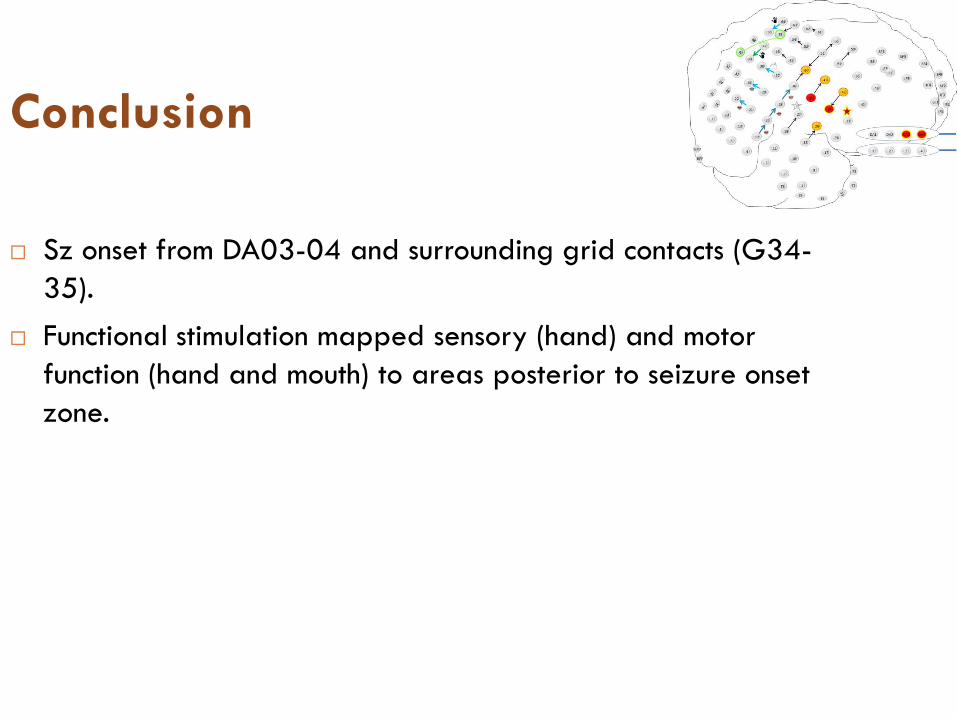
Conclusion
Sz onset from DA03-04 and surrounding grid contacts (G34-
35).
Functional stimulation mapped sensory (hand) and motor
function (hand and mouth) to areas posterior to seizure onset
zone.
Puzzle complete ! Quest ?
Semiology
EEG
PET
SPECT
MEG
Invasive monitoring
- concordant
Plan
Focal resection of gyrus underlying contacts
G34/35/42/45
Follow depth electrode down with further resection.
Prognosis given:
Seizure freedom: 50-60%
Significant seizure reduction: further 20%
Risk of neurological deficit: 2-5%
The end of the journey?
Well post-operatively, no deficit
Seizure free
Top Related