







Languages
Pages
Legal

www.icddrb.org
Engaging private sector providers around universal health coverage:
a qualitative study of motivations and entry points in three cities of Bangladesh
Alayne Adams
Senior Social Scientist
Centre for Equity and Health Systems, icddr,b

www.icddrb.org
The Lancet Series 2014

www.icddrb.org
The urban healthcare landscape
Rapid urbanization and expanding health service needs among urban residents
No public provision of urban primary care services: limited to tertiary facilities, EPI outreach, MNCH services contracted out by local government
Private sector dominates urban healthcare landscape: private hospitals represent 80% of >3500 hospitals in Bangladesh
YET largely undocumented given weak implementation of regulation around licensing or integration into routine health information systems.
2%
12%
86%*
Formal healthcare facilities in Dhaka
n=7350
Public
NGO
Private
*Excluding pharmacies & optical shops
www.icddrb.org
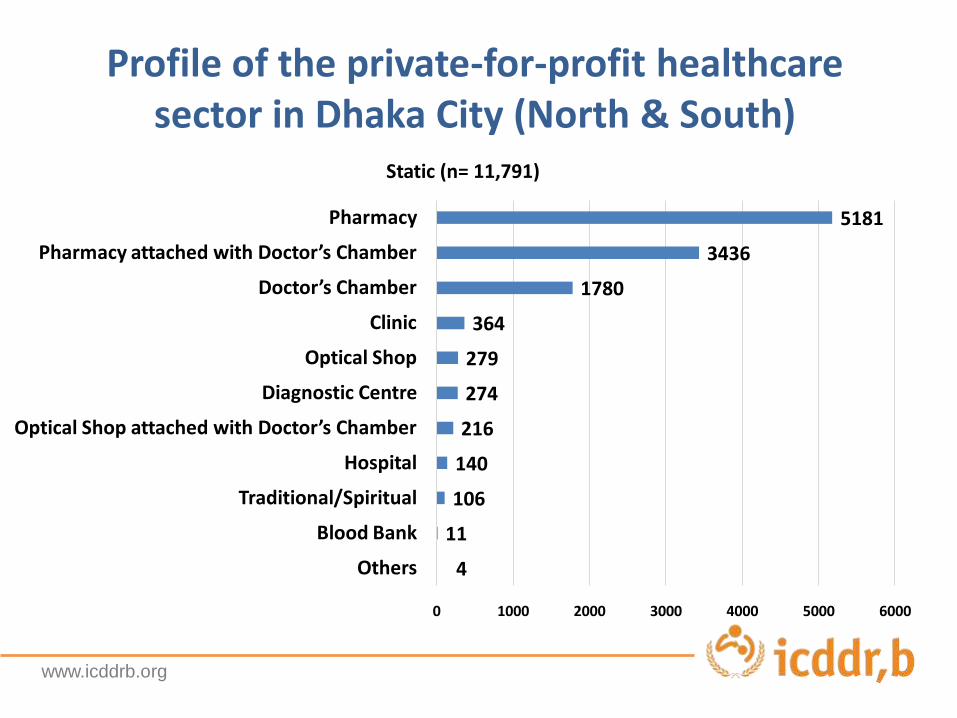
Profile of the private-for-profit healthcare sector in Dhaka City (North & South)
4
11
106
140
216
274
279
364
1780
3436
5181
0 1000 2000 3000 4000 5000 6000
Others
Blood Bank
Traditional/Spiritual
Hospital
Optical Shop attached with Doctor’s Chamber
Diagnostic Centre
Optical Shop
Clinic
Doctor’s Chamber
Pharmacy attached with Doctor’s Chamber
Pharmacy
Static (n= 11,791)

www.icddrb.org
Where do the urban poor seek care?
Largely reliant on the informal private sector - pharmacies -due to proximity and desire for rapid treatment
Almost 30% of slum dwellers and 58% of non-slum dwellers went to private sector for ANC (BUHS, 2013)
65% of poor urban respondents cite proximity as a factor motivating choice (icddr,b, 2104)
Health seeking for last acute health episode among the urban poor in Tongi
Source:, icddr,b, 2014

www.icddrb.org
Not without costs
Rising out-or pocket expenditures impact the
urban poor, leading to medical impoverishment
- Out-of-pocket payments constitute 64% of total
health expenditure
- 3.5% population falls into poverty in 2010 due to
catastrophic health expenditure (HIES, 2010)
Concerns about quality and high service costs of
private sector provision
www.icddrb.org
Universal Health Coverage in Bangladesh
The goal of Universal Health Coverage (UHC) is to
“ensure that all people obtain the health services that they need without
suffering financial hardship when paying them” (WHO, 2014)
Publically financed free services are typically preferred to address inequity and ensure UHC
HOWEVER, increasing pluralism of health care provision challenges this assumption, especially in urban areas
Less than 1% covered by any health protection scheme
With rapid growth of urban populations, especially in poor urban settlements, health systems in Bangladesh must respond

www.icddrb.org
Moving towards UHC in Bangladesh
Population: who is covered?
Current pooled funds
Direct cost:proportion of costs covered
Extend to non-covered
Reduce cost sharing and fees
Include other services

www.icddrb.org
National health financing strategy

www.icddrb.org
Private sector readiness for UHC
In urban areas, UHC is unlikely without private sector engagement - needed for population coverage of quality, affordable services
QUESTION: how feasible is this in the context of private sector motivations and interests?
Objectives of private sector study:
1. To understand the private sector motivations, business strategies and incentives in urban areas
2. To identify areas of potential intervention to improve service quality and access to the urban poor that also serve the business interests of this sector
www.icddrb.org
Methods
Qualitative study in Khulna, Dhaka and Sylhet City Corporations
47 in-depth interviews with private clinic/hospital owners, and formal and informal providers
20 key informant interviews with health managers, clinic owners association leaders
30 exit interviews with patients
30 facility observations
www.icddrb.org
Key findings
Subsidies for the poor are widespread
Multiple motivations underlie business
Concerns about quality and regulation
Some interest in insurance!

www.icddrb.org
Reported provision for the poor by private-for-profit health facilities in Dhaka
While relatively high service costs are charged by the private sector, reports of discounted services to the poor were widespread:
“My visit is 500 taka, if anyone tell me patient is poor or garments worker, I take only 120 taka or less in different situations” (Formal Provider, Dhaka)
*Multiple responses
www.icddrb.org
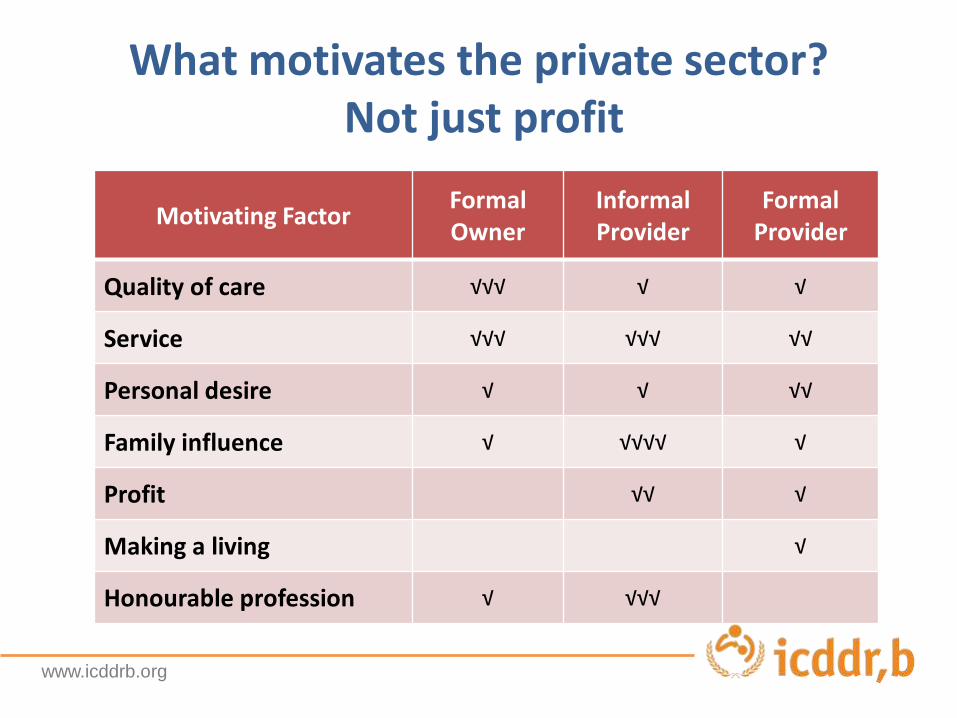
What motivates the private sector?Not just profit
Motivating FactorFormal Owner
Informal Provider
Formal Provider
Quality of care √√√ √ √
Service √√√ √√√ √√
Personal desire √ √ √√
Family influence √ √√√√ √
Profit √√ √
Making a living √
Honourable profession √ √√√

www.icddrb.org
Concerns about quality of care
Almost 40% of private sector respondents noted that variable service costs affect their business interests as well as consumer access to services, and many indicated that Government should intervene
Over a quarter of private sector respondents expressed concern about HR issues:
- Unavailability of specialized full-time consultants- Poorly trained newly graduated MBBS doctors- Lack of qualified nurses
“The number of diploma nurse is insufficient. So, nurses are not available
even after giving money. Without qualified nurse, providing service becomes tough.” (Clinic owner, Sylhet)
www.icddrb.org
Concerns about regulation
Over a quarter of private sector respondents emphasized the need for greater regulation and enforcement of existing law to increase accountability and quality:
“They (Government) have made the laws for everything…in case of miss-enforcement, good law becomes useless.” (Key informant, Khulna)
Confusion and frustration expressed about multiple and uncoordinated regulatory bodies making compliance difficult
The current punitive approach of mobile courts is not appreciated:
“…now if it is seen that mobile court has come and we are running away closing our store, then how can monitoring be done? But if monitoring is done in a way that (helps us) correct our mistakes - If they help us in this way, then it will be good.” (Informal provider, Dhaka)

www.icddrb.org
Private sector readiness for health insurance
Almost 15% of private sector respondents suggested the introduction of health insurance as a strategy to help increase access and utilization of services by the poor.
“Insurance should be made obligatory. To bring each and every person under the medical services, be it rickshaw puller, farmer or even your housemaid, insurance is the only option. If these people can pay mobile phone bills per month, then I don’t believe they can’t pay the premium for insurance every month.” (Formal private clinic
owner, Dhaka)

www.icddrb.org
Challenges in engaging the private sector
Formal private sector facilities tend to specialize in diagnostics or high volume services – primary care functions are provided by thousands of private doctors chambers, and pharmacies but with little regulation
The dualism dilemma - shortage of qualified health human resources available 24/7 both private and public sectors
Stewardship function of government around quality improvement and regulatory oversight is weak

www.icddrb.org
Conclusions
Need to formally engage the private sector around effective coverage of quality services given its massive presence in the urban healthcare market
Indications of readiness to engage with UHC solutions such as health insurance schemes - may provide an entry point to increasing coverage
Achieving UHC objectives with private sector engagement requires the enforcement of regulatory frameworks around pricing, quality, and standards of care
The informal private sector can’t be ignored

www.icddrb.org
Recommendations
Take advantage of multiple private sector motivations around
service and quality (not just profit) in leveraging involvement
Explore different modalities of formalizing support to the poor
through subsidies or the design of insurance schemes that measure
and reward quality provision of services by the private sector
Strengthen government capacity to develop and implement
appropriate policy frameworks to engage with the private sector,
especially with respect to costs, standards of care and MIS
Explore ways to improve quality and minimize harm of informal
private sector i.e. ICT innovations, franchising
Top Related