







Languages
Pages
Legal


Emergency Room Thoracotomy
Marc Pelletier, MDHead, Department of Cardiac Surgery
New Brunswick Heart Centre

CFPC MAINPRO Declaration of Conflict of Interest
Edwards Lifesciences: Proctor, consultant

Today’s goals
What is an ER thoracotomy?
Review determinants of survival
Review indications and contraindications
Realistic goals of ERT
Technique and expectations

“The surgeon who should attempt to suture a wound of the heart would lose the respect of his surgical colleagues.”
Theodore Bilroth, 1882

Ludwig Rehn, 1896, 1st documented successful repair of cardiac laceration.
Blatchford JW. Ludwig Rehn: the first successful cardiorraphy. Ann Thorac Surg 1985;39:492–5.

What is an ER thoracotomy?

What is an ER thoracotomy?

What is an ER thoracotomy?


Why ERT?
ERT is a controversial treatment option
Low chance of survival (4-33%)
Significant resources, risk to health care workers must be considered
Risk to health care workers
Exposure to blood/fluids
One of most “exciting” ER events“Even a 1% chance in a 20 y.o. is worth it!”

Who can survive with ERT?
Mechanism of Injury
Location of Injury
Presence of Vital Signs

Mechanism of Injury
Penetrating thoracic injurySurvival 18-33%
Stab wounds better than gun shot wounds (GSW)
Isolated stab wounds are best (up to 70%)
Blunt traumaSurvival 0-2.5%
Best in those with hypotension with ongoing chest tube losses
Location of Injury
Best chances:Isolated injury to thorax
Cardiac injuries
Single cardiac chamber (versus multiple chambers)
Injuries to great vessels and pulmonary hila carry high mortality
Injuries to abdomenGoal to cross clamp aorta to control bleeding
Penetrating abdo trauma much better than blunt

Presence of Vital Signs
Presence of cardiac activity, or the amount of time since activity, is crucial to survival
0% for arrest at scene
4% when arrest in ambulance
19% when arrest in ED
27% when deterioration but not arrest in ED
When there is “No sign of life”Blunt 0%
Penetrating 0-5%

What are signs of life?
Pupillary response
Spontaneous ventilation
Presence of carotid pulse
Cardiac electrical activity
Measurable or palpable blood pressure
Extremity movement

Accepted Indications
Penetrating Thoracic InjuryTraumatic arrest with previously witnessed cardiac activity (pre-hospital or in-hospital)
Unresponsive hypotension (BP < 70 mmHg)
Blunt Thoracic InjuryUnresponsive hypotension (BP < 70 mmHg)
Rapid exsanguination from chest tube (>1500 ml)

Relative Indications
Penetrating Thoracic InjuryTraumatic arrest without previously witnessed cardiac activity
Penetrating Non-thoracic Injury (i.e. peripheral, abdominal)Traumatic arrest with previously witnessed cardiac activity (pre-hospital or in-hospital)
Blunt Thoracic InjuryTraumatic arrest with previously witnessed cardiac activity (pre-hospital or in-hospital)

Contraindications
Blunt Injuries
Blunt thoracic injuries with no witnessed cardiac activity
Multiple blunt trauma
Severe head injury
Severe multisystem injury
Improperly trained team
Insufficient equipment

Also consider…
2011 prospective multicenter study revealed no survivors:
Blunt trauma with > 10 minutes of pre-hospital CPR
Penetrating trauma with > 15 minutes of pre-hospital CPR
Asystole without cardiac tamponade
Moore et al. Journal of Trauma-Injury Infection and Critical Care. Feb 2011




What are the goals of ER thoracotomy?
Control bleeding
Release cardiac tamponade
Facilitate internal/open cardiac massage
Prevention of air embolism
Exposure of descending aorta for cross-clamping
Repair cardiac or pulmonary injury

Before thoracotomy
Primary causes of traumatic arrest (very different than cardiac arrest)
Hypoxia
Hypovolemia due to hemorrhage
Tension pneumothorax
Cardiac tamponade

Before thoracotomy
Hypoxic arrestIntubation and ventilation
Tension pneumothoraxNeedle decompression or chest tubesPresume bilateral
Massive hemorrhageChest tubes may help localize side of bleedingControl bleeding is more important than massive fluid transfusion
Cardiac tamponadeClassic signs often absentFAST can be helpful

ER Thoracotomy
Need to be prepared
Consult surgical teams in preparing equipment and supplies
Run mock ERT codes twice/year
Ensure ERT algorithm is posted and visible in Trauma bay

Equipment

Incision Decision

Position of patient

Technique – Enter chest
Don’t forget suction!

Incision StepsPosition, prep, drape
Scalpel (No. 10 blade) used to make incision down to ribs.
Skin, subcutaneous fat, pectoralis and serratus muscles
Find intercostal space (4th or 5th ICS ideal)
Hold ventilation while thoracic cavity entered
Incise intercostal muscle
Use scissors to go backwards then frontwards toward sternum
Insert retractor


What now?
Look around, check for bleeding, retract lung
Evacuate blood from left chest
Locate pericardium and assessBulging?
Blood visible?
Assess aorta
Assess lung

What are the goals of ER thoracotomy?
Control bleeding
Release cardiac tamponade
Facilitate internal/open cardiac massage
Prevention of air embolism
Exposure of descending aorta for cross-clamping
Repair cardiac or pulmonary injury

Pericardotomy
Always should be opened
Grasp pericardium and open with scissors
Open above (anterior) to phrenic nerve
Cardiac repair
Start with digital occlusion
Pledgetted mattress suturesLarge needle, large pledgets
3-0 or 4-0 Prolene
Foley catheter


Ventricular Repair
3-0 polypropylene sutures tied over pledgets
Bites 1 cm into normal myocardium
Very little tension is needed



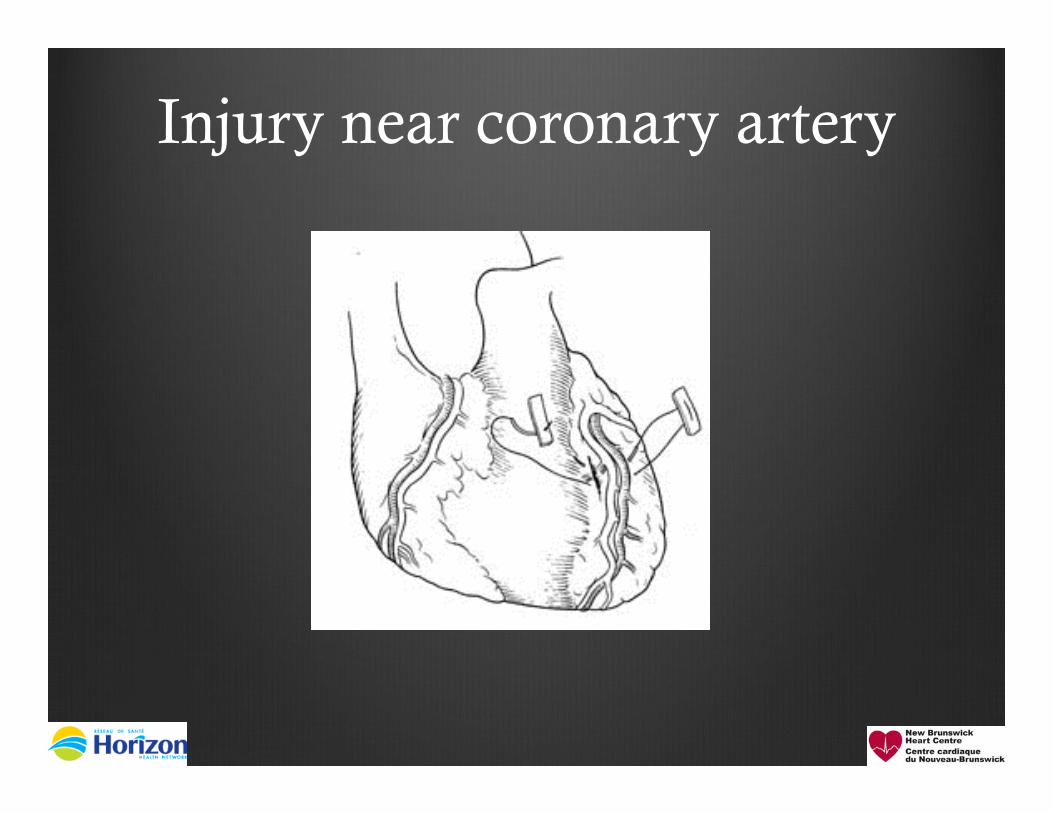
Injury near coronary artery
Place sutures beneath artery (preserve coronary as an “island”)
Other option is to ligate artery and perform bypass
Typical exam question
Injury near coronary artery

Small Atrial Wound
Finger pressure to control bleeding
Mattress suture repair of 3-0 or 4-0 polypropylene with pledget
Purse string
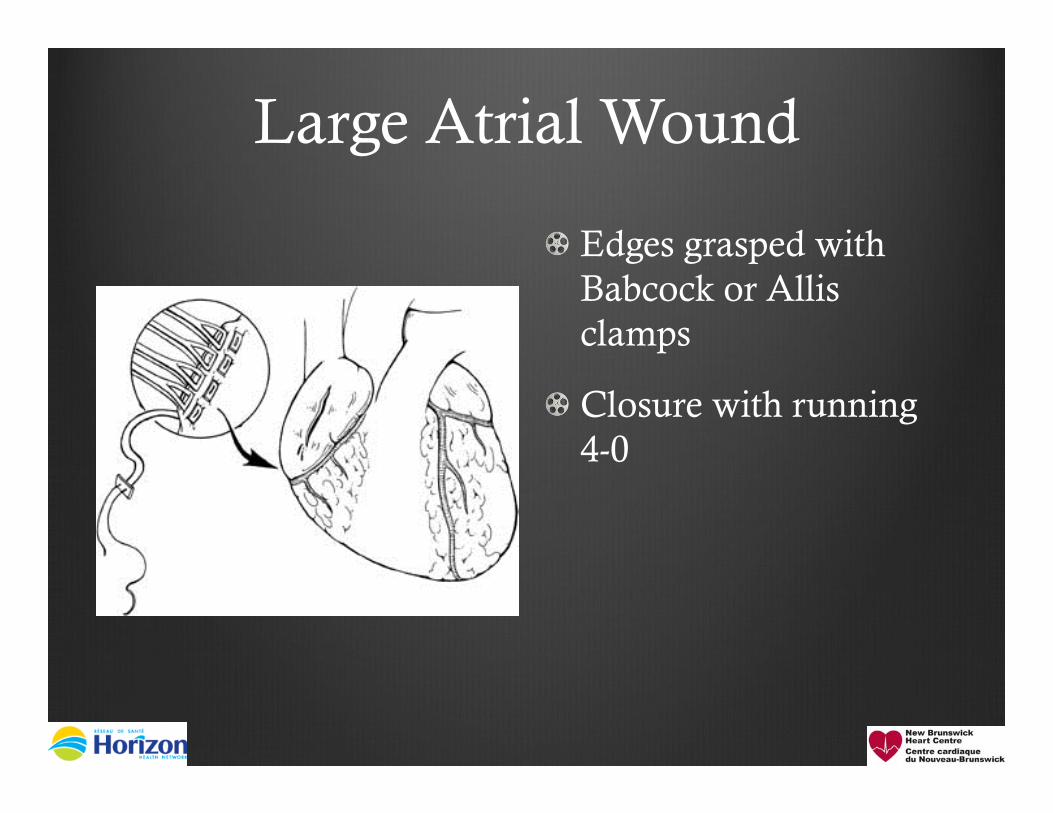
Large Atrial Wound
Edges grasped with Babcock or Allis clamps
Closure with running 4-0

Aortic Cross-clamping
Clamping descending aorta redistributes blood flow to coronary and cerebral arteries
Clamping near aorta can control abdominal hemorrhage
Retract lung superiorly
Aorta and esophagus are next to each other
NG tube may help

Aortic Injury
Usually small wound, sealed off
Finger pressure
Side-biting clamp
Repair with 3-0 or 4-0 with pledget

Internal Cardiac Massage
Perform with 2-handed technique to avoid perforation of the ventricle
Much more efficient (55% of cardiac output versus 20% with external CPR)
Give it a good chance (>15-20 minutes)
Defibrillate at 20 Joules
PearlsBe prepared. Have an algorithm.
Penetrating trauma has a much better chance. Is it even worth it in blunt trauma?
Get a surgeon involved ASAP.
Left anterolateral approach is usually best place to start.
4th ICS is best. Below nipple in men, breast crease in women.
Place handle of retractor downwards
Don’t make incision too low

Pearls (cont…)
Make incision above the rib (avoid neurovascular bundle)
Access to thoracic cavity should take < 2 minutes
Use OR or surgeons if at all possible
You will need a lot of blood!

“Better lucky than good”

“The more I practice, the luckier I get!”

GOOD LUCK!

Top Related