






Languages
Pages
Legal


33 Bulletin• Hospital for Joint Diseases Volume62,Numbers1&2 2004
Abstract
Fracture-dislocations of the elbow remain a complex prob-lem in orthopaedics. The myriad of treatment protocols and methodologies focuses on precise articular alignment and restoration of the skeletal architecture. The goal is to re-establish function as quickly as possible so as to allow rehabilitation involving the full range of motion. Surgical management, primarily reconstruction of the secondary stabilizers of the elbow joint as well as preserving soft tissue structures, subsequently provides the possibility of a speedier recovery. If proper skeletal alignment does not confer enough stability, hinged external fixation becomes an integral part of the treatment strategy for the reconstruc-tive and trauma surgeon.
Elbowdislocationsrepresent10%to25%ofallinju-riestotheelbow,inpatientswithameanageof30.1Theincidenceis6per100,000.2Theelbowjointis
amongthemostcommonlydislocatedmajorjoint,secondonlytotheshoulder.Theusualmechanismissportsrelated:fromafallonanoutstretchedhand.Thenatureofthebonyanatomyoftheelbow,inparticular,thesubcutaneousposi-tionof theolecranon,predisposes this region to frequentdislocations.3Elbow dislocations are classified as simpledislocations if they are not associated with concomitantperiarticularfractures.Thosedislocationsassociatedwithperiarticularfracturesareclassifiedascomplex.Onestudyhasshownthat100%ofelbowdislocationsareassociated
withunrecognizedosteochondralfractures,however,onlythose readily radiographically identifiable fractures aretermed “complex.” Elbow dislocations can be associatedwithradialheadfractures,coronoidfractures,capitellarortrochlearfractures,olecranonfractures,oranycombinationof these(Fig.1).3,4Elbowdislocationsarenamedfor thedirectionof thedisplacementof thedistal fragment.Theposteriordislocationisbyfarthemostcommon.Theanteriordislocationanddivergentdislocation(thehumerusgoesinbetweentheradiusandulna)arerareandassociatedwithhigherenergytrauma.3Theelbowjointcanalsodislocatethroughawidelydisplaceddistalolecranonfracture,referredtoasatrans-olecranondislocation.5
PathomechanicsElbowinjuriesrepresentaspectrumofinstabilitythatstartsasposterolateralinstability,progressestoapercheddisloca-tion,andthenproceedstoacompletedislocation.Duringanelbowdislocationallsupportingligamentsoftheelbow(includingthemedialcollateralligament,lateralulnarcol-lateralligament,andtheanteriorandposteriorcapsule)aredisrupted.Inmostcasesthemuscularoriginsattheepicon-dylesarealsodisrupted.5,6
After closed reduction of a simple elbow dislocationthe majority of cases demonstrate immediate stability intheflexion-extensionarc.Thisstabilityisderivedfromtheskeletalarchitecture.Theulno-humeralisjointisextremelycongruentandimpartsagreatdealofstabilitythroughoutthearcofmotion.Infullextensiontheolecranonprocesslocksintotheolecranonfossaandinfullflexionthecoronoidprocesslocksintoitsfossa.Valgusstabilityisprovidedbytheradiocapitellararticulation,astheradialheadactsasasecondarystabilizertoresistvalgusstress.7-10
The ulnar collateral, or medial collateral ligament, isthemain stabilizeragainstvalgus loads.7,8,9The ligamentoriginatesfromthemedialepicondyleandinsertsontothe
Elbow Fracture-DislocationsThe Role of Hinged External Fixation
Nader Paksima, D.O., M.P.H., and Anand Panchal, B.S.
Nader Paksima, D.O., M.P.H., is anAssociate Professor in theNYU-HJDDepartmentofOrthopaedicSurgery,NewYork,NewYork.AnandPanchal,B.S.,isattheNewYorkCollegeofOsteo-pathicMedicine,NewYork,NewYork.Correspondence:NaderPaksima,D.O.,M.P.H.,HospitalforJointDiseases,NYU-HJDDepartmentofOrthopaedicSurgery,301East17thStreet,NewYork,NewYork10003.

34 Bulletin• Hospital for Joint Diseases Volume62,Numbers1&2 2004
sublime tubercle of the proximal ulna.The ligament hasbeenfoundtoconsistofthreedistinctbands.Theposteriorbundleisconfluentwiththeposteriorcapsuleoftheelbow
joint.Thetransversebundlecontributeslittletothestabilityoftheelbowasbothitsoriginationandinsertionareontheulna.Theanteriorbundleisthemostimportantpartoftheligament. It isa fan-shapedstructure thatbecome taut inextension,juxtaposedbytheposteriorfibers,whicharetautinflexion.Itsoriginisjustposteriortotheaxisofflexionandextensionoftheulno-humeraljoint.6,9,10
Theradialcollateralligament,orlateralcollateralliga-ment,hasitsoriginationatthelateralhumerusatthemid-pointofthetrochleaandcapitellumontheaxisofrotationoftheelbow.It thencoursesdistallyinafan-likepatternbeforemergingwiththeannularligamentandinsertingviaconjoinedfibersonto theproximalulna.These twoformthelateralligamentouscomplexwhichmaintainstheulno-humeralandradio-capitellumarticulations. Injurytothelateralligamentousstructuresresultsinaposterolateralrotatoryinstabilityoftheelbow.7,9-11
The Stable ElbowAfterreductionofthestandardposteriorelbowdislocation(Fig1B),theelbowcanbeputthroughacarefulactiverangeofmotionunderthedirectsupervisionofthesurgeon.Thiscan give invaluable information about the post-reductionstability.Theelbowbecomesmorestablewithincreasingflexionandpronation.Thenumberofdegreesofextensionatwhichtheelbowstartstofeelunstableorstartstosubluxateordislocateshouldbenoted.Anelbowisconsideredstableifitremainsreducedthrougharangeofmotionof40°ofextension lag to full flexion, with the forearm in neutralrotation.Byconventionthisisreferredtoasarangeofmo-tionof40°to135°.Iftheelbowhastobeflexedtomore
Figure 1A,A43-year-oldmalewithunstablefracturedislocationoftheelbow.B,Lateralfilmshowingconcentricreduction,afracturedradialhead,andacoronoidMCLavulsion.
BA
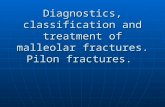
Figure 2Intra-operativeexamination:unstabletovalgusstress,evenafterradialheadreplacement,dislocatableposterolaterallywithflexionoflessthan60°.

35 Bulletin• Hospital for Joint Diseases Volume62,Numbers1&2 2004
than60°inorderforittoremainreduced,itisconsideredunstableandacandidateforsurgicalintervention.Thereisalsoalmostuniversalagreementthatanelbowthatremainsstableat40°orlessofextensionisreallystableandcanbesuccessfully treatedwithout surgery.12The zonebetween40°and60°isagrayzoneofinstability. Assuming that the elbow is stable through a range of40°to135°,thepatientisimmobilizedwithaposteriorlyappliedlongarmsplintthatstartshighuponthehumerusandextendstojustproximaltothemiddlepalmarcrease.Elevationanddigitalrangeofmotionareencouraged.Thepatientshouldthenbeevaluatedbetween3to7daysaftersplintingandtheplasterslabremoved.Theelbowcanbeplacedthroughanactiveassistedrangeofmotionandstabil-ityagainverified.Anteroposteriorandlateralradiographsshould be obtained to ensure a concentric reduction oftheulno-humeral joint.Careful attention to a true lateralradiograph is important to avoid missing an incongruentreduction, or an incarcerated osteochondral fragment inthe joint. Immobilizationbeyond two to threeweekscanleadtoexcessivescarringandlossofmotion.13Thereisanaveragelossof10°ofterminalextensionassociatedwithelbowdislocations.Thedegreeandincidenceofsecondaryelbowstiffnessriseswithincreasedimmobilizationandthepresenceofassociatedinjuriesandre-manipulationoftheelbow.13
Radial Head FracturesRadialheadfracturesarerelativelycommonandseeninupto20%ofalltraumatotheelbow.3Theradialheadfracturesarecausedbyavalgusforceontheelbowas theheadisdrivenintothecapitellum.RadialheadfractureshavebeenclassifiedintofourtypesaccordingtoMason.14Typeonefracturesarenondisplacedfracturesthataretypicallytreated
nonoperatively.Typetwofracturesaredisplacedfracturesinvolving30%ofthearticularsurface.ThemanagementoftheseiscontroversialwithsomesurgeonsusingasignificantblocktomotionasthedeterminingfactorbetweenORIFandnonoperativetreatment.Typethreefracturesarecomminutedandrequireexcisionorimplantarthroplastyinthesettingofelboworforearminstability.Typefourradialheadfracturesarethoseassociatedwithelbowdislocation;theseareusuallydisplacedfracturesandoftencomminuted.3,13
Isolatedradialheadfractureswillnotmaketheelbowunstable.However,whenseeninthesettingofelbowdislo-cationstheradialheadbecomesimportant.Theradialheadfunctionsasasecondarystabilizeragainstvalgusforcewhenthemedialcollateralligamentisincompetent.15
Restoringtheskeletalarchitecturebymeansofopenreduction and internal fixation (ORIF) or arthroplasty oftheradialheadservestostabilizetheelbowinthissetting.Examinationofthewristjointisalsoimportantwhenradialheadfracturesarenotedsinceconcomitantwristpaincanindicate a disruption of the interosseous membrane andsprainofthedistalradio-ulnarjoint(TheEssex-Lopresstilesion).Thepresenceofamedialhematoma,usuallyindi-catingatearoftheMCLinassociationwiththeradialheadfracture,helpstheexaminertounderstandthattheinjuryisnotisolatedtotheradialhead. IftheEssex-LopresstilesionissuspecteditisimportanttoperformanORIForarthroplastyratherthantoexcisetheradialhead.16Excisionoftheradialheadcanleadtoproxi-malmigrationoftheradius.Whenperformingaradialheadarthroplasty torestorestability to theelbowor in thecaseoftheEssex-Lopresstilesion,itisimportanttousearadialheadof sufficient size topreventmigration andoptimizeradio-capitellar contact.The radiocapitellar articulation isdifficulttoreproducewiththecurrentavailableimplants,thus
Figure 4 Placementofhingedexternalfixatorshowingcorrectcenteringonhumero-ulnaraxisofrotation.
Figure 3Placementofhingedexternalfixatorshowingcorrectcenteringonhumero-ulnaraxisofrotation.

36 Bulletin• Hospital for Joint Diseases Volume62,Numbers1&2 2004
asignificantportionofradialheadimplantshavetoberevisedduetopersistentpain.Recentdevelopments,suchasabipolarprosthesisholdpromiseinimprovingarticulation.17,18
Capitellum FracturesFracturesofthecapitellumaregenerallyclassifiedintotwotypes:smaller,shearfractures(Kocher-Lorenz);andlarger,body fractures (Hahn-Steinthal).19Although small shearfragments can effectively be excised, larger fragments,especiallythosethatextendmediallyintothetrochlea,candestabilizetheelbowandshouldbefixed.Osteochondraldamagetothearticularsurfaceofthecapitellumisoftennotedinelbowfracturedislocations.
Coronoid FracturesThecoronoidservesasanimportantstabilizeroftheelbow.The coronoid sits anterior to the humerus and preventsanteriorslideofthehumerusontheulna.ReganandMor-rey20haveclassifiedthecoronoidfracturesintothreetypes.Type one fractures involve the tip of the coronoid andrepresentanindicatorofanelbowdislocationandligamentavulsion.Typetwofracturesinvolve50%ofthecoronoid.Type three fractures involvea fracture through thebaseofthecoronoid.Typetwoandthreefracturesrenderthe
elbow unstable. It has been shown that at least 50% ofthecoronoidmustbepresentinorderforittoeffectivelyfunctionasananteriordoorstoptohumeraltranslation.Amorerecentlyrecognizedfracturepattern–thetypefourfracture– involvesasagittal fractureof thebodyof thecoronoidthatinvolvestheMCLattachmenttothesublimetubercle.Thisfracturepatterniscausedbyavarusmomentappliedtotheelbowinanextendedposition. Openreductionandinternalfixationofacoronoidfrac-tureisanimportantstepinrestoringelbowstability.Thelargefracturefragmentscanbefixeddirectlyorindirectlywithplacementofascreworspeciallydesignedbuttressplates.13,21Themorechallenging,andunfortunatelymorecommon scenario, iswhen there is comminutionof thefragmentandORIFisnotpossible.Inthiscircumstancereattachment of the anterior soft tissues and ligamentsthroughtheuseofsutureanchorsordrillholesservesasasalvageprocedure.13,21
Current Approach to the Complex Elbow Fracture DislocationThereareseveralwaystoapproachtheelbowsurgically.22,23Theposteriorapproachisanextensileapproachthatallowstheposterior,lateral,andmedialsidesoftheelbowtobe
Figure 5Postoperativefollowupatoneweekshowingcorrectplacementofhingedexternalfixator.

37 Bulletin• Hospital for Joint Diseases Volume62,Numbers1&2 2004
exposedthroughoneincision.Othersurgeonshavedescribedaseparatemedialandlateralincision.Thisalsoallowsac-cesstomedialandlateralaspectsofthejointwithpossiblybetteraccesstotheanteriorstructures.Themedialapproachtotheelbow,however,isassociatedwithhighermorbidityandsurgicaltimeasthemedialcutaneousnerveshavetobedissectedandprotected.Injurytothesestructurescanresultinapainfulscar.22,23
Theposteriorapproachinvolvesanincisiondowntothedeepfasciaandfullthicknessflapsareelevatedanteriorlyandlaterally.ThedeepportionoftheKocherintervalcanbedevelopedforaccesstotheradio-capitellarjoint.MinimallycomminutedradialheadfracturescanbefixedwithORIF.Severelycomminutedfracturesaretreatedwithradialheadarthroplasty. It isadvantageous tofixacoronoidfractureprior toreplacingtheradialhead.Whenthecomminutedradialheadhasbeenexcised,thecoronoidcanbevisualizedthroughthedefect.Togetbettervisualizationoftheanteriorstructures,thelateralcapsuleattachmentandtheremainingmuscular attachments to the supracondylar ridge can beelevated.Thisallowstheelbowtobesubluxatedoutandthecoronoidcansometimesbefixedbythisapproach.22
Afterstabilizationoftheradialhead,eitherviaORIForimplantarthroplasty,theelbowisreducedandstabilityisas-
sessedbothradiographicallyandclinically.Intraoperativelytheelbowisconsideredstableifitdoesnotre-dislocateorsubluxateat40°ofextension.12Alternatively,iftheelbowhastobeexcessivelyflexedandpronatedthenitisconsid-eredunstable.24Asdiscussedabove,differentauthorsmaydifferonthedegreeofinstabilitythatisexcessive;however,almostallarewithintherangeof40°to60°(Fig.2).Therangeofmotionjustdescribedismeasuredwiththeforearminneutralrotation.Iftheforearmhastobekeptinpronationtokeeptheelbowfromsubluxatingintraoperatively,thenitisprobablytoounstable. If after fixation of the radial head and coronoid theelbowisstillunstable,thesurgeonmustdecidewhethertodissectmediallytorepairtheMCLorproceeddirectlytoexternalfixation.Whileeachoftheseapproacheshasmeritsincertaincases,itisthisauthor’spreferencetostabilizetheelbowwithahingeddynamicfixatoratthispoint.Bysta-bilizingtheelbowonecandecreaseboththemorbidityandextensivedissectionthataccompanythemedialapproachtotheelbow.25
Ifthecoronoidandradialheadhavebeenaddressedandstabilized,thefixatorcanreliablyimpartenoughstabil-itytotheelbowsothatthemedialcollateralligamentdoesnothavetobedirectlysutured.25-27Themedialcollateral
Figure 6Postoperativefollowupatfourmonths,afterremovalofhardware,showingcorrectarticularalignmentofhumero-ulnarandradio-capitellarjoints.

38 Bulletin• Hospital for Joint Diseases Volume62,Numbers1&2 2004
ligamentistorn100%ofthetimeinasimpledislocation,and late instability from the ligament not healing, evenwhentreatedbyclosedmeans,isexceedinglyrare.11Oncetheelbowhasbeenstabilizedbyexternalfixation,imme-diaterangeofmotioncanbestarted,allowingtheMCLtohealandremodelwhileprotectingtheligamentagainstvalgusstress.25,26Thisconceptissimilartothatoftreatingthemedialcollateralligament(MCL)spraininthekneeandhasagoodtrackrecordinthatregard. Thetechniqueofexternalhingedfixatorapplicationhasbeenwelldescribedpreviouslyandtheauthorsreferthe reader to the descriptions by Jupiter and Ring,25 aswellasMcKeeandcolleagues.26RefertoFigures3,4and5forexamplesofcorrectplacementofahingedexternalfixator. On theotherhand, advocatesof directMCL repairbelievethatbysuturingtheMCLtheelbowmayberen-deredstableenoughso that theuseof thehingecanbeavoided.Thehingedfixatordoespresentsomemorbiditytothepatientandrequiresspendingmoretimeintheop-eratingroom.Theprocedureistechnicallydemandingandthelearningcurvenotveryforgiving.25,26Thepossibilityis quite real, however, that after repairing the MCL theelbowwillstillbeunstable.Inthatsituationonehastheoptionofputtingthehingeonorimmobilizingtheelbowpostoperatively. The latter choice would be associatedwith increasedelbowstiffnessandshouldbeavoided iftheclinicalconditionsallow.12,25
Whentheelbowisimmobilizedpostoperativelywithsplintsandcasts,itisusuallynecessarytoplacetheelbowinsomedegreeofpronationandflexion,preferablyinahingedbrace,tostartsomemotionassoonassofttissuesallow.Carefulfollowupisthenneededtograduallyallowprogressivelymoreextensionandsupination.Thedangerexiststhattheelbowcouldre-dislocate,especiallyinthefirstfewweeks.12,25Thusduringthecourseofthefirstthreeweeks some surgeonswill follow thesepatientsweeklywithradiographicaswellasclinicalexaminations.RefertoFigures6and7asexamplesofpostoperativefollow-up radiologicalandphysicalexaminations. If theelbowshouldre-dislocate,evenifcaughtinatimelybasis,thepatientwillhavetoreturntotheoperatingroom.Thereisamuchhigherrateofheterotopicossificationandstiffnessassociatedwithelbowsthathaverepeatprocedureswithinthefirstfewweeksoftheindexprocedure.3,13
Other alternatives to hinged fixation for stabilizingtheulno-humeral joint,suchas trans-capitellaror trans-olecranonSteinmanpins,shouldbeavoidedastheycauseadditionalarticulardamageandelbowstiffness.13
ConclusionElbowfracture-dislocationsareamongthemostchalleng-ingproblemsfacingorthopaedicsurgeons.Thesecomplexinjuriescanbeeffectivelytreatedthroughastepwiseandlogicalapproach.Thegoalistorestoreenoughstabilitytotheelbowsothatafunctionalrangeofmotioncanbestarted
Figure 7 Patientshowingfunctionalarcofmotionofelbowjointaftersurgeryandphysicaltherapy.

39 Bulletin• Hospital for Joint Diseases Volume62,Numbers1&2 2004
andmaintained.Byreconstructingthebonyanatomymostelbowscanberenderedstable.Thisisaccomplishedbyad-dressingtheanteriordeficitwithfixationorbonegraftingthecoronoidandbyrestoringthesecondarystabilizertovalgusstressbyfixationorarthroplastyoftheradialhead.Ifrestoringtheskeletalanatomydoesnotimpartenoughstability, then hinged external fixation is an invaluableassetinthearmamentariumofthetraumaandreconstruc-tivesurgeon.
AcknowledgmentTheauthorswishtothankKennethKoval,M.D.,forshar-inghisclinicalcasesinpreparationofthispresentationandmanuscript.
References1. MehloffTL,NoblePC,BennettJB,TullosHS:Simpledisloca-
tionoftheelbowintheadult:Resultsafterclosedtreatment.JBoneJointSurgAm70:244-249,1988.
2. JosefssonPO,NilssonBE:Incidenceofelbowdislocation.ActaOrthopScand57:537-538,1986.
3. BrownerBD,JupiterJB,LevineAM,etal:Skeletal Trauma(3rded).Philadelphia:W.B.Saunders,2002.
4. O’Driscoll SW: Classification and evaluation of recurrentinstabilityoftheelbow.ClinOrthop(370):34-43,2000.
5. RingD,JupiterJB,SandersRW,etal:Transolecranonfrac-ture-dislocationoftheelbow.JOrthopTrauma11(8):545-550,1997.
6. JosefssonPO,JohnellO,WendebergB:Ligamentousinjuriesindislocationsoftheelbowjoint,ClinOrthop221:221-225,1987.
7. MorreyBF,AnKN:Functionalanatomyoftheligamentsoftheelbow.ClinOrthop(201):84-90.1985.
8. MorreyBF,AnKN:Valgusstabilityoftheelbow:Adefinitionofprimaryandsecondaryconstraints.ClinOrthop265:187-195,1991.
9. CohenMS,BrunoRJ:Thecollateralligamentsoftheelbow:Anatomyandclinicalcorrelation.ClinOrthop383:123-130,2001.
10. Regan-WD,Korinek-SL,Morrey-BF,An-KN:Biomechani-calstudyofligamentsaroundtheelbowjoint.ClinOrthop271:170-9,1991
11. O’Driscoll SW, Morrey BF, Korinek S,An K-N: Elbowsubluxationanddislocation:Aspectrumofinstability.ClinOrthop280:186-197,1992.
12. MorreyBF:InstructionalCourseLectures,AmericanAcad-emy of Orthopaedic Surgeons. Complex instability of theelbow.JBoneJointSurgAm79:460–469,1997.
13. RingD,JupiterJB:Fracture-dislocationoftheelbow.JBoneandJointSurgAm80(4):566-577,1998.
14. MasonML:Someobservationsonfracturesoftheheadoftheradiuswithareviewofonehundredcases.BrJSurg42:123-132,1954.
15. JensenSL,DeutchSR,OlsenBS,etal:Laxityoftheelbowafterexperimentalexcisionoftheradialheadanddivisionofthemedialcollateralligament:Efficacyofligamentrepairandradialheadprostheticreplacement:Acadaverstudy.JBoneJointSurgBr85(7):1006-1010,2003.
16. StabileKJ,PfaeffleHJ,TomainoMM:TheEssex-Loprestifracture-dislocation:Factorsinearlymanagementandsalvagealternatives.HandClin18(1):195-204,2002.
17. MorreyBF,SchneebergerAG:Anconeusarthroplasty:Anewtechnique for reconstruction of the radiocapitellar and/orproximalradioulnarjoint.JBoneJointSurgAm84(11):1960-1969,2002.
18. FroschKH,KnoppW,DresingK,etal:Abipolarradialheadprosthesis after comminuted radial head fractures: Indica-tions, treatment and outcome after 5 years. Unfallchirurg106(5):367-373,2003.
18. PierceROJr,HodurskiDF:Fracturesofthehumerus,radius,andulnainthesameextremity.JTrauma19:182,1979.
20. ReganW,MorreyBF:Classificationandtreatmentofcoronoidprocessfractures.Orthopedics15(7):845-848,1992.
21. RingDR,JupiterJB:Reconstructionofposttraumaticelbowinstability.ClinOrthop370:44-56,2000.
22. PattersonSD,BainGI,MehtaJA:Surgicalapproachestotheelbow.ClinOrthop370:19-33,2000.
23. HoppenfeldS,deBoerP:Theelbow.In: HoppenfeldS,deBoerP:Surgical Exposures in Orthopaedics(3rded).Philadelphia:Lippincott,Williams,andWilkins,2003.
24. O’DriscollSW:Elbowinstability.HandClinics 10(3):405-415,1994.
25. JupiterJB,RingDM:Treatmentofunreducedelbowdisloca-tionswithhingedexternalfixation.JBoneandJointSurgAm84(9):1630-1635,2002.
26. McKeeMD,BowdenSH,KingGJ,et al:Managementofrecurrent,complexinstabilityoftheelbowwithahingedex-ternalfixator.JBoneJointSurgBr80(6):1031-1036,1998.
27. RuchDS.TriepelCR:Hingedelbowfixationforrecurrentinstabilityfollowingfracturedislocation.Injury 32(4):70-78,2001.
Top Related