







Languages
Pages
Legal

CLINICAL EPIDEMIOLOGY www.jasn.org
Effects of Lowering LDL Cholesterol on Progression ofKidney Disease
Richard Haynes,* David Lewis,* Jonathan Emberson,* Christina Reith,* Lawrence Agodoa,†
Alan Cass,‡ Jonathan C. Craig,§ Dick de Zeeuw,| Bo Feldt-Rasmussen,¶ Bengt Fellström,**Adeera Levin,†† David C. Wheeler,‡‡ Rob Walker,§§ William G. Herrington,* Colin Baigent,*Martin J. Landray,* for the SHARP Collaborative Group
*Clinical Trial Service Unit and Epidemiological Studies Unit, Nuffield Department of Population Health, University ofOxford, Oxford, United Kingdom; †National Institute of Diabetes and Digestive and Kidney Diseases, NationalInstitutes of Health, Bethesda, Maryland; ‡Menzies School of Health Research, Charles Darwin University, Darwin,Northern Territory, Australia; §Sydney School of Public Health, Children’s Hospital at Westmead, University of Sydney,Sydney, New South Wales, Australia; |Department of Clinical Pharmacy and Pharmacology, University of Groningen,University Medical Centre Groningen, Groningen, The Netherlands; ¶Rigshospitalet, University of Copenhagen,Copenhagen, Denmark; **University Hospital, Uppsala, Sweden; ††University of British Columbia, Vancouver, BritishColumbia, Canada; ‡‡University College London, London, United Kingdom; and §§Dunedin School of Medicine,University of Otago, Otago, New Zealand
ABSTRACTLowering LDL cholesterol reduces the risk of developing atherosclerotic events in CKD, but the effects ofsuch treatment on progression of kidney disease remain uncertain. Here, 6245 participants with CKD (noton dialysis) were randomly assigned to simvastatin (20 mg) plus ezetimibe (10 mg) daily or matchingplacebo. The main prespecified renal outcome was ESRD (defined as the initiation of maintenance dialysisor kidney transplantation). During 4.8 years of follow-up, allocation to simvastatin plus ezetimibe resultedin an average LDL cholesterol difference (SEM) of 0.96 (0.02) mmol/L compared with placebo. There was anonsignificant 3% reduction in the incidence of ESRD (1057 [33.9%] cases with simvastatin plus ezetimibeversus 1084 [34.6%] cases with placebo; rate ratio, 0.97; 95% confidence interval [95% CI], 0.89 to 1.05;P=0.41). Similarly, allocation to simvastatin plus ezetimibe had no significant effect on the prespecifiedtertiary outcomes of ESRD or death (1477 [47.4%] events with treatment versus 1513 [48.3%] events withplacebo; rate ratio, 0.97; 95% CI, 0.90 to 1.04; P=0.34) or ESRD or doubling of baseline creatinine (1189[38.2%] events with treatment versus 1257 [40.2%] events with placebo; rate ratio, 0.93; 95% CI, 0.86 to1.01; P=0.09). Exploratory analyses also showed no significant effect on the rate of change in eGFR.Lowering LDL cholesterol by 1 mmol/L did not slow kidney disease progression within 5 years in a widerange of patients with CKD.
J Am Soc Nephrol 25: ccc–ccc, 2014. doi: 10.1681/ASN.2013090965
CKD affects about 1 in 10 adults and is associatedwith increased risks of cardiovascular disease,ESRD, and death.1 Only a minority of patientswith CKD will progress to ESRD (because mostpatients will die first), but the substantially elevatedrisks of morbidity and mortality associated withESRD,2 together with its effects on quality of life3
and cost to health care systems,4 make its preven-tion highly desirable. Although inhibition of therenin-angiotensin system does slow progressionof proteinuric nephropathies,5,6 there is a need
Received September 13, 2013. Accepted January 7, 2014.
R.H. and D.L. contributed equally to this work.
Published online ahead of print. Publication date available atwww.jasn.org.
Correspondence: Dr. Martin J. Landray, Clinical Trial ServiceUnit and Epidemiological Studies Unit, Richard Doll Building, OldRoad Campus, Roosevelt Drive, Oxford OX3 7LF, United King-dom. Email: [email protected]
Copyright © 2014 by the American Society of Nephrology
J Am Soc Nephrol 25: ccc–ccc, 2014 ISSN : 1046-6673/2508-ccc 1

for additional therapies that safely retard the progression ofCKD.
Experimental studies have suggested that lipids may contrib-ute to the progression of kidney disease.7 Previousmeta-analysesof randomized trials (which included patients without CKD andwith mild reductions in eGFR) have indicated that loweringLDL cholesterol might reduce the rate of loss of glomerularfiltration by about 1 ml/min per year.8,9 However, those trialsdid not include patients with advanced CKD (i.e., stage 3B andhigher), who typically progress at a faster rate than those patientsat earlier stages, among whom a similar proportional effectmight yield a worthwhile delay in ESRD.
The Study of Heart and Renal Protection (SHARP) showedthat lowering LDL cholesterol with simvastatin (20 mg) plusezetimibe (10mg) daily in patientswithCKD safely reduces theincidence of major atherosclerotic events10 and provides anopportunity to assess the effects of lowering LDL cholesterolon the progression of kidney disease.
RESULTS
In total, 6245 participants were not on dialysis at the point atwhich theywere randomized to simvastatinplus ezetimibe versusplacebo (Figure 1). This group included 10 patients (5 patientsallocated simvastatin plus ezetimibe, and 5 patients allocatedplacebo) who were initially randomized to simvastatin onlyand received a kidney transplant before rerandomization to sim-vastatin plus ezetimibe versus placebo (but excludes 2 patientswho were identified, after publication of the main trial results,10
as being on dialysis before rerandomization). Among all 6245patients, baseline characteristics were well balanced betweenrandomized treatments (Table 1, Supplemental Table 1). Among6027 (97%) patients with centrally measured creatinine, themean eGFR was 27 (SD=13) ml/min per 1.73 m2, with 3784(63%) patients having stages 4 or 5 CKD (i.e., eGFR,30ml/minper 1.73 m2). Among 5572 (89%) patients with a centrally mea-sured urinary albumin-to-creatinine ratio (ACR), 2357 (42%)patients had macroalbuminuria (ACR.34 mg/mmol). Themost common causes of kidney disease were hypertensive ne-phropathy or renovascular disease (22%), GN (18%), diabeticnephropathy (15%), and cystic kidney disease (11%).
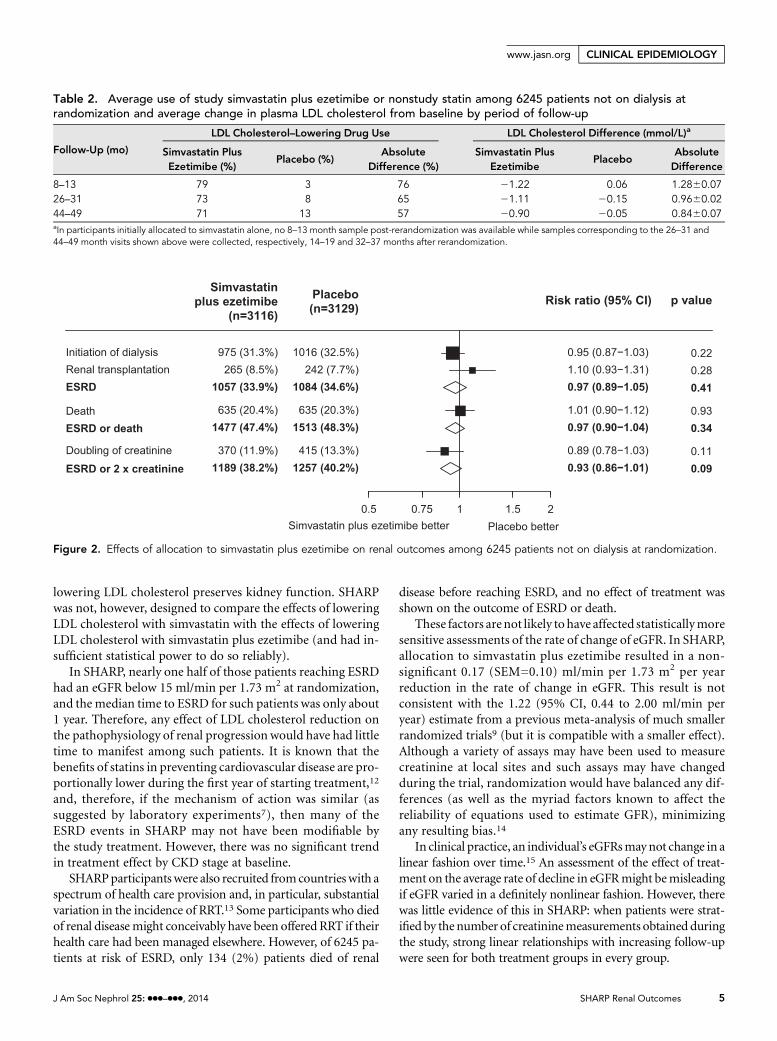
Among surviving patients, the median duration of follow-upwas 4.8 years. Compliance was defined as at least 80% of thescheduled simvastatin plus ezetimibe or placebo tablets havingbeen taken since the previous follow-up. At the study midpoint,2038 (73%) patients allocated simvastatin plus ezetimibe re-mained compliant or were taking a nonstudy statin, whereas 215(8%) patients allocated placebo were taking a nonstudy statin(Table 2). Hence, the average difference between the two ran-domized arms in the proportion taking simvastatin plus ezeti-mibe or nonstudy statin was 65%. The average LDL cholesteroldifference at the same point was 0.96 (SEM=0.02) mmol/L.
During the follow-up period, 1057 (33.9%) participantsallocated simvastatin plus ezetimibe reached ESRD compared
with 1084 (34.6%) patients allocated placebo (rate ratio [RR],0.97; 95% confidence interval [95% CI], 0.89 to 1.05; P=0.41)(Figure 2). Allocation to simvastatin plus ezetimibe was notassociated with a significant reduction in the risk of either ofthe prespecified subsidiary renal outcomes: ESRD or deathfrom any cause (RR, 0.97; 95% CI, 0.90 to 1.04; P=0.34) orESRD or doubling of baseline creatinine (RR, 0.93; 95% CI,0.86 to 1.01; P=0.09).
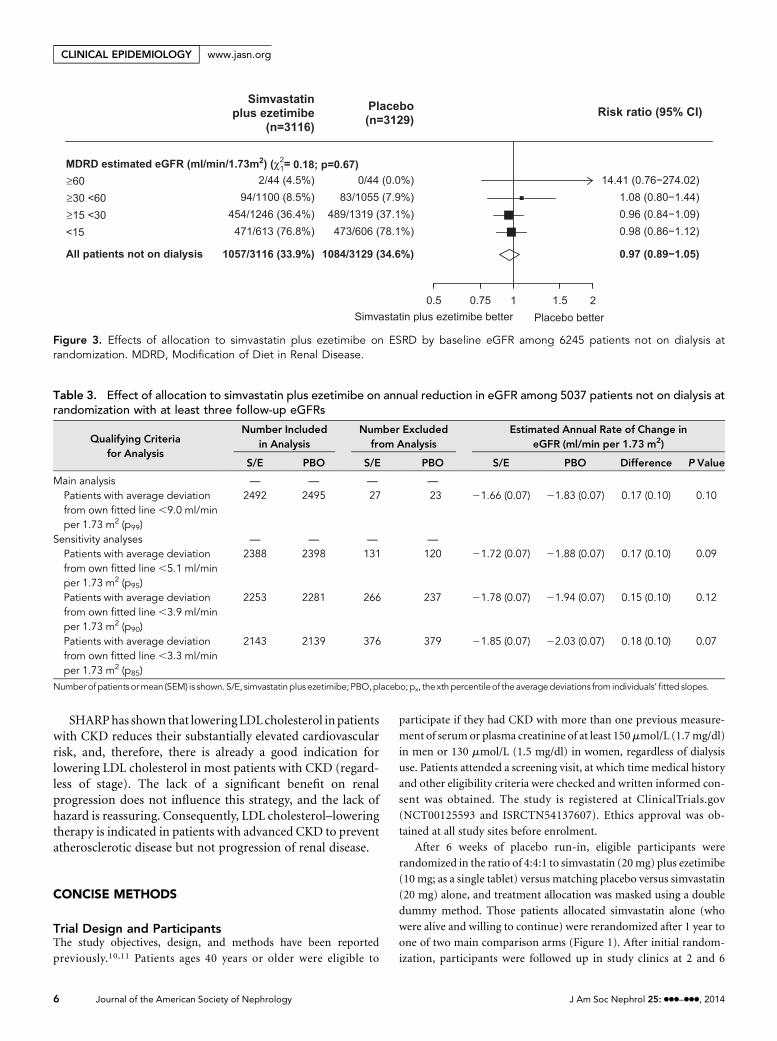
SHARPwas not expected to have sufficient statistical powerto allow reliable estimation of effects of treatment in particularclinical circumstances, and therefore, subgroup analyses wereplanned only as tertiary assessments.11 There was no evidencethat the proportional effect of allocation to simvastatin plusezetimibe on ESRD (or the other renal outcomes) differedbetween participants with different stages of CKD (Figure 3,Supplemental Figures 1 and 2) or among subgroups of partic-ipants defined by a range of other baseline characteristics afteraccounting for multiple testing (Supplemental Figures 1–4).
In total, 5037 (80%) participants had at least three follow-uplocal creatinine measurements in addition to a centrally mea-sured creatinine at randomization. The 50 (1%)patientswith themost extrememean deviations from their own fitted slopes wereexcluded (Table 3). Of the remaining 4987 patients, the mediannumber of creatinine measurements per patient was 10 (inter-quartile range=7–12). Those patients with fewer measurementshad lower eGFR at baseline and a faster average rate of decline ineGFR (Supplemental Figure 5, Supplemental Table 2). Whenparticipants were subdivided by their number of follow-upmeasurements, eGFRdeclined in a clearly linear fashion in everygroup (Supplemental Figure 5).Overall, allocation to simvastatinplus ezetimibe was not associated with a slower rate of changein eGFR (21.66 [SEM=0.07] versus21.83 [SEM=0.07]; abso-lute difference=0.17 [SEM=0.10] ml/min per 1.73 m2 per year;P=0.10) (Table 3). In sensitivity analyses, the estimated differ-ence in the rate of change in eGFR between treatment arms (andits SEM) was virtually identical when alternative approaches toexcluding patients with poorly fitting slopes were used (Table 3).Although those patients with more advanced CKD (whethercharacterized by lower eGFR or greater albuminuria) had fasterrates of progression, there were no trends to suggest any benefit(or hazard) of treatment on the rate of change in eGFR acrossthese subgroups (Figure 4) or any other subgroups (data notshown). In addition, among 3625 patients with centrally ana-lyzed cystatin C at the 2.5-year visit (who had not reached ESRDby that time), there was no significant difference in cystatin CeGFR between patients allocated simvastatin plus ezetimibe andpatients allocated placebo.
Exploratory analyses of effects of treatment on proteinuriaand acute-on-chronic renal failure were also undertaken.Among 3022 patients who had not commenced dialysis andhad provided a urine sample at the study midpoint, there wasno significant difference in geometric mean urinary ACR(simvastatin plus ezetimibe versus placebo: 168 [SEM=8.4]mg/g versus 154 [SEM=7.7] mg/g; P=0.20). Allocation to sim-vastatin plus ezetimibe was not associated with a reduction in
2 Journal of the American Society of Nephrology J Am Soc Nephrol 25: ccc–ccc, 2014
CLINICAL EPIDEMIOLOGY www.jasn.org

the risk of acute-on-chronic renal failure (209 [6.7%] versus231 [7.4%]; RR, 0.91; 95% CI, 0.75 to 1.09; P=0.30).
DISCUSSION
Among 6245 participants with CKD not on dialysis at random-ization, lowering LDL cholesterol by about 1 mmol/L with
simvastatin plus ezetimibe for about 5 years had no significanteffect on the progression of kidney disease to ESRD or thesubsidiary prespecified outcomes of ESRD or death from anycause, orESRDordoublingofbaseline creatinine. Thesefindingsare supported by the absence of a significant effect on thestatistically more sensitive rate of decline of eGFR. Subgroupanalyses did not identify any particular type of participant whoseemed tobenefitmore (or less) comparedwith theoverall result.
Figure 1. Trial profile and participant flow diagram.
J Am Soc Nephrol 25: ccc–ccc, 2014 SHARP Renal Outcomes 3
www.jasn.org CLINICAL EPIDEMIOLOGY

SHARP is the largest trial of LDL lowering in patients withadvanced CKD. With over 2000 ESRD events, it had excellentstatistical power (.90%) to detect a 15% proportional
reduction and good power (.80%) to detect a moremoderate10% reduction in the incidence of ESRD. These data, there-fore, are the most robust data available to assess whether
Table 1. Baseline characteristics by treatment allocation among 6245 patients not on dialysis at randomization
Simvastatin Plus Ezetimibe (n=3116) Placebo (n=3129)
Age at randomization (yr)a 63 (12) 63 (12)Men 1953 (63%) 1929 (62%)Prior vascular diseasea 473 (15%) 459 (15%)Diabetesa 718 (23%) 708 (23%)Current smokera 383 (12%) 379 (12%)Systolic BP (mmHg)a 139 (21) 139 (21)Diastolic BP (mmHg)a 80 (12) 80 (12)Total cholesterol (mmol/L)a 5.01 (1.18) 5.01 (1.15)LDL cholesterol (mmol/L)a 2.87 (0.87) 2.86 (0.85)HDL cholesterol (mmol/L)a 1.14 (0.34) 1.12 (0.34)Triglycerides (mmol/L)a 2.31 (1.63) 2.34 (1.68)Body mass index (kg/m2)a 27.4 (5.5) 27.4 (5.4)Ethnicityb
White 2248 (72%) 2235 (71%)Black 62 (2%) 57 (2%)Asian 748 (24%) 774 (25%)Other/not specified 58 (2%) 63 (2%)
Comedicationa,b
Antiplatelet therapy 614 (20%) 617 (20%)Oral anticoagulant therapy 82 (3%) 93 (3%)ACE inhibitor or ARB 1912 (61%) 1902 (61%)b-Blocker 1119 (36%) 1202 (38%)Calcium channel blocker 1388 (45%) 1356 (43%)Diuretic 1397 (45%) 1384 (44%)Erythropoiesis-stimulating agent 409 (13%) 359 (11%)Sevelamer 40 (1%) 24 (,1%)
MDRD eGFR (ml/min per 1.73 m2)a,c
Mean (SD) 26.6 (12.9) 26.6 (13.1)$60 44 (1%) 44 (1%)$30 to ,60 1100 (37%) 1055 (35%)$15 to ,30 1246 (41%) 1319 (44%),15 613 (20%) 606 (20%)Not available 113 105
Urinary ACR (mg/g)c
Median (interquartile range) 217 (44–787) 196 (43–746),30 545 (20%) 562 (20%)30–300 1032 (37%) 1076 (39%).300 1202 (43%) 1155 (41%)Not available 337 336
Renal diagnosisb,c
GN 528 (18%) 521 (17%)Diabetic nephropathy 445 (15%) 441 (15%)Hypertensive/renovascular 641 (21%) 661 (22%)Cystic kidney disease 329 (11%) 346 (12%)Pyelonephritis 198 (7%) 206 (7%)Other known cause 452 (15%) 434 (15%)Unknown cause 405 (14%) 383 (13%)Not available 118 137
Data are n (%), mean (SD), or median (interquartile range). ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blocker; MDRD,Modification of Diet inRenal Disease.aVariables updated at 1 year for patients originally allocated simvastatin only who were rerandomized to simvastatin plus ezetimibe or placebo.bNot a prespecified category for subgroup analyses.cPercentages exclude participants for whom data were not available for that category.
4 Journal of the American Society of Nephrology J Am Soc Nephrol 25: ccc–ccc, 2014
CLINICAL EPIDEMIOLOGY www.jasn.org
lowering LDL cholesterol preserves kidney function. SHARPwas not, however, designed to compare the effects of loweringLDL cholesterol with simvastatin with the effects of loweringLDL cholesterol with simvastatin plus ezetimibe (and had in-sufficient statistical power to do so reliably).
In SHARP, nearly one half of those patients reaching ESRDhad an eGFR below 15 ml/min per 1.73 m2 at randomization,and the median time to ESRD for such patients was only about1 year. Therefore, any effect of LDL cholesterol reduction onthe pathophysiology of renal progression would have had littletime to manifest among such patients. It is known that thebenefits of statins in preventing cardiovascular disease are pro-portionally lower during the first year of starting treatment,12
and, therefore, if the mechanism of action was similar (assuggested by laboratory experiments7), then many of theESRD events in SHARP may not have been modifiable bythe study treatment. However, there was no significant trendin treatment effect by CKD stage at baseline.
SHARPparticipantswere also recruited fromcountrieswith aspectrum of health care provision and, in particular, substantialvariation in the incidence of RRT.13 Some participants who diedof renal diseasemight conceivably have been offered RRT if theirhealth care had been managed elsewhere. However, of 6245 pa-tients at risk of ESRD, only 134 (2%) patients died of renal
disease before reaching ESRD, and no effect of treatment wasshown on the outcome of ESRD or death.
These factors arenot likely to have affected statisticallymoresensitive assessments of the rate of change of eGFR. In SHARP,allocation to simvastatin plus ezetimibe resulted in a non-significant 0.17 (SEM=0.10) ml/min per 1.73 m2 per yearreduction in the rate of change in eGFR. This result is notconsistent with the 1.22 (95% CI, 0.44 to 2.00 ml/min peryear) estimate from a previous meta-analysis of much smallerrandomized trials9 (but it is compatible with a smaller effect).Although a variety of assays may have been used to measurecreatinine at local sites and such assays may have changedduring the trial, randomization would have balanced any dif-ferences (as well as the myriad factors known to affect thereliability of equations used to estimate GFR), minimizingany resulting bias.14
In clinical practice, an individual’s eGFRsmay not change in alinear fashion over time.15 An assessment of the effect of treat-ment on the average rate of decline in eGFRmight bemisleadingif eGFR varied in a definitely nonlinear fashion. However, therewas little evidence of this in SHARP: when patients were strat-ified by thenumber of creatininemeasurements obtained duringthe study, strong linear relationships with increasing follow-upwere seen for both treatment groups in every group.
Table 2. Average use of study simvastatin plus ezetimibe or nonstudy statin among 6245 patients not on dialysis atrandomization and average change in plasma LDL cholesterol from baseline by period of follow-up
Follow-Up (mo)
LDL Cholesterol–Lowering Drug Use LDL Cholesterol Difference (mmol/L)a
Simvastatin PlusEzetimibe (%)
Placebo (%)Absolute
Difference (%)Simvastatin Plus
EzetimibePlacebo
AbsoluteDifference
8–13 79 3 76 21.22 0.06 1.2860.0726–31 73 8 65 21.11 20.15 0.9660.0244–49 71 13 57 20.90 20.05 0.8460.07aIn participants initially allocated to simvastatin alone, no 8–13 month sample post-rerandomization was available while samples corresponding to the 26–31 and44–49 month visits shown above were collected, respectively, 14–19 and 32–37 months after rerandomization.
Figure 2. Effects of allocation to simvastatin plus ezetimibe on renal outcomes among 6245 patients not on dialysis at randomization.
J Am Soc Nephrol 25: ccc–ccc, 2014 SHARP Renal Outcomes 5
www.jasn.org CLINICAL EPIDEMIOLOGY
SHARPhas shown that loweringLDLcholesterol in patientswith CKD reduces their substantially elevated cardiovascularrisk, and, therefore, there is already a good indication forlowering LDL cholesterol in most patients with CKD (regard-less of stage). The lack of a significant benefit on renalprogression does not influence this strategy, and the lack ofhazard is reassuring. Consequently, LDL cholesterol–loweringtherapy is indicated in patients with advanced CKD to preventatherosclerotic disease but not progression of renal disease.
CONCISE METHODS
Trial Design and ParticipantsThe study objectives, design, and methods have been reported
previously.10,11 Patients ages 40 years or older were eligible to
participate if they had CKD with more than one previous measure-
ment of serumor plasma creatinine of at least 150mmol/L (1.7mg/dl)
in men or 130 mmol/L (1.5 mg/dl) in women, regardless of dialysis
use. Patients attended a screening visit, at which time medical history
and other eligibility criteria were checked and written informed con-
sent was obtained. The study is registered at ClinicalTrials.gov
(NCT00125593 and ISRCTN54137607). Ethics approval was ob-
tained at all study sites before enrolment.
After 6 weeks of placebo run-in, eligible participants were
randomized in the ratio of 4:4:1 to simvastatin (20mg) plus ezetimibe
(10 mg; as a single tablet) versus matching placebo versus simvastatin
(20 mg) alone, and treatment allocation was masked using a double
dummy method. Those patients allocated simvastatin alone (who
were alive and willing to continue) were rerandomized after 1 year to
one of two main comparison arms (Figure 1). After initial random-
ization, participants were followed up in study clinics at 2 and 6
Figure 3. Effects of allocation to simvastatin plus ezetimibe on ESRD by baseline eGFR among 6245 patients not on dialysis atrandomization. MDRD, Modification of Diet in Renal Disease.
Table 3. Effect of allocation to simvastatin plus ezetimibe on annual reduction in eGFR among 5037 patients not on dialysis atrandomization with at least three follow-up eGFRs
Qualifying Criteriafor Analysis
Number Includedin Analysis
Number Excludedfrom Analysis
Estimated Annual Rate of Change ineGFR (ml/min per 1.73 m2)
S/E PBO S/E PBO S/E PBO Difference P Value
Main analysis — — — —
Patients with average deviationfrom own fitted line ,9.0 ml/minper 1.73 m2 (p99)
2492 2495 27 23 21.66 (0.07) 21.83 (0.07) 0.17 (0.10) 0.10
Sensitivity analyses — — — —
Patients with average deviationfrom own fitted line ,5.1 ml/minper 1.73 m2 (p95)
2388 2398 131 120 21.72 (0.07) 21.88 (0.07) 0.17 (0.10) 0.09
Patients with average deviationfrom own fitted line ,3.9 ml/minper 1.73 m2 (p90)
2253 2281 266 237 21.78 (0.07) 21.94 (0.07) 0.15 (0.10) 0.12
Patients with average deviationfrom own fitted line ,3.3 ml/minper 1.73 m2 (p85)
2143 2139 376 379 21.85 (0.07) 22.03 (0.07) 0.18 (0.10) 0.07
Numberofpatients ormean (SEM) is shown.S/E, simvastatinplus ezetimibe; PBO,placebo;px, thexthpercentileof the averagedeviations from individuals’fitted slopes.
6 Journal of the American Society of Nephrology J Am Soc Nephrol 25: ccc–ccc, 2014
CLINICAL EPIDEMIOLOGY www.jasn.org

months and then, every 6 months for at least 4 years. At each of these
visits, information on RRT and all serious adverse events was recor-
ded, and blood samples were taken for serum or plasma creatinine
measurement in the site’s local routine laboratory. Samples of non-
fasting blood (and urine from those patients not on dialysis) for
central laboratory measurement were also collected from all partic-
ipants at randomization and 2.5 years and about 10% of participants
attending study visits at 1 and 4 years after the initial randomization.
These blood samples were cooled, spun, and separated before being
stored locally at240°C. Samples were then shipped on dry ice to the
central laboratory in Oxford, United Kingdom, where assays of lipids,
creatinine, cystatin C, and urinary ACR were conducted. Creatinine,
albumin, and lipids were measured using a Synchron LX20 or
DXC800 analyzer (Beckman Coulter), whereas
cystatin C was measured by immunonephelom-
etry using a Dade Behring BNII nephelometer
(Siemens AG). Creatinine was assayed using a
kinetic alkaline picrate method and calibrated
using material traceable to National Institute
of Standards and Technology Standard Refer-
ence Material 914a, with a mean expanded un-
certainty of 13.4% (7.3% excluding biologic
variation).
Statistical AnalysesThemain prespecified renal outcomewas ESRD,
defined as the initiation of maintenance dialysis
or kidney transplantation.11 Prespecified sub-
sidiary renal outcomes included the composite
outcomes ESRD or death from any cause and
ESRD or doubling of baseline creatinine. It
was also prespecified that the effect of simvastat-
in plus ezetimibe on the rate of change in eGFR
would be explored. Acute-on-chronic renal fail-
ure was reported by investigators as a serious
adverse event and not a prespecified outcome.
Analyses were from time of randomization
to initiation of simvastatin plus ezetimibe or
placebo, such that for those patients initially
allocated simvastatin (20 mg) daily, events
occurring before rerandomization were used
only to update baseline characteristics. All ana-
lysesweredone according to the intention to treat
principle.
eGFR was calculated using the four-variable
Modification of Diet in Renal Disease study
equation.16 For each patient, linear regression
was used to estimate the rate of change in
eGFR from the locally measured creatinine val-
ues (ignoring measurements after ESRD). The
validity of making such a linearity assumption
was assessed graphically. Because the reliability
of such estimated progression rates is affected
by the number of available creatinine mea-
surements (with fewer creatinine measurements
resulting in less reliable estimates of the true progression rate), partic-
ipants with fewer than three follow-up creatinine measurements were
excluded. In addition, participants with the mean deviation from
their own fitted slope in the top 1% of the distribution (of mean
deviations across all participants) were also excluded. The mean
rate of change in eGFR was then compared between participants
allocated simvastatin plus ezetimibe and participants allocated pla-
cebo (both overall and in particular patient subgroups). Sensitivity
analyses were conducted to assess the extent that the results varied if
different criteria were used for exclusion of estimated eGFR slopes
and separately using the Chronic Kidney Disease Epidemiology Col-
laboration equation.17 Analyses were performed using SAS version 9
(Cary Institute) and R version 2.11.1 (www.R-project.org).
Figure 4. Effect of allocation to simvastatin plus ezetimibe on rate of change in eGFRamong 5037 patients not on dialysis at randomization with at least three follow-upeGFRs by baseline (A) eGFR and (B) albuminuria.
J Am Soc Nephrol 25: ccc–ccc, 2014 SHARP Renal Outcomes 7
www.jasn.org CLINICAL EPIDEMIOLOGY

ACKNOWLEDGMENTS
The most important acknowledgement is to the participants in the
Study of Heart and Renal Protection (SHARP) and the local clinical
centre staff, regional and national coordinators, steering committee,
and data monitoring committee.
The study was funded by Merck/Schering-Plough Pharmaceu-
ticals, with additional support from the Australian National Health and
Medical Research Council, the British Heart Foundation, and the UK
Medical Research Council.
The main funding source (Merck/Schering-Plough Pharmaceu-
ticals) participated in initial discussions about trial design, contributed
two nonvoting observers to the steering committee, and had a right to
comment on (but not require changes to) study reports. It had no
involvement in data collection, analysis, interpretation, report writ-
ing, or decision to submit for publication, and it has not received an
unmasked copy of the trial database. The writing committee accepts
full responsibility for the content of this paper. All members con-
tributed to the collection and analysis of the data and the preparation
of the manuscript. All collaborators had an opportunity to contribute
to the interpretation of the results and the drafting of the manuscript.
The SHARP Steering Committee is Colin Baigent (University of
Oxford), Martin J. Landray (University of Oxford), Christina Reith
(University of Oxford), Jonathan Emberson (University of Oxford),
David C. Wheeler (University College London), Charles Tomson
(North Bristol NHS Trust), Christoph Wanner (University of
Wuerzburg), Vera Krane (University of Wuerzburg), Alan Cass
(Charles Darwin University), Jonathan Craig (University of Sydney),
Bruce Neal (University of Sydney), Lixin Jiang (Chinese Academy of
Medical Sciences and PekingUnionMedical College), Lai SeongHooi
(Sultanah Aminah Hospital), Adeera Levin (University of British
Columbia), Lawrence Agodoa (National Institutes of Health), Mike
Gaziano (Harvard Medical School), Bertram Kasiske (University of
Minnesota), Rob Walker (University of Otago), Ziad A. Massy
(University of Picardie Jules Verne), Bo Feldt-Rasmussen (University
of Copenhagen), Udom Krairittichai (Rajavithi Hospital), Vuddidhej
Ophascharoensuk (Chiang Mai University), Bengt Fellström (Uni-
versity Hospital), Hallvard Holdaas (Oslo University Hospital),
Vladimir Tesar (Charles University), Andrzej Wiecek (Medical Uni-
versity of Silesia), Diederick Grobbee (University Medical Center
Utrecht), Dick de Zeeuw (University Medical Centre Groningen),
Carola Grönhagen-Riska (Helsinki University Hospital), Tanaji
Dasgupta (Oxford University Hospitals NHS Trust), David Lewis
(University of Oxford), Will Herrington (University of Oxford),
Marion Mafham (University of Oxford), William Majoni (Royal
Darwin Hospital), Karl Wallendszus (University of Oxford), Richard
Grimm (University of Minnesota), Terje Pedersen (Oslo University
Hospital Ulleval), Jonathan Tobert (TobertMedical Consulting LLC),
Jane Armitage (University of Oxford), Alex Baxter (University of
Oxford), Christopher Bray (University of Oxford), Yiping Chen
(University of Oxford), Zhengming Chen (University of Oxford),
Michael Hill (University of Oxford), Carol Knott (University of Ox-
ford), Sarah Parish (University of Oxford), David Simpson (University
of Oxford), Peter Sleight (University of Oxford), Alan Young (Uni-
versity of Oxford), and Rory Collins (University of Oxford).
DISCLOSURESThe Study ofHeart andRenal Protection (SHARP)was initiated, conducted,
and interpreted independently of the principal study funder (Merck/Schering-
Plough Pharmaceuticals). The Clinical Trial Service Unit and Epidemiological
StudiesUnit,whicharepartof theUniversityofOxford,havea staff policyofnot
accepting honoraria or consultancy fees.
REFERENCES
1. Levey AS, Coresh J: Chronic kidney disease. Lancet 379: 165–180,2012
2. Foley RN, Parfrey PS, Sarnak MJ: Clinical epidemiology of cardiovas-cular disease in chronic renal disease. Am J Kidney Dis 32[Suppl 3]:S112–S119, 1998
3. Evans RW, Manninen DL, Garrison LP Jr., Hart LG, Blagg CR, GutmanRA, Hull AR, Lowrie EG: The quality of life of patients with end-stagerenal disease. N Engl J Med 312: 553–559, 1985
4. US Renal Data System: 2010 Annual Data Report: Atlas of ChronicKidney Disease. Costs of End-Stage Renal Disease, 2010. Available at:http://www.usrds.org/2010/pdf/v2_11.pdf. Accessed June 18, 2013
5. Jafar TH, SchmidCH, LandaM,Giatras I, Toto R, Remuzzi G,MaschioG,Brenner BM, Kamper A, Zucchelli P, Becker G, Himmelmann A,Bannister K, Landais P, Shahinfar S, de Jong PE, de Zeeuw D, Lau J,Levey AS: Angiotensin-converting enzyme inhibitors and progressionof nondiabetic renal disease. Ameta-analysis of patient-level data. AnnIntern Med 135: 73–87, 2001
6. Lewis EJ, Hunsicker LG, Clarke WR, Berl T, Pohl MA, Lewis JB, Ritz E,Atkins RC, Rohde R, Raz I; Collaborative Study Group: Renoprotectiveeffect of the angiotensin-receptor antagonist irbesartan in patients withnephropathy due to type 2 diabetes.NEngl JMed 345: 851–860, 2001
7. Moorhead JF, Chan MK, El-Nahas M, Varghese Z: Lipid nephrotoxicityin chronic progressive glomerular and tubulo-interstitial disease. Lan-cet 2: 1309–1311, 1982
8. Tonelli M, Isles C, Craven T, Tonkin A, Pfeffer MA, Shepherd J, SacksFM, Furberg C, Cobbe SM, Simes J, West M, Packard C, Curhan GC:Effect of pravastatin on rate of kidney function loss in people with or atrisk for coronary disease. Circulation 112: 171–178, 2005
9. Sandhu S, Wiebe N, Fried LF, Tonelli M: Statins for improving renaloutcomes: A meta-analysis. J Am Soc Nephrol 17: 2006–2016, 2006
10. Baigent C, Landray MJ, Reith C, Emberson J, Wheeler DC, Tomson C,Wanner C, Krane V, Cass A, Craig J, Neal B, Jiang L, Hooi LS, Levin A,Agodoa L, GazianoM, Kasiske B,Walker R,Massy ZA, Feldt-RasmussenB, Krairittichai U, Ophascharoensuk V, Fellström B, Holdaas H, Tesar V,Wiecek A, Grobbee D, de Zeeuw D, Grönhagen-Riska C, Dasgupta T,Lewis D, HerringtonW,MafhamM,MajoniW,Wallendszus K, GrimmR,Pedersen T, Tobert J, Armitage J, Baxter A, Bray C, Chen Y, Chen Z, HillM, Knott C, Parish S, Simpson D, Sleight P, Young A, Collins R; SHARPInvestigators: The effects of lowering LDL cholesterol with simvastatinplus ezetimibe in patients with chronic kidney disease (Study of Heartand Renal Protection): A randomised placebo-controlled trial. Lancet377: 2181–2192, 2011
11. Sharp Collaborative Group: Study of Heart and Renal Protection(SHARP): Randomized trial to assess the effects of lowering low-densitylipoprotein cholesterol among 9,438 patients with chronic kidney dis-ease. Am Heart J 160: 785–794, e10, 2010
12. Baigent C, Blackwell L, Emberson J, Holland LE, Reith C, Bhala N, PetoR, Barnes EH, Keech A, Simes J, Collins R; Cholesterol TreatmentTrialists’ (CTT) Collaboration: Efficacy and safety of more intensivelowering of LDL cholesterol: A meta-analysis of data from 170,000participants in 26 randomised trials. Lancet 376: 1670–1681, 2010
13. Jha V,Garcia-GarciaG, Iseki K, Li Z, Naicker S, Plattner B, Saran R,WangAY, Yang CW: Chronic kidney disease: Global dimension and per-spectives. Lancet 382: 260–272, 2013
8 Journal of the American Society of Nephrology J Am Soc Nephrol 25: ccc–ccc, 2014
CLINICAL EPIDEMIOLOGY www.jasn.org

14. Stevens LA, Coresh J, Greene T, Levey AS: Assessing kidney function—measured and estimated glomerular filtration rate. N Engl J Med 354:2473–2483, 2006
15. Li L, Astor BC, Lewis J, Hu B, Appel LJ, Lipkowitz MS, Toto RD,Wang X,Wright JT Jr., Greene TH: Longitudinal progression trajectory of GFRamong patients with CKD. Am J Kidney Dis 59: 504–512, 2012
16. Levey AS, Greene T, Kusek JW, Beck GJ; MDRD Study Group: A sim-plified equation to predict glomerular filtration rate from serum creat-inine [Abstract]. J Am Soc Nephrol 11: 155A, 2000
17. Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF 3rd, Feldman HI,Kusek JW, Eggers P, Van Lente F, Greene T, Coresh J; CKD-EPI (ChronicKidney Disease Epidemiology Collaboration): A new equation to esti-mate glomerular filtration rate. Ann Intern Med 150: 604–612, 2009
This article contains supplemental material online at http://jasn.asnjournals.org/lookup/suppl/doi:10.1681/ASN.2013090965/-/DCSupplemental.
J Am Soc Nephrol 25: ccc–ccc, 2014 SHARP Renal Outcomes 9
www.jasn.org CLINICAL EPIDEMIOLOGY
Top Related