






Languages
Pages
Legal


Dr. Vijay Viswanathan, M.D, Ph.D, MNAMS
Joint DirectorDiabetes Research Centre &M. V. Hospital for Diabetes
Chennai.
WHO Collaborating Centre for Research, Education & Training in diabetes

Factors found in Diabetes and Impaired wound healing
Peripheral neuropathy• Loss of protective sensation
• Autonomic dysfunction
• Impaired neuroinflammatory
reflexWound hypoxia• Macrovascular disease
• Microvascular disease
• Capillary loss
• Microvascular endothelial
dysfunction

Factors found in Diabetes and Impaired wound healing
Abnormal cellular pathways• Chemotaxis
• Fibroblast responsiveness
Excess inflammation• Oxidative stress
• Endothelial dysfunction and impaired nitric oxide
signaling
• Increased inflammatory cytokine expression
• Advanced glycosylation end products (AGEs) and
receptors (RAGE)Deficient precursor cells

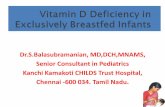
HEMOSTASIS 1 hour
W
O
U
N
D
I
N
G
Platelets
Fibrin
INFLAMMATION days 1 through 7
Proteoglycans
Neutrophils
Macrophages]
LymphocytesPROLIFERATION days 2 through 20
Phases of normal wound healing
Fibroblasts[produce growth factors]
Collagen
Epithelial Cells
Endothelial CellsREMODELING 1 week to 6 months
Collagen Fibril Crosslinking
Scar Maturation
Time from injury

These stimulate synthesis of proteases (MMP’S)
Degrade matrix proteins & growth factors
Disruption in wound healing
Prolonged inflammatory reaction
in no. of neutrophils in the wound
These secrete proinflammatory cytokines (TNF - ), Interleukin (IL - 1)
Due to (1) Bacterial contamination (2) Recurrent painless tissue trauma
What happens in diabetes mellitus to wound healing

Changes at the molecular level in diabetes and their potential interrelationships leading to alterations of macromolecular
functions, which contribute to poor healing and ulcer formation
(a) Diminished neuroinflammatory signalling
NGF Nerve content
Substance P
Neuroinflammatory signalling
Glucose NEP activity

Changes at the molecular level in diabetes and their potential interrelationships leading to alterations of macromolecular
functions, which contribute to poor healing and ulcer formation
(b) Pathways of oxygen free radical production which in turn could damage DNA of cells involved in wound
healing
Glucose Glycation AGE
Activity antioxidant enzymes
GSH
Oxygen free radicals
Damage cellular
DNA
Arginase and NOS activities

Changes at the molecular level in diabetes and their potential interrelationships leading to alterations of macromolecular
functions, which contribute to poor healing and ulcer formation(c) Decreased angiogenesis
TGF - 1
Angiogenesis
NOS activity
NOS activity
NO
NO
IL - 6 bFGF
IL - 6
KGF
VEGF
NGF TGF - 1 IGF - 1 TGF - 1
NGF
KGF
bFGF
IL - 6

Changes at the molecular level in diabetes and their potential interrelationships leading to alterations of macromolecular
functions, which contribute to poor healing and ulcer formation
(d) Diminished ECM deposition
TGF - 1
ECM deposition NO
IGF - 1
Collagen synthesis
GAG synthesis
Neutrophil elastase and cathepsin G activities
TIMP
TGF - 1
MMP activity
TNF

Imbalances in the molecular environments of acute healing wounds and chronic non-healing
wounds
Molecular environment of wounds
Healing wounds
High Mitogenic activity
Low inflammatory cytokines
Low proteases
Mitotically competent cells Chronic Ulcers
Low Mitogenic activity
High inflammatory cytokines
High proteases
Senescent cells

Vijay Viswanathan *, Shiny John Vairamon **, A. Ramachandran *, C. Snehalatha * and Mary Babu **
* : Diabetes Research Centre, Royapuram, Chennai – 13, India
** : Biomaterial division, Central Leather Research Institute, Adyar, Chennai – 20 , India

Aim
To study the role of the inflammatory
status in the delayed wound healing of
diabetic patients

Subjects:
Study groups were:
• Group 1: Non-diabetic controls (n=10)
• Group 2: Patients with diabetes (n=10)
• Group 3: Diabetic neuropaths with foot ulceration [non infected] (n=10)
• Group 4: Diabetic neuropaths with foot ulceration [infected] (n=10)
• Group 5: Diabetic patients with neuroischemia and foot ulceration
[non infected] (n=10)
• Group 6: Diabetic patients with neuroischemia and foot ulceration
[infected] (n=10)

Matrix – degrading metalloproteinases (MMP)
Physiologic mediators of matrix degradation
Zinc dependent endopeptidases, which are capable of collectively degrading all kinds of extracellular matrix proteins
Play an important role in tissue remodeling
Matrix – degrading metalloproteinases (MMP)
Collagenases Gelatinases Stromelysins
Gelatinase A (MMP – 2)
Gelatinase B (MMP – 9)
Product of other cell types, including neutrophils and
keratinocytes

Methods
o Neuropathy was diagnosed ad VPT>25V by biothesiometer
o Peripheral vascular disease was diagnosed as ankle brachial
index (ABI)<0.8
o The expression of Matrix Metalloprotinases in tissue
homogenates (MMP-9) of diabetic foot ulcers and also in the
serum of the subjects (MMP-2) by Zymogram & Western
Blot




Results
MMP-9 active form was expressed in the tissue homogenate
of diabetic patients both in neuropathy & neuroischemic
with infective foot ulcer and not in diabetic patients with
callus
MMP-2 active form was expressed more in the serum of
diabetic patients both in neuropathy and neuroischemic with
infective foot ulceration.

The over expression of matrix
metalloprotinases in the wound tissue
contribute to the delayed wound healing.

Platelet – derived growth factor (PDGF)
PDGF plays a role in most phases of wound healing
displaying a variety of activities including as a
chemoattractant
stimulating cells to secrete growth factors and
inducing the production of several matrix molecules.
[Heldin CH et al., Physiol Rev 1999; 79: 1283 – 1316]
[Goldman R et al., Adv Skin Wound Care 2004; 17: 24 - 35]
Lack of PDGF protein was found in chronic wound fluid from
diabetic patients.
[Castronuovo JJ Jr et al., Am J Surg 1998; 176: 61S – 67S]
Addition of PDGF has been shown to enhance wound healing
and increase wound – breaking strength.
[Pierce GF et al., J Cell Biol 1989; 109: 429 - 440]

Components of Optimal Wound Care
• A comprehensive, standardisedwound care regimen
• Correct underlying condition
• Control infection
• Address ischaemia
• Correct structural defects
• Adequate glycaemic control for diabetic patients
• Adequate debridement
• Appropriate topical management (eg growth factors)

Wound dressings and treatments

• Today there are more than 2000 wound care products available, most of which are different varieties of dressings (Cohen IK, 1998) .
• Most modern dressings contain materials that are highly absorbent, such as alginates or foam. The list of modern wound dressings available is long and impressive; some types include :
Alginates Composites Exudate absorbers Foams Gauzes Hydrocolloids Hydrogels Skin Sealants Transparent Films
(Mulder GD, Haberer PA, Jeter KF, 1998)

Use of Biatin Silver in different types of Diabetic Foot Wounds
Why add Silver?
The antimicrobial of silver (or more accurately silver ions, Ag+) were
exploited long before microbes were discovered.
They selectively bind to thiol groups, which are widely distributed in
bacterial cell wall proteins
Also bind to bacterial DNA [Lansdown, 2002]
The silver added to advanced wound management products (AWMP)
is added in forms designed to make the cations more readily available.

Name : Mrs. Pusphammal
Age: 61 years Sex: Female
Diabetic for 10 years ; HbA1c: 12.2%;
H/O pinprick over right heel – 3 wks back; came
with a right heel abscess; discharging pus;; X-
ray foot showed osteomyelitis of right
calcaneum
Urea / Creatinine / Neuropathy: Normal
Patient underwent debridement and bone
curettage on 6/3/06 ; Normal vascularity
Started on Biatain Ag dressing from 1st Post
operative day
Came for review on 30/3/06 and 5/4/06
Wound looks clean; size has decreased ;
granulations have started covering calcaneum.

Name : Mr. Chinnaiah.P
Age: 68 years Sex: Male
Diabetic for 6 years ; HbA1c: 6.5%;
Admitted with left charcot foot with midfoot
collapse with plantar midfoot ulcer 5 x 5cm with a
cavity underneath with cellulitis leg.
Ulcer debrided on 5/3/06 ; OM of underlying bones
+ ; infected bones curetted ; good vascularity
Started on Biatain dressing from 7/3/06
CAD / Nephropathy (S. Creat : 4.8) ; Neuropathy +
Came for review on 27/3/06
Ulcer has decreased in size ; some maceration
present.

Hippocrates said that: “Healing is a matter
of time, but it is sometimes also a matter of
opportunity”.
Hippocrates (460 BC – 377 BC), Precepts.
This is very relevant concept when applied to
the diabetic foot
Top Related