







Languages
Pages
Legal


Documentation Guidelines February 2018– NYCC Health Centers
This document is to be used as a guide for proper documentation and in conjunction with the
File Review process by both students in the DCP and by clinicians as it relates to quality
assurance. This guide describes proper documentation and location details that are expected in
the SmartCloud EHR. Paper SOAP notes and other documentation items are expected to be
present within the patient’s case file in a similarly organized system. For evaluation and
mentoring purposes, the draft version of SOAP notes submitted by chiropractic students should
be utilized. [In SmartCould, the student’s SOAP note submissions can be viewed by using the
“View Document History” function.]
Contents 1) Privacy practice ............................................................................................................... 3
2) Problem list – The Problem Oriented Medical Record (POMR) ................................ 3
3) Patient history .................................................................................................................. 4
4) Clinical Examination ....................................................................................................... 6
5) Diagnostic testing and diagnostic imaging .................................................................... 8
6) Diagnosis .......................................................................................................................... 8
7) Informed consent ........................................................................................................... 10
8) In-office treatment plan (Patient Care Plan) .............................................................. 13
9) Self-care recommendations / Home Care recommendations .................................... 14
10) Treatment goals ........................................................................................................... 15
11) Outcome measurements .............................................................................................. 16
12) Progress notes .............................................................................................................. 17
13) Patient response to care per formal assessment of patient progress ...................... 18
14) Management plan modification ................................................................................. 20
15) Documentation supports billing ................................................................................. 20
Appendix............................................................................................................................. 21
Privacy practice – details .................................................................................................. 21
Example of an executed Report of Findings (ROF) and Informed Consent (IC) form:
............................................................................................................................................. 21
Patient history – details ....................................................................................................... 25
Clinical examination – Objective Speed Note example: ...................................................... 26

Clinical examination – Examinations page example: ........................................................... 26
Clinical examination – Physical Exam page example: .......................................................... 27
Patient Care Plan (Case Types) ............................................................................................ 27
Example patient care plan in SmartCloud: .......................................................................... 34
Progress notes – SmartCloud Plan Speed Note ................................................................... 36
Discharge documentation: .................................................................................................. 37
In-office treatment plan – details ........................................................................................ 37
Self-care recommendations - details ................................................................................... 37
Treatment goals – details .................................................................................................... 38
Outcome measurements - details ....................................................................................... 40
Revised Oswestry Back Pain Disability Questionnaire ....................................................... 41
Management plan modification – details ............................................................................ 42
Documentation supports billing – details ............................................................................ 42

1) Privacy practice The patient privacy verification is located on the back of the patient registration packet. The
HIPAA Notice of Patient Privacy Practices may be provided to the patient upon request, unless
emergency conditions make it impossible (the latter should be documented). The privacy
verification should be signed by the patient on the first day they present to the health center
and scanned into the patient record in the EHR. A form not dated the first day or signed by the
patient (or a form not present at all) is a clear deficiency.
Click here for detailed privacy practice information
Return to the top.
2) Problem list – The Problem Oriented Medical Record (POMR) POMR is a method of recording data about the health status of a patient in a problem-solving
system. The POMR preserves the data in an easily accessible way that encourages ongoing
assessment and revision of the health care plan by all members of the health care team. The
particular format of the system used varies from setting to setting, but the components of the
method are similar. A data base is collected before beginning the process of identifying the
patient's problems. The data base consists of all information available that contributes to this
end, such as that collected in an interview with the patient and family or others, that from a
health assessment or physical examination of the patient, and that from various laboratory and
radiological tests. It is recommended that the data base be as complete as possible, limited only
by potential hazard, pain or discomfort to the patient, or excessive assumed expense of the
diagnostic procedure. The interview, augmented by prior records, provides the patient's history,
including the reason for contact; an identifying statement that is a descriptive profile of the
person; a family illness history; a history of the current illness; a history of past illness; an
account of the patient's current health practices; and a review of systems. The physical
examination or health assessment makes up the second major part of the data base. The extent
and depth of the examination vary from setting to setting and depend on the services offered
and the condition of the patient. The next section of the POMR is the master problem list. The
formulation of the problems on the list is similar to the [assessment section of the SOAP note].
Each problem as identified represents a conclusion or a decision resulting from examination,
investigation, and analysis of the data base. A problem is defined as anything that causes
concern to the patient or to the caregiver, including physical abnormalities, psychological
disturbance, and socioeconomic problems. The master problem list usually includes active,
inactive, temporary, and potential problems. – An excerpt from Mosby's Medical Dictionary, 9th
edition. © 2009, Elsevier.
See sample Problem List

3) Patient history An appropriate, structured, complete history should be obtained and recorded at any clinical
evaluation. Every clinical evaluation history should include:
- Items relevant to the chief complaint and problems revealed during the evaluation
- A review of medical, social, and family histories, appropriate to the complexity of the
complaint and patient; each element should be noted
- A review of relevant systems
Various mnemonics are used to represent the “core” components of a patient history, some
more common to specific regions or disciplines. These include:
OPQRST (onset, provoking/palliative factors, quality, radiation, site, temporal factors
LMNOPQRST (location, mechanism or medical history, new symptoms, other symptoms,
provoking/palliative factors, quality, radiation, severity, timing)
SOCRATES (site, onset, character, radiation, alleviating factors, timing, exacerbating
factors, severity).
While these can guide the taking of a structured, complete history, it is important that all
relevant information is obtained and recorded, not only regarding the chief presenting
complaint(s) (e.g. course/progression of the complaint, previous treatments and response to
SmartCloud Location: “Problem List” Page
The Problem List in the SmartCloud EHR is the starting point of the patient’s initial and subsequent SOAP
notes. Due to the functionality of the SmartCloud electronic health record, it is necessary to choose a
problem (an ICD-10 code) in order to introduce the subjective history of a patient concern. It should NOT
be considered the final diagnosis at this point since the highest level of understanding of the problem has
not been determined at this time. In order to standardize the entries in the EHR, the subjective
symptomatology should be entered by region of the body for musculoskeletal complaints. It is suggested
that the regional joint dysfunction codes should be used to enter the subjective description or history of a
problem for musculoskeletal complaints (M99.01 through M99.08). For visceral complaints, is suggested
that the general “unspecified” codes be used to start the note (i.e. the “R” ICD-10 codes). Once the
differential diagnosis or highest level of understanding of the patient’s problem is determined, it will be
entered into the problem list before the note is closed. When entering the problem in the problem list,
use one of the macros in the comment box to direct the reader’s attention to the regional area where the
subjective description is already entered and no further details are necessary. Non-musculoskeletal codes
such as hypertension (I10)and type 2 diabetes (E11) should be in the problem list, but not in the SOAP
notes as a treated condition.
CAUTION: Once an ICD-10 code has been entered in the problem list it can only be deactivated, it cannot
be deleted.

prior care), but also for other problems revealed during the evaluation (e.g. headaches indicated
on the systems review, an unreported surgical scar discovered upon examination).
For chief complaint history, review of systems, family history, medical history, and social history,
items should be relevant, obtained to sufficient degree to differentially diagnose, and recorded
in sufficient detail to inform future care and allow third parties to render judgment on standards
of care. Remember that SmartCloud has a separate system of entry for many of the past
medical history and family history items. This includes the Meaningful Use (MU) requirements,
including:
Allergies
Family history
Medications
Smoking history/tobacco use
Vital signs (although not technically history, the vital signs are entered here)
These items should be entered/updated and included in the SOAP note during an examination
visit. In addition, there may be problems that are complicated by or associated with these items
and need to be recorded in the problem list as such, i.e. hypertension, diabetes, etc.
It is also appropriate to report that “the patient reports no changes in family, past medical, or
social history” where these histories have been previously recorded. This statement should be
in subjective freeform section of the subjective speed note in the EHR (Paper notes will require
separate documentation). Remember that Meaningful Use (MU) reporting may require an
update in the patient record (Histories Section of the EHR).
SmartCloud Location: History Speed Note
SmartCloud has the commonly asked questions on the History Speed Note page as easy entry buttons. It
should be emphasized that these may not be able to portray the complete picture. There are both
complaint and subjective freeform tabs. It is necessary to enter information that completes the history of a
problem (in the complaint freeform tab) or general information that does not link to one of the problems
being evaluated (in the subjective freeform tab).
If the patient presents with more than one problem, then each problem needs a complete history unless
there is a reference to a regional or visceral code (see starting a note in “Problem List” above).
Whenever appropriate, a body diagram should be entered in the note with problem areas marked and
labelled.

This item is deficient if patient care documentation lack an appropriate, structured, and sufficiently comprehensive chief complaint, medical, social, and family history, and a review of relevant systems, all correctly documented. See sample history Return to the top.
4) Clinical Examination Clinical examination is necessary for all patients presenting to the clinic whether wellcare, health
clearance or symptomatic. The clinician in consultation with the chiropractic student will need
to decide the appropriate level of evaluation necessary to arrive at a working diagnosis. Further,
this examination should also be used as a risk management tool (similar to a pre-surgical
screening) so that any procedures we select in our treatment plan are safely delivered/modified
for the individual patient.
The examination must include minimal core components. Additional case specific components
that will relate to significant findings are warranted on a case-by-case basis. The case specific
examination will focus on the unique patient condition being examined that might not be
evaluated by the minimum core components. The clinician may direct the student to perform or
not perform specific exam procedures due to special circumstances unique to the patient both
for the core or case specific examinations.
Return to the top.
Minimal core components of the examination (must be performed on all new patient examinations and usually performed on established patient examinations):
Postural evaluation Spinal joint and soft tissue assessment
Spinal range of motion Spinal screening orthopedic assessment
Vital Signs – includes: o Ht., Wt., bilateral B/P, pulse, respiration and
temperature
Neurological assessment o Screening of motor, sensory and reflex
functions related to cervical/lumbar spine and upper/lower extremities
o Pathological reflex
The examination The clinician along with the chiropractic student must: a) Perform, interpret, and document appropriate clinical examination procedures. b) Order and use specific diagnostic tests when appropriate based on information obtained in the case history and other clinical examination procedures (see diagnostic imaging to review). c) Record a working diagnosis based on the highest current level of knowledge and understanding of the patient’s case.

Examples of inappropriate or unacceptable work that would indicate a deficiency:
1) Is not complete (missing key components necessary for diagnostic conclusion i.e.
orthopedic and/or neurological tests not present for a radiculopathy diagnosis)
2) Lacks essential core examination components for a clinical evaluation of a new or existing
patient – missing one or more of the following:
a) vital signs (includes height, weight, B/P, pulse, respirations and temperature) b) postural evaluation c) spinal ROM d) spinal joint and soft tissue assessment e) orthopedic assessment of the region (spinal screening) f) neurological assessment of the region (MRS) and other necessary assessment(s)
3) Lacks essential case-specific examination components – depending on the case, certain
exam procedures would be expected in order to determine the appropriate course for the
patient. Example: Low back complaint does not include evaluation of the abdomen including
auscultation of the abdominal aorta; or thyroid exam in a CTS case or weight issue.
4) Examination results are incompletely documented.
5) Missing/not documented
This item is deficient if essential core or case specific items are missing, or if the documentation of the examination is not clear or absent. See sample Clinical Examination Return to the top.
Case specific examination (determined by the history and area of the condition i.e. shoulder): o May require orthopedic and neurological exam of a peripheral joint/segment of the body.
o Detailed segmental peripheral neurological examination and peripheral vascular examination to
investigate complaints of tingling, numbness or weakness in an extremity.
o Cardiovascular, cardiopulmonary, lymphatic, and/or abdominal examination may be required.
o Specific physical examination procedures should be performed and evaluated when related to
the area of chief complaint.
o Record the results even when negative.
SmartCloud Location: The examination information should be documented in the EHR:
1. Objective Speed Note page 2. Examination page 3. Physical examination page
Paper notes must contain the same elements.

5) Diagnostic testing and diagnostic imaging During each course of care, it must be determined whether or not a patient needs special
testing procedures. Additionally, if a patient has already had testing completed, results should
be requested and reviewed. These reports should be signed by the clinician and scanned into
the patient record. This information may be utilized as part of the diagnosis and management
plan. A summary statement should be documented indicating that the test results were
reviewed.
There are 4 possible outcomes:
1) imaging, lab work, or other special tests WERE critically required in management of
the case and WERE ordered
2) imaging, lab work, or other special tests WERE critically required in management of
the case, but WERE NOT ordered
3) imaging, lab work, or other special tests WERE NOT critically required in management
of the case and WERE NOT ordered
4) imaging, lab work, or other special tests WERE NOT critically required in management
of the case, but WERE ordered
This item is deficient if outcomes 2 or 4 above are indicated in the chart. Outcome 2
represents gross under-management (including ordering the wrong test with information
available at the time), and outcome 4 represents gross over-management. This item is also
deficient if documentation of the review of testing is not noted, management modification if
critically needed is not documented, or the results shared with the patient was not
documented.
Return to the top.
6) Diagnosis The diagnosis should be listed at the highest level of understanding. It should be supported by
the patient’s history and examination findings. The diagnosis should be clearly evident in the
patient file in at least 4 places and on the Patient Encounter Form. The diagnosis/es should be:
SmartCloud Location:
A summary of the results of the diagnostic testing (including the place, date and if appropriate, the reason
for testing) should be listed in the General Assessment section of the Assessment Speed Note. The actual
report should be scanned into the EHR and the summary should be present in the student draft note.

1) Written in plain and medically accurate language (not codes or abbreviations) on the
informed consent form for the patient. See informed consent.
2) Written in the header of the Patient Care Plan both the case type and ICD-10
diagnosis code numbers. See Case Types in appendix. The diagnosis codes should be
listed in the order used in the Plan Speed Note section of the SOAP note. Codes used for
billing should be consistent with the patient encounter form (routing sheet). [Note: In
order to be aware of possible complicating factors, the footer of the patient care plan
should also include all critical review of systems, comorbidities, or other relevant past
medical history findings as well as relevant family history.]
If the diagnosis lacks important elements related to the chief complaint, review of
systems, comorbidities, or other relevant findings, or if the diagnosis is inconsistent
with significant findings, is not a sufficient level of understanding (“radiculopathy, site
unspecified” or “headache” instead of “cervicogenic headache” when these are
indisputably clear), is not current (resolved diagnoses are still listed, or diagnoses that
have been refined in the SOAP notes have not been refined in the care plan), or is
missing, documentation in the chart is deficient.
NOTE: The case type should be listed as a type of ‘care plan’ to avoid student
confusion (a problem may have been present for more than 3 months, but is
being treated on an acute care basis, i.e. 3 visits per week for a period of time
with expectations of resolution in a relative short phase of care). The care plan
should be fairly consistent with the case type selected.
NOTE: A “wellness” case type (non-“medically necessary” elective and generally
non-third party reimbursable care) may have only subluxation diagnoses and
codes without secondary diagnoses and codes. No other case types should have
subluxation codes without secondary codes. There may be secondary codes for
wellness care, but it is not required for elective, wellness-orientated care. Non-
third party reimbursable problems need to be coded, for student management,
but not used in the billing. These problems should be evident in the adjustment
page of the SOAP note with the modalities used to address them (usually
student services and not the clinician’s).
3) Coded in the Plan Speed Note. The Plan Speed Note should have all of the diagnosis
codes entered that are in the header (these codes need to be within chiropractic scope
of practice). They should remain consistent from visit to visit until the problem is
resolved or there is a change, such as a diagnostic imaging revealing a finding or a new
problem arises.
4) Coded in the Problem List. The problem list will also contain any other non-
musculoskeletal conditions of note such as hypertension, diabetes, etc.

5) The Patient Encounter Form. The form also known as the “Routing Sheet” should
have the ICD-10 codes listed in the order for billing and consistent with the order in the
header of the Patient Care Plan and the Plan Speed Note.
Please refer to the case types document and case types decision tree for more detailed
information related to diagnosis.
Click here for example diagnosis in the Plan Speed Note Return to the top.
7) Informed consent Informed consent must be obtained for all diagnoses and procedures, but must particularly address “significant” risk procedures. The informed consent is obtain during the report of findings procedure. It requires documentation of any health risks and management options considering the patient’s health care needs and goals*. The diagnosis should be written out in plain language and highest level of understanding for the patient’s benefit. Including only diagnosis codes and/or abbreviations on the informed consent form does not meet NYCC guidelines. The SOAP note should indicate that informed consent was obtained on the same day it was received. The patient care plan should indicate that informed consent was obtained. The treatment and diagnosis should be consistent across the SOAP, the patient care plan, and the informed consent. The patient and clinician should sign the informed consent form. Any new diagnosis, added treatment modality, or significant risk would require obtaining a new informed consent. An informed consent must be obtained by a licensed provider. In order to train the student, the following procedure and SOAP note documentation is suggested: “the student discussed the report of findings and tenets of the informed consent with the patient while the clinician was present and the clinician confirmed that the patient understood.” The patient and clinician signature are still required on the informed consent form that is scanned into the EHR. *CCE 2013 Accreditation Standards – Meta competency Outcome 4.2 http://www.cce-usa.org/uploads/1/0/6/5/106500339/2018_cce_accreditation_standards.pdf
The Informed Consent process and definition as per the Association of Chiropractic Colleges:
a. Recognizing that all care including diagnostic studies and chiropractic care have some
potential for causing injury to a patient, it is the recommendation of the Association of
Chiropractic Colleges that, prior to performing diagnostic testing and prior to
implementing chiropractic procedures, the patient should be informed about the
SmartCloud location of diagnosis: 1. Problem list 2. Header of Patient Care Plan and in the ‘Problems’ line in the Care Plan 3. Plan Speed note 4. Informed Consent form 5. Patient encounter form (Routing sheet – not found in the EHR but same as Plan Speed Note)

material and inherent risks and common options to the recommended care and the
associated risks, including the risk of refusing care. If the patient wishes to continue
he/she should give his/her consent. The Doctor should have a record in his/her clinical
file documentation which confirms that consent was given by the patient to the
diagnostic testing and/or the chiropractic procedure.
b. “Informed consent" is more of a process than a documented procedure. The
Association of Chiropractic Colleges recommends that the Doctor engage in a thorough,
verbal discussion with the patient, thus enabling the Doctor to be in a position to verify
that he/she took the time to explain the material risks inherent in the recommended
procedures and that the patient consented. Beyond this, the Association of Chiropractic
Colleges recommends that the patient execute some document acknowledging that: (a)
he/she has been part of an informed consent process; (b) that the material risks have
been disclosed to the patient, including a description of those material risks; and (c) that
the patient, after assessment, has agreed ("consented") to the procedures
understanding any material risks which are inherent to that procedure.
c. Whereas it is beneficial for the Doctor to have notations in the clinical records
reflecting that the patient was advised of the material risks and consented to the
treatment, there is no substitute for the patient's written confirmation of those facts. It
is the Association of Chiropractic Colleges belief that the profession and the public
interest are better served by an occasional patient refusing to execute an informed
consent acknowledgment form as opposed to having licensed Doctors exposed to claims
of informed consent violations when, in fact, informed consent was secured but not
irrefutably documented and verified. It is the recommendation of the Association of
Chiropractic College's to document the patient's consent to both the diagnostic
procedures which the practitioner proposes to use, as well as to document the patient's
consent to the "patient care plan" which lists the patient's diagnosis and identifies the
particular procedures and/or modalities to be used.
Resource: ACC Policy - Informed Consent Guidelines
http://www.chirocolleges.org/resources/informed-consent-guideline/

Report of Findings (ROF) and Informed Consent (IC) process and documentation:
Indicators that initiate the need for an IC: Anytime there is a significant change in risk the IC should be obtained, signed, dated and noted on the date of the onset of care for a particular condition. As new complaints/diagnosis(es) arise requiring additional evaluation procedures or different care procedures additional informed consent(s) should be obtained from the patient and documented in the SOAP note(s).
Diagnoses or significant risk procedures in the SOAP or patient care plan that are not consented to in writing by the patient are a clear deficiency. -Return to the top.
SmartCloud Location: 1. The signed Informed Consent form is scanned into the EHR. (see sample IC form)
2. A statement is listed in the Assessment Speed Note, ‘General Assessment’ section indicating that
the patient understood and consented to the treatment plan, health risks, management options
considering the patient’s health care needs and goals (a macro is available for this statement).
3. In the Patient Care Plan, in the Informed Consent Obtained line, indicate “Yes” and list the date. Do
not delete prior dates if they exist.
The clinician or the student with clinician supervision is must discuss the following with the patient prior to rendering care. The report of findings will include: a) The clinical impression/working diagnosis(es) b) The management/treatment plan c) The risks and/or complications that may be apparent regarding the condition itself, or the treatment that may be given d) Any alternatives for the management of the diagnosed conditions e) The likely outcome of chiropractic care and management for the diagnosed conditions. After the patient is informed regarding the above items and related questions answered to his/her satisfaction, the clinician must obtain the patient’s consent to initiate treatment as evidenced by the patient’s and the clinician’s signatures on the IC form. The diagnosis needs to be written out completely. There should be no abbreviations or codes used. The record needs to include a properly executed document indicating that the informed consent has been obtained from the patient. The signed document is not sufficient. A statement in the SOAP note acknowledging that the patient has understood and agreed to the care plan is necessary. Remember that the diagnosis on the IC form must be consistent with the diagnosis listed in the SOAP note(s). The treatment being provided in the SOAP note(s) must be consistent with the treatment indicated on the IC form. These must both be consistent with the “Patient Care Plan.”

8) In-office treatment plan (Patient Care Plan) In the SmartCloud EHR, the In-office treatment plan is located in the Patient Care Plan page. The
Patient Care Plan should contain all the relevant information for the comprehensive
management of this patient including all treatment modalities and specifics of who delivers
these modalities. In addition, all recommendations and factors that are needed to properly
manage the case should be found in the Care Plan. This includes recommendations for lifestyle
changes, exercise, nutrition, wellness and tracking of co-morbidities such as diabetes, and
hypertension. Collaborative care and/or referrals should also be noted here. There should be
dated ongoing notations tracking these recommendation or referrals. Nutrition handouts, rehab
exercise handouts, patient education handouts and/or any correspondence or notes need to be
documented and tracked as part of the plan.
The plan: - Must not have treatment in areas of contraindications (such as manipulation of an
anticoagulated patient whose INR is outside of therapeutic range or joint manipulation
for patients with cancer),
- Must be related to the diagnosis (there should not be a plan for lumbar manipulation
for a patient with acute cervical torticollis),
- should provide expected benefit to the patient
- Must specify parameters (this must include specific location, parameters, settings,
duration, treatment frequency and who applies the modality – clinician or student).
- Must have a planned assessment of patient progress (distinct from the plan end date
– these might be the same date, but there should be a planned assessment of patient
progress noted.
- Would promote patient dependence rather than work towards patient self-efficacy,
(grossly excessive treatment frequency might be an example).
- Needs to include all of the procedures used during treatment in the SOAP note,
- Must include treatment that is appropriate for all chiropractic scope diagnoses and
consistent with the overall patient presentation as well as any treatment/modalities
used by the student for non-billable conditions/problems.
- Includes all management for non-billable or non-musculoskeletal conditions. These
plans may be for conditions that require tracking of collaborative care, referral or
specific outcome measures.
Note: NYCC uses the language “assessment of patient progress” while Smart Cloud indicates “Re-
examination” in the Patient Care Plan. The SmartCloud line labelled “Re-examination” should be the
location of the date of assessment of patient progress and what outcome measures are to be utilized.
Each patient’s case will be unique, but all problems should be addressed. Student draft versions of SOAP
notes should have evidence of complete Patient Care Plans with the above mentioned components
addressed. There must also be evidence of problem tracking and appropriate changes to the Care Plan as
the case progresses.

Click here for a sample patient care plan
Return to the top.
9) Self-care recommendations / Home Care recommendations Self-care recommendations are located in the “Patient Care Plan” listed as “Home Care
Recommendations.” The recommendations should be consistent with best practices to reach a
reasonable objective. There should be appropriate detail and/or parameters listed. There should
be a typed in description or a scanned-in chart copy of all recommended self-care.
SOAP notes should indicate that there was follow up with the patient relative to home care
performance. If this is missing, the deficiency should be noted in the progress notes file review
item.
Work, school or sports restrictions must be noted in the “Patient Care Plan.” A scanned-in copy
of any notes or correspondence in regard to these restrictions should be present in the patient’s
EHR. SOAP notes should indicate that there was follow up with the patient regarding any of
these restrictions possibly with an additional scanned-in note. Example: a ‘return to work note’
should be documented and scanned into the EHR.
This item is deficient if the recommendations are: contraindicated, likely to produce no
benefit (rather than maximally effective), lack needed detail and/or parameters, do not
encourage patient self-efficacy and autonomy, or are absent.
Click here for detailed self-care recommendation information
Return to the top.
SmartCloud Location:
Self-care/ home care recommendations should be located in the ‘Home Care recommendations’ line in the
Patient Care Plan page. These recommendation/orders should also be listed in the Plan Speed Note
freeform section on the day the recommendations/orders were given indicating the patient understood
and agreed with the plan.

10) Treatment goals Treatment goals are located in the “Patient Care Plan.” Goals should be listed and have
corresponding outcome measures. Generally, most conditions can be evaluated with a
subjective measure and a separate objective measure. If not possible to use the accepted and
valid outcome assessment tools (OATs), then SMART goals should be used, or a combination of
SMART goals and OATs. SMART is a mnemonic for Specific, Measurable, Achievable, Relevant
and Timed (https://www.tac.vic.gov.au/__data/assets/pdf_file/0010/27595/clinical-framework-
single.pdf ). In either case, it is necessary to be specific with goals and have an expected date of
achievement as well as what is expected in the short term as appropriate for the case if not
resolution of the problem. The long term goals (if appropriate for the case) should be the best
estimate prediction of the objective being reached in fairly specific time frame. The time frame
is determined by the case type being used (acute or chronic – see “Case Types” in the appendix).
This item is deficient if any element of the goals are not in SMART format, if the goals do not
include a functional component (if appropriate to the case), or are absent.
Two example goals are provided here in poor and in SMART format – other examples are in
detailed treatment goal information.
Poor goals: Reduce hypertonicity SMART goals: No trigger point in upper trapezius will
produce pain greater than 2/10 on palpation within 3
weeks. (Even better than this, goals will focus on
function –see the following)
Poor goals: Be more active SMART goals: Patient will perform 30-50 minutes of
moderate aerobic activity 3 days per week within 4
weeks
General tip: The following terms should not be considered sufficiently specific or measureable:
Amount of hypertonicity (unless a non-subjective measure of detection is included), number of
joint restrictions, ROM in degrees unless double inclinometers are used in the SOAP/clinical
SmartCloud Location:
Goals are located in the Patient Care Plan of SmartCloud. There are both short term and long term sections in the Care Plan. Reasonable goals as outline above need to be entered into these sections unless it is expected that there is only one goal, short term. It is necessary to link the outcome measures with each goal. The outcome measures are listed directly after the goals in the Care Plan. Goals should be adjusted as they are or not met. Student draft notes should show evidence of evaluation of patient goals as the case progresses. Note: Goals listed at the end of the Patient Care Plan are the patient’s goals noted on the intake form. These are not necessarily the short or long term goals listed above. They may be physical, health or activity related. They are listed and should be tracked as the case progresses over time.

exam, or items such as “reduce pain” unless quantified (such as “reduce pain per VAS from 3/10
to 1/10”), etc. A goal is more likely to be specific and measureable by reliable and valid means if
someone unfamiliar with the patient (and even someone clinically untrained) could verify the
status on the goal with the patient without any previous interaction with the patient.
Return to the top.
11) Outcome measurements Outcome measures are described in the Patient Care Plan – and evaluation of this item requires
assessing the plan, as well as care notes to determine if they were used. When outcome
measure scores are obtained, they should be noted in the SOAP note in the “General
Assessment” section of the Assessment Speed Note. There should be a comparison to previous
outcome assessment scores if previously done. In addition, the scores should be noted in the
Outcome Assessment line in the “Patient Care Plan” with the date acquired for easy reference in
future SOAP notes. When used longitudinally, the scores should be related to the achievement
of goals.
This item is deficient if outcome measures are: incorrectly scored or interpreted, not valid or
reliable, not correspondent to the goals (every goal should have a way to measure it), not
used as planned to assess progress, not appropriate to the diagnosis (a headache
questionnaire used for low back pain), not signed, and missing.
NOTE: A measure should only be marked “missing” if it was done and mentioned in the note,
but the score or outcome was not recorded. If the outcome measure simply wasn’t done at all
and should have been, mark that it was “not used longitudinally” for purposes of this review.
NOTE: You may be aware of a better outcome measure than the one that was used, or you may
have an outcome measure you prefer. If an outcome measure was used that does work for the
diagnosis and is reasonable, even if not ideal, do not mark it as deficient. See OAT details
Click here for detailed outcome measurement information
Return to the top.
SmartCloud Location: Outcome Measure Scores and/or SMART goal objectives must be documented:
1. On the date obtained, in the “General Assessment” section of the Assessment Speed note (with comparison to past scores if a longitudinal assessment).
2. In the Outcome Measures line of the Patient Care Plan with the date the scores were obtained for easy reference in future SOAP notes.

12) Progress notes Daily progress notes or SOAP notes track the patient’s progress during the course of care. They
tend to be brief compared with examination visits or formal assessment of patient progress
visits. There are some minimal requirements that will change depending on the patient’s
condition:
- Essential subjective information: How the patient is doing today, how the patient responded
to the prior treatment, if the patient is doing homecare, if there is anything new. Key case
specific information should be present if needed. For example: Are neurologic symptoms
progressing? Did a needed follow-up with an outside provider occur as recommended? Etc.
- Essential objective information: Any treated area should be appropriately examined prior to
treatment (this may simply be observation, palpation, and/or range of motion in simple cases),
and findings during and after care should be reported as appropriate. For Medicare and other
documentation as needed, two elements of PART must be recorded, one of which is A or R (see
below).
- Essential assessment information: Diagnoses for the visit must be recorded in plan speed
note. Response to care must be recorded here or in the Plan Speed Note Freeform section. Case
specific assessment information should be present if critical. It is helpful, but not required for
this file review, that each note indicates the patient’s response to that day’s treatment while still
in the office.
- Essential treatment information: All treatment and clinical reasoning for the visit should be
recorded. For example, if a certain treatment was not rendered per plan, the rationale should be
noted. If care is changed, rationale should be noted. If the treatment indicates “hot pack” and
does not state “per plan” (with the patient care plan elsewhere detailed enough to follow easily)
or does not state location, duration, and setting information in that section of the SOAP, it is
deficient. The same is true for “CMT-D” – it should indicate per noted restrictions, or list
restrictions – and soft tissue manipulation should include indication of muscles, regions,
techniques, or other details that will render the day’s treatment reproducible and
understandable. Referrals, new homecare provided, recommendations, suggestions, and all
clinical reasoning should be captured.
Additional information is available from the NCQA website - GUIDELINES FOR MEDICAL RECORD DOCUMENTATION: http://www.ncqa.org/Portals/0/PolicyUpdates/Supplemental/Guidelines_Medical_Record_Revi
ew.pdf
Progress notes are located in the patient’s record in the EHR and usually labelled SOAP notes. Each note during the review period needs to be assessed by reviewers. Minimal documentation requirements is governed by the PART mnemonic:
P – Pain or problem
A – Alignment

R – Range of motion
T – Tissue texture/tension At least two of the above components must be present in the SOAP and one of them must be the “A” or the “R.” The progress or “follow-up” SOAP notes should track the patient’s progress during a care plan. It is expected that brief description of the patient’s current problem(s) be documented along with significant examination findings (as noted in PART).
This item is deficient if the progress notes do not capture essential subjective, objective,
assessment, or treatment information, or if the notes are not signed or are absent.
See sample Plan Speed Note
Return to the top.
13) Patient response to care per formal assessment of patient
progress This is determined and documented in an “Assessment of Patient Progress” visit, which should
occur consistent with the Patient Care Plan and case type.
The following guidelines constitute the Assessment of Patient Progress (APP) credit for all clinic
courses and evaluated in the APP CRW in ExamSoft. The APP is not a complete examination, but
a review of the patient’s progress at a predetermined date. The date of this assessment may be
changed if the patient presentation warrants. Components of the APP should include any
outcome measures previously used in the case both subjective and functional, i.e. pain diagram
with VAS, Oswestry or Back Bournemouth forms. ROM, orthopedic and neurological tests may
be included if relevant from the onset of the case. The student and clinician should decide what
measures are necessary to update the Patient Care Plan. The APP procedure requires enough
information to determine if the patient requires additional care, home recommendations,
referral or discharge. There needs to be evidence of decision making with regard to the care
plan and future treatment planning.
SmartCloud Location: Progress notes should include the PART notation in the Subjective and Objective Speed Notes of the EHR. The Assessment Speed note should contain pertinent or new information such as imaging or lab reports, or reports from outside healthcare providers. These may affect the prognosis and should be noted. There are additional “buttons” that are generally used during an “Assessment of Patient Progress” visit, example: “Benefits are lasting longer.” The Plan Speed Note must have the diagnosis listed exactly as in the Care Plan Header. The procedure codes should be consistent with the Patient Encounter Form (Routing sheet). Any procedure(s) performed by the student and not billable should be described in either the Adjustment page comments section or in the Plan Speed Note freeform (both contain macros for ease of documentation). The student should insert the Patient Care Plan in the progress note to ensure care is guided properly.

The following process may be helpful: 1. Indicate in the history how the patient is doing now compared to intake and document the
comparison.
2. Re-administer or re-obtain OATs that were listed in the Care Plan, compare to previous
scores and report conclusions. Document the comparison in the General Assessment section
of the SmartCloud as well as the Care Plan.
3. Indicate if goals were met, whether they should remain the same or be revised. This should
be documented in the Care Plan.
4. If a re-examination of the patient is necessary, did it reveal pertinent positives and/or
negatives (of prior ROM, ortho or neuro tests)? Compare the current to the findings at
intake and document the comparison.
5. A revision of the diagnosis may or may not be in order. The student in consultation with the
clinician will make the appropriate changes (if any) in the Care Plan, Plan Speed note for that
day and the Problem List (some APP visits, but not all will rise to the level of E & M coding:
Established Patient Evaluation depending on the case specific needs).
6. If there is to be a continuation of care, then the dates of future assessment and possible
change to the end of care date need to be included in the modified Care Plan. Indicate the
date of last assessment to the right of the start date. Do not change the original start date
unless there is a new condition.
This item is deficient if formal assessment of patient progress occurred, but needed
information cannot be ascertained from the documentation or was not gathered. This item is
also deficient if a formal assessment of progress should have occurred during one of the
recorded visits, but the lack of formal assessment of progress is not satisfactorily explained.
Click here for detailed patient response to care information
Return to the top.
SmartCloud Location: An Assessment of Patient Progress SOAP note should contain all of the elements of a Progress SOAP note with the addition of:
Review of any pertinent testing (ROM, orthopedic or neurological findings) if positive at onset
Documented evidence of longitudinal outcome measure scores (OATs) / SMART goal assessments and comparison with earlier scores / assessments.
Evidence of medical decision making in an updated Patient Care Plan including diagnosis and any changes, continued care with or without changes noted, discharge at MTB or referral.
14) Management plan modification This is documented in the patient’s SOAP notes and would be most likely seen on the
assessment of patient progress (APP) visit or thereafter. However, this could occur at any visit as
clinically warranted. The “Patient Care Plan” must be modified to be consistent with any change
that is expected to continue on in future visits. A dated notation of such change should be
entered in the Care Plan’s ‘Treatment Plan Modifications’ line, i.e. change of a modality such as
cold laser, electric stimulation or rehabilitation exercises.
This item is deficient if the plan is not modified when critically needed (patient harm or
violation of patient autonomy* would result). Examples would be a patient who recovers and
becomes symptom free who is not released from care or transitioned deliberately and with their
consent to wellness care; or a patient who is not responding and whose management is left
unchanged after a reasonable trial (up to 4 treatments for most uncomplicated scenarios, with
perhaps as few as 2 treatments in very clear cut scenarios, such as uncomplicated low back
pain).
* Patient autonomy is the right of a patient to make decisions about their medical care without
their health care provider trying to influence the decision. Patient autonomy does allow for
health care providers to educate the patient but does not allow the health care provider to
make the decision for the patient.
Click here for more management plan modification information
Return to the top.
15) Documentation supports billing This is assessed by comparing plan speed note codes with the documentation supplied from the
ledger.
This item is deficient if CPT codes in the billing and note do not match, the SOAP does not
support the level of CPT code billed, the ICD codes in the billing statements and the billing ICD
codes in the note do not match, or the number of billing records do not match the number of
notes (with the sole exception of non-visit chart entries).
Click here for detailed documentation/billing information
Click here for a sample Patient Encounter Form (Routing Sheet) Return to the top.
The necessary documentation items are noted above in the Assessment of Patient Progress box above.
The Treatment Plan Modifications line in the Care Plan must be dated with the specific changes (changes in procedures such as added treatment modalities or stopped modalities).

Appendix
Privacy practice – details The patient should have a properly executed acknowledgement section of the Patient Intake form from the first visit. This form should be scanned into the patient’s EHR in Smart Cloud or be present in a paper chart. Example of executed HIPAA Privacy
Return to the top.
Example of an executed Report of Findings (ROF) and Informed
Consent (IC) form: Example IC form follows:

NYCC Health Center INFORMED CONSENT FOR TREATMENT
Patient’s Name ____Maya B. Herts__________ Date_____7/31/16___________
Diagnosis Sciatica left side associated with lumbar degenerative disc and joint
dysfunction.
Cervicalgia with cervicothoracic joint dysfunction.
Treatment Modalities (circle all that apply)
Instrument Assisted Adjusting/Activator Chiropractic Adjustment/Manipulation
Cold Laser Therapy Cryotherapy/Ice Pack Electric Muscle Stimulation
Exercise/Stretching Hot Moist Pack (HMP) Ultrasound
Instrument Assisted Soft Tissue Massage (IASTM) Manual Soft Tissue Massage
Other: ______________________________________________________________
I have received information from my doctor about my condition and proposed chiropractic treatment program, including the anticipated benefits, the reasonably foreseeable risks and side effects of the treatment, and alternatives to the proposed treatment, including no treatment. I understand that, as in all health care, there are some risks to chiropractic treatment. The risks include but are not limited to bruising, soreness, worsening of symptoms, muscle strains, sprains, fractures, dislocations, disc injuries, and strokes. I do not expect the doctor to be able to anticipate and explain all risks and complications, and I wish to rely on the doctor to exercise judgment during the course of the procedure which the doctor feels at the time, based upon the facts then known to him or her, is in my best interest. I have had the opportunity to ask questions about my condition and the recommended care, and my doctor has answered all questions to my satisfaction. I understand that I may ask further questions at any time. Comments (optional):
Maya B. Herts 7/31/16
Patient/Guardian Signature Date
Doc Ed Ucator ____7/31/16
Doctor’s Signature Date

Example of SmartCloud Problem List:
Notice that I10 Hypertension is listed in the “Active Problem Records,” but is not listed in the “Problem Records in Current Note” section. The subjective description of the patient’s symptoms is listed in the in the M99.03 Segmental and somatic dysfunction of the lumbar region. The M54.42 Lumbago with sciatica, left side was added once the history and examination determined this to be the ‘highest level of understanding’ diagnosis. The “Onset Comments” to the right of the diagnosis codes directs the reader of the note to the segmental dysfunction where the subjective description was originally recorded. Return to the top

SmartCloud Assessment Speed Note example including IC statement:
The informed consent statement is present in a macro for ease of entry.
For additional help, the following is a list of common errors with informed consent (it is not
necessarily all of the possible errors):
× Form is missing from case
× Abbreviated, missing or incomplete diagnosis
× Diagnosis codes listed with no words (missing diagnosis)
× Diagnosis is inconsistent with diagnosis being treated in SOAP note(s)
× Treatment is not listed or incompletely listed
× Treatment modalities are inconsistent with the plan and/or SOAP note(s)
× Patient’s name and/or signature is missing
× Doctor’s signature is missing
× Date is missing or not consistent with the onset of care
Return to the top.

Patient history – details SmartCloud Subjective Speed Note example:
Notice in the example that there is additional information in the “Complaint Freeform” tab related to the condition that the pre-set “buttons” do not cover. Return to the top.

Clinical examination – Objective Speed Note example:
Clinical examination – Examinations page example:
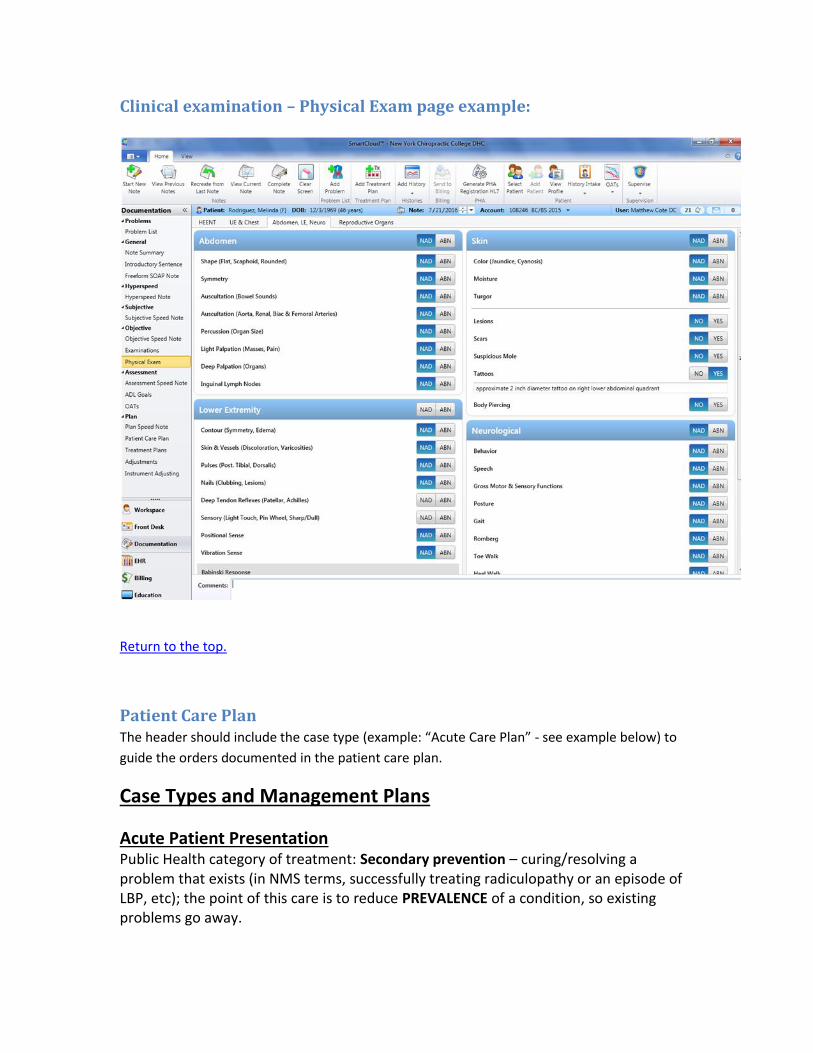
Clinical examination – Physical Exam page example:
Return to the top.
Patient Care Plan The header should include the case type (example: “Acute Care Plan” - see example below) to
guide the orders documented in the patient care plan.
Case Types and Management Plans
Acute Patient Presentation Public Health category of treatment: Secondary prevention – curing/resolving a problem that exists (in NMS terms, successfully treating radiculopathy or an episode of LBP, etc); the point of this care is to reduce PREVALENCE of a condition, so existing problems go away.

Acute Care Presentation Criteria: 1. New patient or Established Patient with new condition or similar condition with
moderate to severe symptoms 2. Initial onset <3 months (if greater than 3 months onset, but patient presents with
moderate to severe symptoms, then an acute treatment approach may be appropriate – see below).
3. Spinal condition is in scope of chiropractic care 4. No contraindications to chiropractic care found
Acute Care Plan must include:
Treatment type including who provides services (student or clinician).
Visit Frequency
Duration of care [Limiting factor: Therapeutic trial of up to 12 visits in 4 weeks]
Assessment date – if progress is documented through outcome measures, then further care may be warranted with expectations of resolution of the condition. If additional trials of care are indicated, supporting documentation should be available for review, including, but not necessarily limited to, documentation of complicating factors and/or comorbidities coupled with evidence of functional gains from earlier trial(s). Efforts toward self-care recommendations should be documented.
NYCC uses the term “Assessment of Patient Progress,” but SmartCloud uses “Re-examination.” Use this line in the Patient Care Plan to document the date of the assessment visit. This date should be consistent with the visit frequency and duration for the therapeutic trial or continued care.
Home/Work recommendations
Goals
Outcome Measures (OM) [Assess outcome measures < 1 month - with improving condition, OMs every 4 weeks thereafter and at discharge]
Chart documentation: - Initial visit history and exam essentials - Follow-up visit SOAP notes need to track the current condition and pertinent evaluation. During course of care: document condition change, dx test results, referrals, co-management, etc. Discharge expected at Maximum Therapeutic Benefit (MTB) within a 1 – 3 month period – document discharge and outcome measure scores.
Exacerbations/Recurrences (subset of acute care) 1 Document exacerbation
a) MTB reached and withdrawal from care documented b) Same or similar condition recurs within 30 days of discharge. Classified as Acute
Recurrence if similar condition is found after 30 days of discharge but needs to be treated in the acute-type care plan.
c) Moderate to severe symptom level d) Discharge at MTB expected as in Acute Care Plan
2 Exacerbation Care Plan (similar to Acute Care Plan with attention to active care and lifestyle modifications)

a) Trial of up to 12 visits in 4 weeks b) Active care recommendation and/or lifestyle modifications c) Consider dx tests, co-management or referral d) Monitor for MTB with Outcome Measures (OMs) e) May be heading for Chronic Care algorithm so discharge notation is necessary with
baseline outcome measures.
Chronic Care
Symptomatic aka Chronic Recurrent Care Public Health category of treatment: Transition from Secondary prevention (expect condition to resolve and a discharge of the patient) to Tertiary prevention (condition may not resolve but quality of life factors may be improved – see next section). 1 Defining characteristics of Recurrent symptom(s) for symptomatic chronic recurrent care
a) Mild symptom level b) Unplanned/unscheduled visit (more than 30 days since withdrawal of care) c) Often conditional discharge at same visit (consider diagnostic testing if progressive
changes noted over time) d) OM score may never reach zero, but should be monitored over time for significant
change that may indicate need for change in plan (may be headed for supportive care algorithm)
2 Document:
a) OM at each visit (pain diagram/functional questionnaire may be necessary) b) Recurrence of previous condition (date and dx) (review any diagnostic testing reports
that may be available) c) Unscheduled visit (walk-in, call-in, etc.) d) Review active care/home recommendations e) Conditional discharge notation with instructions for follow-up only when necessary f) Monitor OM scores over time for significant deterioration (may be indication for plan
change)
Supportive Care aka Ongoing Chronic Care:
Public Health category of treatment: Tertiary prevention – managing a condition that is not curable/resolvable, but working with quality of life issues, management of comorbidities, etc (in NMS terms, this would be care that helps someone with spastic paralysis regain 5 degrees of ROM so they can continue to live independently, but tx is required weekly – or working with the patient who has MS and care is palliative and quality of life, etc); the point of this care is to reduce the MORBIDITY associated with a condition, but not to resolve the condition.
1 Defining characteristics of supportive care case type a) At least 2 withdrawals from care for a problem (example: low back pain) b) MTB documented (outcome measures recorded for baseline measurement)

- Functional assessment tool preferred c) Active care/lifestyle modification attempted d) Assess/consider risk of long term care e) Risk/Benefit ratio must be in patient’s favor f) Long term plan in place with future attempts at withdrawal from care g) Monitor for deterioration of condition or other health concerns – request and/or review
any diagnostic testing reports available 2 Document:
a) 2 withdrawals from care (dates & OM baseline) b) Medical necessity (OM score(s) above baseline) – see medical necessity criteria c) Active care &/or lifestyle modification attempts d) Alternative care consideration e) Risk of long term care assessment (risk/benefit – red flags) f) Set goals with future attempt at withdrawal from care (at 6-10 months) g) Individualized plan w/ long term assessment – visits scheduled appropriately h) Monitor for deterioration of condition – document any complicating factors such as
diagnostic test results that complicate the patient’s condition, for example: a degenerative IVD
Suggested Plan Template: Ongoing Chronic/Supportive care plan In the SOAP note, episodes of care/dates must be documented. Other significant notations should be clear:
Active care/lifestyle modifications recommended in past plans
OM scores at time of discharge(s)
Current OM scores
Red Flags or lack of In the Patient Care Plan notate the following: Date of Assessment and/or the last assessment date New informed consent if necessary Plan of care:
Treatment type/frequency
Active care/lifestyle modifications
Goal(s)
Monitoring method (OMs)
Expected trial withdrawal from care date
Follow-up instructions
Wellness visit/ Elective care (sometimes referred to as “Maintenance” or Preventive care): Public Health category of treatment: Primary prevention – preventing a problem from occurring in the first place (in NMS terms, this would be ergonomics consulting to prevent the overuse syndrome, the carpal tunnel syndrome, the ITB syndrome in a

runner, etc); the point of this care is to reduce INCIDENCE of a condition, so they don’t happen. 1 Goals (one of the following)
a) recognize and reduce the incidence of a condition (prevent overuse syndrome, etc.) b) optimize levels of function (ADLs not limited, but individual wants performance
enhancement) c) maximize performance (athletic activity enhancement/improvement) d) Maintain joint flexibility (correction of subluxation)
2 Methods a) Manipulation b) Nutritional counseling c) Exercise guidance d) Lifestyle modification / patient education e) Monitor health conditions f) Assess any need for referral or co-management
3 Parameters and documentation (Plan Template): a) Document individualized goals a) Consider individual health indicators – use AHRQ ePSS
http://epss.ahrq.gov/PDA/widget.jsp * - be sure to include appropriate “A” level recommendations are acted upon in the plan and SOAP notes.
b) Consider Health Promotion and Wellness Checklist (use BMI calculator, etc.) c) Indicate treatment types/management measures, frequency, outcome measures (if
possible).
Note: Maintenance treatments are an elective form of care. Medicare and many 3rd party payers do not cover it as a “medically necessary” treatment. It is thought of as preventive treatment where further clinical improvement is not expected (if Est. Pt.) Maintenance treatments are not covered by:
- Medicare - Most insurance contracts
* The Electronic Preventive Services Selector (ePSS) is an application designed to provide primary care clinicians and health care teams timely decision support regarding appropriate screening, counseling, and preventive services for their patients. The ePSS is based on the current, evidence-based recommendations of the U.S. Preventive Services Task Force (USPSTF) and can be searched by specific patient characteristics, such as age, sex, and selected behavioral risk factors. Available both as a Web-based selector and as a downloadable PDA application, the ePSS brings information on clinical preventive services that clinicians need - recommendations, clinical considerations, and selected practice tools - to the point of care. Source: US Department of Health and Human Services – Agency for Healthcare Research and Quality (AHRQ)
Annual Check-up Evaluation 1 Yearly physical examination (at appropriate E/M service code†) 2 Assess/identify health risks
a) Focus on spinal health

b) Review/evaluate general health (SF-36 ) 3 Provide advice and education:
a) Promote health – use BMI calculator, nutritional advice, blood pressure check, etc. b) Prevent disease – use AHRQ ePSS http://epss.ahrq.gov/PDA/widget.jsp to
recommend/make referrals 4 Similar to wellness care (but may be covered service for some insurance) CPT codes for Annual Physical Exam
Established Patient: 99395 / 18-39 years old 99396 / 40-64 years old 99397 / 65 years and older New Patient 99385 / 18-39 years old 99386 / 40-64 years old 99387 / 65 years and older
References: National Public Health Partnership, The Language of Prevention. 2006, Melbourne: NPHP website: http://www.nphp.gov.au/publications/language_of_prevention.pdf Baker GA, Farabaugh RJ, Augat TJ, Hawk C, “Algorithms for the Chiropractic Management of Acute and Chronic Spine-Related Pain,“ Topics in Integrative Health Care, 2012, Vol. 3(4) ID: 3.4007 http://www.tihcij.com/pdf/Vol3i4/algorithms-for-the-chiropractic.pdf Globe G, Farabaugh RJ, Hawk C, et al, “Clinical Practice Guideline: Chiropractic Care for Low Back Pain,” JMPT Vol 39(1):1-22, 2016 http://www.jmptonline.org/article/S0161-4754%2815%2900184-0/fulltext NCQA – BPRP definition of acute and subacute care programs, 2007 http://www.ncqa.org/Portals/0/Programs/Recognition/RPtraining/BPRP%20Standards%20Slides.pdf U.S. Dept. HHS. National Guideline Clearinghouse, Best Practices & practice guidelines. Intervention and Practice considered: Spinal manipulation therapy (SMT) (frequency and duration), 2008 http://www.guidelines.gov/content.aspx?id=14231&search=chiropractic New York State Workers’ Compensation Board New York Mid and Low Back Injury Medical Treatment Guidelines http://www.wcb.ny.gov/content/main/hcpp/MedicalTreatmentGuidelines/MidandLowBackInjuryMTG2012.pdf

Ronald J. Farabaugh, DC, Mark D. Dehen, DC, Cheryl Hawk, DC, PhD. Management of Chronic Spine-Related Conditions: Consensus Recommendations of a Multidisciplinary Panel, J Manipulative Physiol Ther. 2010 Sep;33(7):484-92. Epub 2010 Aug 25. Guidelines for Chiropractic Quality Assurance and Practice Parameters (Mercy Guidelines) Dehen MD, Whalen WM, Farabaugh RJ, Hawk C. Consensus terminology for stages of care: acute, chronic, recurrent, and wellness. J Manipulative Physiol Ther. 2010 Jul-Aug;33(6):458-63. Dept. of Health and Human Services, CMS Misinformation on Chiropractic Services bulletin ICN 006953 October 2011 (updated on Aug. 28, 2012) http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/downloads/Chiropractors_fact_sheet.pdf US Department of Health and Human Services – Agency for Healthcare Research and Quality AHRQ ePSS http://epss.ahrq.gov/PDA/widget.jsp

Return to the top.
Does the patient seek care for functional limitation or pain?
Yes
No
Initiate the “Wellness Care”
rubric.
Does the patient seek care to actively
achieve optimum health possible?
Is this the first time for this problem
and is the initial onset <3 months?
Is this the first time for this problem
and is the initial onset >3 months?
No
Yes
Yes
Yes
Suggest appropriate care or referral
outside of the clinic. STOP.
Yes
No
See the “Acute Care” rubric.
Did the patient’s symptoms resolve?
Yes
No
Is the goal resolution of the
(underlying) condition?
Yes
No
Yes
Yes
Does the patient seek care to
actively achieve optimum health
possible?
Is care still appropriate?
No
Yes
Yes
Suggest appropriate care or referral
outside of the clinic. STOP.
Yes
Yes
Consider another trial (if
appropriate), withdrawal, or the
“Supportive Care” rubric.
Case Types Decision Tree – Based on Case Types – 1/21/2014
Yes
Not first TX for presentation. Were
symptoms quiescent for <30 days?
No
Yes
Yes
Is goal to manage symptoms of an
unresolvable underlying condition?
Follow the “Supportive Care” rubric
Yes
No
Yes
Yes
No
Yes
“Exacerbation”
“Recurrence”
Is the “acute care” rubric still
appropriate? (No contraindications,
<2 documented care withdrawals,
modifiable factors?)
Suggest appropriate care or referral
outside of the clinic. STOP.
Yes
See the “Acute
Care” rubric.
No
Yes
Yes
See the “Chronic
Care” rubric.
Is the visit expected to be for the
occasional flare up? (<1 visit/month)
No
Yes
Yes
Yes
Follow the “Symptomatic Care”
rubric
Is goal to manage symptoms of an
unresolvable underlying condition?
No
Yes
Yes
Yes

Example patient care plan in SmartCloud:

Note that the above plan contains all of the pertinent information about the diagnosis and management of the patient including problems within the scope of practice and conditions that need to be tracked or determined to fall into the realm of collaborative care. Return to the top.
Progress notes – SmartCloud Plan Speed Note Sample Plan Speed Note:
Notice that the diagnosis codes are listed in the order of billing and the procedure code is listed
for the billing. The response to treatment/follow-up recommendations are noted in the
‘Freeform’ section.
Return to the top.

Discharge documentation: Note that a patient discharge (or change in care type) would indicate that the day’s visit is
expected to be the last visit for that complaint. The student and clinician will indicate that the
condition is resolved after that visit. The Care Plan must then indicate that the condition is
resolved after the date of visit and no further care is warranted – or – the case type is changing
and a new plan is indicated (for example: acute to chronic).
The student at the direction of the clinician may decide to create a brief non-visit chart entry
with a Freeform SOAP note indicating resolution of the problem for reporting to outside
healthcare professionals. That short discharge summary non-visit chart entry note is the
documentation that the patient is released from care and may be necessary for some 3rd party
payers.
Return to the top.
In-office treatment plan – details NYCC does not use the “Treatment Plan” pages of SmartCloud due to the inconsistent
functionality of the page in the program. Use freeform entry spaces in the “Plan Speed Note”
and/or “Adjustment” section in SmartCloud for any specific treatment details associated with
that day’s visit.
Return to the top.
Self-care recommendations - details Self-care recommendations: Self-care is personal health maintenance. It is any activity an
individual can perform with the intention of improving or restoring health, or treating or
preventing disease.
http://en.wikipedia.org/wiki/Self_care
All details of the self-care should be appropriately stated in the Patient Care Plan. Self-care or
home recommendations may include exercise (location, duration, settings, frequency, reps, sets,
or other parameters), nutritional recommendations (dietary changes/advice), activity
restrictions (work or sports), or simply asking the patient to remain active. All details of the
active care exercise should be appropriately stated in the Patient Care Plan with the date
started.
http://medical-dictionary.thefreedictionary.com/Exercise
Return to the top.

Treatment goals – details Goals should be:
1) In SMART format, and ideally functional (Outcome Assessment Tools such as Oswestry or Bournemouth Questionnaires may work as measures of these goals) 2) Present for all diagnoses 3) Tailored for the specific patient SMART format:
Additional detail:
Specific and measureable goals:
The following terms should not be considered sufficiently specific or measureable: Amount of
hypertonicity (unless a non-subjective measure of detection is included), number of joint
restrictions, ROM in degrees unless double inclinometers are used in the SOAP/clinical exam, or
items such as “reduce pain” unless quantified (such as “reduce pain per VAS from 3/10 to
1/10”), etc. A goal is more likely to be specific and measureable by reliable and valid means if
someone unfamiliar with the patient (and even someone clinically untrained) could verify the
status on the goal with the patient without any previous interaction with the patient.
Achievable goals:

The goals should be able to be achieved by the patient given patient’s status and compliance. A
goal can provide a “stretch”, but should be achievable based on data provided about the patient
in the documentation.
Relevant goals:
The goals should reflect what the patient hopes to be able to accomplish – goals should
therefore reflect the patient’s involvement in goal setting.
Timed goals:
A realistic and appropriate time element should be included. Not providing a time element
would be an error. A time element that is clearly too short based on documentation would be
an error. A time element that is clearly too long (ie, the goal would have been reached well
before the provided time, based on documentation) would be an error. The Case Types
document may helpful in predicting an appropriate time frame.
Poor goals: Reduce hypertonicity SMART goals: No trigger point in upper trapezius will
produce pain greater than 2/10 on palpation within 3
weeks. (Even better than this, goals will focus on
function –see the following)
Poor goals: Reduce cervical ISD SMART goals: Patient will display full, painless, active
cervical range of motion within 4 weeks
Poor goals: Improve posture SMART goals: Patient will utilize sound ergonomics at
work (demonstrated in the office) and do hourly body
awareness checks while at work within 2 weeks.
Poor goals: Eat better SMART goals: Patient will increase vegetable intake to 3
servings/day within 2 weeks and 5 servings/day within 4
weeks
Poor goals: Be more active SMART goals: Patient will perform 30-50 minutes of
moderate aerobic activity 3 days per week within 4
weeks
Poor goals: Quit smoking SMART goals: Patient will move from pre-contemplative
stage to contemplative stage of quitting smoking based
on motivational interviewing within one month
Return to the top.

Outcome measurements - details Outcome Assessment Tools (OATs) should be accepted and validated. A resource for OATs is the
Chiro.org website: http://www.chiro.org/LINKS/Outcome_Assessment.shtml#Functional
Some accepted OATs:
Revised Oswestry Disability Index (ODI)
Neck Disability Index (NDI)
Back Bournemouth Questionnaire
Neck Bournemouth Questionnaire
Roland Morris Questionnaire
Rand SF-36
Headache Disability Index
Disabilities of the Arm, Shoulder and Hand (DASH)
Lower Extremity Functional Scale (LEFS) Other OATs exist and may be required by 3rd party payers, such as Back Index and Neck Index that resemble the ODI and NDI respectively. Additionally, there are Psychosocial Outcome Questionnaires such as:
Fear-Avoidance Beliefs Questionnaire (FABQ)
Keele STarT Back Screening Tool An example of a completed ODI follows
Return to the top.

Revised Oswestry Back Pain Disability Questionnaire
This questionnaire has been designed to give your chiropractor information as to how your low back pain
has affected your ability to manage in everyday life. Please answer every question by placing a mark in the
one box that best describes your condition today. We realize you may feel that two of the statements may
describe your condition, but please mark only the box that most closely describes your current
condition.
Name: Maya B. Herts Date: 7/31/16
PAIN INTENSITY [] I can tolerate the pain I have without having to use pain
medication. [] The pain is bad, but I can manage without having to take pain medication.
[] Pain medication provides me with complete relief from
pain. Pain medication provides me with moderate relief form
pain.
[] Pain medication provides me with little relief from pain. [] Pain medication has no effect on my pain.
PERSONAL CARE (e.g. Washing, Dressing) [] I can take care of myself normally without causing increased pain.
[] I can take care of myself normally, but it increases my
pain. It is painful to take care of myself, and I am slow and
careful.
[] I need help, but I am able to manage most of my personal care.
[] I need help everyday in most aspects of my care. [] I do not get dressed, wash with difficulty, and stay in bed.
LIFTING [] I can lift heavy weights without increased pain.
[] I can lift heavy weights, but it causes increased pain.
[] Pain prevents me from lifting heavy weights off the floor,
but I can manage if the weights are conveniently positioned (eg, on a table).
Pain prevents me from lifting heavy weights, but I can
manage light to medium weights if they are conveniently positioned.
[] I can lift only light weights
[] I cannot lift or carry anything at all
WALKING [] Pain does not prevent me from walking any distance. [] Pain prevents me from walking more than 1 mile.
[] Pain prevents me from walking more than ½ mile.
Pain prevents me from walking more than ¼ mile. [] I can only walk with crutches or a cane.
[] I am in bed most of the time and have to crawl to the toilet
SITTING [] I can sit in any chair as long as I like.
[] I can only sit in my favorite chair as long as I like. Pain prevents me from sitting for more than 1 hour.
[] Pain prevents me from sitting for more than ½ hour
[] Pain prevents me from sitting for more than 10 minutes [] Pain prevents me from sitting at all.
Other Comments:
STANDING [] I can stand as long as I want without increased pain.
[] I can stand as long as I want, but it increases my pain. Pain prevents me from standing more than 1 hour
[] Pain prevents me from standing more than ½ hour.
[] Pain prevents me from standing more than 10 minutes. [] Pain prevents me from standing at all.
SLEEPING [] The pain does not prevent me from sleeping well [] I can sleep well only by using pain medication
[] Even when I take pain medication, I sleep less than 6 hours
Even when I take pain medication, I sleep less than 4 hours
[] Even when I take pain medication, I sleep less than 2 hours
[] Pain prevents me from sleeping at all
SOCIAL LIFE [] My social life is normal and does not increase my pain. [] My social life is normal, but it increases my level of pain.
[] Pain prevents me from participating in more energetic
activities (e.g.) sports, dancing) Pain prevents me from going out very often
[] Pain has restricted my social life to my home
[] I have hardly any social life because of my pain
TRAVELING [] I can travel anywhere without increased pain. [] I can travel anywhere, but it increases my pain.
[] My pain restricts my travel over 2 hours.
[] My pain restricts my travel over 1 hour. My pain restricts my travel to short necessary journeys
under ½ hour
[] My pain prevents all travel except for visits to the physician/chiropractor or hospital
EMPLOYMENT/HOMEMAKING [] My normal homemaking/job activities do not cause pain. [] My normal homemaking/job activities increases my pain,
but I can still perform all that is required of me.
I can perform most of my homemaking/job duties, but pain prevents me from performing more physically stressful
activities (e.g., lifting, vacuuming).
[] Pain prevents me from doing anything but light duties. [] Pain prevents me from doing even light duties.
[] Pain prevents me from performing any job or homemaking chores.
Examiner: E. U.
Score: 27/50 x 100 = 54%

Management plan modification – details As the status of the patient changes it may become necessary to alter the Patient Care Plan. Any changes should have a documented reason for such change. Changes in the plan should be based on outcome assessment scores, diagnostic testing results, SMART goals, or the need for referral, changed therapies, therapy frequency and/or a transition to active care. Documentation of medical decision making should be located in the general assessment section of the Assessment Speed note. To track these changes, it is necessary to indicate the date and the change in the Treatment Plan Modifications line in the Patient Care Plan. These changes may be part of the formal Assessment of Patient Progress procedure or at any visit where appropriate. The plan modification changes and reasoning for such changes should be evident in the student draft as well as the final SOAP note signed by the clinician.
Return to the top.
Documentation supports billing – details
ICD and CPT codes entered on the Patient Encounter form (Routing Sheet) should be the same codes in the patient care plan, the plan speed note, and correspond to the diagnosis listed on the informed consent form. An example of a completed patient encounter form is provided here. Billing diagnoses should be consistent with the care plan diagnosis even if there are minor day-to-day changes. The diagnosis on the patient encounter form should not be changed unless a code is being resolved or added in which case, the clinical rationale should be evident in the general assessment of the SOAP note. If a new code is being added, an informed consent form likely needs to be added as well. An example of a completed Patient Encounter form follows:

Deficiencies include:
SOAP notes do not match the billing record
CPT codes in the billing record do not match the SOAP notes
ICD-10 codes in the billing record do not match the SOAP notes
Return to the top.
Top Related