







Languages
Pages
Legal

Department of medical physiology11th week
Semester: summer
Study program: Dental medicine
Lecture: RNDr. Soňa Grešová, PhD.

1. Pancreas Hormones
2. Pituitary Hormones and theircontrol by the hypothalamus

Pancreas
• Hormones:
– Insulin
– Glucagon
– Amylin
– Somatostatin
– Pancreatic polypeptide

Anatomy of the Pancreas
• is composed of two major types of tissues:
1) the acini (digestive juices)
2) the islets of Langerhans(insulin and glucagon)
• three major types of cells,
– alpha, (25%, glucagon)
– beta, (60%, insulin, amylin)
– delta cells (10%, somatostatin
– PP cells (pancreaticpolypeptide)
Copyright: Hall, J. E., & Guyton, A. C. (2006). Guyton and Hall textbook of medical physiology. Philadelphia, PA: Saunders Elsevier.

Cell-to-cell communication and direct control of secretion
• Insulin inhibits glucagon secretion,
• Amylin inhibits insulin secretion,
• Somatostatin inhibits the secretion of both insulin and glucagon

Insulin
• Insulin and its metabolic effects– insulin affects fat and protein metabolism almost as much as it
does carbohydrate metabolism
• Insulin is a hormone associated with energy abundance– excess amounts of carbohydrates = insulin is secreted in great
quantity– insulin plays an important role in storing the excess energy
(glycogen = liver, muscles)– excess carbohydrates that cannot be stored as glycogen are
converted under the stimulus of insulin into fats and stored in the adipose tissue
– insulin has a direct effect in conversion of amino acids intoprotein (inhibits the breakdown of the proteins that are already in the cells)

Insulin synthesis
• Insulin is synthesized in the beta cells• with translation of the insulin RNA by ribosomes attached
to the endoplasmic reticulum to form an insulin preprohormone
• is then cleaved in the endoplasmic reticulum to form a proinsulin
• this is further cleaved in the Golgi apparatus to form insulin and peptide fragments before being packaged in the secretory granules
• insulin is secreted into the blood in an unbound form (half-life -6 minutes, cleared from the circulation within 10 to 15minutes)
• is degraded by the enzyme insulinase mainly in the liver, to a lesser extent in the kidneys and muscles, and slightly in most other tissues
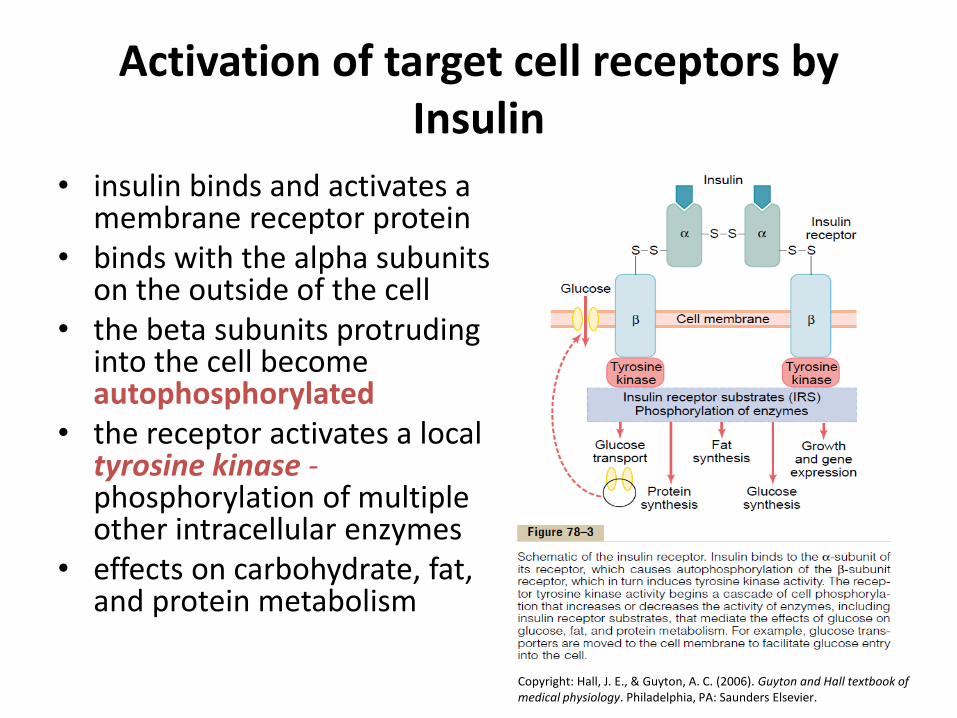
Activation of target cell receptors by Insulin
• insulin binds and activates a membrane receptor protein
• binds with the alpha subunits on the outside of the cell
• the beta subunits protruding into the cell becomeautophosphorylated
• the receptor activates a local tyrosine kinase -phosphorylation of multipleother intracellular enzymes
• effects on carbohydrate, fat, and protein metabolism
Copyright: Hall, J. E., & Guyton, A. C. (2006). Guyton and Hall textbook of medical physiology. Philadelphia, PA: Saunders Elsevier.
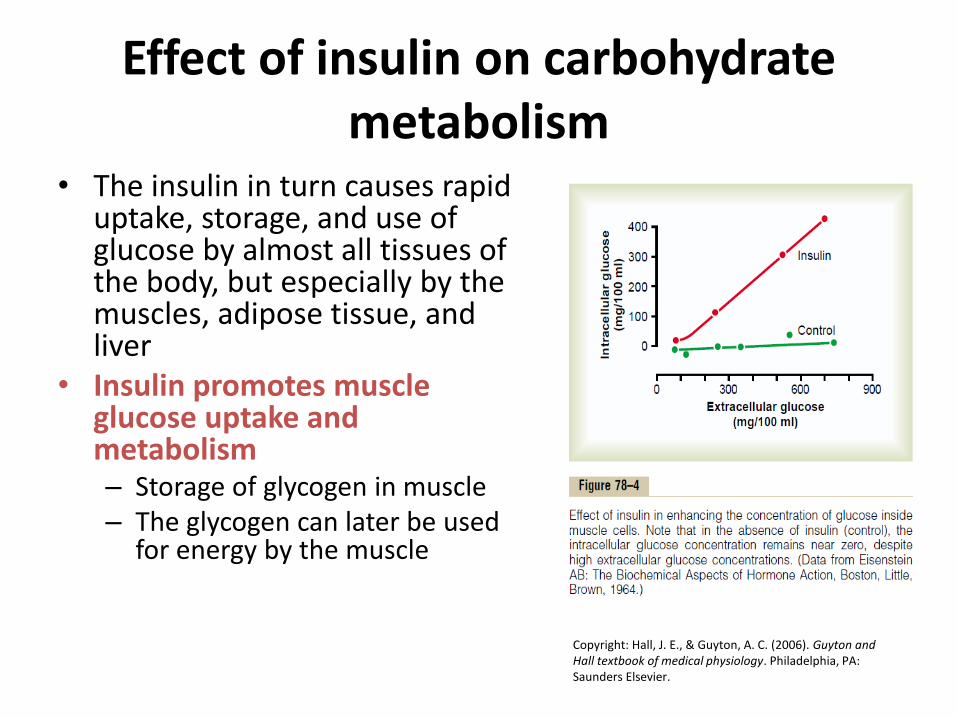
Effect of insulin on carbohydratemetabolism
• The insulin in turn causes rapid uptake, storage, and use of glucose by almost all tissues of the body, but especially by the muscles, adipose tissue, andliver
• Insulin promotes muscleglucose uptake and metabolism– Storage of glycogen in muscle– The glycogen can later be used
for energy by the muscle
Copyright: Hall, J. E., & Guyton, A. C. (2006). Guyton and Hall textbook of medical physiology. Philadelphia, PA: Saunders Elsevier.

Effect of insulin on carbohydratemetabolism
• Insulin promotes liver uptake, storage, and useof glucose– Insulin inactivates liver phosphorylase
– Insulin increasing the activity of the enzyme glucokinase
– Insulin also increases the activities of the enzymesespecially glycogen synthase
The net effect of all these actions is to increase theamount of glycogen in the liver
– Glucose is released from the liver between meals• The decreasing blood glucose causes the pancreas to
decrease its insulin secretion
• then reverses all the effects for glycogen storage

Effect of insulin on carbohydratemetabolism
• Insulin promotes conversion of excess glucoseinto fatty acids and inhibits gluconeogenesis in the liver
– Insulin promotes conversion of excess glucose intofatty acids = packaged as VLDL - transported to theadipose tissue and deposited as FAT
– inhibits gluconeogenesis in the liver by decreasing thequantities and activities of the liver enzymes requiredfor gluconeogenesis

Effect of insulin on carbohydratemetabolism
• Lack of effect of insulin on glucose uptakeand usage by the brain
– the brain cells are permeable to glucose and can use glucose without the intermediation of insulin(retina, germinal epithelium of the gonads)
Effect of insulin on fat metabolism
• Insulin promotes fat synthesis and storage– Insulin increases the transport of glucose into the liver
cells (The glucose is first split to pyruvate in the glycolytic pathway, and the pyruvate subsequently is converted to acetyl coenzyme A (acetyl-CoA), the substrate from which fatty acids are synthesized
– Most of the fatty acids are then synthesized within the liver itself and used to form triglycerides
• Role of insulin in storage of fat in the adiposecells– Insulin inhibits the action of hormone-sensitive lipase– Insulin promotes glucose transport through the cell
membrane into the fat cells

Effect of insulin on fat metabolism
• Insulin deficiency increasesuse of fat for energy– Insulin deficiency causes
lipolysis of storage fat and release of free fatty acids
– Insulin deficiency increasesplasma cholesterol and phospholipidconcentrations
– Excess usage of fats duringinsulin lack causes ketosisand acidosis
Copyright: Hall, J. E., & Guyton, A. C. (2006). Guyton and Hall textbook of medical physiology. Philadelphia, PA: Saunders Elsevier.

Effect of Insulin on proteinmetabolism and on growth
• Insulin promotes protein synthesis and storage
– Insulin stimulates transport of many of the aminoacids into the cells (valine, leucine, isoleucine, tyrosine, phenylalanine)
– Insulin increases the translation of messenger RNA,
– insulin also increases the rate of transcription of selected DNA genetic sequences
– Insulin inhibits the catabolism of proteins
– In the liver, insulin depresses the rate ofgluconeogenesis

Mechanisms of insulin secretion by the pancreatic beta cells
• glucose transporters (GLUT- 2)• glucose is phosphorylated to
glucose-6-phosphate by glucokinase
• Oxidation to form adenosinetriphosphate (ATP)
• Inhibition the ATP-sensitivepotassium channels
• opening voltage-gated calciumchannels,
• fusion of the docked insulin-containing vesicles
• secretion of insulin into the extracellular fluid by exocytosis Copyright: Hall, J. E., & Guyton, A. C. (2006). Guyton and
Hall textbook of medical physiology. Philadelphia, PA: Saunders Elsevier.

Control of insulin secretion
• Increased blood glucose stimulates insulin secretion
• Feedback relation between blood glucoseconcentration and insulin secretion rate
Copyright: Hall, J. E., & Guyton, A. C. (2006). Guyton and Hall textbook of medical physiology. Philadelphia, PA: Saunders Elsevier.

Control of insulin secretion
• Other factors that stimulate insulin secretion– Amino acids (arginine, lysine)– Gastrointestinal hormones (gastrin, secretin,
cholecystokinin, incretins)
• Other hormones and the autonomic nervous system– glucagon, growth hormone, cortisol, and, to a lesser
extent, progesterone and estrogen– Parasympathetic – increase insulin secretion during
hypeglycemic conditions– Symphatetic – increase glucagon secretion and decrease
insulin secretion during hypoglycemia• Epinephrine is especially important in increasing plasma glucose
concentration, far greater increases fatty acids during periods of stress

Control of insulin secretion
• Glucose concentrations are believed to bedetected by specialized neurons of thehypothalamus and brain stem, as well as by glucose-sensing cells in peripheral locationssuch as the liver

Glucagon and its functions
• Glucagon, a hormone secreted by the alpha cells of the islets of Langerhans
• several functions that are diametricallyopposed to those of insulin– increases the blood glucose concentration
• glucagon is also called the hyperglycemichormone

Glucagon and its functions
• Effects on glucose metabolism1) breakdown of liver glycogen (glycogenolysis)– 1. Glucagon activates adenylyl cyclase in the hepatic cell membrane,– 2. the formation of cyclic adenosine monophosphate,– 3. activates protein kinase regulator protein,– 4. activates protein kinase,– 5. activates phosphorylase b kinase,– 6. converts phosphorylase b into phosphorylase a,– 7. promotes the degradation of glycogen into glucose-1-phosphate,– 8. which then is dephosphorylated; and the glucose is released from
the liver cells
2) increased gluconeogenesis in the liver– by activating multiple enzymes that are required for amino acid
transport and gluconeogenesis in the liver, (converting pyruvate to phosphoenolpyruvate)
Glucagon and its functions
• Other effects of glucagon– activates adipose cell lipase, making increased quantities
of fatty acids available to the energy systems of the body
– Inhibits the storage of triglycerides in the liver
• Very high concentrations of glucagon– 1) enhances the strength of the heart;
– 2) increases blood flow in some tissues, especially the kidneys;
– 3) enhances bile secretion;
– 4) inhibits gastric acid secretion
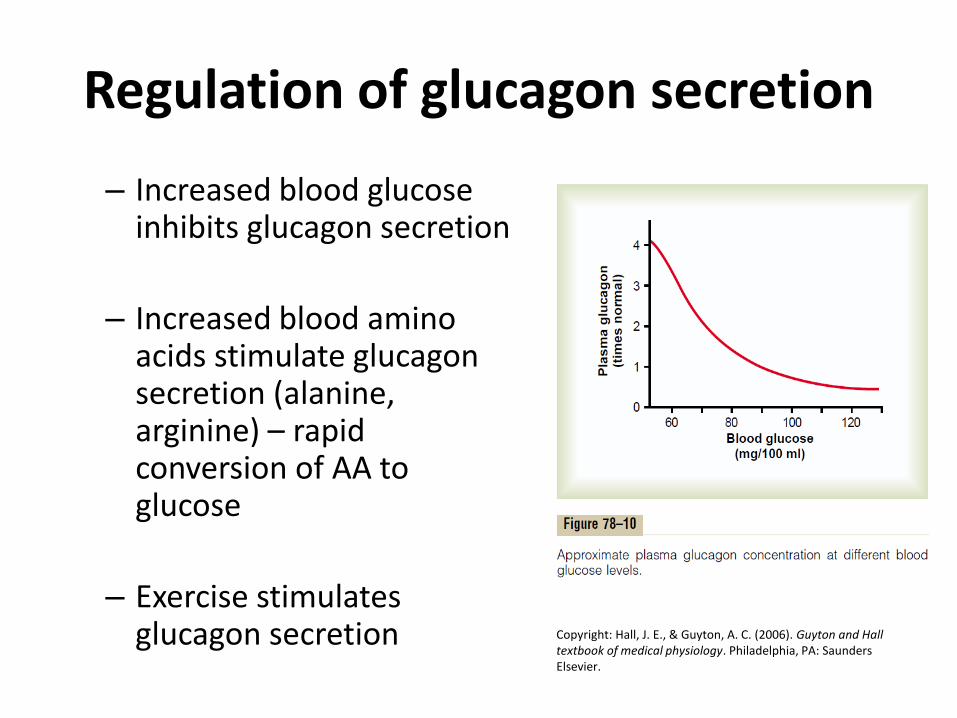
Regulation of glucagon secretion
– Increased blood glucoseinhibits glucagon secretion
– Increased blood aminoacids stimulate glucagonsecretion (alanine, arginine) – rapidconversion of AA to glucose
– Exercise stimulatesglucagon secretion Copyright: Hall, J. E., & Guyton, A. C. (2006). Guyton and Hall
textbook of medical physiology. Philadelphia, PA: Saunders Elsevier.

Regulation of glucagon secretion
• Somatostatin inhibits glucagon and insulin secretion– The delta cells of the islets of Langerhans secrete
the hormone somatostatin
• Somatostatin acts locally within the islets of Langerhansthemselves to depress the secretion of both insulin and glucagon
• Somatostatin decreases the motility of the stomach,duodenum, and gallbladder
• Somatostatin decreases both secretion and absorption in the gastrointestinal tract

Diabetes Mellitus
1. Type I diabetes, also called insulin-dependentdiabetes mellitus (IDDM), is caused by lack ofinsulin secretion
2. Type II diabetes, also called non–insulin-dependent diabetes mellitus (NIDDM), is caused by decreased sensitivity of target tissues to the metabolic effect of insulin. This reduced sensitivity to insulin is often called insulinresistance.
Pituitary Hormones and theircontrol by the hypothalamus

Pituitary gland (hypophysis)
• The anterior pituitarygland(adenohypophysis)– Six important peptide
hormones plus severalless important ones
• Posterior pituitarygland(neurohypophysis)– two important peptide
hormonesCopyright: Hall, J. E., & Guyton, A. C. (2006). Guyton and Hall textbook of medical physiology. Philadelphia, PA: Saunders Elsevier.

Pituitary gland (hypophysis)
• The hormones of the anterior pituitary play major roles in the control of metabolic functions throughout the body– Growth hormone – Adrenocorticotropin (corticotropin– Thyroid-stimulating hormone
(thyrotropin) – Prolactin – two separate gonadotropic
hormones, follicle-stimulating hormone and luteinizing hormone,
• The two hormones secreted by the posterior pituitary play other roles– Antidiuretic hormone (vasopressin– Oxytocin
Copyright: Hall, J. E., & Guyton, A. C. (2006). Guyton and Hall textbook of medical physiology. Philadelphia, PA: Saunders Elsevier.
Anterior pituitary gland
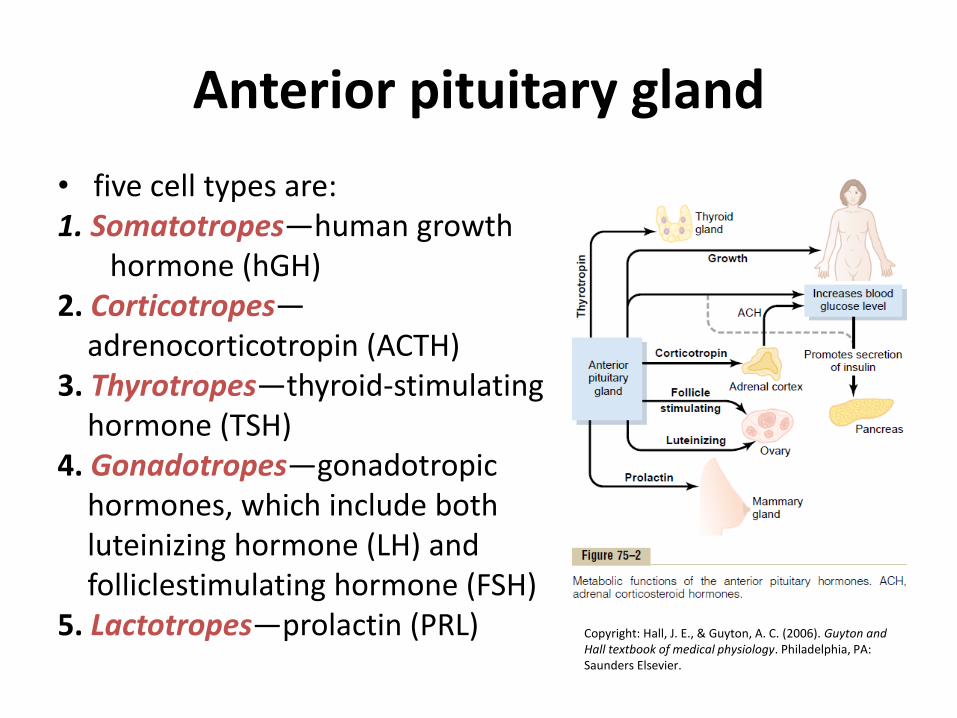
• five cell types are:1. Somatotropes—human growth
hormone (hGH)2. Corticotropes—
adrenocorticotropin (ACTH)3. Thyrotropes—thyroid-stimulating
hormone (TSH)4. Gonadotropes—gonadotropic
hormones, which include both luteinizing hormone (LH) and folliclestimulating hormone (FSH)
5. Lactotropes—prolactin (PRL) Copyright: Hall, J. E., & Guyton, A. C. (2006). Guyton and Hall textbook of medical physiology. Philadelphia, PA: Saunders Elsevier.

Posterior pituitary hormones
• The bodies of the cells are large neurons, called magnocellular neurons, located in the supraoptic and paraventricular nuclei of thehypothalamus
• The hormones are then transported in the axoplasm of the neurons’ to the posteriorpituitary gland

Hypothalamus controlspituitary secretion
• Secretion from the posterior pituitary is controlled by nerve signals that originate in the hypothalamus and terminate in the posterior pituitary
• Secretion by the anterior pituitary is controlled by hormones called hypothalamic releasing and hypothalamic inhibitoryhormones (or factors) bloodvessels = hypothalamic-hypophysial portal vessels
Copyright: Hall, J. E., & Guyton, A. C. (2006). Guyton and Hall textbook of medical physiology. Philadelphia, PA: Saunders Elsevier.

Hypothalamic-Hypophysial portalblood vessels of the anterior pituitary gland
• Hypothalamic releasingand inhibitory hormonesare secreted into themedian eminence and tuber cinereum, anextension of hypothalamic tissue intothe pituatory stalk– tissue fluid
– sinuses of the anteriorpituitary Copyright: Hall, J. E., & Guyton, A. C. (2006). Guyton and
Hall textbook of medical physiology. Philadelphia, PA: Saunders Elsevier.
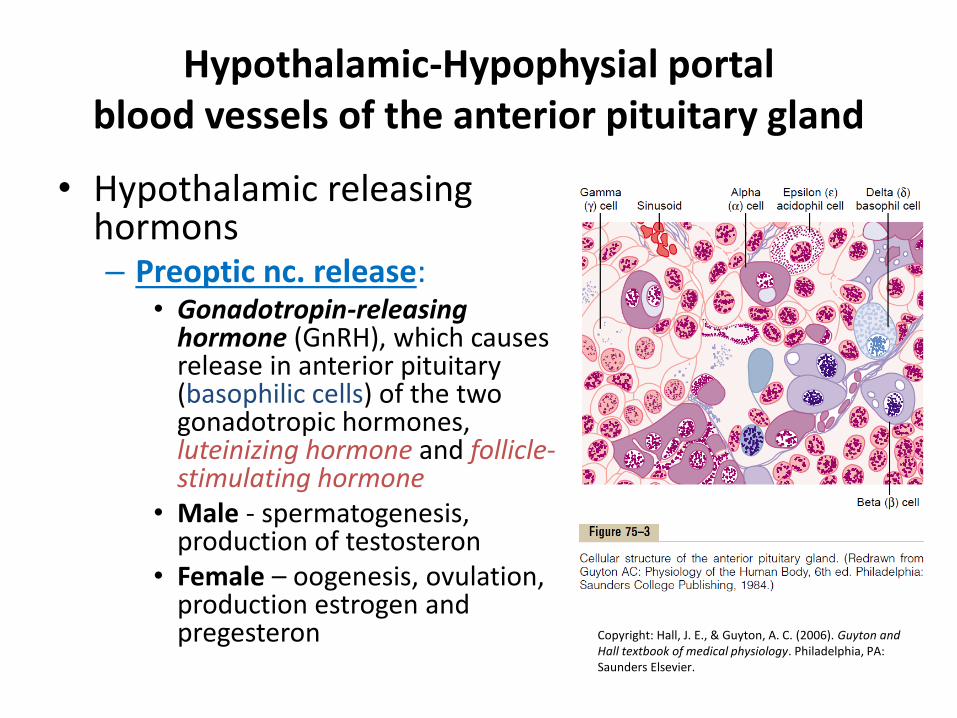
Hypothalamic-Hypophysial portalblood vessels of the anterior pituitary gland
• Hypothalamic releasinghormons– Preoptic nc. release:
• Gonadotropin-releasing hormone (GnRH), which causes release in anterior pituitary(basophilic cells) of the two gonadotropic hormones,luteinizing hormone and follicle-stimulating hormone
• Male - spermatogenesis, production of testosteron
• Female – oogenesis, ovulation, production estrogen and pregesteron Copyright: Hall, J. E., & Guyton, A. C. (2006). Guyton and
Hall textbook of medical physiology. Philadelphia, PA: Saunders Elsevier.

Hypothalamic-Hypophysial portalblood vessels of the anterior pituitary gland
• Hypothalamic releasing and inhibitory hormon– Ventromedial nc. release:
• Growth hormone–releasing hormone (GHRH), which causes release of growth hormone, and growth hormone inhibitory hormone (GHIH), called somatostatin, to the anteriorpituitary (acidophilic cells) which inhibits release of growthhormone
• Growth hormone acts directlyfrom blood and in liver is madesomatomedin Copyright: Hall, J. E., & Guyton, A. C. (2006). Guyton and Hall
textbook of medical physiology. Philadelphia, PA: Saunders Elsevier.

Hypothalamic-Hypophysial portalblood vessels of the anterior pituitary gland
• Hypothalamic releasinghormons– Paraventricular nc. release:
• Thyrotropin-releasing hormone (TRH), which causes release of thyroid-stimulating hormone (TSH) from anteriorpituitary (basophilic cells) T3, T4
• Corticotropin-releasing hormone (CRH), which causesrelease of adrenocorticotropin(ACTH) (basophilic cells) –glucocorticoids (adrenal cortex-zona fasciculata)
Copyright: Hall, J. E., & Guyton, A. C. (2006). Guyton and Hall textbook of medical physiology. Philadelphia, PA: Saunders Elsevier.
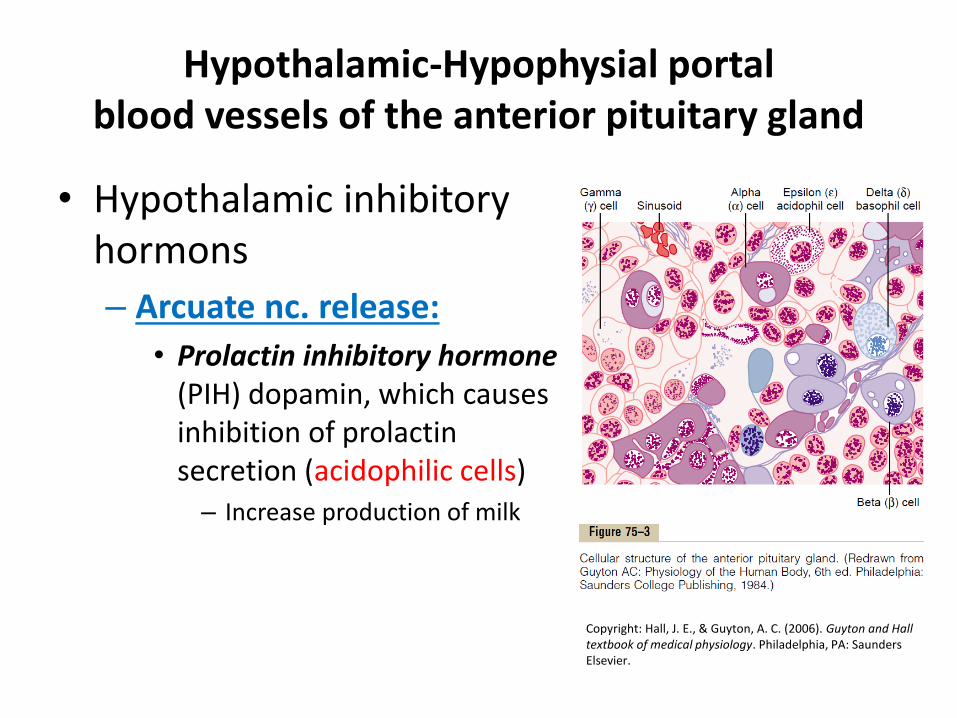
Hypothalamic-Hypophysial portalblood vessels of the anterior pituitary gland
• Hypothalamic inhibitoryhormons
– Arcuate nc. release:
• Prolactin inhibitory hormone (PIH) dopamin, which causesinhibition of prolactinsecretion (acidophilic cells)– Increase production of milk
Copyright: Hall, J. E., & Guyton, A. C. (2006). Guyton and Hall textbook of medical physiology. Philadelphia, PA: Saunders Elsevier.

Physiological functionsof growth hormone
• Growth hormone(somatotropic hormone or somatotropin) promotesgrowth of many body tissues– it promotes increased sizes of
the cells and increasedmitosis, with development of greater numbers of cells and specific differentiation of certain types of cells such as bone growth cells and early muscle cells
– Growth hormone enhances body protein, decreases fat stores, and conservescarbohydrates
Copyright: Hall, J. E., & Guyton, A. C. (2006). Guyton and Hall textbook of medical physiology. Philadelphia, PA: Saunders Elsevier.

Physiological functionsof growth hormone
• Growth hormone enhances almost all facets of amino acid uptake and protein synthesis by cells, while at the same time reducing the breakdown of proteins
• Metabolic effects: – Growth hormone promotes protein deposition in tissues
• Enhancement of amino acid transport through the cell membranes– increasing protein synthesis
• Enhancement of RNA translation to cause protein synthesis by theribosomes– even AA concentrations are not increased
• Increased nuclear transcription of DNA to form RNA– if sufficient energy, amino acids, vitamins, and other requisites for growth
are available
• Decreased catabolism of protein and amino acids– Mobilizes large quantities of free fatty acids from the adipose tissue
(energy)

Physiological functionsof growth hormone
• Metabolic effects:
– Growth hormone enhances fat utilization forenergy
• has a specific effect in causing the release of fatty acids from adipose tissue– increasing the concentration of fatty acids in the body fluids
• Enhances the conversion of fatty acids to acetyl coenzyme A (acetyl-CoA) – its subsequent utilization for energy
• Excessive mobilization of fat from the adipose tissue frequently causes ketosis and a fatty liver

Physiological functionsof growth hormone
• Metabolic effects: – Growth hormone decreases carbohydrate
utilization• 1) decreased glucose uptake in tissues such as skeletal
muscle and fat,
• 2) increased glucose production by the liver,
• 3) increased insulin secretion
• Necessity of insulin and carbohydrate for the growth-promoting action of growth hormone– adequate insulin activity and adequate availability of
carbohydrates are necessary for growth hormone to be effective
Physiological functionsof growth hormone
• Metabolic effects: – Growth hormone stimulates cartilage and bone
growth
• 1) Increased deposition of protein by the chondrocyticand osteogenic cells that cause bone growth,
• 2) Increased rate of reproduction of these cells,
• 3) a specific effect of converting chondrocytes into osteogenic cells, thus causing deposition of new bone

Physiological functionsof growth hormone
• Metabolic effects: – Growth hormone exerts
much of its effect throughintermediate substancescalled “somatomedins” (alsocalled “insulin-like growthfactors”)• Growth hormon in liver
releasing of somatomedins
• Short duration of action of growth hormone but prolonged action of somatomedin C (boundedwith plasma proteins)
Copyright: Hall, J. E., & Guyton, A. C. (2006). Guyton and Hall textbook of medical physiology. Philadelphia, PA: Saunders Elsevier.

Regulation of growthhormone secretion
• Growth hormone is secreted in a pulsatile pattern, increasing and decreasing
• person’s state of nutrition or stress - stimulate secretion
• 1) starvation, especially with severe protein deficiency;
• 2) hypoglycemia or low concentration of fatty acids in the blood;
• 3) exercise;• 4) excitement; • 5) trauma• 6) ghrelin
• Growth hormone increases during the first 2 hours of deep sleep
Copyright: Hall, J. E., & Guyton, A. C. (2006). Guyton and Hall textbook of medical physiology. Philadelphia, PA: Saunders Elsevier.

Regulation of growthhormone secretion
• Role of the hypothalamusin the control of growthhormone secretion– growth hormone–
releasing hormone,
– growth hormoneinhibitory hormone -somatostatin
– are transported to the anterior pituitary gland through the hypothalamic-hypophysial portal vessels
Copyright: Hall, J. E., & Guyton, A. C. (2006). Guyton and Hall textbook of medical physiology. Philadelphia, PA: Saunders Elsevier.

Abnormalities of growthhormone secretion
• Panhypopituitarism– This term means decreased secretion of all the anterior pituitary hormones (present from birth)
• Dwarfism– result from generalized deficiency of anterior pituitary secretion (panhypopituitarism) during childhood
• Panhypopituitarism in the Adult– The general effects:
• 1) hypothyroidism,
• 2) depressed production of glucocorticoids by the adrenal glands,
• 3) suppressed secretion of the gonadotropic hormones so that sexual functions are lost
• Gigantism– the acidophilic, growth hormone–producing cells of the anterior pituitary gland become excessively active, and
sometimes even acidophilic tumors occur in the gland
– the condition occurs before adolescence, before the epiphyses of the long bones have become fused with the shafts,height increases so that the person becomes a giant— up to 8 feet tall
– diabetes mellitus
• Acromegaly– an acidophilic tumor occurs after adolescence— that is, after the epiphyses of the long bones have fused with the
shafts—the person cannot grow taller, but the bones can become thicker and the soft tissues can continue to grow
– membranous bones, kyphosis
• Possible role of decreased Growth hormone secretion in causing changes associated with aging
• Therapy in older people : 1) increased protein deposition in the body, especially in the muscles; 2) decreased fat deposits; 3) a feeling of increased energy
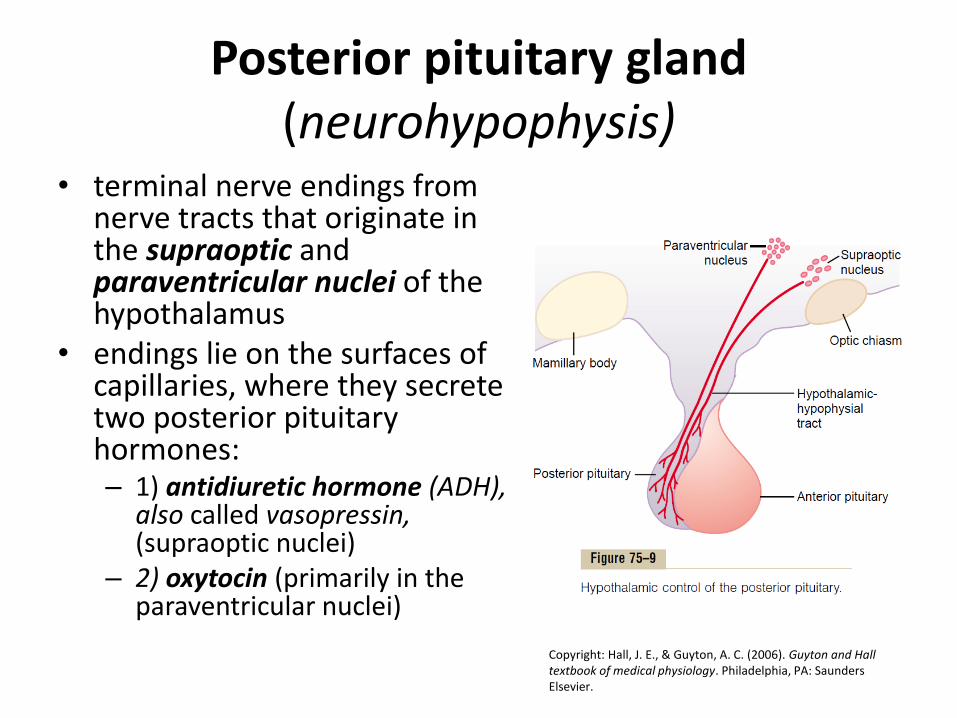
Posterior pituitary gland(neurohypophysis)
• terminal nerve endings from nerve tracts that originate in the supraoptic andparaventricular nuclei of the hypothalamus
• endings lie on the surfaces ofcapillaries, where they secrete two posterior pituitaryhormones:– 1) antidiuretic hormone (ADH),
also called vasopressin, (supraoptic nuclei)
– 2) oxytocin (primarily in theparaventricular nuclei)
Copyright: Hall, J. E., & Guyton, A. C. (2006). Guyton and Hall textbook of medical physiology. Philadelphia, PA: Saunders Elsevier.

Physiological functions of ADH
• ADH acts on the collecting ducts to increase their permeability (aquaporins)
• Regulation of ADH production
– Osmotic regulation
• Osmoreceptors : the extracellular fluid becomes too concentrated, fluid is pulled by osmosis out of the osmoreceptor cell, decreasing its size and initiatingappropriate nerve signals in the hypothalamus to causeadditional ADH secretion

Physiological functions of ADH
• Regulation of ADH production– Vasoconstrictor and pressor effects of ADH, and
increased ADH secretion caused by low bloodvolume• The stimuli for causing intense ADH secretion is
decreased blood volume– The atria have stretch receptors that are excited by overfilling
(inhibition of ADH secretion)
• Decreased stretch of the baroreceptors of the carotidaortic, and pulmonary regions (stimulation ADH secretion)

Oxytocin hormone
• Oxytocin causes contraction of the pregnant uterus– stimulates contraction of the pregnant uterus,
especially toward the end of gestation
• Oxytocin aids in milk ejection by the breasts– In lactation, oxytocin causes milk to be expressed
from the alveoli into the ducts of the breast
– Stimulus suckling stimulus on the nipple of the breast- release of oxytocin by the posterior pituitary gland -contraction of myoepithelial cells (milk letdown or milk ejection)
Top Related