







Languages
Pages
Legal


CUSP for VAP: Feedback on Early Mobility Measure and Implementation
Early Mobility Support Team
Armstrong Institute for Patient Safety and Quality
Department of Anesthesia and Critical Care Medicine
Johns Hopkins University

Armstrong Institute for Patient Safety and Quality
2
Outline
• Where are we now• Early Mobility Support Team• Early Mobility Implementation
– Importance of nurse-led mobilization– Readiness assessment– Mobilization and resources
• Early Mobility Toolkit • ICU Recovery Network• Next steps• Team feedback

Armstrong Institute for Patient Safety and Quality
3
Where are we now?
• Early mobility program implementation• Link to previous VAP Early Mobility calls:
https://armstrongresearch.hopkinsmedicine.org/vap/calls.aspx
• Early mobility data collection and data entry according to sampling strategy
• Feedback and implementation webinar• Introduction of Early Mobility Toolkit

Armstrong Institute for Patient Safety and Quality
4
Early Mobility Support Team
Christopher Wilson PT, DPT, GCS, CCCE
Coordinator of Clinical Education
Beaumont Hospital Troy Acute Care Rehab Services
Margaret Arnold, PT, CEES, CSPHP
Consultant with InspireOUtcomes, LLC
Anita Bemis-Dougherty, PT, DPT, MAS
Director, Department of Clinical Practice
American Physical Therapy Association
Jim Smith, PT, DPT, MA
President, Acute Care Section - APTA
Dale M. Needham, FCPA, MD, PhD
Associate Professor
Outcomes After Critical Illness & Surgery
Division of Pulmonary & Critical Care
Medical Director, Critical Care Physical Medicine & Rehabilitation Program
Johns Hopkins University
Pat Posa RN, BSN, MSA, FAAN
System Performance Improvement Leader, St. Joseph Mercy Hospital, Ann Arbor, MI
Archana Nelliot
Clinical Program Coordinator
Critical Care Physical Medicine and Rehabilitation Program
Johns Hopkins University School of Medicine

Armstrong Institute for Patient Safety and Quality
5
Early Mobility Implementation – Importance of Nurse-led Mobilization
• Chris Wilson PT, DPT, GCS– Coordinator of Clinical Education - Beaumont Health System, Troy, MI– Clinical Assistant Professor – Oakland University, Rochester, MI
• Goal for Early ICU Mobility– Nursing led– Physician driven– Therapist supported and guided
• Activity prescription or activity/ADL prescription

Armstrong Institute for Patient Safety and Quality
6
Early Mobility Implementation – Importance of Nurse-led Mobilization
• Supported by key workflow infrastructure – Keystone rounds, huddles, eliminating barriers
to PT/OT involvement in ICU• PT/OT Standing Order by Med Admin
– Follow through after T/F out of ICU

Safe Patient Handling
1. Staff Safety2. Patient Safety3. Best Care and Early Mobility
Communication
Right EquipmentRight time
Right patient
Just Culture
TRAM Lift Team:
Transfers, Rehab, and
Mobility
Training and Competency
Early and often
assessment
Immediate Huddles and rounds
Access and
ordering
Storage Delivery
Cleaning
Maintenance and upkeep
Integration with PT/OT
Handoff
Like RRT Urgent
calls
Trained and
managed by PT/OT
Metrics and productivity
24:7 coverag
e
Consultation
Activity prescription
Fine tune care
Risky behaviors?
Coaching
Policies and expectations
Nursing, EC,
Transport, Radiology
Continued Competency
Standardized
Dept champions

Armstrong Institute for Patient Safety and Quality
8
Nurse-led Mobilization
• Most ICU nurses know why Early Mobility in the ICU is critically important
• Need to do root cause analysis of barriers and address each through education, training, policies, equipment, communication
• Barriers found upon Beaumont survey:– Safety is a high concern– Risk of injury to patient and self– Accurately dosing mobility, choosing
equipment, and communicating

Can pt lift head off pillow?Raise arms/legs off bed?
Within 12 hrs of admit
Sit pt on Edge of Bed (dangle)
Stryker chair or bed inChair position.
Use mechanical lift for out of bed activity
Yes to both
No to either
Max assist (pt performsLess than 50% of work)
2 person assist
Mod assist (pt performs50% of work)
2 person assist
Min assist (pt performs75% of work)
Nurse to recommendPT evaluation – PT to
recommend equipment
Nursing to get helpto get patient up In chair with belt
Nurse to recommendPT evaluation – PT to
recommend equipment
Nursing tocontinue to dangle/Sit at edge of bed
with belt
Reassess DailyAnd Document Activity
Reassess DailyAnd Document Activity
Reassess DailyAnd Document Activity
Nursing to assist ptTo bedside chair
With belt
Can pt:Sit to stand x3?
March in place x3 each leg?Step forward/back
3x each leg?
Ambulate to bathroomWith belt
Yes
No
If pt not at baselineMobility, recommend
PT evaluation
If able to amb to bath-room safely, amb to
Halls 3x/day with belt
0
2 31
4
Reassess Daily and Document Activity
Nurse to recommendPT evaluation – PT to
recommend equipment
Not on Strict Bedrest
*Adapted with permission. Shay A. Outcomes of an Activity Progression Protocol for Pneumonia and COPD Patients. San Antonio, TX: Summer Institute on Evidence Based Practice; 2006.
Stepping into Safe MobilityNursing Assessment AlgorithmActivity order can be advanced per nursing policy #304


Armstrong Institute for Patient Safety and Quality
11
Nurse-led Mobilization
• Stepping into Safe Mobility– Decision making algorithm– Training tool– Communication tool
• Start from the Heart– 4-8 hour SPHM training
class for all new hire nurses and nursing assistants
– Co-taught by PT and nursing educators

Nurse-led Mobilization
• Pre and post survey indicate improvement in staff perception of:– Decreased risk of injury by 48%– Comfort with their own patient’s mobility by 25%– Improvement in confidence by 32% with mobility of
patients they are unfamiliar with • After implementation of SISM, staff felt:
– Safer, less at risk of injury– More confident to move a patient , determine equipment,
and medical appropriateness for OOB activity– Less reluctant to answer call lights when it is not their
patient

Armstrong Institute for Patient Safety and Quality
13
Readiness Assessment
• Are my patient’s cardiopulmonary and neurological systems functioning well enough to mobilize today?
• Cardiac– No increased pressors last 2 hours– Systolic BP >90<200mmHg– HR>50<140– MAP >65<110mmHg
• Pulmonary– PEEP <10cmH2O– FiO2 <0.6– SPO2 > 88% **
• Neurological– Responds to verbal stimuli

Armstrong Institute for Patient Safety and Quality
14
Readiness Assessment: Other considerations
• Patient factors– Sedation level – if patients are too heavily sedated, they will not be
able to participate in EM– Breathing support for EM intervention– Femoral Lines– ECMO (Extracorporeal Membrane Oxygenation)– Presence of lines, drains, catheters– Patient ability to follow directions
• Other factors– Do you know your ventilator settings and safety parameters– Do you have the right equipment (ambubag, portable ventilator)– Does Respiratory therapy need to be there?– Do you have enough help (Staff and/or equipment)?

Armstrong Institute for Patient Safety and Quality
15
Early Mobility Implementation – Mobilizing Your Patients
• All Early Mobility protocols have a basic flow of 4-5 stages that progress mobility
• Some variations exist in specifics• The goal is always to work towards functional mobility
(Walking and transfers) as soon as safely possible• All patient active movement can be considered
“Mobility” • Start with having the patient help with small things,
then progress to bigger movements and anti-gravity activities.

Armstrong Institute for Patient Safety and Quality
16
Mobilizing Your Patients: Making the most of all care tasks
• Understand ventilator settings and telemetry alarms so that you know when a patient is or is not tolerating an activity
• When repositioning or turning the patient, ask them to do as much of the work as they can
• Have them actively reach their top arm to the opposite side of the bed if possible, turn their head to the side if they can
• If they do well with bed mobility, try to sit them up• Even sitting with feet over edge of bed can be a major
accomplishment. Try to have them balance in sitting and reach with their arms, look up, sit up straight etc. If they are tolerating sitting well, try to stand up.
• When that is successful, try to shift a little weight or march In place
• When that is successful, take some steps

Armstrong Institute for Patient Safety and Quality
17
Mobilizing Your Patients: Safety Considerations
• Always ensure that the patient is tolerating activity by staying within pre-determined safety parameters
• Know what equipment is available to keep you and the patients safe while mobilizing
• Examples of equipment include – Friction reducing /air-assist devices for horizontal assistance– Overhead lifts with slings to lift patients into chairs or ambulate– Mobile floor lifts with slings to lift patients or ambulate patients– Powered and non-powered sit to stand assist devices to help
patients stand up– Specialty beds that assist with chair position, turning, and tilting
patients to full standing positions– Specialized walkers with seats if patient gets tired, and portable
ventilators
Armstrong Institute for Patient Safety and Quality
18
Early Mobility Toolkit
• Framed using the 4Es• Integrates available resources to help you educate
and engage all stakeholders• Proposes protocols to execute an Early Mobility
program: standardize the screening and mobilization of your patients
• Proposes tools to evaluate your progress• Prepared by the Early Mobility Support Team• Toolkit content will evolve based on your feedback
and experiences
Armstrong Institute for Patient Safety and Quality
19
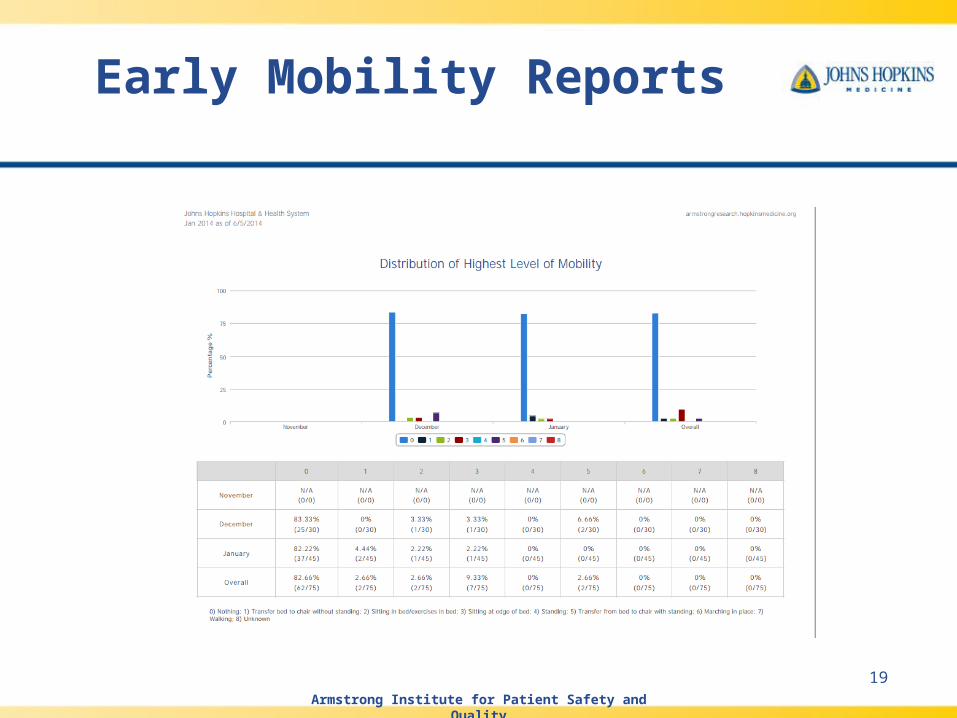
Early Mobility Reports

Armstrong Institute for Patient Safety and Quality
20
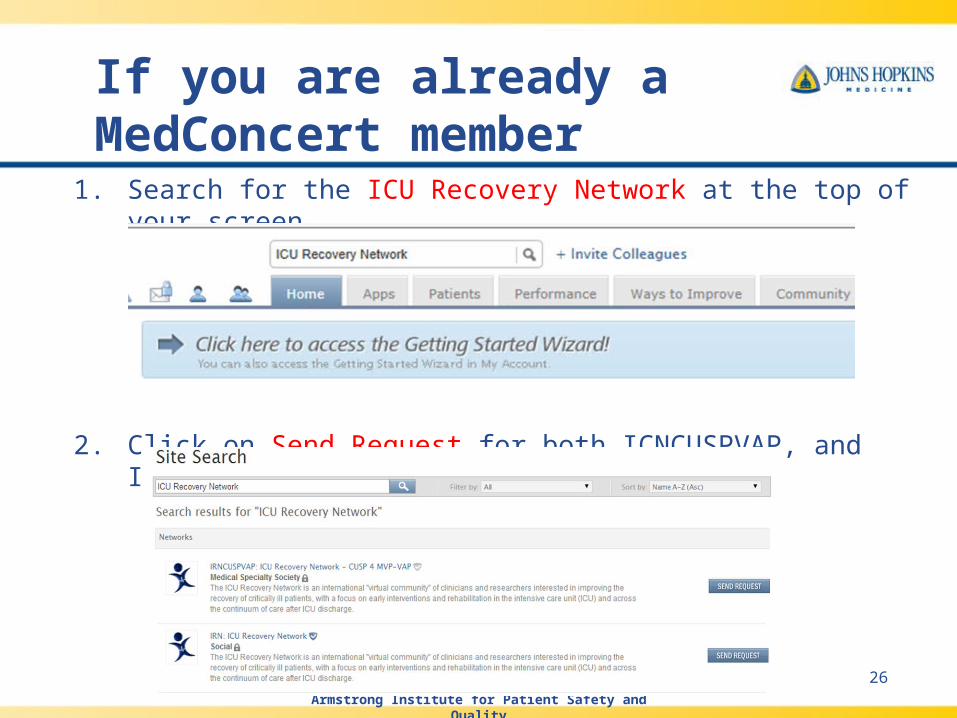
1. Search for the ICU Recovery Network at the top of your screen.
2. Click on Send Request for both ICNCUSPVAP, and IRN.
If you are already a MedConcert member

Armstrong Institute for Patient Safety and Quality
21
If you are already a MedConcert member continued…
3. Complete the request and click on Send.

If you are NOT MedConcert member
1. Request access to the IRN Network by contacting either the [email protected] or [email protected].
2. An administrator will reply to your email, and you will receive a user name and password to help set up your account.

Armstrong Institute for Patient Safety and Quality
23
Next Steps for Early Mobility
• Sign up for the “ICU Recovery Network” (IRN) pm MedConcert and explore resources
• Review the Early Mobility Toolkit and provide suggestions for revisions
• Get your Early Mobility program off the ground if you have not started already

Armstrong Institute for Patient Safety and Quality
24
Resources for Early Mobility
• Link to previous Early Mobility calls: https://armstrongresearch.hopkinsmedicine.org/vap/calls.aspx
• This includes calls from: – 08/30/2012 - Early Mobility and IP Call #2, Early Mobility in the
Critically Ill– 09/12/2013 - Early Mobility - Designing, Conducting & Sustaining
an ICU Rehab Program– 10/03/2013 - Draft - CUSP for VAP Early Mobility Data Collection
Instrument– 01/09/2014 - Early Mobility Data Collection Instrument

Armstrong Institute for Patient Safety and Quality
25
Next Steps for CUSP for VAP Project
• Continue or begin implementing the Data Collection Sampling Strategy between Process Measures and Early Mobility (from April)
• Structural Assessment 3 administered (July)
• Begin data collection for Low Tidal Volume Ventilation measure (August)
Armstrong Institute for Patient Safety and Quality
26
1. Search for the ICU Recovery Network at the top of your screen.
2. Click on Send Request for both ICNCUSPVAP, and IRN.
If you are already a MedConcert member

Armstrong Institute for Patient Safety and Quality
27
Data Collection Sampling Strategy: Began April 1st
27
2014 CUSP for VAP Data Collection Calendar
January
February
March
April
S M T W T F S
S M T W T F S
S M T W T F S
S M T W T F S
1 2 3 4
1
1
1 2 3 4 5
5 6 7 8 9 10 11
2 3 4 5 6 7 8
2 3 4 5 6 7 8
6 7 8 9 10 11 12
12 13 14 15 16 17 18
9 10 11 12 13 14 15
9 10 11 12 13 14 15
13 14 15 16 17 18 19
19 20 21 22 23 24 25
16 17 18 19 20 21 22
16 17 18 19 20 21 22
20 21 22 23 24 25 26
26 27 28 29 30 31
23 24 25 26 27 28
23 24 25 26 27 28 29
27 28 29 30
30 31
May
June
July
August
S M T W T F S
S M T W T F S
S M T W T F S
S M T W T F S
1 2 3
1 2 3 4 5 6 7
1 2 3 4 5
1 2
4 5 6 7 8 9 10
8 9 10 11 12 13 14
6 7 8 9 10 11 12
3 4 5 6 7 8 9
11 12 13 14 15 16 17
15 16 17 18 19 20 21
13 14 15 16 17 18 19
10 11 12 13 14 15 16
18 19 20 21 22 23 24
22 23 24 25 26 27 28
20 21 22 23 24 25 26
17 18 19 20 21 22 23
25 26 27 28 29 30 31
29 30
27 28 29 30 31
24 25 26 27 28 29 30
31
September
October
November
December
S M T W T F S
S M T W T F S
S M T W T F S
S M T W T F S
1 2 3 4 5 6
1 2 3 4
1
1 2 3 4 5 6
7 8 9 10 11 12 13
5 6 7 8 9 10 11
2 3 4 5 6 7 8
7 8 9 10 11 12 13
14 15 16 17 18 19 20
12 13 14 15 16 17 18
9 10 11 12 13 14 15
14 15 16 17 18 19 20
21 22 23 24 25 26 27
19 20 21 22 23 24 25
16 17 18 19 20 21 22
21 22 23 24 25 26 27
28 29 30
26 27 28 29 30 31
23 24 25 26 27 28 29
28 29 30 31
Key: Process Measure data collection Early Mobility data collection No data collection; use this time to catch up on missing Process Measure and Early Mobility data

Armstrong Institute for Patient Safety and Quality
28
Teams
• Tory Hospital - Pennsylvania• Karen Norton
• Holy Cross Hospital - Maryland
• Steve Risch, MSN, RN, CCRN, CCNS• Leola Saucier, BSN MBA CNML• Elly Sullivan, MA, OT

Armstrong Institute for Patient Safety and Quality
29
Questions
• Karol G. Wicker, MHS
Senior Director, Quality Policy & Advocacy
Maryland Hospital Association
• Mary Catanzaro RN BSMT CIC
Project Manager HAIs
Hospital and Healthsystem Association of Pennsylvania
Top Related