





Languages
Pages
Legal


Congenital and acquired Congenital and acquired Hemolytic anemiaHemolytic anemia


Classification of hemolytic anemia
1 Congenital hemolytic anemia (intracorpuscular defect)
2 Acquired hemolytic anemia(mostly extracorpuscular
defect)

CONGENITAL H.A.[ INTRACORPUSCULAR DEFECT ]
1 Hemoglobin defects
a. heme:cong.erythropoietic porphyria b.globin:
Quantitative:α and β Thalassemia quanlitative:hemoglobinopathy[HbE,CS]
2. membrane defect: Hereditary spherocytosis
Hereditary elliptocytosisHereditary stomatocytosis etc.

3. Enzyme defectsA. energy potential defects
EMH:anaerobic,ATP-producing pathwayHexokinase,Pyruvate kinase def.
B.Reduction potential defectsHMP:aerobic,NADPH-producing pathway
G6PD deficiency6PGD deficiencyGlutathione reductase def.Glutathione reductase def.

Acquired H.A.(extracorpuscular defect)
1.Immune HA A.Isoimmune: HDN
Incompatible blood transfusion B.AIHA
2.Non-immune A.Idiopathic B.secondary

secondary
1. Infection:viral, bacteria,parasites
2. Drugs and chemical3. Hematologic diseases and
malignancy4. MAHA: TTP,HUS,Kasabach’Merit
syndrome

Congenital spherocytosis

• Common cause of hemolytic anemia Abnormalities of spectrinspectrin or ankyrinankyrin
( major components of cytoskeleton responsible for RBC shape )
• Transmitted as autosomal dominantautosomal dominant , rarely autosomal recessive
• 25% of patient have no previous familial history



Clinical manifestations
• Newborn Newborn : anemia , hyperbilirubinemia• Infant & childrenInfant & children : severity is variable
- asymptomatic- pallor , fatigue, exercise intolerance- spleen enlarged, jaundice, anemia- pigmented gallstones as age 4-5 yr- profound anemia, high output heart
failure, hypoxia, cardiovascular collapse ,death

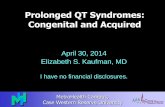
Laboratory findings• Reticulocytosis• Indirect hyperbilirubinemia• Blood smear : spherocyte > 15-20% polychromasia• Marrow : erythroid hyperplasia• Osmotic fragility test• Acidified Glycerol lysis test• Autohemolysis test• Membrane protein analysis

normal CS


normal
OF

Glucose-6-Phosphate Dehydrogenase deficiency ( G-6-PD )

• G6PD is the first enzyme in PPP in glucose metabolism
• Deficiency diminishes the reductive energy of the RC and result in hemolysis
• Severity depends on quantity and type of G6PD and nature of hemolytic agents[an oxidation-reduction mediator]
• X-link recessive transmission by a gene X chromosome• Disease expressed in hemizygous male and
homozygous female

NADPH.(PPP/HMP)
6PG
Glucose
F6P
(EMP) ATP
Pentose phosphate Pathway
Glycolysis
G-6-P
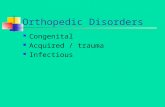
G-6-PD and the G-6-PD and the RBC metabolismRBC metabolism

pathophysiologypathophysiology
Hb
G-6-PD
(Sulf-Hb)
HEINZ’ BODY
HEMOLYSIS
INFECTION/DRUGSCATALASE
H2
O
O2H 2
GLUCOSE
GSH GSSG
NADP NADPH
G-6-P 6-PG
LACTATE HMPS
GSSG RX

Genetics of G6PD
ภาวะพร่�อง G6PD ถ่�ายทอดทาง พ�นธุ�กร่ร่มแบบ
X-linked [XY or XX]
G6PD gene อย��บน chromosome X
-G6PD (+) normal
-G6PD (-) deficient

normal hemizygote (XY) - Gd+
deficient hemizygote (XY) - Gd-
normal homozygote (XX) - Gd+/Gd+
deficient homozygote (XX)- Gd-/Gd-
** heterozygote (XX) - Gd+/gd-

ภาวะปกติ� Gd+/Gd- ratio = 100 : 0
ภาวะพร่�อง G6PD = 0 : 100
มาร่ดาท��เป�น carrier = 50 : 50

ลั�กษณะทางคลั�น�ค แติกติ�างก�นติามชน�ดของ variant แลัะ
ป$จจ�ยจากสิ่��งแวดลั'อม1.Acute hemolytic anemia (AHA)
most common
2.Neonatal jaundice (NNJ)
3.Congenital nonspherocytic hemolytic anemia (CNSHA) lifelong, rare

Acute hemolytic anemia (AHA)
ภาวะปกติ�จะไม�ม�อาการ่ เม)�อได'ร่�บ Oxidative stress
ติามหลั�งการ่ติ�ดเช)+อหร่)อยา บางชน�ดจะม�เม,ดเลั)อดแดงแติกอย�างร่วดเร่,ว
ภายใน 24-48 hr.
อาการ่เป�นแบบ Intravascular hemolysis ซี�ด, เหลั)อง, ป$สิ่สิ่าวะสิ่�เข'มหร่)อสิ่�ด/า, ม'ามไม�โติ อาจม�ไข'ติ/�า คลั)�นไสิ่' ปวดท'อง ท'องเสิ่�ยได'

Drugs –induced hemolysis in G6PD deficiency
• Analgesics and antipyretics:acetanilid• Antimalarial agents:primaquine• Sulfonamide:sulfanilamide• Nitrofurans:furazolidine, nitrofurazone• Sulfones:diaminodiphenylsulfone[DDS]• Miscelleneous:
naphthalene,phenylhydrazine,toluidene blue,nalidixic acid;

การ่ว�น�จฉั�ยโร่ค ทาร่กแร่กเก�ด ม�อาการ่ติ�วเหลั)องในว�นท�� 2-3 หลั�งคลัอด เด,กโติ/ผู้�'ใหญ่� จะม�ปร่ะว�ติ�ซี�ดลังอย�างร่วดเร่,วภายหลั�งจากการ่เป�นไข'หว�ด หร่)ออ)�นๆ หร่)อร่�วมก�บยา, สิ่าร่อาหาร่บางอย�าง ลั�กษณะป$สิ่สิ่าวะท��ผู้�ดปกติ�

ภาวะแทร่กซี'อนRBCdestruction hyperkalemia
ไติวายฉั�บพลั�น (acute tabular necrosis)
ร่ายท��ร่�นแร่ง อาจม� CHF ได'

1. Newborn ABO, sepsis
2. Hb H disease c anemic crisis
3. AIHA
4. Congenital spherocytosis c anemic crisis
การ่ว�น�จฉั�ยแยกโร่ค

Hb, Hct↓
hemoglobinemia, hemoglobinuria
blood smear :
Anisocytosis, poikilocytosis polychromasia, NRC
RC with Hb leakage RC with contracted Hb
ghost cells ,burr cells
bite cells
Lab. Investigation

reticulocytes may reach 30% or more
Heinz bodies +ve transiently, first3-4 days
G6PD Screening test
quantitative G6PD assay ** young RBC have significantly
higher enzyme activities. G6PD activity is within the low normal range

management
1. PRC transfusion when Hb ≤7 gm%2. Check fluid- electrolyte ,
urine output [ARF,K↑]
3. Vital signs[shock, CHF]

คำ��ถ�ม: คำนที่�ม�ภ�วะพร่�อง G6PD ส�ม�ร่ถบร่�จ�คำโลหิ�ตได้�หิร่�อไม�• จ�กก�ร่ว�จ�ยพบว��ในก�ร่เก#บในน�$�ย�ก�นเล�อด้
แข็#ง พบว��ม�RBC survival และviabilityต��กว��ปกต�เพ�ยงเล#กน�อย
• แต�เม�อใหิ�แก�ผู้)�ป*วยและผู้)�ป*วยร่�บปร่ะที่�นย�บ�ง อย��งเช่�น phenacetin,sulphonamide,
vitamin K , primaquine อ�จที่��ใหิ�เก�ด้ก�ร่ที่��ล�ยข็องเม#ด้เล�อด้แด้งได้�
• คำ��ตอบ: คำวร่งด้ก�ร่บร่�จ�คำโลหิ�ตตลอด้ไป





AIHAAIHAAutoimmune hemolytic anemiaAutoimmune hemolytic anemia

AIHA Autoimmune hemolytic anemia
• เป,นภ�วะซี�ด้ซี.งเก�ด้จ�กก�ร่ที่�ร่ ��งก�ยสร่��งautoantibodyข็.$นจ�บก�บRBC membrane ที่��ใหิ�เม#ด้เล�อด้แด้งอ�ย/ส�$นลง
แตกง��ยข็.$น และเก�ด้ภ�วะ hemolytic anemia โด้ยม�กม�กเป,นextracorpuscular defect

Classification of AIHA
1. แบ�งติาม thermal sensitivity หร่)อชน�ดของautoantibody
1.1 warm-reactive AIHA most common autoantibody(IgG) จ�บก�บ RBC- antigenที่�37oC
บ�งร่�ย fix complement ที่��ใหิ�เก�ด้ extravascular hemolysis

1.2 cold-reactiveAIHA ได้�แก�cold-agglutinin disease และparoxysmal cold
hemoglobinuria rare in Thailand.
autoantibody (IgM) จ�บก�บRBC-Ag ที่� 4C. fix complement ที่��ใหิ�เก�ด้intravascular hemolysis. 1.3 mixed type พบได้� 30% ในคำนไที่ย

2.แบ�งติามสิ่าเหติ�2.1 primary AIHA: idiopathic พบได้�30-50% warm-reactive autoab(IgG):most common
paroxysmal-cold hemoglobinuria(IgM) cold agglutinin disease.

2.2 Secondary AIHA :* Collagen disease : SLE, RA, thyroiditis.* Malignancy: HL, NHL, Leukemia, Solid tumor* Immunodeficiency* Infections: Mycoplasma Pn., EBV, CMV, HIV* Drug-induced -20% of cases
penicillin, cephalosporin,quinine, quinidine, Methyldopa* Thalassemia- ไทย

warm-reactive disease
IgG antibodyfixed to Ag
Adherenceto Fc receptorson macrophage
Pathogenesis
cold agglutinin
IgM fixed to Agfixed complement
Adherenceto complement
receptor
lysis by complement
intravascularhemolysis
spleenother RES
cell mediateddestruction
splenic entrapment
spherocytes

AIHA แบ�งติามสิ่าเหติ�Pirojsky (USA) มงคำล เคำร่�อ
ตร่�ช่)199 ร่�ย 100ร่�ย
• Primary 44 31• Secondary 190 69 SLE 10 42 Lymphoma 25 4 Leukemia 77 3 Thalassemia - 6

Clinical manifestationacute onset : prostration, pallor, jaundice pyrexia & hemoglobinuria
abdominal pain-less commonly
gradual onset-fatiques & pallorthe spleen is usually enlarged

Lab investigation* Hb < 6 g/dl* spherocytosis, polychromasia, NRC, fragmented RC* reticulocytosis ( 10-20%)* leukocytosis - common* platelet count - normal* DCT strongly positive, ICT +ve

TREATMENT1. Blood transfusion อ�จจ��เป,นในร่ะยะแร่กที่�ซี�ด้ม�ก ๆ
ป1ญหิ� incompatible crossmatch ต�องแยกร่ะหิว��ง auto antibody/alloantibody
2. Immunosuppressive drugs glucocorticoid : prednisolone 2 mg/kg/d non-steroidal drug : azathioprine,
cyclophosphamide

3. Intravenous immunoglobulin (IVIg)
4. Splenectomy
indication - ไม�ตอบสนองต�อ steroid
- steroid dependent- relapse
- ร่�กษ�หิล�ยว�ธี�แล�วไม�ได้�ผู้ล





unC:\WINDOWS\hinhem.scr

C:\WINDOWS\hinhem.scr FC:\WINDOWS\hinhem.scr
Top Related