






Languages
Pages
Legal


COUNTRY BRIEFING
Eliminating malaria in the DEMOCRATIC PEOPLE’S REPUBLIC OF KOREA
DPRK is working to reduce malaria transmission to 70 percent of the 2011 incidence by 2017, and achieve elimination by 2025.
Overview The Democratic People’s Republic of Korea (DPRK) has experienced a 96 percent reduction in malaria cases since 2001, from more than 140,000 to fewer than 11,000 in 2014. The national malaria program is categorized in the pre-elimination phase by the World Health Organization (WHO).1,2 DPRK first eliminated malaria in the early 1970s and remained malaria-free until cases reemerged in 1998 and quickly spread along the border with the Republic of Korea.3 Malaria cases are reported throughout the country, except in the three northern provinces of Jagang, Ryanggang, and North Hamgyong. The majority of cases occur in the three provinces bordering the demilitarized zone between DPRK and Republic of Korea (Kangwon, North Hwanghae, and South Hwanghae).2–4 Plasmodium vivax is the only malaria parasite found in DPRK, and the primary vector is Anopheles sinensis, a zoophilic mosquito that breeds in rice fields and other fresh, sun-exposed bodies of water.5,6 Secondary vec-tors include An. listeri, An. anthropophagus, and An. yatushi-roensis, which breed in low hills, rice fields, and wetlands.6,7
Malaria in DPRK is unstable and seasonal, with more than 95 percent of annual cases in the past few years reported from May to October, peaking in the summer months.3 About 70 percent of all malaria cases occur among overnight workers in the agricultural and industrial sectors, and, as observed in
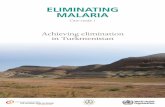
Malaria Transmission LimitsPlasmodium vivax
10,535
0
61
1.02
20.2
Total cases of malaria (100% P. vivax)
Deaths from malaria
% population living in areas of active transmission (total population: 24.9 million)
Annual parasite incidence (cases/1,000 total population/year)
% slide positivity rate
At a Glance1, 2
0 250 500 Kilometres
P. vivax malaria risk is classified into no risk, unstable risk of <0.1 case per 1,000 population (API) and stable risk of ≥0.1 case per 1,000 population (API). Risk was defined using health management information system data and the transmission limits were further refined using temperature and aridity data. Data from the international travel and health guidelines (ITHG) were used to identify zero risk in certain cities, islands and other administrative areas.
Water
P. vivax free
Unstable transmission (API <0.1)
Stable transmission (≥0.1 API)
MARCH 2015 1

COUNTRY BRIEFING
Eliminating malaria in the DEMOCRATIC PEOPLE’S REPUBLIC OF KOREA
Goals:3 1. By 2017, reduce national malaria incidence by 70 percent of the 2011 level. 2. By 2017, reduce malaria incidence in high-risk areas to less than 3 per 1,000 population. 3. Eliminate malaria by 2025.
Reported Malaria Cases*
other Asia Pacific countries, most of the at-risk population re-sides in rural areas.3,8 No malaria deaths have been reported in DPRK in more than 30 years, and mass chemoprophy-lactic efforts, called Mass Primaquine Preventive Treatment (MPPT), have been credited for the successful reduction of the malaria burden to low levels relative to the 2001 peak.7,8 In light of this progress in reducing transmission, DPRK launched a national malaria pre-elimination strategy in 2009 and updated it in 2012, emphasizing microstratification of risk areas, geographical reconnaissance to improve targeting of interventions, intensified surveillance, and community educa-tion, with an ultimate goal of national elimination by 2025.3 DPRK is also a country partner of the Asia Pacific Malaria Elimination Network (APMEN), a network composed of 17 Asia Pacific countries and other partner institutions working to eliminate malaria in the region.9
Source: World Health Organization, World Malaria Report 2014
0
30 000
60 000
90 000
120 000
150 000
1998 2000 2002 2004 2006 2008 2010 2012 2014
Num
ber
of
case
s
10,535 cases
Progress Toward Elimination P. vivax has been endemic and the cause of unstable malaria transmission on the Korean Peninsula for centuries. After Japan invaded Korea in 1910, there was no concerted effort to control malaria during the 35 years of its colonial occupa-tion.10 The end of World War II in 1945 divided the Korean Peninsula into North and South, separated by the demilita-rized zone (DMZ).11 Although malaria case data specific to DPRK was not available during the Korean War (1950–1953), it has been reported that thousands of national and foreign troops were afflicted by P. vivax throughout the Korean Peninsula as a result of wartime conditions. After the war, the number of malaria cases in DPRK reportedly diminished, yet epidemic foci remained along the southern border.10,12 Radi-cal elimination efforts by both DPRK and Republic of Korea, including mass distribution of bed nets and high coverage
MARCH 2015 2
Malaria was eliminated from DPRK in the early 1970s, but in 1998 cases reemerged and quickly spread throughout the southern and central regions. An integrated response that included mass drug administration reduced the malaria burden by 90% between 2001 and 2013.
*DPRK does not distinguish between local and imported when reporting case numbers.

COUNTRY BRIEFING
GNI per capita (US$) $1,045 or less
Country income classification Low income
Total health expenditure per capita (US$) N/A
Total expenditure on health as % of GDP N/A
Private health expenditure as % of total health expenditure
6
Eligibility for External Funding18–20
Economic Indicators21
The Global Fund to Fight AIDS, Tuberculosis and Malaria
Yes
U.S. Government’s President’s Malaria Initiative No
World Bank International Development Association No
of indoor residual spraying (IRS) and antimalarial drugs, led to a dramatic decrease in P. vivax prevalence in the 1960s and 1970s, and by 1979 the WHO declared the entire Korean Peninsula malaria-free.13,14
However, in 1993, a soldier stationed in the DMZ was diag-nosed with the first case of indigenous malaria on the Korean Peninsula in 14 years.15 Soon after, malaria spread in the DMZ and in the Republic of Korea, but the first official indigenous case in the DPRK was not reported until 1998.4 Because DPRK had been free of malaria for so long, there was very limited capacity within the Ministry of Public Health (MoPH) to respond. With the assistance of WHO, the MoPH launched a national malaria control program (NMCP) in 1999, but it was not fully operational until 2001; cases increased dramatically during this three year period, with over 600,000 reported.14,16 The rapid increase in cases was due in part to heavy rainfall and subsequent flooding that led to an increase in stagnant water in rice fields, creating ideal breeding conditions for An. sinensis. Deforestation in the 1990s, coupled with changes in rice-field irrigation systems, also contributed to the resur-gence. Further compounding the matter, the government response to the ballooning epidemic was delayed due to significant economic disruptions and intense flooding.3,12
Beginning in 2002, with support from WHO, malaria control efforts for at-risk populations focused on MPPT. Over the next five years, this large-scale intervention proved successful in decreasing the national caseload from 98,852 confirmed cases in 2002 to 4,795 in 2007; reported cases during this same time period dropped from 241,000 to 7,436.1,16 In addi-tion to MPPT, the NMCP introduced insecticide treated nets (ITNs) and IRS beginning in 2003, but coverage was low due to limited funds.14
In 2008, DPRK successfully applied for a Global Fund Round 8 grant to expand its malaria control efforts and reorient its program toward pre-elimination. The US$21.5 million grant enabled the program to: 1) enhance case management through maximizing confirmed diagnosis and treatment; 2) implement an integrated vector control approach through delivery of IRS and long-lasting insecticide-treated nets (LLINs); 3) encourage community involvement and aware-ness through malaria education campaigns; and 4) improve national and local program management through capacity-building and training.4 However, delays in disbursement of funds led to poor coverage of planned interventions and the number of confirmed cases in 2008 increased by 70 percent to 16,989.1,17 MPPT was not conducted in 2008, but once it
was implemented again in 2009, reported cases decreased by 29 percent.16 IRS and LLIN coverage improved once Round 8 funds were disbursed beginning in 2010, and the NMCP also initiated personal protection measures and com-munity education campaigns.3,17
The NMCP launched an updated pre-elimination strategy in late 2012, with the goals of reducing malaria incidence by 70 percent of the 2011 level by 2017 and achieving national elimination by 2025. Under the updated strategy, MPPT has been identified as a best practice and is a high priority for the program, as are annual IRS and LLIN distribution in medium- and high-risk areas. The NMCP is also using microstratifica-tion and geographical reconnaissance to improve targeting and monitoring of interventions, strengthening case man-agement and outbreak response capabilities, and increasing staff technical capacity through regular trainings and skill development opportunities with partner organizations such as APMEN.3 In 2013, the first full year of implementation of the updated strategy, reported cases dropped to 14,407, a 34 percent decline from 2012. A further 27 percent decline was seen in 2014, with 10,535 cases reported.1,2
Eliminating malaria in the DEMOCRATIC PEOPLE’S REPUBLIC OF KOREA
MARCH 2015 3
N/A: Data not available

COUNTRY BRIEFING
Challenges to Eliminating Malaria Characteristics of the P. vivax malaria parasiteResearch conducted by the MoPH in 2000 indicated that there are two strains of P. vivax in DPRK, one with a short incubation period of 2–3 weeks, and the other with a significantly longer incubation period of 6–18 months. The majority (70–80 percent) of infections in DPRK are caused by the latter strain, which means that most annual infections do not manifest until the following transmission season. MPPT administered prior to the annual transmission season has proven very effective in reducing malaria incidence, but this program requires extensive time and human resources to ensure safety and high coverage.16,17
Sustained financing for eliminationEconomic and trade sanctions prevent DPRK from obtain-ing finances or supplies for malaria elimination activities to which other low-income countries have access. Although the country received Round 8 funding from the Global Fund and US$13.9 million has been allocated under the new funding model for the period 2014–2016, DPRK does not qualify for many other international aid programs. The country receives only sporadic donor support, and domestic resources are insufficient to cover the funding gaps.7,22 Until recently, Republic of Korea provided annual funds and materials to DPRK’s malaria program via WHO, but this support ceased
1. Global Malaria Programme. World Malaria Report 2014. Geneva: World Health Organization; 2014.2. Democratic People’s Republic of Korea National Malaria Control Program. Program data, 2013–2014. Obtained through email
correspondence; 2015.3. Democratic People’s Republic of Korea National Malaria Control Program. National Malaria Pre-elimination Strategy in Democratic
People’s Republic of Korea 2013–2017. December 2012.4. Country Coordinating Mechanism for Democratic People’s Republic of Korea. Round 8 Proposal: Aiming for the pre-elimination of malaria
in the Democratic People’s Republic of Korea through an expanded and comprehensive approach to malaria control programming. The Global Fund to Fight AIDS, Tuberculosis and Malaria; 2008.
5. Ree HI, Hong HK, Paik YH. Study on natural infection of Plasmodium vivax in Anopheles sinensis in Korea. Korean J Parasitol 1967; 5(1): 3–4.6. Sinka ME, Bangs MJ, Manguin S, Chareonviriyaphap T, Patil AP, Temperley WH, et al. The dominant Anopheles vectors of human malaria
in the Asia-Pacific region: occurrence data, distribution maps and bionomic precis. Parasit Vectors 2011; 4:89.7. Thimasarn K. Updates on Malaria Elimination in DPR Korea. Brisbane: Asia Pacific Malaria Elimination Network Inaugural Meeting;
February, 2009.8. Country Coordinating Mechanism for Democratic People’s Republic of Korea. Round 3 Proposal: Sustainable Malaria Control in DPR
Korea. The Global Fund to Fight AIDS, Tuberculosis and Malaria; 2003.9. Asia Pacific Malaria Elimination Network. About APMEN. 2015. [Available from: http://apmen.org/about/].10. Yeo I. The Return of Malaria in Modern Korea. Helsinki: XIV International Economic History Congress, Session 46; 2006.11. Savada AM, Shaw W. South Korea: A Country Study. Washington, DC: Federal Research Division, Library of Congress; 1990. 12. Ree H. Unstable vivax malaria in Korea. Korean J Parasitol 2000; 38:119–138.
Sources
Eliminating malaria in the DEMOCRATIC PEOPLE’S REPUBLIC OF KOREA
MARCH 2015 4
once the Global Fund grant was awarded.17 Persistent food shortages and recent flooding have necessitated the diver-sion of aid toward malnutrition and other infectious diseases, compounding the malaria program’s financing challenges.23,24
Cross-Border CollaborationNo formal cross-border collaboration exists between DPRK and Republic of Korea. This is problematic since most of DPRK’s cases are concentrated in the southern provinces bordering the DMZ. Political tension between the North and South is prohibitive to any formal agreement concerning a peninsula-wide approach to controlling malaria. Small-scale collaborative efforts between DPRK and provincial govern-ments of Republic of Korea facilitated by non-governmental organizations have had success in the past, but these are lim-ited in scope and hindered by ongoing political tensions.25
ConclusionWith the support of WHO, the Global Fund, and UNICEF, DPRK has put forth a strong effort in developing and imple-menting a comprehensive malaria pre-elimination program to combat unstable and relapsing P. vivax with limited resources. Increased cross-border collaboration between the DPRK and the Republic of Korea, greater regional engage-ment through APMEN, reliable funding streams, and contin-ued strengthening of program capacity and interventions are critical for successful elimination of malaria in DPRK by 2025.

COUNTRY BRIEFING
Eliminating malaria in the DEMOCRATIC PEOPLE’S REPUBLIC OF KOREA
MARCH 2015 5
About This BriefingThis Country Briefing was developed by the UCSF Global Health Group’s Malaria Elimination Initiative, in collaboration with the WHO Regional Office for South-East Asia. Malaria transmission risk maps were provided by the Malaria Atlas Project. This document was produced by Gretchen Newby; to send comments or for additional information about this work, please email [email protected].
m a l a r i a a t l a s p r o j e c t
The Malaria Atlas Project (MAP) provided the malaria transmission maps. MAP is committed to disseminating information on malaria risk, in partnership with malaria endemic countries, to guide malaria control and elimination globally. Find MAP online at: www.map.ox.ac.uk.
The Global Health Group at the University of California, San Francisco (UCSF) is an ‘action tank’ dedicated to translating new approaches into large-scale action that improves the lives of millions of people. Launched in 2007, the UCSF Global Health Group’s Malaria Elimination Initiative works at global, regional and national levels to accelerate progress towards eradication by conducting operational research to improve surveillance and response, strengthening political and financial commitment for malaria elimination, and collaborating with country partners to shrink the malaria map.
13. World Health Organization. Synopsis of the World Malaria Situation, 1979. Wkly Epidem Rec 1981; 56: 145–152.14. Pinyowiwat V. Democratic People’s Republic of Korea Malaria Report. World Health Organization Regional Office for Southeast Asia
Malaria Report; 2004.15. Chai IH, Lim GI, Yoon SN, Oh WI, Kim SJ, Chai JY. Occurrence of tertian malaria in a male patient who has never been abroad. Korean
J Parasitol 1994; 32(3): 195–200.16. Pant SD, Chol KY, Tegegn Y, Mandal PP, Chol RK. Mass primaquine preventive treatment for control of Plasmodium vivax malaria in the
Democratic People’s Republic of Korea: a country success story. WHO South East Asia J Public Health 2014; 3(1): 75–80.17. World Health Organization Country Office for Democratic People’s Republic of Korea. Malaria in DPR Korea. WHO SEARO; 2011.18. International Development Association. IDA Borrowing Countries. 2014. [Available from: http://www.worldbank.org/ida/borrowing-
countries.html].19. President’s Malaria Initiative. PMI Focus Countries. 2014. [Available from: http://www.pmi.gov/where-we-work].20. The Global Fund to Fight AIDS, Tuberculosis and Malaria. 2014 Eligibility List. 2014. [Available from: www.theglobalfund.org/documents/
core/eligibility/Core_EligibleCountries2014_List_en/].21. The World Bank. World Development Indicators Database. 2014. [Available from: http://data.worldbank.org/data-catalog/world-
development-indicators].22. The Global Fund to Fight AIDS, Tuberculosis and Malaria. Country Allocations 2014–2016. [Available from: http://www.theglobalfund.org/
en/fundingmodel/allocationprocess/allocations/].23. United Nations Office for the Coordination of Humanitarian Affairs. Democratic People’s Republic of Korea: Humanitarian Needs and
Priorities 2013. DPRKorea: UN Resident Coordinator’s Office ; 2013.24. United Nations Office of the Resident Coordinator. Democratic People’s Republic of Korea: Flooding. Country Emergency Situation
Report No. 3; 2013.25. Hwang JS. Malaria Control Project in the DPRK. Korean Sharing Movement; 2011.
Transmission Limits Map SourcesGuerra CA, Howes RE, Patil AP, Gething PW, Van Boeckel TP, Temperley WH, Kabaria CW, Tatem AJ, Manh BH, Elyazar IRF, Baird JK, Snow
RW and Hay SI. (2010). The international limits and population at risk of Plasmodium vivax transmission in 2009. Public Library of Science Neglected Tropical Diseases, 4(8): e774.
Top Related