







Languages
Pages
Legal

CORE VALUE 1
Holistic Philosophy, Theories, and Ethics
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 1
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 2
3
NURSE HEALER OBJECTIVES
Theoretical
• Examine the United Nations MillenniumGoals.
• Link Florence Nightingale’s legacy of heal-ing, leadership, global action, and her workas a nurse and citizen activist to 21st-centuryintegral and holistic nursing.
• Analyze relationship-centered c are and itsthree components.
• Explore the Theory of Integral Nursing andits application to holistic nursing.
Clinical
• Apply relationship-centered care principlesand components in your practice.
• Compare and contrast the three eras ofmedicine.
• Examine the Theory of Integral Nursing, andbegin the process of integrating the theoryinto your clinical practice.
• Determine if you have an integral worldviewand approach in your clinical practice andother education, research hospital policies,and community endeavors.
Personal
• Create an integral self-care plan.• Examine ways to enhance your integral
understanding in your personal endeavors.• Develop short- and long-term goals related
to increasing your commitment to an inte-gral developmental process.
DEFINITIONS
Holistic nursing: See Chapter 2 definitions.Global health: Exploration of the emerging value
base and new relationships and agendas thatoccur when health becomes an essential compo-nent and expression of global citizenship; anincreased awareness that health is a basic humanright and a global good that needs to be pro-moted and protected by the global community.
Integral: Comprehensive way to organize multiplephenomenon of human experience related tofour perspectives of reality: (1) the individualinterior (personal/intentional), (2) individualexterior (physiology/behavioral), (3) collectiveinterior (shared/cultural), and (4) collective ex-terior (systems/structures).
Integral dialogue: Transformative and visionaryexploration of ideas and possibilities across dis-ciplines where the individual interior (personal/intentional), individual exterior (physiology/behavioral), collective interior (shared/cultural),and collective exterior (structures/systems) areconsidered as equally important to exchangesand outcomes.
Chapter 1
Integral and Holistic Nursing:Local to GlobalBarbara Montgomery Dossey
Portions of this chapter on the Theory of Integral Nurs-ing have been published as: B. M. Dossey, “Theory of Inte-gral Nursing,” Advances in Nursing Science 31, no. 1 (2008):E52–E73.
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 3

Integral health: Process through which wereshape basic assumptions and worldviewsabout well-being and see death as a naturalprocess of living; may be symbolically seen as ajewel with many facets that is reflected as a“bright gem” or a “rough stone” depending onone’s situation and personal growth that influ-ence states of health, health beliefs, and values.
Integral health care: A patient-centered andrelationship-centered caring process thatincludes the patient, family, and communityand conventional, integrative, and integralhealthcare practitioners and services and inter-ventions; a process where the individual inte-rior (personal/intentional), the individualexterior (physiology/behavioral), the collectiveinterior (shared/cultural), and the collectiveexterior (structures/systems) are considered inall endeavors.
Integral healing process: Contains both nurseprocesses and patient/family and healthcareworkers processes (individual interior and indi-vidual exterior), and collective healing processesof individuals and of systems/structures (collec-tive interior and exterior); an understanding ofthe unitary whole person interacting in mutualprocess with the environment.
Integral nurse: A 21st-century Nightingale that isengaged as a “health diplomat” and an integralhealth coach that is coaching for integral health.
Integral nursing: A comprehensive integral world-view and process that includes holistic theoriesand other paradigms; holistic nursing is included(embraced) and transcended (goes beyond); thisintegral process and integral worldview enlargesour holistic understanding of body-mind-spiritconnections and our knowing, doing, and beingto more comprehensive and deeper levels.
Integral worldview: Process where values, beliefs,assumptions, meaning, purpose, and judgmentsare identified and related to how individualsperceive reality and relationships that includesthe individual interior (personal/ intentional),individual exterior (physiology/behavioral),collective interior (shared/cultural), and collec-tive exterior (systems/structures)
Relationship-centered care: A process model ofcaregiving that is based in a vision of community
where the patient–practitioner, community–practitioner, and practitioner–practitioner rela-tionships and the unique set of responsibilities ofeach are honored and valued.
INTEGRAL AND HOLISTIC NURSING
Integral nursing can be described as a comprehen-sive integral worldview and process that includesholistic theories and other paradigms; holisticnursing practice is included (embraced) and tran-scended (goes beyond).1,2 This integral processand integral worldview enlarges our holisticunderstanding of body-mind-spirit connectionsand our knowing, doing, and being to more com-prehensive and deeper levels. These ideas are fur-ther developed under the section on the Theory ofIntegral Nursing.
Holistic nursing is defined as “all nursing prac-tice that has healing the whole person as its goal.”3
As described and developed in Chapter 2 holisticnursing has attained new levels of acceptance andis now officially recognized by the AmericanNurses Association (ANA) as a nursing specialtywith a defined scope and standards of practice.3
Our holistic nursing challenges as describedthroughout this book include ways to learn andintegrate new theories, models, and information,and how to articulate the science and art of holis-tic nursing, complementary and alternativemodalities (CAM), and healing in all areas andspecialties of nursing. Our opportunities to inter-face in collaborative endeavors with various tradi-tional and nontraditional healthcare professionals,healers, disciplines, and organizations can trans-form health care.
Outside of nursing, there continues to be mini-mal understanding and recognition related to thedepth of nurses’ knowledge, expertise, and critical-thinking capacities and skills for assisting others inachieving and maintaining health and well-being.Globalization has changed the picture of globalhealth to one that knows no natural or politicalboundaries.4-7 Global health is the exploration ofthe emerging value base and new relationshipsand agendas that occur when health becomes anessential component and expression of global citi-zenship. It is an increased awareness that health is
4 CHAPTER 1 INTEGRAL AND HOLISTIC NURSING: LOCAL TO GLOBAL
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 4

a basic human right and a global good that needsto be promoted and protected by the global com-munity. Severe health needs exist in almost everycommunity and nation throughout the world.Thus, all nurses are involved in some aspect ofglobal health as their caring and healing endeavorsassist individuals to become healthier. To have ahealthy world we must have healthy people andhealthy environments.
Currently there are 13 million nurses and mid-wives engaged in nursing and providing health carearound the world.8 Together, we are collectivelyaddressing human health—the health of individu-als, of communities, of environments (interior andexterior), and the world as our first priority. Weare educated and prepared—physically, emotion-ally, socially, mentally, and spiritually—to effec-tively accomplish the activities required to create ahealthy world. Nurses are key in mobilizing newapproaches in health education and healthcaredelivery in all areas of nursing. Solutions andevidence-base practice protocols can be shared andimplemented around the world through dialogues,the Internet, and publications.
We are challenged—to act locally and thinkglobally—and to address ways to create healthyenvironments. For example, we can address globalwarming in our own personal habits at home aswell as in our workplace (using green products,using energy efficient fluorescent bulbs, turning offlights when not in the room) and simultaneouslyaddress our own personal health and the health ofthe communities where we live. In 2000, the UnitedNations Millennium Goals were recommended toclearly articulate how to achieve health and decreasehealth disparities (see Table 1-1).9 As we expand ourawareness of individual and collective states of heal-ing consciousness and integral dialogues, we areable to explore integral ways of knowing, doing,and being. We can unite 13 million nurses, mid-wives, and concerned citizens through the Internetto create a healthy world through many endeavorssuch as the Nightingale Declaration (see Table 1-2).You are invited to sign the Nightingale Declarationat http://www. nightingaledeclaration.net. OurNightingale nursing legacy as discussed in the nextsection is the foundation to understanding ourimportant roles as 21st-century nurses.
PHILOSOPHICAL FOUNDATION:FLORENCE NIGHTINGALE’S LEGACY
Florence Nightingale (1820–1910), the philosoph-ical founder of modern secular nursing and the
Philosophical Foundation: Florence Nightingale’s Legacy 5
Table 1-1 UN Millennium Development Goals and Targets
The UN Millennium Development Goals are an ambi-tious agenda for reducing poverty and improving lives.World leaders agreed to these goals at the MillenniumSummit in September 2000. For each goal one or moretargets have been set, most for 2015, using 1990 as abenchmark.
1. Eradicate extreme poverty and hunger.
2. Achieve universal primary education.
3. Promote gender equality and empower women.
4. Reduce child mortality.
5. Improve maternal health.
6. Combat HIV/AIDS, malaria, and other diseases.
7. Ensure environmental sustainability.
8. Develop global partnerships for development.
Source: World Health Organization, WHO Assembly Report:Millennium Development Goals and Targets (Geneva, WHO:2000), http://www.who.int/mdg/en.
Table 1-2 Nightingale Declaration for a Healthy Worldby 2020
“We, the nurses and concerned citizens of the globalcommunity, hereby dedicate ourselves to achieve ahealthy world by 2020.
We declare our willingness to unite in a program ofaction, to share information and solutions, and toimprove health conditions for all humanity—locally,nationally, and globally.
We further resolve to adopt personal practices and toimplement public policies in our communities andnations—making this goal achievable and inevitable bythe year 2020, beginning today in our own lives, in thelife of our nations, and in the world at large.”
Signature _______________________________________
Source: Used with permission, Nightingale Initiative for GlobalHealth, http://www.nightingaledeclaration.net.
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 5

first recognized nurse theorist, was an integralist.An integralist is a person that focuses on the indi-vidual and the collective, the inner and outer, andhuman and nonhuman concerns. Nightingale wasconcerned with the most basic needs of humanbeings and all aspects of the environment (clean air,water, food, houses, etc.)—local to global.4,5,10,11 Shealso experienced and recorded her personal under-standing of the connection with the Divine as anawareness that something greater than her, theDivine, was a major connecting link woven intoher work and life.4,10
Nightingale was a nurse, an educator, admin-istrator, communicator, statistician, and an envi-ronmental activist. Her specific accomplishmentsinclude establishing the model for nursingschools throughout the world and creating a pro-totype model of care for the sick and woundedsoldiers during the Crimean War (1854–1856).She was an innovator for British Army medicalreform that included reorganizing the BritishArmy Medical Department, creating an ArmyStatistical Department, and collaborating on thefirst British Army medical school, includingdeveloping the curriculum and choosing the pro-fessors. She revolutionized hospital data collec-tion and invented a statistical wedge diagramequivalent to today’s circular histograms or cir-cular statistical representation, and in 1858 shebecame the first woman admitted to the RoyalStatistical Society. She developed and wrote pro-tocols and papers on workhouses and midwiferythat lead to successful legislation reform. She wasa recognized expert on the health of the BritishArmy and soldiers in India for over 40 years; shenever went to India but collected date directlyfrom Army stations, analyzed the data, and wroteand published documents, articles, and books onthe topic. Besides her numerous other recogni-tions, she received the Order of Merit in 1902,the first woman to receive this honor. She wroteover 100 combined books and official Armyreports; her 10,000 letters now make up thelargest private collection of letters at the BritishLibrary with 4000 family letters at the WellcomeTrust in London.4,5,10
Today we recognize Nightingale’s work asglobal nursing where she envisioned what ahealthy world might be with her integral philoso-
phy and expanded visionary capacities. Her workincluded aspects of the nursing process (see Chap-ter 8) as well; her work has indeed had an impacton us and will extend far into the future. Nightin-gale’s work was social action that demonstratedand clearly articulated the science and art of anintegral worldview for nursing, health care, andhumankind. Her social action was also sacredactivism,12 the fusion of the deepest spiritualknowledge with radical action in the world. In the1880s Nightingale began to write that it wouldtake 100–150 years before educated and experi-enced nurses would arrive to change the health-care system. We are that generation of21st-century Nightingales who have arrived totransform health care and carry forth her vision ofsocial action and sacred activism to create ahealthy world. Using terms coined by PatriciaHinton Walker, PhD, RN, FAAN, 21st-centuryNightingales are “health diplomats” and “integralhealth coaches” that are “coaching for integralhealth.”13
Nightingale was ahead of her time. Her dedi-cated and focused 50 years of work and service stillinforms and impacts our nursing work and ourglobal mission of health and healing for humanity.Table 1-3 list the themes in her Notes on Hospitals(1859),14 Notes on Nursing (1860),15 her formalletters to her nurses (1872–1900),16 and her “Sick-Nursing and Health-Nursing” (1893).17 Table 1-4shows Nightingale’s themes today that we recog-nize in integral and holistic nursing and total heal-ing healthcare environments.4 The next sectionpresents an overview of the Eras of Medicine.
ERAS OF MEDICINE
Three eras of medicine currently are operationalin Western biomedicine (see Table 1-5).18 Era Imedicine began to take shape in the 1860s, whenmedicine was striving to become increasingly sci-entific. The underlying assumption of this ap-proach is that health and illness are completelyphysical in nature. The focus is on combiningdrugs, medical treatments, and technology. A per-son’s consciousness is considered a by-product ofthe chemical, anatomic, and physiologic aspects ofthe brain and is not considered a major factor inthe origins of health or disease.
6 CHAPTER 1 INTEGRAL AND HOLISTIC NURSING: LOCAL TO GLOBAL
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 6

Eras of Medicine 7
Table 1-3 Florence Nightingale’s Legacy and Themes for Today
Themes Developed in Notes on Hospitals (1859, 1863)
The hospital will do the patient no harm. Four elements essential for the health of hospitals:
• Fresh air • Light
• Ample space • Subdivision of sick into separate buildings or pavilions
Hospital construction defects that prevented health:
• Defective means of natural ventilation and warming
• Defective height of wards
• Excessive width of wards between the opposite windows
• Arrangement of the bed along the dead wall
• More than two rows of beds between the opposite windows
• Windows only on one side, or a closed corridor connecting the wards
• Use of absorbent materials for walls and ceilings, and poor washing of hospital floors
Themes Developed in Notes on Nursing (1860)
Understand God’s laws in nature
• Understanding that, in disease and in illness, nursing and the nurses can assist in the reparative process of a disease and in maintaining health
Nursing and nurses
• Describing the many roles and responsibilities of the nurse
Patient
• Observing and managing the patient’s problems, needs, and challenges, and evaluating responses to care
Health
• Recognizing factors that increase or decrease positive or negative states of health, well-being, disease, and illness
Environment
• Both the internal (within one’s self) and the external(physical space). (See the specifics listed in the next 10 categories.)
Bed and bedding
• Promote proper cleanliness.
• Use correct type of bed, with proper height, mattress, springs, types of blankets, sheets, and other bedding.
Cleanliness (rooms and walls)
• Maintain clean room, walls, carpets, furniture, and dust-free rooms using correct dusting techniques.
• Release odors from painted and papered rooms; discusses other remedies for cleanliness.
• Defective condition of water closets
• Defective ward furniture
• Defective accommodation for nursing and discipline
• Defective hospital kitchens
• Defective laundries
• Selection of bad sites and bad local climates for hospitals
• Erecting of hospitals in towns
• Defects of sewerage
• Construction of hospitals without free circulation of external air
Cleanliness (personal)
• Provide proper bathing, rubbing, and scrubbing ofthe skin of the patient as well as of the nurse.
• Use proper handwashing techniques that includecleaning the nails.
Food
• Provide proper portions and types of food at the righttime, and a proper presentation of food types: eggs,meat, vegetables, beef teas, coffee, jellies, sweets,and homemade bread.
Health of houses
• Provide pure air, pure water, efficient drainage, clean-liness, and light.
Light
• Provide a room with light, windows, and a view thatis essential to health and recovery.
Noise
• Avoid noise and useless activity such as clanking orloud conversations with or among caregivers.
• Speak clearly for patients to hear without having tostrain.
• Avoid surprising the patient.
• Only read to a patient if it is requested.
Petty management
• Ensure patient privacy, rest, a quiet room, andinstructions for the person managing care of patient.
(continues)
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 7

8 CHAPTER 1 INTEGRAL AND HOLISTIC NURSING: LOCAL TO GLOBAL
Table 1-3 Florence Nightingale’s Legacy and Themes for Today (continued)
Themes Developed in Notes on Nursing (1860)
Variety
• Provide flowers and plants and avoid those with fragrances.
• Be aware of effects of mind (thoughts) on body.
• Help patient vary their painful thoughts.
• Use soothing colors.
• Be aware of positive effect of certain music on the sick.
Ventilation and warming
• Provide pure air within and without; open windows and regulate room temperature.
• Avoid odiferous disinfectants and sprays.
Chattering hopes and advice
• Avoid unnecessary advice, false hope, promises, and chatter of recovery.
• Avoid absurd statistical comparisons of patient to recovery of other patients, and avoid mockery of advice given by family and friends.
• Share positive events; encourage visits from a well-behaved child or baby.
• Be aware of how small pet animals can provide comfort and companionship for the patient.
Observation of the sick
• Observe each patient; determine the problems, challenges, and needs.
• Assess how the patient responds to food, treatment, and rest.
• Help patient with comfort, safety, and health strategies.
• Intervene if danger to patient is suspected.
Themes Developed in Letters to Her Nurses (1872–1900)*
All themes above in Notes on Hospitals and Notes on Nursing plus:
Art of nursing
• Explore authentic presence, caring, meaning, and purpose.
• Increase communication with colleagues, patients, and families.
• Build respect, support, and trusting relationships.
Environment
• Includes the internal self as well as the external physical space
Ethics of nursing
• Engage in moral behaviors and values and model it in personal and professional life.
Health
• Integrate self-care and health-promoting and sustaining behaviors.
• Be a role model and model healthy behaviors.
Personal aspects of nursing
• Explore body-mind-spirit wholeness, healing philosophy, self-care, relaxation, music, prayers, and work of service to self and others.
• Develop therapeutic and healing relationships.
Science of nursing
• Learn nursing knowledge and skills, observing, implementing, and evaluating physicians’ orders combined with nursing knowledge and skills.
Spirituality
• Develop intention, self-awareness, mindfulness, presence, compassion, love, and service to God and humankind.
Themes Developed in “Sick-Nursing and Health-Nursing” (1893 Essay)**
All themes above in Notes on Nursing and her Letters to Her Nurses (1872–1893) plus:
Collaboration with others
• Meet with nurses and women at the local, national, and global level to explore health education and how to support each other in creating health and healthy environments.
Health education curriculum and health missioners education
• Include all components discussed in Notes on Nursing.
• Teach health as proactive leadership for health.
Source: Used with permission. B. M. Dossey, “Florence Nightingale’s Tenets: Healing, Leadership, Global Action,” in FlorenceNightingale Today: Healing, Leadership, Global Action, eds. B. M. Dossey et al. (Silver Spring, MD: Nursesbooks.org, 2005).
ED/?whereareTFNsfor * &**
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 8
Eras of Medicine 9
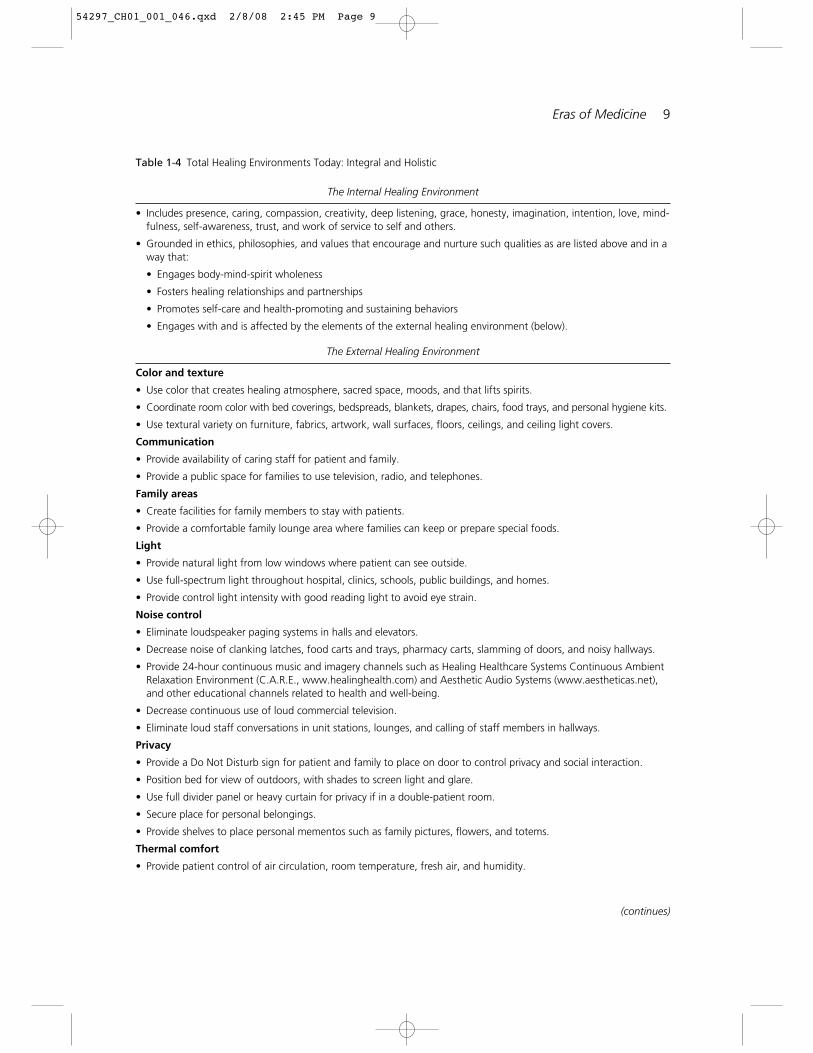
Table 1-4 Total Healing Environments Today: Integral and Holistic
The Internal Healing Environment
• Includes presence, caring, compassion, creativity, deep listening, grace, honesty, imagination, intention, love, mind-fulness, self-awareness, trust, and work of service to self and others.
• Grounded in ethics, philosophies, and values that encourage and nurture such qualities as are listed above and in away that:
• Engages body-mind-spirit wholeness
• Fosters healing relationships and partnerships
• Promotes self-care and health-promoting and sustaining behaviors
• Engages with and is affected by the elements of the external healing environment (below).
The External Healing Environment
Color and texture
• Use color that creates healing atmosphere, sacred space, moods, and that lifts spirits.
• Coordinate room color with bed coverings, bedspreads, blankets, drapes, chairs, food trays, and personal hygiene kits.
• Use textural variety on furniture, fabrics, artwork, wall surfaces, floors, ceilings, and ceiling light covers.
Communication
• Provide availability of caring staff for patient and family.
• Provide a public space for families to use television, radio, and telephones.
Family areas
• Create facilities for family members to stay with patients.
• Provide a comfortable family lounge area where families can keep or prepare special foods.
Light
• Provide natural light from low windows where patient can see outside.
• Use full-spectrum light throughout hospital, clinics, schools, public buildings, and homes.
• Provide control light intensity with good reading light to avoid eye strain.
Noise control
• Eliminate loudspeaker paging systems in halls and elevators.
• Decrease noise of clanking latches, food carts and trays, pharmacy carts, slamming of doors, and noisy hallways.
• Provide 24-hour continuous music and imagery channels such as Healing Healthcare Systems Continuous AmbientRelaxation Environment (C.A.R.E., www.healinghealth.com) and Aesthetic Audio Systems (www.aestheticas.net),and other educational channels related to health and well-being.
• Decrease continuous use of loud commercial television.
• Eliminate loud staff conversations in unit stations, lounges, and calling of staff members in hallways.
Privacy
• Provide a Do Not Disturb sign for patient and family to place on door to control privacy and social interaction.
• Position bed for view of outdoors, with shades to screen light and glare.
• Use full divider panel or heavy curtain for privacy if in a double-patient room.
• Secure place for personal belongings.
• Provide shelves to place personal mementos such as family pictures, flowers, and totems.
Thermal comfort
• Provide patient control of air circulation, room temperature, fresh air, and humidity.
(continues)
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 9
In the 1950s, Era II therapies began to emerge.These therapies reflected the growing aware-ness that the actions of a person’s mind orconsciousness—thoughts, emotions, beliefs,meaning, and attitudes—exerted important effectson the behavior of the person’s physical body.18 Inboth Era I and Era II, a person’s consciousness issaid to be “local” in nature; that is, confined to aspecific location in space (the body itself) and intime (the present moment and a single lifetime).
Era III, the newest and most advanced era, orig-inated in science. Consciousness is said to be non-local in that it is not bound to individual bodies.18
The minds of individuals are spread throughoutspace and time; they are infinite, immortal,omnipresent, and, ultimately, one. Era III thera-pies involve any therapy in which the effects ofconsciousness create bridges between different
persons, as with distant healing, intercessoryprayer, shamanic healing, so-called miracles, andcertain emotions (e.g., love, empathy, compas-sion). Era III approaches involve transpersonalexperiences of being. They raise a person abovecontrol at a day-to-day material level to an experi-ence outside his or her local self.
“Doing” and “Being” Therapies
Holistic nurses use both “doing” and “being”therapies as seen in Figure 1-1. (The reader isreferred to Chapter 2 and Chapter 3 for thespecifics on these therapies that are also referredto as holistic nursing therapies, complementaryand alternative therapies, or integrative and inte-gral therapies). Doing therapies include almost allforms of modern medicine, such as medications,
10 CHAPTER 1 INTEGRAL AND HOLISTIC NURSING: LOCAL TO GLOBAL
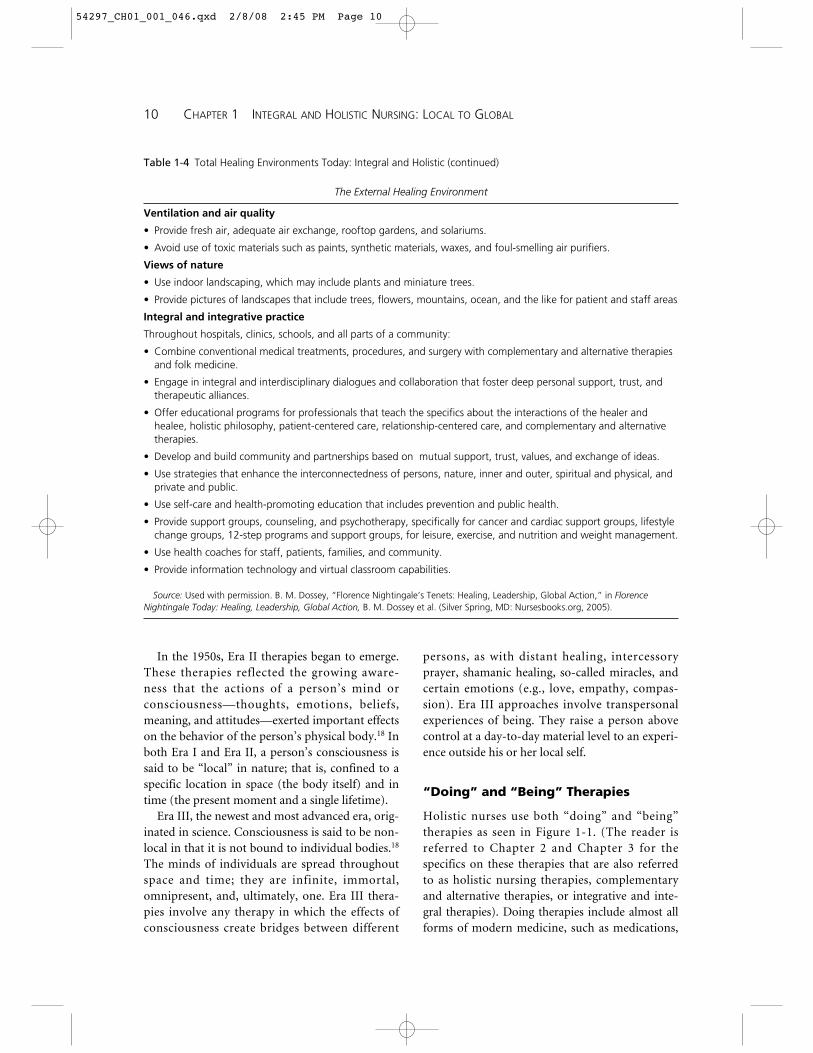
Table 1-4 Total Healing Environments Today: Integral and Holistic (continued)
The External Healing Environment
Ventilation and air quality
• Provide fresh air, adequate air exchange, rooftop gardens, and solariums.
• Avoid use of toxic materials such as paints, synthetic materials, waxes, and foul-smelling air purifiers.
Views of nature
• Use indoor landscaping, which may include plants and miniature trees.
• Provide pictures of landscapes that include trees, flowers, mountains, ocean, and the like for patient and staff areas
Integral and integrative practice
Throughout hospitals, clinics, schools, and all parts of a community:
• Combine conventional medical treatments, procedures, and surgery with complementary and alternative therapiesand folk medicine.
• Engage in integral and interdisciplinary dialogues and collaboration that foster deep personal support, trust, andtherapeutic alliances.
• Offer educational programs for professionals that teach the specifics about the interactions of the healer andhealee, holistic philosophy, patient-centered care, relationship-centered care, and complementary and alternativetherapies.
• Develop and build community and partnerships based on mutual support, trust, values, and exchange of ideas.
• Use strategies that enhance the interconnectedness of persons, nature, inner and outer, spiritual and physical, andprivate and public.
• Use self-care and health-promoting education that includes prevention and public health.
• Provide support groups, counseling, and psychotherapy, specifically for cancer and cardiac support groups, lifestylechange groups, 12-step programs and support groups, for leisure, exercise, and nutrition and weight management.
• Use health coaches for staff, patients, families, and community.
• Provide information technology and virtual classroom capabilities.
Source: Used with permission. B. M. Dossey, “Florence Nightingale’s Tenets: Healing, Leadership, Global Action,” in FlorenceNightingale Today: Healing, Leadership, Global Action, B. M. Dossey et al. (Silver Spring, MD: Nursesbooks.org, 2005).
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 10

procedures, dietary manipulations, radiation, andacupuncture. In contrast, being therapies do notemploy things, but instead use states of conscious-ness.19,20 These include imagery, prayer, meditation,and quiet contemplation, as well as the presence andintention of the nurse. These techniques are thera-peutic because of the power of the psyche to affectthe body. They may be either directed or nondi-rected.20,21 A person who uses a directed mentalstrategy attaches a specific outcome to the imagery,such as the regression of disease or the normaliza-
tion of the blood pressure. In a nondirectedapproach, the person images the best outcome forthe situation, but does not try to direct the situationor assign a specific outcome to the strategy. Thisreliance on the inherent intelligence within one’s selfto come forth is a way of acknowledging the intrin-sic wisdom and self-correcting capacity from within.
It is obvious that Era I medicine uses “doing”therapies that are highly directed in theirapproach. It employs things, such as medications,for a specific goal. Era II medicine is a classic
Eras of Medicine 11
Table 1-5 Eras of Medicine
Era I Era II Era III
Space-Time Local Local NonlocalCharacteristic
Synonym
Description
Examples
Mechanical, material, orphysical medicine
Causal, deterministic,describable by classicalconcepts of space-timeand matter- energy.Mind not a factor;“mind” a result of brainmechanisms.
Any form of therapy focus-ing solely on the effectsof things on the body isan Era I approach—including techniquessuch as acupuncture andhomeopathy, the use ofherbs, etc. Almost allforms of “modern” med-icine—drugs, surgery,irradiation, CPR, etc.—are included.
Mindbody medicine
Mind a major factor in heal-ing within the single per-son. Mind has causalpower; is thus not fullyexplainable by classicalconcepts in physics.Includes but goes beyondEra I.
Any therapy emphasizingthe effects of conscious-ness solely within the individual body is an Era II approach. Psycho-neuroimmunology,counseling, hypnosis,biofeedback, relaxationtherapies, and most typesof imagery-based “alter-native” therapies areincluded.
Nonlocal or transpersonalmedicine
Mind a factor in healingboth within and betweenpersons. Mind not com-pletely localized to pointsin space (brains or bod-ies) or time (presentmoment or single life-times). Mind isunbounded and infinitein space and time—thusomnipresent, eternal,and ultimately unitary orone. Healing at a dis-tance is possible. Notdescribable by classicalconcepts of space-timeor matter-energy.
Any therapy in whicheffects of consciousnessbridge between differentpersons is an Era IIIapproach. All forms ofdistant healing, interces-sory prayer, some typesof shamanic healing,diagnosis at a distance,telesomatic events, andprobably noncontacttherapeutic touch areincluded.
Source: Reprinted with permission from L. Dossey, Reinventing Medicine: Beyond Mind-Body to a New Era of Healing. SanFrancisco: HarperSanFrancisco, 1999. Copyright Larry Dossey.
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 11

body-mind approach that usually does not requirethe use of things, with the exception of biofeed-back instrumentation, music therapy, and use ofCD and videos to enhance learning and experi-ence an increase in awareness of body-mind con-nections. It employs being therapies that can bedirected or nondirected, depending on the mentalstrategies selected (e.g., relaxation or meditation).Era III medicine is similar in this regard. Itrequires a willingness to become aware, momentby moment, of what is true for our inner andouter experience. It is actually a “not doing,” sothat we can become conscious of releasing, empty-ing, trusting, and acknowledging that we havedone our best, regardless of the outcome. As thetherapeutic potential of the mind becomesincreasingly clear, all therapies and all people areseen to have a transcendent quality. The minds ofall people, including families, friends, and thehealthcare team (both those in close proximityand those at a distance), flow together in a collec-tive as they work to create healing and health.
Rational vs. Paradoxical Healing
All healing experiences or activities can bearranged along a continuum from the rationaldomain to the paradoxical domain.21 The degreeof doing and being involved determines thesedomains, as seen in Figure 1-2. Rational healingexperiences include those therapies or events that
make sense to our linear, intellectual thoughtprocesses, whereas paradoxical healing experi-ences include healing events that may seem absurdor contradictory but are, in fact, true.
“Doing” therapies fall into the rational healingcategory. Based on science, these strategies con-form to our worldview of commonsense notions.Often, the professional can follow an algorithm,which dictates a step-by-step approach. Examplesof rational healing include surgery, irradiation,medications, exercise, and diet. On the otherhand, being therapies fall into the paradoxicalhealing category, because they frequently happenwithout a scientific explanation. In psychologicalcounseling, for example, a breakthrough is a para-dox. When a patient has a psychologic break-through, it is clear that there is a new meaning forthe person. However, there were no clearly delin-eated steps leading to the breakthrough. Such an
12 CHAPTER 1 INTEGRAL AND HOLISTIC NURSING: LOCAL TO GLOBAL
Figure 1-1 “Being” and “Doing” TherapiesSource: Reprinted with permission from L. Dossey,
Meaning and Medicine: A Doctor’s Tales of Break-through and Healing, by Larry Dossey, p. 204, NewYork, Bantam Books, 1991. Copyright Larry Dossey.
Paradoxical Healing
Rational Healing
Bei
ng
Doi
ng
Figure 1-2 Continuum of Rational and Paradoxi-cal Healing
Source: Reprinted with permission from L. Dossey,Meaning and Medicine: A Doctor’s Tales of Break-through and Healing, by Larry Dossey, p. 205, NewYork, Bantam Books, 1991. Copyright Larry Dossey.
Paradoxical Healing
Rational Healing
Miracles
Prayer
Placebo effects
Biofeedback
Psychological counseling
Drugs
Irradiation
Surgery
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 12

event is called a breakthrough for the very reasonthat it is unpredictable—thus, the paradox.
Biofeedback also involves a paradox. For exam-ple, the best way to reduce blood pressure or mus-cle tension, or to increase peripheral blood flow, isto give up trying and just learn how to be. Individu-als can enter into a state of being, or passive voli-tion, in which they let these physiologic stateschange in the desired direction. Similarly, the phe-nomenon of placebo is a paradox. If an individualhas just a little discomfort, a placebo does not workvery well. The more pain a person has, however, themore dramatic the response to a placebo medica-tion can be. In addition, a person who does notknow that the medication is a placebo respondsbest. This is referred to as the “paradox of successthrough ignorance.” Prayer and faith fall into thedomain of paradox because there is no rational sci-entific explanation for their effectiveness. Manyscientific studies have been conducted, however.22, 23
Miracle cures also are paradoxical, becausethere is no scientific mechanism to explain them.23
Every nurse has known, heard of, or read about apatient who had a severe illness that had been con-firmed by laboratory evidence but which disap-peared after the patient adopted a being approach.Some say that it was the natural course of the ill-ness; some die and some live. At shrines such asLourdes in France and Medjugorje in Yugoslavia,however, people who experience a miracle cureare said to be totally immersed in a being state.They do not try to make anything happen. Wheninterviewed, these people report experiencing adifferent sense of space and time; the flow of timeas past, present, and future becomes an eternalnow. Birth and death take on new meaning andare not seen as a beginning and an end. These peo-ple go into the self and explore the “not I” tobecome empty so that they can understand themeaning of illness or present situations. To fur-ther integrate these concepts, relationship-centered care is discussed next.
RELATIONSHIP-CENTERED CARE
In integral and holistic nursing, relationship-centeredcare serves as a model of caregiving that is based in avision of community where three types of relation-
ships are identified: (1) patient–practitioner rela-tionship, (2) community–practitioner relationship,and (3) practitioner–practitioner relationship.24
Relationship-based care is also valued as it pro-vides the map and highlights the most directroutes to achieve the highest levels of care and ser-vice to patients and families.25 In 1994, the PewHealth Professions Commission published itsreport on relationship-centered care.24 This re-port serves as a guideline for addressing the bio-psycho-social-spiritual dimensions of individualsin integrating caring, healing, and holism intohealth care. The guidelines are based on the tenetthat relationships and interactions among peopleconstitute the foundation for all therapeutic activi-ties. The three components of relationship-centeredcare are now discussed and shown in Tables 1-6,1-7, and 1-8. Each of these interrelated relation-ships is essential within a reformed system ofhealth care, and each involves a unique set of tasksand responsibilities that address self-awareness,knowledge, values, and skills.
Patient–Practitioner Relationship
In integral health care the patient–practitioner rela-tionship is crucial on many levels. The practitionerincorporates comprehensive biotechnologic carewith psycho-social-spiritual care. To work effec-tively within the patient–practitioner relationship,the practitioner must develop specific knowledge,skills, and values as seen in Table 1-6.24 This includesan expanding self-awareness, understanding thepatient’s experience of health and illness, developingand maintaining caring relationships with patients,and communicating clearly and effectively.
Active collaboration with the patient and familyin the decision-making process, promotion ofhealth, and prevention of stress and illness withinthe family are also part of the relationship. A suc-cessful relationship involves active listening andeffective communication; integration of the ele-ments of caring, healing, values, and ethics toenhance and preserve the dignity and integrity ofthe patient and family; and a reduction of thepower inequalities in the relationship with regardto race, sex, education, occupation, and socioeco-nomic status.
Relationship-Centered Care 13
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 13

Community–Practitioner Relationship
In integral health care the patient and his or herfamily simultaneously belong to many types ofcommunities, such as the immediate family, rela-tives, friends, coworkers, neighborhoods, religiousand community organizations, and the hospitalcommunity. The knowledge, skills, and valuesneeded by practitioners to participate effectively inand work with various communities are shown inTable 1-7. This includes understanding the mean-ing of the community, recognizing the multiplecontributors to health and illness within the com-munity, developing and maintaining relationshipswith the community, and working collaborativelywith other individuals and organizations to estab-lish effective community-based care.24
Practitioners must be sensitive to the impact ofthese various communities on patients and fosterthe collaborative activities of these communities asthey interact with the patient and family. Therestraints or barriers within each community thatblock the patient’s healing must be identified andimproved to promote the patient’s health andwell-being.
Practitioner–Practitioner Relationship
Providing integral care to patients and familiescan never take place in isolation; it involves manydiverse practitioner–practitioner relationships. Toform a practitioner–practitioner relationshiprequires the knowledge, skills, and values shown
14 CHAPTER 1 INTEGRAL AND HOLISTIC NURSING: LOCAL TO GLOBAL
Table 1-6 Patient–Practitioner Relationship: Areas of Knowledge, Skills, and Values
Area Knowledge Skills Values
Source: Pew Health Professions Commission at the Center for the Health Professions, University of California, San Francisco, 1388Sutter Street, Suite 805, San Francisco, California 94109, (415) 476-8181.
Self-awareness
Patient experience ofhealth and illness
Developing and maintain-ing caring relationships
Effective communication
Knowledge of selfUnderstanding self as a
resource to others
Role of family, culture,community in development
Multiple components ofhealth
Multiple threats and con-tributors to health asdimensions of onereality
Understanding of threatsto the integrity of therelationship (e.g., powerinequalities)
Understanding of poten-tial for conflict andabuse
Elements of effectivecommunication
Reflect on self and work
Recognize patient’s lifestory and its meaning
View health and illness aspart of humandevelopment
Attend fully to the patientAccept and respond to
distress in patient andself
Respond to moral andethical challenges
Facilitate hope, trust, andfaith
ListenImpart informationLearnFacilitate the learning of
othersPromote and accept
patient’s emotions
Importance of self-awareness, self-care,self-growth
Appreciation of thepatient as a wholeperson
Appreciation of thepatient’s life story andthe meaning of thehealth-illness condition
Respect for patient’s dig-nity, uniqueness, andintegrity (mind-body-spirit unity)
Respect for self-determination
Respect for person’s ownpower and self-healingprocesses
Importance of being openand nonjudgmental
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 14

in Table 1-8, including developing self-awareness;understanding the diverse knowledge base andskills of different practitioners; developing teamsand communities; and understanding the workingdynamics of groups, teams, and organizations thatcan provide resource services for the patient andfamily.24
Collaborative relationships entail shared plan-ning and action toward common goals with jointresponsibility for outcomes. There is a difference,though, between multidisciplinary care and inter-disciplinary care. Multidisciplinary care consists ofthe sequential provision of discipline-specific healthcare by various individuals. Interdisciplinary care,
Relationship-Centered Care 15
Table 1-7 Community–Practitioner Relationship: Areas of Knowledge, Skills, and Values
Area Knowledge Skills Values
Meaning of community
Multiple contributors tohealth within thecommunity
Developing andmaintaining communityrelationships
Effective community-based care
Various models ofcommunity
Myths and misperceptionsabout community
Perspectives from thesocial sciences, humani-ties, and systems theory
Dynamic change—demographic, political,industrial
History of community,land use, migration,occupations, and theireffect on health
Physical, social, and occu-pational environmentsand their effects onhealth
External and internalforces influencing com-munity health
History of practitioner-community relationships
Isolation of the health carecommunity from thecommunity-at-large
Various types of care, bothformal and informal
Effects of institutionalscale on care
Positive effects of continu-ity of care
Learn continuouslyParticipate actively in com-
munity developmentand dialogue
Critically assess the rela-tionship of health careproviders to communityhealth
Assess community andenvironmental health
Assess implications ofcommunity policyaffecting health
Communicate ideasListen openlyEmpower othersLearnFacilitate the learning of
othersParticipate appropriately in
community develop-ment and activism
Collaborate with otherindividuals andorganizations
Work as member of ateam or healingcommunity
Implement changestrategies
Respect for the integrity ofthe community
Respect for culturaldiversity
Affirmation of relevanceof all determinants ofhealth
Affirmation of the value ofhealth policy in commu-nity services
Recognition of the pres-ence of values that aredestructive to health
Importance of beingopen-minded
Honesty regarding the lim-its of health science
Responsibility to contribute healthexpertise
Respect for communityleadership
Commitment to work forchange
Source: Pew Health Professions Commission at the Center for the Health Professions, University of California, San Francisco, 1388Sutter Street, Suite 805, San Francisco, California 94109, (415) 476-8181.
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 15

however, also includes coordination, joint deci-sion making, communication, shared responsibil-ity, and shared authority.
Because the cornerstone of all therapeutic andhealing endeavors depends on the quality of therelationships formed among the practitioners car-ing for the patient, it is necessary for all practition-ers to understand and respect one another’s roles.Conventional and alternative practitioners need tolearn about the diversity of therapeutic and healingmodalities that they each use. In addition, conven-tional practitioners must be willing to integratecomplementary and alternative practitioners andtheir therapies in practice (i.e., acupuncture, herbs,aromatherapy, touch therapies, music therapy, folkhealers). Such integration requires learning aboutthe experiences of different healers, being open tothe potential benefits of different modalities, andvaluing cultural diversity. Ultimately, the effective-ness of collaboration among practitioners dependson their ability to share problem solving, goal set-ting, and decision making within a trusting, colle-
gial, and caring environment. Practitioners mustwork interdependently rather than autonomously,with each assuming responsibility and accountabil-ity for patient care.
In the next section the Theory of IntegralNursing is discussed. As you read about the fol-lowing Theory of Integral Nursing remember thatthe word integral and integrally informed will beuse often as this is a shift to a deeper level ofunderstanding about being human as related tothe four dimensions of reality. It is incorrect tosubstitute the word holistic as it is not the samething. Consider where you are now in your life—as a novice, intermediate, or expert nurse; youbring a wealth of experiences that inform you atthe professional and personal levels. Begin toexplore the integral process in your thinking,projects, and endeavors. Examine if your ap-proaches are reductionistic, narrow, or limited, orwhether you have an integral awareness and inte-gral understanding that includes the four per-spectives of reality that follow.
16 CHAPTER 1 INTEGRAL AND HOLISTIC NURSING: LOCAL TO GLOBAL
Table 1-8 Practitioner–Practitioner Relationship: Areas of Knowledge, Skills, and Values
Area Knowledge Skills Values
Source: Pew Health Professions Commission at the Center for the Health Professions, University of California, San Francisco, 1388Sutter Street, Suite 805, San Francisco, California 94109, (415) 476-8181.
Self-awareness
Traditions of knowledge inhealth professions
Building teams andcommunities
Working dynamics ofteams, groups, andorganizations
Knowledge of self
Healing approaches ofvarious professions
Healing approaches acrosscultures
Historical power inequitiesacross professions
Perspectives on team-building from the socialsciences
Perspectives on teamdynamics from thesocial sciences
Reflect on self and needsLearn continuously
Derive meaning fromothers’ work
Learn from experiencewithin healingcommunity
Communicate effectivelyListen openlyLearn cooperatively
Share responsibilityresponsibly
Collaborate with othersWork cooperativelyResolve conflicts
Importance of self-awareness
Affirmation and value ofdiversity
Affirmation of missionAffirmation of diversity
Openness to others’ ideasHumilityMutual trust, empathy,
supportCapacity for grace
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 16

THEORY OF INTEGRAL NURSING
Overview
The Theory of Integral Nursing is a grand theorythat presents the science and art of nursing. Itincludes an integral process, integral worldview,and integral dialogues that is praxis—theory inaction.1,2,26 Concepts specific to the Theory of Inte-gral Nursing are in italics throughout this chapter.Please consider these words as a frame of referenceand a way to explain what you have observed orexperienced with yourself and others. An integralprocess is defined as a comprehensive way to orga-nize multiple phenomenon of human experienceand reality from four perspectives: (1) the individ-ual interior (personal/intentional); (2) individualexterior (physiology/behavioral); (3) collectiveinterior (shared/cultural); and (4) collective exte-rior (systems/structures). Holistic nursing practiceis included (embraced) and transcended (goesbeyond) in this integral process.1,2,26 An integralworldview examines values, beliefs, assumptions,meaning, purpose, and judgments related to howindividuals perceive reality and relationships fromthe above four perspectives. Integral dialogues aretransformative and visionary exploration of ideasand possibilities across disciplines where thesefour perspectives are considered as equally im-portant to all exchanges, endeavors, and out-comes.1,2,26 With an increased integral awarenessand an integral worldview, nurses have new possi-bilities and ways to strengthen their capacities forintegral dialogues with each other and other disci-plines. We are more likely to raise our collectivenursing voice and power to engage in social actionin our professional role and work of service forsociety—locally to globally.
To decease further fragmentation in the nurs-ing profession the Theory of Integral Nursingincludes existing theoretical work in nursing thatbuilds on our solid holistic and multidimensionaltheoretical nursing foundation. This theory maybe used with other holistic nursing and nonnurs-ing caring concepts, theories, and research; it doesnot exclude or invalidate other nurse theoristswho have informed this theory (see Chapter 6 andthe Acknowledgements). This is not a freestanding
theory as it incorporates concepts from thephilosophies and various fields that include holis-tic, multidimensionality, integral, chaos, spiraldynamics, complexity, systems, and many otherparadigms.
An integral understanding allows us to morefully comprehend the complexity of humannature and healing; it assists nurses to bring tohealth care and society their knowledge, skills, andcompassion. The integral process and an integralworldview presents a comprehensive map andperspective related to the complexity of wholenessand how to simultaneously address the health andwell-being of nurses, the healthcare team, thepatients, families and significant others, thehealthcare system/structure, and the world.
The nursing profession asks nurses to wraparound “all of life” on so many levels with self andothers that we can often feel overwhelmed. Sohow do we get a handle on “all of life?” The ques-tion always arises “How can overworked nursesand student nurses use an integral approach orapply the Theory of Integral Nursing?” Theanswer is to start right now. By the time you finishreading this chapter you will find the answers tothe above questions. Be aware of healing, the coreconcept in this theory; it is the innate natural phe-nomenon that comes from within a person anddescribes the indivisible wholeness, the intercon-nectedness of all people, and all things.
Reflect on this clinical situation. Imagine thatyou are caring for a very ill patient who needstransporting to a radiology procedure. The currenttransportation protocol between the medical unitand the radiology department lacks continuity. Inthis moment shift your feelings and your interiorawareness (and believe it!) to: “I am doing the bestthat I can in this moment,” and “I have all the timeneeded to take a deep breath and relax my tightchest and shoulder muscles.” This helps you con-nect these four perspective as follows: (1) theinterior self (caring for yourself in this moment):(2) the exterior self (using a research-based relax-ation and imagery integral practice to change yourphysiology); (3) the self in relationship to others(shifting your awareness creates another way ofbeing with your patient and the radiology team
Theory of Integral Nursing 17
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 17

member); and (4) the relationship to the exteriorcollective of systems/structures (considering waysto work with the radiology team member anddepartment to improve a transportation proce-dure in the hospital). An integral worldview andapproach can help each nurse and student nurseincrease her or his self-awareness, as well as theawareness of how one’s self affects others—thepatient, family, colleagues, and the workplace andcommunity. As the nurse discovers her or his owninnate healing from within, one is able to modelself-care and how to release stress, anxiety, andfear that manifest each day in this human journey.All nursing curriculum can be mapped in the inte-gral quadrants discussed later (see the Applicationsection below) that teaches students to think inte-grally and to become aware of an integral perspec-tive and how these four perspectives create thewhole. They can also learn the importance of self-care at all times as faculty also remember that theyare role models and must model self-care andthese integral ideas.
Developing the Theory of IntegralNursing: Personal Journey
As a young nurse attending my first nursing theoryconference in the late 1960s, I was captivated bynursing theory and the eloquent visionary words ofthese theorists as they spoke about the science andart of nursing. This opened my heart and mind tothe exploration and necessity to understand and touse nursing theory. Thus, I began my professionalcommitment to address theory in all endeavors aswell as to increase my understanding of other dis-ciplines that could inform me at a deeper under-standing about the human experience. I realizedthat nursing was neither a “science” or “art” ofnursing, but both/and. From the beginning of mycritical care and cardiovascular nursing focus, Ilearned how to combine science and technologywith the art of nursing. For example, with a patientfollowing an acute myocardial infarction who washaving severe pain, I gave pain medication whilesimultaneously guiding her or him in a relaxationor imagery practice to enhance relaxation andrelease anxiety. I also experienced a difference inmyself when I used this approach to combine thescience and art of nursing.
In the late 1960s, I also began to study andattend workshops on holistic and mind-body-related ideas as well as read in other disciplinessuch as systems theory; quantum physics; integral,Eastern, and Western philosophy and mysticism,and more. I was also reading nurse theorists andother discipline theorists that informed my know-ing, doing, and being in caring, healing, andholism. (See Acknowledgments for specific nursetheorists.) My husband, an internist, who was alsocaring for critically ill patients and their families,was with me on this journey of discovery. As wecared for critically ill patients and their families,some of our greatest teachers, this allowed us toreflect on how to do blend the art of caring heal-ing modalities with the science of technology andtraditional modalities. I joined with a critical careand cardiovascular nursing colleague and soulmate, Cathie Guzzetta, PhD, RN, AHN-BC,FAAN, with whom I could also discuss these ideas.We began to write teaching protocols and give lec-tures in critical care courses as well as write text-books and articles with other contributors.
My husband and I both had health challenges—mine was postcorneal transplant rejection and myhusband’s challenge was blinding migraineheadaches. We both began to take courses relatedto body-mind-spirit therapies (biofeedback, relax-ation, imagery, music, meditation, and otherreflective practices) and began to incorporatethem into our daily lives. As we strengthened ourcapacities with self-care and self-regulationmodalities, our personal and professional philoso-phies and clinical practices changed. We took seri-ously teaching and integrating these modalitiesinto the traditional healthcare setting that today iscalled integrative and integral healthcare. Fromthis point to the present we have always foundmany professional and interdisciplinary healthcarecolleagues to discuss concepts, protocols, andapproaches for practice, education, research, andhealthcare protocols and policies.
As a founding member in 1981 of the AmericanHolistic Nurses Association (AHNA), and withLynn Keegan, PhD, RN, AHN-BC, FAAN, CathieGuzzetta, and many AHNA colleagues (see Chap-ter 2 and Acknowledgments), our collective holis-tic nursing endeavors were recognized as thespecialty of holistic nursing by the American
18 CHAPTER 1 INTEGRAL AND HOLISTIC NURSING: LOCAL TO GLOBAL
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 18

Nurses Association (ANA) in November 2006.The AHNA and ANA Holistic Nursing: Scope andStandards of Practice were published in June 2007.3
I believe that this important holistic specialty cannow be expanded by using an integral lens.
Beginning in 1992 in London during my Flo-rence Nightingale primary historical research ofstudying and synthesizing her original letters,army and public health documents, manuscripts,and books, I deepened my understanding of herrelevance for nursing as Nightingale was indeedan integralist as previous discussed. This led tomy Nightingale authorship4,5,10 and my collabora-tive Nightingale Initiate for Global Health and theNightingale Declaration,11 the first global nursingInternet signature campaign (see Acknowledge-ments). My professional mission now is to articu-late and use the integral process and integralworldview in my nursing and healthcare endeav-ors and to explore rituals of healing with many.1,2
My sustained nursing career focus with nursingcolleagues on wholeness, unity, and healing andmy Florence Nightingale scholarship have re-sulted in numerous protocols and standards forpractice, education, research, and healthcare pol-icy.My integral focus since 2000 and my manyconversations with Ken Wilber and the integralteam and other interdisciplinary integral col-leagues has led to my development of the Theoryof Integral Nursing at this time. It is exciting tosee other nurses expanding the holistic processand incorporating the integral model as well.
Theory of Integral Nursing Intentionsand Developmental Process
The intention (purpose) in a nursing theory is theaim of the theory. The Theory of Integral Nursinghas three intentions: (1) to embrace the unitarywhole person and the complexity of the nursingprofession and health care; (2) to explore thedirect application of an integral process and inte-gral worldview that includes four perspectives ofrealities—the individual interior and exterior andthe collective interior and exterior; and (3) toexpand nurses’ capacities as 21st-century Nightin-gales, health diplomats, and integral healthcoaches that are coaching for integral health—locally to globally. The Theory of Integral Nursing
develops the evolutionary growth processes,stages, and levels of humans development andconsciousness to move towards a comprehensiveintegral philosophy and understanding. This canassist nurses to more deeply map human capaci-ties that begin with healing to evolve to thetranspersonal self and connection with the Divine,however defined or identified, and their collectiveendeavors to create a healthy world.
The Theory of Integral Nursing developmentprocess at this time is to strengthen our 21st-century nursing endeavors and beyond so that wecan more easily expand personal awareness of ourholistic and caring healing knowledge and ap-proaches with traditional nursing and healthcare.Nursing and health care are fragmented. Col-laborative practice has not been realized becauseonly portions of reality are seen as being validwithin health care and society. Often there is alack of respect for each other. We also do not con-sistently listen to the pain and suffering thatnurses experience within the profession, nor dowe consistently listen to the pain and suffering ofthe patient and family members or our colleagues.Self-care is a low priority; time is not given or val-ued within practice settings to address basic self-care such as short breaks for personal needs andmeals, which is made worse by short staffing andovertime. Professional burnout is extremely high,and many nurses are very discouraged. Nurseretention is at a crisis level throughout the world.As nurses integrate an integral process and inte-gral worldview and use daily integral life practices,they will more consistently be healthy and modelhealth and understand the complexities withinhealing. This will then enhance nurses’ capacitiesfor empowerment, leadership, and being changeagents for a healthy world.
Integral Foundation and the Integral Model
The Theory of Integral Nursing adapts work ofKen Wilber (1949–), one of the most significantAmerican new-paradigm philosophers, tostrengthen the core concept of healing. Wilber’sintegral model is an elegant, four-quadrant modelthat has been developed over 35 years. In his eight-volume The Collected Works of Ken Wilber,27,28
Theory of Integral Nursing 19
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 19

Wilber synthesizes in his monumental achieve-ment the best known and most influential re-searchers, theorists, theories, and schools ofthought to show that no individual or disciplinecan determine reality or has all the answers.Many concepts within this integral nursing the-ory have been researched or are in very formativestages and exploration within integral medicine,integral healthcare administration, integral busi-ness, integral healthcare education, integral psy-chotherapy, integral coaching, and more.26-31
Within the nursing profession other nurses arealso exploring integral and related theories andideas.32-40 But as of yet, there is no theory ofnursing that has Nightingale’s philosophicalfoundation as an integralist combined with theintegral process and integral worldview. Whennurses consider the use of an integral lens theyare more likely to expand nurses’ roles in inter-disciplinary dialogues and to explore commonal-ities and to examine differences and how toaddress these across disciplines. Our challenge innursing is to increase our integral awareness aswe increase our nursing capacities, strengths, andvoices in all areas of practice, education,research, and healthcare policy.
Content, Context, and Process
To present the Theory of Integral Nursing, Bar-bara Barnum’sframework to critique a nursingtheory provides an organizing structure that ismost useful.41 Her approach, which examinescontent, context, and process, highlights what ismost critical to understand a theory, and itavoids duplication of explanations within thetheory. In the next section the Theory of IntegralNursing philosophical assumptions are pro-vided. The reader is encouraged to integrate theintegral process concepts and to experience howthe word integral expands one’s thinking andworldview. To delete the word integral or to sub-stitute the world holistic diminishes the impactof the expansiveness of the integral process andintegral worldview and its implications as previ-ously stated. The philosophical assumptions ofthe Theory of Integral Nursing are listed inTable 1-9.1,2
Content Components
Content of a nursing theory includes the subjectmatter and building blocks that give a theory form.It comprises the stable elements that are acted onor that do the acting. In the Theory of IntegralNursing, the subject matter and building blocks areas follows: (1) healing, (2) the meta-paradigm ofnursing, (3) patterns of knowing, (4) the fourquadrants that are adapted from Wilber’s integraltheory (individual interior [subjective, personal/intentional], individual exterior [objective, behav-
20 CHAPTER 1 INTEGRAL AND HOLISTIC NURSING: LOCAL TO GLOBAL
Table 1-9 Theory of Integral Nursing: PhilosophicalAssumptions
1. An integral understanding recognizes the wholenessof humanity and the world that is open, dynamic,interdependent, fluid, and continuously interactingwith changing variables that can lead to greatercomplexity and order.
2. An integral worldview is a comprehensive way toorganize multiple phenomena of human experienceand reality and identifies these phenomena as theindividual interior (subjective, personal), individualexterior (objective, behavioral), collective interior(intersubjective, cultural), and collective exterior(interobjective, systems/structures).
3. Healing is a process inherent in all living things; itmay occur with curing of symptoms, but it is notsynonymous with curing.
4. Integral health is experienced by individuals, and alsogroups, communities, nations, cultures, and ecosys-tems as wholeness with development towards per-sonal growth and expanding states of consciousnessto deeper levels of personal and collective under-standing of one’s physical, mental, emotional, social,spiritual, relational, sexual, and psycho-dynamicdimensions.
5. Integral nursing is founded on an integral worldview,using integral language and integral knowledge thatare enacted in these integral life practices and skills.
6. Integral nursing has the capacity to include all waysof knowing and knowledge development.
7. Integral nursing is applicable in any context, and itsscope includes all aspects of human experience.
8. An integral nurse is an instrument in the healingprocess and facilitates healing through her or hisknowing, doing, and being.
Source: Copyright © Barbara Dossey, 2007.
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 20

ioral], collective interior [intersubjective, cultural],and collective exterior [interobjective, systems/structures]); and (5) “all quadrants, all levels, alllines,” that are adapted from Wilber.26
Content Component #1: Healing
The first content component in the Theory of Inte-gral Nursing is healing, which is illustrated as a dia-mond shape and seen in Figure 1-3a.1,2,4 TheTheory of Integral Nursing enfolds from the cen-tral core concept of healing. It embraces the indi-vidual as an energy field that is connected with theenergy fields of all humanity and the world. Heal-ing is transformed when we consider four perspec-tives of reality in any moment: (1) the individualinterior (personal/ intentional), (2) individualexterior (physiology/ behavioral), (3) collectiveinterior (shared/cultural), and (4) collective exte-rior (systems/ structures). Using our reflectiveintegral lens of these four perspectives of realityassists us to more likely experience a unitary graspon the complexity that emerges in healing.
Healing includes knowing, doing, and being,and is a lifelong journey and process of bringingtogether aspects of oneself at deeper levels of har-mony and inner knowing leading toward integra-tion.1,2,4 This healing process places us in a spaceto face our fears, to seek and express self in its full-ness where we can learn to trust life, creativity,passion, and love. Each aspect of healing has equalimportance and value that leads to more complexlevels of understanding and meaning.
We are born with healing capacities. It is aprocess inherent in all living things. No one cantake healing away from life, although we often getstuck in our healing or forget that we possess itdue to life’s continuous challenges and perceivedbarriers to wholeness. Healing can take place at alllevels of human experience, butit may not occursimultaneously in every realm. In truth, healingwill most likely not occur simultaneously or evenin all realms, and yet, the person may still have aperception of healing having happened.42,43 Heal-ing is not predictable; it may occur with curing ofsymptoms, but it is not synonymous with curing.Curing may not always happen, but the potentialfor healing to occur is always present even untilone’s last breath. Intention and intentionality arekey factors in healing.43,44 Intention is the con-scious determination to do a specific thing or toact in a specific manner; it is the mental state ofbeing committed to, planning to, or trying to per-form an action.43,44 Intentionality is the quality ofan intentionally performed action.
Content Component #2: Meta-Paradigm of Nursing Theory
The second content component in the Theory ofIntegral Nursing is the recognition of the meta-paradigm in a nurse theory—nurse, person, health,and environment (society)—that is seen in Figure1-3b. These concepts are important to the Theoryof Integral Nursing because they are encompassedwithin the quadrants of human experience as seenin Content Component #4. Starting with healing atthe center, a Venn diagram surrounds healing andimplies the interrelated and interdependence andimpact of these domains as each informs and influ-ences the others; a change in one will create adegree of change in the others, thus impactinghealing at many levels.
An integral nurse is defined as a 21st-centuryNightingale engaged in social action and sacredactivism, and as a“health diplomat” and “integralhealth coach” that is “coaching for integralhealth.”5,13 As nurses strives to be integrallyinformed, they are more likely to move to a deeperexperience of a connection with the Divine orInfinite, however defined or identified. Integralnursing provides a comprehensive way to organize
Theory of Integral Nursing 21
Figure 1-3a Healing.Source: Copyright © Barbara Dossey.
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 21

multiple phenomenon of human experience in thefour perspectives of reality as previous described.The nurse is an instrument in the healing processwhere she or he brings one’s whole self into rela-tionship to the whole self of another or a group ofsignificant others that reinforces the meaning andexperience of oneness and unity.
A person is defined as an individual (patient/client, family members, significant others) whoengages with a nurse in a manner that is respectfulof a person’s subjective experiences about health,health beliefs, values, sexual orientation, and per-sonal preferences. It also includes an individualnurse who interacts with a nursing colleague,other healthcare team members, or a group ofcommunity members or other groups.
Integral health is the process through which wereshape basic assumptions and worldviews aboutwell-being and see death as a natural process ofliving. Integral health may be symbolically seen asa jewel with many facets that is reflected as a“bright gem” or a “rough stone” depending onone’s situation and personal growth that influencestates of health, health beliefs, and values.42,43 As
described by Don Beck,45 this jewel may also beseen as a spiral or as a symbol of transformation tohigher states of consciousness to more fullyunderstand the essential nature of our beingnessas energy fields and expressions of wholeness. Thisincludes evolving one’s state of consciousness tohigher levels of personal and collective under-standing of one’s physical, mental, emotional,social, and spiritual dimensions. This acknowl-edges the individual’s interior and exterior experi-ences and the shared collective interior andexterior experiences with others where authenticpower is recognized within each person.Diseaseand illness at the physical level may manifest formany reasons and variables. It is important not toequate physical health, mental health, and spiri-tual health as they are not the same thing. Theyare facets of the whole jewel of integral health.
An integral environment has both interior andexterior aspects. The interior environmentincludes the individual’s feelings, meaning, men-tal, emotional, and spiritual dimensions; it alsoincludes a person’s brainstem, cortex, and so onthat are an internal (inside) aspect of the exterior
22 CHAPTER 1 INTEGRAL AND HOLISTIC NURSING: LOCAL TO GLOBAL
Figure 1-3b Healing and Meta-Paradigm of Nursing.Source: Adapted from B. Carper (1978). Copyright © Barbara Dossey.
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 22

self. It also acknowledges the patterns that maynot be understood that may manifest related tovarious situations or relationships. This may berelated to living and nonliving people and things,such as a deceased relative, animal, or a lost pre-cious object through flashes of memories stimu-lated by a current situation (a touch may bringforth past memories of abuse or suffering).Insights gained through dreams and other reflec-tive practices that reveal symbols, images, andother connections also influence one’s interiorenvironment. The exterior environment includesobjects that can be seen and measured that arerelated to the physical and social in some form inany of the gross, subtle, and causal levels that arediscussed in Component #4.
Content Component #3: Patterns of Knowing
The third content component in the Theory ofIntegral Nursing is the recognition of the patternsof knowing in nursing as seen in Figure 1-3c.
These six patterns of knowing are personal,empirics, aesthetics, ethics, not knowing, andsociopolitical. As a way to organize nursingknowledge Carper,46 in her now classic 1978 arti-cle, identified the four fundamental patterns ofknowing (personal, empirics, ethics, aesthetics)followed by the introduction of the pattern of notknowing in 1993 by Munhall,47 and the pattern ofsociopolitical knowing by White in 1995.48 All ofthese patterns continue to be refined and reframedwith new applications and interpretations.48-58
These patterns of knowing assist nurses in bring-ing themselves into the full expression of beingpresent in the moment, to integrate aestheticswith science, and to develop the flow of ethicalexperience with thinking and acting. (As all pat-terns of knowing in the Theory of Integral Nurs-ing are superimposed on Wilber’s four quadrantsin Figure 1-1e and Figure 1-1f, these patterns willbe primarily be positioned as seen; however, theymay also appear in one, several, or all quadrantsand inform all other quadrants.)
Theory of Integral Nursing 23
Figure 1-3c Healing and Patterns of Knowing in Nursing.Source: Copyright © Barbara Dossey.
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 23

Personal knowing is the nurse’s dynamic processand awareness of wholeness that focuses on thesynthesis of perceptions and being with self.46,49,50
It may be developed through art, meditation,dance, music, stories, and other expressions of theauthentic and genuine self in daily life and nursingpractice.
Empirical knowing is the science of nursing thatfocuses on formal expression, replication, and val-idation of scientific competence in nursing educa-tion and practice.49,50 It is expressed in modelsand theories and can be integrated into evidence-based practice. Empirical indicators are accessedthrough the known senses that are subject todirect observation, measurement, and verification.
Aesthetic knowing is the art of nursing thatfocuses on how to explore experiences and mean-ing in life with self or another that includesauthentic presence, the nurse as a facilitator ofhealing, and the artfulness of a healing environ-ment.50,58 It is the combination of knowledge,experience, instinct, and intuition that connectsthe nurse with a patient or client in order toexplore the meaning of a situation about thehuman experiences of life, health, illness, anddeath. It calls forth resources and inner strengthsfrom the nurse to be a facilitator in the healingprocess. It is the integration and expression of allthe other patterns of knowing in nursing praxis.
Ethical knowing is the moral knowledge in nurs-ing that focuses on behaviors, expressions, anddimensions of both morality and ethics.49,50 Itincludes valuing and clarifying situations to createformal moral and ethical behaviors intersectingwith legally prescribed duties. It emphasizesrespect for the person, the family, and the commu-nity that encourages connectedness and relation-ships that enhance attentiveness, responsiveness,communication, and moral action.
Not knowing is the capacity to use healing pres-ence, to be open spontaneously to the momentwith no preconceived answers or goals to beobtained.47,56-61 It engages authenticity, mindful-ness, openness, receptivity, surprise, mystery, anddiscovery with self and others in the subjectivespace and the intersubjective space that allows fornew solutions, possibilities, and insights toemerge.
Sociopolitical knowing addresses the importantcontextual variables of social, economic, geo-graphic, cultural, political, historical, and otherkey factors in theoretical, evidence-based practiceand research.48,49 This pattern includes informedcritique and social justice for the voices of theunderserved in all areas of society along with pro-tocols to reduce health disparities.
Content Component #4: Quadrants
The fourth content component in the Theory ofIntegral Nursing, as shown in Figure 1-3d, exam-ines four perspectives for all known aspects ofreality, or expressed another way, it is how welook at and describe anything. The Theory of Inte-gral Nursing core concept of healing is trans-formed by adapting Ken Wilber’s integralmodel.26,29,30 Starting with healing at the center torepresent our integral nursing philosophy, humancapacities, and global mission, dotted horizontaland vertical lines are shown to illustrate that eachquadrant can be understood as permeable andporous, with each quadrant experience integrallyinforming and empowering all other quadrantexperiences. Within each quadrant we see “I,”“We,” “It,” and “Its”to represent four perspectivesof realities that are already part of our everydaylanguage and awareness. (When working with var-ious cultures it is important to know that withinmany cultures the “I” comes last or is never ver-balized or recognized as the focus is on the “we”and relationships. However, this development ofthe“I” and awareness of one’s personal values iscritical to a healthy nurse to decrease burnout andincrease nurse renewal and nurse retention.)
Virtually all human languages use first-, second-,and third-person pronouns. First person is “theperson who is speaking,” which includes pronounslike I, me, mine in the singular, and we, us, ours inthe plural. Second person means “the person who isspoken to,” which includes pronouns like you andyours. Third person is “the person or thing beingspoken about,” such as she, her, hers, he, him, his,or they, it, their, and its. For example, if I am speak-ing about my new car, “I” am first person, and“you” are second person, and the new car is thirdperson. If you and I are communicating, the word“we” is used to indicate that we understand each
24 CHAPTER 1 INTEGRAL AND HOLISTIC NURSING: LOCAL TO GLOBAL
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 24

other. “We” is technically first person plural, but ifyou and I are communicating, then you are secondperson and my first person are part of this extraor-dinary “we.” So we can simplify first,,second, andthird person as “I”, “we,” “it,” and “its.”26,29
These four quadrants show the four primarydimensions or perspectives of how we experiencethe world; these are represented graphically as theUpper-Left (UL), Upper-Right (UR), Lower-Left(LL), and Lower-Right (LR) quadrants. It is sim-ply the inside and the outside of an individual andthe inside and outside of the collective. It includesexpanded states of consciousness where one feels aconnection with the Divine and the vastness of theuniverse and the infinite that is beyond words.Integral nursing considers all of these areas in ourpersonal development and any area of practice,education, research, and healthcare policy—localto global. Each quadrant, which is intricately
linked and bound to each other, carries its owntruths and language. The specifics of the quad-rants are as follows and are shown in Table 1-10:
• Upper-Left (UL): In this “I” space (subjec-tive; the inside of the individual) can befound the world of the individual’s interiorexperiences. These are the thoughts, emo-tions, memories, perceptions, immediatesensations, and states of mind (imagination,fears, feelings, beliefs, values, esteem, cogni-tive capacity, emotional maturity, moraldevelopment, and spiritual maturity). Inte-gral nursing requires development of the “I.”
• Upper-Right (UR): In this “It” (objective; theoutside of the individual) space can be foundthe world of the individual’s exterior. Thisincludes the material body (physiology [cells,molecules, neurotransmitters, limbic system],
Theory of Integral Nursing 25
Figure 1-3d Healing and the Four Quadrants (I, We, It, Its).Source: Adapted with permission from Ken Wilber. http://www.kenwilber.com. Copyright © Barbara Dossey.
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 25

biochemistry, chemistry, physics), integralpatient care plans, skill development (health,fitness, exercise, nutrition etc.), behaviors,leaderships skills and integral life practices(see the Process and Integral Nursing Princi-ples section), and anything that we can touchor observe scientifically in time and space.Integral nursing with our nursing colleaguesand healthcare team members includes the“It” of new behaviors, integral assessment andcare plans, leadership and skills development.
• Lower-Left (LL): In this “ We” (intersubjec-tive; the inside of the collective) space can befound the interior collective of how we cancome together to share our cultural back-ground, stories, values, meanings, vision,language, relationships, and how to formpartnerships to achieve a healing mission.This can decrease our fragmentation and
enhance collaborative practice and deep dia-logue around things that really matter. Inte-gral nursing is built upon “We.”
• Lower-Right (LR): In this “Its” space (inter-objective; the outside of the collective) canbe found the world of the collective, exte-rior things. This includes social systems/structures, networks, organizational struc-tures, and systems (including financial andbilling systems in healthcare), informationtechnology, regulatory structures (environ-mental and governmental policies, etc.),and any aspect of the technological envi-ronment and in nature and the naturalworld. Integral nursing identifies the “Its” inthe structure that can be enhanced to createmore integral awareness and integral part-nerships to achieve health and healing—local to global.
26 CHAPTER 1 INTEGRAL AND HOLISTIC NURSING: LOCAL TO GLOBAL
Table 1-10 Integral Model and Quadrants
UPPER LEFT
INDIVIDUAL INTERIOR
(intentional/personal)
“I” space includes self and consciousness (self-care, fears, feelings, beliefs, values, esteem,
cognitive capacity, emotional maturity, moral development, spiritual maturity, personal
communication skills, etc.)
I
WE
COLLECTIVE INTERIOR
(cultural/shared)
“We” space includes the relationship to each other and the culture and worldview (shared
understanding, shared vision, shared meaning,shared leadership and other values, integral dialogues and communication/morale, etc.)
LOWER LEFT
UPPER RIGHT
INDIVIDUAL EXTERIOR
(behavioral/biological)
“It” space that includes brain and organisms (physiology, pathophysiology [cells, molecules, limbic
system, neurotransmitters, physical sensations], biochemistry, chemistry, physics, behaviors [skilldevelopment in health, nutrition, exercise, etc.])
IT
ITS
COLLECTIVE EXTERIOR
(systems/structures)
“Its” space includes the relation to social systems andenvironment, organizational structures and systems(in healthcare—financial and billing systems), educa-tional systems, information technology, mechanicalstructures and transportation, regulatory structures
(environmental and governmental policies, etc.)
LOWER RIGHT
Source: Ken Wilber, Integral Psychology: Consciousness, Spirit, Psychology, Therapy (Boston: Shambhala, 2000). Table adapted withpermission from Ken Wilber (http://www.kenwilber.com) by Barbara M. Dossey.
• Subjective• Interpretive• Qualitative
• Objective• Observable• Quantitative
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 26

On the outside of the Figure 1-3d, we see thatthe left-hand quadrants (Upper Left, Lower Left)describe aspects of reality as interpretive and qual-itative. In contrast, the right-hand quadrants(Upper Right, Lower Right) describe aspects ofreality as measurable and quantitative. When wefail to consider these subjective, intersubjective,objective, and interobjective aspects of realityalready described in each quadrant, this is whatleads our endeavors and initiatives to be frag-mented and narrow and where we often fail toreach identified outcomes and goals. The fourquadrants are a result of the differences and simi-larities in Wilber’s investigation of the manyaspects of identified reality.26-31 The modeldescribes the territory of our own awareness thatis already present within us and an awareness ofthings outside of us. These quadrants help us con-nect the dots of the actual process to more deeplyunderstand who we are and how we are related toothers and all things.
Content Component #5: AQAL (All Quadrants, All Levels)
The fifth content component in the Theory ofIntegral Nursing is the exploration ofWilber’s “allquadrants, all levels, all lines, all states, all types”or A-Q-A-L (pronounced ah-qwul), as seen inFigure 1-3e. These levels, lines, states, and typesare important elements of any comprehensivemap of reality. The integral model simply assistsus in further articulating and connecting all areas,awareness, and depth in these four quadrants.Briefly, these levels, lines, states, and types are asfollows:26,29
• Levels: Levels of development that becomepermanent with growth and maturity (e.g.,cognitive, relational, psychosocial, physical,mental, emotional, spiritual) that representsa level of increased organization or level ofcomplexity. These levels arealso referred toas waves and stages of development. Eachindividual possess the masculine and femi-nine voice or energy. Neither masculine orfeminine is higher or better; they are twoequivalent types at each level of conscious-ness and development.
• Lines: Developmental areas that are knownas multiple intelligences: cognitive line(awareness of what is); interpersonal line(how I relate socially to others); emotional/affective line (the full spectrum of emo-tions); moral line (awareness of what shouldbe); needs line (Maslow’s hierarchy ofneeds); aesthetics line (self-expression of art,beauty, and full meaning); self-identity line(who am I?);spiritual line (where spirit isviewed as its own line of unfolding, and notjust as ground and highest state); and valuesline (what a person considers most impor-tant; studied by Clare Graves and broughtforward by Don Beck45 in his Spiral Dynam-ics Integral that is beyond the scope of thischapter).
• States: Temporary changing forms of aware-ness: waking, dreaming, deep sleep, alteredmeditative states (due to meditation, yoga,contemplative prayer, etc.), altered states(due to mood swings, physiology, andpathophysiology shifts with disease, illness,seizures, cardiac arrest, low or high oxygensaturation, drug induced), peak experiences(triggered by intense listening to music,walks in nature, love making, mystical expe-riences such as hearing the voice of God orthe voice of a deceased person, etc.).
• Types: Differences in personality and mascu-line and feminine expressions and develop-ment (e.g., cultural creative types, personalitytypes, enneagram).
This part of the Theory of Integral Nursing, asshown in Figure 1-3e, starts with healing at thecenter surrounded by three increasing concentriccircles with dotted lines of the four quadrants.This aspect of the integral theory moves to higherorders of complexity through personal growth,development, expanded stages of consciousness(permanent and actual milestones of growth anddevelopment), and evolution. These levels orstages of development can also be expressed asbeing self-absorbed (such as a child or infant) toethnocentric (centers on group, community,tribes, nation) to worldcentric (care and concernfor all peoples regardless of race, color, sex, gender,
Theory of Integral Nursing 27
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 27
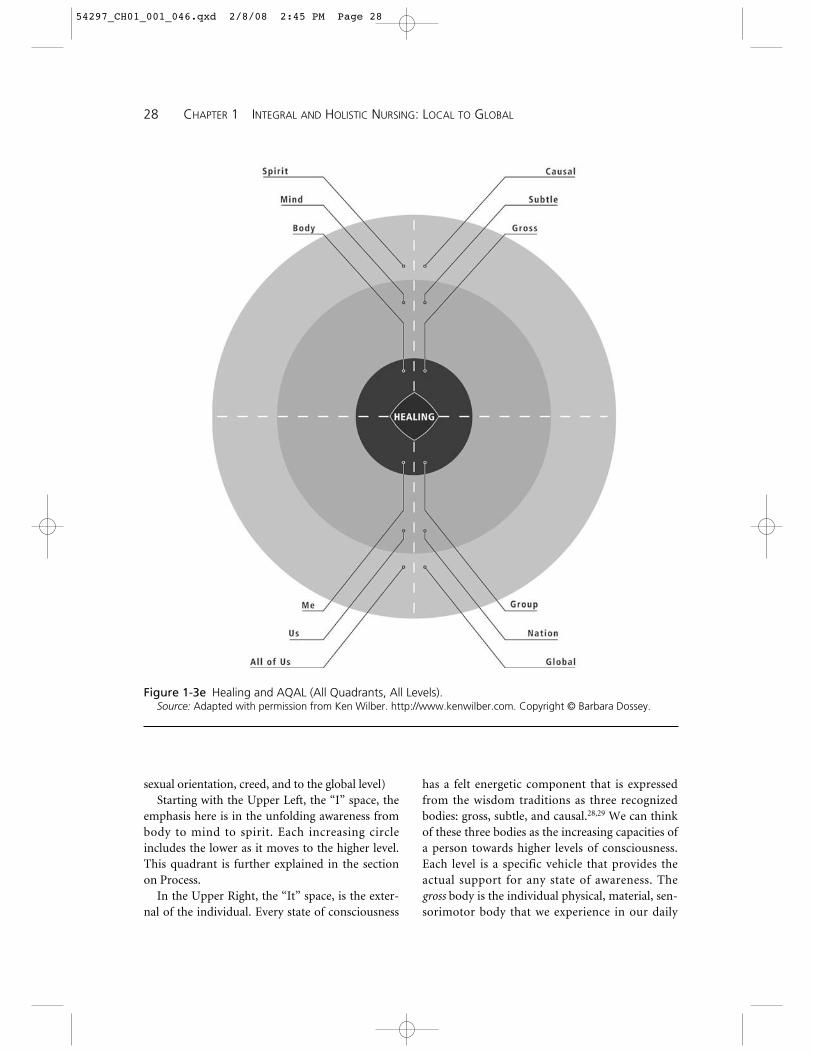
sexual orientation, creed, and to the global level)Starting with the Upper Left, the “I” space, the
emphasis here is in the unfolding awareness frombody to mind to spirit. Each increasing circleincludes the lower as it moves to the higher level.This quadrant is further explained in the sectionon Process.
In the Upper Right, the “It” space, is the exter-nal of the individual. Every state of consciousness
has a felt energetic component that is expressedfrom the wisdom traditions as three recognizedbodies: gross, subtle, and causal.28,29 We can thinkof these three bodies as the increasing capacities ofa person towards higher levels of consciousness.Each level is a specific vehicle that provides theactual support for any state of awareness. Thegross body is the individual physical, material, sen-sorimotor body that we experience in our daily
28 CHAPTER 1 INTEGRAL AND HOLISTIC NURSING: LOCAL TO GLOBAL
Figure 1-3e Healing and AQAL (All Quadrants, All Levels).Source: Adapted with permission from Ken Wilber. http://www.kenwilber.com. Copyright © Barbara Dossey.
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 28

activities. The subtle body occurs when we are notaware of the gross body of dense matter, but of ashifting to a light, energy, emotional feelings, andfluid and flowing images. Examples might be inour shift during a dream, during different types ofbody work, walks in nature, or other experiencesthat move us to a profound state of bliss. Thecausal body is the body of the infinite that isbeyond space and time. Causal also includes allaspects of Era III medicine and nonlocality whereminds of individuals are not separate in space andtime. When this is applied to consciousness, sepa-rate minds behave as if they are linked regardlessof how far apart in space and time they may be.Nonlocal consciousness may underlie phenome-non such as remote healing, intercessory prayer,telepathy, premonitions, as well as so-called mira-cles. Nonlocality also implies that the soul doesnot die with the death of the physical body—hence, immortality forms some dimension of con-sciousness.18,21 Nonlocality can also be bothupper- and lower-quadrant phenomena.
The Lower Left, the “We” space, is the interiorcollective dimension of individuals that cometogether. The concentric circles from the centeroutward represent increasing levels of complexityof our relational aspect of shared cultural values,as this is where teamwork and the interdisciplin-ary and transpersonal disciplinary developmentoccurs. The inner circle represents the individuallabeled as me; the second circle represents alarger group labeled us; the third circle is labeledas all of us to represent the largest group con-sciousness that expands to all people. These lasttwo circles may includes not only people, butanimals, nature, and nonliving things that areimportant to individuals.
The Lower Right, the “Its” space, the exteriorsocial system and structures of the collective, isrepresented with concentric circles. An examplewithin the inner circle might be a group of health-care professionals in a hospital clinic or departmentor the complex hospital system and structure. Themiddle circle expands in increased complexity toinclude a nation; the third concentric circle repre-sents even greater increased complexity to theglobal level where the health of all humanity andthe world are considered. It is also helpful to
emphasize that these groupings are the physicaldynamics such as the working structure of a groupof healthcare professionals versus the relationalaspect that is a lower-left aspect, and the technicaland informatics structure of a hospital or a clinic.
Integral nurses strive to integrate concepts andpractices related to body, mind, and spirit (the alllevels) in self, culture, and nature (“all quadrants”part). The individual interior and exterior— “I”and “It”—as well as the collective interior andexterior—“We” and “Its”—must be developed,valued, and integrated into all aspects of cultureand society. The AQAL integral approach suggeststhat we consciously touch all of these areas and doso in relation to self, to others, and the naturalworld. Yet to be integrally informed does notmean that we have to master all of these areas; wejust need to be aware of them and choose to inte-grate integral awareness and integral practices.Because these areas are already part of our being-in-the-world and can’t be imposed from the out-side (they are part of our makeup from theinside), our challenge is to identify specific areasfor development and find new ways to deepen ourdaily integral life practices.
Wilber uses the term holon to describe any-thing that is itself whole or part of some otherwhole that creates structures from the very small-est to the larger of increasing complexity.26 Theupper half of the model represents the individualholons or the “micro world.” The lower quad-rants represent the social or communal holons orthe “macro world.”These holons creates a hol-archy of natural evolutionary processes. As oneprogresses up a holarchy, the lower levels ofholons are transcended and included and thus arefoundational. All of the entities or holons in theRight-Hand quadrants possess simple location.These are things that are perceived with oursenses such as rocks, villages, organisms, ecosys-tems, and planets. However, none of the entitiesor holons in the Left-Hand quadrants possesssimple location. One cannot see feelings, con-cepts, states of consciousness, or interior illumi-nation. They are complex experiences that exist inemotional space, conceptual space, spiritual space,and in our mutual understanding space. Thedevelopment of one’s individual consciousness as
Theory of Integral Nursing 29
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 29

part of self-care is primary to the development ofall other quadrants and integral thinking, applica-tion, and integration.
Structure
The structure of the Theory of Integral Nursingis seen in Figure 1-3f. All content componentsare overlayed together to create a mandala tosymbolize wholeness. Healing is placed at thecenter, then the meta-paradigm of nursing (inte-gral nurse, person, integral health, integral envi-ronment), the patterns of knowing (personal,empirics, aesthetics, ethics, not knowing,sociopolitical), the four quadrants (subjective,objective, intersubjective, interobjective), and all
quadrants and all levels of growth, development,and evolution. (Note: Although the patterns ofknowing are superimposed as they are in thevarious quadrants, they can also fit into otherquadrants).
Using the language of Ken Wilber and DonBeck and his Spiral Dynamics Integral, individualsmove through primitive, infantile consciousnessto an integrated language that is considered first-tier thinking.26,45 As they move up the spiral ofgrowth, development, and evolution and expandtheir integral worldview and integral conscious-ness, they move into what is considered second-tierthinking and participation. This is a radical leapinto holistic, systemic, and integral modes of con-sciousness. Wilber also expands to a third-tier of
30 CHAPTER 1 INTEGRAL AND HOLISTIC NURSING: LOCAL TO GLOBAL
Figure 1-3f Theory of Integral Nursing (Healing, Meta-Paradigm, Patterns of Knowing in Nursing, FourQuadrants, and AQAL).
Source: Adapted with permission from Ken Wilber. http://www.kenwilber.com. Copyright © Barbara Dossey.
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 30

stages of consciousness that addresses an evendeeper level of transpersonal understanding that isbeyond the scope of this chapter.31
Context
Context in a nursing theory is the environmentin which nursing acts occur and the nature ofthe world of nursing. In an integral nursingenvironment the nurse strives to be an integral-ist, which means that she or he strives to be inte-grally informed and is challenged to furtherdevelop an integral worldview, integral life prac-tices, and integral capacities, behaviors, and skills.An integral nurse values, articulates, and modelsthe integral process and integral worldview, aswell as integral life practices and self-care in nurs-ing practice, education, research, and healthcarepolicies. The term nurse healer is used to describea nurse as an instrument in the healing processand a major part of the exterior healing environ-ment of a patient, family, or another. Nurses assistand facilitate individuals with accessing their ownhealing process and potentials; the nurses do notdo the actual healing. An integral nurse also rec-ognizes self as part of the exterior healing envi-ronment interacting with a person, family, orcolleague and enters into a shared experience (orfield of consciousness) that promotes healingpotentials and an experience of well-being.
A key concepts in an integral healing environ-ment, both interior and exterior, is meaning,which addresses that which is indicated, referredto, or signified.19,62 Philosophical meaning is relatedto one’s view of reality and the symbolic connec-tions that can be grasped by reason. Psychologicalmeaning is related to one’s consciousness, intu-ition, and insight. Spiritual meaning is related tohow one deepens personal experience of a connec-tion with the Divine, or whatever mechanism ormodalities are used by an individual to feel a senseof oneness, belonging, and feeling of connectionin this human journey of life.
Process
Process in a nursing theory is the method bywhich the theory works. An integral healing
process contains both nurse processes and pa-tient, family, and healthcare workers processes(individual interior and individual exterior), andcollective healing processes of individuals and ofsystems/structures (collective interior and exte-rior). This is the understanding of the unitarywhole person interacting in mutual process withthe environment.
There are many opportunities to increase ourintegral awareness, application, and understand-ing each day. Reflect on all that you do each day inyour work and life—analyzing, communicating,listening, exchanging, surveying, involving, syn-thesizing, investigating, interviewing, mentoring,developing, creating, researching, teaching, andcreating new schemes for what is possible. Beforelong you will realize how all these four quadrantsand realities fit together. You will also discover ifyou are completely missing a quadrant, thus animportant part of reality. As we address and valuethe individual interior and exterior, the “I” and“It,” as well as the collective interior and exterior,the “We” and “Its,” a new level of integral under-standing emerges, and we may find that there isalso more balance and harmony each day. We alsodiscover that by incorporating the integral nursingprinciples discussed next we may assist others todiscover their own healing path. The reader isreferred to Figure 1-3f and Table 1-10 for specificscomponents of each quadrant. Figure 1-4 providesexamples of Florence Nightingale quotes as relatedto each integral nursing principle. (Note: This sec-tion is adapted from the author’s previous coau-thored work.)5
Integral Nursing Principle #1: NursingRequires Development of the “I”
Integral Nursing Principle #1 recognizes the inte-rior individual “I” (subjective) space. Each of usmust valued the importance of exploring one’shealth and well-being starting with our own per-sonal exploration and development on many levels.
Nightingale saw nursing first as a calling thatwas very individual and personal. Throughout herlife and nursing career she reflected carefully onher own thoughts, motives, and desires, as well asher own knowledge, skills, and conduct. In her1888 address she wrote: “Nursing work must be
Theory of Integral Nursing 31
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 31

quiet work—An individual work—Anything elseis contrary to the whole realness of the work.Where am I, the individual, in my utmost soul?What am I, the inner woman [man], called ‘I’?—That is the question.”63 It is this developmentof the individual “I” that supports each nurse inhow to deeply understand one’s interior as well ashow to develop the qualities of nursing presence,the aesthetic knowing of nursing as art, and muchmore. As Nightingale wrote in 1868: “Nursing isan art; and if it is to be made an art, it requires asexclusive a devotion, as hard a preparation, as anypainter’s or sculptor’s work; for what is the havingto do with dead canvas or cold marble, comparedwith having to do with the living spirit—the tem-ple of God’s spirit? It is one of the Fine Arts; I hadalmost said, the finest of the Fine Arts.”64
As nurses continually address their stress,burnout, suffering, and soul pain as discussed inthe next principle, this can assist us to understandthe necessity of personal healing and self-caredirectly related to nursing as art where we develop
qualities of nursing presence and inner reflection.Nurse presence is also a way of approaching a per-son that respects and honors the person’s essence;it is relating in a way that reflects a quality of“being with” and “in collaboration with” as dis-cussed in the next principle.56-61 Our own innerwork also helps us to hold deeply a consciousawareness of our own roles in creating a healthyworld.We recognize the importance of addressingone’s own shadow that is described by Jung65 as acomposite of personal characteristics and poten-tials that have been denied expression in life andof which a person is unaware; the ego denies thecharacteristics because they are in conflict andincompatible with a person’s chosen consciousattitude.
In this “I” space integral self-care is valued,which means that integral reflective practices areintegrated and can be transformative in our devel-opmental process. We become more integrallyconscious in our knowing, doing, and being in allaspects of our personal and professional endeav-
32 CHAPTER 1 INTEGRAL AND HOLISTIC NURSING: LOCAL TO GLOBAL
Figure 1-4 Florence Nightingales’s Integral Ideas.Source: Used with permission from the Nightingale Initiative for Global Health, (Washington, DC and Ottawa,
Canada, 2007) and B. M. Dossey, L. C. Selanders, D. M. Beck, and A. Attewell, Florence Nightingale Today: Healing,Leadership, Global Action (Silver Spring, MD: NursesBooks.Org, 2005).
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 32

ors. Mindfulness is the practice of giving attentionto what is happening in the present moment suchas our thoughts, feelings, emotions, and sensa-tions. To cultivate the capacity of mindfulness,practices one may include mindfulness medita-tion, centering prayer, and other reflective practicesuch as journaling, dream interpretation, art,music, or poetry that leads to an experience ofnonseparateness and love; it involves developingthe qualities of stillness and being present forone’s own suffering, which will also allow for fullpresence when with another.
In our personal process, we recognize consciousdying where time and thought is given to contem-plate one’s own death. Through a reflective prac-tice one rehearses and imagines one’s final breathto practice preparing for one’s own death. Thisintegral practice prepares us to not be so attachedto material things and spending so much timethinking about the future but living in thismoment as often as we can and to live fully untildeath comes. We are more likely to participateand fully engage with deeper compassion in thedeath process with others and ultimately with self.Death is seen as the mirror in which the entiremeaning and mystery of life is reflected—themoment of liberation. Within an integral perspec-tive the state of transparency, the understandingthat there is no separation between our practiceand our everyday life, is recognized.1,2,60,61 This is amature practice that is wise and empty of a sepa-rate self.
Integral Nursing Principle #2: Nursing Is Built upon “We”
Integral Nursing Principle #2 recognizes theimportance of the “We” (intersubjective) space.Within nursing, health care, and society, there ismuch suffering, moral suffering, moral distress,and soul pain as seen in Table 1-11.5,60,61 We areoften called upon to “be with” these difficulthuman experiences and to use our nursing pres-ence. Our sense of “We” supports us to recognizethe phases of suffering—“mute” suffering,“expressive” suffering, and “new identity” in suf-fering.60,61 When we feel alone, as nurses, we expe-rience mute suffering; this is an inability toarticulate and communicate with others one’s
own suffering. Our challenge in nursing is to moreskillfully enter into the phase of “expressive” suf-fering where sufferers seek language to expresstheir frustrations and experiences such as in shar-ing stories in a group process. Outcomes of thisexperience often move toward new identity in suf-fering through new meaning-making where onemakes new sense of the past, interprets new mean-ing in suffering, and can envision a new future. Ashift in one’s consciousness allows for a shift inone’s capacity to be able to transform her or hissuffering from causing distress to finding the somenew truth and meaning of it. As we create timesfor sharing and giving voice to our concerns, newlevels of healing may happen.
Nightingale consistently realized the value ofcollaborating well with others, especially nursingcolleagues. She focused upon what “we” as nursescan do together as a team. She saw that sustainablenursing practice constantly requires strong nurs-ing teamwork as expressed in 1883, “Let us run
Theory of Integral Nursing 33
Table 1-11 Suffering, Moral Suffering, Moral Distress,and Soul Pain
Suffering: An individual’s story around pain where thesigns of suffering may be physical, mental, emotional,social, behavioral, and/or spiritual; it is an anguishexperienced—internal and external—as a threat toone’s composure, integrity, and the fulfillment ofintentions.
Moral suffering: Occurs when an individual experi-ences tensions or conflicts about what is the right thingto do in a particular situation; it often involves thestruggle of finding a balance between competing inter-est or values.
Moral distress: Occurs when an individual is unable totranslate moral choices into moral actions and whenprevented by obstacles, either internal or external, fromacting upon them.
Soul pain: The experience of an individual who hasbecome disconnected and alienated from the deepestand most fundamental aspects of one’s self.
Source: Used with permission. J. Halifax, B.M. Dossey, andC.H. Rushton, Being With Dying: Compassionate End-of-LifeTraining Guide (Santa Fe, NM: Prajna Mountain Press, 2007).Adapted from A. Jameston, Nursing Practice: The Ethical Issues(Englewood Cliffs, NJ: Prentice Hall, 1984), and M. Kearney,Mortally Wounded, (New York: Scribner, 1996).
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 33

the race where all may win, rejoicing in their suc-cesses, as our own, and mourning their failures,wherever they are as our own. . . . We are all oneNurse. The very essence of all good organizationsis, that everybody should do her [or his] ownwork in such a way as to help and not hinder everyone else’s work.”66
An integral nurse considers transpersonaldimensions. This means that interactions withothers move from conversations to a deeper dia-logue that goes beyond the individual ego; itincludes the acknowledgment and appreciationfor something greater that may be referred to asspirit, nonlocality, unity, or oneness.1,2,21 Trans-personal dialogues contain an integral worldviewand recognize the role of spirituality that is thesearch for the sacred or holy that involves feelings,thoughts, experiences, rituals, meaning, value,direction, and purpose as valid aspects of the uni-verse. Spirituality is a unifying force of a personwith all that is—the essence of beingness andrelatedness that permeates all of life and is mani-fested in one’s knowing, doing, and being; it isusually, though not universally, considered theinterconnectedness with self, others, nature, andGod/LifeForce/Absolute/Transcendent. From anintegral perspective, spiritual care is an interfaithperspective that takes into account dying as adevelopmental process and natural human pro-cess that emphasizes meaningfulness and humanand spiritual values.1,2,60,61 Religion is recognizedas the codified and ritualized beliefs, behaviors,and rituals that take place in a community of like-minded individuals involved in spirituality. Ourchallenge is to enter into deep dialogue to morefully understand religions different than our own sothat we may be tolerant where there are differences.
In this “We” space nurses comes together andare conscious of sharing their worldviews, beliefs,priorities, and values related to working togetherin ways to enhance integral self-care and integralhealth care. Deep listening is valued; this is beingpresent and focused with intention to understandwhat another person is expressing or not express-ing. Bearing witness to others, the state achievedthrough reflective and mindfulness practices, isalso valued.1,2,60,61 Through mindfulness one isable to achieve states of equanimity, the stability of
mind that allows us to be present with a good andimpartial heart no matter how beneficial or diffi-cult the conditions; it is being present for the suf-ferer and suffering just as it is while maintaining aspacious mindfulness in the midst of life’s chang-ing conditions.60,61 Compassion is bearing witnessand loving kindness, which is manifest in the faceof suffering. The realization of the self and anotheras not being separate are experienced; it is the abil-ity to open one’s heart and be present for all levelsof suffering so that suffering may be transformedfor others, as well as for the self.A useful phrase toconsider is “I’m doing the best that I can.”60 Com-passionate care assists us in living as well as whenbeing with the dying person, the family, and oth-ers. We can touch the roots of pain and becomeaware of new meaning in the midst of pain, chaos,loss, and grief.
Integral action is the actual practice and processthat creates the condition of trust where a plan ofcare is cocreated with the patient, and care can begiven and received. Full attention and intention tothe whole person, not merely the current present-ing symptoms, illness, crisis, or tasks to be accom-plished, reinforces the person’s meaning andexperience of community and unity. Engagementbetween an integral nurse and a patient and thefamily or with colleagues is done in a respectfulmanner; each patient’s subjective experience abouthealth, health beliefs, and values are explored. Wedeeply care for others and recognize our own mor-tality and that of others.
The integral nurse uses intention, which is theconscious awareness of being in the presentmoment with self or another person to help facili-tate the healing process; it is a volitional act oflove.60 An awareness of the role of intuition is alsorecognized, which is the perceived knowing ofevents, insights, and things without a conscioususe of logical, analytical processes; it may beinformed by the senses to receive information.Intuition is a type of experience of sudden insightinto a feeling, a solution, or problem where timeand things fit together in a unified experience suchas understanding about pain and suffering, or amoment in time with another. This is an aspectwithin the pattern of unknowing. Integral nursesrecognize love as the unconditional unity of self
34 CHAPTER 1 INTEGRAL AND HOLISTIC NURSING: LOCAL TO GLOBAL
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 34

with others.This love then generates loving kind-ness, theopen, gentle, and caring state of mindful-ness that assist one’s with nursing presence.
There is an awareness of integral communicationthat is a free flow of verbal and nonverbal inter-change between and among people and pets andsignificant beings such as God/LifeForce/Absolute/Transcendent. This type of sharing leads to explo-rations of meaning and ideas of mutual under-standing and growth and loving kindness.
Integral Nursing Principle #3: “It” Is About Behavior and SkillDevelopment
Integral Nursing Principle #3 recognizes theimportance of the individual exterior “It” (objec-tive) space. n this “It” space of the individual exte-rior each person develops and integrates her or hisintegral self-care plan. This includes skills, behav-iors, and action steps to achieve a fit body and toconsider body strength training and stretching, aswell as the conscious eating of healthy foods. It isalso modeling integral life skills. For the integralnurse and patient this is also the space where the“doing to” and “doing for” occurs. However, theintegral nurse also combines her or his nursingpresence with nursing acts to assist the patient toaccess personal strengths, to release fear and anxi-ety, and to provide comfort and safety. There isthe awareness of conscious dying to assist thedying patient who wishes to have minimal med-ication and treatment to stay as alert as possiblewhile receiving comfort care until she or he makestheir death transition.
Nightingale saw nursing as an integral and spiri-tual practice where each nurse blends her or hisknowledge in combination with her or his ongoingobservations, to develop and refine one’s own nurs-ing practice—to continually combine the externalobservations of the body and behaviors and, thus,to develop new skills and behaviors. About thisdynamic, Nightingale eloquently observed andwrote in 1876:
When we obey all God’s laws as to clean-liness, fresh air, pure water, good habits,good dwellings, good drains, food anddrink, work and exercise, health is the
result: when we disobey, sickness.110,000 lives are needlessly sacrificedevery year in this kingdom by our dis-obedience, and 22,000 people are need-lessly sick all year round. And why?Because we will not know, will not obeyGod’s simple health laws. No epidemiccan resist thorough cleanliness and freshair.67
Within this integral nursing principle, integralnurses with nursing colleagues and healthcareteam members compile the data around physiolog-ical and pathophysiological assessment, nursingdiagnosis, outcomes, and plans of care (includingmedications, technical procedures, monitoring,treatments, protocols, implementation, and evalu-ation). This is also the space that includes patienteducation and evaluation. Integral nurses cocreateplans of care with patients when possible combin-ing caring-healing interventions and modalitiesand integral life practices that can interface andenhance the success of traditional medical and sur-gical technology and treatment. Some commoninterventions are relaxation, music, imagery, mas-sage, touch therapies, stories, poetry, healing envi-ronment, fresh air, sunlight, flowers, soothing andcalming pictures, pet therapy, and more.
Integral Nursing Principle #4: “Its” Is Systems and Structures
Integral Nursing Principle #4 recognizes theimportance of the exterior collective “Its” (inter-objective) space. In this “Its” space integral nursesand the healthcare team come together to examinetheir work, their priorities, use of technologies,and any aspect of the technological environment.They also create exterior healing environmentsthat incorporate nature and the natural worldwhen possible such as with outdoor and indoorhealing gardens, use of green materials with sooth-ing colors, and sounds of music and nature. Inte-gral nurses identify how they might work togetheras an interdisciplinary team to deliver more effec-tive patient care and coordination of care.
Nightingale saw nursing as a profession wherecontinual progress with self and others requiredattention and wrote about this in 1897:
Theory of Integral Nursing 35
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 35

Nursing takes a whole life to learn.Wemust make progress in it every year . . . Ithas been recorded that the three princi-ples which represent the deepest wantsof human nature, both in the East andthe West, are the principles of discipline,of religion (or the tie to God) of content-ment. . . . Nursing is not an adventure, assome have now supposed: “Where foolsrush in where angels fear to tread.”It is avery serious, delightful thing, like life,requiring training, experience, devotionnot by fits and starts, patience, a powerof accumulating, instead of losing—allthese things.We are only on the thresh-old of training.68
Application
This section offers examples of how to apply theTheory of Integral Nursing to practice, education,research, healthcare policy, and global nursing.
Practice. The Theory of Integral Nursing can beused by a nurse in any clinical situation to exploreaspects of integral awareness within all quadrants.The following example illustrates this point. Fol-lowing a shopping trip with her husband anddaughter, a woman had a seizure as she sat in hercar. She lost consciousness but regained a con-scious and alert state within several minutes. Thehusband immediately drove her to an emergencyroom. Which is more important in this situation?Is it the patient’s brain (Upper Right—neuralpathways and brain seizure focal areas) or thepatient’s and family’s mind (Upper Left—emo-tions, meaning, thoughts, perceptions, fears)? Oris it the nurse (Upper Left) or the nurse with theneurologist working together (Lower Left) or theemergency room (Lower Right) more important?
Using an integral approach, the answer is thatall of these questions are equally important to pre-vent this individual from further seizures andpotential complications. When all quadrants areaddressed a collaborative, integral treatment plancan be developed. It is also important to ensurethat the patient and the family are kept aware of
what is happening, and the patient flow in theemergency room is kept at a safe and effectivepace. Each quadrant represents an equal onefourth of reality, of the totality of our being andexistence. This model helps us touch and link allaspects of reality, including the importance of thenurse addressing her or his own needs.
An another example of use of the Theory ofIntegral Nursing principles and the integralprocess is Diane Pisanos,69 RNC, MS, NNP, whointegrates these ideas to organized her life andhealth coaching practice as seen in Figure 1-5.Another examples is Linda Bark,70 PhD, RN,MCC,who uses the integral model in her As OneIntegral Coaching70 and holistic nursing practice.
Education. The Theory of Integral Nursing can as-sist educators to be aware of all quadrants whileorganizing and designing curriculum,34 continuingeducation courses, health education presentations,teaching guides, and protocols. In most curricu-lums there is minimal focus on the individual sub-jective “I” and the collective intersubjective “We”;the emphasis is on passing an examination orlearning a new skill or procedure; thus, the learneronly retains small portions of what is taught.Before teaching any technical skills, the instructormight guide a student or patient in a relaxationand imagery rehearsal of the event to encouragethe student to be in the present moment.
The reader is referred to Chapter 35 and thework of Cynthia Barrere, PhD, RN, AHN-BC, andher nurse educators colleagues who use the The-ory of Integral Nursing in their undergraduatecurriculum. Darlene Hess,71 PhD, NP, AHN-BC,uses the Theory of Integral Nursing in her BrownMountain Visions consulting practice to design anRN-to-BSN curriculum as seen in Table 1-12.Hess also uses the integral process in her privatepractice. These Theory of Integral Nursing princi-ples and the integral model are being used to orga-nize an eight-day intensive integral end-of-lifecare professional training program.60,61 This train-ing program balances didactic presentations andexperiential group process work. For every 90minutes of didactic, there is a related 90 minutesof experiential integral process practices that rein-
36 CHAPTER 1 INTEGRAL AND HOLISTIC NURSING: LOCAL TO GLOBAL
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 36

forces the didactic. This also helps with the trueretention and learning of knowledge.
Research. The Theory of Integral Nursing can assistnurses to consider the importance of qualitativeand quantitative research.37,38,72 Often among scien-tists, researchers, and educators there are argu-ments as to whether qualitative or quantitativeresearch is more important. Wilber often uses theterm flatland thinking and approaches to describethe thinking of individuals who use a reductionisticperspective that can be situated in any quadrant, orwhen they try to explain all of both the interior andexterior dimensions through only quantitativemethodologies with a focus on empirical data.28
Our challenges in integral nursing are to considerthe findings from both qualitative and quantitativedata and always consider triangulation of datawhen appropriate. We must always value introspec-tive, cultural, and interpretive experiences, andexpand our personal and collective capacities of
consciousness as evolutionary progression towardsachieving our goals. In other words, knowledgedoes emerge from all four quadrants.
Healthcare Policy. The Theory of Integral Nursingcan guide us to consider many areas related tohealthcare policy. Compelling evidence in all of thehealthcare professions shows that the origins ofhealth and illness cannot be understood by focusingonly on the physical body. Only by expanding theequations of health, exemplified by an integralapproach or an AQAL approach to include our entirephysical, mental, emotional, social, and spiritualdimensions and interrelationships, can we accountfor a host of health events. Some of these include, forexample, the correlations between poor health andshortened life span; job dissatisfaction and acutemyocardial infarction; social shame and severe ill-ness; immune suppression and increased death ratesduring bereavement; improved health and longevityas spirituality and spiritual awareness is increased.
Theory of Integral Nursing 37
Figure 1-5 Integral Coaching Model.Used with permission. Copyright © Diane Pisanos, RNC, MS, AHN-BC, NNP, Life & Health Coach, Consultant,
Denver, CO.
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 37
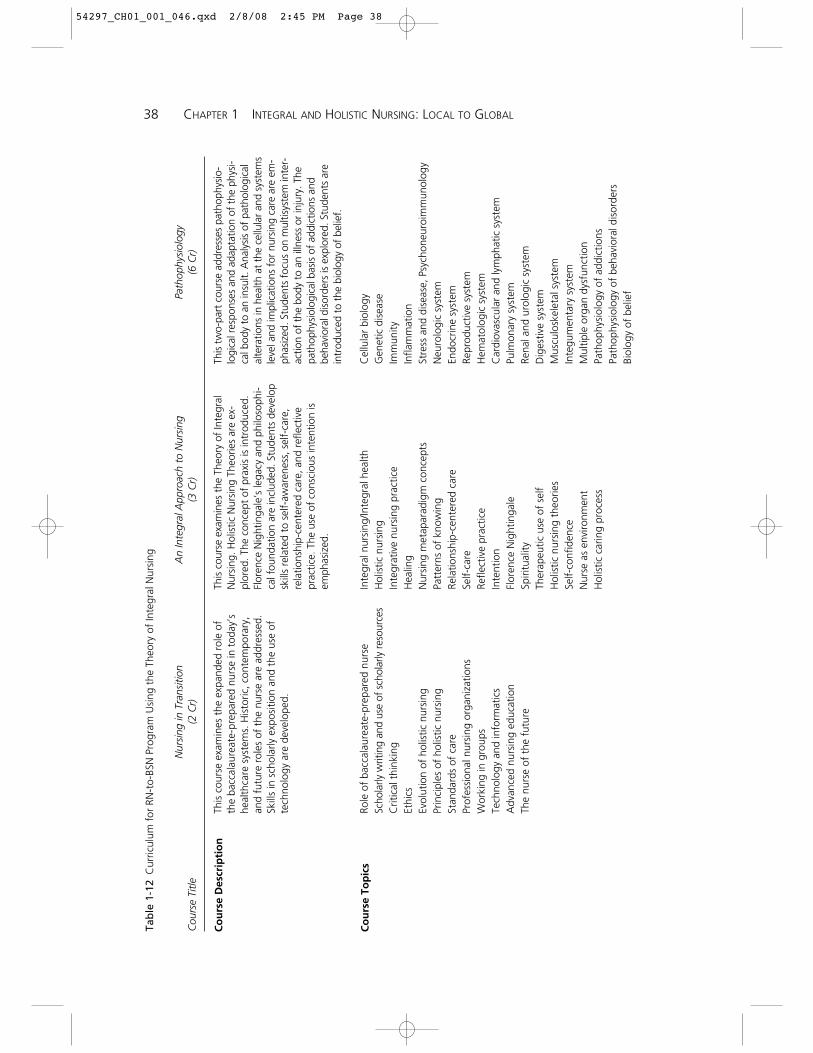
38 CHAPTER 1 INTEGRAL AND HOLISTIC NURSING: LOCAL TO GLOBAL
Tab
le 1
-12
Cur
ricul
um f
or R
N-t
o-BS
N P
rogr
am U
sing
the
The
ory
of In
tegr
al N
ursi
ng
Nur
sing
in T
rans
ition
An
Inte
gral
App
roac
h to
Nur
sing
Path
ophy
siol
ogy
Cou
rse
Title
(2 C
r)(3
Cr)
(6 C
r)
This
cou
rse
exam
ines
the
exp
ande
d ro
le o
fth
e ba
ccal
aure
ate-
prep
ared
nur
se in
tod
ay’s
heal
thca
re s
yste
ms.
His
toric
, con
tem
pora
ry,
and
futu
re r
oles
of
the
nurs
e ar
e ad
dres
sed.
Skill
s in
sch
olar
ly e
xpos
ition
and
the
use
of
tech
nolo
gy a
re d
evel
oped
.
Role
of
bacc
alau
reat
e-pr
epar
ed n
urse
Scho
larly
writ
ing
and
use
of s
chol
arly
res
ourc
esC
ritic
al t
hink
ing
Ethi
csEv
olut
ion
of h
olis
tic n
ursi
ngPr
inci
ples
of
holis
tic n
ursi
ngSt
anda
rds
of c
are
Prof
essi
onal
nur
sing
org
aniz
atio
nsW
orki
ng in
gro
ups
Tech
nolo
gy a
nd in
form
atic
sA
dvan
ced
nurs
ing
educ
atio
nTh
e nu
rse
of t
he f
utur
e
This
cou
rse
exam
ines
the
The
ory
of In
tegr
alN
ursi
ng. H
olis
tic N
ursi
ng T
heor
ies
are
ex-
plor
ed. T
he c
once
pt o
f pr
axis
is in
trod
uced
.Fl
oren
ce N
ight
inga
le’s
lega
cy a
nd p
hilo
soph
i-ca
l fou
ndat
ion
are
incl
uded
. Stu
dent
s de
velo
psk
ills
rela
ted
to s
elf-
awar
enes
s, s
elf-
care
,re
latio
nshi
p-ce
nter
ed c
are,
and
ref
lect
ive
prac
tice.
The
use
of
cons
ciou
s in
tent
ion
isem
phas
ized
.
Inte
gral
nur
sing
/Inte
gral
hea
lthH
olis
tic n
ursi
ngIn
tegr
ativ
e nu
rsin
g pr
actic
eH
ealin
gN
ursi
ng m
etap
arad
igm
con
cept
sPa
tter
ns o
f kn
owin
gRe
latio
nshi
p-ce
nter
ed c
are
Self-
care
Refle
ctiv
e pr
actic
eIn
tent
ion
Flor
ence
Nig
htin
gale
Spiri
tual
ityTh
erap
eutic
use
of
self
Hol
istic
nur
sing
the
orie
sSe
lf-co
nfid
ence
Nur
se a
s en
viro
nmen
tH
olis
tic c
arin
g pr
oces
s
This
tw
o-pa
rt c
ours
e ad
dres
ses
path
ophy
sio-
logi
cal r
espo
nses
and
ada
ptat
ion
of t
he p
hysi
-ca
l bod
y to
an
insu
lt. A
naly
sis
of p
atho
logi
cal
alte
ratio
ns in
hea
lth a
t th
e ce
llula
r an
d sy
stem
sle
vel a
nd im
plic
atio
ns f
or n
ursi
ng c
are
are
em-
phas
ized
. Stu
dent
s fo
cus
on m
ultis
yste
m in
ter-
actio
n of
the
bod
y to
an
illne
ss o
r in
jury
. The
path
ophy
siol
ogic
al b
asis
of
addi
ctio
ns a
ndbe
havi
oral
dis
orde
rs is
exp
lore
d. S
tude
nts
are
intr
oduc
ed t
o th
e bi
olog
y of
bel
ief.
Cel
lula
r bi
olog
yG
enet
ic d
isea
seIm
mun
ityIn
flam
mat
ion
Stre
ss a
nd d
isea
se, P
sych
oneu
roim
mun
olog
yN
euro
logi
c sy
stem
Endo
crin
e sy
stem
Repr
oduc
tive
syst
emH
emat
olog
ic s
yste
mC
ardi
ovas
cula
r an
d ly
mph
atic
sys
tem
Pulm
onar
y sy
stem
Rena
l and
uro
logi
c sy
stem
Dig
estiv
e sy
stem
Mus
culo
skel
etal
sys
tem
Inte
gum
enta
ry s
yste
mM
ultip
le o
rgan
dys
func
tion
Path
ophy
siol
ogy
of a
ddic
tions
Path
ophy
siol
ogy
of b
ehav
iora
l dis
orde
rsBi
olog
y of
bel
ief
Co
urs
e D
escr
ipti
on
Co
urs
e To
pic
s
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 38
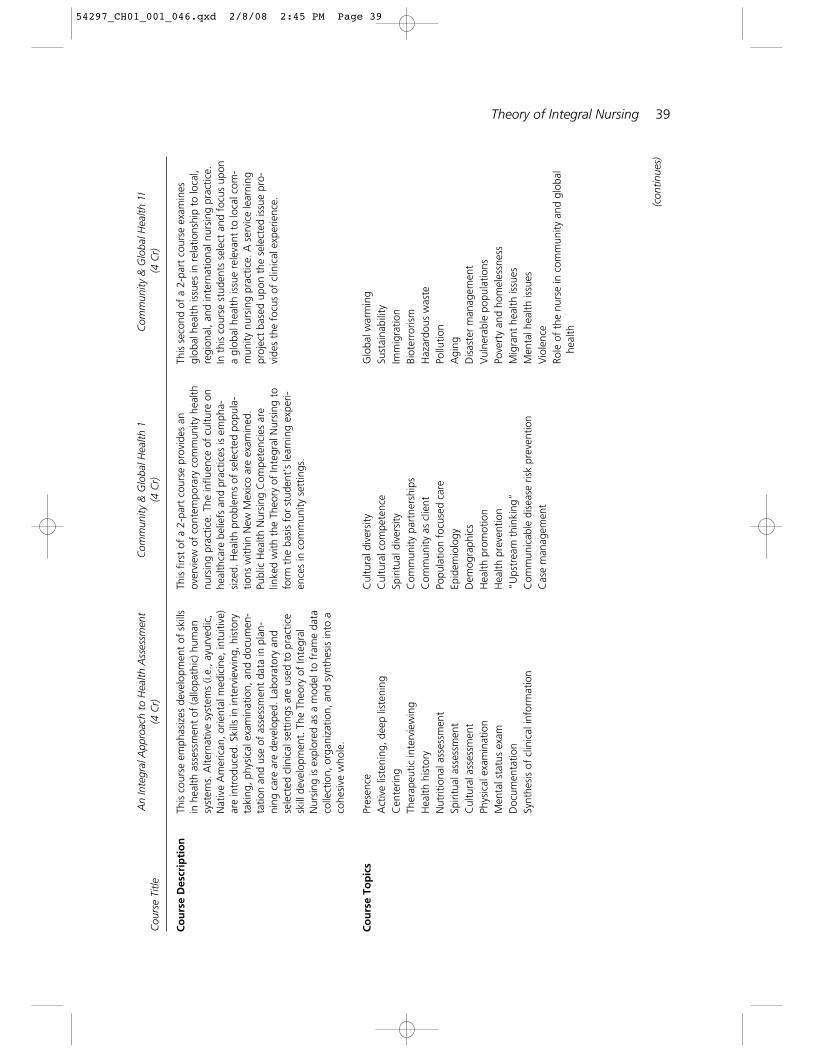
Theory of Integral Nursing 39
An
Inte
gral
App
roac
h to
Hea
lth A
sses
smen
tC
omm
unity
& G
loba
l Hea
lth 1
Com
mun
ity &
Glo
bal H
ealth
1I
Cou
rse
Title
(4 C
r)(4
Cr)
(4 C
r)
This
cou
rse
emph
asiz
es d
evel
opm
ent
of s
kills
in h
ealth
ass
essm
ent
of (a
llopa
thic
) hum
ansy
stem
s. A
ltern
ativ
e sy
stem
s (i.
e., a
yurv
edic
,N
ativ
e A
mer
ican
, orie
ntal
med
icin
e, in
tuiti
ve)
are
intr
oduc
ed. S
kills
in in
terv
iew
ing,
his
tory
taki
ng, p
hysi
cal e
xam
inat
ion,
and
doc
umen
-ta
tion
and
use
of a
sses
smen
t da
ta in
pla
n-ni
ng c
are
are
deve
lope
d. L
abor
ator
y an
dse
lect
ed c
linic
al s
ettin
gs a
re u
sed
to p
ract
ice
skill
dev
elop
men
t. T
he T
heor
y of
Inte
gral
Nur
sing
is e
xplo
red
as a
mod
el t
o fr
ame
data
colle
ctio
n, o
rgan
izat
ion,
and
syn
thes
is in
to a
cohe
sive
who
le.
Pres
ence
Act
ive
liste
ning
, dee
p lis
teni
ngC
ente
ring
Ther
apeu
tic in
terv
iew
ing
Hea
lth h
isto
ryN
utrit
iona
l ass
essm
ent
Spiri
tual
ass
essm
ent
Cul
tura
l ass
essm
ent
Phys
ical
exa
min
atio
nM
enta
l sta
tus
exam
Doc
umen
tatio
nSy
nthe
sis
of c
linic
al in
form
atio
n
This
firs
t of
a 2
-par
t co
urse
pro
vide
s an
over
view
of
cont
empo
rary
com
mun
ity h
ealth
nurs
ing
prac
tice.
The
influ
ence
of
cultu
re o
nhe
alth
care
bel
iefs
and
pra
ctic
es is
em
pha-
size
d. H
ealth
pro
blem
s of
sel
ecte
d po
pula
-tio
ns w
ithin
New
Mex
ico
are
exam
ined
.Pu
blic
Hea
lth N
ursi
ng C
ompe
tenc
ies
are
linke
d w
ith t
he T
heor
y of
Inte
gral
Nur
sing
to
form
the
bas
is f
or s
tude
nt’s
lear
ning
exp
eri-
ence
s in
com
mun
ity s
ettin
gs.
Cul
tura
l div
ersi
tyC
ultu
ral c
ompe
tenc
eSp
iritu
al d
iver
sity
Com
mun
ity p
artn
ersh
ips
Com
mun
ity a
s cl
ient
Popu
latio
n fo
cuse
d ca
reEp
idem
iolo
gyD
emog
raph
ics
Hea
lth p
rom
otio
nH
ealth
pre
vent
ion
“Ups
trea
m t
hink
ing”
Com
mun
icab
le d
isea
se r
isk
prev
entio
nC
ase
man
agem
ent
This
sec
ond
of a
2-p
art
cour
se e
xam
ines
glob
al h
ealth
issu
es in
rel
atio
nshi
p to
loca
l,re
gion
al, a
nd in
tern
atio
nal n
ursi
ng p
ract
ice.
In t
his
cour
se s
tude
nts
sele
ct a
nd f
ocus
upo
na
glob
al h
ealth
issu
e re
leva
nt t
o lo
cal c
om-
mun
ity n
ursi
ng p
ract
ice.
A s
ervi
ce le
arni
ngpr
ojec
t ba
sed
upon
the
sel
ecte
d is
sue
pro-
vide
s th
e fo
cus
of c
linic
al e
xper
ienc
e.
Glo
bal w
arm
ing
Sust
aina
bilit
yIm
mig
ratio
nBi
oter
roris
mH
azar
dous
was
tePo
llutio
nA
ging
Dis
aste
r m
anag
emen
tV
ulne
rabl
e po
pula
tions
Pove
rty
and
hom
eles
snes
sM
igra
nt h
ealth
issu
esM
enta
l hea
lth is
sues
Vio
lenc
eRo
le o
f th
e nu
rse
in c
omm
unity
and
glo
bal
heal
th
Co
urs
e D
escr
ipti
on
Co
urs
e To
pic
s
(con
tinue
s)
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 39
40 CHAPTER 1 INTEGRAL AND HOLISTIC NURSING: LOCAL TO GLOBAL
Tab
le 1
-12
Cur
ricul
um f
or R
N-t
o-BS
N P
rogr
am U
sing
the
The
ory
of In
tegr
al N
ursi
ng (c
ontin
ued)
An
Inte
gral
App
roac
h to
H
ealth
Pol
icy
from
an
In
tegr
al C
omm
unic
atio
n an
d Ev
iden
ce-B
ased
Pra
ctic
eIn
tegr
al P
ersp
ectiv
eTe
achi
ng
Cou
rse
Title
(4 C
r)(3
Cr)
(2 C
r)
This
cou
rse
exam
ines
res
earc
h m
etho
dolo
gies
utili
zed
in n
ursi
ng r
esea
rch.
Em
phas
is is
on
utili
zatio
n of
res
earc
h fin
ding
s to
est
ablis
hev
iden
ce-b
ased
nur
sing
inte
rven
tions
. Stu
-de
nts
anal
yze
rese
arch
fin
ding
s ai
med
at
sele
cted
hea
lth c
once
rns.
Stu
dent
s ex
plor
ede
finiti
ons
of e
vide
nced
-bas
ed p
ract
ice
and
exam
ine
how
wor
ldvi
ews
influ
ence
res
earc
h.
His
toric
al e
volu
tion
of n
ursi
ng r
esea
rch
Qua
ntita
tive
rese
arch
Q
ualit
ativ
e re
sear
ch
Ethi
cs in
nur
sing
res
earc
hTh
eory
and
res
earc
h fr
amew
orks
Out
com
es r
esea
rch
Stat
istic
s U
sing
res
earc
h in
an
inte
gral
nur
sing
pra
ctic
eA
ltern
ativ
e ph
iloso
phie
s of
sci
ence
This
cou
rse
emph
asiz
es e
mpo
wer
ing
stud
ents
with
kno
wle
dge,
ski
lls, a
nd a
ttitu
des
to e
ffec
tch
ange
in h
ealth
pol
icy
to im
prov
e he
alth
care
del
iver
y. S
tude
nts
anal
yze
cont
empo
rary
heal
th c
are
issu
es o
f co
ncer
n to
nur
sing
and
lear
n st
rate
gies
for
eff
ectiv
e in
volv
emen
t in
polic
y-m
akin
g de
cisi
ons
and
polic
y im
plem
en-
tatio
n. S
tude
nts
exam
ine
wor
k en
viro
nmen
tsan
d th
e im
pact
of
orga
niza
tiona
l sys
tem
s on
the
qual
ity o
f ca
re. S
tude
nts
appl
y th
e Th
eory
of In
tegr
al N
ursi
ng t
o a
curr
ent
heal
th p
olic
yis
sue
in a
pos
ition
pap
er e
xpre
ssed
ora
lly t
o a
grou
p.
Cur
rent
hea
lth c
are
tren
dsH
ealth
car
e de
liver
y sy
stem
sH
ealth
car
e fin
anci
ng
Com
plex
ity a
nd c
hang
e th
eory
Empo
wer
men
t Ef
fect
ive
patie
nt a
dvoc
acy
Nav
igat
ing
the
legi
slat
ive
proc
ess
Hea
lth c
are
refo
rmC
omm
unic
atin
g th
e es
senc
e of
nur
sing
/de
velo
ping
a n
ursi
ng v
oice
This
cou
rse
exam
ines
com
mun
icat
ion
tech
-ni
ques
, cou
nsel
ing,
coa
chin
g, a
nd t
each
ing
stra
tegi
es t
o en
hanc
e an
d fa
cilit
ate
cogn
itive
and
beha
vior
al c
hang
e. S
tude
nts
inte
grat
epr
inci
ples
of
inte
gral
com
mun
icat
ion,
inte
gral
heal
th c
oach
ing,
mot
ivat
iona
l int
ervi
ewin
g,an
d N
on-V
iole
nt C
omm
unic
atio
n.
Mot
ivat
iona
l Int
ervi
ewin
gEd
ucat
iona
l the
ory
Fund
amen
tals
of
Hea
lth C
oach
ing
Hel
ping
oth
ers
crea
te h
ealth
y lif
esty
les
Hel
ping
oth
ers
navi
gate
the
hea
lthca
re s
yste
mN
on-V
iole
nt C
omm
unic
atio
n (N
VC
)Pr
esen
ceLe
arni
ng s
tyle
sIn
stru
ctio
nal d
esig
n m
etho
dsC
ouns
elin
gW
ays
of k
now
ing
Co
urs
e D
escr
ipti
on
Co
urs
e To
pic
s
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 40

Theory of Integral Nursing 41
Tota
l Cre
dit
Hou
rs: 4
2
Sour
ce:C
ourt
esy
of D
arle
ne R
. Hes
s, P
hD, A
PRN
-BC
, AH
N-B
C, ©
200
7.
Tran
sfor
mat
iona
l Lea
ders
hip
Inte
grat
ing
Com
plem
enta
ry &
Alte
rnat
ive
In
tegr
al N
ursi
ng P
ract
ice
in
Nur
sing
A
ppro
ache
s to
Nur
sing
Se
nior
Pro
ject
C
ours
e Ti
tle(3
Cr)
(4 C
r)(3
Cr)
This
cou
rses
foc
uses
on
the
prin
cipl
es o
ftr
ansf
orm
atio
nal l
eade
rshi
p as
app
lied
to t
henu
rse
lead
er a
t th
e be
dsid
e, w
ithin
an
orga
ni-
zatio
n, in
the
com
mun
ity, a
nd in
the
pro
fes-
sion
. The
stu
dent
is in
trod
uced
to
Com
plex
itySc
ienc
e, A
ppre
ciat
ive
Inqu
iry, a
nd E
mot
iona
lIn
telli
genc
e. C
aree
r ad
vanc
emen
t th
roug
hlif
elon
g le
arni
ng is
em
phas
ized
.
Tran
sfor
mat
iona
l Mod
elLe
ader
ship
dev
elop
men
tC
ompl
exity
Sci
ence
Pr
ofes
sion
al e
thic
sIn
terd
isci
plin
ary
lead
ersh
ipA
ppre
ciat
ive
Inqu
iryEm
otio
nal I
ntel
ligen
ceC
onfli
ct r
esol
utio
n/M
edia
tion
Del
egat
ion
Cus
tom
er n
eeds
and
exp
ecta
tions
Vis
ioni
ng a
nd s
trat
egic
pla
nnin
gM
anag
ing
care
acr
oss
the
cont
inuu
mIm
prov
ing
qual
ity a
nd p
erfo
rman
ceH
uman
res
ourc
e m
anag
emen
t
This
cou
rse
prov
ides
an
intr
oduc
tion
to e
vi-
denc
e-ba
sed
com
plem
enta
ry a
nd a
ltern
ativ
eap
proa
ches
to
heal
th c
are.
Stu
dent
s ac
quire
know
ledg
e re
late
d to
alte
rnat
ive
and
com
ple-
men
tary
hea
ling
mod
aliti
es t
hat
can
be in
cor-
pora
ted
into
pro
fess
iona
l nur
sing
pra
ctic
ean
d se
lf ca
re p
ract
ices
. Stu
dent
s ex
perie
nce
and
deve
lop
begi
nnin
g sk
ills
in t
he p
rovi
sion
of C
AM
mod
aliti
es a
s th
ey in
tera
ct w
ith p
rac-
titio
ners
in s
elec
ted
clin
ical
set
tings
.
NIC
AM
Who
le m
edic
al s
yste
ms
Min
d-Bo
dy in
terv
entio
nsEn
ergy
the
rapi
esBi
olog
ical
ly-b
ased
the
rapi
esM
anip
ulat
ive
and
body
-bas
ed t
hera
pies
Ther
apeu
tic e
nviro
nmen
tA
rts
and
heal
ing
This
cou
rse
prov
ides
the
stu
dent
an
oppo
rtu-
nity
to
criti
cally
exa
min
e in
-dep
th a
per
sona
llyre
leva
nt t
opic
in p
repa
ratio
n fo
r an
exp
ande
dro
le a
s an
inte
gral
nur
se. S
tude
nts
deve
lop
lear
ning
obj
ectiv
es, a
lear
ning
con
trac
t, a
ndcr
iteria
for
eva
luat
ion
of p
roje
ct o
utco
mes
.
Co
urs
e D
escr
ipti
on
Co
urs
e To
pic
s
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 41

Global Health Nursing. The Theory of IntegralNursing can assist us in using an integral world-view and organizing structure to see where we fallshort and where we excel in prevention educationand healthcare delivery. Our challenge asintegralnurses is that we see global health imperatives ascommon concerns of humankind; they are notisolated problems in far-off countries. LikeNightingale, we must see prevention and preven-tion education as important to the health ofhumanity.4-7
The first priority of nursing is devotion tohuman health—of individuals, of communities,and the world. Integral nurses are educated andprepared—physically, emotionally, mentally, andspiritually—to effectively accomplish the activitiesrequired for healthy people and healthy environ-ments.4-5 An integral approach can help us concep-tualize and map what is missing from caregivingand care delivery. With an integral worldview, col-lectively we can move closer to achieving globalhealth. Ensuring basic survival needs has beenidentified as the single most important thingneeded to build responsive and effective health sys-tems in all countries.6 An increasingly severe globalnursing shortage is threatening nursing’s ranks inalmost every nation in the world.8 The health andhappiness of people everywhere in the global com-munity are the only common ground for a secureand sustainable prosperous future. Yet, a healthyworld still requires nurses knowledge, expertise,wisdom, and dedication. If today’s nurses, mid-wives, and allied health professionals are nurturedand sustained in innovative ways, they can be-come, like Nightingale—effective voices calling forand demonstrating the healing, leadership, andglobal action required to achieve a healthyworld.4,5,11 This can strengthen nursing’s ranks andhelp the world to value and nurture nursing’sessential contributions. As Nightingale said “Wemust create a public opinion, which must drive thegovernment instead of the government having todrive us. . . . an enlightened public opinion, wise inprinciple, wise in detail.”73
We can explore all aspects of the Theory ofIntegral Nursing and apply them to our endeavorsin the underserved communities and populations.Often in the developed world of health care we
believe that decent care is being able to have accessto technology, procedures, tests, or surgery whenwe need it and as quickly as we want. And this isstill a limited view of what integral or even holistichealth care is, since primary prevention such asself-care is rarely given its just due in healthcareinitiatives. However, the majority of the worlddoes not have access as in wealthy developednations.
Consider the World Health Organization(WHO) call for “decent care” for HIV/AIDSpatients and their families throughout the world.7
As you read this reflect on the Theory of IntegralNursing and see how all aspects of this theory arecovered in this WHO “decent care” description.The primary objective is to delineate a new termwithin the taxonomy and politics of HIV/AIDScare—“decent care”—that repositions the individ-ual as the focal point of the care cycle and agencythat emphasizes not only what type or kind of careindividuals receive, but also how that care isreceived. Decent care implies the comprehensiveideal that the medical, physiological, psychologi-cal, and spiritual needs of others are addressed.This includes universal access to treatment withutilization and enforcement of universally ac-cepted precautionary measures for healthcarepractitioners, along with adequate supplies andequipment, safe food, free access to clean water,autoclaves, laundries, and safe methods for steril-izing and disposing of infected materials in incin-erators. An integral worldview and approachconnects all theory content components, quad-rants, and processes to map the various steps toevolve a complete plan of care with the patientand the community that includes the health andsafety of caregivers as well.
CONCLUSION
The Theory of Integral Nursing addresses how wecan increase our integral awareness, our wholeness,and healing, and strengthen our personal and pro-fessional capacities to more fully open to the mys-teries of life’s journey and the wondrous stages ofself-discovery with self and others. Our timedemands a new paradigm and a new languagewhere we take the best of what we know in the sci-
42 CHAPTER 1 INTEGRAL AND HOLISTIC NURSING: LOCAL TO GLOBAL
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 42

Acknowledgments 43
ence and art of nursing that includes holistic andhuman caring theories and modalities. With anintegral approach and worldview we are in a betterposition to share with others the depth of nurses’knowledge, expertise, and critical-thinking capaci-ties and skills for assisting others in creating healthand healing. Only an attention to the heart of nurs-ing, for “sacred” and “heart” reflect a commonmeaning, can we generate the vision, courage, andhope required to unite nursing in healing. Thisassists us as we engage in healthcare reform toaddress the challenges in these troubled times—local to global. This is not a matter of philosophy,but of survival.
Directions forFUTURE RESEARCH
1. Examine the components of relationship-centered care for clinical practice, educa-tion, research, and healthcare policy.
2. Analyze the Theory of Integral Nursing andits application in holistic nursing practice,education, research, and healthcare policy.
Nurse HealerREFLECTIONS
After reading this chapter, the nurse healer will beable to answer or to begin a process of answeringthe following questions:
• How can I apply more of the components ofrelationship-centered-care components eachday?
• In what ways can the Theory of IntegralNursing inform my personal and profes-sional endeavors?
• What integral awareness and practices may Iconsider for development in my personaland professional life?
ACKNOWLEDGMENTS
The Theory of Integral Nursing does not excludeor invalidate other nurse theorists who have alsoinformed my Theory of Integral Nursing, specifi-
cally Florence Nightingale; Jean Watson, PhD,RN, AHN-BC, FAAN; Helen Erickson, PhD, RN,AHN-BC, FAAN; Margaret A. Newman, PhD, RN,FAAN; Patricia Benner, PhD, RN, FAAN; Rose-marie R. Parse, DNSc, RN, FAAN; Anne Boykin,PhD, RN; Martha E. Rodgers, PhD, RN; PeggyChinn, PhD, RN, FAAN; Afaf I. Meleis, PhD, RN,FAAN; and Madeline Leininger, PhD, RN.
I acknowledge Lea Gaydos, PhD, RN, AHN-BC;James Baye, BSN, RN; Barbara Barnum, PhD, RN,FAAN; Jennifer Reich, MA, MS, APRN BC,ACHPN; Darlene R. Hess, PhD, NP, AHN-BC;Cynda H. Rushton, PhD, RN, FAAN; and GeneieEverett, PhD, RN, for critiques and suggestions forthe Theory of Integral Nursing.
Credit is given to the following individuals: toAndrew Harvey who coined the term sacredactivism; Patricia Hinton Walker, PhD, RN, FAAN,who coined the terms and concept nurses as healthdiplomats, integral nurse coaches, and coaching forintegral change, and to Lea Gaydos, PhD, RN, CS,AHN-BC, who introduced me to the jewel meta-phor with healing and integral health.
I also want to acknowledge my American Holis-tic Nurses Association colleagues, many of whom Ihave worked with for over three decades, particu-larly Cathie E. Guzzetta, PhD, RN, AHN-BC,FAAN; Lynn Keegan, PhD, RN, AHN-BC, FAAN;Lea Gaydos, PhD, RN, AHN-BC; Charlie McGuire,MSN, RN, AHN-BC; Noreen Frisch, PhD, RN,AHN-BC, FAAN; Carla Mariano, PhD, RN, AHN-BC, FAAN; Charlotte Eliopoulos, PhD, RN, MPH,ND; and all the members of former and currentAHNA Elder Council; the former and present Jour-nal of Holistic Nursing editors; and the former andcurrent AHNA Leadership Council. In November2006 the collective AHNA holistic nursing endeav-ors were recognized as a specialty by the AmericanNurses Association (ANA). I believe that our chal-lenge now is to move the holistic paradigm to anintegral paradigm and language.
I express deep gratitude to Roshi Joan Halifax,Cynda Rushton, PhD, RN, FAAN, and the facultyand facilitation team of the Being With Dying Pro-fessional Training Program in Compassionate End-of-Life Care at Upaya Zen Center, Santa Fe, NewMexico, for the wisdom we have shared in councilprocess, bearing witness, and mindfulness practices.
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 43

I acknowledge the exciting endeavors with myNightingale Initiative for Global Health (NIGH)and the Nightingale Declaration Campaign(NDC) colleagues Deva-Marie Beck, PhD, RN;Cynda Rushton, PhD, RN, FAAN; Wayne Kines;Eleanor Kibrick; William Rolph; and Don de Silva;and our future collaborative endeavors that are indevelopment and scheduled through 2020. Visithttp://www.nightingaledeclaration.net for moreinformation.
I recognize the work of Nightingale scholarsDeva-Marie Beck, PhD, RN, and Louise Selanders,EdD, RN, FAAN, with whom I have worked forover two decades, and who have assisted me in theFlorence Nightingale Services at the WashingtonNational Cathedral in 2001 and 2004 and in futureservices yet to be scheduled.I also recognized thededicated work of Nightingale scholar LynnMcDonald, editor of The Collected Works ofFlorence Nightingale (16 volumes, http://www.sociology.uoguelph.ca/fnightingale). The work ofFlorence Nightingale scholar Alex Attewell, for-mer director of the Florence Nightingale Museum(http://www.florence-nightingale.co.uk/index.php) in London is also recognized.
I acknowledge my many conversations withKen Wilber and the Integral Institute team, partic-ularly Diane Hamilton, Willow Pearson, SophiaDiaz, Clint Fuhs, Nicole Fegley, and Kelley Bearer,who have challenged me to bring my integral workforward.
NOTES
1. B. M. Dossey, “Theory of Integral Nursing,” Advancesin Nursing Science 31, no. 1 (2008): E52–E73.
2. B. M. Dossey, Integral Nursing: Practice, Education,Research, Policy (In press).
3. American Holistic Nurses Association & the AmericanNurses Association, Holistic Nursing Practice: Scope andStandards (Silver Spring, MD: Nursesbooks.org, 2007).
4. B. M. Dossey et al., Florence Nightingale Today: Heal-ing, Leadership, Global Action (Washington, DC:NurseBooks.org, 2005).
5. B. M. Dossey, D. M. Beck, and C. H. Rushton, “Night-ingale’s Vision for Collaboration,” inNursing WithoutBorders: Values, Wisdom and Success Markers, eds. S. Weinstein and A. M. Brooks (Indianapolis, IN:Sigma Theta Tau, 2008), 13–29.
6. L. O. Gostin, “Meeting the Survival Needs of theWorld’s Least Healthy People,” Journal of AmericanMedical Association 298, no. 2 (2007): 225–227.
7. T. Karpf, N. Tashima, and C. Crain, Restoring Hope:Building a Foundation for Decent Care: World HealthReport on Decent Care, (Copenhagen, Denmark, 2008).
8. International Council of Nurses, The Global Shortageof Registered Nurses: An Overview of Issues and Action(Geneva: International Council of Nurses 2004),http://www.icn.ch/global/shortage.pdf.
9. United Nations, United Nations Millennium Develop-ment Goals (New York: United Nations, 2000), http://www.un.org/millenniumgoals/html.
10. B. Dossey, Florence Nightingale: Mystic, Visionary, Healer(Philadelphia: Lippincott, Williams & Wilkins, 2000).
11. Nightingale Initiative for Global Health. NightingaleDeclaration, http://www.nightingaledeclaration.net.
12. A. Harvey, Sacred Activism, http://www.andrewharvey.net/sacred_activism.html.
13. P. H. Walker, personal communication, May 15, 2007.
14. F. Nightingale, Notes on Hospitals, (London: John W.Parker & Son, 1859).
15. F. Nightingale, Notes on Nursing, (London: Harrison,1860).
16. F. Nightingale, “Letter from Miss Nightingale to theProbationer-Nurses in the ‘Nightingale Fund’ at St.Thomas’s Hospital, and the Nurses Who Were For-merly Trained There, 1888,” in Florence NightingaleToday: Healing, Leadership, Global Action, eds. B. M.Dossey et al. (Silver Spring, MD: Nursesbooks.org,2005), 203–285.
17. F. Nightingale, “Sick-Nursing and Health-Nursing,” inFlorence Nightingale Today: Healing, Leadership, GlobalAction, eds. B. M. Dossey et al. (Silver Spring, MD:Nursebooks.org, 2005), 288–303.
18. L. Dossey, Reinventing Medicine: Beyond Mind-Body To aNew Era of Healing (San Francisco: HarperSanFrancisco,1999).
19. L. Dossey, Meaning and Medicine: A Doctor’s Tales ofBreakthrough and Healing (New York: Bantam Books,1991).
20. L. Dossey, Healing Words: The Power of Prayer and thePractice of Medicine (San Francisco: HarperSanFrancisco,1993).
21. L. Dossey, Recovering the Soul: Scientific and SpiritualSearch (New York: Bantam, 1989).
22. L. Dossey, “Spirituality, Prayer, and Medicine: What Isthe Fuss Really About?”Virtual Mentor Ethics Journalof the American Medical Association 7, no. 5 (2005),http://www.virtualmentor.org.
23. L. Dossey, Healing Beyond the Body: The InfiniteReaches of the Mind (Boston: Shambhala, 2000).
44 CHAPTER 1 INTEGRAL AND HOLISTIC NURSING: LOCAL TO GLOBAL
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 44

Notes 45
24. C. Tresoli, Pew-Fetzer Task Force on Advancing Psy-chosocial Health Education: Health Professions Educa-tion and Relationship-Centered Care (San Francisco:Commission at the Center for the Health Professions,University of California, 1994).
25. M. Koloroutis, ed., Relationship-Based Care: A Modelfor Transforming Practice (Minneapolis, MN: CreativeHealth Care Management, 2004).
26. K. Wilber, Integral Psychology (Boston: Shambhala,2000).
27. K. Wilber, The Collected Works of Ken Wilber, Vols.1–4 (Boston: Shambhala, 1999).
28. K. Wilber, The Collected Works of Ken Wilber, Vols.5–8 (Boston: Shambhala, 2000).
29. K. Wilber, Integral Operating System (Louisville, CO:Sounds True, 2005).
30. K. Wilber, Integral Life Practice (Denver, CO: IntegralInstitute, 2005).
31. K. Wilber, Integral Spirituality (Boston: Shambhala,2006).
32. J. Baye, “Nursing in Canada with the Integral Frame-work,” (In press).
33. J. Baye, “Royal Jubilee Hospital Pre-Acudose Deploy-ment Integral Assessment,” (In press).
34. C. S. Clark, “An Integral Nursing Education: Explo-ration of the Wilber Quadrant Model,” InternationalJournal of Human Caring 10, no. 3 (2006): 22–29.
35. K. Fiandt et al., “Integral Nursing: An EmergingFramework for Engaging the Evolution of the Profes-sion,” Nursing Outlook 51, no. 3 (2003): 130–137.
36. N. C. Frisch, “Nursing Theory in Holistic NursingPractice,” in Holistic Nursing: A Handbook for Practice,eds. B. M. Dossey and L. Keegan, 5th ed. (Sudbury,MA: Jones & Bartlett, 2008).
37. J. F. Quinn et al., “Research Guidelines for Assessingthe Impact of the Healing Relationship in ClinicalNursing,” Alternative Therapies in Health and Medicine9, no. 3 (2003): A65–A79.
38. R. Zahourek, “Holistic Nursing Research,” in HolisticNursing: A Handbook for Practice, eds. B. M. Dosseyand L. Keegan, 5th ed. (Sudbury, MA: Jones & Bartlett;2008).
39. J. Watson, Caring Science as Sacred Science (Philadel-phia: F. A. Davis, 2005).
40. O. J. Jarrín, “An Integral Philosophy and Definition ofNursing,” AQAL: Journal of Integral Theory and Prac-tice 2, no. 4 (2007): XX–XX.
41. B. S. Barnum, Nursing Theory: Analysis, Application,Evaluation, 6th ed. (Philadelphia: Lippincott Williams& Wilkins, 2004).
42. H. L. Gaydos, “The Experience of Immobility Due toTrauma,” Holistic Nursing Practice 19, no. 1 (2005):40–43.
43. H. L. Gaydos,“The Co-Creative Aesthetic Process: ANew Model for Aesthetics in Nursing,” InternationalJournal of Human Caring 7 (2004): 40–43.
44. R. Zahourek,“Intentionality Forms the Matrix ofHealing: A Theory,” Alternative Therapies in Healthand Medicine 10, no. 6 (2004): 40–49.
45. D. Beck, “Spiral Dynamics Integral,” http://www.spiraldynamics.net.
46. B. A. Carper,“Fundamental Patterns of Knowing inNursing,” Advances in Nursing Science 1, no. 1 (1978):13–23.
47. P. L. Munhall“Unknowing: Toward Another Patternof Knowing in Nursing,” Nursing Outlook 41, no. 3(1993): 125–128.
48. J. White, “Patterns of Knowing: Review, Critique, andUpdate,” Advances in Nursing Science 17, no. 2 (1995):73–86.
49. J. B. Averill and P. T. Clements,“Patterns of Knowingas a Foundation for Action-Sensitive Pedagogy,” Qual-itative Health Research 17, no. 3 (2007): 386–399.
50. P. L. Chinn and M. K. Kramer, Theory and Nursing:Integrated Knowledge Development, 6th ed. (St. Louis,MO: Mosby, 2004).
51. W. R. Cowling, “Pattern, Participation, Praxis, andPower in Unitary Appreciative Inquiry,” Advances inNursing Science 27, no. 3 (2004): 202–214.
52. J. Fawcett et al., “On Nursing Theories and Evidence,”Journal of Nursing Scholarship 33, no. 2 (2001):115–119.
53. A. L. Meleis, Theoretical Nursing: Development andProgress, 3rd ed., rev. (Philadelphia: LippincottWilliams & Wilkins, 2005).
54. M. A. Newman, “A World of No Boundaries,”Advances in Nursing Science 26, no. 4(2003): 240–245.
55. B. Barnum, Spirituality in Nursing: From Traditional toNew Age, 2nd ed. (New York: Springer, 2003).
56. M. A. Burkhardt and M. G Najai-Jacobson, “Spiritual-ity and Healing,” in Holistic Nursing: A Handbook forPractice, eds. B. M.Dossey and L. Keegan, 5th ed. (Sud-bury, MA: Jones & Bartlett, 2008).
57. M. McKivergin, “Nurse as an Instrument of Healing,”in Holistic Nursing: A Handbook for Practice, eds. B. M.Dossey and L. Keegan, 5th ed. (Sudbury, MA: Jones &Bartlett, 2008).
58. J. A. Engebretson, “Heterodox Model of Healing,”Alternative Therapies in Health and Medicine 4, no. 2(1998): 37–43.
59. J. G. Koerner, Nursing Presence: The Essence of Nursing(New York: Springer, 2007).
60. J. Halifax, B. M. Dossey, and C. H. Rushton, BeingWith Dying: Compassionate End-of-Life Training GuideCare (Santa Fe, NM: Prajna Mountain Press, 2007).
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 45

61. C. H. Rushton, J. Halifax, and B. M. Dossey, “Beingwith Dying,” American Nurse Today 2, no. 9 (2007):1–3.
62. L. Dossey, “Samueli Conference on Definitions andStandards in Healing Research: Working Definitionsand Terms,” Alternative Therapies in Health and Medi-cine 9, no. 3 (2003): A11.
63. F. Nightingale, “To the Probationer-Nurses in theNightingale Fund School at St. Thomas’ Hospital fromFlorence Nightingale, 16th May 1888 (Privatelyprinted),” in Florence Nightingale Today: Healing,Leadership, Global Action, eds. B. M. Dossey et al. (Sil-ver Spring, MD: Nursebooks.org, 2005), 274.
64. F. Nightingale, “Una and the Lion,” Good Words June(1868), 362, in B. M. Dossey, Florence Nightingale:Mystic, Visionary, Healer (Philadelphia: Lippincott,Williams and Wilkins, 2000), 294.
65. C. G. Jung, The Archetypes and the Collective Uncon-scious, 2nd ed., Vol. 9, Part I (Princeton, NJ: Bollingen,1981).
66. F. Nightingale, “To the Nurses and ProbationersTrained Under the ‘Nightingale Fund’1883, Privatelyprinted,” (London: Spottiswoode), in FlorenceNightingale Today: Healing, Leadership, Global Action,eds. B. M. Dossey et al. (Silver Spring, MD: Nurse-books.org, 2005), 267.
67. F. Nightingale, Address from Miss Nightingale to theProbationer-Nurses in the ‘Nightingale Fund’ at St.Thomas’s Hospital, and the Nurses who were FormerlyTrained There, Privately Printed, 1897” (London:Spottiswoode), in Florence Nightingale Today: Healing,Leadership, Global Action, eds. B. M. Dossey et al. (Sil-ver Spring, MD: Nursebooks.org, 2005), 283-284.
68. F. Nightingale, “To the Probationer-Nurses in theNightingale Fund School at St. Thomas’ Hospital fromFlorence Nightingale 16th May 1897, Privatelyprinted,” in Florence Nightingale Today: Healing, Lead-ership, Global Action, eds. B. M. Dossey et al. (SilverSpring, MD: Nursebooks.org, 2005), 283.
69. D. Pisanos, Integral Coaching Model, personal com-munication, June 25, 2007.
70. L. Bark, As One Coaching, http://www.asonecoaching.com.
71. D. R. Hess, Curriculum for an RN to BSN programusing the Theory of Integral Nursing,personal com-munication, September 17, 2007.
72. S. Esbjorn-Hargens, “Integral Research: A Multi-Method Approach to Investigating Phenomena,” Con-structivism in the Human Sciences 11, no. 1 (2006):79–107.
73. F. Nightingale, Letter to Sir Frederick Verney. 23November 1892, Add. Mss. 68887 ff102-05.
46 CHAPTER 1 INTEGRAL AND HOLISTIC NURSING: LOCAL TO GLOBAL
54297_CH01_001_046.qxd 2/8/08 2:45 PM Page 46
Top Related