







Languages
Pages
Legal


Copyright
by
Djordje Adnadjevic
2010

The Thesis committee for Djordje Adnadjevic
Certifies that this is the approved version of the following thesis
Development of a Suction Detection System for a Motorized
Pulsatile Blood Pump
Approved bySupervising Committee:
Raul Longoria
Dragan Djurdjanovic

Development of a Suction Detection System for a Motorized
Pulsatile Blood Pump
by
Djordje Adnadjevic, B.S.
Thesis
Presented to the Faculty of the Graduate School of
The University of Texas at Austin
in Partial Fulfillment
of the Requirements
for the Degree of
Master of Science in Engineering
The University of Texas at Austin
August 2010

Acknowledgments
I would like to thank my graduate advisor, Dr. Raul Longoria, for his insightful support
and guidance. In addition, this thesis would not have been possible without the financial
support of Windmill Cardiovascular Systems, and assistance from engineers Thomas Pate
and Jeffrey Gohean. Lastly, I thank Dr. Carolyn Seepersad for her assistance with helping
me fabricate the ventricle mold described in Chapter 3.
Djordje Adnadjevic
The University of Texas at Austin
August 2010
iv

Development of a Suction Detection System for a Motorized
Pulsatile Blood Pump
Djordje Adnadjevic, M.S.E.
The University of Texas at Austin, 2010
Supervisor: Raul Longoria
A computational model has been developed to study the effects of left ventricular
assist devices (LVADs) on the cardiovascular system during a ventricular collapse. The
model consists of a toroidal pulsatile blood pump and a closed loop circulatory system.
Together, they predict the pump’s motor current traces that reflect ventricular suck-down
and provide insights into torque magnitudes that the pump experiences. In addition, the
model investigates likeliness of a suction event and predicts reasonable outcomes for a few
test cases.
Ventricular collapse was modeled with the help of a mock circulatory loop consisting
of a artificial left ventricle and centrifugal continuous flow pump. This study also investi-
gates different suction detection schemes and proposes the most suitable suction detection
algorithm for the TORVAD TM pump, toroidal left ventricular assist device. Model predic-
tions were further compared against the data sampled during in vivo animal trials with the
TORVAD TM system. The two sets of results are in good accordance.
v

Contents
Acknowledgments iv
Abstract v
List of Tables viii
List of Figures ix
Chapter 1 Introduction and Literature Review 1
1.1 Congestive Heart Failure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
1.2 Mechanical Assist Devices . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
1.3 Ventricular Collapse . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
1.4 Suction Detection Schemes . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
1.5 Motivation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Chapter 2 Model of the Pulsatile Blood Pump, Cardiovascular System, and
Connection Interface 8
2.1 Model of the Motorized Pulsatile Blood Pump . . . . . . . . . . . . . . . . 10
2.2 Model of the Cardiovascular System . . . . . . . . . . . . . . . . . . . . . . 13
2.3 Model of the Pump-CVS Interface . . . . . . . . . . . . . . . . . . . . . . . 15
2.4 Initial Verification of the Model . . . . . . . . . . . . . . . . . . . . . . . . . 20
Chapter 3 Experimental Suction Parameterization: Variable Orifice Resis-
tance 23
3.1 Ellipsoidal Approximation of the Left Ventricle . . . . . . . . . . . . . . . . 23
3.1.1 LV Rapid Prototyping and LV Silicon Mold . . . . . . . . . . . . . . 24
3.1.2 Mock Loop Ventricle . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
3.2 Experimental Estimation of Flow Characteristics during Ventricular Collapse
via Mock Circulatory Loop . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
vi

Chapter 4 Suction Detection Algorithm 33
4.1 Detection Methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
4.1.1 Sensory Input Alone . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
4.1.2 Harmonic Distortion Analysis of a Signal . . . . . . . . . . . . . . . 34
4.1.3 Spectral/Time Domain Masking . . . . . . . . . . . . . . . . . . . . 35
4.2 Suction Detection for TORVAD TM . . . . . . . . . . . . . . . . . . . . . . . 35
Chapter 5 Results 37
5.1 Defining Thresholds . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
5.2 Suction Event . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39
5.2.1 Suction Event Effects on CVS . . . . . . . . . . . . . . . . . . . . . . 40
5.2.2 Suction Event Effects on Toroidal Pump . . . . . . . . . . . . . . . . 47
Chapter 6 Conclusions 49
Appendix A Cardiovascular System Summary 51
Appendix B Matlab Files 56
Bibliography 62
Vita 67
vii
List of Tables
1.1 NYHA heart failure classification system . . . . . . . . . . . . . . . . . . . . 3
2.1 Typical PMDC parameter values used for simulation in this thesis. . . . . . 12
2.2 Subscript definitions for the CVS . . . . . . . . . . . . . . . . . . . . . . . . 14
2.3 Relevant design parameter for the inlet cannula . . . . . . . . . . . . . . . . 19
viii

List of Figures
1.1 The heart . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
1.2 Left ventricular assist device (LVAD). . . . . . . . . . . . . . . . . . . . . . 4
1.3 Intramyocardial bruising . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
2.1 Overall model diagram. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
2.2 Toroidal pulsatile blood pump . . . . . . . . . . . . . . . . . . . . . . . . . . 10
2.3 Toroidal blood pump Bond Graph. . . . . . . . . . . . . . . . . . . . . . . . 11
2.4 Cardiovascular system schematic . . . . . . . . . . . . . . . . . . . . . . . . 13
2.5 Cardiovascular system Bond Graph. . . . . . . . . . . . . . . . . . . . . . . 14
2.6 Inflow tip, designed by Windmill CVS. . . . . . . . . . . . . . . . . . . . . . 15
2.7 Fluid flow through orifice . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
2.8 Pressure vs. Flow across orifice. . . . . . . . . . . . . . . . . . . . . . . . . 17
2.9 Bond graph model of the pump-CVS junction. . . . . . . . . . . . . . . . . 18
2.10 Model of the elastic tube. . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
2.11 A PV Loop case study . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
2.12 PV Loop obtained via cardiovascular system model . . . . . . . . . . . . . . 21
2.13 PV Loop obtained via cardiovascular system model, with pump attached . 22
3.1 LV computer aided design . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
3.2 LV mold making process . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
3.3 Mock loop left ventricle . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
3.4 Mock loop schematic . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
3.5 Mock circulatory loop . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
3.6 Biomedicus pump . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
3.7 Differential wet-to-wet pressure transducer . . . . . . . . . . . . . . . . . . . 30
3.8 Experimental parametrization: Measurements . . . . . . . . . . . . . . . . . 31
3.9 Experimental parametrization: P vs. Q . . . . . . . . . . . . . . . . . . . . 31
3.10 Experimental parametrization: R vs. Vlv . . . . . . . . . . . . . . . . . . . . 32
ix

5.1 Pump current and piston position, no suction . . . . . . . . . . . . . . . . . 38
5.2 Pump current derivative, no suction . . . . . . . . . . . . . . . . . . . . . . 38
5.3 Pump current and derivative: suction . . . . . . . . . . . . . . . . . . . . . 39
5.4 Left ventricle short axis diameter . . . . . . . . . . . . . . . . . . . . . . . . 41
5.5 Physiological impacts of suction . . . . . . . . . . . . . . . . . . . . . . . . . 42
5.6 Reduced preload suction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43
5.7 Changing pump aspiration rates . . . . . . . . . . . . . . . . . . . . . . . . 44
5.8 Synchronous and asynchronous pump aspiration . . . . . . . . . . . . . . . 45
5.9 Sweeping the R-wave delay . . . . . . . . . . . . . . . . . . . . . . . . . . . 45
5.10 Suction event during different heart rates . . . . . . . . . . . . . . . . . . . 46
5.11 Pump parameters during suction event . . . . . . . . . . . . . . . . . . . . . 48
B.1 Pump and CVS Simulink Model . . . . . . . . . . . . . . . . . . . . . . . . 61
x

Chapter 1
Introduction and Literature
Review
In this work, a computational model of the motorized blood pump and cardiovascular system
has been developed in order to study the effects of ventricular collapse caused by mechanical
assist devices. To provide a background for this model, we will present a brief history and
overview of mechanical assist devices, an introduction to the mechanistic features of heart
failure, and a general overview of the structure and relevant phenomena of ventricular suck-
down.
1.1 Congestive Heart Failure
The heart is the organ that supplies blood and oxygen to all parts of the body. It is the
body’s natural blood pump, composed of four chambers (two atria and two ventricles) and
four heart valves (mitral, aortic, tricuspid and pulmonary). Blood coming back through
the pulmonary and systemic veins enters the left and right atria, respectively. The atria are
thin-walled compliant storage chambers which contract minimally, immediately preceding
the contraction of the ventricles during systole. During diastole, when the heart is at rest,
blood flows from the left and right atria into the left and right ventricles. The ventricles
serve as the main pumps for the system and are composed of thick muscle fibers. From the
left and right ventricles, blood is pumped into the systemic and pulmonary circulations. The
septum is a thick wall of cardiac muscle cells that separates two lower chambers from each
other. Electrical signals serve as the heart’s triggering mechanism, traveling first through
the atria, down the septum, and then on to the ventricles [24].
1

Figure 1.1: The heart: normal (left) and dilated (right).
Congestive heart failure (CHF) is a consequence (a sympotom) of a condition called
dilated cardiomyopathy (DCM). This disease is characterized by a severe decrease in the
heart’s ability to pump blood [8, 30]. The death rate for patients with severe CHF is about
50% within the first year, and 70% within five years. Even with advances in medicine and
science, those numbers are increasing, due to the fact that people are living longer and that
they are surviving cardiovascular disease and heart attacks more than any time in history
[29]. This effectively means that science has contributed to keeping people alive, but with
their heart in a weakened state [15].
There is no single cause of heart failure, instead a number of factors can contribute
to myocardial weakening. The most common ones are hypertension (high blood pressure)
and coronary artery disease, which often go one with another. Congenital heart defects may
also lead to CHF, as well as myocardial infarction (heart attack), cardiomyopathy, valvular
disease, heart tumors, etc [36]. Whatever the cause, the effect is almost always reduced
myocardial function and increased ventricular volume (Figure 1.1). There exist different
levels of heart failure, and a commonly used classification scale has been developed by the
New York Heart Association [5]. Refer to Table 1.1 for the classification scheme.
2

I Mild No limitation: ordinary physical exercise does not cause un-
due fatigue, dyspnoea or palpitations.
II Mild Slight limitation of physical activity: comfortable at rest but
ordinary activity results in fatigue, palpitations or dyspnoea.
III Moderate Marked limitation of physical activity: comfortable at rest
but less than ordinary activity results in symptoms.
IV Severe Unable to carry out any physical activity without discom-
fort: symptoms of heart failure are present even at rest with
increased discomfort with any physical activity.
Table 1.1: New York Heart Association heart failure classification system.
1.2 Mechanical Assist Devices
Mechanical assist devices are used for patients with a severe (class IV) heart failure. This
effectively means that no donor heart is readily available for transplantation, and in order
to sustain a life, mechanical assists are employed as a bridge to transplant. This is not the
only time when mechanical assists are used; they also serve as a destination therapy under
which the heart reverses remodeling process and restores close-to-normal flow rates [22].
Their use has therefore increased significantly in recent years [7].
Mechanical assist devices have been around for more than half a century. They were
first used in 1953 for cardiopulmonary bypass surgical procedure during which external
mechanisms keep the circulation of fluids going until the surgery is finished [14]. Today
there exist fully implantable artificial hearts as well as left ventricular assist devices, which
aid the cardiac output of the native heart, while allowing it to pump a portion of blood too.
It is important to note that the focus of this study is the LVAD.
Left ventricular mechanical assists are either pulsatile or continuous flow devices.
This means that the LVAD can be devised to operate as a positive displacement (piston)
pump or as a rotodynamic pump in which kinetic energy is added to the fluid by increasing
the flow velocity [26]. There have been several studies on the effects of the these two pump
types on the cardiovascular system. In vitro tests have proven that an optimally timed
pulsatile system is more effective at unloading a dilated heart [37, 38]. Nonetheless, in vivo
animal trials during heart failure have shown that end organ blood supply was not affected
by assist method [10]. In addition, Litwak et al. performed a series of in vivo and in vitro
experiments, concluding that pulsatile and continuous pumps are equally as effective at
aiding the delivery of blood to organs [19, 20, 21]. The pulsatile system may have a slight
clinical advantage, whereas continuous systems are much easier to implement and maintain,
3
and are much less prone to failure.
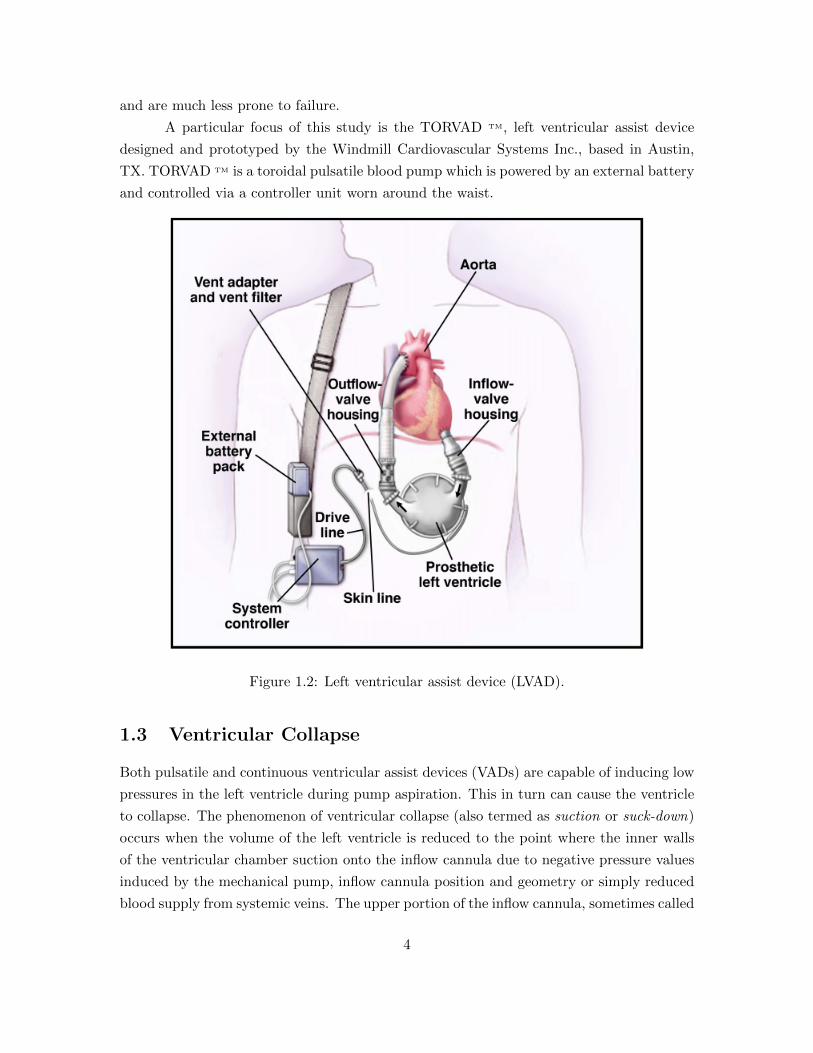
A particular focus of this study is the TORVAD TM, left ventricular assist device
designed and prototyped by the Windmill Cardiovascular Systems Inc., based in Austin,
TX. TORVAD TM is a toroidal pulsatile blood pump which is powered by an external battery
and controlled via a controller unit worn around the waist.
Figure 1.2: Left ventricular assist device (LVAD).
1.3 Ventricular Collapse
Both pulsatile and continuous ventricular assist devices (VADs) are capable of inducing low
pressures in the left ventricle during pump aspiration. This in turn can cause the ventricle
to collapse. The phenomenon of ventricular collapse (also termed as suction or suck-down)
occurs when the volume of the left ventricle is reduced to the point where the inner walls
of the ventricular chamber suction onto the inflow cannula due to negative pressure values
induced by the mechanical pump, inflow cannula position and geometry or simply reduced
blood supply from systemic veins. The upper portion of the inflow cannula, sometimes called
4

cannula tip, is a thin, solid tube that serves as the interface between the ventricular assist
device and the heart. Ventricular suck-down is extremely dangerous because it can cause
bruising (petechiae) or even tearing of the endocardial surface. As a consequence, chances
of heart arrhythmias rise and there is even a risk associated with blood clot formation.
Figure 1.3: Intramyocardial bruising of the swine’s heart due to suction. Note the dark red
spots in the vicinity of the inflow cannula.†
Ventricular collapse can also be damaging to the ventricular assist device due to the
rapid onset of the flow resistance and therefore high torque demands on the pump, which
can impair drive components or cause control instability. Hence, it is critical for a left
ventricular assist device to be able to prevent onset of a suction event.
Given that it is desired to unload the left ventricle in a patient with end stage
congestive heart failure (CHF), the LVAD needs to reduce the volume of the left ventricle
to relieve the wall stress caused by the distention of the ill myocardium. Since the left
ventricle is in failure, it cannot eject as much fluid and gets backed up with blood, causing
the ventricle to swell. Chronic wall stress induces cardiac remodeling and the heart grows
in order to try to eject more blood. In the long run, this turns out to be a futile attempt
because as the surface area inside of the ventricle increases, the heart must generate more
force to get the same pressure. The purpose of the mechanical assist is to relax the native
ventricle by relieving the wall stress and restore the blood flow rates back to healthy-heart
†Courtesy of Windmill Cardiovascular System, Inc.
5

values. Consequently, heart’s need for oxygen and glucose diminishes since it has to work
less, which leads to decline in heart rate (it drops down to normal 60 beats/sec instead
of 90 beats/sec, both at rest). In order to achieve this improvement, the LVAD must
remove significant volume of blood from the left ventricle which, on the other hand, puts
the ventricular walls at risk of sucking down onto the inflow cannula. Design parameters,
such as cannula geometry, ventricular morphology, mechanical assist actuation rates and
timing, cannula insertion site, etc., all have more or less significant effects on the probability
of ventricular collapse occurring. Knowing that several of these variables are outside of the
control of the designer, ventricular suction cannot be avoided passively while maintaining
high LVAD flow rates. Therefore, it is mandatory that the LVAD system controller be able
to detect the onset of a ventricular suck-down and take different forms of action to prevent
it from becoming a damaging event.
1.4 Suction Detection Schemes
Various methods have been used to detect and prevent the onset of the suction event. Most
of the continuous flow pumps, such as DeBakey VAD, have built in flow sensors, which
are simply monitoring the amount of fluid that passes through the pump at any instant.
Decline in the quantity of fluid sends a command to the controller unit, which then takes
appropriate action to prevent a complete ventricular collapse. Some of the LVAD systems
use other types of transducers, such as pump speed (RPM counters), to detect the onset of
a suction event [23]. Voigt et al. propose a combined input from speed and current sensors
to sense the onset of a suction event [39]. However, detecting suction via sensors is often
considered insufficient, although it may not necessarily be so as we will explore in this study.
In recent years, several approaches in addition to sensory input have been used to
solve the suction detection problem. These include frequency [43] and time based [40]
methods. However, Ferreira et al. managed to combine these two approaches into one. A
proposed scheme of a suction detector consisted of frequency domain techniques which were
supplemented by a time-frequency-based feature extraction algorithm of the pump flow
signal [12]. The frequency domain indices SI1 and SI2 correspond to the fluctuation in
energy of the harmonic and subharmonic contents of the pump flow signal respectively. The
time-frequency feature extraction algorithm detects variations in the standard deviation of
instantaneous frequency of pump flow. Obviously, this method requires a flow sensor to
monitor circulation rates.
Previous algorithms often trigger off one predefined suction threshold, which de-
pends on the mechanistic features of the pump. A suction detection system that combines
multiple hemodynamic indices to produce a more reliable and robust overall suction detec-
6

tor was investigated in [2]. Because there is a great variety of suction patterns, one index
may correspond better to a certain pattern than others. Hence, the combined response to
multiple suction indices can identify a broad range of patterns compared with a detection
relying on a single index.
1.5 Motivation
The TORVAD TM left ventricular assist device is a toroidal pulsatile blood pump that has
been prototyped by Windmill Cardiovascular Systems (Austin, TX). The pumping system
is unique in that it can be synchronized to aspirate its stroke at a known time in the cardiac
cycle. This can be used to aid in the prevention of the suction phenomenon. However, as
it has been observed in many animal trials, ventricular suction cannot be avoided by this
means alone. It is therefore desired to implement a sensing mechanism to detect the onset
of suction and to take control measures, such as stopping the VAD stroke entirely, when the
beginning of the suction event is detected. Given the necessary LVAD durability, size, and
mechanical simplicity, it is undesirable to implement a flow sensor or a pressure transducer
as a part of the TORVAD TM system. A proposed method to detect suction is to monitor
the motor current signal required by TORVAD TM and use it to predict torque requirements
on the motor. Because a suction event causes a rapid rise in inflow cannula resistance, this
will manifest itself in a rapid increase in motor torque and thus current. It is hypothesized
that a suction event will present a unique current spike which can be differentiated from the
normal motor currents for the TORVAD TM system and consequently used as a threshold
to prevent a full-blown suction event.
Chapter 2 introduces both a motorized pulsatile blood pump model and a cardio-
vascular system model, as well as the connection interface model between the two. Chapter
3 describes the parametrization of the model and, therefore, ventricular collapse (suction
event) through experimental trial and error methods, bringing the model and experimental
results together. Chapter 4 explores the most widely used suction detection schemes and
focuses on the most suitable one for TORVAD TM. Using the model, Chapter 5 defines
threshold values indicative of the suction event with TORVAD TM. Additionally, the same
chapter explores different scenarios during which ventricular collapse is more or less likely
to occur and how this phenomenon affects the cardiovascular system as well as the pump.
7

Chapter 2
Model of the Pulsatile Blood
Pump, Cardiovascular System, and
Connection Interface
This chapter presents two major models: a model of the motorized pulsatile blood pump and
a model of the human cardiovascular system (CVS). The developed pump model is based
on the permanent magnet direct current (PMDC) motors. The model of the cardiovascular
system consists of the left heart and the accompanying blood vessels, and it was adopted
from the master’s thesis written by Jeffrey Gohean [15] at The University of Texas at Austin.
The two models are coupled such that physical constraints are met: the pump draws the
blood from the left ventricle and supplies it to the aorta and, therefore, the rest of the CVS.
The interface between the two systems is modeled via orifice plate equation, which is based
on Bernoulli’s Equation.
The complete system was modeled via the Bond Graph technique and simulation was
carried out in The MathWorks TM, Simulink R© software package. The bond graph notation
describes dynamical properties of systems using standard elements that are coupled with
each other with the use of power bonds. The power bond connects the ports of the elements
and indicates the energy flow through the system. More information on modeling via Bond
Graphs can be found in the literature [3, 4]. The Simulink software package is a graphical
environment for multidomain simulation and model-based design for dynamic and embedded
systems.
The complete Bond Graph model of the system is shown in Figure 2.1. Separate
Bond Graph models of the pulsatile blood pump, cardiovascular system, and the interface
between the two are shown in Figures 2.3, 2.5 and 2.9, respectively.
8

R : Rmi
1 0
1
0
Se
R : Rat
C : Cat
Prs
Pat Qat
Plv Qsa 1
R : Rsa
Δ Psa
0
C : Csa
Psa ˙ Vsa
Qoc
Vat ˙
Qao
R : Rao
Δ Pao
Qic
1
Qmi
Clv Vlv ˙ elv ˙
Sf
Δ Pmi
0 Cla Vla ˙ ela ˙
Sf
Qrs
R : Rrs 1Δ Prs
Prs
Se
Pla
Δ Pat 1
T
R : Rorice
Δ Pori
Γ I : Ic ˙
Pp
Tp
Vlv
1
: r x Ap
I : Ip
Tr
R : Rb
h ˙ G
: Km
Tm ω
Vm
i
λ
1
Vr
R : Rm
Se Vs
I : L
˙
Cardiovascular System
Connection Interface
Rotary Blood Pump
1
Pc
0 C : Cc Δ Vc ˙
Figure 2.1: Overall model diagram.
9

2.1 Model of the Motorized Pulsatile Blood Pump
The mechanism that comprises the main portion of the motorized pulsatile blood pump is
shown in Figure 2.2. It consists of a direct current (DC) motor which drives two pistons
inside of a toroidal body via two links. Only one piston moves through the toroidal chamber
at a time, while the other is stationary and rests between inlet and outlet openings.
The wound-field DC motors are usually classified as shunt-wound, series-wound, and
compound-wound. In addition to these, permanent-magnet and brushless DC motors are
also available, normally as fractional-horsepower DC motors [31]. Permanent magnet DC
motors are used in applications which require relatively low torques and economic use of
space. Because the motor under consideration is driving a low-power pump (low torque)
that is implanted into patients (small size), we will model the motorized pulsatile blood
pump as a PMDC motor, even though a practical implementation may use a brushless DC
motor.
Motor
Outlet Inlet
Piston
Figure 2.2: Toroidal pulsatile blood pump.
A PMDC motor can be modeled very effectively with just a few parameters. These
10

normally include resistive parameters such as the friction in the rotor bearings and electrical
resistance in the coil windings, inductive term due to inductance caused by coil windings,
and the gyrator coefficient of the motor. Since the pump under consideration is a positive
displacement toroidal pump, the rotational inertia of the piston is yet another significant
design parameter, along with the piston area and its distance from the rotational axis. It is
important to emphasize that the piston motion is angular and for the purpose of this thesis
follows the equation
Piston Position =
∫480
(1− cos
(2π t
Tc
))dt, (2.1)
where t is time and Tc is the duration of pump stroke (time required for piston to make one
revolution) in seconds.
The amount of fluid displaced by this pump is determined by the volume inside of
the torus (less the piston volumes) and is given by
Stroke V olume = ApCt , (2.2)
where Ap is the piston area and Ct is the circumference of the torus.
1Se :V
i
R:R
mVri
I:L
λi
GYKm
Vm
i
τm
ω 1
R:R
bτrω
I:Ip
hω
TFr × Apτp
ω
Pp
Q
Figure 2.3: Toroidal blood pump Bond Graph.
State equations describing the dynamics of the pump in terms of flux linkage λ and
angular momentum h are outlined in equations (2.3) and (2.4), respectively. Position of the
rotor is monitored through an information state θ (equation (2.5)), which is being detected
11

by an angular-velocity to angular-position sensor model. The desired piston position, also
termed tracking curve, is controlled via proportional-integral-derivative (PID) controller.
Note that the control variable is the supply voltage V , where a power supply of about 14V
is assumed available. Thus, in this model, saturation limits impose upper and lower bounds
on input signals in order to suppress unlimited draw of power.
λ = V − Rm
Lλ− Km
Iph (2.3)
h =Km
Lλ− Rb
Iph− rApPp (2.4)
θ =
∫ω(t) dt =
∫1
Iph(t) dt (2.5)
The values used in this model, shown in Table 2.1, were adopted from the left
ventricular assist device called TORVAD TM, prototyped by the accompany named Windmill
Cardiovascular Systems based in Austin, TX.
Motor Parameter Symbol Value Units
Supply Voltage V 10− 14 V
Gyrator Coefficient Km 0.124 V secrad
Two Phases in Series Resistance Rm 2.6 Ω
Damping Coefficient Rb 8.1× 10−5 Nmsecrad
Two Phases in Series Inductance L 2.58× 10−3 H
Inertia of the Rotating Piston Ip 1.851× 10−5 kgm2
Area of the Piston Ap 2× 10−4 m2
Distance from the Rotation Axis r 0.03 m
Stroke Volume ∀s 37.6 ml
Table 2.1: Typical PMDC parameter values used for simulation in this thesis.
12

2.2 Model of the Cardiovascular System
Several comprehensive models of the cardiovascular systems have been developed in recent
years [1, 15, 18]. Gohean developed a computational model specifically to study the effect
of mechanical assist devices on the cardiovascular system [15]. Both the systemic and
pulmonary circulation have been modeled to complete the loop around the area of focus,
namely the aorta and large arteries. This thesis however, adopts only the model of the left
heart (left ventricle and left atrium), along with the accompanying left heart valves (mitral
and aortic), and the systemic circulation (arteries and arterial tree) from Gohean’s work.
As the left heart comprises the biggest portion of the myocardial muscle, and since LVADs
are connected to the heart at the left ventricular apex site, the adopted portion of Gohean’s
model appears sufficient to study ventricular collapse.
Pulmonary Circulation
Systemic Circulation
Arterioles
Capillaries
Arteries
Veins
Veins
Heart
Valve
Arteries
ArteriolesCapillaries
LA LV
RV RA
C ( t)
A
B B
B
BB
1
23
4 6
57
9
10111213
14 15 B1617
18 B1920 20
2121
22B22
B B24 24
23 23
8
BB
BB
B
x
yz
p
α β
1
αβαβ
β
β
αβ
α
α
α
α β α β
2
3
4
α β3
α β3
22
2
3
2
αβ2
Figure 2.4: Cardiovascular system schematic, from [15]. Only left heart along with the
systemic circulation has been adopted (marked in red).
The model is shown in Figure 2.5 in terms of Bond Graph modeling technique.
Detailed description of the model, including parameters and ordinary differential equations,
is outlined in Appendix A.
13

R : Rmi
1 0
1
0
Se
R : Rat
C : Cat
Torvad
Prs
Pat Qat
Plv Qsa 1
R : Rsa
Δ Psa
0
C : Csa
Psa ˙ Vsa
Qoc
Vat ˙
Qao
R : Rao
Δ Pao
Qic
1
Qmi
Clv Vlv ˙ elv ˙
Sf
Δ Pmi
0 Cla Vla ˙ ela ˙
Sf
Qrs
R : Rrs 1Δ Prs
Prs
Se
Pla
Δ Pat TM
Figure 2.5: Cardiovascular system Bond Graph.
Subscript Definition
rs Right side pulmonary venous return
la Left atrial
mi Mitral
lv Left ventricular
ao Aortic
ic Inlet cannula
oc Outlet cannula
sa Systemic arteries
at Arterial tree
Table 2.2: Subscript definitions for the cardiovascular system Bond Graph.
14

2.3 Model of the Pump-CVS Interface
Patients suffering from congestive heart failure (CHF) often receive mechanical assists as
a bridge to real heart transplantation or as a method of therapy under which the heart
undergoes remodeling to its original shape. A mechanical assist device is interfaced to
the ventricular chamber via cannula. Most often, the left ventricular apex is chosen as
the site for pump cannula tip insertion. One such cannula tip was designed by Windmill
Cardiovascular Systems and is employed with the TORVAD TM left ventricular assist device.
Note that the cannula tip shown in Figure 2.6 is made out of plastic material for the research
purposes. Clinical cannula tips have identical geometry, albeit made out of steel. The
cannula tip shown was fabricated only for in vitro testing.
Figure 2.6: Inflow tip, designed by Windmill CVS.
Ventricle-to-pump fluid coupling losses can be modeled via orifice flow relations.
Namely, the flow from the heart can be modeled similar to the flow from a pipe with large
diameter relative to an orifice. As fluid flows through this pipe, it encounters a narrow
section and it is forced to converge. Pressure and velocity change as a consequence of a
change in flow area [26]. It turns out that the pressure at point (1) in the figure below is
larger than at point (2) within the vena contracta (the point in a fluid stream where the
diameter of the stream is the smallest).
15

Figure 2.7: Fluid flow through orifice, from [26].
In the absence of viscous effects, Bernoulli’s equation can be applied at two points
on the streamline which passes through the middle of the interface:
P1 +1
2ρV1
2 + ρgz1 = P2 +1
2ρV2
2 + ρgz2 , (2.6)
where P is the thermodynamic pressure of the fluid as it flows (sometimes termed as static
pressure), 12ρV
2 is the dynamic pressure, and ρgz is the hydrostatic pressure, due to po-
tential energy variations of the fluid as a result of change in elevation [26]. Under the
assumption of a horizontal setup (no change in elevation), hydrostatic pressure terms can-
cel out in Bernoulli’s equation, which then simplifies to
∆Pori =1
2ρV2
2 − 1
2ρV1
2 , (2.7)
where ∆Pori = P1 − P2 is the pressure across the orifice. Based on the fluid dynamics laws
of conservations, which are expressed using the Reynolds Transport Theorem, the mass and
therefore the flow is conserved inside of the pipe:
Q = A1V1 = A2V2 ⇒ V1 =A2V2A1
, (2.8)
where A1, A2 and V1, V2 are cross sectional areas and velocities at points (1) and (2).
Substituting V1 into equation (2.7), and solving for velocity at point (2) we get
V2 =
√2(∆Pori)
ρ(1− β4), (2.9)
where β = D2/D1 (ratio of the diameters at points 1 and 2). Note that non ideal effects
occur for a couple of reasons: 1) vena contracta area A2 is less than the area of the orifice
Ao by some percentage (A2 = CcAo) and 2) turbulent flow near the cannula introduces a
16
loss which cannot be calculated theoretically. Hence, an orifice discharge coefficient, Cd is
used to accommodate for these phenomena. The equation (2.8) finally becomes
Q = CdAo
√2(∆Pori)
ρ(1− β4), (2.10)
where Ao = πd2/4 (refer to figure 2.7). It is important to realize that Cd is a function of
β = d/D and Reynolds number Re = ρV D/µ, where V = Q/A1. Nominal values of Cd
are in the vicinity of 0.6; however, they also depend on the geometry of the orifice plate
(cannula), whether the edges are beveled or sharp on the cannula, placement of pressure
taps etc. Thus, it is usually necessary to experimentally determine the value of the discharge
coefficient Cd for cannula in order to parameterize this model accurately.
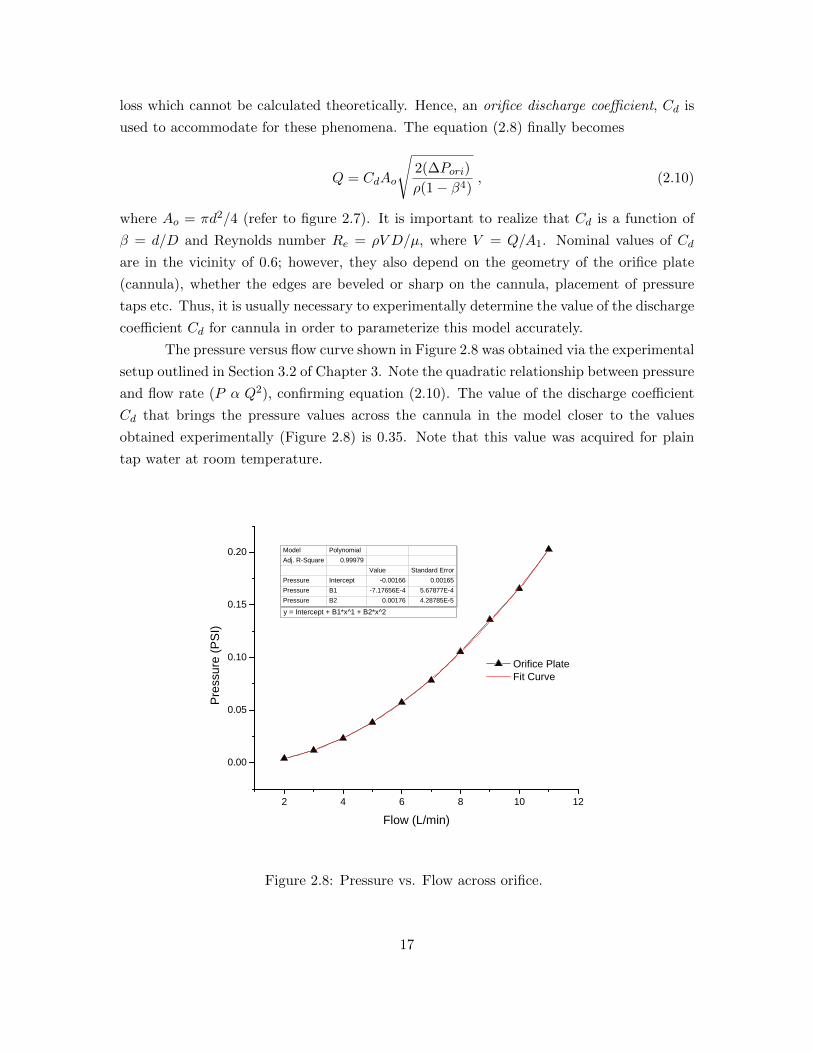
The pressure versus flow curve shown in Figure 2.8 was obtained via the experimental
setup outlined in Section 3.2 of Chapter 3. Note the quadratic relationship between pressure
and flow rate (P α Q2), confirming equation (2.10). The value of the discharge coefficient
Cd that brings the pressure values across the cannula in the model closer to the values
obtained experimentally (Figure 2.8) is 0.35. Note that this value was acquired for plain
tap water at room temperature.
2 4 6 8 1 0 1 2
0 . 0 0
0 . 0 5
0 . 1 0
0 . 1 5
0 . 2 0
O r i f i c e P l a t e F i t C u r v e
Pressu
re (PS
I)
F l o w ( L / m i n )
Model PolynomialAdj. R-Square 0.99979
Value Standard ErrorPressure Intercept -0.00166 0.00165Pressure B1 -7.17656E-4 5.67877E-4Pressure B2 0.00176 4.28785E-5y = Intercept + B1*x^1 + B2*x^2
Figure 2.8: Pressure vs. Flow across orifice.
17
1 0
Qoc = Qp
Qic
Clv
1 R : Rorice
Δ Pori
Γ I : Ic ˙
Pp
Vlv
: r x Ap
1
Pc
0 C : Cc Δ Vc ˙
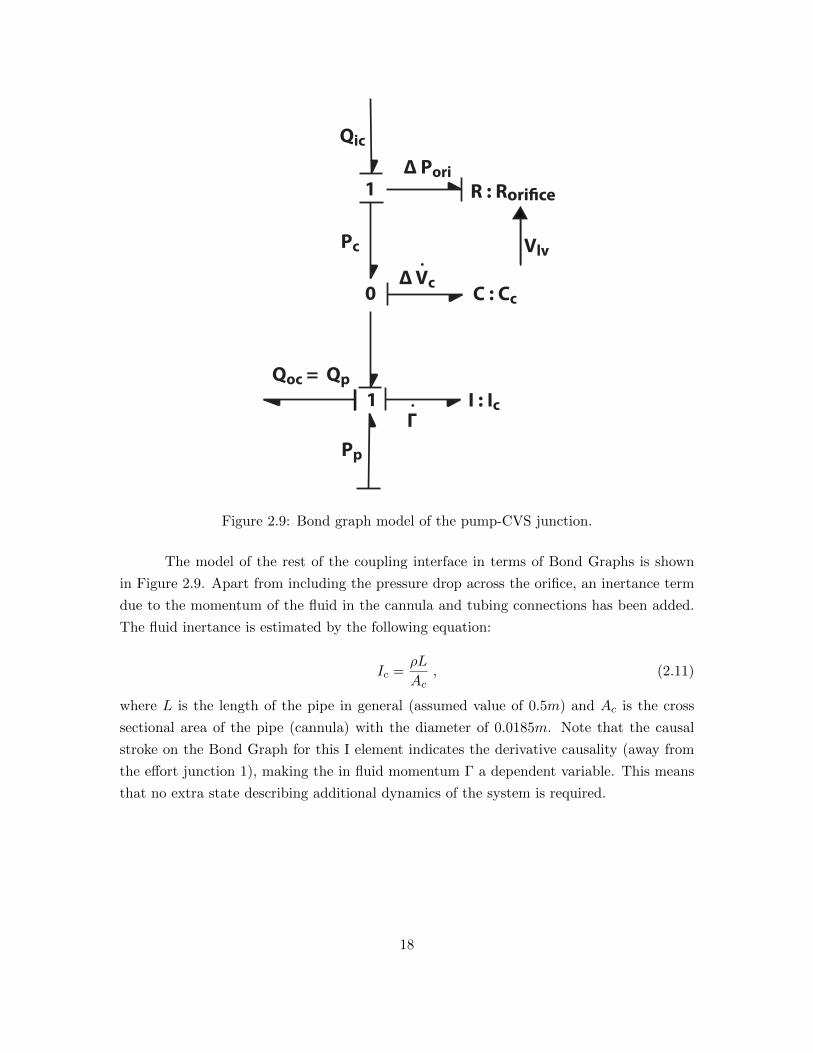
Figure 2.9: Bond graph model of the pump-CVS junction.
The model of the rest of the coupling interface in terms of Bond Graphs is shown
in Figure 2.9. Apart from including the pressure drop across the orifice, an inertance term
due to the momentum of the fluid in the cannula and tubing connections has been added.
The fluid inertance is estimated by the following equation:
Ic =ρL
Ac, (2.11)
where L is the length of the pipe in general (assumed value of 0.5m) and Ac is the cross
sectional area of the pipe (cannula) with the diameter of 0.0185m. Note that the causal
stroke on the Bond Graph for this I element indicates the derivative causality (away from
the effort junction 1), making the in fluid momentum Γ a dependent variable. This means
that no extra state describing additional dynamics of the system is required.
18

Qoc
Qic
R L
Figure 2.10: Model of the elastic tube.
Besides the inertia of the fluid that is developed as the fluid flows through the
cannula, the elastic effect of the cannula itself was modeled. Namely, for an incompressible
fluid, we can determine the expression for the capacitance of the tube’s elastic effects, since
the tube expands. After the expansion, the area of the cannula is
Af = πR2f = π(R+ ∆R)2 = πR2 + 2πR∆R+ π(∆R)2 , (2.12)
where R is the original radius and ∆R is the change in the original radius. ∆R, which
represents expansion in the radial direction, can be approximated from formulas for stress
and strain [42], yielding
∆R =PR2
Et(1− ν
2) , (2.13)
where P is external pressure, E is Young’s elastic modulus of the cannula material, t is
the thickness of the cannula, and ν is Poisson’s ratio of the cannula material. In reality,
the inlet cannula may be made from a material such as expanded polytetrafluoroethylene
(ePTFE), which is completely inert and extremely biocompatible; the body does not reject
parts made out of this material.
Parameter Definition Value
L Cannula length 0.5m
t Cannula thickness 0.003m
R Cannula radius 0.0184m
E ePTFE Young’s modulus 0.5GPa
ν ePTFE Poisson’s ratio 0.46
Table 2.3: Relevant design parameter for the inlet cannula.
19

Neglecting the last term on first approximation, equation (2.12) reduces to
Af = πR2 + 2πR∆R = A+ ∆A. (2.14)
Therefore, the volume change due to tube expansion is
V ∼= (∆A)L = 2πRR2L
Et(1− ν
2)P. (2.15)
Recognizing the original volume term of the cannula (Vo = πR2L) in the above
expression we can rewrite the above equation as
V =2VoR
Et(1− ν
2)P ⇒ P =
1
CcV , (2.16)
where Cc is the elastic compliance for expansion∗ of the cannula used in the model
Cc =2VoR
Et(1− ν
2). (2.17)
Sources of effort such as Plv, Psa, and Pp are defined from the cardiovascular system
model and the model of the toroidal pulsatile pump, respectively. Inflow cannula flow Qic
and outflow cannula flow Qoc dictate the change of volume inside of the elastic canula.
Outflow cannula flow Qoc is equal to that of the pump Qp since no elastic effects were
modeled inside the pump.
2.4 Initial Verification of the Model
This section shows several test cases that verify the functionality of the base model. One
way to verify the model is to plot so called PV Loops of the patient data and the model,
and hence investigate how they compare. Left ventricular pressure-volume (PV) loops are
derived from pressure and volume values found in the cardiac cycle. To generate a PV loop
for the left ventricle, the left ventricular pressure is plotted against left ventricular volume
at multiple time points during a complete cardiac cycle.
∗Note that a different compliance could be required for collapse of the cannula.
20

Figure 2.11: A case study of measured LV pressure, volume and wall thickness during a
cardiac cycle of a healthy person (left). Relationship between LV volume and pressure
(right).
Figure 2.11 shows an example of a patient’s measured LV pressure, volume and wall
thickness during a cardiac cycle. Looking at the right portion of the above figure, points
21-36 constitute the blood filling phase, 1-5 constitute the isovolumic contraction phase, 5-
17 constitute the blood ejection phase, and 17-21 constitute the isovolumic left ventricular
relaxation phase [44, 45].
0 20 40 60 80 100 120 140 1600
20
40
60
80
100
120
140
160
V(mL)
P(m
mH
g)
Figure 2.12: PV Loop obtained via cardiovascular system model
21

Figure 2.12 shows the plot of several cardiovascular cycles (heart beats) of the healthy
left ventricle. Note that the blue lines eventually start to overlap, signaling that the model
has reached a steady state. On average, ventricular volume is at 110ml (vertical line through
the middle of the PV Loop) and the average left ventricular pressure is about 80mmHg
(horizontal line through the middle of the PV Loop), which is very similar to the values
on the previous page. The volume of the blood that gets ejected with each heart beat is
contained within two vertical isovolumic lines, and this value is 70ml on average.
0 50 100 1500
20
40
60
80
100
120
140
160
180
V(mL)
P(m
mH
g)
Figure 2.13: PV Loop obtained via cardiovascular system model, with pump attached
Figure 2.13 shows how the overall model performs with the model of a toroidal
pulsatile blood pump attached to the cardiovascular system model. Note that the volume
of the left ventricle is constantly changing as we go around the PV loop (slanted vertical
lines). This means that there is no isovolumic period during the cardiac cycle; rather the
pump is altering the left ventricular volume constantly as it actuates along with the heart.
Now that we have verified that the joint model of the pump, cardiovascular system
and the interface between them works, we will go ahead and attempt to model ventricular
collapse. The phenomenon of the ventricular suck-down will be superimposed on top of the
base model described in this chapter.
22

Chapter 3
Experimental Suction
Parameterization: Variable Orifice
Resistance
The model described in Chapter 2 has been further parameterized in this chapter to simulate
suction event dynamics inside of the left ventricle. The suction event has been superimposed
onto the base model described earlier. This chapter describes the process of obtaining
relevant parameters that would enable modeling and simulating suction events. The chapter
includes a section on development of a physical approximation of the left ventricle as well
as a section on experimental estimation of ventricular collapse using data from testing with
an artificial left ventricle and a mock circulatory loop.
3.1 Ellipsoidal Approximation of the Left Ventricle
Left ventricle shape and hence the volume is often approximated via ellipsoid [32, 33].
Volume of an ellipsoid is given by
V =4
3πabc,
where a, b and c are elliptic radii.
Assuming that two of the radii are same and that the LV appears as half of an
ellipsoid, the above equation becomes
V =4
6πab2. (3.1)
Equation (3.1) was used to design an artificial left ventricle, along with the LV ge-
23

ometry data obtained from the literature. Taking into account end diastolic left ventricular
volume of a healthy person, atrioventricular plane to heart apex distance (long axis), diame-
ter of the left ventricle (short axis distance) and the ventricular wall thickness, the following
3D model was developed in SolidWorks CAD design software:
(a) (b)
Parameter Value
Volume (ml) 120∗
Long Axis (mm) 84†
Short Axes (mm) 26.12‡
Wall Thickness (mm) 12∗
Interface Length (mm) 50.8§
(c)
Figure 3.1: LV computer aided design: (a) Triangle edges; (b) Shaded; (c) Dimensions.
3.1.1 LV Rapid Prototyping and LV Silicon Mold
Rapid prototyping (RP), a fast turnaround additive manufacturing technology, was used
to fabricate the part shown in Figure 3.1. Once the SolidWorks part was developed and
converted into RP machine readable format, the file was submitted for manufacturing.
The end product of this process was a rigid left ventricle shown in Figure 3.2. Next,
this rigid part was used to create a two-part silicon mold, which on the other side was meant
∗Values from [13, 9]†Values from [34]‡Value determined from eq. 3.1, by specifying LV volume and long axis radius§Cylindrically shaped mock loop interface of length L = 50.8mm (2in) was added to the ellipsoid
24

to help create a flaccid ventricle. A more elaborative explanation on creating soft ventricle
is contained in Subsection 3.1.2.
The left ventricle mold was made out of “kneand-a-mold” artisan clay, which is a
platinum cured silicone mold making system. This material was placed on top of the rigid
left ventricle as well as inside of it, and was left to cure for an hour. The resulting two-part
mold is shown in the following figure, along with the rigid RP ventricle.
(a) (b)
(c) (d)
Figure 3.2: LV mold making process: (a), (b) Rapid prototyped ventricle; (c), (d) Silicon
mold.
3.1.2 Mock Loop Ventricle
The final stage of the design is realization of a soft left ventricle that is capable of ap-
proximating material properties of cardiac muscle. The heart muscle has heterogeneous
elasticity traits that are hard to mimic within one artificial ventricle. Sarcomere, which is a
single muscle cell, changes its elasticity depending on whether the heart muscle is in systole
(contraction) or diastole (relaxation). Furthermore, heart muscle elastic modulus in the
longitudinal or meridional direction is different from that in the latitudinal or circumferen-
tial direction [41]. Thus, a static elasticity value of a heart muscle in diastole was chosen
as an approximation to human heart elastic qualities. Young’s modulus of a cardiac muscle
in diastole ranges from 46kN/m2 to 100kN/m2 according to Yettram et al. [41]. Pao et
al. [28] used a simpler cross-sectional analysis of the left ventricle and suggested a diastolic
25

value of 92kN/m2.
In order to achieve the above mentioned values for left ventricular Young’s modulus,
arbitrary heart-like elastic materials were tried. Among others, polyvinyl chloride with
phthalate plasticizer, often termed as plastisol, seemed to satisfy the requirements. Plastisol
is a white, milk-like base to which softeners and hardeners can be added to achieve desired
stretchiness and/or stiffness. The cure time for plastisol is temperature dependent: the
higher the temperature, the faster the cure¶. Hot material can be poured into molds and
left to cool down to room temperature. A Collapsible left ventricle is shown in Figure 3.3.
(a) (b)
Figure 3.3: Mock loop left ventricle: (a) Supine position and (b) Standing position.
Several different ratios of the base material and softener were tried until cured plas-
tisol Young’s modulus matched that of a heart in diastole. Experimental procedures showed
that four parts of plastisol base P0010RB to one part of softener RD-55 achieved Young’s
modulus of 72.6kN/m2 on average, which falls within the range found in the literature
for diastolic elasticity values. Recall that the slope of the stress versus strain curve is the
Young’s modulus of elasticity:
E ≡ tensile stress
tensile strain=σ
ε=
F/A0
∆L/L0=
FL0
A0∆L
where,
• E is the Young’s modulus (modulus of elasticity)
• F is the force applied to the object
• A0 is the original cross-sectional area through which the force is applied
• L is the amount by which the length of the object changes
• L0 is the original length of the object.
¶Manufacturer (QCM COMPANY INC.) does not recommend going above 380-400 F as that can resultin burned plastisol
26

3.2 Experimental Estimation of Flow Characteristics during
Ventricular Collapse via Mock Circulatory Loop
Parametrization of flow characteristics during a suction event was done experimentally with
the aid of mock circulatory loop. Mock circulation loops are generally used to evaluate the
performance of cardiac assist devices prior to animal and clinical testing [16]. A compress-
ible, translucent plastisol chamber that mimics the size, shape and motion of a left ventricle
is desired to assist in pressure/flow studies around inflow cannula during VAD support.
The aim of this study was therefore to design and construct a mock circulation loop with a
naturally shaped flexible left ventricle and evaluate its performance during suction events.
The data extracted during this series of experiments was used to parametrize the
model outlined in the previous chapter in order to study effects of ventricular collapse on
the mechanical assist device and human cardiovascular system.
Figure 3.4: Mock loop schematic.‖
Yuhki et al. [43] have performed studies with the mock circulatory loop and artificial
silicon ventricle in order to study ventricular collapse. In particular, intention was to detect
suction and flow regurgitation based on the motor current waveform so that pump operation
mode can be optimized and patient saved from potential suffering. Similar mock loops were
developed by others though for different purposes. Cassot et al. [6] developed a physical
model to simulate left heart and systemic circulation. In addition, they wanted to visualize
‖Components of the loop are not drawn to scale.
27

flow patterns inside of the ventricle at the early filling stage as well as at the onset of
ventricular systole. Pantalos et al. [27] saw mock circulation fit to test mechanical assist
devices for healthy and pathological states. They argued that in vitro studies via these
loops should be well suited for developing experimental protocols, testing device feedback
control algorithms, investigating flow profiles, and training surgical staff on the operational
procedures of cardiovascular devices.
Majority of these loops consist of a combination of the following components:
• pneumatically driven artificial left ventricle
• mechanical assist device
• pressure, flow, velocimeter sensors
• visualization aids (dye, scope, cameras)
• arterial/aortic compliance chamber
• tubing of certain length
• restrictions to flow simulating resistance,
and the outline of the ones used to parametrize the ventricular collapse in this study is
shown in Figure 3.5.
28

(a)
# Item
1 Instrumentation amplifier
2 Power Supply 1
3 Power Supply 2
4 Oscilloscope
5 Biomedicus pump
6 Flow Probe
7 Differential pressure sensor
8 Inflow cannula
9 Artificial ventricle
10 Pressure resorvoire
(b)
Figure 3.5: Mock circulatory loop: (a) Experimental setup and (b) Components.
29

The Medtronic bio-pump called BioMedicus is a centrifugal blood pump used for
extracorporeal circulatory support for patients under cardiopulmonary bypass (a technique
which temporarily substitutes the function of the heart and lungs during surgical procedure).
The pump impeller has a series of smooth-surfaced rotating cones which pull the blood into
the vortex created by the rotation, after which the blood is propelled out of the system.
The flow probe TX-40 comes factory calibrated and interfaces through a connector to the
control console.
Figure 3.6: Bimedicus centrifugal blood pump and the flow probe.
A differential pressure sensor (OMEGAs PX26-001DV) was placed across the cannula
tip since the pressure change should manifest itself at this site at the moment of ventricular
suck-down. The PVC cannula tip that is inserted into the artificial ventricle reflects the
pristine design of the steel tip utilized with TORVAD TM, left ventricular assist device
prototyped by Windmill Cardiovascular Systems, Inc.
Figure 3.7: Differential wet-to-wet pressure transducer placed across cannula tip.
30

Figure 3.8: Experimental suction parametrization: Measurements were taken while the
volume of the left ventricle was varied with the clamp.
0 2 4 6 8 1 0 1 20 . 0
0 . 1
0 . 2
0 . 3
0 . 4
0 . 5 L V V o l u m e = 1 2 0 m l L V V o l u m e = 9 6 m l L V V o l u m e = 7 2 m l L V V o l u m e = 4 8 m l L V V o l u m e = 2 4 m l L V V o l u m e = 1 0 m l
Pressu
re (ps
i)
F L o w ( L / m i n )Figure 3.9: Experimental suction parametrization : P vs. Q. Resistance value (flow coeffi-
cient) increases as the ventricle collapses.
31

0 . 0 0 0 0 0 0 . 0 0 0 0 4 0 . 0 0 0 0 8 0 . 0 0 0 1 20 . 0 0 E + 0 0 0
1 . 0 0 E + 0 1 0
2 . 0 0 E + 0 1 0
3 . 0 0 E + 0 1 0
4 . 0 0 E + 0 1 0
5 . 0 0 E + 0 1 0
6 . 0 0 E + 0 1 0 R e s i s t a n c e E x p o n e n t i a l F i t o f R e s i s t a n c e
Resis
tance
(Pa m
3 )/sec
L V V o l u m e ( m 3 )
Equation y = y0 + A*exp(R0*x)Adj. R-Square 0.88535
Value Standard ErrorResistance y0 3.3267E10 5.52756E9Resistance A 4.56144E10 7.75395E9Resistance R0 -28689.58334 14619.71142
Figure 3.10: Experimental suction parametrization: Rorifice vs. Vlv obtained from figure
3.9.
Dependency of the resistance (flow coefficient) on the left ventricular volume is ex-
pressed in equation (3.2). This relation is used to modulate resistance values across the
cannula interface during ventricular collapse (Figures 2.1 and 2.9, connection interface sec-
tion). Implementation of the volume-based resistance brought together experimental results
and the Simulink model.
Rorifice = 3.26E10 + 4.56E10e−28689.6Vlv (3.2)
The above expression was used as a means of inducing ventricular suction event in
the model. The following chapter will get the reader familiarized with a suction detection
algorithm proposed for detecting the onset of a ventricular collapse.
32

Chapter 4
Suction Detection Algorithm
This chapter investigates suction detection schemes and focuses on the most plausible one
based on the mechanistic features of the TORVAD TM system and experience of engineers
working at Windmill Cardiovascular Systems, Inc.
Suction has been investigated for pumps involved in heavy industry applications such
as sewage systems, water supply networks etc., in order to prevent malfunctioning of the
pumping mechanisms due to clogging [35]. In addition, occurrence of suction phenomenon
and its detection has been studied in left ventricular assist devices [2, 12, 23, 39, 40, 43], as
outlined in the introductory chapter, Section 1.4. It is important to understand implications
of the suction phenomenon well in order to be able to approach and solve the problem
appropriately. For instance, its occurrence is highly undesirable, even for short periods of
time for it can induce high torque demands and damage the pump system performance,
causing instability problems. More importantly, suction events can leave petechia (bruises)
on the ventricle walls and interventricular septum (the wall separating the left and right
ventricles of the heart). Occurrence of ventricular suck-down can also induce tachycardia,
which is a heart rate that exceeds the normal range for a resting heart beat [36].
Multiple, readily available signals can be used as indices of an imminent suction
event. Variations in the flow, speed, current, and power waveforms (or their combination)
are often employed as mechanisms to detect the onset and/or presence of ventricular col-
lapse. Processing and analysis of these inherent pump system parameters can be done in
time [40] and frequency domains [43]. Time domain mechanisms include correlation tech-
niques as well as linear and non-linear signal processing. Frequency domain mechanisms
include various real-time spectral analysis methods using different kinds of Fourier Trans-
forms (FFTs and DFTs), as well as other linear and non-linear signal processing techniques.
Section 4.1 of this chapter introduces some commonly used suction detection schemes
for LVADs in general. Section 4.2 focuses on arguably the most suitable suction detection
33

algorithm for TORVAD TM left ventricular assist device.
4.1 Detection Methods
An extensive list of suction detection schemes is outlined in the patent called Method and
System for Detecting Ventricular Collapse [25]. We will go through few items on this list
and present advantages and disadvantages of each method, in an attempt to identify the
most viable one for a positive displacement toroidal pump, such as the TORVAD TM.
4.1.1 Sensory Input Alone
In certain designs, such as the DeBakey LVAD, the flow signal provided via the flow sensor or
flow meter is specifically analyzed for suction detection. Monitoring the flow rates through
the pump is considered an acceptable method of detecting suction, although not the most
assuring one. In addition to only one sensory input, a combination of several of these signals
such as motor current, power and speed may be used to avoid false positives for instance.
However, this means alone (via sensors) is often considered insufficient, and additional signal
processing is used to get positive triggers when suction event occurs.
4.1.2 Harmonic Distortion Analysis of a Signal
Fluctuations in the flow, speed, current, and power signals in the time-domain will result in
corresponding variation in their frequency-domain representations. Thus, real time spectral
content information of these signals may be used to detect ventricular collapse. Several
kinds of suction indices can be generated based on harmonic spectral analysis:
i) harmonic distortion
ii) total spectral distortion (harmonic distortion and noise)
iii) sub-fundamental distortion (distortion below the fundamental frequency)
iv) super-fundamental distortion (distortion above the fundamental frequency)
v) the ratio of the super-fundamental distortion to the sub-fundamental distortion
vi) super-physiologic distortion (distortion at frequencies above the assumed maximum
physiologic fundamental frequency-typically 4 Hz or 240 BPM)
vii) and the spectral dispersion or “width” of the resulting flow waveform.
The potential drawback of this method is that it can be computationally expensive. Onset
of a suction event may go undetected if the controller is not fast enough and does not have
digital signal processing (DSP) capabilities. This method also poses an issue of defining
34

what is meant by a real-time frequency spectrum of a signal. Again, we find an answer
by determining how fast a micro-controller can execute all the operations and produce a
probability index of the suction event in a timely fashion, preventing a complete ventricular
collapse.
4.1.3 Spectral/Time Domain Masking
In addition to spectral harmonic indices previously described, spectral content of the mea-
sured signal may be used differently to detect onset of a suction event. Essentially, the
spectral content generated by the FFT is compared to a predetermined spectral mask.
Hence, the presence of a suction event is determined based on the comparison. The signals
whose spectral components fall within the mask indicate suction and, conversely, signals
whose spectral components fall outside the mask indicate normal operating conditions.
A similar approach can be used for time domain analysis methods. A particular
method cross-correlates the incoming time-sampled signal (for example, the flow or cur-
rent signal) with predetermined time-domain waveforms which exemplify the imminence of
ventricular suck-down. The mask waveforms are selected sequentially or are based on the
probability of occurrence in that particular patient derived experientially through clinical
evaluation. A correlation coefficient signifies a perfect match or indicates no correlation at
all. The correlation coefficient is compared to predetermined thresholds to derive a suction
probability index. If the calculated correlation coefficient exceeds a predetermined value,
ventricular collapse is imminent. Conversely, if the calculated correlation coefficient is below
the predetermined value, suction is not present.
Drawbacks of the spectral masking method are identical to the Harmonic Distortion
Analysis method, that is, a lack of micro-controller computational power may produce non-
real-time triggers. A time domain approach relies on experimentally determined masks
that are obtained via clinical evaluation of patients. Given that mechanical assist devices
go through rigorous animal trials before they are approved for clinical usage in patients,
this method may not be the most appropriate, since suction detection should be operational
from the moment a patient receives an implant.
4.2 Suction Detection for TORVAD TM
The TORVAD TM left ventricular assist device is a pulsatile positive displacement toroidal
blood pump. The algorithm under consideration was derived based on the mechanistic
features of the TORAVD system and computational abilities of the micro-controller unit.
As it was described earlier, suction detection schemes need some kind of a sensory input
35

(flow, current, speed etc.) and some sort of a processing algorithm that behaves in a robust
manner.
The TORVAD TM ventricular assist device provides two types of inherently available
signals: a) piston position (and therefore velocity) and b) current magnitudes, which are
closely related to the amount of torque inquired by the pump due to the change in load.
The proposed scheme consists of two steps:
1. The current signal may be combined with motor position error as a means for imple-
menting the needed motor action to prevent further suction.
2. Additional signal analysis is desired as a means of providing not only algorithm re-
dundancy but also supplementary suction event thresholds. The time derivative of
the pump’s current i can be calculated and used as an extra precaution:
di(t)
dt=−i(to + 2∆t) + 8i(to + ∆t)− 8i(to −∆t) + i(to − 2∆t)
12∆t+ ϑ(∆t)4 (4.1)
In numerical analysis, given a line grid in one dimension, the five-point stencil of a
point in the grid is made up of the point itself together with its two adjacent neighbors on
each side. It is used to write finite difference approximations to derivatives at grid points.
Note that the above formula is fourth order in accuracy ϑ(∆t)4, and that it follows from
the Taylor’s Series expansion around the central point [11]. Time step ∆t is defined as a
reciprocal of the sampling frequency fs.
36

Chapter 5
Results
Having made a base model in Chapter 2 (the pump, cardiovascular system and the can-
nula/tube interface) and experimentally parametrized suction flow characteristics in Chap-
ter 3, with a suction detection algorithm (Chapter 4) we proceed into evaluating how these
three systems interact with each other. This chapter presents several test cases that were
used to investigate likeliness of a suction event occurrence, and evaluate suction detection
algorithm. In addition, this chapter describes examples of suction events obtained during
animal trials with TORVAD TM and compares those to the ones obtained from simulations.
Lastly, the chapter also depicts how ventricular collapse affects the cardiovascular system
as well as the pump.
5.1 Defining Thresholds
The following figures compare the regular mode of operation of the model against the in
vivo animal trial data, for verification purpose. Suction thresholds were determined based
on the figures presented in this section and they indicate the onset of a suction event.
It is hypothesized that suction events will produce higher torque demands on the motor
than usual during ventricular collapse, which, by virtue of how the motor operates, will
require higher draw of power, manifested in the sudden current increase. Hence, based on
the observation of Figure 5.1 we can safely note that normal mode of operation does not
require current amplitudes higher then approximately 0.7 amperes for the model, and 0.6
amperes for the animal trial case.
37
0 . 0 0 0 . 7 5 1 . 5 0 2 . 2 5 3 . 0 0 3 . 7 50 . 0
0 . 2
0 . 4
0 . 6
0 . 8
1 . 0
t ( s e c )
Curre
nt (Am
p)
0
3 6 0
7 2 0
1 0 8 0
1 4 4 0
1 8 0 0
Piston
Positi
on (D
eg)
(a)
2 4 2 6 2 8 3 00 . 0 0
0 . 2 5
0 . 5 0
0 . 7 5
1 . 0 0
t ( s e c )
Curre
nt (Am
p)
0
1 0 0 0
2 0 0 0
3 0 0 0
4 0 0 0
Piston
Positi
on
(b)
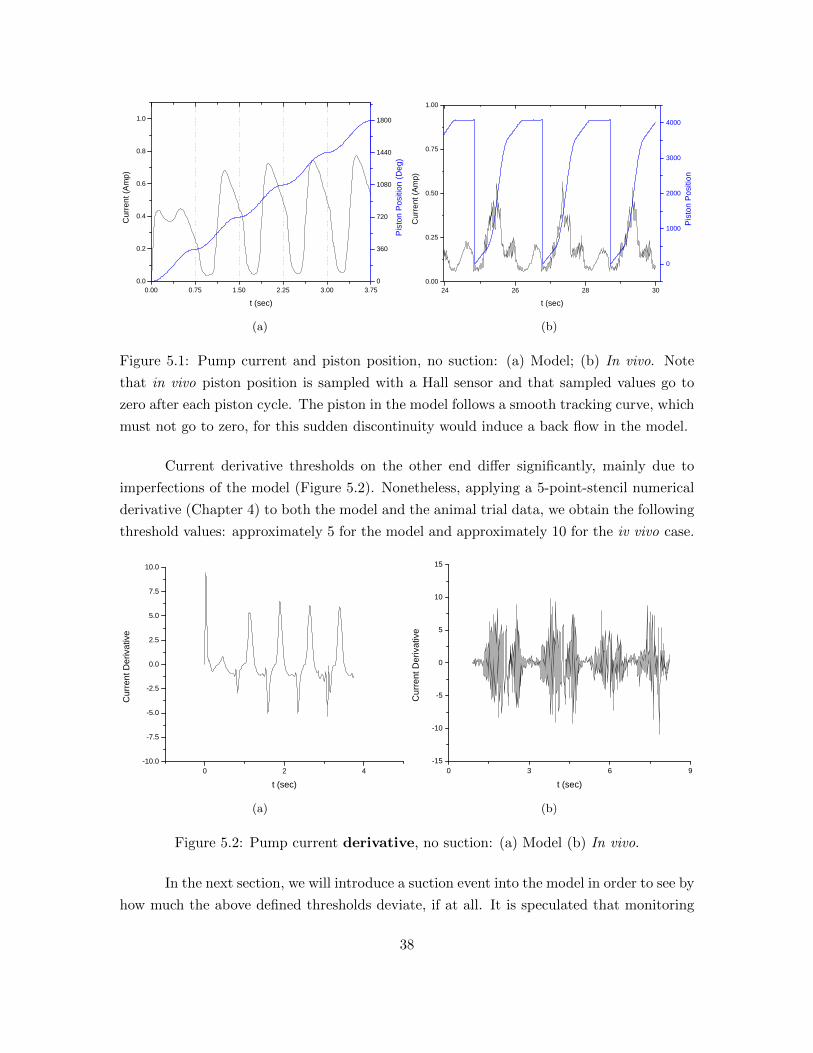
Figure 5.1: Pump current and piston position, no suction: (a) Model; (b) In vivo. Note
that in vivo piston position is sampled with a Hall sensor and that sampled values go to
zero after each piston cycle. The piston in the model follows a smooth tracking curve, which
must not go to zero, for this sudden discontinuity would induce a back flow in the model.
Current derivative thresholds on the other end differ significantly, mainly due to
imperfections of the model (Figure 5.2). Nonetheless, applying a 5-point-stencil numerical
derivative (Chapter 4) to both the model and the animal trial data, we obtain the following
threshold values: approximately 5 for the model and approximately 10 for the iv vivo case.
0 2 4- 1 0 . 0
- 7 . 5
- 5 . 0
- 2 . 5
0 . 0
2 . 5
5 . 0
7 . 5
1 0 . 0
Curre
nt De
rivati
ve
t ( s e c )
(a)
0 3 6 9- 1 5
- 1 0
- 5
0
5
1 0
1 5
Curre
nt De
rivati
ve
t ( s e c )
(b)
Figure 5.2: Pump current derivative, no suction: (a) Model (b) In vivo.
In the next section, we will introduce a suction event into the model in order to see by
how much the above defined thresholds deviate, if at all. It is speculated that monitoring
38

these thresholds only, that is current and its rate of change, is sufficient to detect the
ventricular collapse.
5.2 Suction Event
Typical instance of a suction event, which occurred during an animal trial conducted by
Windmill Cardiovascular Systems is shown in Figure 5.3. The model predicts an increase in
current values. Note that the base threshold value of 0.5 amperes, which we have previously
defined, was exceeded significantly in both the model and reality. In addition, derivative
thresholds have been surmounted in both instances; however, the maximum indices differ
significantly. This should not pose a problem, as we are only interested in tracking no-
suction values and taking controller action when these are exceeded.
0 2 40
2
4
6
8
1 0
Curre
nt (Am
p)
t ( s e c )
(a)
0 1 0 2 0 3 00 . 0
0 . 5
1 . 0
1 . 5
2 . 0
2 . 5
3 . 0
3 . 5
4 . 0
Curre
nt (Am
p)
t ( s e c )
(b)
0 1 2 3 4- 4 0 0
- 2 0 0
0
2 0 0
4 0 0
6 0 0
Curre
nt De
rivati
ve
t ( s e c )
(c)
0 1 0 2 0 3 0
- 8 0
0
8 0
Curre
nt De
rivati
ve
t ( s e c )
(d)
Figure 5.3: (a) Pump current from the model and (b) pump current sampled during animal
trials. (c) Pump current derivative from the model and (d) pump current derivative
calculated from animal trial data. Few aspiration cycles are shown along with the suction
event occurring, and later declining.
39

5.2.1 Suction Event Effects on CVS
Now that the suction indices have been defined for both the current and its rate of change,
and further verified/compared with the animal trial data, we will investigate what physio-
logical effects suction events could possibly have on the cardiovascular system. Note that
there is no available physiological data from the animal trials that we can compare output
of the model against. Therefore, the model will be used to provide us with insights into
physiological consequences, while investigating different modes of operation of the pump,
which is virtually impossible during animal trials and especially patient trials.
A suction event induces ventricular collapse. This phenomenon is most likely to
occur just at the cannula insertion site as it was explained in the introductory chapter and
shown in Figure 1.3. Tracking left ventricular volume during the model simulation gives
insights into suction event occurrence. Yet, a better way of visualizing suction event can be
achieved by tracking the left ventricular diameter:
d =
√6VlvLπ
, (5.1)
where L is the longitudinal radius of the ellipsoid. Recall that the left ventricular shape
and therefore the volume can be estimated with a half ellipsoid (equation (3.1)). Knowing
that the average distance from the atrio-ventricular plane to ventricular apex is L = 8.4cm
and having the state variable Vlv readily available at every time step during simulation, we
can estimate how the ventricular diameter changes at the atrio-ventricular plane, i.e. short
axis diameter of the ellipsoid.
40

0 2 40
1
2
3
4
5
6
7Le
ft ve
ntric
le d
iam
eter
(cm
)
t (sec)
(a)
0 2 40
1
2
3
4
5
6
7
Left v
entric
le dia
meter
(cm)
t ( s e c )
(b)
Figure 5.4: Left ventricle short axis diameter, approximated at the atrio-ventricular plane:
(a) Suction and (b) Normal. Values in the graph for suction case are below the range found
in the literature for the normal end systolic and end diastolic short axis diameters, which
are in the 3.8cm− 5.8cm rage [17].
It is apparent that a suction event is occurring at the apex of the left ventricle and
around the cannula (Figure 1.3). Thus, we can infer from the figures above and from the
fact that the left ventricle is essentially triangularly shaped, that the LV apical diameter
got smaller as well with a reduction of atrio-ventricular diameter, down the same long axis.
Referring to the plots below (Figure 5.5), we observe that at the precise moment when
the ventricular suck-down occurs (approximately at t = 1.75sec), pressure and volume of the
left ventricle get distorted. Namely, pressure values in a healthy person are 120/80mmHg
(peak systolic over peak diastolic pressure), as it can be seen at the bottom portion (b) of
Figure 5.5. The upper portion (a) of the same figure shows an increase in the left ventricular
pressure (150/100mmHg), along with the increase in the aortic flow peak values (from
40L/min to 50L/min). Recall that toroidal pump draws blood out of the left ventricle and
via a parallel pathway injects it into aorta and therefore the rest of systemic circulation.
Thus, during a suction event, there appears an initial burst of the into the aorta due to
higher torque demand on the pump, which then declines as the ventricle starts to collapse.
41

0 0.5 1 1.5 2 2.5 3 3.50
50
100
150Pressures, mmHg: Left ventricle (blue), Left Atrium (green), Systemic arteries (red)
0 0.5 1 1.5 2 2.5 3 3.50
100
200Pressure left ventricle in mmHg (blue), and Volume left ventricle in ml (red)
0 0.5 1 1.5 2 2.5 3 3.50
50Aortic valve flow in L\min (blue), and Pump Flow in L/min (green)
(a)
0 0.5 1 1.5 2 2.5 3 3.50
50
100
150Pressures, mmHg: Left ventricle (blue), Left Atrium (green), Systemic arteries (red)
0 0.5 1 1.5 2 2.5 3 3.5
0
100
200Pressure left ventricle in mmHg (blue), and Volume left ventricle in ml (red)
0 0.5 1 1.5 2 2.5 3 3.50
50Aortic valve flow in L\min (blue), and Pump Flow in L/min (green)
(b)
Figure 5.5: (a) Physiological impacts of suction: (Top) Systemic pressures get distorted;
(Middle) Volume and pressure of the left ventricle deviate from smooth cycling, i.e. volume
gets lower at time t = 1.75 sec, indicating additional draw of blood; (Bottom) There is no
steady aortic flow as before and the LVAD pump actuates irregular bursts of the fluid. (b)
No suction condition modeled.
42

Test case 1: Suction Event Effects on CVS during Reduced Preload
In cardiac physiology, preload is the pressure stretching the ventricle of the heart, after
passive filling of the ventricle and subsequent atrial contraction. The preload gets smaller
for ill myocardium, which is when mechanical assist is desirable. We will alter this inflow
pressure (preload) in the model by reducing the openness of the mitral valve. Essentially,
this step increases the resistance to the flow at the atrio-ventricular plane, inducing lower
than usual rates of filling of the left ventricle. It is hypothesized that such phenomenon
would increases the likeliness of the suction event.
0 1 2 3 40
40
80
120
160
0 1 2 3 40
40
80
120
160
0 1 2 3 40
40
80
120
160
Reduced Preload, Induced Suction
Vol
ume
LV (m
l)
Normal Preload, Induced Suction
t (sec)
Normal Preload, No Suction Modeled
Figure 5.6: Reduced preload suction: (Top) Ventricular collapse is more likely to occur
with reduced preload; (Middle) Ventricular collapse occurs, but less likely; (Bottom) No
ventricular collapse.
Left ventricular volume changes constantly during the cardiac cycle period. Just
before the blood ejection, the left ventricular volume is at maximum and this phase of the
cardiac cycle is called diastole. During systole or the myocardial contraction phase, the
blood is ejected out of the ventricles. Left ventricular volume is smallest just at the end of
systolic phase.
From the bottom portion of the figure above, we see that while the suction event is
excluded from the model (but the pump model is still connected), the lowest left ventricular
43

volume is approximately at 60ml. In addition, note that cardiac cycles are very smooth,
uniform, and alike in appearance.
Normal preload, but with the suction event included in the model (middle portion of
the same figure), shows that ventricular collapse happened two times in four cardiac cycles.
It has also reduced the end systolic volume to approximately 30mm. Note that ventricular
volume cycles do not resemble one another as much.
Finally, the reduced preload case (top portion of the same figure) shows that end
systolic volume is pulled below 10ml over the period of 4 cardiac cycles. Ventricular collapse
occurred 3 times, each time further reducing the end systolic volume. Note that cardiac
cycles appear very distorted, indicating that the pump is drawing blood constantly out of
the ventricle, while the ventricle itself does not have time to refill properly.
Test case 2: Suction Event Effects on CVS during Asynchronous Timing
Now that we have settings that give us consistent suction, in this section we will sweep the
R-wave delay and the pump’s stroke time to generate a map of where suction risk is the
greatest. R-wave is the initial upward deflection of the QRS complex in the normal electro-
cardiogram (ECG). It represents early depolarization of the ventricles during the cardiac
cycle. Tracking the time between two consecutive R-waves tells us how long the cardiac
cycle period is. Thus, we will vary the heart rate, as well as the pump actuation times in
order to investigate the likeliness of a ventricular collapse.
Changing pump aspiration rates
Pump
Pump
Changing PumpAspiration Rates
Tp Tp Tp
1/2Tc1/2Tc 1/2Tc1/2Tc 1/2Tc1/2Tc
(a)
(b)
Figure 5.7: (a) Cardiac cycle period Tc is in sync with the pump cycle period Tp; (b) Pump
aspirates two times during a single heart beat.
Thus far, while investigating likeliness of a suction event and its consequences on
CVS, the pump aspiration cycle Tp was starting and ending at the same time as the cardiac
cycle period Tc. This mode of operation is graphically depicted in part (a) of the above
figure. Next, we will explore what happens to the cardiovascular system during a suction
event as the pump aspirates at the faster rate than the heart beats (part (b)).
44

−20 0 20 40 60 80 100 120 140−20
0
20
40
60
80
100
120
140
160
V (mL)
P (
mm
Hg)
(a)
−50 0 50 100 150 200−20
0
20
40
60
80
100
120
140
160
180
V (mL)
P (
mm
Hg)
(b)
Figure 5.8: (a) Synchronous and (b) Asynchronous pump aspiration effects on left ventric-
ular PV loop.
It is evident from the above figure that having the pump aspirate twice as fast rel-
ative to the length of the cardiac cycle induces significant distortion on the left ventricular
pressure-volume (PV) loop during a suction event. Recall from Chapter 2 that PV loops
are an excellent tool for visualizing changes in ventricular function in response to changes
in preload (filling pressure), afterload (systemic pressure) and inotropy (force or energy of
muscular contractions).
Sweeping the R-wave delay
Pump
Pump
Pump
Sweeping the R-wave Delay
Tp Tp Tp
Tp Tp Tp
Tp Tp Tp(a)
(b)
(c)
Figure 5.9: Cardiac cycle period Tc increases from being two times shorter than the pump
aspiration cycle Tp (a), towards being 3/4 of Tp (b), and finally towards being longer than
the pump cycle (c).
45

Although sweeping the R-wave delay can be mistakenly regarded as the same kind of a test
case as changing pump aspiration rates in terms of timing, note that what differentiates
these two tests is the fact that left ventricular contractile properties stay the same while
the cardiac period Tc changes. In other words, heart muscle properties and blood ejection
volumes do not change, only the heart beats faster or slower.
0 20 40 60 80 100 1200
20
40
60
80
100
120
140
160
V (mL)
P (
mm
Hg)
(a)
0 20 40 60 80 100 120 1400
50
100
150
V (mL)
P (
mm
Hg)
(b)
0 50 100 1500
20
40
60
80
100
120
140
V (mL)
P (
mm
Hg)
(c)
Figure 5.10: PV loop during suction event at the heart rate of (a) 90 BPM (b) 70 BPM
and (c) 60 BPM.
Note from the figure above that the model predicts higher chance of a ventricular
collapse occurring at higher heart rates (Tc = 1/2Tp). The PV loop certainly deviates in
all three situations (90, 70 and 60 beats per minute), relative to the no-suction simulation
46

results shown in Chapter 2. Nonetheless, the suction event is constantly declining as the
heart rate decreases (PV loop becomes more circular and relatively smoother, (a)→ (b)→(c)). Intuitively this makes sense, since higher heart rate means more contractions of the
cardiac muscle, which during the suction event increases the probability of a ventricular
collapse, manifested in the distort PV loop.
5.2.2 Suction Event Effects on Toroidal Pump
Ventricular suck-down can also be damaging to the ventricular assist device due to the
rapid onset of the flow resistance and therefore high torque demands on the pump, which
can impair drive components and/or cause control instability.
It was presented thus far that suction events considerably alter pump’s operation
mode, manifested in the rapid increase of the current (Figure 5.3, part (a)). It was also
shown that the pump’s aspiration rates undergo process of rapid change (Figure 5.5, part
(a), bottom section). The following figure shows what kind of back pressure the toroidal
pulsatile blood pump experiences during the suction event and what kind of a power draw
can be expected. Note that the feedback tracking curve starts to lag at a time t = 1.80 sec
compared to the reference tracking curve. The PID controller is essentially having a hard
time driving the piston in the prescribed motion during suction. The power draw is limited
to 64Watt imposed with the saturation limits on the current and voltage; otherwise the
suction event would require a much larger draw of power due to large back pressure, which
would create even higher current spikes.
47
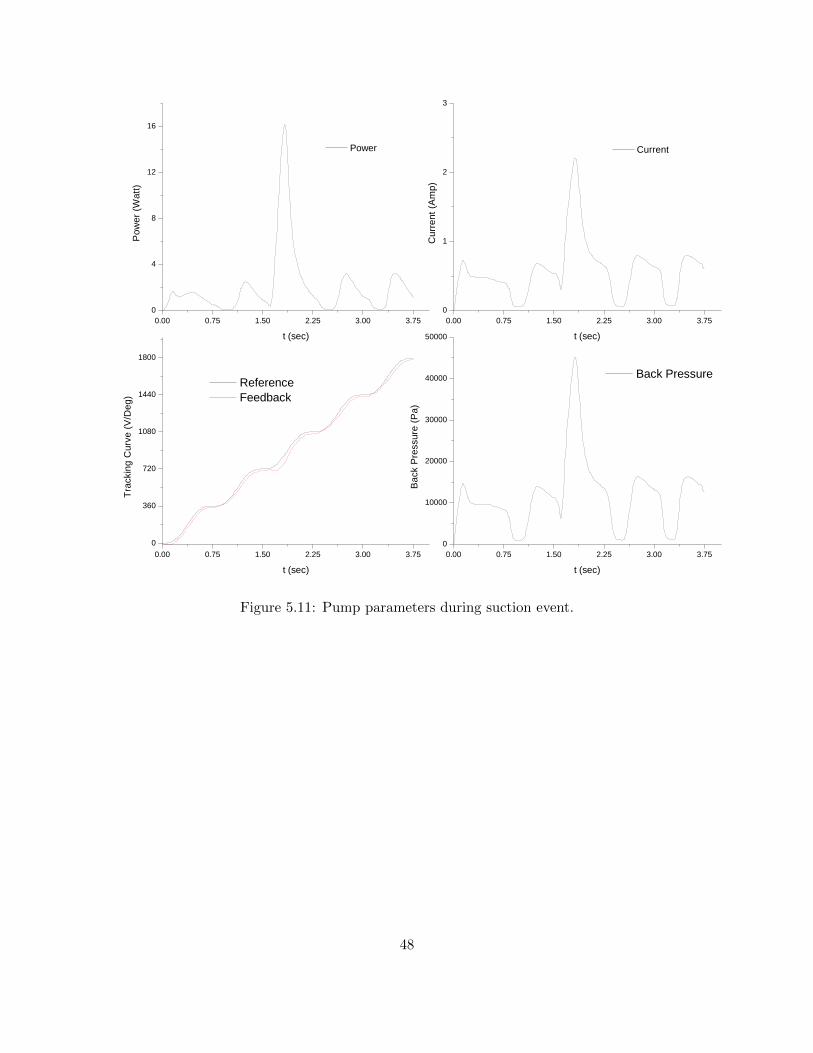
0 . 0 0 0 . 7 5 1 . 5 0 2 . 2 5 3 . 0 0 3 . 7 50
4
8
1 2
1 6
P o w e rPo
wer (W
att)
t ( s e c )0 . 0 0 0 . 7 5 1 . 5 0 2 . 2 5 3 . 0 0 3 . 7 5
0
1
2
3
C u r r e n t
Curre
nt (A
mp)
t ( s e c )
0 . 0 0 0 . 7 5 1 . 5 0 2 . 2 5 3 . 0 0 3 . 7 50
3 6 0
7 2 0
1 0 8 0
1 4 4 0
1 8 0 0
R e f e r e n c e F e e d b a c k
Track
ing C
urve (
V/Deg
)
t ( s e c )0 . 0 0 0 . 7 5 1 . 5 0 2 . 2 5 3 . 0 0 3 . 7 5
0
1 0 0 0 0
2 0 0 0 0
3 0 0 0 0
4 0 0 0 0
5 0 0 0 0
B a c k P r e s s u r e
Back
Pres
sure
(Pa)
t ( s e c )
Figure 5.11: Pump parameters during suction event.
48

Chapter 6
Conclusions
A computational model was developed to study the effects of left ventricular assist devices
on the cardiovascular system during a ventricular collapse. The model consisted of a toroidal
pulsatile blood pump and a closed loop circulatory system. Together, they predicted the
pump’s current traces which reflect ventricular suck-down and provide insights into torque
magnitudes that the pump experiences. In addition, the model investigated likeliness of a
suction event and predicted reasonable outcomes for a few test cases. Effects of a suction
event on the cardiovascular system were observed and studied with three different methods:
left ventricular pressure-volume (PV) loops, left ventricular volume, and left ventricular
diameter.
The restricted flow through the cannula during ventricular collapse was parameter-
ized with the aid of a mock circulatory loop consisting of an artificial left ventricle and a
centrifugal continuous flow pump. This study also investigated different suction detection
schemes and proposed the most promising suction detection algorithm for the TORVAD TM
pump, toroidal left ventricular assist device. The suction detection algorithm was selected
based on the mechanistic features of the TORVAD TM and the particularity of its design.
Model predictions were further compared against the data collected during in vivo animal
trials with the TORVAD TM system and the results showed reasonable accordance.
Recommendations
Additional processing of the pump current signal in real life TORVAD TM applications
may be of crucial importance in suction detection. Namely, during practical TORVAD TM
usage such as animal trials, sampled signals are not as clean as in the model simulations.
The noise in signals may produce similar thresholds as the ones that we defined in this
study. This essentially increases the probability of false positives, events that trigger LVAD
49

controller action to prevent suction when suction is not actually taking place. Thus, signal
integration (smoothing) and cubing (stray spike elimination), may be a good method of
improving algorithm robustness. This approach can be applied to both the pristine current
signal and its derivative.
Although the proposed suction detection algorithm along with next to minimal signal
processing seems quite straightforward, there are a few things that need to be considered
with regards to its execution time. The TORVAD TM controller unit executes the main
program along with other background routines, which all together take a certain number of
clock cycles. Thus, the maximum controller loop speed will need to be taken into account
in order to determine how quickly a decision could be made. For instance, consider a time
window from the point of the onset of the suction resistance until a full-blown ventricular
collapse. There is a chance that the suction might happen so fast that the controller will
not have enough time to react and prevent it from fully occurring due to increased number
of calculations and therefore clock cycles.
Future Work
There is plenty of room for model improvements, which possibly could provide better un-
derstanding of suction events and their impact on the cardiovascular system and the pump.
The present pump model includes only one rotating piston and motor, whereas the
TORVAD TM system actually has two driving mechanisms and two pistons. The two pistons
take turns during pump actuation: while one is rotating, the second one acts as a valve,
preventing regurgitant pump flow. The additional dynamics could appear due to pump
aspiration timing imposed by the second piston.
The circulatory blood system can be expanded to include the entire cardiovascular
system, and not just the left heart and systemic circulation. This would give insights into
suction event effects on the right heart and pulmonary side of the cardiovascular circulation.
The model of the suction event itself can be improved to reflect more realistic behav-
ior of the ventricular collapse. This study described the geometric aspect of the ventricular
suck-down, which was obtained via mock circulation loop consisting of an artificial left ven-
tricle and continuous flow pump. It is speculated that mass inertia of the cardiac tissue near
cannula insertion site could add highly non-linear behavior to the suction event. Finally,
the TORVAD TM system could be used in the future to experimentally parametrize ventric-
ular collapse with the aid of the artificial left ventricle, as opposed to using the Biomedicus
continuous flow pump. Pulsatile flow pumps, such as TORVAD TM, could yield more non-
linear behavior of the variable resistance across the cannulation site during the ventricular
suck-down.
50

Appendix A
Cardiovascular System Summary
51

!
"#
#"#
( )
+−−=
LA
LA
LAT
TTte
π2cos1
2
1 TtTT
LA≤≤−
0=LA
e
"#
( ) ( )0max
10
LALALA
VVB
LALAVVeEeAP LALALA −+=
−−
"#
MIRSLA QQV −=
$
LA
e %"#
maxLAE &" '
(
T )*+',-
t ./
LA
T "# *
LA
P "#
LA
A 00'
LA
B 01(
LA
V "#
0LAV %
MI
Q 2
RS
Q flow from right side

3
"
#"
−=
δ
π
LV
LVT
te cos1
2
1 δ
cTt <≤0
( )( )
−
−+=
δ
δπ
1cos1
2
1
LV
c
LVT
Tte
ccTtT <≤δ
0=LV
e
"
( ) ( ) ( )0max
101LVLVLV
VVB
LVLVLVVVeEeAeP LVLVLV −+−=
−−
"
VADAOMILV
QQQV −−=
$
LV
e %"
maxLVE &" 0'
(
T )*+',-
t ./
LV
T " 00
δ 4 *
LV
P "
LV
A 5'
LV
B 36(
LV
V "
0LVV % 5
MI
Q 2
AO
Q 2
VAD
Q #72

8
2
9
MI
LVLA
MIR
PPQ
−=
#
AO
SALV
AOR
PPQ
−=
, 2
RS
LARS
RSR
PPQ
−=
$
MIQ 2
AO
Q 2
RSQ 2
LAP "#
LV
P "
RSP 3'
MI
R 5' (
AO
R 5' (
RSR 35'
(

0
#
SA
ATSA
SAR
PPQ
−=
SA
SAVADAO
SAC
QQQP
−+=
#
AT
VSAT
ATR
PPQ
−=
AT
ATSA
ATC
QQP
−=
$
SA
Q 2
AO
Q 2
VAD
Q #72
AT
Q 2
SA
P
AT
P
VS
P '
SA
R 0' (
AT
R 15' (
SA
C 5'
(
AT
C '
(

Appendix B
Matlab Files
clear all
global Tc TLV delta phi
HR = 80; % heart rate in BPM, 80
Tc = 60/HR; % cardiac cycle period, SPB (sec per beat)
Tcp = 0.75; % sec, pump aspiration time per cycle
% "Rori" parameters for the orifice delta pressure i.e. dP = Rori * Q|Q|
% note, this is theoretical value, used only for base model simulations
Cd = 0.3; % friction factor, geometry of the orifice dependent
ro = 1060; % kg/m^3, density blood
d1 = 0.0558; % m, LV end diastolic diameter, person w/ 1.5 m^2 of skin area
d2 = 0.01854; % m, diameter cannula
Ac= (d2)^2*pi/4; % m^2, cannula orifice area
Rori=ro/2/(Cd/sqrt(1-(d2/d1)^4))^2/Ac^2;
% motor parameters
Km = 0.124; % (V sec)/rad, constant gyrator coefficient
Rm = 2.6; % Ohms, two phases in series resistance
Rb = 8.1e-5; % (N m sec)/rad, damping coefficient of motor
L = 2.58e-3; % H, inductance of two phases in series
56

Ip = 1.851e-5; % kg m^2, mass moment of inertia, piston
Ap = 2e-4; % m^2, area piston, 1cm x 2cm
r = 0.03; % m, moment arm to piston, assumed value %0.03
Vin = 11; % V, supply voltage, 0 - 14V
% inlet cannula
rho = 1060; % kg/m^3, density blood
Lc = 0.5; % m, cannula length
d2 = 0.01854; % m, diameter cannula
Ac = (d2)^2*pi/4; % m^2, cannula orifice area
Ic = rho*Lc/Ac; % kg/m^4, fluid inertia in the cannula
E = 500e6; % Pa, Young’s modulus PTFE material
v = 0.46; % no units, Poisson’s ratio for PTFE
tc = 0.002; % m, cannula wall thickness
Vc = pi*(d2/2)^2*Lc; % m^3, cannula volume
Cc = 2*Vc*(d2/2)*(1-v/2)/E/tc; % m^3/Pa, cannula compliance
% left ventricle
ELVmax = 2; % maximum LV elastance, mmHg/mL
ELVmax = ELVmax*1.333e8; % Pa/m^3
TLV = 0.44; % LV contraction time, s
delta = 0.6; % elastance peak percent shift
ALV = 0.01; % passive elastance coefficient, mmHg
ALV = ALV*133.3; % Pa
BLV = 0.06; % passive elastance coefficient, 1/mL
BLV = BLV*1e6; % 1/m^3
% left atrium
ELAmax = 0.05; % mmHg/mL
57

ELAmax = ELAmax*1.333e8; % Pa/m^3
TLA = 0.06; % LA contraction time, s
ALA = 0.44; % passive elastance coefficient, mmHg
ALA = ALA*133.3; % Pa
BLA = 0.049; % passive elastance coefficient, 1/mL
BLA = BLA*1e6; % 1/m^3
% arterial system
CSA = 5e-5; % systemic artery compliance, mL/mmHg
CSA = CSA*7.502e-9; % m^3/Pa
CAT = 1; % artery tree compliance, mL/mmHg
CAT = CAT*7.502e-9; % m^3/Pa
RSA = 0.04; % systemic artery resistance, mmHg s/mL
RSA = RSA*1.333e8; % Pa-s/m^3
RAT = 0.79; % artery tree resistance, mmHg s/mL
RAT = RAT*1.333e8; % Pa-s/m^3
% valve flows
RMI = 0.005; % mitral valve resistance, mmHg s/mL
RMI = RMI*1.333e8; % Pa-s/m^3
RAO = 0.005; % aortic valve resistance, mmHg s/mL
RAO = RAO*1.333e8; % Pa-s/m^3
RRS = 0.025; % right side resistance, mmHg s/mL
RRS = RRS*1.333e8; % Pa-s/m^3
% inputs
PRS = 20; % right side pressure, mmHg
PRS = PRS*133.3; % Pa
PVS = 10; % venous system pressure, mmHg
PVS = PVS*133.3; % Pa
% Initial conditions
VLVo = 4; % zero pressure volume, mL
VLVo = VLVo*1e-6; % m^3
VLAo = 5; % zero pressure volume, mL
VLAo = VLAo*1e-6; % m^3
VSAo = CSA*75*133.3;
58

VATo = CAT*75*133.3;
tend = 5*Tc; % sec, simulation length, 5 heart beats
%%%%%%%%%%%%%%%%%%%%%%%%%%%%% simulation command %%%%%%%%%%%%%%%%%%%%%%%%%%
sim(’pump_and_CVS_v3’)
%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%
figure(1)
subplot(3,1,1), plot(tout,PLV/133.3,tout,PLA/133.3,tout,PSA/133.3)
legend(’PLV’,’PLA’,’PSA’)
title(’Pressures, mmHg’)
axis([0 3.75 0 150])
subplot(3,1,2), plot(tout,simout_vlv*1e6,’red’,tout,PLV/133.3,’blue’)
title(’PLV (blue) mmHg and VLV (red) ml’);
axis([0 20 -100 100])
subplot(3,1,3), plot(tout,QAO*6e4,tout,simout_pumpflow*6e4)
title(’Aortic Valve Flow (blue) L\min, Pump Flow (green) L/min’)
axis([0 3.75 0 50])
figure(2)
% plot double y axis
[AX,H1,H2] = plotyy(tout,simout_cur,tout,simout_track);
xlabel(’t (sec)’)
set(get(AX(1),’Ylabel’),’String’,’Current (Amp)’)
set(get(AX(2),’Ylabel’),’String’,’Piston Position (Deg)’)
59

figure(3)
% plot PV loop
plot(simout_vlv*1e6,PLV/133.3)
xlabel(’V (mL)’), ylabel(’P (mmHg)’)
figure(4)
% plot resistance across the orifice vs. volume LV
plot(simout_vlv*1e6,simout_Rori)
xlabel(’V (mL)’), ylabel(’R__ori (Pa m^3/sec)’)
% save suction function R=R(Vlv)
% 3.26E10 + 4.56E10*exp(-28689.6*u)
60

ow
rate
into
VA
D
ow
rate
from
VA
DSi
mpl
e CV
S M
odel
v1. 1
0/13
/08
jg,rg
l
Q p
ump
to C
VS
PUM
P <<
<−−−
−−−−
−−−−
−−−−
−−−−
−−−−
−−−−
−−−−
−−−−
−−−−
−−−−
−−−−
−−−−
−−−−
−−−−
−−−−
−−−−
−−−−
−−−−
−−−−
−−−−
−−−−
−−−−
−−−−
>>>C
VS
doub
le c
lick
to c
hang
e
doub
le
clic
k to
cha
nge
****
****
***C
ontin
uous
Tra
ckin
g Cu
rve*
****
****
*
QA
O_
4PSA3
PLA
_2
PLV_1
sqrt
2
sqrt
sqrt
1
sqrt
sqrt
sqrt
m2c
m
100
i
1/L
1 s
gam
ma_
dot
Ic*A
p*r/
Ip
eLV,
eLA
eLV
f(u)
eLA
f(u)
delta
Vol
ume
com
plia
nt tu
be (m
^3)
dP_o
ri −
Pres
sure
Acr
oss
Ori
cecm
ps2l
pmin
2−K
−
cmps
2lpm
in1
−K−
cmps
2lpm
in
−K−
cm2m
l
−K−
Vr
Rm/L
Volu
me
LV (m
l)
Volta
ge
Vm
Km/Ip
View
Tra
ckin
g Cu
rve9
View
Tra
ckin
g Cu
rve8
View
Tra
ckin
g Cu
rve7
View
Tra
ckin
g Cu
rve5
View
Tra
ckin
g Cu
rve4
View
Tra
ckin
g Cu
rve3
View
Tra
ckin
g Cu
rve2
View
Tra
ckin
g Cu
rve1
1
View
Tra
ckin
g Cu
rve1
0
View
Tra
ckin
g Cu
rve1
View
Res
ultin
gSy
nchr
onou
s T
rack
ing
Curv
e (3
.75
sec
long
, i.e
. 10
pum
p st
roke
s)(3
60 d
eg p
er 0
.75/
2 se
c of
str
oke
leng
th)
VSA
dot
VSA1 s
VLVd
otVL
V1 s
VLA
dot
VLA1 s
VATd
otVA
T1 s
Tr
Rb/Ip Tp
Ap*
r
To W
orks
pace
9
sim
out_
Rori
To W
orks
pace
8
sim
out_
trac
k
To W
orks
pace
7
sim
out_
curf
To W
orks
pace
6
sim
out_
pum
pow
To W
orks
pace
5
sim
out_
vlv
To W
orks
pace
4
sim
out_
cur
To W
orks
pace
3
QA
O
To W
orks
pace
2
PSA
To W
orks
pace
14
sim
out_
pid
To W
orks
pace
13
sim
out_
pow
To W
orks
pace
12
sim
out_
pp
To W
orks
pace
11
sim
out_
diam
To W
orks
pace
10
sim
out_
der
To W
orks
pace
1
PLV
To W
orks
pace
PLA
Tm
Km
Tc1
Tc
TcTc
Sync
hron
ous
Trac
king
Cur
veG
ener
ator
9
f(u)
Sync
hron
ous
Trac
king
Cur
veG
ener
ator
8
f(u)
Sync
hron
ous
Trac
king
Cur
veG
ener
ator
7
f(u)
Sync
hron
ous
Trac
king
Cur
veG
ener
ator
5
f(u)
Sync
hron
ous
Trac
king
Cur
veG
ener
ator
4
f(u)
Sync
hron
ous
Trac
king
Cur
veG
ener
ator
3
f(u)
Sync
hron
ous
Trac
king
Cur
veG
ener
ator
2
f(u)
Sync
hron
ous
Trac
king
Cur
veG
ener
ator
11
f(u)
Sync
hron
ous
Trac
king
Cur
veG
ener
ator
10
f(u)
Sync
hron
ous
Trac
king
Cur
veG
ener
ator
1
f(u)
Suct
ion
Func
tion:
Base
d on
Exp
erim
anta
lD
ata
f(u)
Suct
ion
Even
t Cur
ve
Satu
ratio
n
Resu
lting
Sync
hron
ous
Tra
ckin
g Cu
rve
f(u)
Resi
stan
ceor
ice
nosu
ctio
n
Rori
QRSf(u
)
QM
I
f(u)
QA
O
f(u)
Q p
ump
Ap*
r/Ip
Pum
p Fl
oww
(L/m
in)
Prod
uct1
Prod
uct
Pres
sure
can
nula
(Pa)
Ppis
ton
(Pa)
Pow
er S
atur
ated
Posi
tion
Sens
or
Pist
on A
ngul
ar V
eloc
itySh
aft
Posi
tion
Volts
Pist
on P
ositi
onVo
lts/D
egre
es
Pc
1/Cc
PVS
PVSPR
S
PRS
PLV
f(u)
PLA
f(u)
Om
ega
1/Ip
Mat
hFu
nctio
n1
mod
Mat
hFu
nctio
n
mod
LV s
hort
axi
s di
amet
er (m
)
Inte
grat
or1
1 s
Inte
grat
or
1 s
Gro
und
GSA
−K−
GA
T
−K−
Flow
Qic
(L/m
in)
Filte
red
pum
p Fl
ow (L
/min
)
Fcn
f(u)
Der
ivat
ive
du/d
t
DPS
A
DPR
S
DPM
I
DPA
TD
PAO
Curr
ent U
nFilt
ered
(Am
ps)
Curr
ent F
ilter
ed (A
mps
)
Curr
ent D
eriv
ativ
e1
PID
Conn
ect/
Dis
conn
ect
the
Pum
p to
CVS
Conn
ect/
Dis
conn
ect
Suct
ion
Even
t
Conn
ect/
Dis
conn
ect
Satu
ratio
n Li
mit
Cloc
k2
Cloc
k
CSA
−K−
CAT
−K−
Aor
tic V
alve
Flo
w
Ang
ular
Vel
ocity
Filt
er7
1
0.05
s+1
Filt
er6
1
0.05
s+1
Filt
er5
1
0.05
s+1
Filt
er4
1
0.05
s+1
Filt
er3
1
0.05
s+1
Filt
er2
1
0.05
s+1
Filt
er1
1
0.05
s+1
Filt
er1
0.05
s+1
VLVd
ot
Vlv
Vlv
Vlv
PRS
VLA
dot
QRS
PLA
PLA
PLV
PLV
PLV
QM
I
QM
I
QM
I
VSA
dot
PSA
PSA
PSA
PSA
QA
O
QA
OQ
SAQ
SAQ
SAVA
Tdot
PAT
PAT
QA
TPV
S
h
h
h
h
h
h
h_do
t
h_do
t
Ppga
mm
a_do
t
Qp
Qp
Qp
lam
bda
lam
bda
Vin
Vt_d
otVt
Pt
Pt
Pt
dP_o
ri
Qic
Qic
Figure B.1: Pump and CVS Simulink Model
61

Bibliography
[1] M. Awasthi. Development of a cardio-vascular simulator for evaluation of ventricular
assist devices. Master’s thesis, University of Illinois at Urbana-Champaign, 2003.
[2] L. Baloa. Certainty-weighted system for the detection of suction in ventricular assist
devices. PhD thesis, University of Pittsburgh, Pittsburgh, PA, 2001.
[3] W. Borutzky. Bond Graph Methodology: Development and Analysis of Multidisci-
plinary Dynamic System Models. Springer-Verlag london Limited, Germany, 1st edi-
tion, 2010.
[4] P. Breedveld and J. van Amerongen. Dynamische systemen: modelvorming en simulatie
met bondgrafen. Technical report, Open Universiteit, Enschede.
[5] A. Brostrom. Information point. J Clin Nurs, 12(2):234–234, 2003.
[6] F. Cassot, D. Morvan, P. Issartier, and R. Pelissier. New versatile physical model
fitting the systemic circulation accurately. Medical and Biological Engineering and
Computing, 23:511–516, 1985.
[7] A. J. Clegg, D. A. Scott, E. Loveman, J. Colquitt, J. Hutchinson, P. Royle, and
J. Bryant. The clinical and cost-effectiveness of left ventricular assist devices for end-
stage heart failure: a systematic review and economic evaluation. Health Technol
Assess, 9(45):1–148, 2005.
[8] D. V. Cokkinos and B. S. Lewis. Heart failure overview. Heart Failure Reviews,
11(2):193–197, 2006.
[9] A. A. Elkamhawy and H. Chandna. Minimum detectable defect thickness in spect
myocardial perfusion test: Phantom study with 99mTc and 201Tl. J Nucl Med Technol,
29(4):183–188, 2001.
[10] K. Eya, E. Tuzun, J. Conger, H. K. Chee, D. Byler, C. Nojiri, O. H. Frazier, and
K. Kadipasaoglu. Effect of pump flow mode of novel left ventricular assist device
62

upon end organ perfusion in dogs with doxorubicin induced heart failure. ASAIO J,
51(1):41–49, 2005.
[11] J. D. Faires and R. L. Burden. Numerical Methods. Brooks Cole, 3rd edition, 2002.
[12] A. Ferreira, M. A. Simaan, J. R. Boston, and J. F. Antaki. Frequency and time-
frequency based indices for suction detection in rotary blood pumps. IEEE Xplore,
2:1064–1067, 2006.
[13] J. Freiberg. Absolute quantitation of left ventricular wall and cavity parameters using
ECG-gated PET. Journal of Nuclear Cardiology, 11(1):38–46, 2004.
[14] J. H. Gibbon. Application of a mechanical heart and lung apparatus to cardiac surgery.
Minn Med, 37(3):171–185, 1954.
[15] J. R. Gohean. A closed-loop multi-scale model of the cardiovascular system for eval-
uation of ventricular assist devices. Master’s thesis, Cockrell School of Engineering,
Univeristy of Texas at Austin, May 2007.
[16] S. Gregory, D. Timms, M. J. Pearcy, and G. Tansley. A naturally shaped silicone
ventricle evaluated in a mock circulation loop: A preliminary study. Journal of Medical
Engineering and Technology, 33(3):185–191, 2009.
[17] L. F. Hsu, P. Jas, P. Sanders, S. Garrigue, M. Hocini, F. Sacher, Y. Takahashi, M. Rot-
ter, J. L. Pasqui, C. Scave, P. Bordachar, J. Clmenty, and M. Hassaguerre. Catheter
ablation for atrial fibrillation in congestive heart failure. The New England Journal of
Medicine, 351(23):2373–2383, 2004.
[18] T. Korakianitis and Y. Shi. A concentrated parameter model for the human cardiovas-
cular system including heart valve dynamics and atrioventricular interaction. Medical
Engineering & Physics, 28(7):613–628, 2005.
[19] K. N. Litwak, S. Kihara, M. V. Kameneva, P. Litwak, A. Uryash, Z. Wu, and B. P.
Griffith. Effects of continuous flow left ventricular assist device support on skin tissue
microcirculation and aortic hemodynamics. ASAIO J, 49(1):103–107, 2003.
[20] K. N. Litwak, S. C. Koenig, R. C. Cheng, G. A. Giridharan, K. J. Gillars, and G. M.
Pantalos. Ascending aorta outflow graft location and pulsatile ventricular assist provide
optimal hemodynamic support in an adult mock circulation. Artif Organs, 29(8):629–
635, 2005.
63

[21] K. N. Litwak, S. C. Koenig, H. Tsukui, S. Kihara, Z. Wu, and G. M. Pantalos. Effects
of left ventricular assist device support and outflow graft location upon aortic blood
flow. ASAIO J, 50(5):432–437, 2004.
[22] J. D. Madigan, A. Barbone, A. F. Choudhri, D. L. Morales, B. Cai, M. C. Oz, and
D. Burkhoff. Time course of reverse remodeling of the left ventricle during support
with a left ventricular assist device. Journal of Thoracic and Cardiovascular Surgery,
121:902–908, 2001.
[23] D. G. Mason, A. K. Hilton, and R. F. Salamonsen. Reliable suction detection for
patients with rotary blood pumps. ASAIO Journal, 54:359–366, 2008.
[24] D. E. Mohrman and L. J. Heller. Cardiovascular Physiology (Lange Physiology Series).
McGraw-Hill, 5th edition, 2003.
[25] G. F. Morello. Method and system for detecting ventricular collapse. Patent, Feb 2007.
US 7175588.
[26] B. R. Munson, D. F. Young, and T. H. Okiishi. Fundamentals of Fluid Mechanics.
John Wiley & Sons, Inc., United States of America, 5th edition, 2006.
[27] G. M. Pantalos, S. C. Koenig, K. J. Gillars, G. A. Giridharan, and D. L. Ewert. Char-
acterization of an adult mock circulation for testing cardiac support devices. ASAIO
Jouranl, 50:37–46, 2004.
[28] Y. C. Pao, E. L. Ritman, R. A. Robb, and E. H. Wood. A finite element method for
evaluating cross-sectional Young’s Modulus of diastolic left ventricle. 1975. Proceedings
of 28th meeting of ACEMB, 385.
[29] K. Rasmusson, J. Hall, and D. Renlund. Heart failure epidemic boiling to the surface.
Nurse Pract, 31(11):12–21, 2006.
[30] W. J. Remme and K. Swedberg. Treatment of chronic heart failure. guidelines for the
diagnosis and treatment of chronic heart failure. Eue Heart J, 22(17):1527–1560, 2001.
[31] G. Rizzoni. Fundamentals of Electrical Engineering. McGraw-Hill, United States of
America, 1st edition, 2009.
[32] F. B. Sachse and G. Seemann. Modeling of cardiac electro-mechanics in a truncated
ellipsoid model of left ventricle. In Surgery Simulation and Soft Tissue Modeling, 2003.
Proceedings (Lecture Notes in Computer Science).
64
[33] D. Sobic-Saranovic, V. Bosnjakovic, S. Pavlovic, M. Veljovic, N. Kozarevic, J. Sapon-
jski, Z. Petrasinovic, M. Ostojic, V. Artiko, M. Todorovic-Tirnanic, and V. Obradovic.
Methods for the quantification of left ventricular volumes assessed by radionuclide
ventriculography (first part). Glas Srp Akad Nauka Med, NIL(48):11–30, 2005.
[34] P. Sundblad and B. Wranne. Influence of posture on left ventricular long- and short-axis
shortening. AJP - Heart and Circulatory Physiology, 283(1):1302–1306, 2002.
[35] P. U. Thamsen. Cutting clogging in wastewater systems. World Pumps., 2009.
This is an electronic document. Date of publication: March 25, 2009. Date re-
trieved: June 30, 2010. http://www.worldpumps.com/view/894/cutting-clogging-in-
wastewater-systems/.
[36] G. Tortora and S. Grabowski. Principles of Anatomy and Physiology. Harper & Row
New York, 1987.
[37] S. Vandenberghe, P. Segers, J. F. Antaki, B. Meyns, and P. R. Verdonck. Hemodynamic
modes of ventricular assist with a rotary blood pump: continuous, pulsatile, and failure.
ASAIO J, 51(6):711–718, 2005.
[38] S. Vandenberghe, P. Segers, B. Meyns, and P. Verdonck. Unloading effect of a rotary
blood pump assessed by mathematical modeling. Artif Organs, 27(12):1094–1101, 2003.
[39] O. Voigt, R. J. Benkowski, and G. F. Morello. Suction detection for the micromed
debakey left ventricular assist device. ASAIO Journal, pages 321–328, 2005.
[40] M. Vollkron, H. Shima, L. Huber, R. Benkowski, G. Morello, and G. Wieselthaler.
Development of a suction detection system for axial blood pumps. Artificial Organs,
28(8):709–716, 2004.
[41] A. L. Yettram and C. A. Vinson. Orthotropic elastic moduli for left ventricular me-
chanical behaviour. Medical and Biological Engineering and Computing, 17(1):25–30,
1979.
[42] W. Young and R. Budynas. Roark’s Formulas for Stress and Strain. McGraw-Hill
Professional, 7th edition, 2001.
[43] A. Yuhki, E. Hatoh, M. Nogava, M. Miura, Y. Shimazaki, and S. Takatani. Detection
of suction and regurgitation of the implantable centrifugal pump based on the motor
current waveform analysis and its application to optimization of pump flow. Artificial
Organs, 23(6):532–537, 1999.
65

[44] L. Zhong, D. N. Ghista, E. Y. Ng, and S. T. Lim. Passive and active ventricular
elastances of the left ventricle. BioMedical Engineering OnLine, pages 4–10, 2005.
[45] L. Zhong, D. N. Ghista, E. Y. Ng, S. T. Lim, R. S. Tan, and L. P. Chua. Explaining
left ventricular pressure dynamics in terms of LV passive and active elastances. J.
Engineering in Medicine, 220 Part H, 2006.
66

Vita
Djordje Adnadjevic was born in Belgrade, Serbia on 26 May 1985, the son of Nikola Adnad-
jevic and Darinka Adnadjevic. After obtaining his high school diploma at Warwick Valley
High School, NY, he received the Bachelor of Science degree in Electrical Engineering from
The University of Texas at Austin. He applied to The University of Texas at Austin for
enrollment in their mechanical engineering program. He was accepted and started graduate
studies in January, 2009.
Permanent Address: 910 Duncan Lane Apt 53
Austin, TX 78705
This thesis was typeset with LATEX 2ε∗ by the author.
∗LATEX 2ε is an extension of LATEX. LATEX is a collection of macros for TEX. TEX is a trademark of theAmerican Mathematical Society. The macros used in formatting this thesis were written by Dinesh Das,Department of Computer Sciences, The University of Texas at Austin, and extended by Bert Kay, James A.Bednar, and Ayman El-Khashab.
67
Top Related