






Languages
Pages
Legal


CHRONIC COMPLICATIONS OF
DIABETES MELLITUS
Microvascular
complications:
• Diabetic retinopathy
• Diabetic nephropathy
• Diabetic neuropathy
Macrovascular
complications
Systemic atheroscerosis
Mixted: diabetic foot

Pathogeny of chronic complications
in diabetes mellitus
Main factors:
• Genetic factors
• Duration of diabetes
• Metabolic control
Pathogenic mechanisms:
• Glycosilation of proteins
• Poliol pathway activation
• Increased production of oxidative stress
• Haemorrheological disturbancies

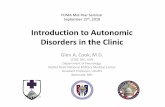
Post-prandial hyperglycaemia
Post-prandial hyperglycaemia contributes HbA1c ~1%
B=breakfast; L=lunch; D=dinner.
Adapted from Riddle MC. Diabetes Care. 1990;13:676-686.
Pla
sm
a g
luco
se
(m
g/d
L)
300
200
100
0
Time of day (h)
6 12 18 24 6
Uncontrolled Diabetes HbA1c 8%
Fasting hyperglycaemia
Basal hyperglycaemia contributes ~2%
B
L
D
Normal HbA1c ~5%
CONTRIBUTIONS OF FASTING AND POST-
PRANDIAL GLYCEMIA IN INCREASING HbA1c

Classification of diabetic
retinopathy Non-proliferative DR:microaneurisms, “hard” exudates,microhaemorrhagies
- Oftalmologic control in 1 year
Diabetic maculopathy:macular oedema or ischaemical disorders
-ophtalmologic control in 3-4 months
Preproliferative DR:”soft” exudates,haemorrhagies
Ophtalmologic cntrol in 2-3 months
Proliferative retinopathy:capillary new vessels
Ophtalmologic control in 2-3 months.
Advanced eye disease:detached retina, rubeosis iridis,neovascular glaucoma

SCREENING OF DIABETIC
RETINOPATHY
TYPE OF
DIABETES
FIRST EYE
FUNDOSCOPY
USUAL
EXAMINATION
TYPE 1 3-5YEARS
AFTER
DIAGNOSIS
EVERY YEAR
TYPE 2 AT FIRST
DIAGNOSIS
EVERY YEAR
PREGNANCY Preconception
al and during
pregnancy

Main mechanisms of atherogenesis in
diabetes
Disturbancies in concentration,composition and lipoproteins
Glycosilation end-products in plasma and arterial wall
Oxidisation and glycosilatin of LDL
Procoagulant status
Insulinresistance and hyperinsulinism
Muscle cell proliferation and “foam’cells in vascular wall

Mechanisms Contributing to
Arterial Disease in Metabolic Syndrome and
Type 2 Diabetes
Adapted from Libby et al. Circulation. 2002;106:2760-2763.

Cardiac disturbancies in diabetes
Hyperglycemia
Macroangiopathy Autonomic cadiac neuropathy
Microangiopathy
Diabetic cardiomiopathy
Genetic factor
Age,sex
Family history
Endothelial
dysfunction
Oxidative
stress Procoagulant
status
Protein
glycosilation
insulinresistence
dyslipidemia
Arterial
hypertension
Abdominal
obesity

DIABETIC NEPHROPATHY

The evolution of glomerular filtrate and urinary
albumin excretion

STAGE I –RENAL HYPERFILTRATION AND
HYPERTROPHY
• AT FIRST DIAGNOSIS OF DIABETES
• reversible
• 20-50 % of GFR (>150 ml/min/1,73 m2)
• After decreasing glycemia: 50% - GFR is normalising
50% - hiperfiltration
microalbuminuria
• Intermitent microalbuminuria:increasing the glomeruli
and kidneys
• Normal blood pressure

STAGE II –SILENT, NORMOALBUMINURIC
STAGE
• In first five years of diabetes
• Renal biopsy:thickening of basal membrane and
mesangium
• GFR is increased ( 20-50 %)
• UAER is normal
• normal BP

STAGE III – EARLY NEPHROPATHY
• After 6-15years of diabetes
• The progression is stopped by a good metabolic
control
• Persistent microalbuminuria (30-300 mg/24 h) –
• GFR is increased, but is decreasing with 3-5
ml/min/year
• Normal or little increased blood pressure ( with 3
mm Hg/year)
• Much more histological abnormalities +glomerular
obstructions

STAGE IV –CLINIC DIABETIC
NEPHROPATHY
• After 15-25 years of diabetes
• Clinic proteinuria (albuminuria > 300 mg/24 ore)
• GF progressivelly( 8-12 ml/min/year)
• 3 substages: - early(GF > 130 ml/min)
- intermmediary (GF < 100 ml/min)
- advanced (GF < 70 ml/min)
• BP ( with 5 mm Hg/year)
• Morphopatology:progressive glomerular sclerosis
distruction of renal mass
•Good glycemic and BP control is delaying the
progression of renal disease.
•

STAGE V –CHRONIC RENAL FAILURE
• After 25-30 years of diabetes
• Proteinuria
• Urinary ureea<10g/24h
• GF < 10 ml/min
• BP
• Morphopatology: severe glomerular occlusions and lesion

V. SCREENING FOR MICROALBUMINURIA
Every year :
• At puberty or 5 years of type 1 diabetes
• At first diagnosis of type 2 diabetes

ADA. Diabetes Care. 2005;28(suppl 1):S1-79.
• Diet
• Physical exercise
• Smoking cessation
• Weight control
• HbA1c <7%
• Glucose (mg/dL):
Preprandial 90–130
Postprandial <180
• Dyslipidemia: Statines
• Hypertension : ≥2 classes
of drugs
• Microalbuminuria:
ACE or ARB
• Aspirin
• CHD: ACE, -blockers
• CVD/risc: ACE
Optimising lifestyle Intensive glycemic
control
Intensive treatment
to decrease
cadiovascular
risk
Optimal treatment of arterial hypertension in
diabetic patient

Hyperglycemia
polyol pathway
Intracellular hyperosmolarity
Decreasing intracellular
myoinositol
Decreasing activity decreasing axonal flow decreased phosphoinositol Na+/K+ ATP-ase
Axonal demyelinisation

CLASSIFICATION AND STAGING of DIABETIC
NEUROPATHY ADA: Consensus San Antonio
Subclinical neuropathy
• Abnormal Electrodiagnostic Tests
1.decreased nerve conduction velocity
2.decreased amplitude of evoked muscle or nerve action potential
• Abnormal Quantitative Sensory Testing
1.vibratory/tactile
2.thermal
3.others
• Abnormal Autonomic Function Tests
1.Diminished sinus arrhythmia
2.Diminished sudomotor function
3.Increased pupillary latency

Clinical neuropathy
Diffuse neuropathy
1.distal symmetric sensorimotor polyneuropathy
-primarly small-fiber neuropathy
-primarly large fiber neuropathy
- mixed
2.autonomic neuropathy
a.abnormal pupillary function
b.sudomotor dysfunction
c.genito-urinary autonomic neuropathy
-bladder dysfunction
-sexual dysfunction
d.gastro-intestinal autonomic neuropathy
-gastric atony
-gallbladder atony
-diabetic diarrhea
-hypoglycemia unawareness

Clinical neuropathy
e.Cardiovascular autonomic neuropathy
f.Hypoglycemia unawareness
Focal Neuropathy 1.Mononeuropathy
2.Mononeuripathy multiplex
3.Plexopathy
4.Radiculopathy
5.Cranial neuropathy

AUTONOMIC NEUROPATHY
• Cardiovascular -tachycardia, exercise
intolerance
-cardiac denervation
-orthostatic hypotension
• Gastrointestinal -esophageal dysfunction
-gastroparesis
-diarrhea
-constipation
-fecal incontinence
• Genitourinary
- erectile dysfunction
- retrograde ejaculation
-cystopathy
-neurogenic bladder
• Neurovascular -heat intolerance
-gustatory sweating
-dry skin
-impaired skin blood flow
• Pupillary • Decreased diameter of dark
adapted pupil

Clinical manifestations of cardiac
autonomic neuropathy
Exercise intolerance • Impairment of exercise tolerance
• Reduced response to heart rate and blood pressure
• Decreased cardiac output
• Decreased ejection fraction
• Systolic dysfunction
• Decrease in diastolic filling
Intraoperative cardiovascular lability
Increased necessity for vasopresor support
Excessive vasodilation with anesthesia due to loss of normal vasoconstrictor response and tachycardia
Orthostatic hypotension • Dizziness
• Weakness
• Fatigue
• Visual blurring
• Neck pain
Sylent myocardial ischemia • Decreased perception of anginal
pain, often accompanied by unexplained fatigue, confusion, tiredness, edema, hemoptysis, nausea, vomiting, diaphoresis, arrhytmias, cough or dyspnea
Top Related