







Languages
Pages
Legal


Choice of Anticonvulsant for Prevention and Management of Eclamptic Seizures
FFemi Oladapoemi Oladapo
Maternal and Fetal Health Research Unit,Maternal and Fetal Health Research Unit,Department of Obstetrics & Gynaecology,Department of Obstetrics & Gynaecology,
Olabisi Onabanjo University, Olabisi Onabanjo University, Sagamu, NigeriaSagamu, Nigeria
On behalf of the Guideline Development Group for theOn behalf of the Guideline Development Group for theWHO Recommendations on Preeclampsia and EclampsiaWHO Recommendations on Preeclampsia and Eclampsia

Outline
• Background
• Anticonvulsants for PE/E
• WHO guideline development process
• Evidence summary on clinical effectiveness
• Interpretation of evidence
• Implications for clinical practice
Background
• PE/E accounts for significant maternal and perinatal morbidity and mortality particularly in the developing countries
• Stopping the progression of PE to E is key to improving outcome
• Making the right choice of anticonvulsant is important for optimal care
• Substandard care in management persists despite overwhelming evidence on effective interventions
• Uncertain pathophysiology and associated multisystemic complications raise safety concerns regarding drug treatment

Anticonvulsants for PE/E: magnesium sulfate
• First introduced for eclampsia in the 1920s
• Not a traditional anticonvulsant
• Mechanism of action is poorly understood
• Dosage regimens have evolved over the years
• Side effects: Common: flushing Less common: nausea, vomiting, muscle weakness, thirst, headache,
drowsiness and confusion Rare: respiratory depression, respiratory and cardiac arrest

Anticonvulsants for PE/E: diazepam
• A benzodiazepine
• First suggested for eclampsia in the 1960s
• A traditional anticonvulsant also used for a wide range of conditions
• Core medicine in the World Health Organization's 'Essential Drugs List‘
• Common side effects: drowsiness, confusion and amnesia

Anticonvulsants for PE/E: phenytoin
• Suggested for eclampsia in the 1980s
• Widely used for acute and long-term control of seizures
• Acts as anticonvulsant without causing sedation
• Prevents onset of but not useful for aborting seizures
• Side effects: hypotension, cardiac arrhythmias, nystagmus and ataxia.
Anticonvulsants for PE/E: lytic cocktail
• Usually a combination of chlorpromazine (antipsychotic) promethazine (H1 histamine antagonist) and pethidine (opioid analgesic)
• First introduced and used to be standard treatment in India
• Individual component has sedative effects on the CNS
• No longer in widespread use
• Side effects: cardiac arrhythmias (chlorpromazine) hallucinations, incoordination (promethazine), seizures (chlorpromazine, promethazine and pethidine)
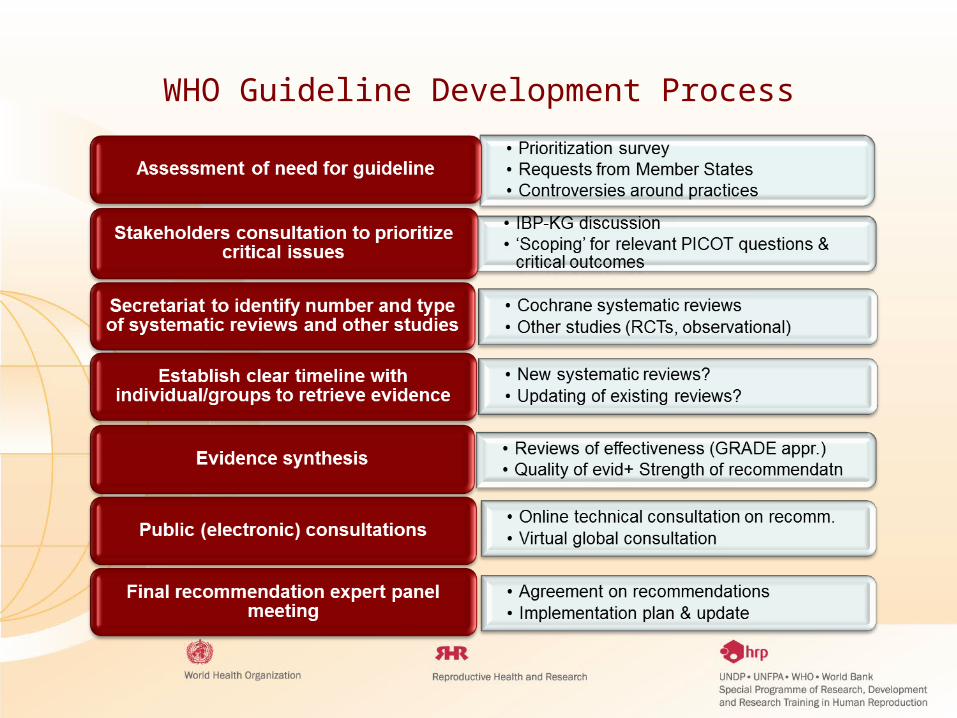
WHO Guideline Development Process

Critical outcomes for WHO recommendations on PE/E
Outcomes Proxy
Eclampsia PE (if it is an intervention for preventing PE); Severe hypertension; Severe PE/HELLP
Recurrence of convulsions --
Severe maternal morbidity Organ failure
Maternal death --
Perinatal death Stillbirth, neonatal death, any baby death
Admission to neonatal intensive care unit
--
Apgar scores at 5’ < 7 --
Adverse events of intervention Toxicity (as defined); Calcium gluconate administration for MgSO4

Evidence summaries: prevention of eclampsia
• A Cochrane review of 15 RCTs investigated the relative effects of anticonvulsants for prevention of eclampsia (Duley et al, 2010)
Magnesium sulfate versus placebo or no anticonvulsants Magnesium sulfate versus phenytoin
Magnesium sulfate versus diazepam
Magnesium sulfate versus nimodipine Magnesium sulfate versus isosorbide
Magnesium chloride with methyldopa.
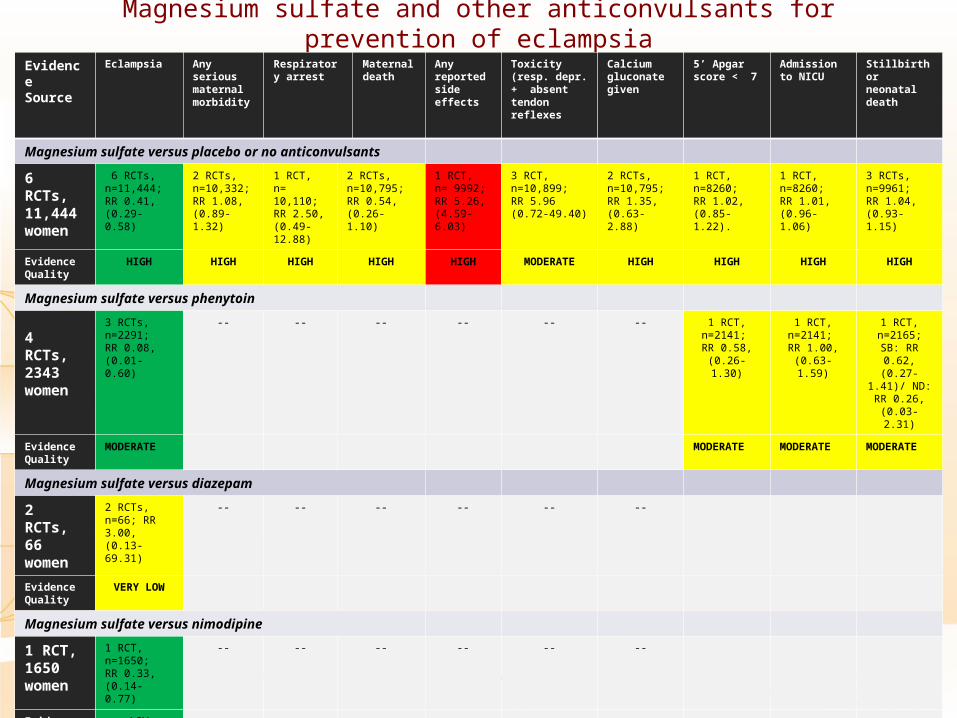
Magnesium sulfate and other anticonvulsants for prevention of eclampsia
Evidence Source
Eclampsia Any serious maternal morbidity
Respiratory arrest
Maternal death
Any reported side effects
Toxicity (resp. depr. + absent tendon reflexes
Calcium gluconate given
5’ Apgar score < 7
Admission to NICU
Stillbirth or neonatal death
Magnesium sulfate versus placebo or no anticonvulsants
6 RCTs, 11,444 women
6 RCTs, n=11,444; RR 0.41, (0.29- 0.58)
2 RCTs, n=10,332; RR 1.08, (0.89-1.32)
1 RCT, n= 10,110; RR 2.50, (0.49-12.88)
2 RCTs, n=10,795; RR 0.54, (0.26-1.10)
1 RCT, n= 9992; RR 5.26, (4.59-6.03)
3 RCT, n=10,899; RR 5.96 (0.72-49.40)
2 RCTs, n=10,795; RR 1.35, (0.63-2.88)
1 RCT, n=8260;RR 1.02, (0.85-1.22).
1 RCT, n=8260; RR 1.01, (0.96-1.06)
3 RCTs, n=9961; RR 1.04, (0.93-1.15)
Evidence Quality
HIGH HIGH HIGH HIGH HIGH MODERATE HIGH HIGH HIGH HIGH
Magnesium sulfate versus phenytoin
4 RCTs, 2343 women
3 RCTs, n=2291; RR 0.08, (0.01-0.60)
-- -- -- -- -- -- 1 RCT, n=2141; RR 0.58,
(0.26-1.30)
1 RCT, n=2141; RR 1.00,
(0.63-1.59)
1 RCT, n=2165; SB:
RR 0.62, (0.27-1.41)/
ND: RR 0.26, (0.03-2.31)
Evidence Quality
MODERATE MODERATE MODERATE MODERATE
Magnesium sulfate versus diazepam
2 RCTs, 66 women
2 RCTs, n=66; RR 3.00, (0.13-69.31)
-- -- -- -- -- --
Evidence Quality
VERY LOW
Magnesium sulfate versus nimodipine
1 RCT, 1650 women
1 RCT, n=1650;RR 0.33, (0.14-0.77)
-- -- -- -- -- --
Evidence Quality
LOW
Evidence summaries: treatment of eclampsia
• Three Cochrane reviews separately investigated the effects of magnesium sulfate compared to:
Diazepam (Duley et al, 2000)
Phenytoin (Duley et al, 2010a)
Lytic cocktail (Duley et al, 2010b)

Magnesium sulfate and other anticonvulsants for treatment of eclampsia- maternal outcomes
Evidence Source
Recurrence of convulsions
Maternal death
Any serious morbidity
ICU admission
Renal failure Pulm. oedema
Resp. depr. Mech. ventilation
CVA Cardiac arrest
Coma >24 hours
Magnesium sulfate versus diazepam
Cochrane review 7 RCTs, 1396 women
7 RCTs, n=1390; RR 0.43, (0.33-0.55)
6 RCTs, n=1336; RR 0.59, (0.38-0.92)
2 RCTs, n=956; RR 0.88, (0.64-1.19)
3 RCTs, n=1034;RR 0.80 (0.59, 1.07)
5 RCTs, n=1164; RR 0.85 (0.53-1.36)
3 RCTs, n=1013; RR 0.86 (0.35 to 2.07)
3 RCTs, n=1025; RR 0.86 (0.57 to 1.30)
3 RCTs, n=1025;RR 0.73, (0.45 to 1.18)
4 RCTs, n=1225; RR 0.62, (0.32-1.18)
4 RCTs, n=1085; RR 0.80 (0.41 -1.54)
--
Evidence Quality
HIGH MODERATE MODERATE MODERATEMODERATE MODERATE MODERATE MODERATEMODERATE MODERATE
Magnesium sulfate versus phenytoin
Cochrane review 6 RCTs, 972 women
6 RCTs, n=972; RR 0.34 (0.24-0.49)
3 RCTs, n=847;RR 0.50 (0.24-1.05)
1 RCT, n=775; RR 0.94 (0.73-1.20)
1 RCT, n=775; RR 0.67 (0.50-0.89)
3 RCTs, n=902;RR 1.52 (0.98-2.36)
3 RCTs, n=902; RR 0.92 (0.45-1.89)
1 RCT, n= 775;RR 0.71 (0.46-1.09)
2 RCTs, n=825; RR 0.68 (0.50-0.91)
1 RCT, n=775;RR 0.54, (0.20-1.46).
1 RCT, n=775; RR 1.16, (0.39-3.43)
--
Evidence Quality
HIGH MODERATE MODERATE HIGH MODERATE MODERATE MODERATE MODERATE
Magnesium sulfate versus lytic cocktail
Cochrane review 3 RCTs, 397 women
3 RCTs, n=397; RR 0.06 (0.03-0.12)
3 RCTs, n=397; RR 0.14 (0.03-0.59)
-- -- 2 RCTs, n=307; RR 0.64 (0.22-1.85)
-- 2 RCTs, n=198; RR 0.12 (0.02-0.91)
1 RCT, n=90; RR 0.20 (0.01-4.05)
1 trial, n=108;RR 0.22 (0.01-4.54).
2 RCTs, n=307; RR 0.26 (0.03-2.34)
1 RCT, n=108; RR 0.04 (0.00-0.74)
Evidence Quality
MODERATE MODERATE LOW MODERATE

Magnesium sulfate and other anticonvulsants for treatment of eclampsia- fetal outcomes
Evidence Source Stillbirth Neonatal death Perinatal death Admission to Special care Nursery
5 ‘ Apgar score < 7
Magnesium sulfate versus diazepam
Cochrane review 7 RCTs, 1396 women
5 RCTs, n=799; RR 0.97 (0.70-1.34)
4 RCTs, n=759; RR 1.18 (0.75-1.84)
4 RCTs, n=788 ;RR 1.04 (0.81-1.34)
3 RCTs, n=634;RR 0.92 (0.79-1.06)
3 RCTs, n=643; RR 0.70 (0.54-0.90)
Evidence Quality MODERATE HIGH HIGH
Magnesium sulfate versus phenytoin
Cochrane review 6 RCTs, 972 women
2 RCTs, n=665;RR 0.83 (0.61-1.13)
2 RCTs, n=665;RR 0.95 (0.59-1.53)
2 RCTs, n=665; RR 0.85 (0.67-1.09)
1 RCT, n=518; RR 0.73 (0.58-0.91)
1 RCT, n=518; RR 0.86 (0.52-1.43)
Evidence Quality MODERATE MODERATE MODERATE HIGH MODERATE
Magnesium sulfate versus lytic cocktail
Cochrane review 3 RCTs, 397 women
2 RCTs, n=177; RR 0.33 (0.01-7.16)
2 RCTs, n=177; RR 0.37 (0.14-1.00).
Any baby death: 2 RCTs, n=177; RR 0.35 (0.05-2.38)
-- --
Evidence Quality VERY LOW VERY LOW VERY LOW

Alternative magnesium sulfate regimens for treatment of pre-eclampsia and eclampsia
• Evidence derived from a Cochrane review of 6 RCTs involving 866 women (Duley et al, 2010c)
• 2 RCTs (451 women) compared regimens for eclampsia
• 4 RCTs (415 women) compared regimens for PE

Alternative magnesium sulfate regimens for treatment of PE and EEvidence Source
Eclampsia Maternal death
Recurrence of convulsions
Any serious morbidity
Renal failure
Resp arrest
Toxicity (Resp depr.
Calcium gluconate given
Any side effects
Stillbirth or neonatal death
Admission to SCBU
5’ Apgar score < 5
Loading dose alone versus loading dose plus maintenance regimen for women with eclampsia
1 RCT, 401 women
N/A 1 RCT, n=401; RR 0.89 (0.37-2.14)
1 RCT, n=401; RR 1.13 (0.42-3.05)
-- -- -- -- -- -- Stillbirth: 1 RCT n=401; RR 1.13 (0.66-1.92)
-- --
Quality VERY LOW VERY LOW VERY LOW
Lower dose regimens versus standard dose regimens over 24 hours for women with eclampsia
1 RCT, 50 women
N/A -- 1 RCT, n=50RR 3.00, (0.13-70.30).
-- Oliguria: 1 RCT, n=50, RR 0.20 (0.03-1.59)
-- Absent tendon reflexes: 1 RCT, n=50;RR 0.25 0.06-1.06
-- -- -- -- --
Quality VERY LOW VERY LOW
VERY LOW
Intravenous versus standard intramuscular maintenance regimen for 24 hours for women with pre-eclampsia
1 RCT, 17 women
1 RCT, n=17; RR Not estimable
-- -- -- 1 RCT, n=17; RR 3.33 (0.15-71.90)
-- 1 RCT, n=17; RR 3.33 (0.15-71.90)
-- -- 1 RCT, n=17; RR 1.25 (0.09-17.02)
-- --
Quality VERY LOW VERY LOW
VERY LOW
VERY LOW
Short versus standard (24 hours) duration of postpartum maintenance regimen for women with pre-eclampsia
3 RCTs, 398 women
3 RCTs, n=394; RR Not estimable
-- -- -- -- -- 1 RCT, n=196; RR Not estimable
-- -- -- -- --
Quality LOW LOW
Evidence Interpretation
• Evidence supports the use of magnesium sulfate in severe PE to prevent progression to eclampsia
• Clear evidence that magnesium sulfate treatment in eclampsia reduces the incidence of further fits
• Clear evidence that magnesium sulfate is more effective than diazepam, phenytoin and lytic cocktail in preventing further eclamptic fit
• No clear evidence on which MgSO4 dosage regimen is better than the other
• Most trials providing the evidence used clinical monitoring in women undergoing treatment and none used serum monitoring
Implications for clinical practice
• Development of WHO Recommendations on PE & E is currently underway
• Magnesium sulfate is the drug of choice for preventing and treating convulsions in severe PE & E (WHO 2003. Managing Complications in Pregnancy and Childbirth)
• Magnesium sulfate schedules for severe PE and eclampsia (WHO MCPC):Loading dose
4 g of 20% magnesium sulfate solution IV over 5 min Plus10 g of 50% magnesium sulfate solution IM (5 g in each buttock)
Maintenance dose 5 g of 50% magnesium sulfate solution IM into alternate buttock every four hours If 50% solution is not available, give 1 g of 20% magnesium sulfate solution IV every
hour by continuous infusion
For recurrent convulsions: 2 g of 50% magnesium sulfate IV over 5 min

THANK YOU
Top Related