






Languages
Pages
Legal


Chemotherapy and targetedagents in 1st line
Presenter
Ramon Salazar
Head of Medical Oncology Dpt.
Catalan Institute of Oncology. Barcelona. Spain

DisclosuresR. Salazar has served in a consultant or advisory role for Amgen, Merck
Serono, Roche Dx and enjoyed research funding for Roche Dx, Roche Pharma and Merck Serono

Metastatic
Palliation Acute
5-FU
BSC
Palliation Chronic
Multidisciplinary
Multi ‘optional’
Curative
6 months
> 5 years
mCRC (R)Evolution
• Slide courtesy of M Peeters.
h1

Slide 3
h1 I dont like this slide, please deleteh501wrss, 26/05/2015

Oral/IV fluoropyrimidines
Irinotecan
Oxaliplatin
Raltitrexed
Bevacizumab
Cetuximab
Panitumumab
Regorafenib
Aflibercept
An
gio
gen
esis
Gro
wth TAS-102†
Ramucirumab
Chemo Backbone:
• Slide courtesy of M Peeters.Fluorouracil (25 mg/mL injection) Summary of Product Characteristics, Hospira; Capecitabine (XELODA®), Summary of Product Characteristics, Roche; Raltitrexed (Tomudex®) Summary of Product Characteristics, Hospira; Irinotecan (Campto®) Summary of Product Characteristics, Pfizer; Oxaliplatin (Eloxatin®) Summary of Product Characteristics, Sanofi; Bevacizumab (Avastin®) Summary of Product Characteristics, Roche; Aflibercept (Zaltrap®) Summary of Product Characteristics, Sanofi; Regorafenib (Stivarga®) Summary of Product Characteristics, Bayer; Cetuximab (Erbitux®) Summary of Product Characteristics, Merck Serono; Panitumumab (Vectibix®) Summary of Product Characteristics, Amgen; PR Newswire 02-03-15. Available at: http://www.prnewswire.co.uk/news-releases/taiho-submits-tas-102-marketing-authorisation-application-to-the-european-medicines-agency-for-the-treatment-of-refractory-metastatic-colorectal-cancer-294606511.html. Accessed 21-04-15.
†Marketing Authorisation Applicationsubmitted to the to the European Medicines
Agency in March 2015 for TAS-102for use in the treatment of refractory mCRC.
h4

Slide 4
h4 TAS 102 is not antiangiogenic, is a fluoromirimidin like citotoxic, so I change its location in the graph accordinglyh501wrss, 26/05/2015

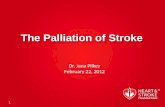
OxaliplatinEFC 4584: time to tumour progresssion
Rothenberg M, et al. Proc Am Soc Clin Oncol 2003;22:252 (abst 1011)
Rothenberg ML, et al. J Clin Oncol 2003;11:2059–69
Pro
ba
bil
ity
1.0
0.8
0.6
0.4
0.2
0
0 5 10 15 20Months
FOLFOX4 vs LV5FU2: p<0.0001
LV5FU2 vs Eloxatin®: p<0.008
5.62.6
1.9
FOLFOX4
Eloxatin®
LV5FU2

Regimen N RR PFS OSAuthor
Douillard/AIO 338 23% 4.4 14.1Douillard
+ Irinotecan 35% 6.7 17.4 Lancet
2000
FL (Saltz) 440 21% 4.3 12.6 Saltz
+ Irinotecan 39% 7.0 14.8 NEJM
2000
AIO 430 32% 6.4 16.9 Köhne
AIO+Irinotecan 54% 8.5 20.1
2003
Irinotecan

Intergroup study N9741: efficacy results
Goldberg RM, et al. J Clin Oncol 2004;22:23–30
IFL FOLFOX
Overall survival (months)
15 19.5 p=0.002
Time to progression (months)
6.9 8.7 p=0.0009
Response rate (%) 31 45 p=0.03
IFL = irinotecan, 5-FU/LV
FOLFOX = 5-FU/LV + oxaliplatin
FOLFOX also outperformed IROX

FOLFIRI followed by FOLFOX6 or the reverse sequence in
advanced colorectal cancer: a randomized GERCOR study
FOLFIRIFOLFIRI FOLFOX6FOLFOX6
OXL100 mg/m2
R
FOLFOX6FOLFOX6 FOLFIRIFOLFIRI
Prog
Prog
Prog
Prog
Tournigand C, André T, Achille E et al.J.
Clin Oncol 2004, 22 (2)
CPT11 180 mg/m2N=226

Logrank
p = 0.26
Pro
ba
bilid
ad
0.0
0.2
0.4
0.6
0.8
1.0
0 4 8 12 16 20 24 28 32
Median (months)
Folfiri 8.5
Folfox 8.0
Months
Pro
ba
bilid
ad
0.0
0.2
0.4
0.6
0.8
1.0
0 6 12 18
Months
Median (months)
Folfiri 2.5
Folfox 4.2
Logrank
p = 0.003
EFFICACY VARIABLES
TIME TO 1ST LINE PROG TIME TO 2ND LINE PROG
Tournigand C, André T, Achille E et al.J. Clin Oncol 2004, 22 (2)

Chemo Backbone 1st line
Cancer Invest. 2016;34(2):94-104. doi: 10.3109/07357907.2015.1104689. Epub 2016 Feb 11.XELOX vs. FOLFOX in metastatic colorectal cancer: An updated meta-analysis.
Guo Y1, Xiong BH2, Zhang T3, Cheng Y1, Ma L4.
• Folfiri-Folfox are the preferred options
• Simillar PFS and OS
• Sequence does not influence outcome (Tournigand)
• Xelox not inferior than Folfox
• But Folfox has prevailed probably because of differential toxicity profiles
• Pooled analysis revealed that there were no statistical differences between both arms in OS, and ORR. XELOX arm had a higher incidence of thrombocytopenia, hand-foot syndrome, and diarrhea, whereas neutropenia had a higher incidence in the FOLFOX group. For mCRC, the effect of XELOX is similar to FOLFOX.

Small molecule TKI
VEGFR-2
PP
PP
Lymphangiogenic factors
VEGF-DVEGF-C
Regorafinib†
Bevacizumab1
Anti-VEGF-A antibody
VEGF-A
Aflibercept1
VEGF-BPIGF
Fusion protein/VEGF Trap
mCRC Targeted Therapy: Anti-angiogenics
• Adapted from 1. Fakih M. Expert Rev Anticancer Ther 2013;13:427–38;Ciombor KK, et al. Pharmgenomics Pers Med 2014;7:137–44.
• †Additional targets include: PDGFR-β, FGFR1, TIE2, KIT, RET, and BRAF.PIGF, placental growth factor; TK(I), tyrosine kinase (inhibitor);VEGF(R), vascular endothelial growth factor (receptor).
No (clinical) predictive biomarker
h2

Slide 11
h2 add ramucirumab as an anti VEGFR2h501wrss, 26/05/2015

Metastatic
CRC (1rst line)
ECOG 0-1
R
IFL +
bevacizumab 5mg/kg(Q2W)
(n = 403)
IFL + placebo(Q2W)
(n = 411)Endpoints: OS; PFS, ORR, QoL,
duration of response
IFL + placebo IFL + bevacizumab p-value
1-year survival rate (%) 63.4 74.3 < 0.001
ORR (%) 34.8 44.8 0.004
Median duration of response (mo) 7.1 10.4 0.001

Xelox + placebo Xelox +
bevacizumab
FOLFOX-4 +
placebo
FOLFOX-4 +
bevacizumab
PFS HR = 0.77; 97.5 CI, 0.63 – 0.94 HR = 0.89; 97.5 CI, 0.73 – 1.08
PFS (on-treatment) HR = 0.61; 97.5 CI, 0.48 – 0.78 HR = 0.65; 97.5 CI, 0.50 – 0.84

Metastatic
CRC (1rst line)
ECOG 0-2
> 70y old
capecitabine +
bevacizumab 5mg/kg
(n = 140)
capecitabine
(n = 140)
R

Anti-EGFR mAbs Inhibit EGFR Dimerisationand Subsequent Downstream Signalling
• Berg M, Soreide K. Discov Med 2012;14:207–14;Freeman D, et al. J Clin Oncol 2008;26(Suppl 15):abstract 14536 (and poster). • ©2007 Amgen Inc. All rights reserved
EGFREGFR homodimer
RAS
GTP RAS
GDPRAF
MEK
ERK
ElkMyc
JNK
Jun
JNKK
PAK
Nck
Rac
PLCγ
PKC
PTEN
PI3K
S6K
AKT
mTOR
Proliferation
Anti-apoptosis
Survival
Angiogenesis
Metastasis
Fos
EGF
TGF-α
EGFR
Anti-EGFR mAb
(panitumumab/cetuximab)

Ligand
EGFR
Grb2
Sos Ras
BRAF
MEK
ERK
Specific mutations result in a constitutively active RAS protein

RAS
Inactive
GDP
Active
RAS
GTP
Schubbert S, et al. Nat Rev Cancer 2007;7:295−308.
Specific mutations result in a constitutively active RAS
protein
Normal:− Growth
− Proliferation
− Differentiation
RAS
Inactive
GDP
Active
RAS
GTP
Wild-type RAS
Abnormal: − Growth
− Proliferation
− Differentiation
Mutant RAS

PRIME study RAS analysis KRAS, NRAS and BRAF mutation hotspots
Based on Douillard JY, et al. N Engl J Med 2013; 369:1023-34;Oliner KS, et al. EJC 2013; 49 (suppl 3):abstract 2275 (and poster). Percentages have been rounded; 7 patients harboured either KRAS or NRAS codon 59 mutations
EXON 2 EXON 3 EXON 4EXON 1
12 13 61 117 146
EXON 2 EXON 3 EXON 4EXON 1
12 13 61 117 146
EXON 15 EXON 16EXON 1
600
40% 5% 6%
4% 4% 0%
59
59
9%
Among WT KRAS exon 2 patients, an additional 17% of tumours
with RAS mutations were found
12 13 61 117 14659
12 13 61 117 14659
600
Overall RAS
ascertainment rate: 90%
NRAS
BRAF
KRAS

Prevalence of extended RAS mutations across studies
Extended RAS
total
KRAS
Exon 3
KRAS
Exon 4
NRAS
Exon 2
NRAS
Exon 3
NRAS
Exon 4
59 61 117 146 12 13 59 61 117 146
OPUS1 26.3% 5.9% 9.3% 6.8% 5.1% 0.8%
PICCOLO1 9.8% NR 3.7% 6.3% NR NE
200204081 17.6% 4.8% 5.0% 4.2% 3.0% 1.1%
200501811 20.5% 4.6% 7.9% 2.3% 5.8% 0
PRIME1 17.4% 3.7% 5.6% 3.4% 4.1% 0
FIRE-31 16.0% 4.3% 4.9% 3.8% 2.0% 0
PEAK1 20.1% 4.1% 7.7% 5.4% 5.9% 0
COIN1 8.4% 2.1% NE 0.9% 3.0% NE
CRYSTAL1 14.7% 3.3% 5.6% 3.5% 2.8% 0.9%
SUMMARY1 19.9%
(16.7%,
23.4%)
4.3%
(3.3%, 5.5%)
6.7%
(5.7%, 7.9%)
3.8%
(3.0%, 4.8%)
4.8%
(3.4%, 6.8%)
0.5%
(0.2%, 1.2%)
CALGB1 15.3% 1.8% 5.9% 2.3% 4.2% 0
1. Sorich MJ, et al. Ann Oncol 2015;26:13–21; 2. Lenz H, et al. Ann Oncol 2014;25(suppl 4):abstract 5010 (and oral presentation)
pamitumumab
cetuximab
1st Line
Trials:

Improved outcome with better patient selectionHazard ratios KRAS exon 2 WT All RAS WT Any RAS MT
CRYSTAL1,2
PFS (p-value)
OS (p-value)
n=666
0.70 (0.0012)
0.80 (0.0093)
n=367
0.56 (0.0002)
0.69 (0.0034)
n=460
1.10 (NS)
1.05 (NS)
OPUS3,4
PFS (p-value)
OS (p-value)
n=179
0.57 (0.0064)
0.86 (0.39)
n=87
0.53 (0.063)
0.94 (0.80)
n=167
1.29 (0.013)
1.54 (0.157)
PRIME5
PFS (p-value)
OS (p-value)
n=656
0.80 (0.02)
0.83 (0.07)
n=512
0.72 (0.004)
0.78 (0.04)
n=548
1.31 (0.008)
1.25 (0.03)
PEAK6
PFS (p-value)
OS (p-value)
n=285
0.87 (0.353)
0.62 (0.009)
n=170
0.65 (0.029)
0.63 (0.058)
NA
FIRE-37
PFS (p-value)
OS (p-value)
n=592
1.06 (0.55)
0.77 (0.0017)
n=342
0.93 (0.54)
0.70 (0.011)
n=178
1.31 (0.085)
1.09 (0.60)
CALGB 804058
PFS (p-value)
OS (p-value)
n=1,137
1.04 (NS)
0.93 (NS)
n=526
1.1 (NS)
0.9 (NS)
NA
For information only. No formal statistical comparison was made. 1. Van Cutsem E, et al. 2011; 2. Ciardiello F, et al. 2014; 3.
Bokemeyer C, et al. 2011; 4. Tejpar S, et al. 2014; 5. Douillard JY, et al. 2013; 6. Schwartzberg LS, et al. 2014; 7. Stintzing S, et al.
2014; 8. Lenz H, et al. 2014.
pamitumumab
cetuximab
1st Line
Trials:

Click icon to add picture
Study design
21
Randomized Phase III trials of 1st line Erbitux + FOLFIRI1,2
1. Van Cutsem E, et al. N Engl J Med 2009;360:1408–1417;
2. Heinemann V, et al. Lancet Oncol 2014;15:1065–1075;
3. Tejpar S, et al. JAMA 2016; epub 10 Oct 2016;
4. Heinemann V, et al. Oral presentation at ESMO 2016;
5. Van Cutsem E, et al. Oral presentation at ESMO 2016
CRYSTAL and FIRE-3
*Investigator‘s choice
• Primary endpoint: PFS
Retrospective analyses of outcome by primary tumor location
were conducted for the RAS wt populations3–5
Tumor location analyses
CRYSTAL1 FIRE-32
Previously untreated EGFR-expressing
mCRC
Previously untreated KRAS (exon 2) wt
mCRC
Erbitux + FOLFIRI (n=599)
FOLFIRI alone (n=599)
Erbitux + FOLFIRI (n=297)
Bevacizumab + FOLFIRI (n=295)
R R
• Primary endpoint: Investigator-assessed ORR

Click icon to add picture
Study design
22
Open-label, randomized Phase III study: 1st line FOLFOX4 ± Erbitux in RAS wt mCRC1
FOLFOX4: Oxaliplatin 85 mg/m2, d1, q2w; LV 200 mg/m2 days 1 and 2, q2w; 5-FU 400 mg/m2 bolus, then 22h continuous infusion 600 mg/m2, days 1 and 2, q2w; Erbitux 400 mg/m2 day 1, then 250 mg/m2
qw
Previously untreated RAS wt
mCRC
No requirement for detectable tumor
EGFR expression
(n=393)
R
Endpoints:
• Primary: PFS
• Secondary: ORR, OS, safety
1. Qin S, et al. WCGC 2016 (Abstract No. O-025);
2. Qin S, et al. ESMO 2016 (Abstract No. 527P)
Prospectively planned subgroup analysis conducted to evaluate
the impact of EGFR expression on outcomes2
Erbitux + FOLFOX4
(n=193)
FOLFOX4 alone
(n=200)
Treatment until PD or unacceptable toxicity
TAILOREGFR expression

Click icon to add picture
Key
data
23
Similar outcomes with 1st line Erbitux + FOLFOX4 irrespective of EGFR expression*
(RAS wt)1
*Erbitux is indicated for treatment of patients with EGFR-expressing, RAS wt
mCRC5
†Analyzed by immunohistochemistry; 354/393 paQents (90%) were evaluable;
‡Erbitux + FOLFOX4 vs FOLFOX4 alone
1. Qin S, et al. ESMO 2016 (Abstract No. 527P);
2. Qin S, et al. WCGC 2016 (Abstract No. O-025);
3. Van Cutsem E, et al. J Clin Oncol 2015;33:692–700;
4. Van Cutsem E, et al. N Engl J Med 2009;360:1408–1417;
5. Erbitux SmPC, June/2014
% EGFR-
positive
cells†
No.
paPents‡
PFS‡ ORR‡
Medians, months HR (95% CI) % OR (95% CI)
0 85 vs 77 9.2 vs 7.9 0.62 (0.41–0.92) 67.1 vs 35.1 3.77 (1.97–7.23)
>0–10 35 vs 48 11.3 vs 7.4 0.62 (0.35–1.11) 71.4 vs 41.7 3.50 (1.38–8.88)
>10–20 15 vs 14 9.3 vs 8.1 0.45 (0.15–1.39) 73.3 vs 42.9 3.67 (0.77–17.4)
>20–35 9 vs 14 7.5 vs 9.2 1.34 (0.47–3.86) 44.4 vs 64.3 0.44 (0.08–2.46)
>35 29 vs 28 7.0 vs 5.2 0.73 (0.40–1.35) 44.8 vs 35.7 1.46 (0.50–4.24)
TAILOREGFR expression
PFS and ORR benefit with Erbitux + FOLFOX4 vs FOLFOX4 alone was
independent of EGFR expression level
Outcomes with Erbitux + CT in the subgroup without detectable EGFR expression were
comparable with those in:
(1) 1. The overall TAILOR population2
(2) 2. The RAS wt subgroup of CRYSTAL,3 which enrolled only patients with EGFR-expressing tumors4

Panitumumab randomized 1st Line TrialsTowards 40 month median OS
1. Boeckx N, et al. Ann Oncol 2016;27(Suppl 6):abstract 89P (and poster);2. Douillard JY, et al. N Engl J Med 2013;369:1023‒34;3. Schwartzberg LS, et al. J Clin Oncol 2014;32:2240‒7;4. Peeters M, et al. Clin Cancer Res 2015;21:5469‒79.
Phase 3
1st-line mCRC
Panituumab + FOLFOX4
PEAK3
(NCT00819780)
PRIME2
(NCT00364013)FOLFOX4
Panitumumab + mFOLFOX6
Bevacizumab + mFOLFOX6
Phase 2
1st-line mCRC
R
R
WT RAS
Panitumumab +
FOLFOX4
(n = 259)
FOLFOX4
(n = 253)
Median PFS, mo†2 10.1 7.9
HR
(95% CI)
P-value
0.72
(0.58–0.90)P = 0.004
Median OS, mo†2 26.0 20.2
HR
(95% CI)
P-value
0.78
(0.62–0.99)
P = 0.04
ORR, n (%)†‡3
(95% CI)
149 (59)
(52–65)
114 (46)
(40–53)
Adjusted OR
P-value
1.63
P = 0.009
AE, %2
Grade 3/4
Grade 5
(n = 256)
84.8
5.5
(n = 250)
70.0
6.4

Phase 2 PEAK study overviewmFOLFOX6 + panitumumab or bevacizumab in1st-line treatment of mCRC
1. Schwartzberg LS, et al. J Clin Oncol 2014;32:2240−7;2. Rivera F, et al. Eur J Cancer 2015;51(Suppl 3):S1‒S810:abstract 2014 (and poster).www.amgentrials.com Protocol ID: 20070509; ClinicalTrials.gov identifier: NCT00819780.
†Final analysis.WT RAS = WT KRAS and NRAS exons 2, 3, 4.
• Primary endpoint: PFS1
• No planned formalhypothesis testing
• Prespecified extendedRAS analysis1,2
• RAS ascertainment rate: 82%
WT RAS
Panitumumab
+ mFOLFOX6
(n = 88)
Bevacizumab
+ mFOLFOX6
(n = 82)
Median PFS, mo†2 12.8 10.1
HR
(95% CI)
P-value
0.68(0.48–0.96) P = 0.029
Median OS, mo†2 36.9 28.9
HR
(95% CI)
P-value
0.76
(0.53–1.11)
P = 0.15
ORR, %†2 (n = 88)
65
(n = 81)
60
OR
(95% CI)
P-value
1.12
(0.56‒2.22)
P = 0.86
AEs, %1
Grade 3/4
Grade 5
(n = 86)
89.5
4.7
(n = 80)
72.5
8.8
mCRC
WT KRAS1
(N = 285)
R
Panitumumab 6 mg/kg
(Q2W) +
mFOLFOX6 (Q2W)
Bevacizumab 5 mg/kg
(Q2W) +
mFOLFOX6 (Q2W)

Cytoreduction (shrinkage)
MOLECULAR PROFILE
Treatment of metastatic diseaseEMSO 2016 mCRC Zurich treatment algorithm
*Note: There was an error in Figure 4 of the original Epub ahead of print manuscript(version mdw235v1); the molecular profiles indicated were incorrectly labelled ‘WT’.Correction made at the final manuscript: Van Cutsem E, et al. Ann Oncol 2016; 27:1386-22
†Patients assessed as ‘fit’ or ‘unfit’ according to medical condition,not due to malignant disease; ‡Separate algorithm.
OMD, oligometastatic disease.
Assessment of clinical condition of the patient
Unfit (but may be suitable)†Fit†Unfit†
BSCGOAL
MT BRAF*MT RAS*WT RAS
Patients
with clearly
resectable
metastases
Surgery alone;
surgery with
perioperative/
postoperative
CT
Re-evaluation/assessment of response Q2M
GOAL
Cytoreduction (shrinkage)
Continue
Progressivedisease
Disease control
Continue;
maintenance;
or pause
Second-line
Surgery
Disease control (control progression)
MOLECULAR PROFILE
MT BRAF*MT RAS*WT RAS
Re-evaluaQon/assessment of response Q2−3M
Continue;
maintenance;
or pause
Progressivedisease Second-line
FP + bevacizumab;
reduced dose doublet;
anti-EGFR
OMD†
CT +
bevacizumab
Combination CT +
bevacizumab
CT doublet +
anti-EGFR
CT triplet ±
bevacizumab
CT doublet +
bevacizumab
CT doublet +
biological

Right colon
• +++ MSI-high1,2
• +++ CIMP-high1,2
• +++ CMS13
• +++ Serrated pathway2†
Molecular pathways/tumour classification modelsCIMP-high, MSI-high and CMS distribution varies between colorectal locations
1. Yamauchi M, et al. Gut 2012;61:847–54;2. Missiaglia E, et al. Ann Oncol 2014;25:1995‒2001;3. Guinney J, et al. Nat Med 2015;21:1350‒6 (and Supplementary Figure 10).
+++ denotes that a molecular or morphological subtype ismore prevalent compared with other colorectal segments.
†CIN expression and serrated pathway data are not available for rectal tumours.CIMP, CpG island methylator phenotype; CIN, chromosomal instability;
CMS, Consensus Molecular Subtypes; MSI, microsatellite instability.
Left colorectum
Colon
• +++ CIN+2†
• +++ CMS23
• +++ EREG expression2‡
• MT KRAS1
• EGFR expression1
• Molecular heterogeneity may be captured by the anatomical location of
the tumour
Right colon
• +++ MT BRAF1,2
• MT KRAS1
• EGFR expression1

Click icon to add picture
Study design
28
Randomized Phase III trials of 1st line Erbitux + FOLFIRI1,2
1. Van Cutsem E, et al. N Engl J Med 2009;360:1408–1417;
2. Heinemann V, et al. Lancet Oncol 2014;15:1065–1075;
3. Tejpar S, et al. JAMA 2016; epub 10 Oct 2016;
4. Heinemann V, et al. Oral presentation at ESMO 2016;
5. Van Cutsem E, et al. Oral presentation at ESMO 2016
CRYSTAL and FIRE-3
*Investigator‘s choice
• Primary endpoint: PFS
Retrospective analyses of outcome by primary tumor location
were conducted for the RAS wt populations3–5
Tumor location analyses
CRYSTAL1 FIRE-32
Previously untreated EGFR-expressing
mCRC
Previously untreated KRAS (exon 2) wt
mCRC
Erbitux + FOLFIRI (n=599)
FOLFIRI alone (n=599)
Erbitux + FOLFIRI (n=297)
Bevacizumab + FOLFIRI (n=295)
R R
• Primary endpoint: Investigator-assessed ORR

29
Click icon to add picture
Key
data
Unprecedented OS benefit with Erbitux + CT vs CT alone in left-sided RAS wt mCRC1,2
CRYSTAL
Tumor location analysis
RAS wt
Left-sided Right-sided
Erb + CT
(n=142)
CT alone
(n=138)
Erb + CT
(n=33)
CT alone
(n=51)
ORR
% 72.5 40.6 42.4 33.3
OR (95% CI) 3.99 (2.40–6.62) 1.45 (0.58–3.64)
p-value <0.001 0.43
PFS
Median, months 12.0 8.9 8.1 7.1
HR (95% CI) 0.50 (0.34–0.72) 0.87 (0.47–1.62)
p-value <0.001 0.66
OS
Median, months 28.7 21.7 18.5 15.0
HR (95% CI) 0.65 (0.50–0.86) 1.08 (0.65–1.81)
p-value 0.002 0.76
CT = FOLFIRI; Erb, Erbitux
Clear poor prognostic effect of right-
sided tumor location in both arms
Unprecedented OS benefit in left-
sided mCRC with Erbitux + CT vs CT
alone
1. Tejpar S, et al. JAMA Oncol 2016; epub 10 Oct 2016;
2. Van Cutsem E, et al. Oral presentation at ESMO 2016
No difference in outcomes between
arms in right-sided tumors, but
conclusions are limited by small
sample size

Click icon to add picture
Key
data
30
Unprecedented OS benefit with Erbitux + CT vs bevacizumab + CT in left-sided RAS wt
mCRC1,2
FIRE-3Tumor location analysis
1. Tejpar S, et al. JAMA Oncol 2016; epub 10 Oct 2016;
2. Heinemann V, et al. Oral presentation at ESMO 2016
RAS wt
Left-sided (n=306) Right-sided (n=88)
Erb + CT
(n=157)
Bev + CT
(n=149)
Erb + CT
(n=38)
Bev + CT
(n=50)
ORR
% 68.8 61.7 52.6 50.0
OR (95% CI) 1.37 (0.85–2.19) 1.11 (0.48–2.59)
p-value 0.23 0.83
PFS
Median, months 10.7 10.7 7.6 9.0
HR (95% CI) 0.90 (0.71–1.14) 1.44 (0.92–2.26)
p-value 0.38 0.11
OS
Median, months 38.3 28.0 18.3 23.0
HR (95% CI) 0.63 (0.48–0.85) 1.31 (0.81–2.11)
p-value 0.002 0.28
CT = FOLFIRI; Erb, Erbitux; bev, bevacizumab
Clear poor prognostic effect of right-
sided tumor location in both arms
Unprecedented OS benefit in left-
sided mCRC with Erbitux + CT, with
pronounced increase in median OS
(>10 months)
No difference in outcomes between
arms in right-sided tumors, but
conclusions are limited by small
sample size

Click icon to add picture
Key
data
31
Unprecedented OS benefit with Erbitux + CT vs bevacizumab + CT in left-sided
RAS/BRAF wt mCRC1
FIRE-3Tumor location analysis
1. Heinemann V, et al. Oral presentation at ESMO 2016
RAS/BRAF wt
Left-sided Right-sided
Erb + CT
(n=143)
Bev + CT
(n=139)
Erb + CT
(n=28)
Bev + CT
(n=37)
ORR
% 67.8 62.6 47.4 42.0
OR 1.26 1.37
p-value 0.38 0.61
PFS
Median, months 11.1 11.1 8.0 10.5
HR 0.89 1.70
p-value 0.37 0.046
OS
Median, months 38.7 28.6 18.9 23.6
HR 0.62 1.31
p-value 0.002 0.34
CT = FOLFIRI; Erb, Erbitux; bev, bevacizumab
Data consistent w RAS wt
subgroup analysis
Borderline-significant increase in PFS
with bevacizumab, but no significant
difference in OS or ORR. However,
conclusions are limited by small
sample size

Tumor location analysis
Click icon to add picture
Key
data
32
Venook AP, et al. Oral presentation at ESMO 2016
CT = Investigator’s choice of FOLFIRI or mFOLFOX6
*Adjusted for biologic, protocol CT, prior adjuvant therapy, prior RT, age, sex, synchronous disease, in place primary, liver metastases
CALGB/SWOG 80405 trial
RAS wt
Left-sided Right-sided
Erb + CT
(n=173)
Bev + CT
(n=152)
Erb + CT
(n=71)
Bev + CT
(n=78)
PFS
HR (95% CI) 0.84 (0.66–1.06) 1.64 (1.15–2.36)
p-value 0.15 0.006
Treatment × tumor location
interaction (p-value)*0.001
OS
Median, months 39.3 32.6 13.7 29.2
HR (95% CI) 0.77 (0.59–0.99) 1.36 (0.93–1.99)
p-value 0.04 0.10
Treatment × tumor location
interaction (p-value)*0.009
Longer PFS with bevacizumab vs
Erbitux, but no difference in OS
between arms, in right-sided
tumors; conclusions are limited
by small sample size
Unprecedented, significant OS benefit with Erbitux + CT vs bevacizumab
+ CT in left-sided RAS wt mCRCSignificant treatment × tumor location interaction for
PFS and OS
Clear poor prognostic effect of
right-sided tumor location on
OS in both arms
Unprecedented efficacy of Erbitux + CT vs bevacizumab + CT in left-sided RAS wt mCRC

Panitumumab outcome by tumour location analysisBackground
1. Boeckx N, et al. Ann Oncol 2016;27(Suppl 6):abstract 89P (and poster);2. Douillard JY, et al. N Engl J Med 2013;369:1023‒34;3. Schwartzberg LS, et al. J Clin Oncol 2014;32:2240‒7;
• Retrospective, exploratory analysis of outcomes by primary tumour location for patients with WT RAS and WT RAS/WT BRAF mCRC participating in:1
Phase 3
1st-line mCRC
Panituumab + FOLFOX4
PEAK3
(NCT00819780)
PRIME2
(NCT00364013)FOLFOX4
Panitumumab + mFOLFOX6
Bevacizumab + mFOLFOX6
Phase 2
1st-line mCRC
R
R

Click icon to add picture
Key
data
34
Trend for greater efficacy of 1st line panitumumab + FOLFOX vs FOLFOX in left- vs
right-sided tumors (RAS wt)1,2
Panitumumab trialsTumor location analyses
Trial
(line)Treatments
Tumor
locationPatients, n ORR, %
PFS OS
Median, monthsHR
(95% CI)*Median, months
HR
(95% CI)*
Phase III
PRIME
(1st line)
Pani + FOLFOX4
vs FOLFOX4
Left 169 vs 159 68 vs 53 12.9 vs 9.20.72
(0.57–0.90)30.3 vs 23.6
0.73
(0.57–0.93)
Right 39 vs 49 42 vs 35 7.5 vs 7.00.80
(0.50–1.26)11.1 vs 15.4
0.87
(0.55–1.37)
Phase II PEAK
(1st line)
Pani +
mFOLFOX6 vs
bev +
mFOLFOX6
Left 53 vs 54 64 vs 57 14.6 vs 11.50.65
(0.21–2.00)43.4 vs 32.0
0.84
(0.22–3.27)
Right 22 vs 14 63 vs 50 8.7 vs 12.6 0.84
(0.18–3.79)17.5 vs 21.0
0.45
(0.08–2.49)
1. Peeters M, et al. Oral presentation at ESMO 2016;
2. Boeckx C, et al. ESMO 2016 (Abstract No. 89P);
3. Rivera F, et al. ECC 2015 (Abstract No. 2014);
4. Peeters M, et al. Clin Cancer Res 2015;21:5469–5479
Bev, bevacizumab; pani, panitumumab; *Adjusted for
BRAF status, prior adjuvant CT and ECOG PS
Significant increase in OS and PFS only in the left-sided
subgroup of PRIME

Click icon to add picture
Key
data
35
Trend for greater efficacy of 1st line panitumumab + FOLFOX vs FOLFOX in left- vs
right-sided tumors (RAS/BRAF wt)1,2
Panitumumab trialsTumor location analyses
Trial
(line)Treatments
Tumor
locationPatients, n ORR, %
PFS OS
Median, monthsHR
(95% CI)Median, months
HR
(95% CI)
Phase III
PRIME
(1st line)
Pani + FOLFOX4
vs FOLFOX4
Left 156 vs 148 70.3 vs 54.8 12.9 vs 9.30.69
(0.54–0.88)32.5 vs 23.6
0.67
(0.56–0.86)
Right 26 vs 32 52.0 vs 41.2 8.9 vs 7.30.71
(0.40–1.27)22.5 vs 21.5
0.94
(0.53–1.67)
Phase II PEAK
(1st line)
Pani +
mFOLFOX6 vs
bev +
mFOLFOX6
Left 52 vs 53 63.5 vs 58.5 14.6 vs 11.50.67
(0.44–1.02)43.4 vs 32.0
0.77
(0.46–1.28)
Right 13 vs 13 69.2 vs 46.2 10.3 vs 12.60.88
(0.39–2.02)22.5 vs 23.3
0.63
(0.26–1.54)
1. Peeters M, et al. Oral presentation at ESMO 2016;
2. Boeckx C, et al. ESMO 2016 (Abstract No. 89P);
3. Rivera F, et al. ECC 2015 (Abstract No. 2014);
4. Peeters M, et al. Clin Cancer Res 2015;21:5469–5479
Data consistent with RAS wt
subgroup analysis1,2

Summary: A review of the clinical evidence
• Left versus Right
• Subgroup of Subgrup Analysis Evidence
• Anti-EGFR superior in all endpoints in the left tumors (except PFS in Fire 3)
• Right side sobgroup analysis flawed with small numbers
• CALGB and Fire 3 clearly favour Bev vs cetuximab
• (recent NCCN guidelines have deleted anti EGFR option in the right)
• PEAK phase 2 trial not clear
• Anti EGFR still increase RR on the right
• In practice, mutational status of KRAS/NRAS should be obtained upfront for mCRC to decide on the best therapeutic option
• Simillar results in RAS wt than in RAS/BRAF wt
• BRAF mutants do poorly unmet medical need
• can be treated with the same standards but clinical trials warranted
• Sequence of chemo-biological combos has not been tested
• Low use biologicals 2nd line impact OS
1. Douillard JY, et al. N Engl J Med 2013; 369:1023-342. Peeters M, et al J Clin Oncol 2014; 32 (suppl 3):LBA387 (and oral presentation).3. Patterson SD, et al. J Clin Oncol 2013; 31 (suppl):abstract 3617 (and poster).

• Population: Left colon or rectum unresectable metastatic (M1) adenocarcinoma
• Primary endpoint: OS
• Hypothesis Arm A pmab � bmab: 40 months
• Hypothesis Arm B bmab � pmab: 30 months
Phase III CR SEQUENCE conceptPlanned study designTTD-Intergroup studyPI R Salazar/A Carrato
PD, progressive disease.

Cooperative groups (CG)
Country N. Coordinator Group CountriesSites
estimated
Feasibilities II
received
Patients
per year
SpainRamón Salazar
Alfredo CarratoTTD 1 57 57 320
Portugal Helder Mansinho GICD 1 18 13 90
GreeceDemetris
PapamichaelEORTC 1* 1 20
Italy Stefano Cascinu AIOM 1 UNK 0 UNK
Germany Michel Geissler EORTC 1 15 0 90
Austria
Gerald Prager CECOG
1 4 3 20
Hungary 1 1 1 15
Bosnia
Herzegovina? 1* 1 12
Chez republic 1 1 1 12
Romania 2 1 34
Serbia 1 1 20
Slovakia ? 1 1 10
Latvia 2* 2 12
Belgium Marc Peeters BGDO 1 15 1 75
France Julien Taieb AGEO 1 11 2 36
TOTALS 8 130 85 766
* Sites without any mark under country field require study drug provision

http://ico.gencat.cat
@ICOnoticies
www.facebook.com/ICOnoticies
Institut Català d’Oncologia
ICO l’HospitaletHospital Duran i Reynals
Av. Granvia de L’Hospitalet, 199-20308908 L’Hospitalet de Llobregat
ICO BadalonaHospital Germans Trias i Pujol
Ctra. del Canyet s/n08916 Badalona
ICO GironaHospital Doctor Trueta
Av. França s/n17007 Girona
ICO Camp de Tarragona i Terres de l’EbreHospital Joan XXIIIC. Dr. Mallafrè Guasch, 4 43005 TarragonaHospital Verge de la Cinta
C. de les Esplanetes, 14 43500 Tortosa

BACK UP SLIDES

Therapeutic Progress in Advanced CRC and Improvements in OS Over Time
• Adapted from Vickers M. Oncol Exch 2013;12;30–3. • Bev, bevacizumab; BSC, best supportive care; C’mab, cetuximab; FU, fluorouracil; P’mab, panitumumab.
30
25
20
15
10
5
Ove
rall
su
rviv
al (m
onth
s)
1970 1980 1990 1995 2000 2005 2010 2013BSC
5-FUIrinotecanOxaliplatinCapcitabine Bev P’mab
C’mab Aflibercept TAS-102Regorafenib
0

Assaigs clínics: Bevacizumab
ESTUDI de Hurwitz et al. (Fase III):
Bevacizumab+IFL (irinotecan/5FU/leucovorin) vs Placebo+IFL
Resultats:
Variable principal: SG
Mediana de SG: 20,3 mesos per a bevacizumab+IFL vs 15,6 mesos per a
placebo+IFL (HR=0,66; p<0,001).
Variable secundària: SLP, taxa de resposta
Mediana de SLP: 10,6 mesos per bevacizumab+IFL vs 6,2 mesos per
placebo+IFL (HR: 0,54; p<0,001).
Taxa de resposta: 44,8% per a bevacizumab+IFL i de 34,8% per a
placebo+IFL (p=0,004).

Assaigs clínics: BevacizumabESTUDI de Saltz et al. (Fase III):
Bevacizumab+FOLFOX-4/XELOX vs FOLFOX-4/XELOX+placebo
Resultats:
Variable principal: SLP
Mediana de SLP: 9,4 mesos per a bevacizumab + XELOX/FOLFOX-4 vs 8,0 mesos
per a XELOX/FOLFOX-4 + placebo (HR: 0,83; IC 97,5%: 0,72-0,95; p=0,0023).
Variable secundària: SG, taxa de resposta
Mediana de SG: 21,3 mesos per a bevacizumab associat a XELOX/FOLFOX-4 vs
19,9 mesos per a XELOX/FOLFOX-4 (HR: 0,89; IC 97,5%: 0,76-1,03; p=0,077).
Taxa de resposta (segons un comité independent): 38% en ambdós grups de
tractament (OR: 1,0; IC97,5%:0,78-1,28; p=0,99).

Bevacizumab
• L’estudi AVEX té com a població diana pacients d’edat avançada amb CCRM
• Es va emprar capecitabina com a comparador en incloure pacients que no esconsideraven candidats a tractament amb oxaliplatí o irinotecà.
• Resultats:
SLP: capecitabina+BVZ 9,1 mesos vs capecitabina 5,1 mesos;
HR 0,53 (0,41-0,69); p<0,0001
SG: capecitabina+BVZ 20,7 mesos vs capecitabina 16,8 mesos;
HR 0,79 (0,57-1,09); p=0,18

Summary: A review of the clinical evidence
• The anti-EGFR MoAb panitumumab has (Level 1 evidence) activity in all lines of mCRC treatment:
• In 1st line in combination with FOLFOX1
• In 2nd line in combination with FOLFIRI2
• In 3rd line as single agent3
• In all lines, refinement of patient selection by expanded search for KRAS/NRAS mutations improves the risk-benefit ratio of panitumumab
• In practice, mutational status of KRAS/NRAS should be obtained upfront for mCRC to decide on the best therapeutic option
• Panitumumab is safe and increases ETS, DpR, RR in combination withchemo 1st line
• correlate both with PFS, OS and Resection Rates
• LLD: panitumumab in combination with chemotherapy is of choice
1. Douillard JY, et al. N Engl J Med 2013; 369:1023-342. Peeters M, et al J Clin Oncol 2014; 32 (suppl 3):LBA387 (and oral presentation).3. Patterson SD, et al. J Clin Oncol 2013; 31 (suppl):abstract 3617 (and poster).

Panitumumab outcome by tumour location analysisMethods (1 of 2)
Boeckx N, et al. Ann Oncol 2016;27(Suppl 6):abstract 89P (and poster). ECOG, Eastern Cooperative Oncology Group.
• Primary tumour side was ascertained either by description of:
• The primary tumour surgery in the patient case report form or
• The operative resection specimen on the pathology report
• Ascertainment of tumour side was blinded to treatment allocationand clinical outcome
• Primary tumour side categorisation:
• Right-sided: tumours located in the caecum to transverse colon (inclusive)
• Left-sided: tumours located in the splenic flexure to rectum (inclusive)
• HRs for OS and PFS were adjusted for BRAF status, adjuvant chemotherapy and ECOG performance status

PRIME study post-hoc analysis (ETS and response)
PFS and OS by ETS (30% cut-off) at Week 8(updated analysis)
Douillard JY, et al. Eur J Cancer 2015;51:1231−42.
†Includes patients with baseline and Week 8 tumour shrinkage data only;‡Assessing the overall relationship between Week 8 tumour shrinkage and PFS at 6 months;
§Assessing the overall relationship between Week 8 tumour shrinkage and OS at 2 years.
Panitumumab + FOLFOX4 FOLFOX4
ETS < 30% ≥ 30% < 30% ≥ 30%
n (%)† 89 (41) 130 (59) 138 (62) 83 (38)
Median PFS, months
(95% CI)
9.3
(6.7–10.7)
14.9
(12.8–18.6)
7.0
(5.7–7.8)
10.9
(9.3–11.7)
HR
(95% CI)
P-value
0.56
(0.42–0.76)
0.0001
0.62
(0.47–0.83)
0.0014
Phi coefficient‡ 0.30
Median OS, months
(95% CI)
18.2
(14.2–22.5)
34.5
(29.8–40.7)
16.0
(14.2–18.8)
30.7
(23.6–36.2)
HR
(95% CI)
P-value
0.52
(0.38–0.70)
< 0.0001
0.46
(0.34–0.63)
< 0.0001
Phi coefficient§ 0.33
WT RAS

Panitumumab outcome by tumour location analysisSummary of results
Boeckx N, et al. Ann Oncol 2016;27(Suppl 6):abstract 89P (and poster).
WT RAS
N pts
(left/right)
OS, months PFS, months CR + PR, %
Left Right Left Right Left Right
PRIME (Phase 3, 1st line)
Pmab + FOLFOX 169/39 30.3 11.1 12.9 7.5 68 42
FOLFOX 159/49 23.6 15.4 9.2 7.0 53 35
HR
(95% CI)
--
0.73(0.57‒0.93)
0.87(0.55‒1.37)
0.72(0.57‒0.90)
0.80(0.50‒1.26)
--
--
PEAK (Phase 2, 1st line)
Pmab + FOLFOX 53/22 43.4 17.5 14.6 8.7 64 64
Bev + FOLFOX 54/14 32.0 21.0 11.5 12.6 57 50
HR(95% CI)
--
0.84(0.22‒3.27)
0.45(0.08‒2.49)
0.65(0.21‒2.00)
0.84(0.18‒3.79)
--
--
181 (Phase 3, 2nd line)
Pmab + FOLFIRI 150/31 20.1 10.3 8.0 4.8 50 13
FOLFIRI 148/39 16.6 8.1 5.8 2.4 13 3
HR(95% CI)
--
0.96(0.74‒1.23)
1.14(0.68‒1.89)
0.88(0.69‒1.12)
0.75(0.45‒1.27)
--
--

Panitumumab outcome by tumour location analysisEfficacy outcomes by tumour location in patients with WT RAS/WT BRAF disease
Boeckx N, et al. Ann Oncol 2016;27(Suppl 6):abstract 89P (and poster).
WT RAS/
WT BRAF
PRIME PEAK Study 181
Pmab +
FOLFOX FOLFOX
Pmab +
FOLFOX Bev + FOLFOX
Pmab +
FOLFIRI FOLFIRI
Pts, n (left/right) 156/26 148/32 52/13 53/13 143/22 144/26
Median OS, months
Left 32.5 23.6 43.4 32.0 20.1 16.9
HR (95% CI) 0.67 (0.56‒0.86) 0.77 (0.46‒1.28) 0.97 (0.76‒1.26)
Right 22.5 21.5 22.5 23.3 11.9 10.9
HR (95% CI) 0.94 (0.53‒1.67) 0.63 (0.26‒1.54) 0.84 (0.46‒1.54)
Median PFS, months
Left 12.9 9.3 14.6 11.5 8.0 6.6
HR (95% CI) 0.69 (0.54‒0.88) 0.67 (0.44‒1.02) 0.89 (0.70‒1.14)
Right 8.9 7.3 10.3 12.6 6.8 3.7
HR (95% CI) 0.71 (0.4‒1.27) 0.88 (0.39‒2.02) 0.62 (0.34‒1.13)
CR + PR, %
Left 70.3 54.8 63.5 58.5 50.7 13.5
Right 52.0 41.4 69.2 46.2 19.0 3.8

Click icon to add picture
Study
design
51
US randomized Phase III trial of 1st line Erbitux + CT vs bevacizumab + CT in KRAS (exon 2) wt mCRC1,2
1. Venook AP, et al. ASCO 2014 (Abstract No. LBA3);
2. Lenz HJ, et al. ESMO 2014 (Abstract No. 501O);
3. Venook AP, et al. Oral presentation at ESMO 2016
CALGB/SWOG 80405 trial
*Investigator‘s choice
Endpoints:
• Primary: OS
• Secondary: ORR, PFS, TTF, DoR, eligibility for surgery, safety
Previously untreated KRAS (exon
2) wt mCRC
(n=1137)
Erbitux +
FOLFIRI or mFOLFOX6*
(n=578; RAS wt, n=270)
Bevacizumab +
FOLFIRI or mFOLFOX6*
(n=559; RAS wt, n=256)
R
Retrospective analysis of outcome by primary tumor location
was conducted for the RAS wt population3
Tumor location analysis

PEAK study RAS analysis Subsequent therapy (longer follow-up analysis)
Schwartzberg LS, et al. J Clin Oncol 2014;32:2240−7.
†Time to subsequent therapy is time interval from random assignment date to time of subsequent therapy; WT RAS = WT KRAS and NRAS exons 2/3/4.
Therapy received after the protocol treatment phase
Panitumumab+ mFOLFOX6
(n = 88)
Bevacizumab+ mFOLFOX6
(n = 82)
Anti-EGFR mAb
n (%) 19 (22) 30 (37)
Median time to subsequent therapy (months)† 14.7 15.4
Anti-VEGF
n (%) 35 (40) 27 (33)
Median time to subsequent therapy (months)† 13.0 10.6
Irinotecan-, oxaliplatin-, or fluoropyrimidine-containing chemotherapy
n (%) 53 (60) 50 (61)
Median time to subsequent therapy (months)† 10.5 9.7
WT RAS

PRIME study KRAS exon 2 analysis Grade 3/4 AEs of interest (primary analysis)
Douillard JY, et al. J Clin Oncol 2010;28:4697−705.AE, adverse event; MedDRA, Medical Dictionary for Regulatory Activities.
WT KRAS = WT KRAS in codons 12/13.
AE1 by MedDRA, %
WT KRAS exon 2 MT KRAS exon 2
Panitumumab+ FOLFOX4
(n = 322)FOLFOX4(n = 327)
Panitumumab+ FOLFOX4
(n = 217)FOLFOX4(n = 218)
Patients with any event 84 69 80 73
Neutropenia 42 41 37 47
Skin toxicity 36 2 30 1
Diarrhoea 18 9 20 10
Neurological toxicities 16 16 17 17
Hypokalaemia 10 5 9 4
Fatigue 9 3 7 5
Mucositis2,3 9 < 1 6 3
Hypomagnesaemia 6 < 1 6 < 1
Paronychia3 3 0 2 0
Pulmonary embolism 3 2 3 4
Febrile neutropenia4 2 2 3 3
Infusion-related reaction (panitumumab)3 < 1 - 0 -
Fatal AEs5, % 5 6 8 31Included all events regardless of relation to therapy; 2Results are based on the following pre-specified list of preferred terms: stomatitis,
mucosal inflammation, aphthous stomatitis, mouth ulceration, mucosal dryness, and mucosal ulceration; 3No grade 4; 4There was 1 Grade 5 febrile neutropenia in the panitumumab arm (MT KRAS exon 2 group); 5Includes cases in which primary cause of death was reported to be
disease progression; 2 were reported to be related to panitumumab (pneumonia and pneumonitis), both in the WT KRAS subgroup..
Top Related