







Languages
Pages
Legal

CHAPTER IICHAPTER II
Osteoporosis: Osteoporosis: treatmentstreatments

La Lettre du Rhumatologue
Results of the FREEDOM study (open-label) at 5 years
● Effects of denosumab : BMD evaluation at 5 years
● After 3 years of treatment : 2 343 "long term" group
2 207 "de novo" group
BMD increase continues at 5 years of treatment
Tolerance: no ONJ or atypical fractures in the"long term" group; 2 ONJ cases in the « de novo » group
Incidence of new NVF
BL 1 2 3 4 5 BL 1 2 3 4 5
Treatment duration (years) Treatment duration (years)
02468
101214
-2
0
2
4
6
8Lumbar BMD Total hip BMD
BM
D v
aria
tion
(%, C
I 95)
Denosumab Placebo
*
**
*
**
**
** *
*
*p < 0,002 versus placebo and baseline values
1 2 3 4 50,0
0,5
1,0
1,5
2,0
2,5
3,0
3,5
Yea
rly in
cide
nce
ofno
nver
tebr
al fr
actu
res
(%)
3,1
2,6 2,7
2,0
2,3
1,9
1,2 1,1
FREEDOM Extension study
Placebo Denosumab
Var
iatio
n de
la D
MO
(%
, IC
95)
Yearss
ASBMR 2010 - D’après Papapoulos (1025)
20Osteoporosis: treatments

La Lettre du Rhumatologue ASBMR 2010 - D’après Jamal S et al., Toronto, Canada, abstr. 1068, actualisé
Denosumab : different efficacy by level of renal function ?
● Stratification in 4 subgroups according to creatinine clearance
Antifracture efficacity of denosumab is comparable with respect to renal function No differences in incidence of adverse events
BMD variation (%)
15-29ml/mn
(n = 73)
30-59ml/mn
(n = 2 817)
60-89ml/mn
(n = 4 069)
> 90ml/mn
(n = 842)
Lumbar5.0
(-0.8-10.8)8.9
(8.4-9.3)9.0
(8.6-9.4)8.1
(7.2-8.9)
Femoral neck5.9
(3.3-8.5)5.1
(4.7-5.5)5.2
(4.9-5.5)5.6
(4.9-6.3)
Total hip5.9
(3.0-8.7)6.4
(6.1-6.7)6.4
(6.2-6.7)5.8
(5.2-6.3)
N1 3 691 3 702 33 31 1 309 1 332 1 962 1 924 394 413
All patients 15-29ml/mn
30-59 ml/mn
60-89 ml/mn
> 90 ml/mn
0
1
2
3
4
5
6
7
8
9
10
7.2
2.3
9.1
3.2
7.0
2.9
7.0
1.8
8.1
3.1
Placebo (n = 3 906) Denosumab (n = 3 902)
Inci
denc
e of
ver
tebr
al f
ract
ures
(3
yea
rs, (
%)
BMD Variation within the 4 groups over 3 years
* *
*
*
21Osteoporosis: treatments
*p < 0.05
Incidence of vertebral fractures

La Lettre du Rhumatologue
● Design: at the end of 3 years of the HORIZON study, female patients treated with zoledronic acid were randomly assigned to 2 groups : placebo (Z6 : n = 616) or continuation of treatment (Z3P3 : n = 617)
● Résultats– Difference of femoral BMD between the Z6 group and the Z3P3 placebo group = 1 %– No difference between the 2 groups for clinical fractures– Reduction of 52 % in the number of radiologic vertebral fractures (n = 14 versus n = 30) within the Z6/Z3P3 group
Zoledronic acid long-term treatment does not expose to an increased risk of side effects The question of the interest of prolonged treatment remains open
3 4,5 6
0
-0,5
-1
-1,5
0,5
2,5
2
1,5
1 Z6
Z3P3
Ans
Evo
lutio
n (%
)
1 %p < 0,001
Femoral neck BMD
0
5
10
15
Initial study (0-3 years)
Z3P3
Éxtension study(3-6 years)
Z6
PBO10,9 %
ZOL3,3 %
6,2 %(20/486)
3,0 %(14/469)
RR = 0,48IC95 (0,3 -0,9)
p = 0,03
Reduction : -52 %
New radiological vertebral fractures
Fem
ale
patie
nts
(%)
HORIZON study 6-year extension
ASBMR 2010 - D’après Black (1070)
22Osteoporosis: treatments
La Lettre du Rhumatologue ASBMR 2010 - D’après Black D et al., San Francisco, États-Unis, abstr. 1028, actualisé
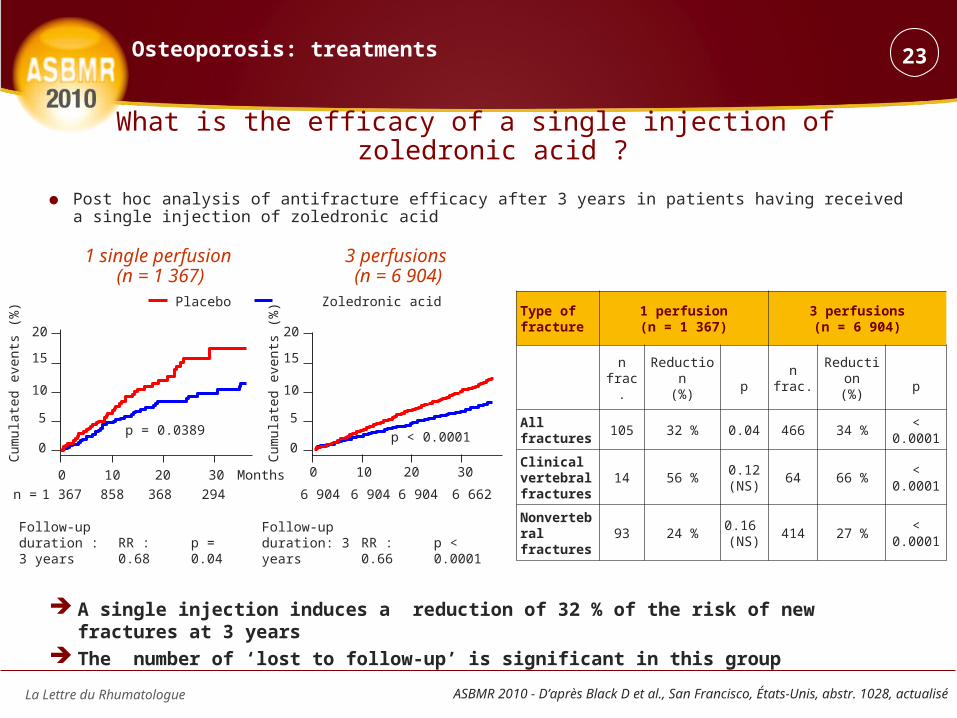
What is the efficacy of a single injection of zoledronic acid ?
● Post hoc analysis of antifracture efficacy after 3 years in patients having received a single injection of zoledronic acid
A single injection induces a reduction of 32 % of the risk of new fractures at 3 years The number of ‘lost to follow-up’ is significant in this group
0 10 20 30
0
5
10
15
20
0 10 20 30
0
5
10
15
20
Zoledronic acidPlacebo
p = 0.0389 p < 0.0001
1 367 858 368 294 6 904 6 904 6 904 6 662n =
1 single perfusion (n = 1 367)
3 perfusions (n = 6 904)
Follow-up duration : 3 years
Type of fracture
1 perfusion(n = 1 367)
3 perfusions(n = 6 904)
nfrac.
Reduction(%) p
nfrac.
Reduction(%) p
All fractures
105 32 % 0.04 466 34 % < 0.0001
Clinical vertebral fractures
14 56 %0.12(NS)
64 66 % < 0.0001
Nonvertebral fractures
93 24 %0.16 (NS)
414 27 % < 0.0001
Cum
ulat
ed e
vent
s (%
)
RR : 0.68 p = 0.04Follow-upduration: 3 years
RR : 0.66 p < 0.0001
23Osteoporosis: treatments
Cum
ulat
ed e
vent
s (%
)
Months
La Lettre du Rhumatologue
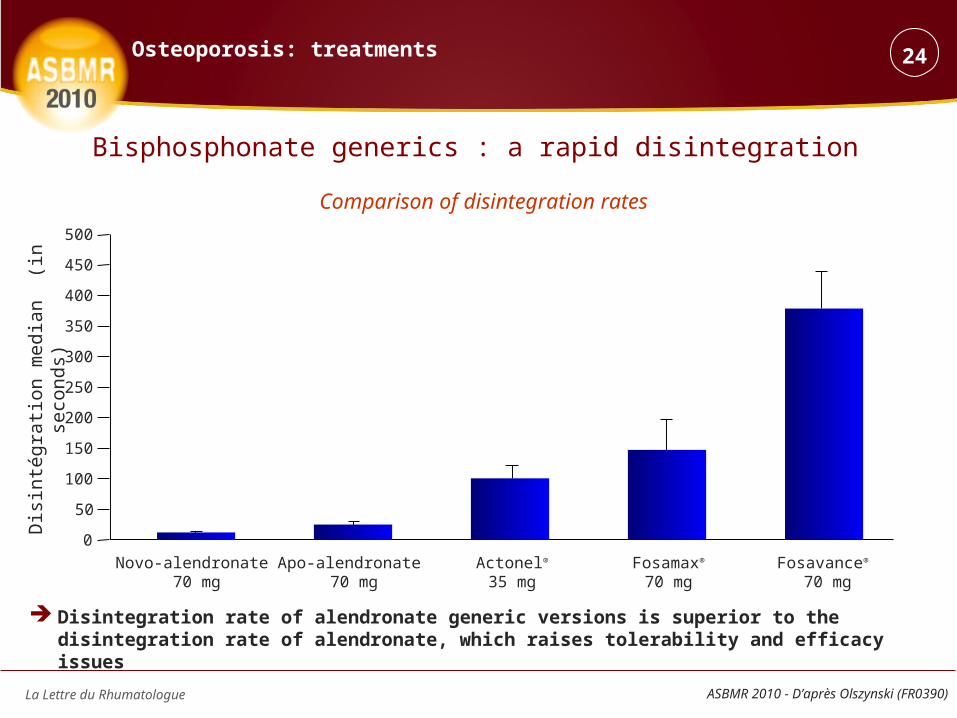
Disintegration rate of alendronate generic versions is superior to the disintegration rate of alendronate, which raises tolerability and efficacy issues
Dis
inté
grat
ion
me
dian
(in
se
con
ds)
Comparison of disintegration rates
Novo-alendronate 70 mg
Apo-alendronate 70 mg
Actonel®
35 mgFosamax®
70 mgFosavance®
70 mg
0
50
100
150
200
250
300
350
400
450
500
Bisphosphonate generics : a rapid disintegration
ASBMR 2010 - D’après Olszynski (FR0390)
24Osteoporosis: treatments

La Lettre du Rhumatologue
Diagnostic criteria for atypical femoral fracture
● Major criteria– Fracture line in a proximal site should be under the lesser trochanter and , in distal
site, over the femoral condyles– It should be a nontraumatic fracture, or following a low-energy trauma– Fracture line should be transversal or oblique, with a < 30° angle– It should be a noncomminuted fracture– Complete fractures involve the entire crossection of the bone, from one cortical to
the other, with a possible internal « thorn » – Incomplete fractures affect only the external cortical
Exclusion criteria: femoral neck fractures, intertrochanteric fractures with a subtrochanteric extension, periprosthetic or pathological fractures within the context of primary bone tumors or bone metastasis
All major criteria are required for diagnosis The minor criteria are not necessary (for diagnosis) but sometimes (we) come across their association
Minor criteria– Periosteal reaction on the external cortical– Increase of cortical thickness– Dull pain prodromes in thigh s and inner thighs– Bilateral fracture– Delayed cicatrization– Associated comorbidities : rheumatoid arthritis, vitamin D insufficiency, hypophosphatasia…– Associated therapies : bisphosphonates, corticoids, proton pump inhibitors …
Medial spine
Short-oblique configuration
Noncomminuted
ASBMR 2010 – Task Force concernant les fractures fémorales atypiques (16 octobre 2010)
25Osteoporosis: treatments
La Lettre du Rhumatologue
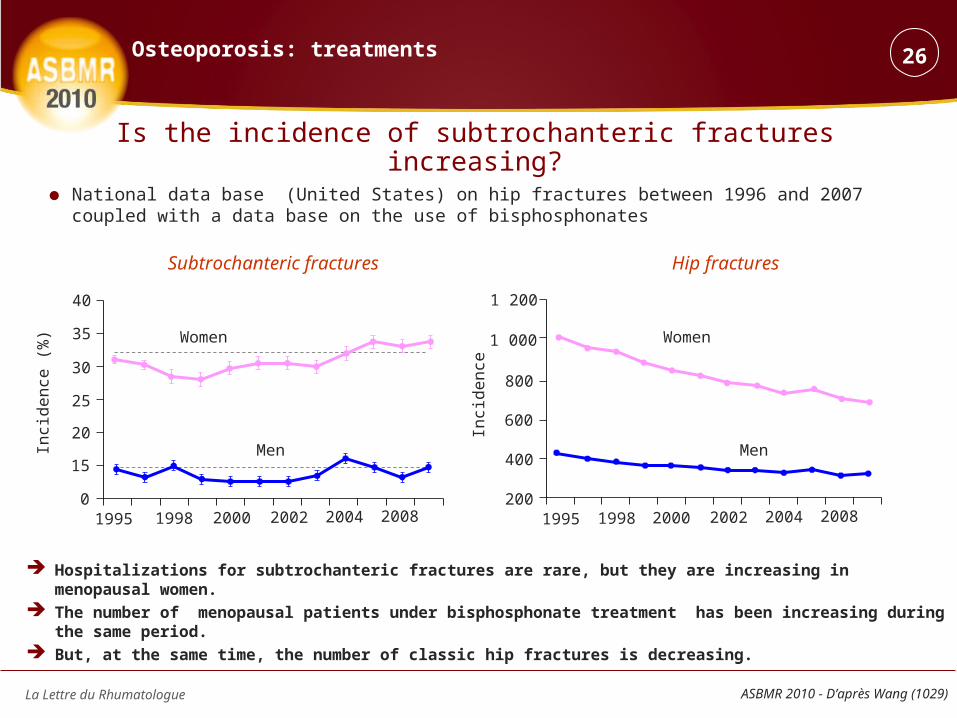
Is the incidence of subtrochanteric fractures increasing?
● National data base (United States) on hip fractures between 1996 and 2007 coupled with a data base on the use of bisphosphonates
Hospitalizations for subtrochanteric fractures are rare, but they are increasing in menopausal women. The number of menopausal patients under bisphosphonate treatment has been increasing during the same period. But, at the same time, the number of classic hip fractures is decreasing.
19950
1998 2000 2002 2004 2008 1995 1998 2000 2002 2004 2008
15
20
25
30
35
40
200
400
600
800
1 000
1 200
Inci
de
nce
Inci
de
nce
(%
) Women
Men
Women
Men
Subtrochanteric fractures Hip fractures
ASBMR 2010 - D’après Wang (1029)
26Osteoporosis: treatments

La Lettre du Rhumatologue
For these atypical femoral fractures,
● no association with alendronate in the New Zealand study
● an apparent association between BP and atypical fractures in the Australian study, but with a very weak frequency of the latter
● treatment benefits prevail over potential risk
● 2 retrospective monocenter 5-year studies : radiographic analysisNew Zealand study : 71 subtrochanteric and diaphyseal fractures, of which 11 atypical fractures
Alendronate median duration not specified
All BP : RR = 2.1 (0.5-8.2), p = 0.16
Australian study : 152 subtrochanteric and diaphyseal fractures, of which 20 atypical fractures
Alendronate median duration 5.1 years
All BP : RR = 37.4 (12.9-119), p < 0.001
Atypical (11) Typical (60)
Age (years) 81 (66-96) 81 (44-100)
Men/Women 1/10 11/49
Alendronate 4 8
Etidronate 0 5
Calcium 6 18
Vitamin D 6 14
Glucocorticoïds 2 5
IPP 0 4
Fracture background 6 28
Total Diaphyse Subtrochanter Distal
Atypical 20 15 5 0
Typical 132 15 65 52
BisphosphonatesAlendronate
(median duration)Risedronate
(median duration)
Atypical(n = 20)
17 (85 %)15
(5.1 ans)2
(3 ans)
Typical(n = 132)
3 (2.3 %) 2 (3.5 ans) 1 (1 an)
ASBMR 2010 - D’après Warren (1030) et Girgis (1071)
27Osteoporosis: treatments
Are patients who received long acting bisphosphonates at risk for atypical fractures ?

La Lettre du Rhumatologue
What is the incidence of subtrochanteric and diaphyseal fractures before and after treatment against osteoporosis ?
● National Danish registry, matched-centrals study● Each user of an antiosteoporosis treatment between 1996 and 2006 (n = 103 562) was matched,
after adjustment for age and sex, with 3 controls (n = 310 683)
There was an increased risk for subtrochanteric and diaphyseal fractures before starting the treatment against osteoporosis. This increased risk was especially high in the year preceding start of treatment.
With alendronate, such increased risk diminishes progressively with treatment.
Alendr
onat
e
Clodro
nate
Étidro
nate
Iban
dron
ate
Pamidr
onat
ePTH
Raloxif
ene
Risedr
onat
e
Stront
ium
Zoledr
onat
e0
4
8
12
16
20
IRR
(IC
95)
0
1
2
3
4
5
6
7
> 10
year
s
5-10
year
ss
1-5
year
s
< 1y
earn
< 1
year
1-5
year
s
> 5
year
ss
Before and after periods
IRR
(IC
95) Before
After
Subtrochanteric fractures and alendronate
ASBMR 2010 - D’après Vestergaard (1072)
28Osteoporosis: treatments
La Lettre du Rhumatologue ASBMR 2010 - D’après Kelly (FR0355)
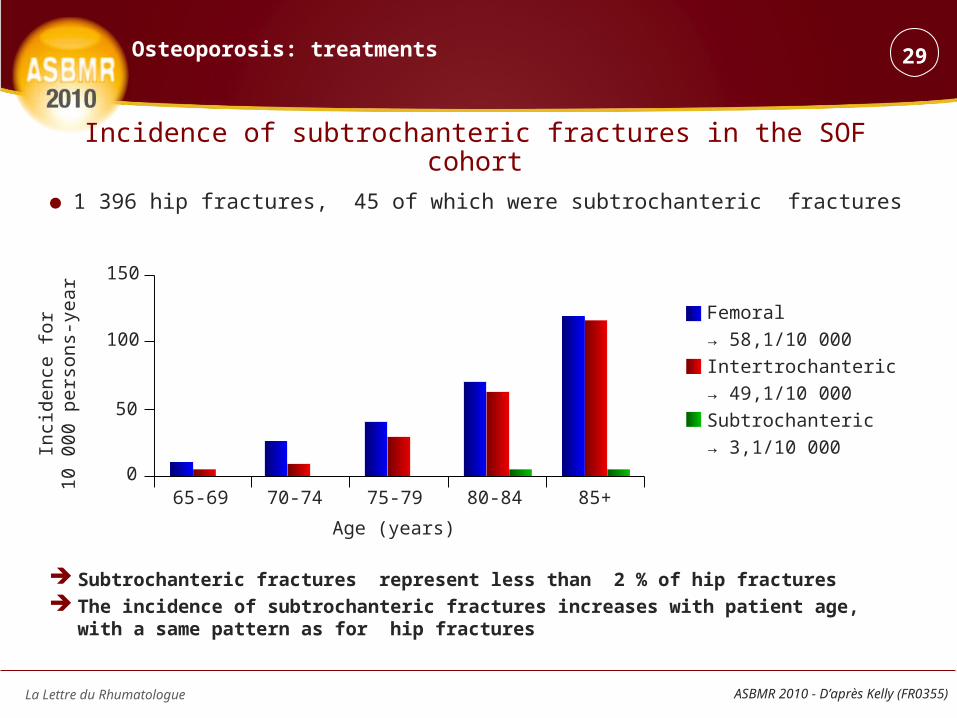
Incidence of subtrochanteric fractures in the SOF cohort
● 1 396 hip fractures, 45 of which were subtrochanteric fractures
Subtrochanteric fractures represent less than 2 % of hip fractures The incidence of subtrochanteric fractures increases with patient age, with a same pattern as
for hip fractures
Femoral
→ 58,1/10 000
Intertrochanteric
→ 49,1/10 000
Subtrochanteric
→ 3,1/10 000
0
50
100
150
65-69 70-74 75-79 80-84 85+
Age (years)
Inci
denc
e fo
r10
000
pe
rso
ns-y
ear
29Osteoporosis: treatments

La Lettre du Rhumatologue
Breast cancer risk is reduced with alendronate
● Cohort study from a Danish national registry● Women > 50 years,without cancer history that have been treated with alendronate from 1996 to 2005
– 30 606 users– 4 centrals matched for to age and sex (n = 122 424)
This national registry, based on a cohort study, shows a significant reduction of the risk of developping and dying from breast cancer in postmenopausal women treated with alendronate
0
1
2
3
Co
mb
ine
d I
nci
de
nce
(%
)
0 2 4 6 8 Years
Controls
Alendronate
Diagnostic of breast cancerRR = 0.74 (0.66-0.84) ; p < 0.001
Death due to breast cancerRR = 0,52 (0,40-0,68) ; p < 0,001
ASBMR 2010 - D’après Abrahamsen (SU0128)
30Osteoporosis: treatments
La Lettre du Rhumatologue
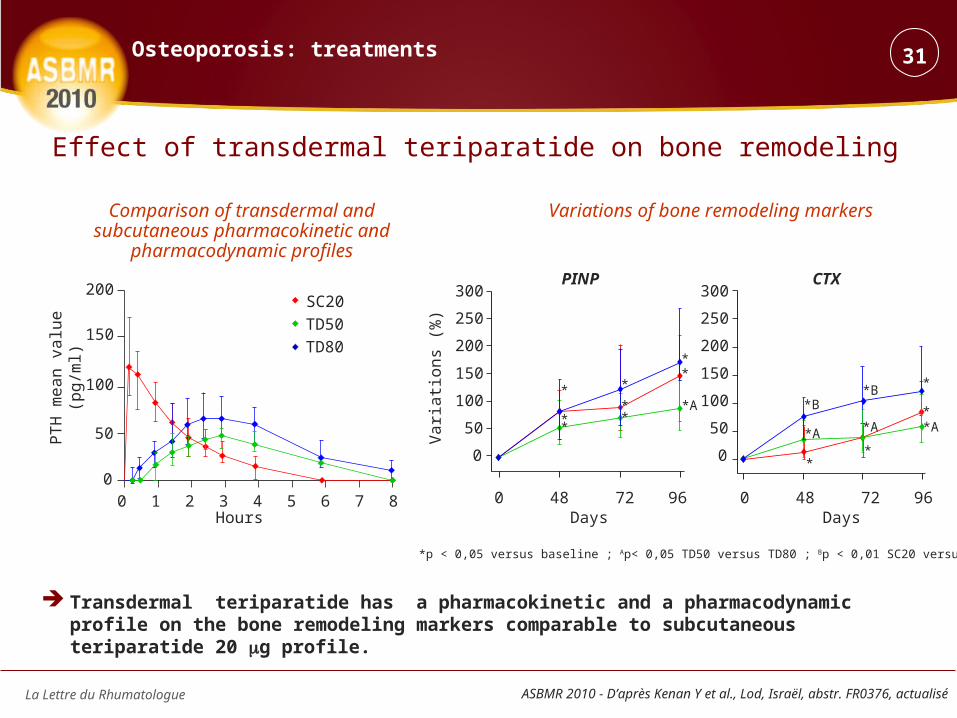
Comparison of transdermal and subcutaneous pharmacokinetic and
pharmacodynamic profiles
Transdermal teriparatide has a pharmacokinetic and a pharmacodynamic profile on the bone remodeling markers comparable to subcutaneous teriparatide 20 g profile.
Variations of bone remodeling markers
PT
H m
ea
n v
alu
e
(pg
/ml)
Hours
Va
riatio
ns
(%)
ASBMR 2010 - D’après Kenan Y et al., Lod, Israël, abstr. FR0376, actualisé
0 1 2 3 4 5 6 7 80
50
100
150
200SC20
TD50
TD80
0 48 72 96 0 48 72 96
0
50
100
150
200
250
300
0
50
100
150
200
250
300PINP CTX
DaysDays
31Osteoporosis: treatments
Effect of transdermal teriparatide on bone remodeling
*B
*A
*
*B
*A
*
*
**A
*
**
*
**
**
*A
*p < 0,05 versus baseline ; Ap< 0,05 TD50 versus TD80 ; Bp < 0,01 SC20 versus TD80

La Lettre du Rhumatologue ASBMR 2010 - D’après Gee AH et al., Cambridge, Royaume-Uni, abstr. 1250, actualisé
What is the impact of teriparatide on the cortical bone of women with osteoporosis?
● In vivo study using High Resolution Cortical Thickness mapping● 65 women (median age: 67.5 years) from the EUROFORS study, treated with teriparatide for 2 years
At 24 months teriparatide increases the cortical thickness of
● Tension zones involved in walking (muscle insertion sites)
● Upper part of the cortical, critical zone for the susceptibility to hip fracture risk
Mapping and significance of cortical thickness modifications (besides the femoral head)
24 months - baselineThickness variations (%)
-2 0 2 4 6 8 0,05 0,025 0p for topographic distribution(a) p = 0,00000004(b) p = 0,00007 (c) p = 0,00007
32Osteoporosis: treatments
La Lettre du Rhumatologue
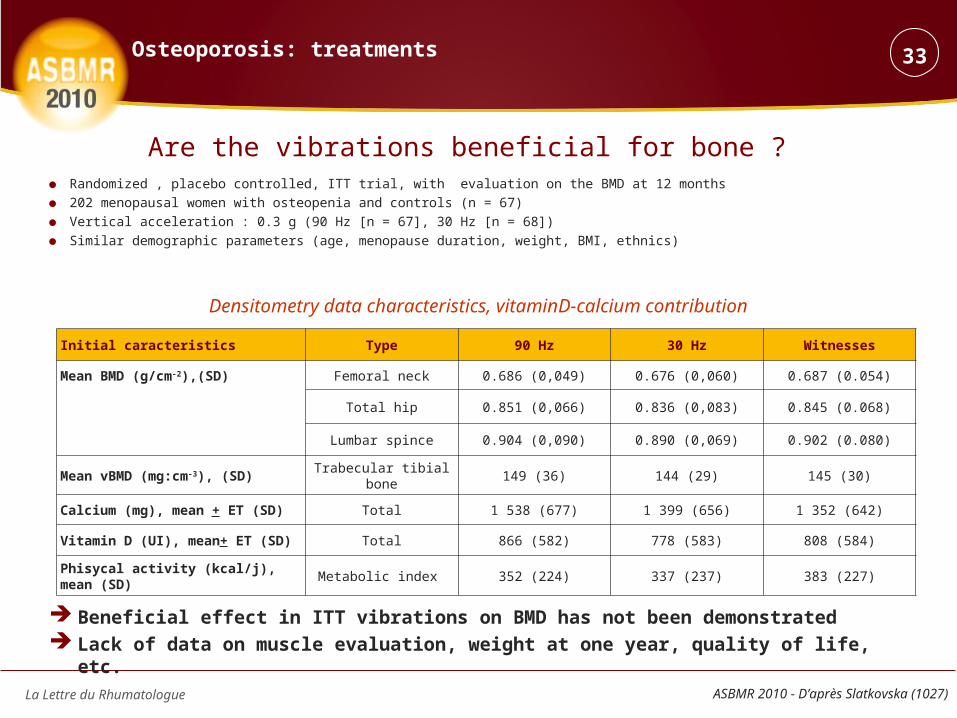
Are the vibrations beneficial for bone ? ● Randomized , placebo controlled, ITT trial, with evaluation on the BMD at 12 months
● 202 menopausal women with osteopenia and controls (n = 67)
● Vertical acceleration : 0.3 g (90 Hz [n = 67], 30 Hz [n = 68])
● Similar demographic parameters (age, menopause duration, weight, BMI, ethnics)
Beneficial effect in ITT vibrations on BMD has not been demonstrated Lack of data on muscle evaluation, weight at one year, quality of life, etc.
Densitometry data characteristics, vitaminD-calcium contribution
Initial caracteristics Type 90 Hz 30 Hz Witnesses
Mean BMD (g/cm-2),(SD) Femoral neck 0.686 (0,049) 0.676 (0,060) 0.687 (0.054)
Total hip 0.851 (0,066) 0.836 (0,083) 0.845 (0.068)
Lumbar spince 0.904 (0,090) 0.890 (0,069) 0.902 (0.080)
Mean vBMD (mg:cm-3), (SD) Trabecular tibial bone 149 (36) 144 (29) 145 (30)
Calcium (mg), mean + ET (SD) Total 1 538 (677) 1 399 (656) 1 352 (642)
Vitamin D (UI), mean+ ET (SD) Total 866 (582) 778 (583) 808 (584)
Phisycal activity (kcal/j), mean (SD) Metabolic index 352 (224) 337 (237) 383 (227)
ASBMR 2010 - D’après Slatkovska (1027)
33Osteoporosis: treatments

La Lettre du Rhumatologue ASBMR 2010 - D’après Jamal S et al., Toronto, Canada, abstr. 1252, actualisé
NTG seems to have beneficial effects on bone remodeling and BMD at 24 months
BMD variations at 24 months Markers variations at 12 months
34Osteoporosis: treatments
An explosive treatment… nitroglycerin (NTG) !
Var
iatio
ns (
%)
Lumbar spine
Femoral neck
Var
iatio
ns (
%)Urinary NTX
Var
iatio
ns (
%)
Var
iatio
ns (
%) PAL osseuses
0 3 12
0 3 12 240
50
100
150
80
100
120
140
160
50,8 %(43,7 à 60,2)
21,3 %(21,6 à 22,1)
-2
0
2
4
6
8
10
10
8
6
4
2
0
-2
12 24
12 24
Months
Months
Mois
Months
7,0 %(5,5 à 8,5)
6,7 %(5,2 à 8,2)
Placebo NTG ointment
Top Related